Embed Size (px)
Citation preview

Nature-Nurture Interplay in Aggression and Antisocial
Behaviour
Emily Simonoff
Institute of Psychiatry
London
Size of the Problem
• Conduct disorders are the most common group of child psychiatric disorders
• In the UK, over one quarter have been to CAMHS and three-quarters have sought some professional help
Comorbidity
• About one-third of cases have another mental disorder
• About two-thirds have either a physical of developmental disorder
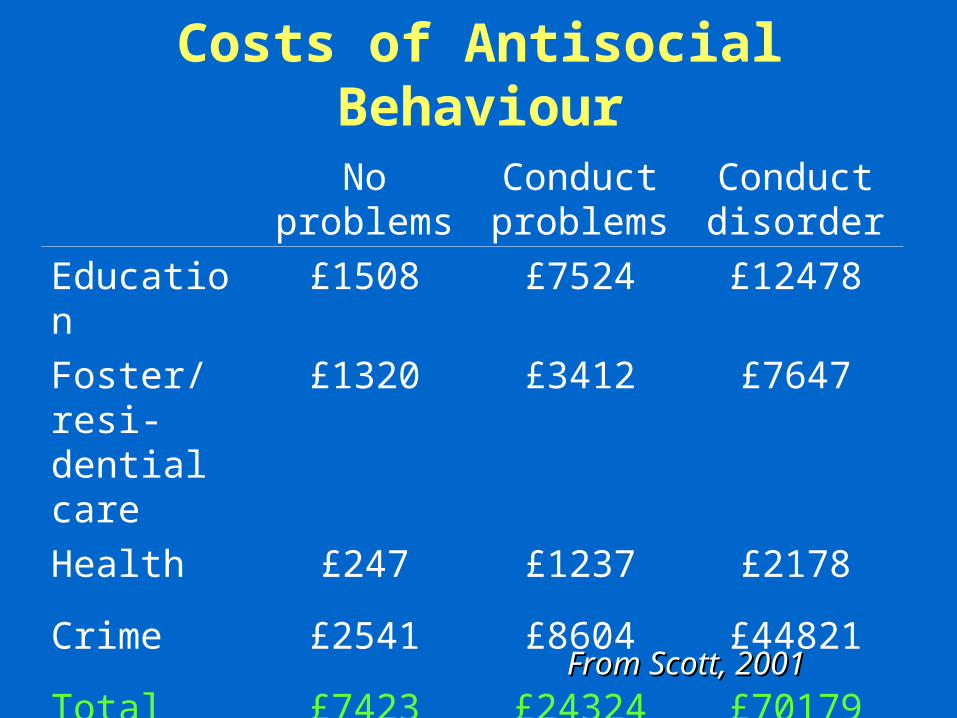
Costs of Antisocial Behaviour
No problems
Conduct problems
Conduct disorder
Education £1508 £7524 £12478
Foster/resi-dential care
£1320 £3412 £7647
Health £247 £1237 £2178
Crime £2541 £8604 £44821
Total £7423 £24324 £70179
From Scott, 2001From Scott, 2001
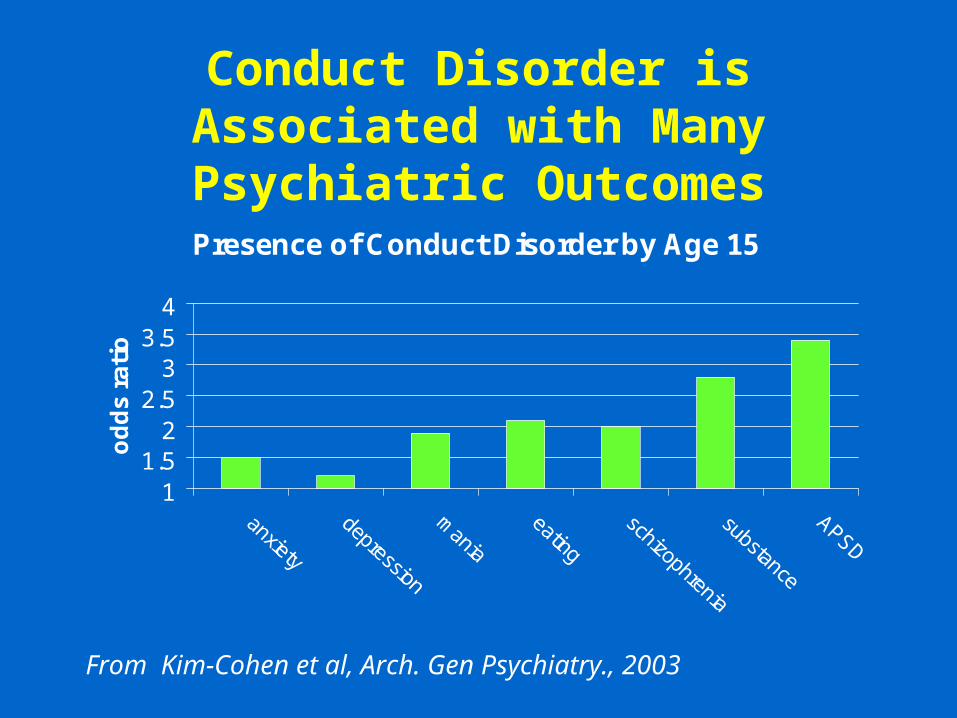
Conduct Disorder is Associated with Many Psychiatric Outcomes
Presence of Conduct Disorder by Age 15
11.5
22.5
33.5
4
anxiety
depression
mania
eating
schizophrenia
substance
APSD
od
ds
ra
tio
From Kim-Cohen et al, Arch. Gen Psychiatry., 2003
Treatment Effects
• Community parenting programs of preschoolers– non-significant effect favouring intervention
• Research/academic programs for preschool to primary school– 0.5-1.0 SD treatment effect
• Multisystemic therapy– 0.5 SD treatment effect
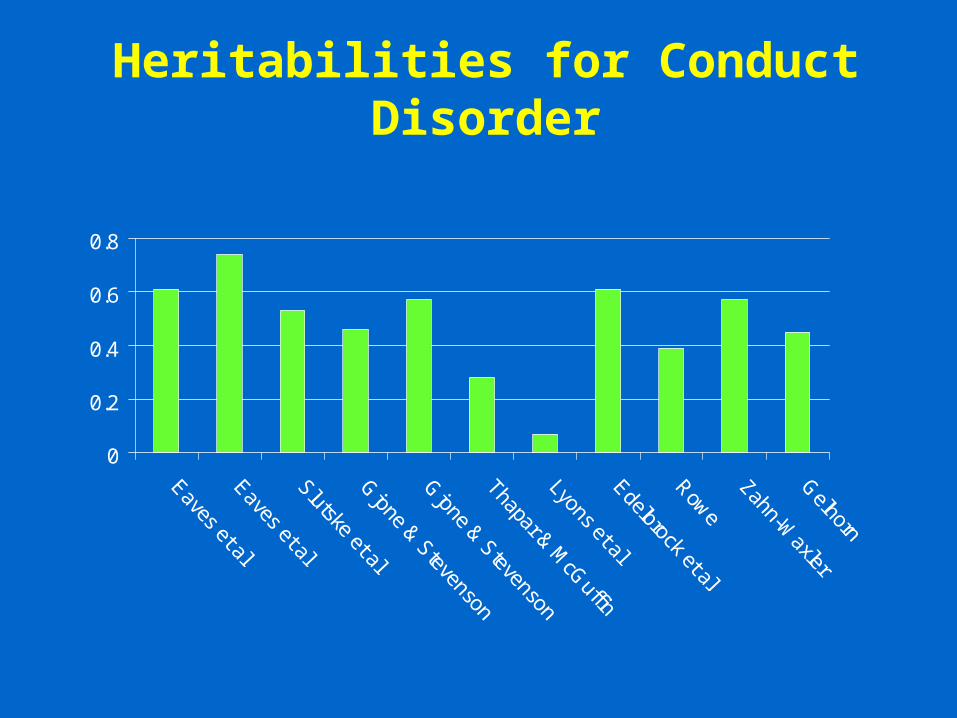
Heritabilities for Conduct Disorder
0
0.2
0.4
0.6
0.8
Eaves et alEaves et alSlutske et alGjone & Stevenson
Gjone & Stevenson
Thapar & McG
uffin
Lyons et alEdelbrock et al
Rowe
Zahn-Waxler
Gelhorn
What do we know about precursors of antisocial behaviour?
Cognitive
Family
School
Neighbourhood
Behavioural &Personality--Individual
Cognitive Risk Factors for Antisocial Behaviour
• Low IQ• Low verbal skills• Deficits in executive functioning, including
attentional problems• Poor academic attainments
– ? Cause or effect
Parental Risk Factors for Antisocial Behaviour
• Marital discord
• Paternal criminality
• Maternal depression
• Poor parental supervision
• Harsh and inconsistent discipline
Are family factors environmental or genetic?Are they causal or responsive?
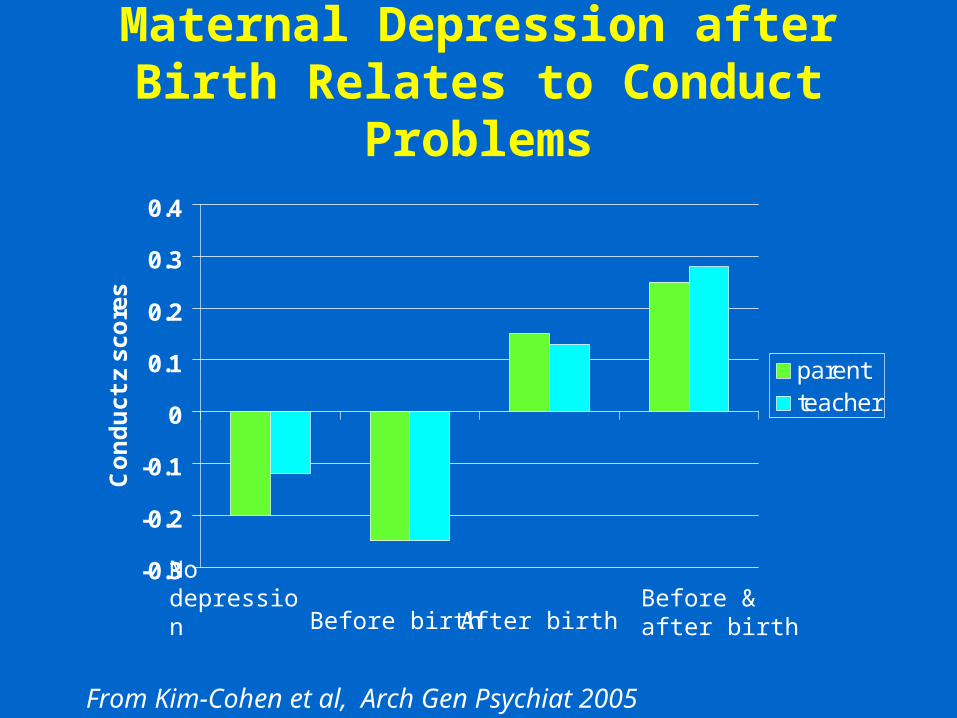
Maternal Depression after Birth Relates to Conduct Problems
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0.4
Co
nd
uc
t z
sc
ore
s
parentteacher
No depression Before birth After birth
Before & after birth
From Kim-Cohen et al, Arch Gen Psychiat 2005
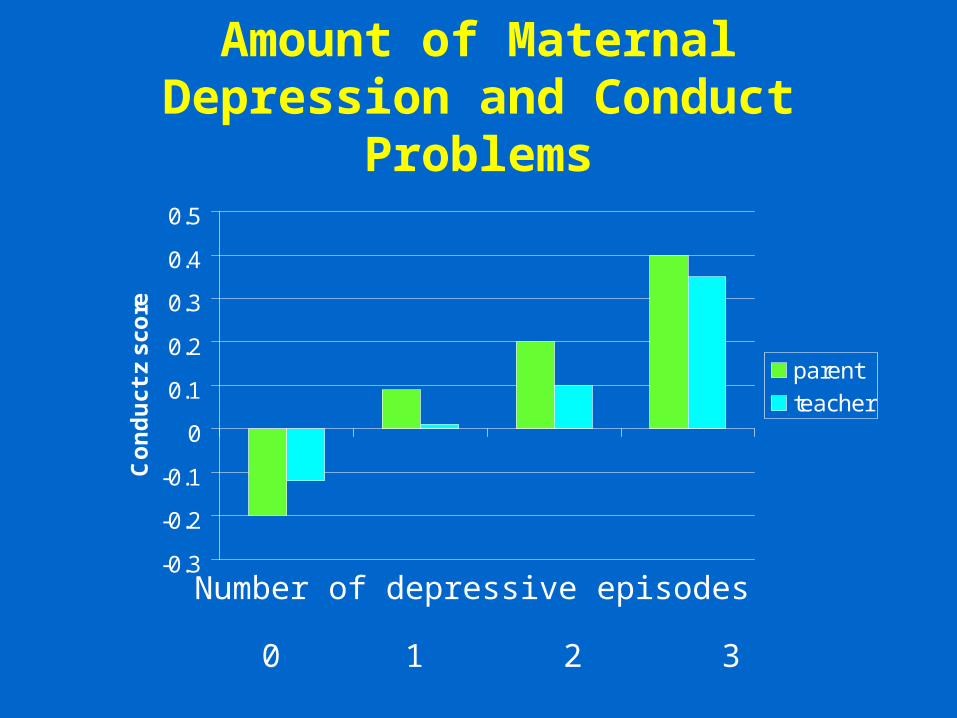
Amount of Maternal Depression and Conduct Problems
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0.4
0.5
Co
nd
uc
t z
sc
ore
parent
teacher
0 1 2 3
Number of depressive episodes
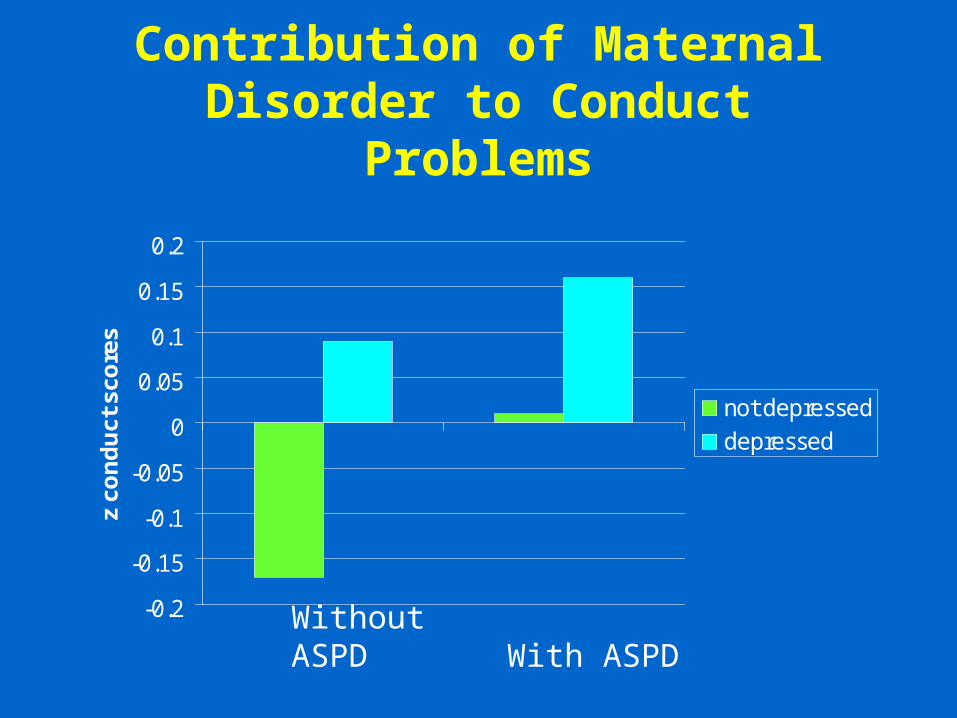
Contribution of Maternal Disorder to Conduct Problems
-0.2
-0.15
-0.1
-0.05
0
0.05
0.1
0.15
0.2
z co
nd
uct
sco
res
not depressed
depressed
Without ASPD With ASPD
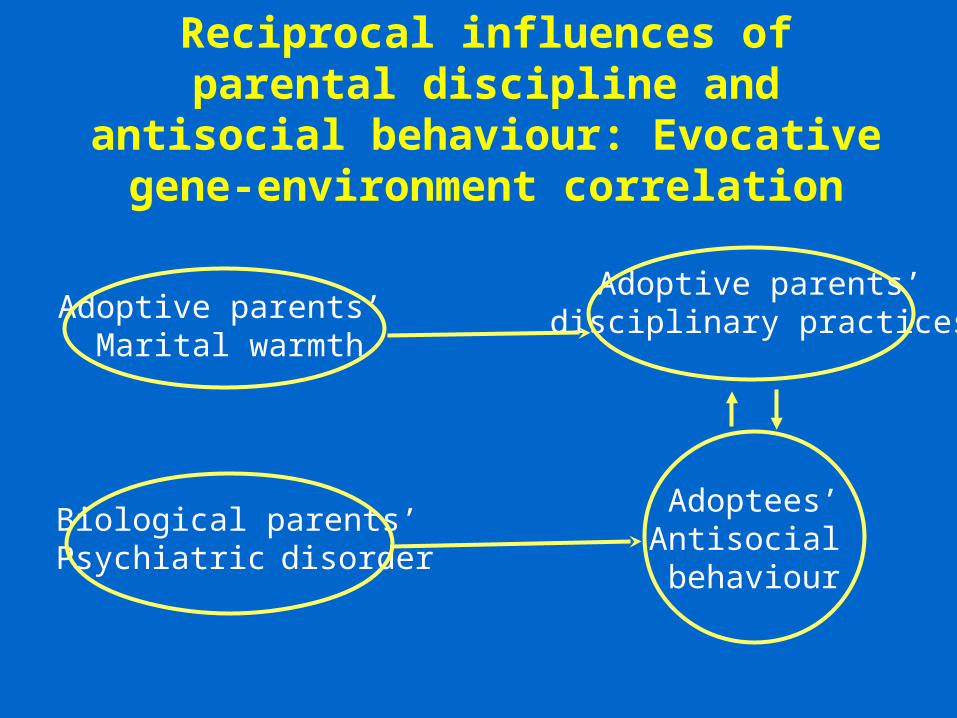
Reciprocal influences of parental discipline and antisocial behaviour:
Evocative gene-environment correlation
Adoptive parents’ Marital warmth
Adoptive parents’disciplinary practices
Biological parents’Psychiatric disorder
Adoptees’Antisocial behaviour
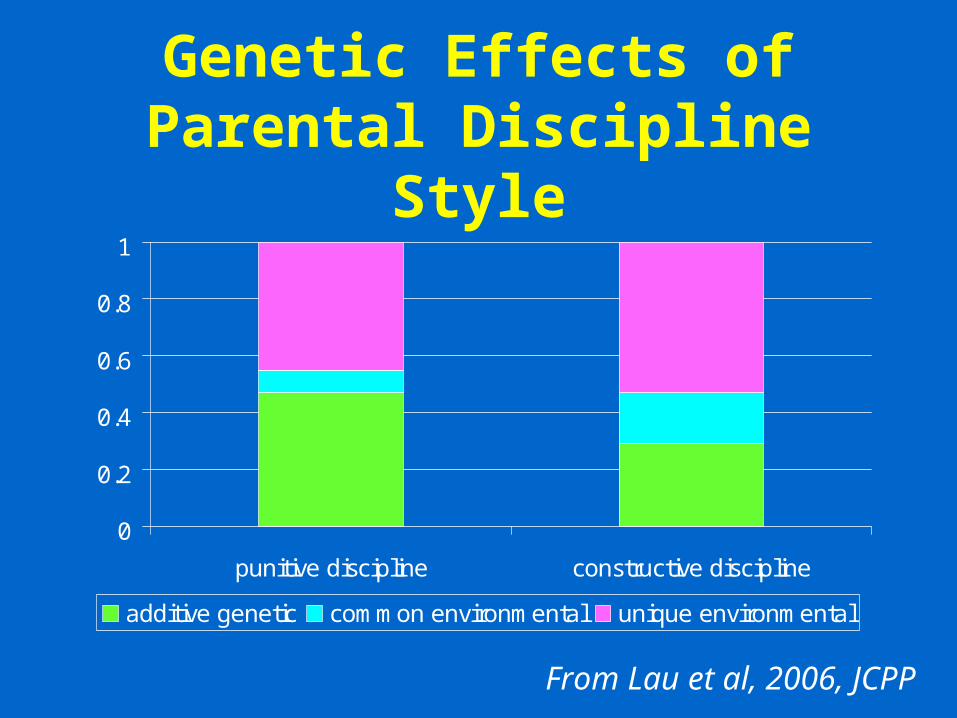
Genetic Effects of Parental Discipline Style
0
0.2
0.4
0.6
0.8
1
punitive discipline constructive discipline
additive genetic common environmental unique environmental
From Lau et al, 2006, JCPP
Monoamine Oxidate A
• X linked
• Genetic mutation lading to reduced MAO A activity associated with mild mental retardation and impulsive behaviour
• No evidence for direct role of MAO A in antisocial behaviour
Effect of Monoamine Oxidase A on Brain
Low MAO A activity associated with:• Reduced volume of amygdala, cingulate
gyrus insula and hypothalamus• Increased amygdala activation to
emotional arousal and emotional memory (latter in males only)
• Decreased anterior cingulate activation to inhibition in males only
From Meter-Linden berg et al (2006) PNAS
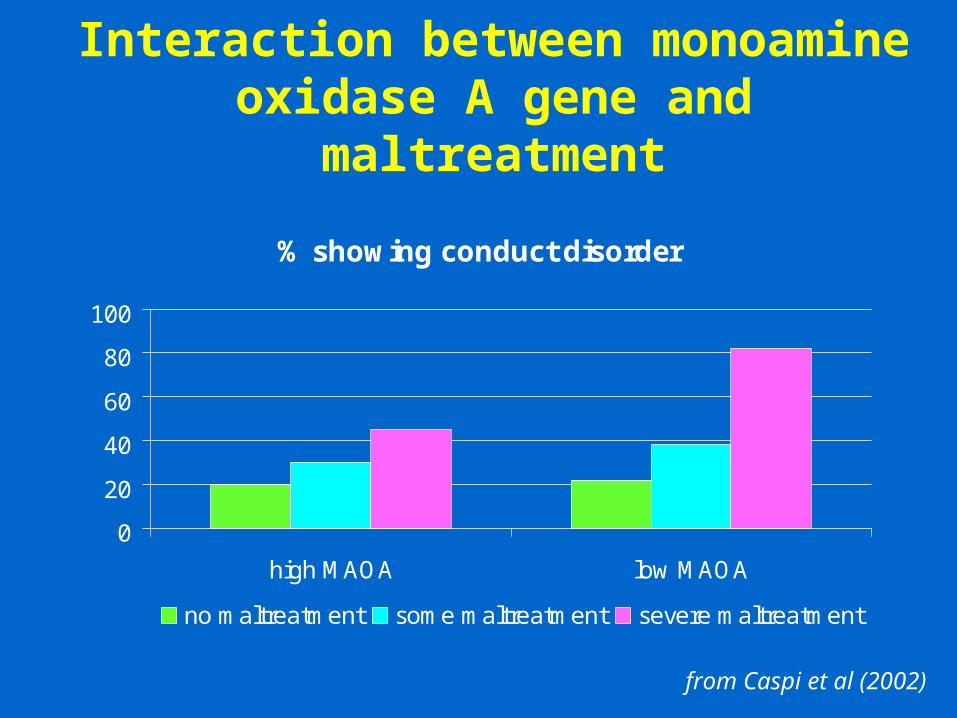
Interaction between monoamine oxidase A gene and maltreatment
from Caspi et al (2002)
% showing conduct disorder
0
20
40
60
80
100
high MAOA low MAOA
no maltreatment some maltreatment severe maltreatment
Social Risk Factors for Antisocial Behaviour
• Family poverty
• Minority ethnic status
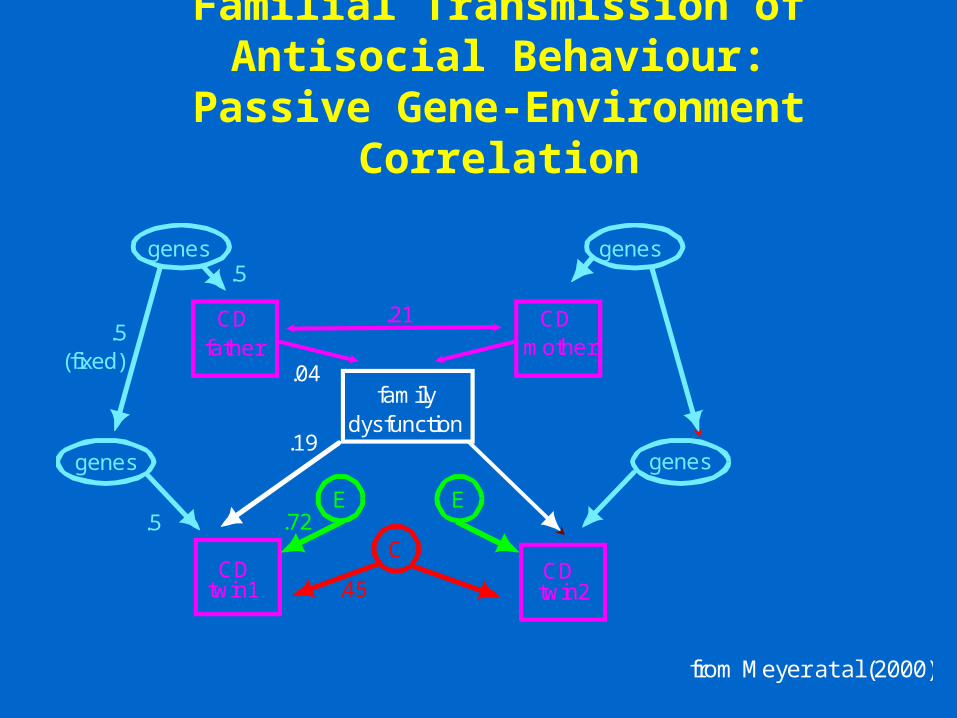
Familial Transmission of Antisocial Behaviour:
Passive Gene-Environment Correlation
genes genes
genesgenes
CDfather
CDmother
familydysfunction
CDtwin1
CDtwin2
E E
.5
.21
.04
.5(fixed)
.5
.19
C
.45
.72
from Meyer at al (2000)
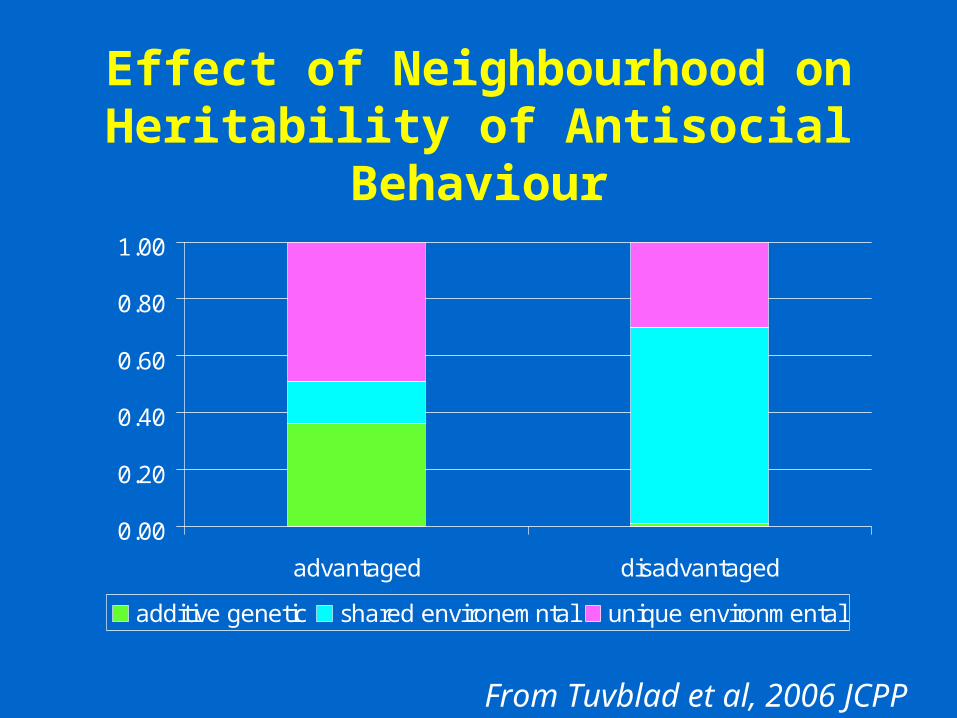
Effect of Neighbourhood on Heritability of Antisocial Behaviour
0.00
0.20
0.40
0.60
0.80
1.00
advantaged disadvantaged
additive genetic shared environemntal unique environmental
From Tuvblad et al, 2006 JCPP
Neighbourhood Influences on Antisocial Behaviour
• Urban environment• High crime neighbourhood• Neighbourhood with high drug availability• Neighbourhood social cohesion• Exposure to violence• Delinquent peer group
Access to antisocial activities may increase antisocial behaviour
School Effects on Conduct Problems
• School variation in delinquency, disruptiveness and absenteeism, having accounted for intake characteristics
• ‘better’ behaviour associated with school characteristics of:
• Clear leadership• Good classroom management• Academia emphasis• Consistent sanctions for misbehaviour
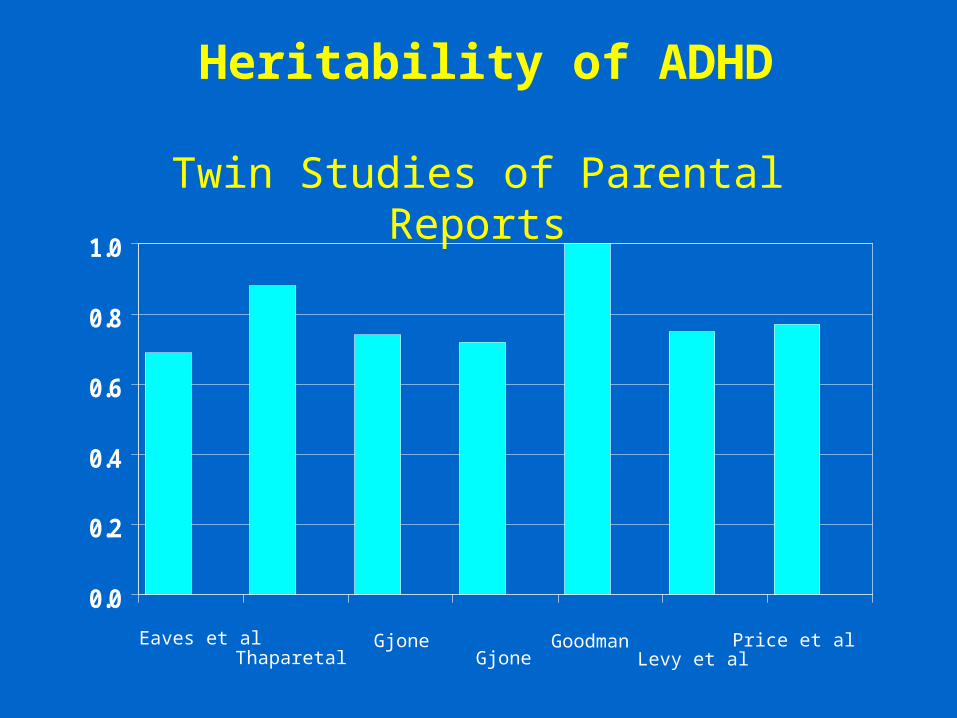
Heritability of ADHD
Twin Studies of Parental Reports
0.0
0.2
0.4
0.6
0.8
1.0
Eaves et alThaparetal
GjoneGjone
GoodmanLevy et al
Price et al
Shared genetic effects between ADHD and conduct disorder
ADHD Conduct disorder
Phenotypic correlation 0.3
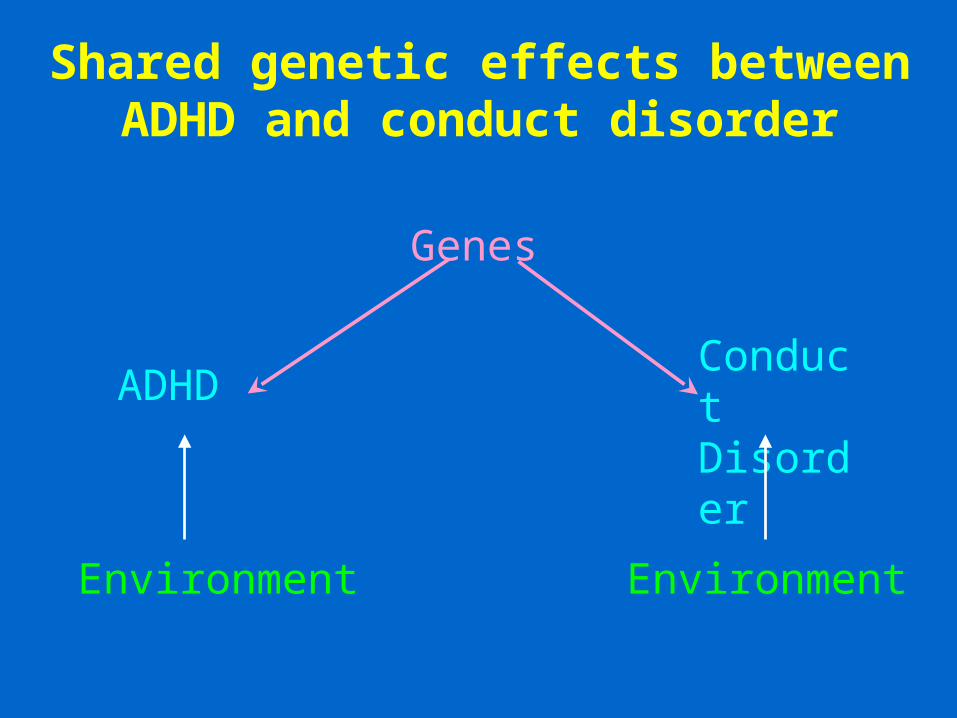
Shared genetic effects between ADHD and conduct disorder
Genes
ADHDConduct Disorder
Environment Environment
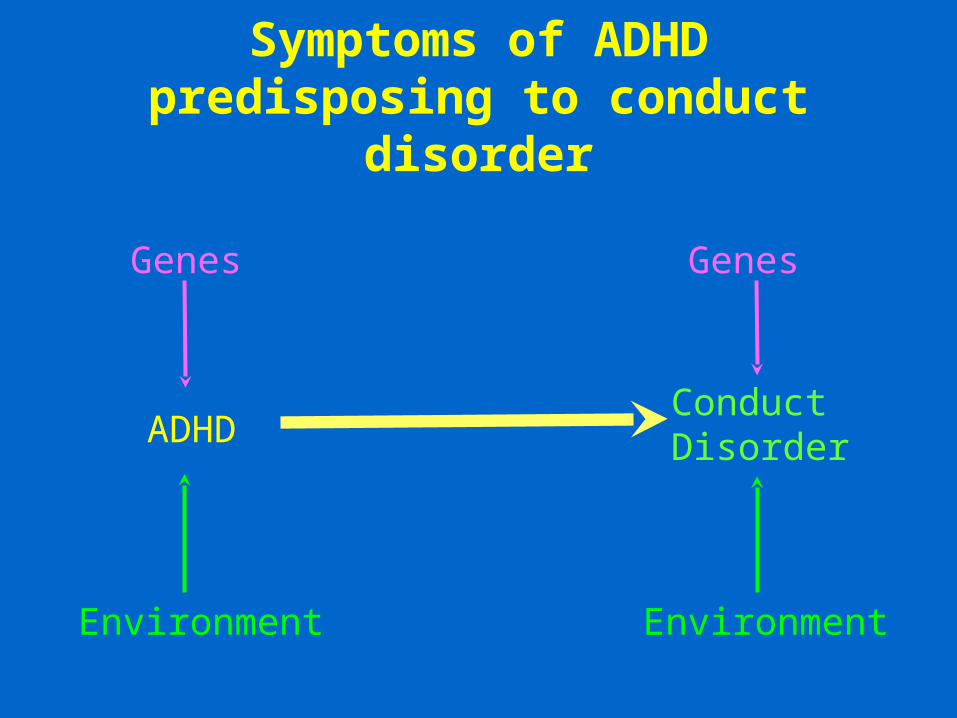
Symptoms of ADHD predisposing to conduct disorder
Genes
ADHD
Environment
Genes
Conduct Disorder
Environment
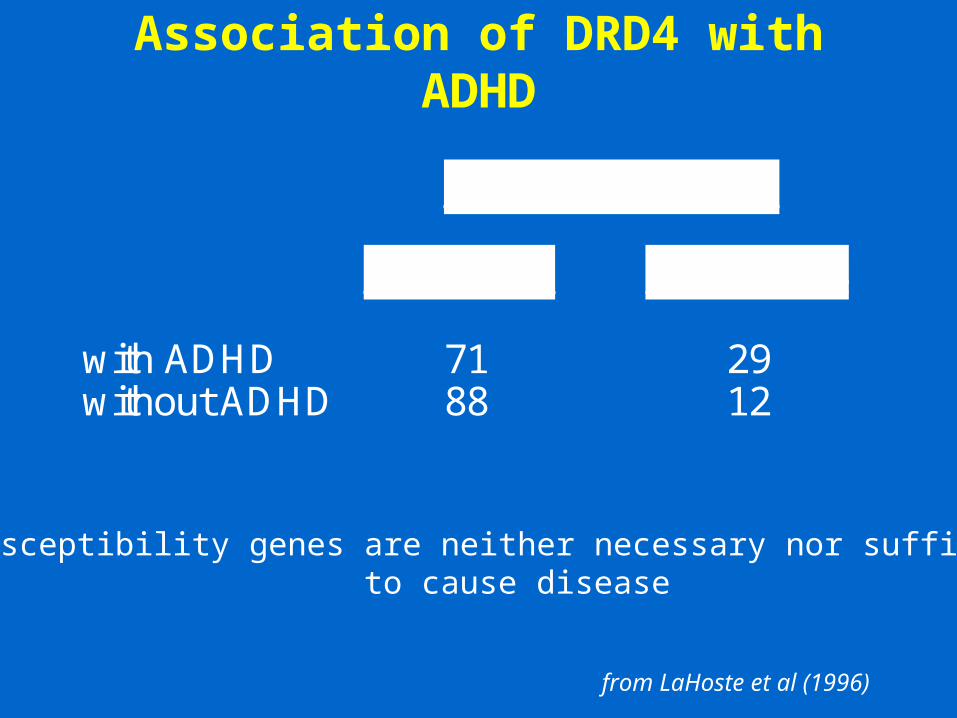
Association of DRD4 with ADHD
% allelic variation
<7 repeats 7-8 repeats
with ADHD 71 29without ADHD 88 12
Susceptibility genes are neither necessary nor sufficient to cause disease
from LaHoste et al (1996)
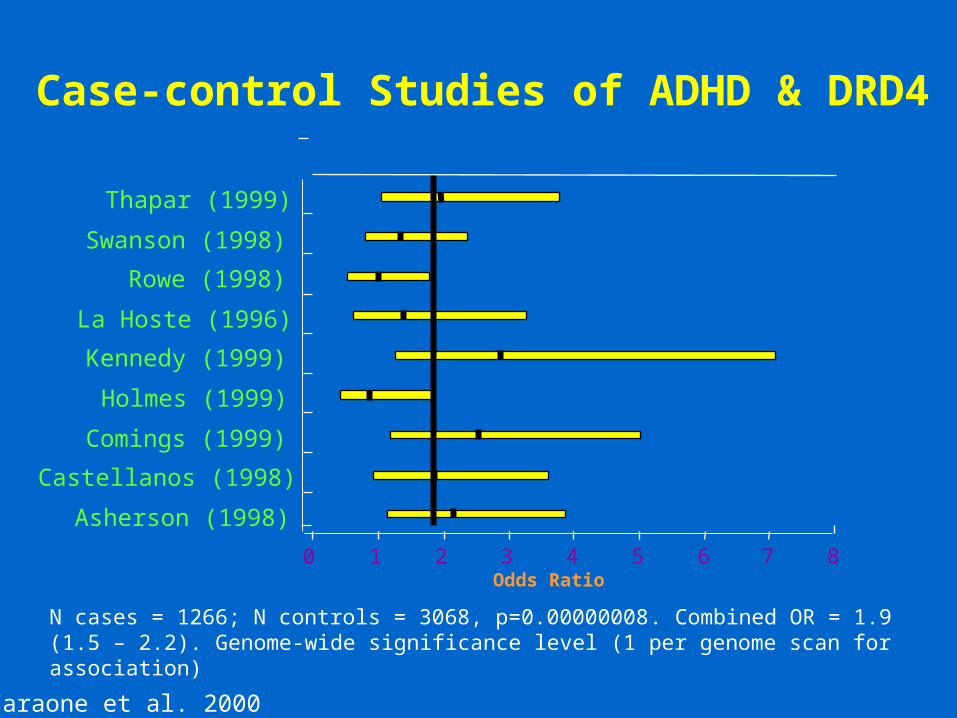
Asherson (1998)
Castellanos (1998)
Comings (1999)
Holmes (1999)
Kennedy (1999)
La Hoste (1996)
Rowe (1998)
Swanson (1998)
Thapar (1999)
0 1 2 3 4 5 6 7 8Odds Ratio
N cases = 1266; N controls = 3068, p=0.00000008. Combined OR = 1.9 (1.5 – 2.2). Genome-wide significance level (1 per genome scan for association)
Case-control Studies of ADHD & DRD4
Faraone et al. 2000
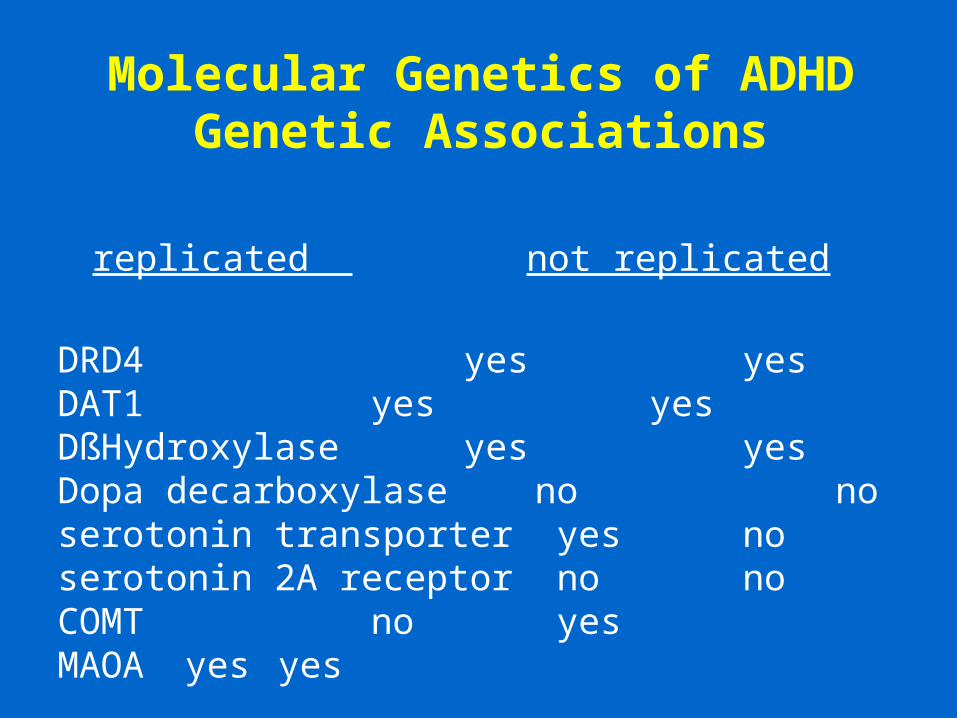
Molecular Genetics of ADHDGenetic Associations
replicated not replicated
DRD4 yes yesDAT1 yes yesDßHydroxylase yes yesDopa decarboxylase no noserotonin transporter yes noserotonin 2A receptor no noCOMT no yesMAOA yes yes
Implications for Early DetectionShould genetic tests be used to guide
us in determining who is at risk
• How sensitive and specific are genetic tests in determining who will have disorder?
• Will early detection alter the prognosis or treatment for disorder?
• Are genetic studies the most efficient in identifying at risk populations?
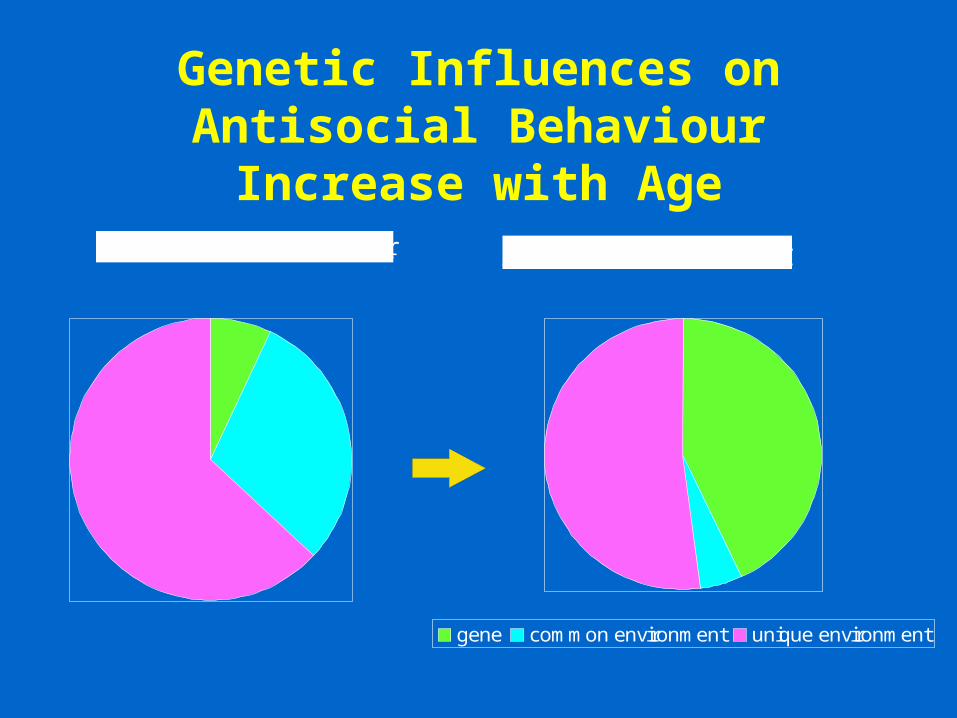
Genetic Influences on Antisocial Behaviour Increase with Age
Childhood conduct disorder Adult antisocial personality
gene common environment unique environment
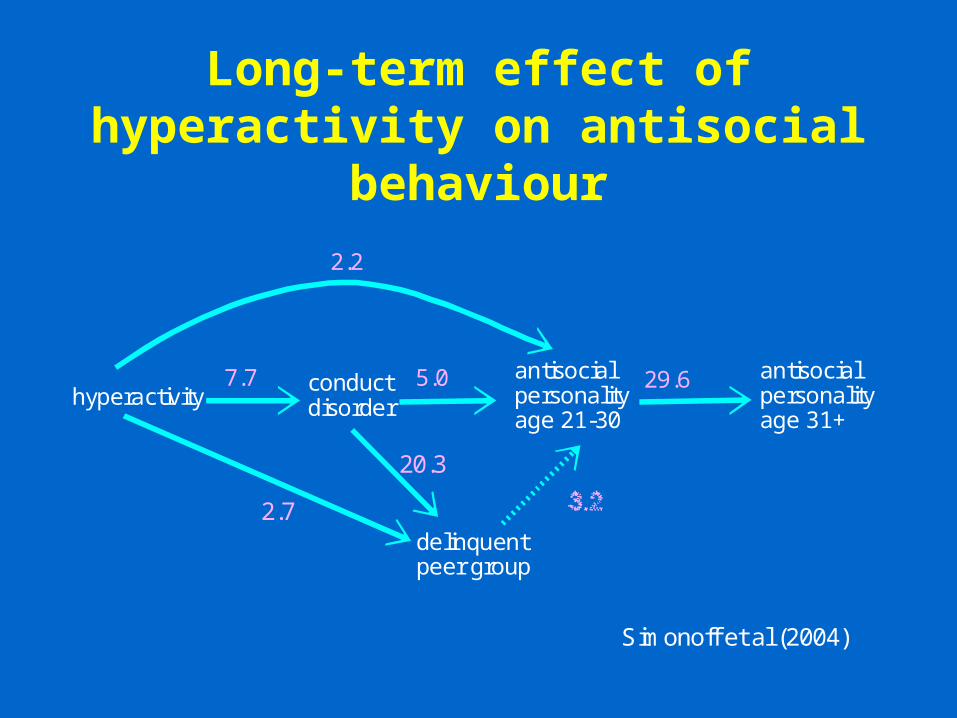
Long-term effect of hyperactivity on antisocial behaviour
hyperactivityconductdisorder
antisocialpersonalityage 21-30
antisocialpersonalityage 31+
7.7 5.0 29.6
2.2
delinquentpeer group
2.7
20.3
Simonoff et al (2004)
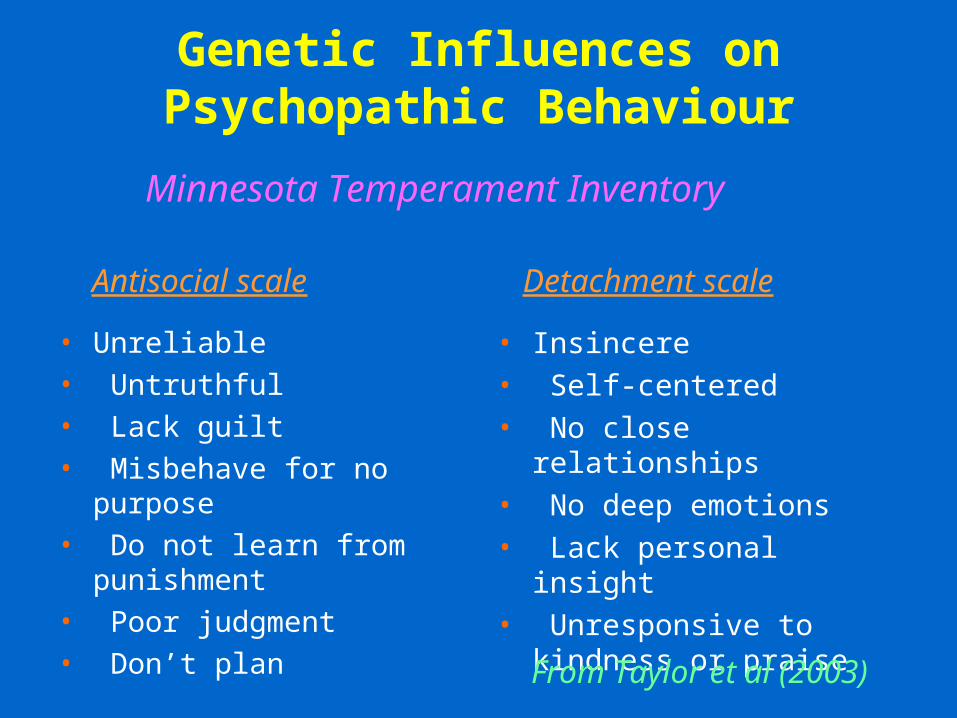
Genetic Influences on Psychopathic Behaviour
• Unreliable
• Untruthful
• Lack guilt
• Misbehave for no purpose
• Do not learn from punishment
• Poor judgment
• Don’t plan
• Insincere
• Self-centered
• No close relationships
• No deep emotions
• Lack personal insight
• Unresponsive to kindness or praise
Minnesota Temperament Inventory
From Taylor et al (2003)
Antisocial scale Detachment scale
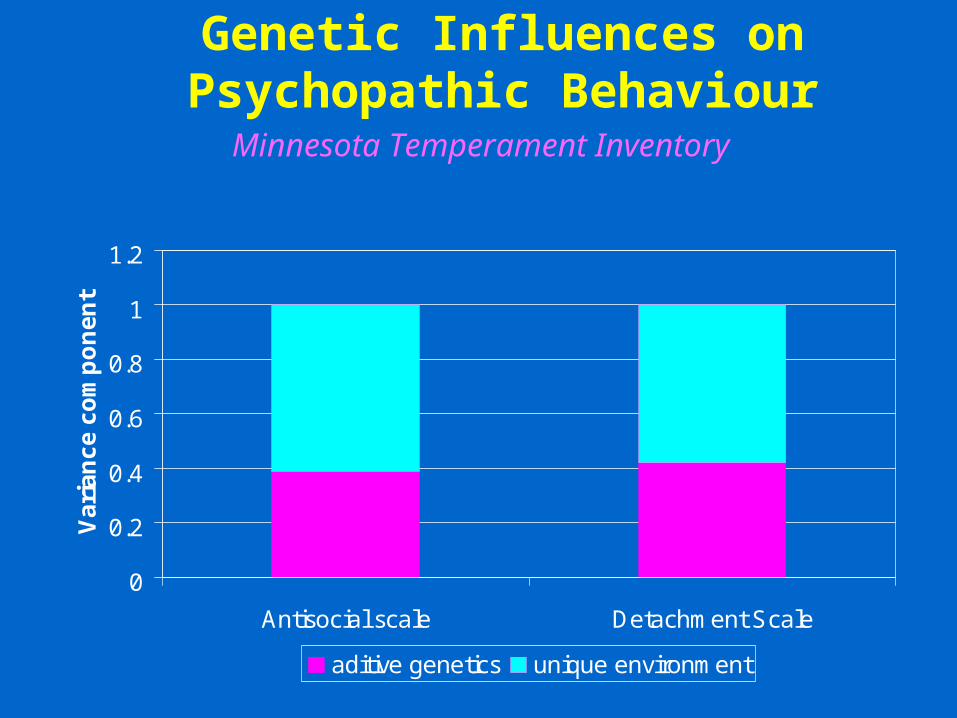
Genetic Influences on Psychopathic Behaviour
Minnesota Temperament Inventory
0
0.2
0.4
0.6
0.8
1
1.2
Antisocial scale Detachment Scale
Va
ria
nc
e c
om
po
ne
nt
aditive genetics unique environment
Callous/unemotional and antisocial behaviour in 7 year olds
• Does not show feelings or emotions
• helpful if someone is hurt, upset or feeling ill
• feels bad or guilt when done something wrong
• considerate of others’ feelings
• kind to younger children• concerned about how well
s/he is doing in school
• Often has temper tantrums or hot tempers
• generally obedient, usually does what adults request
• often lies or cheats• steals from home school
or elsewhere
Callous/unemotional Antisocial
Viding et al 2005

Childhood callous/unemotional traits and antisocial behaviour
0
0.2
0.4
0.6
0.8
1
caullous unemotionaltraits
antisocialbehaaviour/high C/U
antisocial behaviournl C?U
vari
an
ce c
om
po
ne
nt
genes common environment unique envionment
Viding et al, 2005
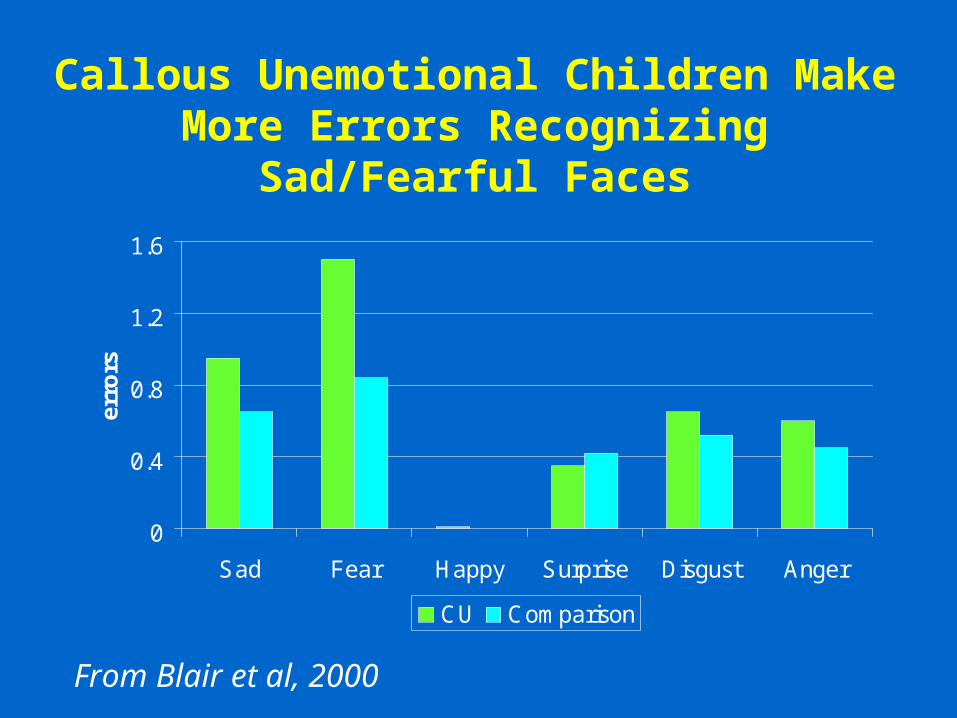
Callous Unemotional Children Make More Errors Recognizing Sad/Fearful Faces
0
0.4
0.8
1.2
1.6
Sad Fear Happy Surprise Disgust Anger
erro
rs
CU Comparison
From Blair et al, 2000
Cognitive Dysfunction in Psychopathy
• Failure to make stimulus-reinforcement associations particularly in relation to fearful or distressed stimuli
• Disruption in ability to alter stimulus-response associations
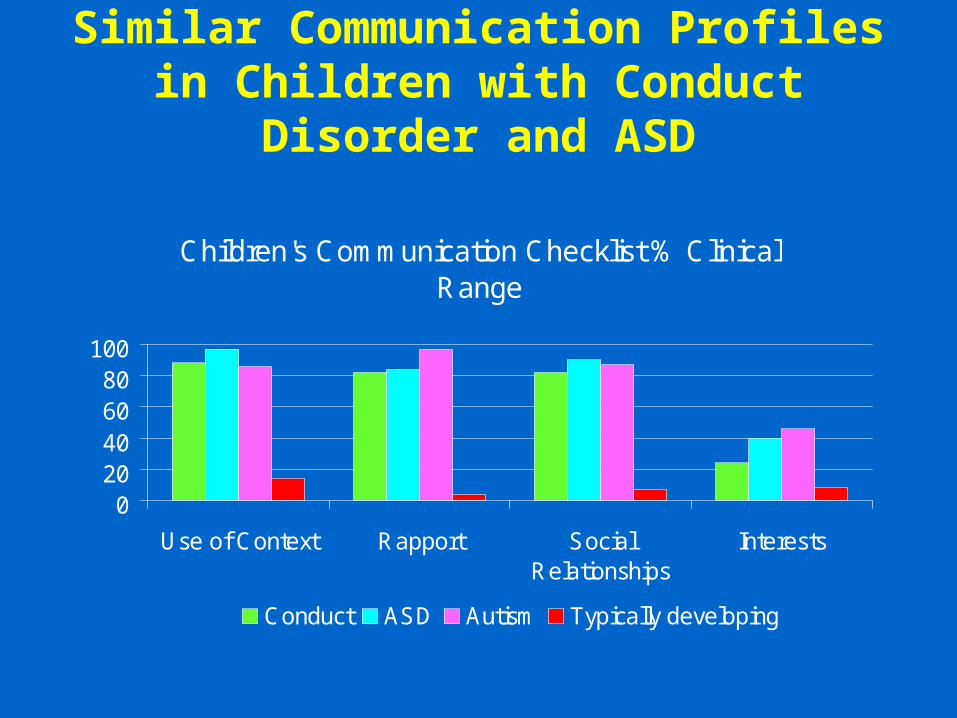
Similar Communication Profiles in Children with Conduct Disorder and ASD
Children's Communication Checklist % Clinical Range
020406080
100
Use of Context Rapport SocialRelationships
Interests
Conduct ASD Autism Typically developing
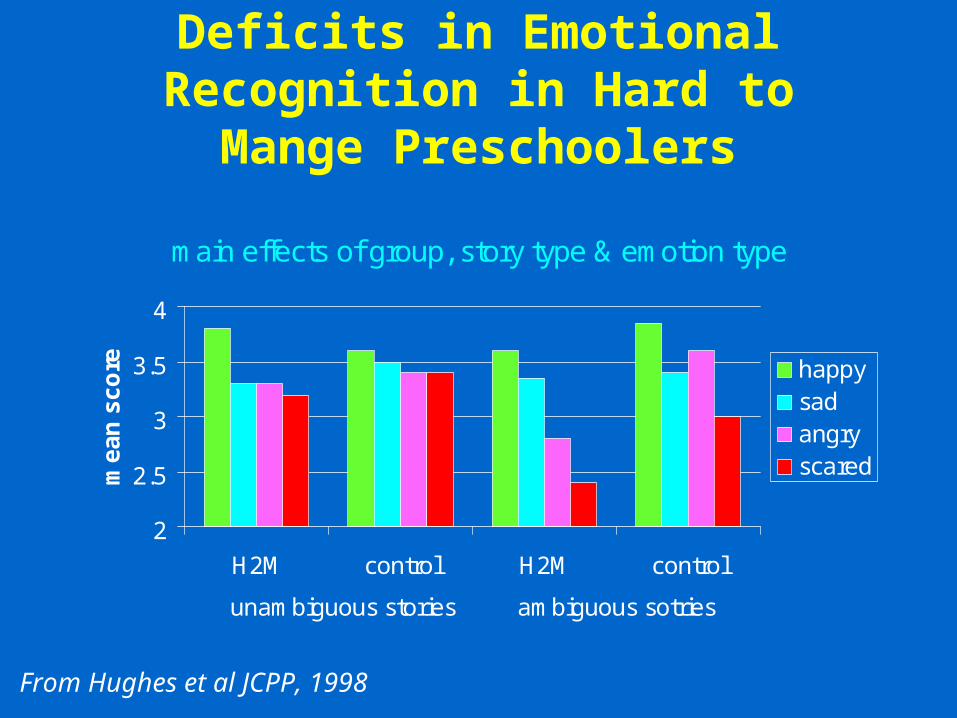
Deficits in Emotional Recognition in Hard to Mange Preschoolers
main effects of group, story type & emotion type
2
2.5
3
3.5
4
H2M control H2M control
unambiguous stories ambiguous sotries
me
an
sc
ore happy
sadangryscared
From Hughes et al JCPP, 1998
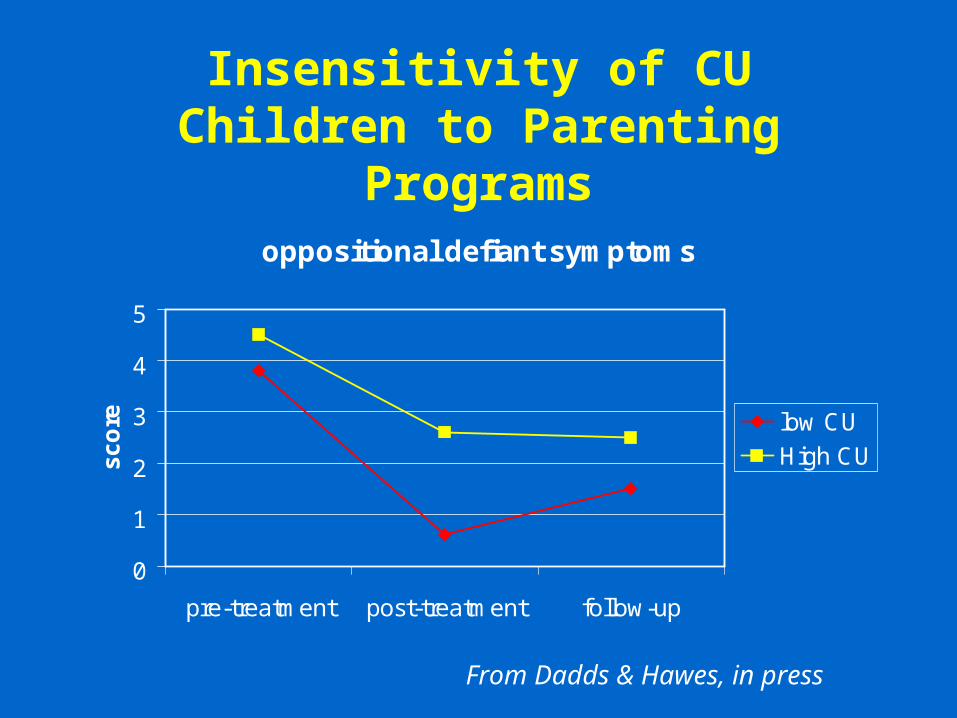
Insensitivity of CU Children to Parenting Programs
oppositional defiant symptoms
0
1
2
3
4
5
pre-treatment post-treatment follow-up
sc
ore low CU
High CU
From Dadds & Hawes, in press
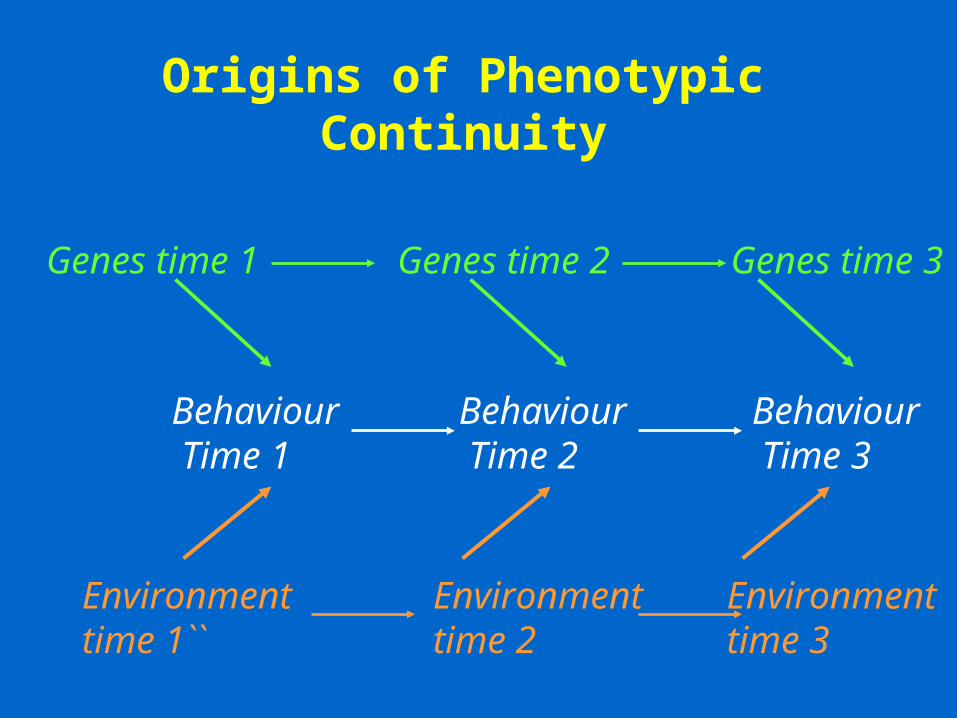
Origins of Phenotypic Continuity
Behaviour Time 1
Behaviour Time 2
Behaviour Time 3
Genes time 1 Genes time 2 Genes time 3
Environment time 1``
Environment time 2
Environment time 3
Implications for Research Directions
• Studies of antisocial behaviour need to begin early in life
• Risk factor research must start with adequate description of the child on a variety of dimensions
• Integration of measurement of risk factors from many perspectives is necessary