-
8/16/2019 Nature the Immune System and the Gut
1/10
Initially, all microorganisms were viewed aspathogens that cause
and propagate infectiousdiseases and, as a field, immunology was
builtaround the paradigm that the host immunesystem should
recognize and eliminate theseintruders (non-self) while tolerating
self-molecules to preserve homeostasis. However,the persistent
association of animal and plantspecies with obligate and
facultative symbionts now shows that both bacteria and
theireukaryote hosts benefit from their coopera-tive relationships.
These benefits suggest thatco-evolution has selected mechanisms
thatpromote and maintain associations betweenbacteria and
eukaryotes. In humans, trillionsof bacteria are distributed in
complex andsite-specific communities on the skinand at mucosal
surfaces, and the largestcommunity is found in the distal gut. As
thesebacteria encode hundreds of genes that are
absent in the human genome1, the idea hasemerged that together
with our microbiota,we form superorganisms in which energy
andmetabolites can be exchanged2 and homeo-stasis is
maintained by the immune system3.Therefore, a new paradigm proposes
that theimmune system has evolved to accommodatecolonization by
symbiotic bacterial commu-nities of increasing complexity while
retainingthe capacity to fight pathogens.
The gastrointestinal tract is the primarysite of interactions
between the host and themicrobiota. How bacterial colonization
of
the gut might influence the developmentand functions of the
immune system hasbecome a major focus of interest. A
prevalenttheory, derived from hypotheses that werefirst postulated
by Metchnikoff a centuryago, proposes that individual members ofthe
microbiota might influence the balancebetween pro-inflammatory and
regulatoryhost responses and that alterations in thecomposition of
the microbiota (a process thatis known as dysbiosis) could
jeopardize hostimmune responses and promote the devel-opment of
various inflammatory disorders.Here, we discuss the principles that
governthe interactions between the intestinal micro-biota and the
host immune system, both inhealth and in disease. Moreover, we
stresshow the complexity of the gut ecological sys-tem and the
reciprocal nature of the regula-tion of the immune system and of
microbial
community structures must be consideredbefore one can draw any
conclusions aboutthe role of the microbiota in disease andpropose
therapeutic interventions.
The host–microbiota interaction in the gut
The intestine is an open ecological systemthat is colonized
immediately after birthby a microbial population that reachesan
impressive density of 1012 bacteria pergram of luminal content in
the distal gut.Colonization is initiated by maternallyacquired
bacteria during birth; these
bacteria are then followed by hundredsof environmentally
acquired species,which differ between individuals butmainly belong
to two bacterial phylotypes,Firmicutes spp. and Bacteroidetes
spp.2,4.A growing number of studies supportthe view that eukaryotic
hosts and theirsymbionts have co-evolved towards mutu-alistic
interactions that are based on thenutritional benefits that each
partner gainsfrom the association5 (BOX 1). However,the huge
collection of bacteria at the gutsurface is also a major threat to
host integ-
rity and has driven the selection of highlyflexible
defence mechanisms, which enableeukaryotic hosts to cope with
their micro-bial environment and compensate for theirless rapid
genetic adaptation.
The gut immune system. Recent reviewshave highlighted how
the microbiota elicitsinnate and adaptive immune mechanismsthat
cooperate to protect the host and main-tain intestinal
homeostasis6,7. Epithelial cellsare a central component of the
immunesystem of the gut. In a similar manner toimmune cells,
epithelial cells express recep-tors for microbial-associated
molecularpatterns (MAMPs). These receptors activatesignalling
cascades that finely tune epithelialcell production of
antimicrobial productsand chemokines, depending on the signalsthat
are delivered by the microbiota (FIG. 1).Thus, gut epithelial cells
form a potent andinducible physico-chemical barrier, whichlimits
microbial growth and access to thegut surface. They can also
recruit leukocytesto complement their barrier function or
toparticipate in the activation of gut adap-tive immune responses.
In mammals, the
development of gut-associated lymphoidtissues (GALTs) is
initiated before birth bya genetic programme8. However,
GALTmaturation and the recruitment of IgA-secreting plasma cells
and activated T cellsto mucosal sites only occurs after birth andis
strictly dependent on microbiota-derivedsignals; these signals
influence the crosstalkbetween epithelial cells and gut
dendriticcells (DCs), thereby modulating the natureand intensity of
intestinal B and T cellresponses7,9 (FIG. 2). In
immunocompetentmice, intestinal colonization stimulates
O P I N I O N
The immune system and the gutmicrobiota: friends or foes?
Nadine Cerf-Bensussan and Valérie Gaboriau-Routhiau
Abstract | The mammalian intestine is home to a complex
community of trillions of
bacteria that are engaged in a dynamic interaction with the host
immune system.
Determining the principles that govern host–microbiota
relationships is the focus
of intense research. Here, we describe how the intestinal
microbiota is able toinfluence the balance between pro-inflammatory
and regulatory responses and
shape the host’s immune system. We suggest that improving our
understanding of
the intestinal microbiota has therapeutic implications, not only
for intestinal
immunopathologies but also for systemic immune diseases.
PERSPECTIVES
NATURE REVIEWS | IMMUNOLOGY VOLUME 10 | OCTOBER 2010
| 735
© 20 Macmillan Publishers Limited. All rights reserved10
-
8/16/2019 Nature the Immune System and the Gut
2/10
the production of secretory IgA, the dif-ferentiation of
effector T helper 1 (T
H1),
TH2 and T
H17 cells, and the development of
regulatory T (TReg
) cells10.It is increasingly clear how these adap-
tive immune elements cooperate with innateimmune cells to
strengthen the gut barrierand protect the host from invading
patho-gens. An outstanding issue now is to definehow individual
members of the microbiotaor microbiota-derived products can
affectthe balance between pro-inflammatory and
regulatory immune responses, and to establishwhether the
composition of the microbiotacan influence the development of
inflamma-tory diseases in and beyond the gut. Beforeconsidering the
possible role of the microbiotain disease, we will first highlight
how the dif-ferent colonization strategies of individualmembers of
the microbiota can influence thedevelopment and function of the gut
immunesystem and show that, ultimately, it is the hostimmune system
that determines whether abacterium is a friend or a foe.
Anti-inflammatory roles of the microbiota. Current
results indicate that a trade-off isestablished between the host
immune sys-tem and the bulk of the microbiota, so thatin a healthy
individual, intestinal coloniza-tion stimulates host production of
micro-bicidal peptides11 and secretory IgA, whichin turn
contain the microbiota within theintestinal lumen and neutralize
MAMPs12.These mechanisms protect the host fromthe systemic
translocation of bacteria orbacterial products and from the
outburst ofpro-inflammatory cascades in intestinal epi-thelial and
innate cells13. Conversely, the resi-dent bacteria also benefit
from the symbioticrelationship and can thrive in the mucus,thus
minimizing destruction by host-derivedinflammatory mediators. Hosts
and bacteriahave evolved additional strategies to main-tain
‘friendly’ relationships. Thus, signallingcascades that occur
downstream of Toll-like
receptors (TLRs) can be desensitized bycontinuous exposure to
lipopolysaccharide(LPS)14 or can be attenuated by other
solublemediators that are produced by the micro-biota (FIG. 1).
Furthermore, some microbiota-derived soluble products can promote
thefunctions of T
Reg cells15,16.
The mechanism that maintains thisfriendly relationship has been
elucidatedin the case of Bacteroides fragilis, which is
acommon culturable member of the micro-biota15. This bacterium
possesses an unusualcapsular polysaccharide A (PSA) that is ableto
drive the differentiation of interleukin-10(IL-10)-secreting T
Regcells. Colonization by
a wild-type B. fragilis, but not by a mutantstrain that
lacks PSA, protected mice fromthe severe experimental colitis that
is induced
Box 1 | Mutualistic relationships between hosts and their
intestinal microbiota
The human intestine harbours an estimated 100 trillion bacteria,
70–80% of which cannot yet be
cultured. Each individual is thought to host several hundred
species of bacteria from only 7 to 9
phylotypes; these are mainly Gram-positive Firmicutes spp. (most
notablyClostridium spp.,
Enterococcus spp. and Lactobacillus spp.) and
Gram-negative Bacteroidetes spp. Recent
metagenomics studies predict a core of ~1,200 prevalent species
and a total intestinal
microbiome that contains 150-fold more genes than the human
genome4. The gut microbiome
encodes a core of redundant bacterial genes that are likely to
be needed to resist stressfulconditions in the host
intestine63 and to harvest nutrients that are necessary for
bacterial
growth2,4. Competition between bacteria with distinct metabolic
requirements might explain the
massive and rapid shifts in the structure of the intestinal
microbial community that are provoked
by changes in host diet64. In addition to the genes that are
necessary for microbial adaptation to
the host environment, the gut microbiome encodes multiple
biosynthetic pathways that are
predicted to greatly increase the host’s capacity to metabolize
glycans and xenobiotics and to
synthesize vitamins2,4. Moreover, studies in gnotobiotic
mice have shown the broad influence of
the gut microbiota on host physiology. Intestinal colonizaton
induces a spectrum of intestinal
and metabolic changes, which promote the digestion and
absorption of nutrients and stimulate
fat storage65,66, accelerate gut epithelial renewal and alter
epithelial locomotor activity67. The
signalling pathways that are involved remain largely elusive,
but recent observations suggest
that overlapping mechanisms have been selected during
host–microbiota co-evolution that
simultaneously control host metabolic and innate immune
responses to the microbiota. In mice,
inactivation of Toll-like receptor 5 (TLR5), which is a receptor
for bacterial flagellin that has an
established role in host innate immune responses, results in
severe obesity and profoundalterations in the microbiota
structure68. Furthermore, peroxisome proliferator-activated
receptor-γ (PPARγ), which is a transcription factor that
has a central role in glucidolipidicmetabolism, can control the
production of microbicidal peptides by colonocytes and serves
as a feedback mechanism for the activation of nuclear factor-κB
(NF-κB) in enterocytes69.
Glossary
Ankylosing enthesopathy
An inflammatory autoimmune disease of the joints
that naturally occurs in mice on a C57BL/10 genetic
background; the disease is similar to human ankylosing
spondylitis. The pathology is characterized by the
proliferation of cartilage and connective tissue, which
culminates in ankylosis of the joints.
Germinal centres
Highly specialized and dynamic microenvironments that
are located in secondary lymphoid tissues and give rise
to secondary B cell follicles during an immune response.
Germinal centres are the main sites of B cell proliferation
and differentiation, which leads to the generation of
memory B cells and plasma cells that produce high-affinity
antibodies.
Gnotobiotic mice
Germ-free mice are born and raised in sterile isolators
and are devoid of colonization by any microorganisms,
but after they have been experimentally colonized by
known bacteria, they are said to be gnotobiotic. They
are kept in isolators to control their bacterial status.
IgE-associated allergies
Type 1 hypersensitivity reactions that are mediated by
IgE, which induces mast cell activation and degranulation.
Such immune reactions are seen in asthma, allergic rhinitis,
systemic anaphylaxis and food allergies.
Obligate and facultative symbionts
Obligate microbial symbionts need to colonize a hostto develop
and multiply, unlike facultative microbial
symbionts, which can also develop outside a host.
Pathobionts
Microbial symbionts that can cause defined disease in
predisposed hosts following changes in the gastrointestinal
environment.
Microbiome
The whole genome of all of the microorganisms that
colonize a specific environment.
Peyer’s patches
Collections of lymphoid follicles that are located in the
intestinal mucosa and are particularly abundant in the ileal
mucosa. Together with mesenteric lymph nodes, they form
the inductive compartment for intestinal immune responses.
Proteobacteria
Gram-negative microorganisms that colonize very distinct
environments and are the second largest group of bacteria
on earth. Proteobacteria that colonize the intestine include
commensal, pathogenic and opportunistic species, such
asSalmonella, Shigella and Helicobacter spp. and
Escherichia
coli strains. In healthy adults, proteobacteria
represent less
than 1% of the enteric microbiota, but they are a major
cause of intestinal and extraintestinal diseases.
Type VI secretion system
(T6SS). Like T3SS and T4SS, T6SS is a multi-subunit
complex that acts like a ‘needle and syringe’ to
translocate bacterial products across the
double-membrane of Gram-negative bacteria into
the cytoplasm of eukaryotic cells.
Xenobiotics
Chemical compounds that are foreign to a living organism
and that can be toxic, even at low concentrations.
P E R S P E C T I V E S
736 | OCTOBER 2010 | VOLUME 10
www.nature.com/reviews/immunol
© 20 Macmillan Publishers Limited. All rights reserved10
-
8/16/2019 Nature the Immune System and the Gut
3/10
|
Intestinal lumen
Intestinalepithelial cellMYD88
TLR
PAMP
p50 p65
p50 p65
p65
PPAR γ
PPAR γ
NF-κB
IκB
IRAK1Expression of IRAK1decreased by LPSfrom microbiota
Nuclear translocationof NF-κB
NF-κB transcribespro-inflammatorycytokines andchemokines
anddefensins
IκB ubiquitylated andtargeted to the proteasomefor
degradation
ROS induced bymicrobiota inhibitubiquitin ligases
PPAR γ induced in
response to microbiotaLPS diverts NF-κBfrom nucleus
PPAR γ upregulatescolonic β-defensinsto sustain gut
barrier
Pathway impairedin patients withCrohn’s disease
Bacterium
by Helicobacter hepaticus15,17. Furthermore,administration of
PSA reduced the sever-ity of disease in a model of
trinitrobenzenesulphonic acid (TNBS)-induced colitis17.Therefore,
B. fragilis may represent a proto-type peace-keeper
strain. Yet the outcomeof host–microbiota interactions cannot
bepredicted from only the bacterium itself, anda bacterium that is
beneficial for an immuno-competent host can become a dangerous
foewhen the immune system is weakened. Thisis illustrated by the
fact that B. fragilis causessevere sepsis in immunocompromised
hosts.Likewise, normally harmless members of themicrobiota can
initiate intestinal inflamma-tion in individuals who cannot mount
effi-cient intestinal humoral responses18,19 and inindividuals
with impaired intestinal immuno-regulation, most notably in those
who lack afunctional IL-10 signalling pathway 20,21.
Promotion of effector immune responses. Although certain
members of the microbiotahave adopted peace-keeper activities to
colo-nize the intestine, others are, undoubtedly,endowed with
pro-inflammatory properties.One such group, which has recently
attractedmuch attention, is segmented filamentousbacteria (SFB).
These unculturable speciessettle in the rodent intestine at the
time ofweaning and stimulate the postnatal matu-ration of immune
responses in the mousegut. Mice that are colonized by a
microbiotathat lacks SFB have weaker IgA
antibodyresponses22 and much poorer intestinalT cell responses
compared with mice thatare colonized with SFB. Notably, mice that
arecolonized by an SFB-deficient microbiotalack mucosal T
H17 cells10,23. Furthermore,
these animals cannot control colonization bythe invasive
pathogen Citrobacter rodentium,which suggests that
microbiota-inducedimmune responses participate in the bar-rier
function of the flora23. This hypothesisis also supported by recent
work that showsthat the destruction of the microbiota fol-lowing
treatment with antibiotics can jeop-ardize innate immune responses
in the gut
and promote colonization by pathogens24.A striking feature of
SFB is their strong
adherence to the surface epithelium of theileum and the Peyer’s
patches shortly afterweaning25. This is in contrast with most
othermembers of the microbiota, which remainentrapped within the
mucus and have littleor no physical contact with host
epithelium25.This attachment, which is perhaps necessaryto initiate
the replication of SFB, is likely tofacilitate the sampling and
presentation ofSFB antigens to T cells by DCs in the Peyer’spatches
and to stimulate pro-inflammatory
signalling pathways in epithelial cells andDCs, resulting in
robust innate and adap-tive immune responses in the
intestine10,23.Such behaviour is characteristic of bona
fidepathogens, which use host inflammatoryresponses to eliminate
the resident flora andto colonize the remaining niches26,27.
Thisattachment might enable SFB to settle in the
mouse intestine, but it also benefits the hostby strengthening
the gut barrier. Strikingly,on the basis of morphological studies,
SFBhave been detected in all species studied fromarthropods to
mammals, including humans,and closely related 16S rRNA sequences
havebeen found in chickens, trout and rodents25,28.Therefore, it is
tempting to speculate that this
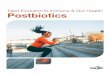
Figure 1 | Modulation of intestinal epithelial cell
pro-inflammatory responses by the microbiota.
In a similar manner to immune cells, epithelial cells detect
microbes through pattern-recognition recep-tors, including
Toll-like receptors (TLRs). Upon TLR ligation, adaptor proteins,
such as myeloid differen-
tiation primary-response protein 88 (MYD88), are recruited and
activate signalling cascades, notably
the nuclear factor-κB (NF-κB) pathway, which stimulates the
transcription of antimicrobial proteins,pro-inflammatory cytokines
and chemokines. In resting cells, NF-κB is sequestered in the
cytoplasm byits inhibitor IκB. Following TLR activation, IκB is
phosphorylated, ubiquitylated and degraded by theproteasome, which
allows nuclear translocation of NF-κB and transcription of NF-κB
target genes. Thispathway can be modulated by microbiota-derived
factors, preventing excessive and potentially delete-
rious host pro-inflammatory responses. Immediately after birth,
expression of the interleukin-1 receptor-
associated kinase 1 (IRAK1), which is the proximal activator of
the NF-κB cascade, is downregulated bymicrobiota-derived
lipopolysaccharide (LPS)14. The polyubiquitylation and degradation
of IκB can beinhibited by commensal bacteria, which inhibit a
common ubiquitin ligase by inducing reactive oxygen
species (ROS)70. Peroxisome proliferator- activated
receptor-γ (PPARγ), which is induced in response toTLR4
activation by LPS71, can also divert NF-κB from the nucleus72.
Checkpoints that are controlled bythe microbiota are indicated by T
bars. Interestingly, PPARγ positively controls the expression
of the
colonic microbicidal peptide defensin 1 (REF. 69) and thus
can simultaneously sustain the gut barrierand prevent excessive
inflammation. This mechanism may be impaired in a subset of
patients with
colonic Crohn’s disease69. PAMP, pathogen-associated molecular
pattern.
P E R S P E C T I V E S
NATURE REVIEWS | IMMUNOLOGY VOLUME 10 | OCTOBER 2010
| 737
© 20 Macmillan Publishers Limited. All rights reserved10
-
8/16/2019 Nature the Immune System and the Gut
4/10
|
Intestinal epithelium
Lamina propria
Bacterium
CD103+ DC
Peyer’s patch and CD103+ DCsmigrate to MLNs and
initiateadaptive immune responses
Peyer’s patch
Intestinal lumen
Microbiota-derived productsactivate TLRs
BAFF and APRILpromote T cell-dependent andT cell-independentIgA
class-switching
IgA+ plasma cell
IgA molecules aretranscytosed by polymericIgA receptors and
retainbacteria in the mucus
DimericsecretoryIgA
Mucus layer
TLR
M cell
Naive T cell
TCR
MHC
Peptide
Epithelialcell
BAFF,APRIL
a
cb
TSLP,TGFβ,retinoicacid
Tolerogenic DC FOXP3+
TReg cell
TH17 cell TH1 cell
ATPSAA
InflammatoryDCs
IL-1, IL-6,IL-23
IL-12
SFB
B. fragilis capsularpolysaccharide A
B. fragilis
TReg cellinduction
TReg cells maintaintolerance to foodand commensals
TH1 and TH17 cells sustain intestinal barrierby recruiting
macrophages and neutrophilsand inducing antibacterial defensins
Bacterial ATP andbacteria-inducedSAA activate DCs
SFB induceIL-12-producingDCs by unknownmechansims
CX3CR1-expressingphagocyte
Direct sampling of bacteria in lumen?Antigen transfer?
CD103+ DCs acquirebacterial antigens
Transcytosed bacteria areacquired by DCs, which activateadaptive
immune responses
Figure 2 | | Modulation of adaptive immune responses in the gut
by the
microbiota. a | Intestinal adaptive immune responses can be
initiated in
Peyer’s patches or in mesenteric lymph nodes (MLNs). Activated T
and B cells
subsequently leave these lymphoid tissues and home to the
intestinal lamina
propria via the bloodstream. Bacteria are mainly sampled by
Peyer’s patch
dendritic cells (DCs) after transcytosis across the specialized
epithelium that
overlays these lymphoid organs. It has also been suggested that
a population
of CX3C-chemokine receptor 1 (CX3CR1)+ lamina propria cells
with both DC-
and macrophage-like characteristics can send dendrites into the
intestinal
lumen and directly capture bacteria. Their role in antigen
presentation
remains controversial73,74, but they may pass antigens to lamina
propria
CD103+ DCs, which can migrate to the MLNs and present
antigens to T cells74.
b | Microbiota-derived products activate Toll-like
receptors (TLRs) that are
expressed by intestinal epithelial cells, which leads to the
production of
B cell-activating factor (BAFF) and a proliferation-inducing
ligand (APRIL);
these cytokines promote both T cell-dependent and T
cell-independent IgA
class-switching responses in the intestine75,76. Plasma cells
produce dimeric
IgA molecules that are transcytosed into the intestinal lumen by
the epithe-
lial polymeric Ig receptor, the expression of which is
upregulated by the
microbiota. The extracellular part of this receptor remains
associated with
IgA following release into the lumen and forms secretory IgA.
These
secretory IgA molecules form immune complexes with bacteria,
which are
then retained in the mucus. c | CD103+ DCs are
‘conditioned’ by epithelial
cell-derived factors, such as thymic stromal lymphopoietin
(TSLP), transform-
ing growth factor-β (TGFβ) and retinoic acid, to acquire a
tolerogenic pheno-type; these DCs can promote the induction of
forkhead box P3 (FOXP3) +
regulatory T (TReg
) cells77. Bacteria-derived products, such as the capsular
polysaccharide A from Bacteroides fragilis, can further promote
the induction
of interleukin-10 (IL-10)-producing TReg cells through a
TLR2-dependentmechanism15,17. However, some commensal bacteria can
stimulate the dif-
ferentiation of inflammatory mucosal T cells. T helper 17 (TH17)
cell differen-
tiation can be promoted by bacteria-derived ATP, which activates
a subset of
DCs that produce IL-1β, IL-6 and IL-23 (REF. 78), or by serum
amyloid A pro-tein (SAA), which is an acute phase protein that is
produced in response to
segmented filamentous bacteria (SFB)23. SFB can also drive the
expansion of
mucosal TH1 cell populations11, presumably by inducing IL-12
production by
DCs. In addition, inflammatory DCs might stimulate the
conversion of
TReg
cells into TH17 and/or T
H1 cells in the lamina propria (not shown)79. T
H1
and TH17 cells maintain the intestinal barrier by recruiting and
activating
macrophages and neutrophils that eliminate penetrating bacteria.
IL-22 that
is produced by a subset of TH17 cells can also promote the
production of
antibacterial defensins by epithelial cells. M cell, microfold
cell.
P E R S P E C T I V E S
738 | OCTOBER 2010 | VOLUME 10
www.nature.com/reviews/immunol
© 20 Macmillan Publishers Limited. All rights reserved10
-
8/16/2019 Nature the Immune System and the Gut
5/10
|
Intestinal colonization by SFB
Effects on intestinal compartmentEffects on peripheral
compartment
Arthritis inK/BxN mice
Increasedseverity of EAE
Physiological inflammationstrengthens gut barrier
inimmunocompetent hosts
Intestinal inflammationin SCID mice transferredwith effector T
cells
• Stimulation of innate immuneresponses e.g. Reg
IIIβ /γ production
• Stimulation of CD4+ T cell responses e.g.↑ TH1,
TH2, TH17 and TReg cells
• Induction of IgA responses• Recruitment and
activation of IELs
• Increased germinal centreformation in the spleen
↑ Autoantibody-secretingIgG plasma cells
↑ Circulating immunecomplexes
• Enhancedsensitizationfollowingchallenge withMOG
peptide
unusual symbiont has a particularly impor-tant role in shaping
the gut immune systemacross evolution. However, again, the out-come
of SFB–host interactions depends onthe immune status of the host;
SFB has beenassociated with the development of
intestinalinflammation29 or arthritis30 in mice
withimpaired immunoregulation and can alsoaggravate experimental
autoimmune enceph-alomyelitis31 (FIG. 3). Interestingly, SFB
alonewere not able to induce intestinal inflamma-tion in
immunodeficient mice and insteadsynergized with a pathogen-free
flora. Thisfinding highlights how interactions in themicrobiota
community can influence hostimmune responses, thereby adding
anadditional level of complexity.
The case of pathobionts. A particular sub-set of bacteria
further exemplifies how thebehaviour of the microbiota is dependent
on
the immune status of the host. Although thesebacteria, which are
known as pathobionts,colonize the gastrointestinal tract of
manyindividuals asymptomatically, they also havethe potential to
cause disease. A recent studyshowed that Helicobacter hepaticus,
whichis a member of the epsilon subgroup ofproteobacteria, uses its
type VI secretion system (T6SS) to regulate bacterial
colonization andinhibit host innate and adaptive immuneresponses,
thereby actively maintainingsymbiotic relationships with
immunocom-petent hosts32. However, this bacterium cancause severe
typhocolitis in Il10–/– mice orin the severe combined
immunodeficient(SCID) transfer model of colitis. Thesefindings
highlight the central role of hostadaptive regulatory responses in
main-taining symbiotic relationships with themicrobiota32.
In humans, the most classical exampleof a pathobiont is
Helicobacter pylori, whichuses various mechanisms to dampen
hostimmune responses and persist in the stom-ach. Gastric
colonization by this bacteriumremains asymptomatic in most
individu-als and has even been suggested to protect
against the development of oesophagealcarcinomas owing to
downmodulation ofgastric acid secretion. Yet this bacteriumis the
major cause of gastritis and gastriccancers. The circumstances that
lead to thisbacterium becoming a serious health con-cern are not
completely understood but arethought to include the selection of
specifi-cally aggressive strains and/or host predis-posing factors,
notably polymorphisms ingene promoters that increase the
productionof tumour necrosis factor (TNF) or IL-1β,which is a
pro-inflammatory cytokine
with potent acid-suppressive properties33.Other recently
characterized pathobiontsinclude enterotoxigenic B.
fragilis (ETBF),which can stimulate colonic inflammationand
tumorigenesis in predisposed multipleintestinal neoplasia
(MIN) mice34, and someEscherichia coli strains, which can
promotegut inflammation in patients with Crohn’sdisease35,36.
Intestinal dysbiosis and IBDs
Inflammatory bowel diseases (IBDs) are
thought to arise owing to a combination ofgenetic and
environmental factors that resultin dysregulated immune responses
to the gutmicrobiota and the subsequent developmentof gut
inflammation20. Compelling evidencefrom a variety of studies has
shown dysbiosisin patients with IBD compared with healthycontrols,
and this suggests a causative role fordysbiosis in gut
inflammation.
Several scenarios can be considered.Pro-inflammatory bacteria,
such as entero-invasive Escherichia coli strains, are
morefrequently seen in the ileal mucosa of
patients with Crohn’s disease than in healthycontrols, which
suggests that these bacteriacan initiate disease36. Yet to induce
intestinalinflammation, the prototype E. coli LF82strain first
needs to bind to an epithelialcell-expressed receptor. This
receptoris absent in the normal ileal mucosa but isupregulated by
interferon-γ (IFNγ) andTNF that are produced during
intestinalinflammation35,37. An alternative hypo-thesis suggests
that the reduced frequencyof a Firmicutes species,
Faecalibacterium
prausnitzii, in the intestinal microbiota isa causative
factor of Crohn’s disease16. Thisstrain releases an unidentified
soluble factor,which inhibits pro-inflammatory epithelialcell
responses in vitro and attenuatesinflammation in a mouse
model of colitis16.
Other studies, however, suggest thatmore global changes in the
compositionof the microbiota are associated with IBD,such as
abnormal adherence of bacteria tothe gut mucosa, reduced bacterial
diversity,decreased levels of resident Firmicutes spp.and/or
Bacteroides spp. and an overgrowth
Figure 3 | Effects of SFB colonization on the immune
system. Segmented filamentous bacteria
(SFB) are spore-forming bacteria that are related to the genus
Clostridium28. Inherited from the
mother microbiota, SFB develop strong interactions with the
ileal mucosa and in immunocompe-
tent mice, the bacteria can largely recapitulate the inducing
effects of the whole microbiota on
the postnatal maturation of the gut immune system. SFB induce
the production of Reg IIIβ/γ micro-bicidal peptides10,23,80,
which protect against colonizing pathogens24. Additionally, SFB
simultane-
ously activate strong secretory IgA responses22, induce the
recruitment and activation of cytotoxic
intraepithelial lymphocytes (IELs)81 and drive various T
cell responses, including a robust T helper 17
(TH17) cell response11,23. In immunocompetent mice, SFB-induced
pro-inflammatory and regulatory
responses balance each other, which results in physiological
inflammation that strengthens the
gut barrier. By contrast, colonization by SFB promotes the
development of colitis in severe com-
bined immunodeficient (SCID) mice that have been reconstituted
with effector T cells29. Intestinal
colonization by SFB can also promote the development of
inflammatory diseases outside of the
gut. SFB promote arthritis in autoimmune non-obese diabetic
(NOD) mice that express a trans-
genic T cell receptor (TCR) that is specific for a self peptide
(known as K/BxN mice), an effect
ascribed to the induction of TH17 cells 30. SFB also enhance the
severity of myelin oligodendrocyte
glycoprotein (MOG)-induced experimental autoimmune
encephalomyelitis (EAE). These aggravating
effects may reflect the strong adjuvant properties of SFB.
TReg
cells, regulatory T cells.
P E R S P E C T I V E S
NATURE REVIEWS | IMMUNOLOGY VOLUME 10 | OCTOBER 2010
| 739
© 20 Macmillan Publishers Limited. All rights reserved10
-
8/16/2019 Nature the Immune System and the Gut
6/10
|
a b
Physiological microbiota
Pathobiont
Damaged epithelialbarrier, increasedbacterial adherenceand
penetration
‘Peace-keeping’bacterium
Mucus
Laminapropria
Healthyepithelial
barrier
Physiological inflammation
Pathological inflammation
TH17 cell
TReg cellTH1 cell
IgA+
plasma cell
Gutlumen
Healthy gut environmentAltered gut environmentAntibiotics, diet,
hygiene,pollutants, virus?
Dysbiosis
Decrease in ‘peace-keeping’ bacteriaand increase in
pathobionts
Severe monogenicimmunodeficiencyIL-10R mutations,
CVID
Immunegene variantsNOD2, ATG16L1,
IL-23R, IRGM
Genetics
Environment
Stress, diet, infections, vaccine?
Altered host immune system
of proteobacteria38–40. Strikingly, comparablechanges in the
microbiota have been seenin mice in which intestinal
inflammationwas induced by either an invasive pathogenor by the
injection of transgenic T cellsthat attacked the gut epithelium27.
In thesetwo distinct models, host inflammationsuppressed the growth
of Firmicutes andBacteroides spp., allowing proteobacteria,which
are apparently more resistant to host-derived microbicidal factors,
to outcompetethese normally dominant resident bacteria27.Notably,
outgrowth of proteobacteria was
also seen in Il10–/– mice after, but not before,the onset
of intestinal inflammation, whichfurther highlights the profound
influence ofthe host immune response on the structureof the
microbial community 27.
Together, these observations underscorethe confounding role of
host-predisposingfactors and the difficulty in assigning acausative
role for dysbiosis in IBD. However,experimental evidence suggests
that intes-tinal inflammation can select for bacterialspecies with
colitogenic properties. In
T -bet –/– Rag2–/– ulcerative
colitis (TRUC) mice, the
inability of DCs to properly regulate TNFproduction results in a
severe and highlypenetrating colitis. Intestinal
inflammationspontaneously progresses to colonic dyspla-sia and
rectal adenocarcinoma; therefore,disease progression in this model
is similarto that seen in human IBD41,42. TRUC colitiscan be
prevented by eradicating the micro-biota with broad-spectrum
antibiotics.Moreover, in a situation that recalls rarereports of
intrafamilial transmission of IBDin humans, colitis can be
transmitted fromTRUC mice to wild-type mice in both cross-fostering
and co-housing experiments41.Furthermore, the microbiota in
TRUCmice exhibits complex changes, includingselective enrichment of
two proteobacteria,Proteus mirabilis and Klebsiella
pneumonia.These two bacteria are not sufficient toinduce colitis in
gnotobiotic TRUC mice;however, they can colonize the intestine
of wild-type mice and, in concert with apathogen-free
microbiota, induce colonicinflammation43. These data highlight
howthe host immune response can shape themicrobiota and eventually
lead to the selec-tion of aggressive bacteria, which not
onlysurvive in the inf lamed gut but also promoteinflammation.
What are the therapeutic implicationsof these findings? At the
very least, theyexplain the difficulties in establishing
andmaintaining remission in patients with IBDusing drugs that
target host inflammatorycomponents or the microbiota without
alsocorrecting host-predisposing factors. Theyhighlight the
importance of identifyingsuch predisposing factors and
designingmore specific therapies for IBD. They alsosuggest the need
for combined approachesthat can restore local ecological
conditionsand correct dysbiosis to reinstate
balancedhost–microbiota interactions in the longterm (FIG. 4).
Microbiota and systemic immunity
So far we have focused on the roles of themicrobiota in
intestinal immunity, both
in health and disease; however, growingevidence suggests that
the intestinal micro-biota can also have an important impact onthe
development of the peripheral immunesystem. Moreover, dysbiosis has
beenimplicated in the development of extra-intestinal
immune-mediated diseases. It willbe crucial to determine the extent
to whichthe impact of the microbiota dependson the host immune
status, whether indi-
vidual bacterial species can exert distinctiveroles and,
ultimately, whether the observeddysbiosis has a causative role in
disease.
Figure 4 | Schematic representation of host–microbiota
interactions in the healthy and
inflamed gut. a | In healthy hosts, an efficient immune
barrier contains the microbiota in the gut
lumen and feedback mechanisms avoid excessive activation of host
immune responses. ‘Peace-
keeping’ bacteria that release anti-inflammatory products
participate in the tuning of host responses
towards tolerance and help to prevent the pro-inflammatory
effects of any pathobionts that are
present in the microbiota, thus maintaining intestinal
homeostasis. b | Immunodeficient patients,
who lack an important component of the gut barrier (for example,
secretory immunoglobulins in
patients with common variable immunodeficiency (CVID)19) or a
key regulatory pathway (for exam-
ple, loss-of-function mutations that affect the interleukin-10
receptor (IL-10R)21) spontaneouslydevelop intestinal inflammation
when exposed to the microbiota. In more common forms of inflam-
matory bowel disease (IBD), a complex genetic background results
in more subtle alterations of gut
immune responses that may weaken the gut barrier and/or impair
immunoregulation82. In these indi-
viduals, lifestyle changes or medical practices (for example,
stress, diet, hygiene, smoking, antibiotics,
vaccines or appendectomy) may promote the onset of gut
inflammation by affecting the immune
balance and/or the gut microbiota82. Intestinal inflammation
results in increased bacterial adherence,
epithelial damage and increased entry of bacteria into the
intestinal lamina propria, thus sustaining
a vicious inflammatory circle. Moreover, inflammation can favour
the selection of aggressive patho-
bionts, which are more resistant to host-derived microbicidal
mediators26,27, and reduce the number
of peace-keeping species16, which results in even more severe
and uncontrolled inflammation. These
pathobionts might become sufficiently aggressive to also cause
disease in immunocompetent indi-
viduals43. ATG16L1, autophagy-related 16-like 1; IRGM,
immunity-related GTPase family M; SCID,
severe combined immunodeficient; TH cell, T helper cell;
T
Reg cell, regulatory T cell.
P E R S P E C T I V E S
740 | OCTOBER 2010 | VOLUME 10
www.nature.com/reviews/immunol
© 20 Macmillan Publishers Limited. All rights reserved10
-
8/16/2019 Nature the Immune System and the Gut
7/10
Effects on the peripheral immune system. The exact impact
of the gut microbiota onthe host’s peripheral immune system is
con-troversial. Two groups have convincinglyshown that specific
immune responses tothe intestinal microbiota are largely confinedto
the intestinal lymphoid compartment inimmunocompetent mice with an
efficientgut barrier13,44,45. However, studies compar-ing mice that
were raised in conventionalor germ-free conditions highlight
theimportance of the intestinal microbiota forthe development of
the peripheral immunesystem in immunocompetent hosts. Notably,the
spleens of germ-free mice contain fewerand smaller germinal
centres46 and decreasednumbers of memory CD4+ T cells,
andcytokine production by these T cells shows aT
H2-type profile47.The mechanisms that underlie the
stimulatory effects of the microbiota on the
peripheral immune system of immuno-competent hosts are not well
understood.Recent work suggests that soluble factorsthat are
produced by the microbiota cantranslocate from the gut to the
bloodstreamand activate innate immune cells. Forexample, the
opsonophagocytic activity ofneutrophils is primed by
microbiota-derivedpeptidoglycan, which results in
enhancedprotection against pneumococcal sepsis48.Moreover,
monocolonization with B. fragilis corrects systemic T cell
deficiencies andthe T
H1/T
H2 imbalance of germ-free mice
due to the stimulation of DC IL-12 produc-tion by the
bacterium’s unusual capsularpolysaccharide47.
Allerg y and dysbiosis. The ‘hygienehypothesis’,
which has been revisedseveral times since its initial formula-tion
by Strachan in 1989, stipulates thatdecreased exposure to
infectious agents,as well as changes in the intestinal micro-biota
during infancy, might alter immuneregulatory networks and account
for thedramatic increase in the incidence ofallergic diseases that
has been observed in
developed countries49. Several studies havereported differences
in the compositionof the faecal microbiota of infants whodevelop an
allergic disease and those whodo not. Notably, a decreased
frequencyof Lactobacillus and Bifidobacterium spp.has
been suggested to precede the onsetof allergy 50, and
prophylactic approaches,which are based on the administration
ofprobiotics to mothers and newborns athigh risk for IgE-associated
allergies, havebeen initiated. A recent study reportsthat 1 month
of prenatal and 6 months of
postnatal pre- and probiotic supplementa-tion can reduce the
incidence of eczemaand food-specific IgE in a subset of high-risk
children who are born by caesareansection51. This protective effect
was notseen in vaginally delivered children andwas transient, as it
was significant at2 years of age but not by 5 years of age.
The results of such interventions remainconflicting and a
causative link between dys-biosis, which is induced by changes in
life-style or recent medical practices, and allergyremains
difficult to establish51,52. Moreover,experimental studies that
support the roleof the microbiota in the development ofallergic
diseases are still scarce (TABLE 1). Onestudy has reported
increased developmentof allergic airway disease in mice that
weretreated with a short course of oral antibiot-ics53. Another
interesting study showed thatTLR4 activation by
microbiota-derived
LPS was necessary to prevent anaphylaxisafter oral immunization
with the peanut-derived allergen Arah 1. TLR4-deficient
orantibiotic-treated mice showed an increasedT
H2-type skewing of cytokine responses
compared with control mice. Conversely,activation of TLR9 by
oral administration ofCpG oligodeoxynucleotides could
abrogateallergic symptoms and correct the T
H1/T
H2
imbalance54. However, additional work isneeded to delineate
whether and how thecomposition of the microbiota mightinfluence the
onset of allergy.
Autoimmunity and the microbiota. Thepossibility that
the intestinal microbiota isinvolved in the development of
systemicautoimmunity has recently attracted grow-ing attention.
Changes in the composition ofthe gut flora have been reported in
patientsin the early phases of rheumatoid arthritis55 when
compared with a control group withfibromyalgia. However, such
studies cannotestablish a link between dysbiosis and thedevelopment
of disease. Therefore, the roleof the microbiota has been more
directlyaddressed by comparing the onset and/or
severity of experimental autoimmune dis-eases in germ-free mice
with disease onsetand/or severity in mice that have beencolonized
by a diverse microbiota.
In several models of autoimmunity,the progression of disease was
compa-rable between both sets of mice56–58. Inother models,
contradictory roles for themicrobiota have been reported (TABLE
1).The microbiota was shown to triggerdisease in several mouse
models of auto-immune arthritis. For example, in a mousestrain that
is prone to the spontaneous
development of an autoimmune ankylosingenthesopathy , disease
does not developunder germ-free conditions. Furthermore,disease
develops in mice that are colonizedwith a mixture of culturable
anaerobesbut not in mice that are colonized withLactobacillus or
Staphylococcus spp.59. Thisfinding suggests a role for a
specific com-ponent (or components) of the microbiotain disease
progression. A triggering rolefor the microbiota, specifically for
SFB, wasalso seen in the autoimmune arthritis thatdevelops in K/BxN
mice30. In this model,an uncontrolled T
H17 cell response that is
induced by SFB stimulated the productionof autoantibodies and
led to the deposi-tion of immune complexes in the joints(FIG. 3).
The microbiota also promoteddisease in another IL-17-dependent
modelof arthritis, which develops in mice thatlack the IL-1
receptor antagonist60. Finally,
the microbiota and, to a lesser degree, SFBenhanced the severity
of experimentalautoimmune encephalomyelitis31. Theaggravating role
of the microbiota in thesemodels is consistent with its central
role inthe induction of T
H17 cell responses.
By contrast, the microbiota was shownto have a protective role
in collagen-induced arthritis61 and to prevent
diabetesdevelopment in myeloid differentiationprimary-response
protein 88 (MYD88)-deficient non-obese diabetic (NOD) mice62,as in
both models disease was more severeif animals were housed in
germ-free condi-tions. It remains unclear why a protectiverole for
the microbiota during the develop-ment of diabetes is seen in the
presenceof impaired TLR signalling. The completelack of TLR
signalling in Myd88–/– Trif(TIR-domain-containing adaptor
proteininducing IFNβ)–/– mice has been associ-ated with
abnormal bacterial translocationinto the spleen and activation of
systemicadaptive responses. It will be interesting toevaluate
whether comparable mechanismsoperate in Myd88–/– NOD mice
and par-ticipate in the protection against diabetes.
Interestingly, the caecal microbiota of Myd88–/– NOD
mice differed significantlyfrom that of NOD mice and could
attenuatethe development of type 1 diabetes whentransferred to the
newborn progeny ofgerm-free NOD mice62; this suggests thatone or
more species that confer protectionagainst disease might have been
selectedfor in the NOD mice with impairedTLR signalling.
Taken together, these data providenovel examples of the complex
interplaythat exists between the host immune
P E R S P E C T I V E S
NATURE REVIEWS | IMMUNOLOGY VOLUME 10 | OCTOBER 2010
| 741
© 20 Macmillan Publishers Limited. All rights reserved10
-
8/16/2019 Nature the Immune System and the Gut
8/10
also indicates the possible contribution ofthe intestinal
microbiota to immunologicaldiseases outside the gut. However, from
themicrobial perspective, the host is simply acomplex environment
and the distinctionbetween health and disease is importantonly as
far as it affects microbial fitness.The challenge that lies ahead
is to determinewhen changes in our microbiota are theprimary cause
of a disease and when thesechanges merely reflect the enormous
capacityof bacteria for rapid and continuous genetic
system and the microbiota, and the dif-ficulties in attempting
to delineate therespective roles of host predisposingfactors and
specific bacterial species. Todetermine the therapeutic
implicationsof these observations, further research isneeded to
elucidate how the microbiotais able to influence peripheral
immuneresponses and how such microbiota-driven responses can
interfere with theimmunological mechanisms that underliea given
autoimmune disease.
Conclusion
An increasing number of studies are pro-gressively unravelling
the fascinating inter-actions that occur between eukaryotes
andtheir bacterial symbionts. It is now clearthat the intestinal
microbiota profoundlyinfluences host metabolic and immunepathways
and participates in human healthand disease. Compelling evidence
shows apivotal role for the microbiota in the devel-opment of many
gastrointestinal diseases,from inflammation to cancer. Recent
work
Table 1 | Effect of the microbiota on systemic
immune-mediated diseases
Model Animal strain Protocol to alter microbiota Observed
effects Refs
Allergy
IgE-mediated food allergyto peanut allergen
Weanling C3H mice orC57BL/6 mice
Oral cocktail of antibiotics for 3 weeks Induction of
anaphylacticsymptoms, increased production ofIgE and IL-13
54
Tlr4 mutant or Tlr4–/– mice None
IgE-mediated allergicairway disease inducedby Aspergillus
fumigatus spores or ovalbumin
BALB/c and C57BL/6 mice Oral cefoperazone (Cefobid,
Pfizer;Cefazone, Pharco B International)for 5 days and a single
oral gavage ofCandida albicans
Increase in pulmonary eosinophilsand enhanced synthesis of IgE,
IL-5and IL-13
49,53
Autoimmunity
Systemic lupuserythematosus
MRL/lpr mice Germ-free mice No change in autoimmunity
58
APECED Aire–/– mice* Germ-free mice No change in
autoimmunity 56
Spontaneous gastritis Aid–/– mice‡ Germ-free mice No
change in autoimmunity 57
Collagenous arthritis Fischer rats (resistant) Germ-free rats
Enhanced humoral responses 61
Dark Agouti rats (sensitive) Germ-free rats Increased
severity
Type 1 diabetes NOD mice§ x Myd88 –/–mice Germ-free
mice Increased incidence and severity 62
NOD Myd88–/–mice Colonization with specificpathogen-free
flora
No disease
Spontaneous ankylosingenthesopathy
Male B10.BR mice Germ-free mice No disease 59
Colonization with probioticLactobacillus spp.
No disease
Colonization with a mixture ofBacteroides, Enterococcus,
Veillonella and Staphylococcus spp.
Disease restored
Spontaneous arthritis Il1Ra–/– BALB/c mice Germ-free
mice No disease 60
Colonization with Lactobacillus bifidus Disease restored
Il1Ra–/– Tlr4–/– mice None Same disease
incidence,decreased severity
Il1Ra–/– Tlr2–/– mice None Increased severity
Autoimmune arthritis KRN-C57BL/6|| NOD mice Germ-free mice
No disease 30
Colonization with segmentedfilamentous bacteria
Disease restored
Experimentalautoimmuneencephalomyelitis
C57BL/6J mice Germ-free mice Weak severity 31
Specific pathogen-free flora Maximal severity
Colonization with segmentedfilamentous bacteria
Intermediate severity
Aid, activation-induced cytidine deaminase; Aire,
autoimmune regulator; APECED, autoimmune
polyendocrinopathy-candidiasis-ectodermal dystrophy;
IL,interleukin; Il1Ra, IL-1 receptor antagonist; Myd88, myeloid
differentiation primary-response protein 88; NOD, non-obese
diabetic; Tlr , Toll-like receptor. *AIREregulates the
transcription of peripheral autoantigens in medullary thymic
epithelial cells and is necessary for thymic negative selection;
‡AID is central forclass-switch recombination and somatic
hypermutation in B cells; §NOD mice provide a polygenic model of
type 1 diabetes; ||Mice with a transgenic T cell receptoragainst a
self peptide that is derived from glucose-6-phosphate
isomerase.
P E R S P E C T I V E S
742 | OCTOBER 2010 | VOLUME 10
www.nature.com/reviews/immunol
© 20 Macmillan Publishers Limited. All rights reserved10
-
8/16/2019 Nature the Immune System and the Gut
9/10
19. Malamut, G. et al. The enteropathy associated with
common variable immunodeficiency: the delineated
frontiers with celiac disease. Am. J.
Gastroenterol.
15 Jun 2010 (doi:10.1038/ajg.2010.214).
20. Bouma, G. & Strober, W. The immunological and
genetic basis of inflammatory bowel disease. Nature
Rev. Immunol. 3, 521–533 (2003).
21. Glocker, E. O. et al. Inflammatory bowel disease
and
mutations affecting the interleukin-10 receptor.
N. Engl. J. Med. 361, 2033–2045 (2009).
22. Talham, G. L., Jiang, H. Q., Bos, N. A. & Cebra, J.
J.
Segmented filamentous bacteria are potent stimuli ofa
physiologically normal state of the murine gut
mucosal immune system. Infect. Immun. 67,
1992–2000 (1999).
23. Ivanov, I. I. et al. Induction of intestinal Th17 cells
by
segmented filamentous bacteria. Cell 139, 485–498
(2009).
24. Brandl, K. et al. Vancomycin-resistant enterococci
exploit antibiotic-induced innate immune deficits.
Nature 455, 804–807 (2008).
25. Klaasen, H. L. et al. Intestinal, segmented,
filamentous
bacteria in a wide range of vertebrate species.
Lab. Anim. 27, 141–150 (1993).
26. Lupp, C. et al. Host-mediated inflammation disrupts
the intestinal microbiota and promotes the overgrowth
of Enterobacteriaceae . Cell Host Microbe 2, 119–129
(2007).
27. Stecher, B. et al. Salmonella enterica serovar
typhimurium exploits inflammation to compete with
the intestinal microbiota. PLoS Biol. 5, 2177–2189
(2007).
28. Snel, J. et al. Comparison of 16S rRNA sequences of
segmented filamentous bacteria isolated from mice,
rats, and chickens and proposal of “Candidatus
Arthromitus”. Int. J. Syst. Bacteriol. 45,
780–782
(1995).
29. Stepankova, R. et al. Segmented filamentous
bacteria
in a defined bacterial cocktail induce intestinal
inflammation in SCID mice reconstituted with
CD45RBhigh CD4+ T cells. Inflamm. Bowel
Dis. 13,
1202–1211 (2007).
30. Wu, H.-S. et al. Gut-residing segmented filamentous
bacteria drive autoimmune arthritis via T helper 17
cells. Immunity 32, 815–827 (2010).
31. Lee, Y. K., Menezes, J. S., Umesaki, Y. &
Mazmanian, S. K. Microbes and health sackler
colloquium: proinflammatory T-cell responses to gut
microbiota promote experimental autoimmune
encephalomyelitis. Proc. Natl Acad. Sci. USA 28 Jul
2010 (doi:10.1073/pnas.10000.82107).
32. Chow, J. & Mazmanian, S. K. A pathobiont of the
microbiota balances host colonization and
intestinalinflammation. Cell Host Microbe 7, 265–276
(2010).
33. Polk, D. B. & Peek, R. M. Jr. Helicobacter
pylori :
gastric cancer and beyond. Nature Rev. Cancer 10,
403–414 (2010).
34. Wu, S. et al. A human colonic commensal promotes
colon tumorigenesis via activation of T helper type 17
T cell responses. Nature Med. 15, 1016–1022
(2009).
35. Carvalho, F. A. et al. Crohn’s disease adherent-
invasive Escherichia coli colonize and induce
strong
gut inflammation in transgenic mice expressing
human CEACAM. J. Exp. Med. 206, 2179–2189
(2009).
36. Darfeuille-Michaud, A. et al. High prevalence of
adherent-invasive Escherichia coli associated with
ileal
mucosa in Crohn’s disease. Gastroenterology 127,
412–421 (2004).
37. Barnich, N. et al. CEACAM6 acts as a receptor for
adherent-invasive E. coli , supporting ileal mucosa
colonization in Crohn disease. J. Clin.
Invest. 117,1566–1574 (2007).
38. Frank, D. N. et al. Molecular-phylogenetic
characterization of microbial community imbalances in
human inflammatory bowel diseases. Proc. Natl Acad.
Sci. USA 104, 13780–13785 (2007).
39. Sokol, H. et al. Specificities of the fecal microbiota
in
inflammatory bowel disease. Inflamm. Bowel Dis. 12,
106–111 (2006).
40. Swidsinski, A., Weber, J., Loening-Baucke, V., Hale, L.
P.
& Lochs, H. Spatial organization and composition of
the mucosal flora in patients with inflammatory bowel
disease. J. Clin. Microbiol. 43, 3380–3389 (2005).
41. Garrett, W. S. et al. Communicable ulcerative
colitis
induced by T-bet deficiency in the innate immune
system. Cell 131, 33–45 (2007).
42. Garrett, W. S. et al. Colitis-associated colorectal
cancer
driven by T-bet deficiency in dendritic cells. Cancer
Cell
16, 208–219 (2009).
43. Garrett, W. et al. Enterobacteriaceae act in
concert
with the gut microbiota to induce spontaneous and
maternally-transmitted colitis. Cell Host Microbe
(in the press).
44. Konrad, A., Cong, Y., Duck, W., Borlaza, R. &
Elson, C. O. Tight mucosal compartmentation of the
murine immune response to antigens of the enteric
microbiota. Gastroenterology 130, 2050–2059
(2006).
45. Slack, E. et al. Innate and adaptive immunity
cooperate flexibly to maintain host-microbiota
mutualism. Science 325, 617–620 (2009).46. Bauer, H.,
Horowitz, R. E., Levenson, S. M. &
Popper, H. The response of the lymphatic tissue
to the microbial flora. Studies on germfree mice.
Am. J. Pathol. 42, 471–483 (1963).
47. Mazmanian, S. K., Liu, C. H., Tzianabos, A. O. &
Kasper, D. L. An immunomodulatory molecule of
symbiotic bacteria directs maturation of the host
immune system. Cell 122, 107–118 (2005).
48. Clarke, T. B. et al. Recognition of peptidoglycan
from
the microbiota by Nod1 enhances systemic innate
immunity. Nature Med. 16, 228–231 (2010).
49. Noverr, M. C. & Huffnagle, G. B. The ‘microflora
hypothesis’ of allergic diseases. Clin. Exp.
Allergy 35,
1511–1520 (2005).
50. Sjogren, Y. M., Jenmalm, M. C., Bottcher, M. F.,
Bjorksten, B. & Sverremark-Ekstrom, E. Altered early
infant gut microbiota in children developing allergy up
to 5 years of age. Clin. Exp. Allergy 39, 518–526
(2009).
51. Kuitunen, M. et al. Probiotics prevent
IgE-associated
allergy until age 5 years in cesarean-delivered children
but not in the total cohort. J. Allergy Clin.
Immunol.
123, 335–341 (2009).
52. Penders, J., Stobberingh, E. E., van den Brandt, P. A.
& Thijs, C. The role of the intestinal microbiota in the
development of atopic disorders. Allergy 62,
1223–1236 (2007).
53. Noverr, M. C., Falkowski, N. R., McDonald, R. A.,
McKenzie, A. N. & Huffnagle, G. B. Development of
allergic airway disease in mice following antibiotic
therapy and fungal microbiota increase: role of host
genetics, antigen, and interleukin-13. Infect. Immun.
73, 30–38 (2005).
54. Bashir, M. E., Louie, S., Shi, H. N. & Nagler-Anderson,
C.
Toll-like receptor 4 signaling by intestinal microbes
influences susceptibility to food allergy. J.
Immunol.
172, 6978–6987 (2004).
55. Vaahtovuo, J., Munukka, E., Korkeamaki, M.,
Luukkainen, R. & Toivanen, P. Fecal microbiota in early
rheumatoid arthritis. J. Rheumatol. 35, 1500–1505
(2008).56. Gray, D. H., Gavanescu, I., Benoist, C. & Mathis,
D.
Danger-free autoimmune disease in Aire-deficient
mice. Proc. Natl Acad. Sci. USA 104, 18193–18198
(2007).
57. Hase, K. et al. Activation-induced cytidine
deaminase
deficiency causes organ-specific autoimmune disease.
PLoS ONE 3, e3033 (2008).
58. Maldonado, M. A. et al. The role of environmental
antigens in the spontaneous development of
autoimmunity in MRL-lpr mice. J. Immunol. 162,
6322–6330 (1999).
59. Sinkorova, Z., Capkova, J., Niederlova, J.,
Stepankova, R. & Sinkora, J. Commensal intestinal
bacterial strains trigger ankylosing enthesopathy of
the ankle in inbred B10.BR (H-2k) male mice. Hum.
Immunol. 69, 845–850 (2008).
60. Abdollahi-Roodsaz, S. et al. Stimulation of TLR2
and
TLR4 differentially skews the balance of T cells in a
mouse model of arthritis. J. Clin. Invest. 118,
205–216 (2008).61. Breban, M. A., Moreau, M. C., Fournier,
C.,
Ducluzeau, R. & Kahn, M. F. Influence of the bacterial
flora on collagen-induced arthritis in susceptible and
resistant strains of rats. Clin. Exp. Rheumatol. 11,
61–64 (1993).
62. Wen, L. et al. Innate immunity and intestinal
microbiota in the development of Type 1 diabetes.
Nature 455, 1109–1113 (2008).
63. Giraud, A. et al. Dissecting the genetic components
of adaptation of Escherichia coli to the mouse
gut.
PLoS Genet. 4, e2 (2008).
64. Turnbaugh, P. J., Backhed, F., Fulton, L. & Gordon, J.
I.
Diet-induced obesity is linked to marked but reversible
alterations in the mouse distal gut microbiome.
Cell Host Microbe 3, 213–223 (2008).
65. Backhed, F. et al. The gut microbiota as an
environmental factor that regulates fat storage.
Proc. Natl Acad. Sci. USA 101, 15718–15723 (2004).
adaptation to new ecological conditions. Anin-depth
understanding of the principlesand mechanisms that underlie
microbialcommunity structures and host–symbiontrelationships will
be pivotal for the develop-ment of therapeutic approaches that
manip-ulate the intestinal microbiota to maintainhuman health.
Nadine Cerf-Bensussan and Valérie Gaboriau-Routhiau
are at the Institut National de la Santé et de la
Recherche Médicale (INSERM) U989, Université Paris
Descartes, 156 rue de Vaugirard, 75730 Paris
Cedex 15, France; and the Institut National de la
Recherche Agronomique (INRA) UM1319, Domaine de
Vilvert, 78350 Jouy-en-Josas, France.
Correspondence to N.C.-B.
e-mail: [email protected]
doi:10.1038/nri2850
1. Costello, E. K. et al. Bacterial community variation
in
human body habitats across space and time. Science
326, 1694–1697 (2009).
2. Gill, S. R. et al. Metagenomic analysis of the human
distal gut microbiome. Science 312, 1355–1359
(2006).3. Eberl, G. A new vision of immunity: homeostasis of
the
superorganism. Mucosal Immunol. 5 May 2010
(doi:10.1038/mi.2010.20).
4. Qin, J. et al. A human gut microbial gene catalogue
established by metagenomic sequencing. Nature 464,
59–65 (2010).
5. Moran, N. A., McCutcheon, J. P. & Nakabachi, A.
Genomics and evolution of heritable bacterial
symbionts. Annu. Rev. Genet. 42, 165–190 (2008).
6. Garrett, W. S., Gordon, J. I. & Glimcher, L. H.
Homeostasis and inflammation in the intestine.
Cell 140, 859–870 (2010).
7. Hooper, L. V. & Macpherson, A. J. Immune
adaptations that maintain homeostasis with the
intestinal microbiota. Nature Rev. Immunol. 10,
159–169 (2010).
8. Eberl, G. & Lochner, M. The development of
intestinal lymphoid tissues at the interface of self
and microbiota. Mucosal Immunol. 2, 478–485
(2009).9. Rescigno, M. & Di Sabatino, A. Dendritic cells
in
intestinal homeostasis and disease. J. Clin.
Invest.
119, 2441–2450 (2009).
10. Gaboriau-Routhiau, V. et al. The key role of
segmented
filamentous bacteria in the coordinated maturation of
gut helper T cell responses. Immunity 31, 677–689
(2009).
11. Vaishnava, S., Behrendt, C. L., Ismail, A. S.,
Eckmann, L.
& Hooper, L. V. Paneth cells directly sense gut
commensals and maintain homeostasis at the
intestinal host-microbial interface. Proc. Natl Acad.
Sci. USA 105, 20858–20863 (2008).
12. Peterson, D. A., McNulty, N. P., Guruge, J. L. &
Gordon, J. I. IgA response to symbiotic bacteria as a
mediator of gut homeostasis. Cell Host Microbe 2,
328–339 (2007).
13. Macpherson, A. J. & Uhr, T. Induction of protective
IgA by intestinal dendritic cells carrying commensal
bacteria. Science 303, 1662–1665 (2004).
14. Lotz, M. et al. Postnatal acquisition of
endotoxintolerance in intestinal epithelial cells. J. Exp.
Med. 203, 973–984 (2006).
15. Mazmanian, S. K., Round, J. L. & Kasper, D. L.
A microbial symbiosis factor prevents intestinal
inflammatory disease. Nature 453, 620–625
(2008).
16. Sokol, H. et al. Faecalibacterium
prausnitzii is an
anti-inflammatory commensal bacterium identified
by gut microbiota analysis of Crohn disease patients.
Proc. Natl Acad. Sci. USA 105, 16731–16736
(2008).
17. Round, J. L. & Mazmanian, S. K. Inducible
Foxp3+
regulatory T-cell development by a commensal
bacterium of the intestinal microbiota. Proc. Natl
Acad. Sci. USA 107, 12204–12209 (2010).
18. Fagarasan, S. et al. Critical roles of
activation-induced
cytidine deaminase in the homeostasis of gut flora.
Science 298, 1424–1427 (2002).
P E R S P E C T I V E S
NATURE REVIEWS | IMMUNOLOGY VOLUME 10 | OCTOBER 2010
| 743
© 20 Macmillan Publishers Limited. All rights reserved10
mailto:[email protected]:[email protected]
-
8/16/2019 Nature the Immune System and the Gut
10/10
66. Samuel, B. S. et al. Effects of the gut microbiota
on
host adiposity are modulated by the short-chain
fatty-acid binding G protein-coupled receptor, Gpr41.
Proc. Natl Acad. Sci. USA 105, 16767–16772
(2008).
67. Turnbaugh, P. J. et al. The human microbiome
project.
Nature 449, 804–810 (2007).
68. Vijay-Kumar, M.et al. Metabolic syndrome and
altered
gut microbiota in mice lacking Toll-like receptor 5.
Science 328, 228–231 (2010).
69. Peyrin-Biroulet, L. et al. Peroxisome proliferator-
activated receptor γ activation is required formaintenance
of innate antimicrobial immunity in thecolon. Proc. Natl Acad. Sci.
USA 107, 8772–8777
(2010).
70. Kumar, A. et al. Commensal bacteria modulate
cullin-dependent signaling via generation of reactive
oxygen species. EMBO J. 26, 4457–4466 (2007).
71. Dubuquoy, L. et al. Impaired expression of
peroxisome
proliferator-activated receptor γ in ulcerative
colitis.Gastroenterology 124, 1265–1276 (2003).
72. Kelly, D. et al. Commensal anaerobic gut bacteria
attenuate inflammation by regulating nuclear-
cytoplasmic shuttling of PPAR-γ and RelA.
NatureImmunol. 5, 104–112 (2004).
73. Chieppa, M., Rescigno, M., Huang, A. Y. &
Germain, R. N. Dynamic imaging of dendritic cell
extension into the small bowel lumen in response to
epithelial cell TLR engagement. J. Exp. Med. 203,
2841–2852 (2006).
74. Schulz, O. et al. Intestinal CD103+, but not
CX3CR1+,
antigen sampling cells migrate in lymph and serve
classical dendritic cell functions. J. Exp.
Med. 206,
3101–3114 (2009).
75. Tsuji, M. et al. Preferential generation of follicular
B
helper T cells from Foxp3+ T cells in gut Peyer’s
patches. Science 323, 1488–1492 (2009).
76. Cerutti, A. & Rescigno, M. The biology of intestinal
immunoglobulin A responses. Immunity 28, 740–750(2008).
77. Coombes, J. L. & Powrie, F. Dendritic cells in
intestinal
immune regulation. Nature Rev. Immunol. 8,
435–446 (2008).
78. Atarashi, K. et al. ATP drives lamina propria
TH17 cell
differentiation. Nature 455, 808–812 (2008).
79. Zhou, L., Chong, M. M. & Littman, D. R. Plasticity
of
CD4+ T cell lineage differentiation. Immunity 30,
646–655 (2009).
80. Keilbaugh, S. A. et al. Activation of
RegIIIβ/γ andinterferon γ expression in the intestinal
tract of SCIDmice: an innate response to bacterial colonisation
of
the gut. Gut 54, 623–629 (2005).
81. Umesaki, Y., Okada, Y., Matsumoto, S., Imaoka, A. &
Setoyama, H. Segmented filamentous bacteria are
indigenous intestinal bacteria that activate
intraepithelial lymphocytes and induce MHC class II
molecules and fucosyl asialo GM1 glycolipids on the
small intestinal epithelial cells in the ex-germ-free
mouse. Microbiol. Immunol. 39, 555–562 (1995).
82. Mayer, L. Evolving paradigms in the pathogenesis of
IBD. J. Gastroenterol. 45, 9–16 (2010).
AcknowledgementsThe authors thank W. Garrett for sharing
unpublished data.
Their work is supported by grants from the Institut National
de la Santé et de la Recherche Médicale (INSERM), theInstitut
National de la Recherche Agronomique (INRA) and
the Agence Nationale de la Recherche and Fondation
Princesse Grace. The authors are partners of the European
Community networks Cross-Talk (contract number
PITN-GA-2008-215553) and Tornado (FP7 222720).
Competing interests statementThe authors declare no competing
financial interests.
FURTHER INFORMATIONNadine Cerf-Bensussan’s
homepage: http://www.
fondationimagine.org/Nadine-Cerf-Bensussan_uk.php
ALL LINKS ARE ACTIVE IN THE ONLINE PDF
P E R S P E C T I V E S
744 | OCTOBER 2010 | VOLUME 10
www.nature.com/reviews/immunol
http://www.fondationimagine.org/Nadine-Cerf-Bensussan_uk.phphttp://www.fondationimagine.org/Nadine-Cerf-Bensussan_uk.phphttp://www.fondationimagine.org/Nadine-Cerf-Bensussan_uk.phphttp://www.fondationimagine.org/Nadine-Cerf-Bensussan_uk.php