Embed Size (px)
Citation preview

MelanomaTreatment Guidelines for Patients
Version IV/ January 2008


The mutual goal of the National Comprehensive Cancer Network® (NCCN®) andthe American Cancer Society (ACS) partnership is to give patients and the generalpublic state-of-the-art cancer treatment information in a language that is easy tounderstand. This information, based on the NCCN’s Clinical Practice Guidelines,is meant to help you talk with your doctor about your treatment. These guide-lines do not replace your doctor’s expertise and clinical judgment . Each patient’ssituation must be evaluated individually. It is important to discuss the guidelinesand all information about treatment options with your doctor.
MelanomaTreatment Guidelines for Patients
Version IV/ January 2008

The NCCN Clinical Practice Guidelines are developed for health professionalsby a diverse panel of experts. These guidelines are a statement of the authors’consensus regarding the scientific evidence and their views of currently acceptedapproaches to treatment. The NCCN guidelines are updated as new informationbecomes available. The patient information version is updated accordingly andis available on-line through the NCCN and the ACS Web sites. To be sure youhave the most recent version, contact the NCCN at 1-888-909-NCCN or the ACSat 1-800-ACS-2345.
©2008 by the National Comprehensive Cancer Network (NCCN) and the AmericanCancer Society (ACS). All rights reserved. The information herein may not bereprinted in any form for commercial purposes without the express writtenpermission of the ACS. Single copies of each page may be reproduced for personaland non-commercial uses by the reader.

Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Making decisions about melanoma treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
About the skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Types of skin cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Tests and exams for melanoma diagnosis and work up (evaluation) . . . . . . . . . . 8
Melanoma stages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Types of treatment for melanoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Complementary and alternative therapies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
About Clinical Trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Other things to consider during and after treatment . . . . . . . . . . . . . . . . . . . . . . . . 19
Protecting your skin from sun exposure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Checking your skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Work-up (evaluation) and treatment guidelines . . . . . . . . . . . . . 23Decision trees
Work-up (evaluation) of melanoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Work-up and treatment of lower stage melanoma (in situ, and stages I and II) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Work-up and treatment for higher stages of melanoma: stages III and IV . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Follow-up after initial treatment of melanoma . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Treatment of recurrent melanoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Treatment of melanoma with distant metastasis . . . . . . . . . . . . . . . . . . . . . . . . 40

City of Hope
Dana-Farber/Brigham and Women’s Cancer Center Massachusetts General Hospital Cancer Center
Duke Comprehensive Cancer Center
Fox Chase Cancer Center
Huntsman Cancer Institute at the University of Utah
Fred Hutchinson Cancer Research Center/Seattle Cancer Care Alliance
Arthur G. James Cancer Hospital and Richard J. Solove Research Institute at The Ohio State University
The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins
Robert H. Lurie Comprehensive Cancer Center of Northwestern University
Memorial Sloan-Kettering Cancer Center
H. Lee Moffitt Cancer Center & Research Institute
Roswell Park Cancer Institute
Siteman Cancer Center at Barnes-Jewish Hospital and Washington University School of Medicine
St. Jude Children’s Research Hospital/University of Tennessee Cancer Institute
Stanford Comprehensive Cancer Center
University of Alabama at Birmingham Comprehensive Cancer Center
UCSF Helen Diller Family Comprehensive Cancer Center
University of Michigan Comprehensive Cancer Center
UNMC/Eppley Cancer Center at The Nebraska Medical Center
The University of Texas M.D. Anderson Cancer Center
Vanderbilt-Ingram Cancer Center
Member Institutions

Introduction
This booklet was written to give patientsinformation about the way melanoma istreated at the nation’s leading cancer centers.Originally developed for cancer specialists bythe National Comprehensive Cancer Network(NCCN), these treatment guidelines havenow been written in an easier-to-understandversion by the American Cancer Society(ACS). To get more copies of these guidelines,call the ACS at 1-800-ACS-2345 or the NCCNat 1-888-909-NCCN, or visit these organiza-tions’ Web sites at www.cancer.org (ACS) andwww.nccn.org (NCCN).
Since 1995, doctors have looked to theNCCN for advice on treating cancer. The NCCNClinical Practice Guidelines were developedby a diverse panel of experts from 21 of thenation’s leading cancer centers.
For more than 90 years, the public hasrelied on the American Cancer Society forinformation about cancer. The Society’sbooks, brochures, and Web pages providecomprehensive, current, and understandableinformation to hundreds of thousands ofpatients, their families, and friends. Thiscollaboration between the NCCN and ACSprovides an authoritative and understandablesource of cancer treatment information forthe general public. These patient guidelineswill help you better understand how to makedecisions about your cancer care that areimportant to you.
These patient guidelines will help you bet-ter understand your cancer treatment options.We urge you to discuss them with your doctor.After reading these guidelines, you might startby asking the following questions:
• What is my cancer’s stage?• Where is my cancer located? • How far has my cancer spread? • How does the stage influence my
outlook for cure and survival and mytreatment options?
• What treatment options do I have? • What are the risks or side effects
associated with each of my treatmentoptions, and how are they likely toaffect my quality of life?
• What should I do to be ready for treatment, reduce side effects of treatment, and hasten my recovery?
• When will I be able to return to normalactivities?
• Are there any clinical trials that Ishould consider?
In addition to these questions, be sure towrite down some of your own. For instance,you might want more information about howlong it will take you to recover from surgeryso you can plan your work schedule. Or youmay want to ask about clinical trials.
Making decisions aboutmelanoma treatment
The American Cancer Society estimates thataround 60,000 new melanomas are diagnosedin the United States each year. The number ofnew melanomas diagnosed in the US everyyear is increasing. Since 1973, the incidencerate for melanoma (the number of newmelanomas diagnosed per 100,000 peopleeach year) has more than doubled and themortality rate for melanoma (the number of
5

deaths from melanoma per 100,000 peopleeach year) has increased. The good news isthat melanoma mortality rates have onlyslightly increased during the past 10 years.
Although melanoma is a serious disease,it can be treated and cured. It is importantthat you receive care from a team of healthcare professionals who are experienced intreating melanoma. This team may include adermatologist, surgeon, medical oncologist,radiation oncologist, pathologist, nurse, radi-ologist, and social worker — often along withyour primary care doctor.
The information in this booklet is intendedto help you understand your options fortreatment of melanoma so that you and yourcancer care team can work together todecide which treatment is best for you.
On the pages after the general informationabout melanoma, you will find flowchartsthat doctors call “Decision Trees.” The chartsrepresent different stages of melanoma. Eachone shows you step-by-step how you and yourdoctor can arrive at the choices you need tomake about your treatment.
To reach an informed decision, you needto understand some of the medical termsthat your doctors use. You may feel you’re onfamiliar ground already, or perhaps you needto refer to the various sections listed in thetable of contents. In this booklet you will findnot only background information on melan-oma, but also explanations of melanomastages, work-up (evaluation), and treatments— all categories used in the flowcharts.
6
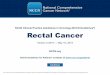
Figure 1. The layers of the skin
Epidermis
Sweat gland
Lymph vesselHair follicle
Blood vessel
Sweat glandBasal cell
Melanocyte
Squamous cell
Epidermis
Dermis
Subcutis

About the skin
The skin has 3 layers: epidermis, dermis, andsubcutis (see Figure 1). The top layer is theepidermis. The epidermis is very thin, aver-aging only 0.2 mm (about 1⁄100 of an inch). Itprotects the deeper layers of skin and theorgans of the body from the environment.
The outermost part of the epidermis iscalled the stratum corneum, or horny layer. Itis made up of dead cells of the epidermis thatare continually shedding. Below the stratumcorneum are layers of living cells called squa-mous cells. These cells form an importantprotein called keratin. Keratin is part of theskin’s ability to protect the rest of the body.The lowest part of the epidermis, the basallayer, is formed by basal cells. These cells con-tinually divide to form new cells to replacethe older ones that wear off the skin’s surface.
Melanoma comes from cells calledmelanocytes that are also present in the epi-dermis. These skin cells produce the protectivepigment called melanin. Melanin gives a tanor brown color to the skin and helps protectthe deeper layers of the skin from the harmfuleffects of the sun. The basal lamina separatesthe epidermis from the deeper layers of skin.
The middle layer of the skin is called thedermis. The dermis is much thicker than theepidermis. It contains hair follicles, sweatglands, blood vessels, and nerves that are heldin place by a protein called collagen. Collagen,which is made by skin cells called fibroblasts,gives the skin its resilience and strength.
Below the skin is the subcutis. The subcutisand the lowest part of the dermis form a net-work of collagen and fat cells. The subcutis
conserves heat and has a shock-absorbingeffect that helps protect the body’s organsfrom injury.
Types of skin cancer
Skin cancers are divided into 2 general types:melanoma and non-melanoma. Non-melanoma skin cancers (usually basal cell andsquamous cell cancers) are the most commoncancers of the skin. They are called non-melanoma skin cancer because they developfrom skin cells other than melanocytes.Because they rarely spread elsewhere in thebody, they are treated differently.
Melanoma is a cancer that begins in themelanocytes, the cells that produce the skincoloring or pigment known as melanin.Because most melanoma cells still producemelanin, melanoma tumors are often brownor black. Although melanoma is much lesscommon than basal cell and squamous cellcancers, it can be more dangerous. Melanoma,like basal cell and squamous cell cancers, isalmost always curable in its early stages. But,melanoma is much more likely than basal orsquamous cell cancer to spread to otherparts of the body.
Melanomas can occur anywhere on theskin, but are more likely to develop in certainlocations. The trunk is the more common sitein men. In women, the legs are more com-monly affected. Having darkly pigmentedskin lowers the risk of being diagnosed withmelanoma, but it is not a guarantee that youwill not develop melanoma. Anyone, includingpeople with dark skin, can develop this
7

cancer on the palms of the hands, soles of thefeet, and under the nails. Melanomas of thepalms, soles, and nails represent about halfof all melanomas in African Americans butfewer than 10% of melanomas in whites.
Tests and exams formelanoma diagnosis andwork-up (evaluation)
How is melanoma diagnosed? Any new skin wound (lesion), or change, spot,or growth on your skin could be melanoma.Your doctor will examine it and other testswill be used to find out whether it ismelanoma, non-melanoma, or some otherskin condition. An exact diagnosis can onlybe made by a biopsy of the skin
History and physical examination Usually the first step is for your doctor to takeyour medical history which will include ques-tions about your symptoms and risk factors.The doctor will ask when the skin lesion firstappeared and whether it has changed in sizeor appearance. You may also be asked aboutpast exposures to known causes of melanomaand whether anyone in your family has hadmelanoma.
During the physical examination, yourdoctor will note the size, shape, color, andtexture of the area in question and look forany bleeding or scaling. The rest of your bodywill be checked for spots and moles that maybe related to melanoma. The doctor will alsoexamine lymph nodes near the abnormalarea of skin. Lymph nodes, also called lymphglands, are small bean-shaped collections of
immune system tissue that are found alonglymphatic vessels. Enlarged lymph nodesmay suggest the spread of a melanoma tothese structures.
If your doctor is not a specialist in skindisorders (a dermatologist), you may be sentto one for further evaluation and a biopsy.
Types of skin biopsy If the doctor thinks a melanoma might bepresent, he or she will take a sample of skinfrom the suspicious area to be looked atunder a microscope. This is called a skinbiopsy. There are different ways to take thesample of your skin. The choice depends onthe size of the affected area and its locationon your body. Any biopsy is likely to leave ascar. Because different methods producedifferent types of scars, you should ask thedoctor about biopsies and scarring before theprocedure is done. Skin biopsies are doneusing a local anesthetic. Which means onlythe involved area will be numbed with medi-cine. When this is done you will likely feel asmall needle stick and a little burning withsome pressure for less than a minute.
All skin biopsy samples are looked at undera microscope. The skin sample is sent to apathologist, a doctor who has been speciallytrained in the microscopic examination anddiagnosis of tissue samples. Often, the skinsample is sent to a dermatopathologist, adermatologist or pathologist who has hadextra training in making diagnoses from skinsamples and may be more experienced withcertain skin cancers than a general pathologist.He or she will determine if the cells lookdysplastic, that is, abnormal, or if they looklike they may become cancerous.
8

Incisional and excisional biopsies An incisional biopsy removes only a part ofthe tumor. If the entire tumor is removed, itis called an excisional biopsy. A narrow rimof normal skin (called the margin) is takenwith this biopsy for further examination, andthe edges of the wound are sewn together.Both types of biopsies can be done usinglocal anesthesia. Excisional biopsy is themethod usually preferred when melanoma issuspected.
Punch biopsy A punch biopsy removes a small sample ofskin. The doctor uses a punch biopsy tool thatlooks like a tiny, round cookie cutter. Oncethe skin is numbed with a local anesthetic,the doctor rotates the punch biopsy tool onthe surface of the skin until it cuts through allthe layers of the skin, including the epidermis,dermis, and the upper parts of the subcutis.Punch biopsy may be appropriate for areassuch as the palm, sole, finger, toe, face, ear, orfor very large lesions.
Shave biopsy After numbing the area with a local anesthetic,the doctor “shaves” off the top layers of theskin (the epidermis and part of the dermis)with a surgical blade. A shave biopsy is usefulin diagnosing many types of skin diseases andin treating benign (non-cancerous) moles.However, if an invasive melanoma is suspected,a shave biopsy sample may not be deepenough to precisely measure its thickness ordepth of invasion. If melanoma is suspected,a shave biopsy is usually not done.
Blood tests There are no specific blood tests formelanoma, but sometimes a blood test forLDH (lactate dehydrogenase) levels might behelpful. LDH is an enzyme found in the bloodthat may be elevated when a lot of cancer cellsare present or when the liver has been damagedby cancer. Blood LDH levels can be a markerfor widespread melanoma. LDH levels areseldom elevated when the melanoma is firstdiagnosed.
Imaging tests These tests use x-rays, magnetic fields, orradioactive substances to create pictures ofthe inside of the body to look at the extent ofspread of the cancer. Imaging tests such ascomputed tomography (CT) scans, magneticresonance imaging (MRI) scans, and positronemission tomography (PET) scans may be usedto see whether the melanoma has spread toother organs or to lymph nodes deep insidethe body. These tests may not always beneeded and are used mostly for patients withknown or suspected metastases (spread).
Chest x-ray A chest x-ray may be taken to find out whetherthe melanoma has spread (metastasized) tothe lungs. A chest x-ray is sometimes notneeded for patients with very early (thin)melanoma.
Computed tomography The CT (computed tomography) scan is anx-ray procedure that produces detailed cross-sectional images of your body. Instead oftaking 1 picture, like a usual chest x-ray, a CT
9

scanner takes many pictures as it rotatesaround you. You will need to lie still on atable while this is being done. A computerthen combines these pictures into an imageof a slice of your body. The machine producesmultiple images of the part of your body thatis being studied.
Often after the first set of pictures is taken,you will get an intravenous (IV) injection of aspecial dye (called a radiocontrast agent)that helps better outline structures in yourbody. A second set of pictures is then taken.The dye can cause some people get hives or,rarely, more serious allergic reactions liketrouble breathing and low blood pressure canoccur. Be sure to tell the doctor, before youget this scan, if you have ever had a reactionto any contrast material used for x-rays. TheCT may show melanoma that has spread toyour lungs or liver and can help find enlargedlymph nodes that might contain cancer.
Magnetic resonance imaging MRI (magnetic resonance imaging) scans useradio waves and strong magnets instead ofx-rays. The energy from the radio waves isabsorbed and then released in a pattern formedby the type of tissue and by certain diseases.A computer translates the pattern of radiowaves given off by the tissues into very detailedcross-sectional images of parts of the body. Acontrast material might be injected just aswith CT scans. (Please see the discussionabove.) MRI can be very useful for looking fortumors in the brain and spinal cord.
Positron emission tomography PET (positron emission tomography) scansuse glucose (a form of sugar) that contains a
radioactive atom. Cancer cells absorb largeamounts of the radioactive sugar because oftheir high rate of metabolism. The sugar isinjected into a vein and after a certainamount of time you are put into the PETmachine where a special camera can detectthe radioactivity. A PET scan may supple-ment the results of the CT and MRI scans.Sometimes a PET scan will be combined witha CT scan. This is called a PET/CT scan. Ingeneral, scans with radioactive compoundsare easy to take. There are usually no sideeffects, and you are exposed to only a tinyamount of radioactive material.
Procedures and tests to findmetastases (spread) Sentinel lymph node mapping and biopsyThis has become a standard procedure forfinding melanoma that has spread to nearbylymph nodes. Sentinel lymph node mappingcan find the lymph nodes that drain lymphfluid from the area of the skin where themelanoma started. If the melanoma hasspread, these lymph nodes are usually the firstplace it will go. That is why these lymph nodesare called sentinel nodes (sentinel means towatch over the tumor, so to speak).
To map the sentinel lymph node, sometime before surgery the doctor injects a smallamount of radioactive material into themelanoma. By checking various lymph nodeareas with a radioactivity detection devicelike a Geiger counter, the doctor can see whatgroup of lymph nodes the melanoma is mostlikely to travel to. Then the doctor injects asmall amount of a harmless blue dye into thesite of the melanoma. After about an hour, a
10

11
surgeon makes a small incision in the identi-fied lymph node area. The lymph nodes canthen be checked to find which one has turnedblue or become radioactive. When the sentinelnode has been found, it is removed and lookedat under a microscope. If melanoma cells arefound in this lymph node, the remaining lymphnodes in this area are surgically removed andalso checked for cancer. This is called lymphnode dissection. If the sentinel node does notcontain melanoma cells, no more lymphnode surgery is needed.
If a lymph node near a melanoma isabnormally large, a fine needle aspiration orsurgical biopsy of that lymph node is doneand the sentinel node procedure may not beneeded.
Fine needle aspiration biopsy A fine needle aspiration (FNA) biopsy uses asyringe with a very thin needle to remove cellsfrom a mass. A local anesthetic is sometimesused to numb the area. This test rarely causesmuch discomfort and does not leave a scar.FNA may be used to biopsy enlarged lymphnodes near a melanoma to find out if thecancer has metastasized (spread). Sometimesthe doctor will look at a CT scan or ultra-sound to guide the needle into a mass.
Surgical (excisional) lymph node biopsy: In this procedure, an abnormally large lymphnode is removed surgically through a smallskin incision. A local anesthetic is generallyused. This technique is often done if a lymphnode’s size suggests spread of melanoma, butthe FNA did not find any melanoma cells.
Diagnosis of metastatic melanoma Although many melanomas are completelycured, some melanomas spread so quicklythat a patient can have metastases to thelymph nodes, lungs, brain, gastrointestinal(GI) tract, or liver while the originalmelanoma is still small. On the other hand,melanoma that has spread to other parts ofthe body sometimes may not be found untillong after the original melanoma wasremoved from the skin.
When it has spread like this, the metastaticmelanoma in certain organs might be con-fused with a cancer starting in that organ. Forexample, melanoma that has spread to thelungs might be confused with a primary lungcancer (cancer that starts in the lungs).Special tests can be done on biopsy samplesto tell whether it is a melanoma or some otherkind of cancer. This is important becausedifferent cancers are treated differently.
Examination of the skin biopsy It is important to measure the thickness of amelanoma under a microscope because thisis believed to be one of the best ways to deter-mine the prognosis (or outlook for survival).
The pathologist examining the skinbiopsy specimen measures the thickness ofthe melanoma under the microscope with adevice called a micrometer, which is like avery small ruler. This technique is called theBreslow measurement. The thinner themelanoma, the better the prognosis. In gen-eral, melanomas less than 1 millimeter (mm)in depth (about 1⁄25 of an inch) have a verysmall chance of spreading. As the melanomabecomes thicker, it has a greater chance of

spreading. The thickness of the melanomaalso guides the choice of treatment.
Another system describes the thickness ofa melanoma in relation to its penetration intothe skin instead of actually measuring it. TheClark level of a melanoma uses a scale ofRoman numerals I to V to describe thickness(with higher numbers indicating a deepermelanoma). The Clark level Roman numeralsshould not be confused with the stage group-ing Roman numerals.
• Clark level I: the melanoma stays in theepidermis
• Clark level II: the melanoma has begunto penetrate to the upper dermis
• Clark level III: the melanoma involvesmost of the upper dermis
• Clark level IV: the melanoma has pene-trated to the lower dermis
• Clark level V: the melanoma has pene-trated very deeply, to the subcutis
In the newest classification, the Breslowmeasurement of thickness has become moreuseful than the Clark level of penetration asthe first prognostic factor. This is because thethickness measurement is easier and dependsless on the pathologist’s judgment. But some-times the Clark level tells us that a melanomais more advanced than we may think it isfrom the Breslow measurement. Therefore,both systems are often used to help stage amelanoma.
In either system, the melanoma has a worseprognosis if the pathologist says it is ulcerated.(This means the layer of skin covering themelanoma is absent).
Melanoma stages
Staging is a process of describing how far acancer has spread. This includes describingthe size of the skin tumor and whether it hasspread to any other organs. A staging systemis a standard way for your health care team tosummarize the extent of your cancer.
The American Joint Committee on Cancer(AJCC) staging system is used most often todescribe the extent of melanoma. In this sys-tem, each cancer is given a T category, an Ncategory, and an M category.
• The T category is based on the tumor’sthickness and whether it is ulcerated(there is no layer of skin covering themelanoma).
• The N category reflects whether themelanoma has spread to lymph nodesnear the melanoma. The N categoryalso reflects whether the melanomacancer cells are beginning to spreadand are found in lymphatic channelsconnecting to the lymph nodes.
• The M category indicates whether thereis spread (metastases) to distant organs.
In TNM staging, information about thetumor, lymph nodes, and metastasis is com-bined to assign a stage according to a processcalled stage grouping. The stage is thendescribed using 0 and Roman numerals fromI to IV.
Several tests and procedures are used togather information about a melanoma andwhether it has spread to lymph nodes anddistant organs. This information is used toassign T, N, and M categories and a groupedstage.
12

Descriptions of grouped stages The stages used in these guidelines are as follows:
Stage 0: The melanoma is in situ, meaningthat it involves the epidermis but has not spreadto the dermis. This is also called Clark level I.
Stage IA: The melanoma is less than orequal to 1.0 mm or about 1⁄25 inch in thicknessand no ulceration is present. Using the Clarksystem, this can be level II or III. It appears tobe localized in the skin and has not beenfound in lymph nodes or distant organs.
Stage IB: The melanoma is less than orequal to 1.0 mm in thickness and is ulcerated,or Clark IV or V, or it is between 1.01 and 2.0mm and is not ulcerated. It appears to belocalized in the skin and has not been foundin lymph nodes or distant organs.
Stage IIA: The melanoma is between 1.01mm and 2.0 mm in thickness and is ulcerated,or it is between 2.01 and 4.0 mm and is notulcerated. It appears to be localized in theskin and has not been found in lymph nodesor distant organs.
Stage IIB: The melanoma is between 2.01mm and 4.0 mm in thickness and is ulcerated,or it is thicker than 4.0 mm and is not ulcer-ated. It appears to be localized in the skinand has not been found in lymph nodes ordistant organs.
Stage IIC: The melanoma is thicker than4.0 mm and is ulcerated. It appears to belocalized in the skin and has not been foundin lymph nodes or distant organs.
Stage III: The melanoma has spread to thelymph nodes nearest the affected skin area.There is no distant spread.
Stage IV: The melanoma has spreadbeyond the original area of skin and thenearby lymph nodes to other organs, such asthe lung, liver, or brain, or to distant areas ofthe skin or lymph nodes.
Types of treatment formelanoma
After the diagnostic tests are done, your cancercare team will recommend one or more treat-ment options. Consider the options withoutfeeling rushed. If there is anything you do notunderstand, ask to have it explained. Thechoice of treatment depends largely on thethickness of the primary tumor and the stageof the disease.
Types of surgery for melanoma Wide local excision When the diagnosis of melanoma is estab-lished by biopsy, a wide local excision is doneto decrease the chance of local recurrence.More tissue is removed around the melanomasite, and the tissue from the final excision isexamined to make sure that no cancer cellsremain in the skin. The size of the marginremoved (the edge of healthy tissue aroundthe melanoma) depends on the thickness ofthe tumor.
13

Tumor thickness Recommended margins
In situ 0.5 cm (1 inch = 2.54 cm)
Less than 1 mm 1 cm
1 to 2 mm 1 to 2 cm
2 to 4 mm 2 cm
Over 4 mm At least 2 cm
If the melanoma is on a finger or toe, thetreatment may be to amputate as much of thatdigit as is necessary to get clear margins.
Lymph node evaluation After the diagnosis of melanoma is made, thedoctor will examine the lymph nodes nearestthe melanoma. If the lymph nodes are notenlarged, then a sentinel node biopsy proce-dure may be done. Sentinel lymph node biopsyis usually recommended if the melanoma ismore than 1 mm thick, but may be consideredfor thinner melanomas. If the sentinel lymphnode does not show cancer, then it is unlikelythat the melanoma has spread to the lymphnodes and there is no need for a lymph nodedissection. If the sentinel lymph node is posi-tive, removal of the remaining lymph nodes isusually advised.
If the regional lymph nodes feel hard orlarge, and FNA or biopsy shows metastaticmelanoma, a lymph node dissection may bedone. This procedure removes most of thelymph nodes in that area. They will be exam-ined under a microscope to see how manylymph nodes contain cancer.
Lymph node removal can cause some sideeffects that may be permanent. The mosttroublesome is called lymphedema. Lymphnodes in the groin or under the arm help
drain fluid from the limbs. Without them,fluid may back up and cause swelling in theleg or arm. Most patients do not get lym-phedema. Elastic stockings or sleeves can helpsome people with this condition. Sometimesspecial devices that squeeze the limbs areused and may be helpful. The side effects,along with the discomfort from the surgeryitself, are why this procedure is not doneunless the doctor thinks it is necessary.Discuss risks of the possible side effects andways to prevent them with your doctor.
Surgery for Metastatic Melanoma Once melanoma has spread from the skin todistant organs (such as the lungs or brain),the cancer is unlikely to be curable by surgery.Even when only 1 or 2 metastases are foundby imaging studies such as CT or MRI scans,other areas of metastasis are likely to bepresent that are too small to be found bythese scans. Surgery is sometimes done inthese cases. If one or even a few metastasesare present and can be completely removed,surgery may help some patients live longer.Also, removing a metastasis that is causingsymptoms may help improve the patient’squality of life.
Immunotherapy Immunotherapy enhances and encourages apatient’s immune system to recognize anddestroy cancer cells more effectively. Severaltypes of immunotherapy are used to treatpatients with melanoma. Some are beingstudied as adjuvant therapy. Adjuvant therapyis treatment given after surgery that is intendedto destroy any cancer cells that may not havebeen removed by the surgery.
14

Bacille Calmette-GuerinImmunotherapy with BCG (Bacille Calmette-Guerin) is used for the treatment of advancedor recurrent melanoma. BCG vaccine containsan inactivated form of the bacteria thatcauses tuberculosis and is used to immunizepeople against tuberculosis. BCG has alsobeen shown to boost the immune system ofpatients with melanoma. It is given by directinjection into the melanoma lesions (this iscalled intralesional therapy).
Cytokine therapyCytokines are proteins that activate theimmune system in a general way. Cytokinetherapy is a type of immunotherapy. Twocytokines, interferon-alpha and interleukin-2(IL-2), can help boost immunity in patientswith melanoma. Both drugs can help shrinkmetastatic (stage III and IV) melanoma inabout 10% to 20% of patients. IL-2 is given asan intravenous (IV) injection. For advanced orrecurrent melanoma IL-2 is injected directlyinto the melanoma lesion (intralesional ther-apy). Side effects of cytokine therapy mayinclude fever, chills, aches, depression, andsevere tiredness. Interleukin-2, particularly inhigh doses, can cause fluid to collect in thebody, so the person swells up and can feelquite sick. Some patients may need to be hos-pitalized because of this problem.
Interferon therapyInterferons are immune substances producednaturally by the body in response to infection.A man-made version of interferon (alfa-2b) canbe administered systemically by intravenous(IV) injection or under the skin (subcutaneousinjection). Interferons can be used as adjuvant
therapy (additional therapy following initialtreatment). Side effects include fever, chills,aches and severe tiredness. Interferons canalso have an effect on the heart and liver.Patients should be treated by an oncologistwho is experienced with this therapy.Interferons given to patients with stage IIImelanoma following surgery can delay therecurrence of melanoma, but may not prolongpatients’ lives. Your decisions about adjuvanttherapy should take into account the poten-tial benefits and side effects of this treatment.
Vaccine therapyMelanoma vaccines are experimental thera-pies that are being tested in patients with stageIII or stage IV melanoma. Anti-melanomavaccines are, in some ways, like the vaccinesused to prevent diseases caused by virusessuch as polio, measles, and mumps. Anti-virusvaccines usually contain weakened or killedviruses or parts of a virus that cannot causethe disease. The vaccine stimulates the body’simmune system to destroy the more harmfultype of virus. In the same way, weakenedmelanoma cells or parts of melanoma cellscalled antigens can be injected into a patientin an attempt to stimulate the body’s immunesystem to destroy melanoma cells. Usually, themelanoma cells are mixed with substancesthat help stimulate the body’s immune system.
Chemotherapy for melanoma Chemotherapy is systemic therapy using anti-cancer drugs. The drugs are usually injectedinto a vein or given by mouth. These medicinestravel through the bloodstream to all parts ofthe body, where they attack cancer cells that
15

have already spread beyond the skin to lymphnodes and other organs.
Chemotherapy drugs kill cancer cells butalso kill some normal cells, such as the blood-producing cells of the bone marrow, the cellslining the gastrointestinal (GI) tract, and cellsof hair follicles. Short-term side effects ofsystemic chemotherapy might include nauseaand vomiting, loss of appetite, hair loss, andmouth sores.
Because chemotherapy can kill normalblood cells, patients may have low blood cellcounts, which can result in:
• an increased chance of infection (dueto a shortage of white blood cells)
• bleeding or bruising after minor cutsor injuries (due to a shortage of bloodplatelets)
• fatigue (often due to low red blood cellcounts, but also can be caused by thechemotherapy alone)
Most side effects disappear once treatmentis stopped. There are treatments for many ofthe short-term side effects of chemotherapy,so be sure to discuss side effects with yourcancer care team. For example, anti-nauseadrugs can be given to prevent or reducenausea and vomiting.
Only a few chemotherapy drugs are usedfor stage IV melanoma. Although chemother-apy is usually not as effective in melanoma asin some other types of cancer, it may relievesymptoms or extend the survival time of somepatients with stage IV melanoma.
The preferred treatment for advanced ormetastatic melanoma is participation in aclinical trial. As another option, patients with
advanced melanoma can be treated with high-dose interleukin-2, or with the chemotherapydrugs dacarbazine (DTIC) or temozolomideeither alone or combined with other drugslike, cisplatin and vinblastine. Chemotherapymay also be given in combination with inter-feron alfa and/or interleukin-2.
Hyperthermic isolated limb perfusion is atype of chemotherapy sometimes used fortreating metastatic melanomas confined tothe arm or leg. This method temporarily sep-arates the circulation of the involved limbfrom the rest of the body and injects highdoses of chemotherapy into the artery feed-ing the limb. This allows high doses to begiven to the area of the tumor without expos-ing internal organs to these doses that wouldotherwise cause severe side effects. Usually thefluid is warmed to 102° to 104° F. Melphalanis the drug most often used in this procedure.Limb perfusion is done to help controldisease in the affected extremity but it is notthought to improve survival time.
Radiation therapyRadiation therapy uses high-energy rays orparticles to kill cancer cells. External beamradiation therapy focuses radiation from out-side the body on the skin tumor. This type ofradiation therapy is used for treating somepatients with melanoma.
Radiation therapy is not commonly used totreat the primary tumors of melanoma (theoriginal melanoma that developed on the skin).But it may be considered in some patientswhose melanoma has come back (recurred).
16

CO2 laser ablation This treatment may be used in some patientswith several small nodules of metastaticmelanomas that have spread along the skin.The CO2 laser is a type of laser used for skinproblems. It emits a very high energy beamthat destroys superficial (shallow) skin lesions.
Supportive care Most of this document discusses ways to curepeople with melanoma or to help them livelonger by removing or destroying melanomacancer cells. But, another important goal is tohelp you feel as well as you can and to continueto do the things in life that you want to do.This is called supportive care. Don’t hesitateto discuss your symptoms or how you arefeeling with your cancer care team. There areeffective and safe ways to treat symptomsyou may be having, as well as most of the sideeffects caused by treatment for melanoma.
Pain is often a concern for patients withadvanced cancer. Growth of the canceraround certain nerves may cause severe pain.It is important that patients not hesitate totell their doctors if they have pain. For mostpatients, treatment with morphine or otheropioids (prescription medicines that are thestrongest pain relievers available) will reducethe pain considerably. For more informationon the treatment of cancer pain, please contactthe ACS or NCCN to request a copy of theCancer Pain Treatment Guidelines for Patients.
Complementary andalternative therapies
Complementary and alternative medicinesare a group of different types of health carepractices, systems, and products that are notpart of your usual medical treatment. They mayinclude Chinese herbs, special supplements,acupuncture, massage, and a host of othertypes of treatment. You may hear about differ-ent treatments from your family and friends.People may offer all sorts of things, such asvitamins, herbs, stress reduction, and moreas a treatment for your cancer or to help youfeel better. Some of these treatments areharmless in certain situations, while othershave been shown to cause harm. Most of themare of unproven benefit.
The American Cancer Society definescomplementary medicine or methods asthose that are used in addition to your regularmedical care. If these treatments are carefullymanaged, they may add to your comfort andwell-being. Alternative therapies are definedas those that are used instead of your regularmedical care. Some of them have been provenharmful, but are still promoted as “cures.” Ifyou choose to use these alternatives, they mayreduce your chance of fighting your cancer bydelaying or replacing regular cancer treatment.
There is a great deal of interest today incomplementary and alternative treatmentsfor cancer. Many are being studied to find outif they are truly helpful to people with cancer.Before changing your treatment or adding anyof these methods, it is best to discuss thisopenly with your doctor or nurse. Some meth-ods can be safely used along with standardmedical treatment. But others can interfere
17

with standard treatment or cause seriousside effects. That is why it’s important to talkwith your doctor. More information aboutcomplementary and alternative methods ofcancer treatment is available through theAmerican Cancer Society’s toll-free numberat 1-800-ACS-2345 or on our Web site atwww.cancer.org.
About Clinical Trials
All drugs used to treat cancer or otherdiseases must undergo clinical trials in orderto determine their safety and effectivenessbefore the Food and Drug Administration(FDA) can approve them for use. Treatmentsused in clinical trials are often found to havereal benefits. Researchers conduct studies ofnew treatments to answer the followingquestions:
• Is the treatment helpful?• How does this new type of treatment
work?• Does it work better than other
treatments already available? • What side effects does the treatment
cause? • Do the benefits outweigh the risks,
including side effects? • Which patients will the treatment
most likely help?
During cancer treatment, the doctor maysuggest taking part in a clinical trial. Scientistsconduct clinical trials only when they believethat the treatment being studied may bebetter than other treatments.
All patients in a clinical trial are closelywatched by a team of experts to monitortheir progress very carefully. The study isdone to find out if the new treatment willwork better than the standard treatment andif the side effects are worse or less. The newtreatment may have some side effects, whichthe doctor will discuss with the patientbefore the clinical trial is started.
Deciding to Enter a Clinical TrialTaking part in any clinical trial is completelyvoluntary. Doctors and nurses explain thestudy in detail and provide a consent form toread and sign. This form states that thepatient understands the risks and wants toparticipate. Even after signing the form andthe trial begins, the patient may leave thestudy at any time, for any reason.
Taking part in the study will not keepanyone from getting other medical care theymay need. Patients should always check withtheir health insurance company to find outwhether it will cover the costs of taking partin a clinical trial.
Participating in a clinical trial evaluatingnew, improved methods for treating cancermay help the patient directly, and it may helpother people with cancer in the future. Forthese reasons, members of the NationalComprehensive Cancer Network and theAmerican Cancer Society encourage partici-pation in clinical trials.
18

How can I find out more aboutclinical trials that might be rightfor me?The American Cancer Society offers a clinicaltrials matching service that will help you finda clinical trials that is right for you. You canreach this service at 1-800-303-5691 or ourWeb site http://clinicaltrials.cancer.org. Basedon the information you give about yourcancer type, stage, and previous treatments,this service compiles a list of clinical trialsthat match your medical needs. The servicewill also ask where you live and whether youare willing to travel so that it can look for atreatment center you can get to.
You can also get a list of current clinicaltrials by calling the National CancerInstitute’s Cancer Information Service tollfree at 1-800-4-CANCER (1-800-422-6237) orby visiting the NCI clinical trials Web site atwww.cancer.gov/clinical_trials/.
More information about clinical trials isavailable through the American CancerSociety’s toll-free number at 1-800-ACS-2345or on our Web site at www.cancer.org.
Other things to considerduring and after treatment
During and after treatment for your melanomayou may be able to speed up your recoveryand improve your quality of life by taking anactive role. Learn about the benefits and dis-advantages of each of your treatment optionsand ask questions of your cancer care team ifthere is anything you do not understand.Learn about and look out for side effects oftreatment and report these promptly to your
cancer care team so that they can take stepsto reduce them.
Remember that your body is as unique asyour personality and your fingerprints.Although understanding your cancer’s stageand learning about your treatment optionscan help predict what health problems youmay face, no one can say for sure how you willrespond to cancer or its treatment.
You may have special strengths such as ahistory of excellent nutrition and physicalactivity, a strong family support system, or adeep faith, and these strengths may make adifference in how you respond to cancertreatment. There are also experienced pro-fessionals in mental health services, socialwork services, and pastoral services who mayassist you and your family in coping withyour illness.
You can help in your own recovery fromcancer by making healthy lifestyle choices. Ifyou use tobacco, stop now. Quitting willimprove your overall health, and the full returnof the sense of smell may help you enjoy ahealthy diet. If you use alcohol, limit howmuch you drink. Have no more than 1 drinkper day if you are a woman or 2 drinks per dayif you are a man. Good nutrition can help youget better during and after treatment. Eat anutritious and balanced diet, with plenty offruits, vegetables, and whole grain foods. If youare having eating problems, ask your cancercare team if you may benefit from talkingwith a dietician.
If you are in treatment for cancer, be awareof the battle that is going on in your body.Radiation therapy and chemotherapy all addto the fatigue caused by the disease itself. Tohelp you with the fatigue, plan your daily
19

activities around when you feel your best. Getplenty of sleep at night. Ask your cancer careteam about a daily exercise program to helpyou feel better.
A cancer diagnosis and its treatment aremajor life challenges, with an impact on youand everyone who cares for you. Before youget to the point where you feel overwhelmed,consider attending a meeting of a local sup-port group. If you need assistance in otherways, contact your hospital’s social servicedepartment or the American Cancer Society.
Protecting your skin fromsun exposure
Everyone needs to protect his or her skinfrom the harmful effects of the sun. Sunlightcontains ultraviolet radiation (UV), which candamage the genes in your skin cells. Tanninglamps and booths are another source ofultraviolet radiation. Excessive exposure tolight from these sources can increase the riskof skin cancer, including melanoma. Theamount of UV exposure depends on theintensity of the radiation, length of time theskin was exposed, and whether the skin wasprotected with clothing and sunscreen.
The most important ways to protect yourskin is by avoiding being outdoors in intensesunlight too long and to protect your skinwhenever you are outdoors. You can continueyour usual outdoor activities and protect yourskin at the same time by doing the following:
Seeking shade: The simplest and mosteffective way to limit exposure to ultraviolet
(UV) light is to avoid being outdoors in sun-light too long. This is most important in themiddle of the day when UV light is mostintense. Seek shade under a tree or umbrellawhenever possible.
Protecting your skin with clothing: Youcan protect most of your skin with clothing,including a shirt with long sleeves and a hatwith a broad brim. Tightly woven and darkcolored fabrics generally provide the best sunprotection.
Using sunscreen: Sunscreens with anSPF of 15 or more should be used on areas ofskin exposed to the sun, particularly when thesunlight is strong. Always follow directionswhen putting on sunscreen. You should applysunscreen before you go outside, use itthickly on all sun-exposed skin, and reapplyit every 2 hours. A 1-ounce application (apalmful of sunscreen) is recommended. Manysunscreens wear off with sweating and swim-ming and must be reapplied for maximumeffectiveness. Use sunscreen even on hazydays or days with light or broken cloud coverbecause the UV light still comes through.
Sunscreen should not be used to gain extrasun exposure time. Sunscreen will not preventmelanoma; it just reduces the amount of UVlight exposure. Researchers have found thatmany people use sunscreens so that they canstay out in the sun longer. But, by extendingtheir time in the sun, they end up receivingthe same amount of UV light exposure as ifthey hadn’t used sunscreen at all. All excessivesun exposure is unhealthy. Sunscreen shouldnot be used to allow a person more time inthe sun.
20

Wearing sunglasses: Wrap-around sun-glasses with 99% to 100% UV absorptionprovide the best protection for the eyes andthe skin area around the eyes.
Avoiding other sources of UV light: Theuse of tanning beds and sun lamps is not safe.The UV radiation they deliver can damageyour skin. Their use may increase your risk ofdeveloping melanoma.
Checking your skin
As part of your follow-up care, your doctormay talk to you about checking your skin ona regular basis. You should know the patternof your existing moles, blemishes, freckles,and other marks on your skin so that you’llnotice any changes. Self-examination is bestdone in front of a full-length mirror. A hand-held mirror can be used for areas that arehard to see.
It is important to know the differencebetween a normal mole (sometimes called anevus) and a melanoma. A normal mole isgenerally an evenly colored brown, tan, or
black spot on the skin. It can be either flat orraised. It can be round or oval. Moles aregenerally less than 6 mm (1⁄4 inch) in diameter(about the width of a pencil eraser). A molecan be present at birth, or it can appear duringchildhood or young adulthood. Several molescan appear at the same time, especially onareas of the skin exposed to the sun. Molesmay fade away in older people.
A spouse or other partner may be able tohelp you with these examinations, especiallyfor those hard-to-see areas, like the back ofyour thighs and buttocks. All areas should beinspected, including the palms and soles, thelower back, and the back of the legs. Friendsand family members can also help by point-ing out areas of skin that look different. Besure to show your doctor any spots that con-cern you. Your doctor will also examine yourskin on your follow-up visits.
Spots on the skin that are changing in size,shape, or color should be evaluated as soonas possible. Any unusual sore, lump, blemish,marking, or change in the way an area of theskin looks or feels should be looked at byyour doctor.
21

22
NOTES

23
Work-up (evaluation) andtreatment guidelines
Decision trees
The Decision Trees (or flow charts) on the following pages represent treatmentoptions for melanoma based on how thick it is and how far it has spread. Eachone shows you step-by-step how you and your doctor can arrive at the choicesyou need to make about your treatment.
Keep in mind that this information is not meant to be used without the expertiseof your own doctor, who is familiar with your situation, medical history, andpersonal preferences.
You may even want to review this booklet with your doctor, who can show youwhich of the Decision Trees apply to you. Ask your doctor about the specificstage your disease is in (i.e., tumor, nodes, metastasis) which refers to howdeeply the melanoma is extending into the underlying skin and whether it hasspread beyond the skin. This information will also help you know which DecisionTrees apply to you. We’ve left some blank spaces in the Decision Trees for you oryour doctor to add notes about the treatments. You also might use this space towrite down some questions to ask your doctors about the treatments.
People with any stage of melanoma have the option of participating in a clinicaltrial. Taking part in that type of study does not prevent you from getting othermedical care you may need.
The NCCN guidelines are updated as new significant information become avail-able. To be sure you have the most recent version, consult the Web sites of theACS (www.cancer.org) or NCCN (www.nccn.org). You may also call the NCCN at1-888-909-NCCN or the ACS at 1-800-ACS-2345 for the most recent informationon these guidelines. If you have questions about your cancer or cancer treatment,please call the ACS any day at any time at 1-800-ACS-2345.

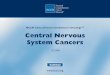
Work-up (evaluation) of melanoma This Decision Tree begins when you or yourdoctor finds an abnormal looking skin growthor spot (called a skin lesion). If the lesion lookssuspicious for melanoma the first step is abiopsy. The whole lesion, if possible, should beremoved, along with 1 to 3 mm (about 1⁄25 to2⁄25 inch) of surrounding normal skin (calledthe margin). If this is not possible, then thethickest part of the lesion should be removed,including the full depth of the lesion.
Any further testing is based on what theskin lesion looks like under the microscope.Sometimes the first biopsy is not adequatefor complete evaluation and a second biopsymight be recommended. A pathologist (adoctor who specializes in examining tissuesamples) who is experienced with skin tumorswill examine the specimen to determine if itis a melanoma. He or she will do all of thefollowing:
24
Treatment Guidelines for Patients
Clinical presentation Diagnosis
Suspicious dark-coloredskin lesion such as amole, blemish, or spot
Biopsy
Diagnosiscan’t be made
Melanomadiagnosed
Biopsy again

25
• measure the thickness of the lesion(Breslow scale);
• note how deeply it grows into theunderlying normal tissue (Clark level);
• check whether the top of the lesion hasulcerated (determine if the epidermisor outer layer of the skin is no longerpresent)
• look for cancer at the edges of the biopsy• look for clusters of melanoma cells in
the skin near the biopsy site (this iscalled satellitosis)
If the diagnosis of melanoma is confirmed,you should have a complete history andphysical examination. Your doctor will ask ifany members of your family have been diag-nosed with melanoma. The physical exami-nation will include a thorough inspection of allof your skin; looking for any enlarged lymphnodes, particularly near the melanoma; andlooking for enlarged organs. These evaluationswill give information about the specific stage ofyour melanoma and the best treatment plan.
©2008 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Work-up (evaluation) of melanoma
Pathology evaluationand report
Preliminary work-up
The pathology report should identify:
• Breslow scale – a measurement ofthickness
• Clark level – describes how deep the melanoma cells have grown
• Whether there is ulceration
• Whether there is cancer at theedges (margins) of the biopsy
• Whether there are separate clustersof melanoma cells in the skin nearthe biopsy site
The doctor will do:
• Complete history (including askingabout any family history ofmelanoma)
• Physical examination, especially ofthe entire skin, lymph node areasnear the melanoma, and organs

Work-up and treatment of lowerstage melanoma (in situ, andstages I and II)If your melanoma is stage 0 (in situ), meaningthat is has not spread beyond the outer layerof the skin, no further tests are needed. Theonly treatment should be a wider excision ofthe melanoma and of the surrounding area.About 0.5 cm (1⁄5 inch) of extra skin (margin)
should be removed. Sentinel node biopsy is notneeded. No adjuvant (additional) treatmentis recommended.
If your melanoma is stage I or II, imagingtests such as a CT, PET scan, or MRI may beadvised if you are having symptoms or if yourphysical exam suggests that melanoma mayhave spread beyond the skin. A chest x-raymay be recommended for stage IB or stage II
26
Treatment Guidelines for Patients
Clinical stage Initial work-up
Further imaging by CTscan, PET scan, or MRIif having symptoms orsigns of spread
No further tests needed
• Chest x-ray (optional)
• Further imaging by CTscan, PET scan, or MRI ifhaving symptoms or signsof spread (especially forStage IIB and IIC)
Discuss the value ofsentinel lymph nodebiopsy with the doctor
Stage 0In situ
Stage IA – low risk:(less than or equalto 1 mm thick,Clark level II or III,no ulceration)
Stage IB – intermediateto high risk:(less than or equal to 1 mm thick, with ulceration, or Clarklevel IV or V)
OR
Stage II – intermediateto high risk:(more than 1mm thick with or withoutulceration, with nolymph node spread)

melanomas. The next step is wide excision ofthe melanoma, which will include removal of1 to 2 cm of surrounding normal skin depend-ing on the thickness of the melanoma.
Your doctor may also recommend a biopsyof 1 or more sentinel nodes when the excision
is done in order to help determine yourfuture risk of recurrence and to help guidetreatment decisions. Although a sentinelnode biopsy is an option if you have Stage IAdisease, it is considered more strongly forstage IB and stage II disease. This is because
27
Work-up and treatment of lower stage melanoma (in situ, and stages I and II)
©2008 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
See the Decision Treefor follow-up (page 34)
See the Decision Treefor follow-up (page 34)
Primary (main)treatment
Adjuvant (additional)treatment
Wide excision (with or without sentinelnode biopsy) with theremoval of an extra 1to 2 cm of surroundingnormal skin for 1 to 2mm thick lesions
Wide excision with theremoval of an extra 1to 2 cm of surroundingnormal skin for 1 to 2mm thick lesions, andsentinel node biopsy
• If lesion is less than 4 mm thick: Observation*, or Clinical trial
• If lesion is more than 4 mm thick: Clinical trial, orInterferon injections, orObservation*
See Decision Tree for stageIII treatment (page 30)
Wide excision of tumorwith removal of anextra 0.5 cm (1⁄5 inch) ofsurrounding normal skin
Sentinel nodedoes not contain cancer
If lesion isstage IA
If lesion isstage IA
If lesion isstage IB or II
If lesion isstage IB or II
Sentinel nodecontains cancer
* Observation means close follow-upwith no treatment

spread to the lymph nodes is more likelywith higher stage disease. Further treatmentdecisions will depend on whether or not thesentinel lymph node biopsy is done, and if so,whether or not melanoma cells are found inthe lymph nodes.
If you have stage IA disease (low risk) anddid not have a sentinel node biopsy, or if the
sentinel node biopsy result is negative, no fur-ther treatment with close follow-up is usuallyrecommended.
If you have stage IB or stage II disease,further treatment may be recommended evenif the sentinel lymph node biopsy result isnegative, since people with these disease stageshave a higher risk of recurrence. Because it is
28
Treatment Guidelines for Patients
NOTES

not certain what treatment is best, no furthertreatment with very close follow-up is oneoption. Another option you might consider isentering a clinical trial. If your melanoma isthicker than 4 mm, treatment with interferoninjections may be recommended.
For both stage I and stage II disease, if thelymph nodes were found to contain melanoma,
then the patients will be treated as if theyhave stage III disease, which is described inthe Decision Tree starting on page 30.
The follow-up plan after initial treatmentof all stages of melanoma is outlined in theDecision Tree on page 34.
NOTES
29
Work-up and treatment of lower stage melanoma (in situ, and stages I and II) (continued)

Work-up and treatment for higherstages of melanoma: stages III and IVThis Decision Tree describes treatment ofadvanced melanoma, defined as Stage III or IV.
Stage III describes any tumor with involve-ment of the lymph nodes, but without spread todistant sites. Lymph node spread is subdividedinto minimal spread that can only be detected
30
Treatment Guidelines for Patients
Clinical or pathologic stage
Work-up
Stage III,Sentinel node contains melanoma
Stage III,Lymph nodes enlargedand contain melanoma
Stage III in-transitMelanoma
Stage IV,Metastatic
• Other imaging tests if needed to evaluate symptoms(CT with or without PET scan or MRI)
• Chest x-ray (optional)
• Blood LDH test (optional)
• Fine needle aspirate (FNA) biopsy (preferred) or lymph node biopsy
• Chest x-ray (optional)
• Blood LDH level (optional)
• CT scan of pelvis if groin lymph nodes are enlarged
• Other imaging tests if needed to evaluate symptoms (CT with orwithout PET scan or MRI)
• FNA biopsy of skin lesion (preferred) or lymph node biopsy
• Chest x-ray (optional)
• Blood LDH level (optional)
• Other imaging tests if needed to evaluate symptoms(CT with or without PET scan or MRI)
• FNA (preferred) or biopsy of the distant site
• Chest x-ray or chest CT
• Blood LDH level
• Consider abdominal/pelvic CT scan or head MRI and/or PET scan
• Other imaging tests if needed to evaluate symptoms

by looking at the sentinel lymph node biopsyunder the microscope, or more advancedspread which is suspected on the basis of
enlarged lymph nodes found during a physicalexam. Stage III in-transit melanoma describesa tumor with several nodules of melanoma
31
Work-up and treatment of higher stage melanoma (stages III and IV)
©2008 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Treatment is the same as fordistant disease (see page 40)
Ifmelanomalesionsdisappear
Primary (main) treatment
• Wide excision of tumor with removal ofup to a 2 cm margin of normal skin, AND
• Surgical removal of all lymph nodes in the involved area (if node biopsy contained melanoma)
• Excision of lesions with removal of enough surrounding skin to have a clear margin, OR
• Consider sentinal lymph node biopsy, OR
• Injection of BCG or interleukin-2 into lesions, OR
• CO2 Laser treatment, OR
• Perfuse the area with melphalan solution, OR
• Consider a clinical trial, OR
• Radiation therapy, OR
• Systemic therapy such as:· High-dose IL-2, OR· Chemotherapy such as dacarbazine, or
temozolomide alone, or combined with cisplatin and vinblastine, OR
· Chemotherapy as above with IL-2 and/or interferon alfa
• Remove all the lymph nodes in thearea of the sentinel node, OR
• Clinical trial
Adjuvant (additional)treatment
Observation*, OR
Clinical trial, OR
Interferon alfa injections,OR
Consider radiation to thearea of the cancerouslymph nodes
Clinical trial, OR
Observation*, OR
Interferon alfa injections
Clinical trial, OR
Observation*, OR
Interferon alfa injections
* Observation means close follow-up with no treatment

32
mainly found between the primary tumor andthe lymph nodes. Additional imaging testsmay be recommended for all types of stage IIIdisease, depending on the physical exam andsymptoms. Imaging tests may include CT scan,PET scan, MRI. Chest x-ray and blood tests,such as lactate dehydrogenase (LDH) levelsare optional.
For stage III melanoma with minimalinvolvement of lymph nodes (based on thesentinel node biopsy), the recommendedtreatment is removal of all the lymph nodes inthe area of the sentinel node. A clinical triallooking at alternatives to complete lymphnode removal is another option.
When the lymph nodes are enlarged, abiopsy is first recommended. The preferredbiopsy technique is a fine needle aspiration,where a needle is placed into the enlargedlymph nodes to remove a sample of cells.Alternatively, an excisional biopsy may bedone where the physician uses a scalpel to
open the skin and remove a lymph node.Following the biopsy, a wide excision of thetumor with the removal of up to 2 cm of sur-rounding normal skin is recommended.
If the lymph node biopsy result was posi-tive, all the lymph nodes in the involved areashould be removed. Following the surgery,additional therapy may be recommended.Because it is not certain which treatment isbest, you may not receive any further treat-ment but instead continue with the doctorclosely watching you. Other options includeentering a clinical trial or treatment withinterferon injections. Finally, if the cancerwas stage IIIC, radiation therapy to the areaof cancerous lymph nodes is recommendedeither alone or combined with any of theabove treatments.
Biopsy is the first step for stage III in-transit melanoma, to make sure that thesenodules are melanoma. If possible, all tumornodules should be removed along with
Treatment Guidelines for Patients
NOTES

enough surrounding normal skin. This may becombined with a sentinel node biopsy. If thisis not possible, injections of Bacille Calmette-Guerin (BCG) vaccine or interleukin-2 (IL-2)directly into the melanoma is a treatmentoption. Tumor nodules also might bedestroyed with laser therapy (discussed onpage 17). If the melanoma is located on alimb, another possible treatment is to perfusethe area with a melphalan solution heated to102° to 104° F, referred to as hyperthermicperfusion (discussed on page 16). Because itis not certain which treatment is best, youmight want to consider entering a clinicaltrial. Other possible treatments are radiationtherapy to the area, or systemic treatment,such as high-dose interleukin therapy, orchemotherapy with dacarbazine (DTIC) ortemozolomide (either alone or combined withcisplatin and vinblastine), or chemotherapycombined with interleukin-2 (IL-2) and/orinterferon alfa. If all the melanoma lesions
completely disappear with initial treatment,you can consider a clinical trial for ongoingtreatment, careful observation by your doctor,or additional therapy with interferon injections.
Finally, if your melanoma is stage IV,meaning it has spread to distant sites, the firststep should be a biopsy of one of those distantsites to confirm that it is truly a metastasis.The biopsy can be a fine needle aspiration oran excisional biopsy. Other tests that may bedone are a chest x-ray and/or chest CT andblood LDH level. CT scans of the abdomenand pelvis, PET scans, or MRI of the brain maybe considered, as well as other imaging testsdepending on your symptoms or physicalexam. Treatment for stage IV melanoma isdescribed in the Decision Tree “Treatment ofmelanoma with distant metastasis” startingon page 40.
The follow-up plan after initial treatmentof all stages of melanoma is outlined in theDecision Tree on page 34.
33
Work-up and treatment of higher stage melanoma (stages III and IV) (continued)
NOTES

Follow-up after initial treatment ofmelanomaAll patients with treated melanoma, regardlessof stage, should have a complete skin exami-nation every year.
Patients with stage 0 melanoma need nofollow-up other than routine medical historyand physical exam, yearly skin exams by aphysician, and monthly self-exams of the skin.
Patients with stage IA melanoma shouldalso have a medical history and physical exam
done at least yearly, with special attentionpaid to the skin and lymph nodes. Monthlyself-exams of skin and lymph nodes shouldbe considered.
If your melanoma was stage IB to III,thicker than 1 mm, and had or had not spreadto your lymph nodes, a complete history andphysical exam should be done every 3 to 6months for 3 years, then every 4 to 12 monthsfor 2 years, and then yearly. Chest x-rays andblood tests every 3 to 12 months are optional.
34
Treatment Guidelines for Patients
Clinical or pathological stage
Follow-up
Stage 0In situ
Stage IA1 mm or less thick,no ulceration
Stage IB to III1 mm or thicker withor without spread tolymph nodes
• Complete history and physical exam,withemphasis on skin and lymph nodes
• Complete skin exam every year
• Consider self-exam of all skin and lymphnodes near melanoma site monthly
• Complete history and physical exam, every 3 to 12months, with emphasis on skin and lymph nodes
• Complete skin exam every year
• Consider self-exam of all skin and lymph nodesnear melanoma site monthly
• Complete history and physical exam, with emphasis onlymph nodes and skin, every 3 to 6 months for 3 years,then every 4 to 12 months for 2 years, and then every year
• Complete skin exam every year
• Chest x-ray every 3 to 12 months (optional)
• LDH level and blood counts every 3 to 12 months (optional)
• CT scans if symptoms or physical exam changes
• Consider self-exam of all skin and lymph nodes nearmelanoma site monthly

CT scans may be done if your symptoms orphysical exam results change. You may alsowant to consider examining the skin andlymph nodes near the melanoma site monthly.
Any suspicious areas should be biopsiedto check for recurrent melanoma. If themelanoma comes back in the scar or nearby
skin or lymph nodes, it should be evaluatedas described in the Decision Tree “Treatmentof recurrrent melanoma” which starts onpage 36. If it comes back in distant sites, itsevaluation is described in the “Treatment ofmelanoma with distant metastasis” DecisionTree beginning on page 40.
35
Follow-up after initial treatment of melanoma
©2008 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Recurrence(biopsy should be done if possible)
Melanoma comes backin the surgical scar
Melanoma comes backin skin around originalsite or in track towardnearby lymph nodes
Melanoma comes backin local lymph nodes
Melanoma is found at sites distant from the original lesionand in local lymph nodes
See the Decision Tree“Treatment of recurrentmelanoma” on page 36
See Decision Tree “Treatmentof melanoma with distantmetastasis” on page 40

Treatment of recurrent melanoma The work-up and treatment of recurrentmelanoma is based on whether the melanomahas come back at the site of the originalexcision, near the original skin site, or in thelymph nodes. In all situations a biopsy shouldbe done to make sure recurrent melanoma is
present. Additional imaging tests and bloodtests depend on the site of recurrence, associ-ated symptoms, and the physical exam.
If the melanoma recurs in the surgical scar,a chest x-ray, blood counts, and a test for bloodlactate dehydrogenase (LDH) levels may bedone along with CT scan, PET scan, or brain
36
Treatment Guidelines for Patients
Type of recurrence Work-up
Melanoma recurs inthe surgical scar
Melanoma recurs in skinaround original site orin-transit toward nearbylymph nodes
Melanoma recurs inlocal lymph nodes
No previous lymphnode surgery
Previous lymphnode surgery
• Biopsy to confirm melanoma
• Chest x-ray (optional)
• LDH level, blood counts (optional)
• CT scan, PET, MRI may be done if symptoms are present
• Fine needle aspirate (preferred) or excisional biopsy
• Chest x-ray and/or chest CT
• CT scan of pelvis if groin lymph nodes are enlarged
• Other CT scans or other imaging tests (PET, MRI) ifneeded to evaluate symptoms
• LDH level, blood counts (optional)
• Fine needle aspirate (preferred) orlymph node removal for biopsy
• Chest x-ray and/or chest CT
• LDH level
• CT scan of pelvis if groin lymphnodes are enlarged
• Abdominal/pelvic CT, MRI ofbrain, and/or PET scan if needed

37
©2008 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Treatment of recurrent melanoma
Treatment of recurrence
Cancer cannot be removed
All cancerremoved
Cancer notremovedor there is distantspread
• Surgical removal of the recurrent melanoma, withpossible sentinel node biopsy, OR
• Injection of BCG or interleukin-2 into lesions, OR
• CO2 Laser treatment, OR
• Perfusion with melphalan-containing solution, OR
• Radiation therapy to lesions, OR
• Systemic therapy as described for Stage III in-transitmelanoma (see page 31), OR
• Clinical trial
Surgical removal of all areas of melanomaand lymph nodes from the involved area
Surgical removal of allthe melanoma and anyremaining lymph nodes
Surgical removal of the recurrent melanomaalong with appropriate amount of surroundingnormal skin
Sentinel node biopsy may be done
• Observation*, OR
• Clinical trial, OR
• Treatment with interferonalfa injections
• Consider radiation therapy,AND/OR
• Treatment with interferonalfa injection, OR
• Clinical trial, OR
• Observation*
• Radiation therapy AND/OR
• Systemic therapy (see page 31), OR
• Clinical Trial, OR
• Observation*
• Radiation therapy, OR
• Systemic therapy (see page 31), OR
• Clinical Trial
* Observation means close follow-up with no treatment

MRI, as needed to evaluate your symptoms.The melanoma should be surgically removedalong with adequate surrounding normalskin. If the nearby lymph nodes have notbeen biopsied, a sentinel node biopsy may berecommended, based on the thickness of therecurrent melanoma.
The risk of spread to distant areas is higherif one or several nodules are present aroundthe original site of the cancer or between it andthe nearby lymph nodes (in-transit). Therefore,a chest x-ray, CT scan, PET scan, or brain MRIcould be considered depending on yoursymptoms and physical exam, or for staging.Tests for blood LDH levels and blood countsare optional. If possible, all the in-transitmetastases should be removed and a sentinelnode biopsy should be considered at the same
time. If this is not possible, then one treatmentoption is to inject Bacille Calmette-Guerin(BCG) vaccine or interleukin-2 (IL-2) directlyinto the lesions. The lesions also might bedestroyed with laser therapy (discussed onpage 17).
Another possible treatment is to perfuseor infuse the area, if it is a limb, with a heatedmelphalan solution (discussed on page 16).Other possible treatments are radiation ther-apy to the area or systemic therapy, such ashigh dose interleukin-2 (IL-2) therapy orchemotherapy with dacarbazine (DTIC) ortemozolomide (either alone or in combinationwith cisplatin and vinblastine), or chemo-therapy in combination with interleukin-2(IL-2) and/or interferon alfa. Because it is notcertain which treatment is best, you might
38
Treatment Guidelines for Patients
NOTES

consider entering a clinical trial. After any oneof these initial treatments, additional therapymay be recommended either in a clinical trialor with interferon injection.
When melanoma comes back in lymphnodes, a chest x-ray and/or a chest CT shouldbe done. A blood test for LDH levels shouldalso be done. A pelvic CT scan is recommendedif the lymph nodes in the groin are enlarged.Other imaging tests may be considereddepending on your symptoms. These includea CT scan of the abdomen and pelvis, an MRIof the brain, and/or a PET scan. If the lymphnodes had not been removed before, then asmany as possible should be surgicallyremoved along with any other melanoma inthe area, if possible. If some lymph nodes were
removed, then all remaining lymph nodesshould be removed.
Additional therapy is often recommendedeven if surgery removes all the melanoma.Options include radiation therapy to thenode area and/or interferon alfa injections.Participation in a clinical trial or observationare other options.
If the melanoma cannot be removedcompletely, then radiation to destroy theremaining tumor cells and/or additionalsystemic treatment is recommended. A clinicaltrial or observation are other options.
If the lymph nodes cannot be removed bysurgery, then systemic therapy or radiationto relieve symptoms may be considered.Participation in a clinical trial is another option.
39
Treatment of recurrent melanoma (continued)
NOTES

Treatment of melanoma withdistant metastasis Melanoma that has come back or is initiallydiagnosed in distant sites requires a biopsy toconfirm the diagnosis. You should have achest x-ray and/or a CT scan of your chest.Other imaging tests may be recommendeddepending on symptoms and physical exam,including a CT scan of the abdomen andpelvis, MRI of your brain, or a PET scan. Ablood test of lactate dehydrogenase (LDH)levels should also be done.
If there are only a small number of metas-tases, several options may be considered.Surgery may be an option if the melanomahas not metastasized to other areas. Or, youcan wait to see if any new metastasesdevelop. If there are no new metastases andthe tumor is not spreading quickly, surgery toremove the metastases can be considered. Ifthere is no further evidence of cancer aftersurgery, options include participation in aclinical trial, or observation, or interferoninjections. If the metastases cannot beremoved completely or if new ones develop
40
Treatment Guidelines for Patients
Stage Work-up Treatment
Stage IV
Melanoma iswidespread
Fewmetastases
Manymetastases
• Fine needle aspiration(preferred) or other typeof biopsy of a distantmetastasis to confirmdiagnosis
• Chest x-ray and/or CT scan
• Abdominal/pelvic CT
• MRI of brain
• PET scan if needed
• LDH level
Surgical removal
OR
OR
Observe, thenrepeat scans
Treat the same as“Many metastases”(see below)

during the waiting period, then the treatmentwill be as if there were many metastases.
If many areas of metastases are seen onimaging studies, surgery is usually not an
option. If the cancer has not spread to yourbrain, and you are in otherwise good healthyou may consider entering a clinical trial.Other options include systemic treatment
41
©2008 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Treatment of melanoma with distant metastasis
If cancergrows andpatient is ingood health
If brain metastases are present
No other areas of cancerare found
Other areas ofcancer are found
All cancerremoved
Cancer notall removed
• Clinical trial preferred, OR
• Systemic therapy as above ifhealth is good, OR
• Supportive care
• Consider removal of metastasis orradiation if symptoms are present
If no brain metastases:
• Clinical trial preferred, OR
• Treatment with high-doseInterleukin-2, OR
• Chemotherapy with dacarbazineor temozolomide with or withoutcisplatin and vinblastine, OR
• Chemotherapy as above, with or without IL-2 and/or interferon alfa, OR
• Supportive care and treatment ofsymptoms only
• Clinical trial preferred, OR
• Chemotherapy with drugs notgiven before, OR
• Supportive care and treatmentof symptoms only
Clinical trial, OR
Observation*, OR
Interferon alfainjections
Surgery toremove cancer
See treatment for“Many metastases”(below)
See treatment for“Many metastases”(below)
* Observation means close follow-up with no treatment

such as high-dose interleukin therapy, orchemotherapy with dacarbazine (DTIC) ortemozolomide (either alone or combined withcisplatin and vinblastine), or chemotherapyin combination with interleukin-2 (IL-2)and/or interferon alfa. If the cancer growsduring one of these treatments and your
health is fair to good, another one of thesetreatments may be offered. Another option issupportive care with treatment of symptomsor participation in a clinical trial.
If the MRI shows brain metastases, youmay be offered the following options: a clinicaltrial; systemic treatment such as high dose
42
Treatment Guidelines for Patients
NOTES

NOTES
interleukin-2 therapy, chemotherapy withdacarbazine (DTIC) or temozolomide (eitheralone in combination with cisplatin and vin-blastine); or chemotherapy in combinationwith interleukin-2 (IL-2) and/or interferon
alfa. Supportive care is another option. It mayinclude surgery or radiation therapy to controlthe symptoms related to the metastases ( forexample, gastrointestinal bleeding, ulcerationof metastases, or swollen lymph nodes).
43
Treatment of melanoma with distant metastasis (continued)

Current Cancer Treatment Guidelines for Patients
Advanced Cancer and Palliative Care Treatment Guidelines for Patients(English and Spanish)
Bladder Cancer Treatment Guidelines for Patients (English and Spanish)
Breast Cancer Treatment Guidelines for Patients (English and Spanish)
Cancer Pain Treatment Guidelines for Patients (English and Spanish)
Cancer-Related Fatigue and Anemia Treatment Guidelines for Patients(English and Spanish)
Colon and Rectal Cancer Treatment Guidelines for Patients (English and Spanish)
Distress Treatment Guidelines for Patients (English and Spanish)
Fever and Neutropenia Treatment Guidelines for Patients with Cancer(English and Spanish)
Lung Cancer Treatment Guidelines for Patients (English and Spanish)
Melanoma Cancer Treatment Guidelines for Patients (English and Spanish)
Nausea and Vomiting Treatment Guidelines for Patients with Cancer(English and Spanish)
Non-Hodgkin’s Lymphoma Treatment Guidelines for Patients (English and Spanish)
Ovarian Cancer Treatment Guidelines for Patients (English and Spanish)
Prostate Cancer Treatment Guidelines for Patients (English and Spanish)

Terri Ades, MS, APRN-BC, AOCNAmerican Cancer Society
Alan N. Houghton, MD / ChairMemorial Sloan-Kettering Cancer Center
Christopher K. Bichakjian, MDUniversity of MichiganComprehensive Cancer Center
Joan McClure, MSNational Comprehensive Cancer Network
Dorothy Shead, MSNational Comprehensive Cancer Network
Mary Dwyer Rosario, MSNational Comprehensive Cancer Network
Elizabeth Brown, MDNational Comprehensive Cancer Network
Kimberly A. Stump-Sutliff, RN,MSN, AOCNSAmerican Cancer Society
Hema Sundar, PhDNational Comprehensive Cancer Network
The Melanoma Treatment Guidelines for Patients were developed by a diverse group of expertsand are based on the NCCN clinical practice guidelines. These patient guidelines were writtenfor patients, reviewed, and published with the help from the following individuals:
The original NCCN Melanoma Clinical Practice Guidelines were developed by the followingNCCN Panel Members:
Christopher K. Bichakjian, MDUniversity of MichiganComprehensive Cancer Center
Daniel G. Coit, MDMemorial Sloan-Kettering Cancer Center
Adil Daud, MDH. Lee Moffitt Cancer Center &Research Institute
Raza A. Dilawari, MDSt. Jude Children’s ResearchHospital/University of TennesseeCancer Institute
Dominick DiMaio, MDUNMC Eppley Cancer Center at The Nebraska Medical Center
Jared A. Gollob, MDDuke Comprehensive Cancer Center
Naomi B. Haas, MDFox Chase Cancer Center
Allan Halpern, MDMemorial Sloan-Kettering Cancer Center
Alan N. Houghton, MD / ChairMemorial Sloan-Kettering Cancer Center
Mohammed Kashani-Sabet, MDUCSF Helen Diller FamilyComprehensive Cancer Center
William G. Kraybill, MDRoswell Park Cancer Institute
Julie R. Lange, MDThe Sidney Kimmel ComprehensiveCancer Center at Johns Hopkins
Anne Lind, MDSiteman Cancer Center at Barnes-Jewish Hospital and WashingtonUniversity School of Medicine
Mary Martini, MDRobert H. Lurie ComprehensiveCancer Center of NorthwesternUniversity
Merrick I. Ross, MDThe University of Texas M. D. Anderson Cancer Center
Wolfram E. Samlowski, MDHuntsman Cancer Institute at the University of Utah
Stephen F. Sener, MDRobert H. Lurie ComprehensiveCancer Center of NorthwesternUniversity
Kenneth K. Tanabe, MDDana-Farber/Brigham and Women’sCaner Center | MassachusettsGeneral Hospital Cancer Center
John A. Thompson, MDFred Hutchinson Cancer ResearchCenter/Seattle Cancer Care Alliance
Vijay Trisal, MDCity of Hope
Marshall M. Urist, MDUniversity of Alabama atBirmingham ComprehensiveCancer Center
Michael J. Walker, MDArthur G. James Cancer Hospital &Richard J. Solove Research Instituteat The Ohio State University

©2008, American Cancer Society, Inc.No.951904
1.800.ACS.2345www.cancer.org
1.888.909.NCCNwww.nccn.org