-
8/3/2019 NCM Renal Disorders
1/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Chapter 44
Management of Patients WithRenal Disorders
-
8/3/2019 NCM Renal Disorders
2/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Acute Renal Failure
Acute renal failure (ARF) is a sudden and almostcomplete loss of
kidney function (decreased GFR) over a
period of hours to days. Oliguria (less than 400 mL/day of
urine) is the most
common clinical situation seen in ARF; anuria (less than50
mL/day of urine).
Increase serum creatinine and BUN levels and retentionof other
metabolic waste products (azotemia) normallyexcreted by the
kidneys.
-
8/3/2019 NCM Renal Disorders
3/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Causes of Acute Renal Failure
Hypovolemia
Hypotension
Reduced cardiac output and heart failure
Obstruction of the kidney or lower urinary tract
Obstruction of renal arteries or veins
-
8/3/2019 NCM Renal Disorders
4/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins4
Acute Renal Failure Acute renal failure is a sudden, usually
reversible deterioration in normal renalfunction.
It can be classified according to underlyingcause as:
1. Prerenal:
a. Hypovolemia.
b. Impaired cardiac efficiency.
c. Vasodilatation.
-
8/3/2019 NCM Renal Disorders
5/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins5
Acute Renal Failure (contd)
2. Postrenal obstruction:
a. Urinary tract obstruction.
b. Tumors.
3. Intrarenal:
a. Acute nephritis.
b. Antibiotics.
c. NSAIDs.
-
8/3/2019 NCM Renal Disorders
6/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins6
Acute Renal Failure (contd)
Diagnostic Evaluation:
1. Serum creatinine levelthe most reliablemeasure of the GFR,
found to be rising
2. Radionuclide studies to evaluate GFR and
renal
blood flow and distribution
3. Urinalysisreveals proteinuria, hematuria,
casts
-
8/3/2019 NCM Renal Disorders
7/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
Phases of Acute Renal Failure
-
8/3/2019 NCM Renal Disorders
8/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
Initiation
Begins with the initial insult to the kidney
-
8/3/2019 NCM Renal Disorders
9/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
Oliguria Rise in the serum concentration of substances
usuallyexcreted by the kidneys
urea, creatinine, uric acid, inorganic acids and the
intracellular cations (potassium and magnesium) Minimum needed
for elimination of metabolic waste
products 400 ml / day
Uremic symptoms appear
Hypokalemia develops
Nonoliguric forms are found after nephrotoxicantibiotics, burns,
traumatic injury, halogenatedanesthetic agents
-
8/3/2019 NCM Renal Disorders
10/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
DiuresisGradually the urinary output increases because
the glomerular filtration has started recovering
Laboratory values stop rising
Uremic symptoms may continue
Watch for dehydration
-
8/3/2019 NCM Renal Disorders
11/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
Recovery
Improvement in renal function
May take 3 to 12 months
Lab values return to normal gradually
-
8/3/2019 NCM Renal Disorders
12/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
Clinical Manifestations of ARF
appear critically ill and lethargic, with persistent
nausea,vomiting, and diarrhea.
The skin and mucous membranes are dry fromdehydration, and the
breath may have the odor of urine(uremic fetor).
Central nervous system signs and symptoms include
drowsiness, headache, muscle twitching, and seizures.
-
8/3/2019 NCM Renal Disorders
13/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
-
8/3/2019 NCM Renal Disorders
14/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
-
8/3/2019 NCM Renal Disorders
15/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
15
Acute Renal Failure (contd) Treatment:
1. Correction of any reversible cause of acuterenal failure (ie,
surgical relief ofobstruction)
2. Correction and control of fluid andelectrolyte imbalances
3. Restoration and maintenance of stable
vital signs
4. Maintenance of nutrition with low-sodium,low- potassium,
low-phosphate, moderate-protein diet
-
-
8/3/2019 NCM Renal Disorders
16/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
Nursing Management
MONITORING FLUID AND ELECTROLYTE BALANCE
paying careful attention to fluid intake (intravenousmedications
should be administered in the smallestvolume possible), urine
output, apparent edema,distention of the jugular veins, alterations
in heartsounds and breath sounds, and increasing difficultyin
breathing.
Accurate daily weights, as well as intake and outputrecords, are
essential.
-
8/3/2019 NCM Renal Disorders
17/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
Nursing Management
MONITORING FLUID AND ELECTROLYTE BALANCE
Hyperkalemia is treated with glucose and insulin,calcium
gluconate, cation-exchange resins(Kayexalate), or dialysis. Fluid
and other electrolytedisturbances are often treated with
hemodialysis,peritoneal dialysis, or other continuous
renalreplacement therapies..
-
8/3/2019 NCM Renal Disorders
18/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
Nursing Management
REDUCING METABOLIC RATE
Bed rest may be indicated to reduce exertion and themetabolic
rate during the most acute stage of thedisorder. Fever and
infection, both of which increasethe metabolic rate and catabolism,
are prevented ortreated promptly
PROMOTING PULMONARY FUNCTION assisted to turn, cough, and take
deep breaths
frequently to prevent atelectasis and respiratory
tractinfection.
-
8/3/2019 NCM Renal Disorders
19/72Copyright 2010 Wolters Kluwer Health | Lippincott Williams
& Wilkins
Nursing Management
PREVENTING INFECTION
Asepsis is essential with invasive lines and cathetersto
minimize the risk of infection and increasedmetabolism.
An indwelling urinary catheter is avoided wheneverpossible
because of the high risk for UTI associated
with its use.
-
8/3/2019 NCM Renal Disorders
20/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Nursing Management
PROVIDING SKIN CARE
Massaging bony prominences, turning the patientfrequently, and
bathing the patient with cool water
are often comforting and prevent skin breakdown. PROVIDING
SUPPORT
The purpose and rationale of the treatments areexplained to the
patient and family by the physician.
High levels of anxiety and fear, however, maynecessitate
repeated explanation and clarification bythe nurse.
The family members may initially be afraid to touchand talk to
the patient during the procedure but
should be encouraged and assisted to do so.
-
8/3/2019 NCM Renal Disorders
21/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins21
Chronic Renal Failure
Chronic renal failure is irreversible destructionof nephrons so
that they are no longer
capable of maintaining normal fluid andelectrolyte balance.
Causes:
1. Recurrent UTIs.
2. Toxic agents.
3. Diabetic nephropathy.
-
8/3/2019 NCM Renal Disorders
22/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins22
Chronic Renal Failure (contd)
Complications:
1. Azotemia/uremianitrogen waste productsaccumulating in blood.
Toxic levels manifestthemselves in many ways such as coma,
headache, gastrointestinal disturbances,neuromuscular
disturbances.
2. Metabolic acidosisas a result of decreasingGFR
3. Electrolyte imbalance
4. Severe anemiakidneys unable to stimulateerythropoietin;
uremic toxins depleteerythrocytes; nutritional deficiencies.
5. Hypertensionrenal ischemia stimulates
-
8/3/2019 NCM Renal Disorders
23/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins23
Chronic Renal Failure (contd)
Clinical Manifestations:
1. Decreased appetite and energy level
2. Increased urinary output and fluidintake
3. Bone or joint pain
4. Delayed or absent sexual maturation
5. Growth retardation
-
8/3/2019 NCM Renal Disorders
24/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins24
Chronic Renal Failure (contd)
Diagnostic Evaluation:
Determine extent of disease; monitorprogression.
1. Serum studies
a. Decreased hematocrit, hemoglobin, Na+,Ca++;
increased K+, phosphorous
b. As renal function declines, BUN, uric acid,
-
8/3/2019 NCM Renal Disorders
25/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins25
Chronic Renal Failure (contd)
2. Urine studies:
a. Specific gravityincreased or decreased
b. 24-hour urine for creatinine clearance isdecreased
(increased creatinine in urine) reflectingdecreased
GFR.
c. Changes in total output
-
8/3/2019 NCM Renal Disorders
26/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins26
Chronic Renal Failure (contd)
Treatment:
1. Correction of calcium phosphorousimbalance. Administer
activated vitamin D toincrease calcium absorption and
calciumphosphate binders with meals to bind
phosphate in the gastrointestinal tract.
2. Correction of acidosis with buffers such asBicitra
3. Diets should meet caloric needs of the child
-
8/3/2019 NCM Renal Disorders
27/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins 27
Chronic Renal Failure (contd)
4. Correction of anemia through the use oferythropoietin
(Epogen) administered
subcutaneously at home
5. Growth retardation should be evaluated forpossible use of
growth hormone.
6. Treatment options for end-stage renaldisease are
hemodialysis, peritoneal dialysis,or transplantation.
7. Institute dialysis therapy while transplant-
-
8/3/2019 NCM Renal Disorders
28/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins 28
Chronic Renal Failure (contd)
Nursing Management:
A. Ensuring Safety
1. Protect the patient from the effects ofdecreased
level of consciousness and involuntarymovements
by maintaining crib or bed side rails upand padded,
as necessary.
-
8/3/2019 NCM Renal Disorders
29/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins 29
Chronic Renal Failure (contd)
B. Educating About Chronic RenalFailure
1. Because numerous issues may interferewith the
patient's psychological and socialdevelopment and
education, help the patient and familyto cope with:
a. Uncertainty regarding the course of thedisease and
ultimate prognosis.
-
8/3/2019 NCM Renal Disorders
30/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Nursing Process: The Care of the Patientwith Renal
FailureDiagnoses
Excess fluid volume
Imbalanced nutrition
Deficient knowledge
Risk for situational low self-esteem
-
8/3/2019 NCM Renal Disorders
31/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Nursing Process: The Care of the Patientwith Renal
FailurePlanning
Goals may include maintaining of IBW without excessfluid,
maintenance of adequate nutritional intake,
increased knowledge, participation of activity withintolerance
improved self-esteem, and absence ofcomplications.
-
8/3/2019 NCM Renal Disorders
32/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Excess Fluid Volume
Assess for signs and symptoms of fluid volume excess,and keep
accurate I&O and daily weights
Limit fluid to prescribe amounts
Identify sources of fluid
Explain to patient and family the rationale for
therestriction
Assist patient to cope with the fluid restriction
Provide or encourage frequent oral hygiene
-
8/3/2019 NCM Renal Disorders
33/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Imbalanced Nutrition
Assess nutritional status; weight changes and lab data
Assess patient nutritional patterns and history; note
foodpreferences
Provide food preferences within restrictions
Encourage high-quality nutritional foods whilemaintaining
nutritional restrictions
Assess and modify intake related to factors thatcontribute to
altered nutritional intake, eg, stomatitis oranorexia
Adjust medication times related to meals
-
8/3/2019 NCM Renal Disorders
34/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Risk for Situational Low Self Esteem
Assess patient and family responses to illness andtreatment
Assess relationships and coping patterns
Encourage open discussion about changes and concerns
Explore alternate ways of sexual expression
Discuss role of giving and receiving love, warmth,
andaffection
-
8/3/2019 NCM Renal Disorders
35/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
DIALYSIS
used to remove fluid and uremic waste products from thebody when
the kidneys cannot do so.
The need for dialysis may be acute or chronic.
Acute dialysis is indicated when there is a high and risinglevel
of serum potassium, fluid overload, or impendingpulmonary edema,
increasing acidosis, pericarditis, and
severe confusion. It may also be used to remove
certainmedications or other toxins (poisoning or
medicationoverdose) from the blood.
-
8/3/2019 NCM Renal Disorders
36/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
DIALYSIS
Chronic or maintenance dialysis is indicated in chronicrenal
failure, known as end-stage renal disease (ESRD),
in the following instances: the presence of uremic signsand
symptoms affecting all body systems (nausea andvomiting, severe
anorexia, increasing lethargy, mentalconfusion), hyperkalemia,
fluid overload not responsiveto diuretics and fluid restriction,
and a general lack ofwell-being.
-
8/3/2019 NCM Renal Disorders
37/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
HEMODIALYSIS
most commonly used method of dialysis
It is used for patients who are acutely ill and require
short-term dialysis (days to weeks) and for patients withESRD
who require long-term or permanent therapy. Adialyzer (once
referred to as an artificial kidney) servesas a synthetic
semipermeable membrane, replacing therenal glomeruli and tubules as
the filter for the impaired
kidneys.
Treatments usually occur three times a week for at least3 to 4
hours per treatment
-
8/3/2019 NCM Renal Disorders
38/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
HEMODIALYSIS
Diffusion, osmosis, and ultrafiltration are the principleson
which hemodialysis is based.
The toxins and wastes in the blood are removed bydiffusionthat
is, they move from an area of higherconcentration in the blood to
an area of lowerconcentration in the dialysate.
The dialysate is a solution made up of all the
importantelectrolytes in their ideal extracellular
concentrations.
-
8/3/2019 NCM Renal Disorders
39/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
HEMODIALYSIS
Excess water is removed from the blood by osmosis, inwhich water
moves from an area of higher solute
concentration (the blood) to an area of lower
soluteconcentration (the dialysate bath).
Ultrafiltration is defined as water moving under highpressure to
an area of lower pressure. This process ismuch more efficient at
water removal than osmosis.
Because patients with renal disease usually cannotexcrete water,
this force is necessary to remove fluid toachieve fluid
balance.
-
8/3/2019 NCM Renal Disorders
40/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
HEMODIALYSIS
Dialyzers, or artificial kidneys, are either flat-platedialyzers
or hollow-fiber artificial kidneys that contain
thousands of tiny cellophane tubules that act assemipermeable
membranes. T
he blood flows through the tubules, while a solution
(thedialysate) circulates around the tubules. The exchange ofwastes
from the blood to the dialysate occurs through
the semipermeable membrane of the tubules .
-
8/3/2019 NCM Renal Disorders
41/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
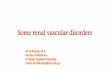
Hemodialysis System
-
8/3/2019 NCM Renal Disorders
42/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
VASCULAR ACCESS
Access to the patients vascular system must beestablished to
allow blood to be removed, cleansed, and
returned to the patients vascular system at ratesbetween 200 and
800 mL/minute.
-
8/3/2019 NCM Renal Disorders
43/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
VASCULAR ACCESS
SUBCLAVIAN, INTERNAL, JUGULAR, AND FEMORALCATHETERS
Immediate access to the patients circulation for
acutehemodialysis is achieved by inserting a double-lumen
ormultilumen catheter into the subclavian, internal jugular,or
femoral vein.
Although this method of vascular access involves somerisk (eg,
hematoma, pneumothorax, infection,thrombosis of the subclavian
vein, and inadequate flow),it can be used for several weeks.
-
8/3/2019 NCM Renal Disorders
44/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Hemodialysis Catheter
-
8/3/2019 NCM Renal Disorders
45/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
VASCULAR ACCESS
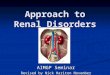
FISTULA
A more permanent access, known as a fistula, is created
surgically (usually in the forearm) by joining(anastomosing) an
artery to a vein, either side to side orend to side
The fistula takes 4 to 6 weeks to mature before it is
ready for use.
-
8/3/2019 NCM Renal Disorders
46/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
VASCULAR ACCESS
GRAFT
An arteriovenous graft can be created by subcutaneously
interposing a biologic, semibiologic, or synthetic graftmaterial
between an artery and vein
The most commonly used synthetic graft material isexpanded
polytetrafluoroethylene (PTFE).
Grafts are usually placed in the forearm, upper arm, orupper
thigh.
Infection and thrombosis are the most commoncomplications of
arteriovenous grafts
-
8/3/2019 NCM Renal Disorders
47/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Internal Arteriovenous Fistula and Graft
-
8/3/2019 NCM Renal Disorders
48/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
COMPLICATIONS OF HEMODIALYSIS
atherosclerotic cardiovascular disease, heart failure,coronary
heart disease and anginal pain, stroke, andperipheral vascular
insufficiency, anemia and fatigue,gastric ulcers and other
gastrointestinal problems occurfrom the physiologic stress of
chronic illness, medication,sleep problems
-
8/3/2019 NCM Renal Disorders
49/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
COMPLICATIONS OF HEMODIALYSIS
Hypotension may occur during the treatment as fluid isremoved.
Nausea and vomiting, diaphoresis, tachycardia,and dizziness are
common signs of hypotension.
Painful muscle cramping may occur, usually late indialysis as
fluid and electrolytes rapidly leave theextracellular space.
Exsanguination may occur if blood lines separate ordialysis
needles accidentally become dislodged.
Dysrhythmias may result from electrolyte and pHchanges or from
removal of antiarrhythmic medicationsduring dialysis.
-
8/3/2019 NCM Renal Disorders
50/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
COMPLICATIONS OF HEMODIALYSIS
Air embolism is rare but can occur if air enters thevascular
system.
Chest pain may occur in patients with anemia orarteriosclerotic
heart disease.
Dialysis disequilibrium results from cerebral fluid shifts.
Signs and symptoms include headache, nausea and
vomiting, restlessness, decreased level of consciousness,and
seizures. It is more likely to occur in acute renalfailure or when
blood urea nitrogen levels are very high(exceeding 150 mg/dL)
-
8/3/2019 NCM Renal Disorders
51/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
NURSING MANAGEMENT
MEETING PSYCHOSOCIAL NEEDS
give the patient and family the opportunity to
express feelings of anger and concern over thelimitations that
the disease and treatment imposeand over possible financial
problems and jobinsecurity.
PROMOTING HOME AND COMMUNITY-BASED CARE
Good communication between the dialysis staff (inthe hospital
and outpatient clinic), unit staff, andhome care nurses is
essential for providing sound,continuous care.
-
8/3/2019 NCM Renal Disorders
52/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Peritoneal Dialysis
The goals of peritoneal dialysis are to remove toxicsubstances
and metabolic wastes and to re-establishnormal fluid and
electrolyte balance.
Patients with diabetes or cardiovascular disease, manyolder
patients, and those who may be at risk for adverseeffects of
systemic heparin are likely candidates forperitoneal dialysis.
With this method, instead of being cleaned by an
artificialmembrane outside the body, the blood is cleaned insidethe
body, through the Peritoneum. This is the thinmembrane that
surrounds the outside of the organs inthe abdomen.
http://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/glossary.php
-
8/3/2019 NCM Renal Disorders
53/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Peritoneal Dialysis
The peritoneum allows waste products to pass through itand is
very rich in small blood vessels. By running adialysis fluid into
the peritoneal cavity, through a tubecalled a Tenckhoff Catheter -
and then out again - wastecan be filtered from the blood.
What is the Peritoneal Dialysis Fluid?
Peritoneal dialysis fluid is a sugar (glucose)
solutioncontaining other salts. Bags come in 3 strengths
(1.36%,2.27% and 3.86% or light, medium and heavy) - the"heavier"
the bag (ie.3.86%), more water will beremoved from the body.
http://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/glossary.php
-
8/3/2019 NCM Renal Disorders
54/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Peritoneal Dialysis
If you have a lot of fluid in the body, you would useheavy bags
to remove fluid. If you are dehydrated, youwould use some light
bags so that the dialysis does notremove fluid.
The sugar solution can be a problem for diabetic patientsand
changes in therapy may be needed. New solutionsare being developed
- Protein or starch.
http://www.kidneypatientguide.org.uk/site/glossary.phphttp://www.kidneypatientguide.org.uk/site/GoodNutrition.phphttp://www.kidneypatientguide.org.uk/site/GoodNutrition.phphttp://www.kidneypatientguide.org.uk/site/glossary.php
-
8/3/2019 NCM Renal Disorders
55/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Peritoneal Dialysis
-
8/3/2019 NCM Renal Disorders
56/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Peritoneal Dialysis
-
8/3/2019 NCM Renal Disorders
57/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Complications of Peritoneal Dialysis
Peritonitis (inflammation of the peritoneum) is the mostcommon
and most serious complication of peritonealdialysis.
characterized by cloudy dialysate drainage, diffuseabdominal
pain, and rebound tenderness.
one to three rapid exchanges with a 1.5% dextrosesolution
without added medications are completed towash out mediators of
inflammation and to reduceabdominal pain.
Antibiotic therapy continues for 10 to 14 days.
-
8/3/2019 NCM Renal Disorders
58/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Complications of Peritoneal Dialysis
LEAKAGE
Leakage of dialysate through the catheter site may occur
immediately after the catheter is inserted.
dialysis is withheld for several days to give the incisionand
exit site time to heal.
-
8/3/2019 NCM Renal Disorders
59/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Complications of Peritoneal Dialysis
BLEEDING
A bloody effluent (drainage) may be observed
occasionally
The hypertonic fluid pulls blood from the uterus, throughthe
opening in the fallopian tubes, and into the peritonealcavity.)
Bleeding is common during the first fewexchanges after a new
catheter insertion because someblood exists in the abdominal cavity
from the procedure.
-
8/3/2019 NCM Renal Disorders
60/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Question
Is the following statement True or False?
Failure of the temporary dialysis access accounts for
mosthospital admissions of patients undergoing
chronichemodialysis.
-
8/3/2019 NCM Renal Disorders
61/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Answer
False
Failure of the permanent, not the temporary, dialysisaccess
accounts for most hospital admissions of patientsundergoing chronic
hemodialysis.
-
8/3/2019 NCM Renal Disorders
62/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Nursing Management of the Hospitalized
Patient on Dialysis (1 of 2)
Protection of vascular access; assess site for patency andsigns
of potential infection, and do not use for bloodpressure or blood
draws.
Monitor fluid balance indicators and monitor IV
therapycarefully; accurate I&O, IV administration pump.
Assess for signs and symptoms of uremia and
electrolyteimbalance; regularly check lab data.
Monitor cardiac and respiratory status carefully.
Hypertension: monitor blood pressure,antihypertensive agents
must be held on dialysisdays to avoid hypotension.
-
8/3/2019 NCM Renal Disorders
63/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Nursing Management of the Hospitalized
Patient on Dialysis (2 of 2)
Monitor all medications and medication dosages carefully.Avoid
medications containing potassium and magnesium.
Address pain and discomfort.
Stringent infection control measures.
Dietary considerations: sodium, potassium, protein, andfluid;
address individual nutritional needs.
Skin care: pruritis is a common problem; keep skin cleanand well
moisturized, and trim nails and avoid scratching.
CAPD catheter care.
-
8/3/2019 NCM Renal Disorders
64/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Kidney Surgery
A patient may undergo surgery to remove obstructionsthat affect
the kidney (tumors or calculi), to insert atube for draining the
kidney (nephrostomy,ureterostomy), or to remove the kidney involved
inunilateral kidney disease, renal carcinoma, orkidney
transplantation.
-
8/3/2019 NCM Renal Disorders
65/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Kidney Surgery
Preoperative considerations Patient preparation to ensure that
optimal renal
function is maintained is mandatory.
Fluids are encouraged to promote increased
excretion of waste products before surgery,
unlesscontraindicated
If kidney infection is present preoperatively, wide-spectrum
antimicrobial agents may be prescribed toprevent bacteremia.
Antibiotic agents must be given
with extreme care because many are toxic to thekidneys.
Coagulation studies (prothrombin time, partialthromboplastin
time, platelet count) may be
indicated if the patient has a history of bruising
andbleeding.
-
8/3/2019 NCM Renal Disorders
66/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Kidney Surgery
Perioperative concerns
Renal surgery requires various patient positions to
expose the surgical site adequately.
Postoperative management
Potential hemorrhage and shock
Because the kidney is a highly vascular organ Fluid and blood
component replacement is
frequently necessary in the immediatepostoperative period to
treat intraoperative bloodloss
-
8/3/2019 NCM Renal Disorders
67/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Kidney Surgery
Potential abdominal distention and paralytic ileus
Abdominal distention is relieved by decompression
through a nasogastric tube
Oral fluids are permitted when the passage offlatus is noted
Potential infection
Potential thromboembolism
Low-dose heparin therapy may be initiated
-
8/3/2019 NCM Renal Disorders
68/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Patient Positioning and Incisional
Approaches
-
8/3/2019 NCM Renal Disorders
69/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Renal Transplantation
-
8/3/2019 NCM Renal Disorders
70/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Postoperative Nursing Management
Assessment: include all body systems, pain, fluid andelectrolyte
status, and patency and adequacy of urinarydrainage system
Diagnoses: ineffective airway clearance, ineffectivebreathing
pattern, acute pain, fear and anxiety, impairedurinary elimination,
and risk for fluid imbalance
Complications: bleeding , pneumonia, infection, and DVT
-
8/3/2019 NCM Renal Disorders
71/72
Copyright 2010 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Interventions
Pain relief measures and analgesic medications
Promote airway clearance and effective breathing patternby
appropriate pain relief, deep breathing coughingexercises, and
incentive spirometry and positioning
Monitor UO and maintain potency of urinary drainagesystems
Use strict asepsis with catheter and appropriatetechnique in
providing all care
Monitor for signs and symptoms of bleeding
Encourage leg exercises, early ambulation, and monitorfor signs
of DVT
-
8/3/2019 NCM Renal Disorders
72/72
Patient Teaching
Instruct both patient and family
Drainage system care
Strategies to prevent complications
Signs and symptoms
Follow-up care
Fluid intake
Health promotion and health screening