Embed Size (px)
Citation preview

\PERGAMON Neuropsychologia 26 "0888# 40Ð55
9917Ð2821:87:,*see front matter Þ 0887 Elsevier Science Ltd[ All rights reservedPII] S 9 9 1 7 Ð 2 8 2 1 " 8 7 # 9 9 9 5 5 Ð 8
Naturalistic action production following right hemisphere strokeMyrna F[ Schwartza\b�\ Laurel J[ Buxbauma\b\ Michael W[ Montgomerya\Eileen Fitzpatrick!DeSalmea\ Tessa Harta\ Mary Ferraroa\ Sonia S[ Leec\
H[ Branch Coslettb\a
aMoss Rehabilitation Research Institute\ 0199 West Tabor Road\ Philadelphia\ 08030!2988 PA\ USAbTemple University\ Philadelphia\ PA\ USA
cAmerican University\ Washington\ DC\ USA
Received 6 November 0886^ accepted 4 May 0887
Abstract
An unselected group of right hemisphere\ semi!acute stroke patients "n�29# was run on a laboratory test of naturalistic actionproduction and was found to commit errors of action at a higher rate than what was previously reported for recovering head injurypatients ðSchwartz et al[\ Naturalistic action impairment in closed head injury[ Neuropsychology\ 0886\ 7\ 48Ð61Ł[ There were strongsimilarities in how these two patient groups responded to variations in task demands and in the pattern of errors they produced[Hemispatial biases were evident in the errors of right hemisphere patients with neglect but not those without neglect^ and neglectpatients also many errors that were unrelated to the spatial layout[ We argue that a non!speci_c resource limitation * which mighttranslate as reduced arousal or e}ort * is central to the breakdown of naturalistic action production after brain damage\ and righthemisphere patients are especially vulnerable to this resource limitation and its behavioral consequences[ Þ 0887 Elsevier ScienceLtd[ All rights reserved[
Keywords] Right hemisphere stroke^ Naturalistic action^ Supervisory attention^ Neglect^ Resource capacity
0[ Introduction
As neuropsychologists become more involved in pati!ent rehabilitation\ there is growing interest in how neuro!logical disorders impact real world behavior and howbest to assess and ameliorate this impact[ Examples ofthis trend include the development of ecological assess!ments of memory\ attention\ and executive dysfunctionð24\ 49\ 40Ł^ empirical studies of real!life planning andproblem solving in frontal lobe patients ð2\ 32Ł^ and theapplication of neuropsychological theories to thevocational re!training of patients with amnesia ð00Ł[
In a related vein\ our group has sought to elucidate thebehavioral and brain mechanisms underlying everydayaction skills\ such as preparing a cup of co}ee\ by lookingat how such activities are a}ected by di}erent types ofneurological impairments[ We documented severe dis!ruption in case studies involving patients with mesialfrontal infarction ð30Ł\ closed head injury ð5\ 27\ 39Ł andfrontal dementia ð4Ł[ And we found a surprising absence
�Corresponding author[ Tel[] ¦0!104!3458594^ fax] ¦0!104!3458403^ e!mail] mschwarÝvm[temple[edu
of impairment in a semantic dementia patient whoseknowledge of objects was seriously compromised ð4Ł[
The point of departure for many of these studies wasthe NormanÐShallice theory of attention and action ð11Ł\as applied to frontal lobe syndromes ð31\ 32\ 34Ł[ Thetheory maintains that simple\ routine activities are self!organized through interactive networks of goal\ actionand object schemas ð7Ł[ For complex or non!routineactivities\ additional mechanisms come into play\ e[g[\ toinhibit routine schemas from _ring\ form temporary goal!action schema linkages\ and sustain the activation in thesetemporary linkages ð33Ł[ Collectively\ these mechanismscomprise the supervisory attention system[0 Damage toprefrontal cortex is said to compromise the functions ofthis system\ thereby causing the breakdown of complexpurposive action and the perseverative intrusions of inap!propriate routines that are characteristic of the frontaldysexecutive syndrome[
It has been argued that everyday action skills occupy
0 In early formulations of the theory\ the supervisory attention systemwas described as a unitary entity that performed multiple functions[More recent accounts describe it as componential\ and neurologicallyinstantiated in multiple separable networks ð33\ 35Ł[

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð5541
a middle ground between simple and complex\ routineand novel\ and that the supervisory system plays a greateror lesser role in their planning and execution\ dependingon circumstances and the cognitive status of the actorð25\ 26Ł[ This implies that supervisory system damagemight be causally implicated in the breakdown of every!day action in recovering head injury and other types ofcerebral damage[
In Schwartz et al[ ð28Ł\ we sought to test the supervisoryattention "SA# account of routine action breakdown inclosed head injury "CHI#\ along with two other accountsalso derived from frontal lobe theory "procedural^ work!ing memory#[ We generated predictions from these frontalaccounts regarding how patients at risk for routine actionbreakdown would respond to various manipulations oftask and context\ including the presence of distractorobjects\ the addition of a second task\ and the require!ment to search a drawer for needed items[ Among thepredictions we derived from the SA account was that therate of errors in CHI would exceed that of a neuro!logically intact control group only in the conditionsinvolving task compounding and drawer search[ In thesimpler conditions involving a single task\ with or withoutdistractors\ the demands on supervisory attention shouldbe minimal^ hence a de_cit restricted to supervisory atten!tion would be expected to have little impact[
The weakening of SA control predisposes to environ!mental intrusions[ If this is the cause of routine actiondisorders in CHI\ patients should be driven to distractoruse\ utilization behavior\ and other such errors of {{com!mission||[ Errors of omission\ whereby a critical step inthe task is left out\ should be less likely to occur[
The _ndings from the study did not support the predic!tions of the SA account\ nor of the other frontal accountswe considered[ The CHI group made more errors even onthe simplest condition\ and there was a strong associationbetween error score and clinical severity[ Patients andcontrols were distinguished primarily by omission errors^the proportional distribution of commission errors wasstrikingly similar in the two groups[ Adding complexityimpacted the rate of omissions but not commissionerrors^ and the correlation with clinical severity wasweaker for commission errors than omissions[
To account for the full range of _ndings\ including thecontinuity of e}ects between controls\ mild\ and severepatients\ we proposed an account based on limited!capacity resources[ According to this account\ the neuro!logically intact controls responded to the simple taskrequirements by allocating minimal resources\ whichmade them vulnerable to occasional errors\ such as reach!ing for a distractor object when the target was in view\or anticipating an upcoming step in the task ð1\ 10\ 16Ł[CHI patients\ we proposed\ were subject to an additionalrestriction in resource capacity\ which made them morevulnerable to errors[ As to why omission errors shouldbe especially sensitive to task di.culty and clinical sever!
ity\ we speculated that severe resource limitation mighttranslate into poverty of e}ort or\ more mechanistically\failure to resolve the competition for schema selectionsuch that none of the candidate action schemas reachesthreshold[
1[ Study 0
Diminished attentional resources and poverty of e}ortare well recognized consequences of right hemispherebrain damage "e[g[\ ð8\ 03\ 05\ 14\ 18Ł#[ If the resourceaccount of everyday action breakdown is correct\ righthemisphere patients would be expected to show heigh!tened vulnerability to errors of action[ This might also bepredicted on the basis of the right hemisphere|s spe!cialized role in sustaining attention ð12\ 38Ł\ since recentresearch has established a correlation between sustainedattention performance and reported frequency of every!day action slips ð21Ł[
To date\ the only relevant evidence concerns patientswith severe neglect who fail to act on objects in lefthemispace[ Consequently\ we sought to determinewhether an unselected group of patients recovering fromright hemisphere stroke would commit action errors inexcess of controls\ and whether the characteristics of theirperformance would show similarities to what we hadpreviously observed in the patients with CHI[
1[0[ Method
1[0[0[ SubjectsPatients were recruited from consecutive inpatient
admissions to the stroke service of MossRehab Hospital[Patients between the ages of 07 and 79 were consideredfor the study if they had sustained a single cer!ebrovascular accident con_ned to the right cerebral hemi!sphere[ Patients with a history of previous stroke\ headinjury\ or other neurologic disorders were excluded\ aswere those su}ering from major psychiatric disorders"i[e[\ major depression\ psychosis# at the time of study[Inclusion was also based on three behavioral criteria\tested informally by the patient|s clinical team] "0# Abilityto follow and understand task instructions^ "1# sen!sorimotor function adequate to perform the tasks^ "2#arousal and behavior control adequate for a 29minutetesting session[
The data to be reported are from 29 patients withRCVA\ all of whom were receiving in!patient rehabili!tation at the time of testing[ Twenty!six patients hadundergone acute CT or MRI studies that con_rmed alesion restricted to the right cerebral hemisphere "twowere not scanned^ two scans\ performed in the acute post!infarct state\ were negative#[ Fifteen patients had rightcortical damage that included frontal cortex^ 4 had right

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð55 42
Table 0Summary statistics
Characteristics Controls "n�07# RCVA patients "n�29#
M SD range M SD range
Age 51[8 8[4 27Ð66 48[0 02[0 14Ð65Years of education 02[7 1[2 09Ð07 00[1 1[6 5Ð05Days post onset − 44[2 095[5 8Ð494FIM − 65[0 06[1 35Ð000
The control group consisted of 4 males and 02 females[ The right CVA "RCVA# group consistedof 08 males and 00 females[ FIM�functional independence measure[
cortical damage that spared the frontal lobe^ and 5 hadright subcortical damage[1
The functional independence measure "FIM# ð01Ł wasused as a measure of clinical severity[ The FIM consists of07 items which measure disability in motor and cognitivefunctions on a 6!point scale[ The RCVA patients in thisstudy achieved a mean score of 65 out of a possible 015"range 35Ð000#\ which corresponds to an average ratingof 3 "minimal assistance required#[
Twenty!_ve patients were also given a neurologicalexam by our team|s behavioral neurologist "H[B[C[#[ Thisincluded administration of the NIH stroke scale ð3Ł\which measures 04 impairment symptoms on scales of 9Ð1\ 9Ð2\ or 9Ð3[ To take one particularly relevant example\scores for the neglect item are assessed by closely observ!ing the patient during the 19min examination for evi!dence of orienting asymmetry or inattention tocontralesional side of body or space[ Obvious mani!festation of asymmetry or inattention is scored a 1\ subtlemanifestation is scored a 0[ Among the 14 patients whowere assessed\ one earned a 1!score and 03 others earneda 0!score[ The remaining ten subjects had no neglect bythis clinical assessment[
Other symptoms assessed by the stroke scale includehemiparesis "present in 85) of assessed patients# andimpaired arousal "somnolence# "9)#[ We added someadditional items\ using the same scoring format\ to detectimpairments in short term memory "present in 53) ofpatients# as well as in ipsilesional sensori!motor func!tioning] _nger dexterity "25) of patients#\ pro!prioception "9)#\ motor initiation "9)# and limb praxis"04)#[
The control group was comprised of 07 non braininjured subjects drawn from the same geographic areaas the patients[ Patient and control groups are closelymatched in age but not gender distribution "Table 0#[However\ in our previous study we found that males andfemales erred at the same rate^ and that appears to betrue in this study\ as well "see below#[
1 For 12 patients\ copies of the neuroimaging studies were madeavailable to us and were read by the project neurologist "H[B[C[#[
1[0[1[ ProceduresThe multi!level action test "MLAT# is built on three
{{primary|| tasks*making a slice of toast with butter andjam^ wrapping a present^ and packing a lunchbox[ These{{primary|| tasks are performed under four conditions]"0# Solo!Basic\ in which all and only the materials neededare presented in the array^ "1# Solo!Distractors\ in whichfunctionally!related "and frequently\ visually similar# dis!tractor items are also presented "e[g[\ hot!dogs are thedistractor for lunch meat^ masking tape for scotch tape^hot plate for toaster^ spatula for knife^ see Table 1#^ "2#Dual!Basic\ in which the subject performs one primarytask\ and another speci_ed task\ in any order "e[g[\ wrap!ping a present and preparing a letter for mailing# and "3#Dual!Search\ in which some of the materials needed toperform the two tasks are in a closed drawer\ along withother irrelevant items[ All conditions are untimed[
Table 1 shows the design of the MLAT study[ Thereare three forms of the test\ each representing a uniquepairing of task and condition[ To minimize testing timeand practice e}ects\ each subject performed only oneform[ Form assignment was done through a minimizationmethod ð13Ł\ which assigned each new subject to the formwith the smallest sum of marginal totals matching thatsubject|s clinical characteristics "e[g[\ FIM score^anteriorÐposterior extent of lesion# and demographicpro_le "see Table 2#[ The order in which the four con!ditions were performed was partially counterbalancedaccording to a Latin Square design[
Subjects perform the MLAT while seated at a {{U||shaped table\ upon which all task materials are placedwithin reach[ The location of items is standardized foreach form and condition[ The items needed to completea given task or subtask are distributed rather than clus!tered\ with equal representation of key objects on theleft and right of midline[ For example\ in the present!wrapping task\ the gift box\ tape\ and gift are on the left^the wrapping paper\ scissors\ and bow are on the right[For the Dual!Search condition\ the drawer is attached tothe table just to the right of midline[
At the start of each condition\ the subject is read a setof instructions "e[g[\ {{prepare a slice of toast with butter

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð5543
Table 1Multi!level action test "MLAT# study design
MLAT condition Form A Form B Form C
Solo!Basic present toast lunchboxSolo!Distractors lunchboxa presentb toastc
Dual!Basic toast¦co}ee lunchbox¦schoolbag present¦letterDual!Search present¦letter toast¦co}ee lunchbox¦schoolbag
aDistractors are applesauce\ paper towel roll\ spatula\ hot dogs\ glass\ school bag[bDistractors are electric tape\ stapler\ snippers\ paper bag[cDistractors are hot plate\ nail _le\ vegetable shortening\ mustard[
Table 2Demographic and clinical factors balanced across forms
Characteristics Form A Form B Form C
M SD M SD M SD
ControlsAge 44[2 09[9 54[4 7[3 56[7 4[0Years of education 03[6 1[3 02[1 1[6 02[6 0[7RCVA patientsAge 46[3 05[0 48[0 02[1 50[9 8[5Years of education 00[1 2[1 09[6 1[9 00[7 1[8FIM 63[9 05[9 72[1 05[8 57[6 07[2
In forms A\ B\ and C\ there were 5 control subjects each and 00\ 09\ and 8 right CVA "RCVA#patients\ respectively[
FIM�functional independence measure[
and jam||# and is shown a corresponding picture[ Theinstructions include other pertinent information as well"e[g[\ for Solo!Distractors] {{Use just what you need||^ forDual!Search] {{Some of the materials you need may be inthis drawer||#[ Subjects are required to repeat the instruc!tions before beginning[ This sometimes necessitates asecond or third reading of the instructions[
The examiner|s interactions with the patients are pre!scribed and limited[ Giving physical assistance in casesof hemiparesis is allowed\ but only to help complete a stepwhich the patient has initiated[ Requests for informationduring the task are given a uniform response] {{Every!thing you need is out there "or in the drawer#[ Just dothe best you can||[ When the request for informationconcerns objects in neglected hemispace\ the examineradds\ {{Be sure to look all around||[
To avoid penalizing subjects for failing to remembertask instructions\ we use a prompting procedure] Sixtyseconds of inaction or o}!task behavior trigger a rep!etition of the instructions[ After the fourth such instruc!tional prompt\ that condition is terminated and the nextcondition is begun[ Otherwise\ a condition ends when thesubject indicates that s:he is _nished[
Subjects performed the MLAT in a single\ hour!longsession[ Conditions were separated by a short break[
1[0[2[ ScoringPerformance was simultaneously videotaped from
head!on and overhead cameras\ and the videotapes wereused for scoring[ Each condition was scored for errors\and an error score was computed which expressed thesum of errors on the entire form[
Table 3 shows the taxonomy used to code errors[ Thefour error types of greatest theoretical interest are objectsubstitution\ sequence\ omission\ and action addition[Object substitutions are coded whenever the subject per!forms an action which is appropriate to the task\ butinvolves a distractor or another semantically or func!tionally related object[ Sequence is a composite categorywhich comprises several error types] performing a laterstep in advance of an earlier step "so!called antici!pation:omission errors#^ transposing two ordered steps"reversal# and unnecessarily repeating a step or subtask"perseveration#[ We reserve the omission code for {{pure||omissions!those not conditioned by another error[ Anaction impacted by an object substitution is not coded asan omission^ neither is the deleted action in an antici!pation:omission error "e[g[\ closing the thermos without_lling it#[ "Examples of omissions\ and other error types\are shown in Table 3#[ The action addition code denotesany action that is not clearly in the service of the task^

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð55 44
Table 3Summary of MLAT error taxonomy—––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––Omission
e[g[\ fail to use stamp on letter^ fail to use cream in co}ee[Sequence
= Anticipation:omission] seal thermos before _lling^ close lunchbox before packed[= Reversal] stir mug of water\ then add grinds[= Perseveration] make two sandwiches[
Object substitutione[g[\ stir co}ee with fork "instead of spoon#^ place bread on hot!plate "instead of toaster#[
Action additionAction not interpretable as step in task^ includes {{utilization behavior|| and anomalous actions^ e[g[\ cut gift box^ pack extraneous items into
schoolbag[Gesture substitution
Correct object used with incorrect gesture^ e[g[\ spoon "rather than pour# cream into cup[Grasp:spatial misorientation
Misorientation of the object relative to the hand or to another "reference# object^ e[g[\ grasp wrong end of scissors "misoriented relative to hand#^place stamp on envelope sideways "misoriented relative to reference object#[Spatial misestimation
Spatial relationship between two or more objects incorrect^ act otherwise well!executed^ e[g[\ cut paper much too small for gift[Tool omission
e[g[\ spread jelly with _nger "instead of knife#[Quality
Inappropriate or inexact quantity "spatial or volume#^ e[g[\ _ll thermos with juice to point of over~ow[
this includes utilization acts ð34Ł and other behaviorsgenerally attributed to distractibility or disinhibition[
To minimize mistakes and maintain an acceptable levelof inter!rater reliability\ we developed detailed scoringsheets which enumerate\ for each condition of each form\an exhaustive listing of error descriptions and theirassociated codes[ Scorers simply enter a check mark nextto the appropriate error description\ or\ if the observederror is not listed\ write it in[ Using this system to inde!pendently score the MLAT videotapes of 03 CHI pati!ents\ pairs of trained coders agreed on a mean of 65) ofrecorded errors "SD 00# ð28Ł[
2[ Results
2[0[ Error scores
2[0[0[ Control subjectsThe 07 control subjects committed a total of 18 errors
"Mn[ 0[5\ range 9Ð3#[2 There was no correlation betweenerror score and age "p�9[41# or education "p�9[72#\ andmales and females did not di}er "MannÐWhitney test\p×9[39#[
2[0[1[ RCVAThe RCVA group committed 514 errors "Mn[ 19[7\
SD 03[8^ range 9Ð42#[ Error scores correlated with age
2 The normative standard used to identify errors was based on pilotstudies[ In the current study "see also ð28Ł#\ any act of omission orcommission that deviated from that normative standard was coded asan error\ whether occurring in controls or patients[
"r�9[33^ p�9[90# but not with education "r�9[98^p×9[59# or time elapsed since stroke "r�9[06\ p×9[29#[Males and females did not di}er "MannÐWhitney test\p×9[79#[ Error score also correlated with clinical sever!ity\ as measured by both the FIM "r�−9[54^ p³9[990#and the "expanded# stroke scale "r�9[35^ p³9[94#[ Table4 shows the demographic and clinical data for individualpatients\ along with information on lesion localization[Patients with higher error scores tend to have lesions thatinclude the frontal lobes\ but in a multiple regressionanalysis that contained FIM\ presence:absence of frontalinvolvement did not contribute signi_cantly to the pre!diction of error score "p for the model ³9[90^ p for yes:nofrontal ×9[2#[3
2[0[2[ Effect of conditionsThe e}ect of the conditions manipulation was exam!
ined in a repeated measures ANOVA which had con!dition "Solo!Basic^ Solo!Distractors^ Dual!Basic^ Dual!Search# as the within subjects factor and group "RCVA^controls# and form "A\ B\ C# the between factors[ Inthis\ and all other parametric tests to be reported\ thedependent measure\ number of errors\ was transformedby square root to normalize variance[ E}ects are sig!ni_cant at p³9[94 or\ in the case of post!hoc t!tests\ atthe level required by Bonferroni correction[
Main e}ects were signi_cant only for group "F"0\31#�34[1#[ Means for RCVA exceeded controls on allfour conditions "t×3[4 for all paired comparisons# "see
3 This is also what Schwartz et al[ found in their CHI study ð28Ł[

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð5545
Table 4
Subject ID( Form Gender Age Educ[ FIM MLAT Lesion Location"s#a Source oferrors lesion data
11 C M 37 05 35 42 DLF\ IP\ SP chart5 C M 62 01 79 35 AT\ PT\ IP\ WM\ CS scan
00 A M 52 01 38 31 DLPF\ IP\ AT\ PT scan3 C F 69 09 63 39 DLPF\ DLF\ IP\ AT\ PT scan6 C M 48 7 42 27 DLPF\ DLF\ AT\ WM scan
15 C F 55 8 58 27 DLF\ IP\ AT\ PT\ WM scan0 A M 63 NA 65 23 CS scan
09 A F 61 5 52 23 IP\ AT\ PT\ WM scan12 C M 58 05 36 20 DLF\ IP\ SP scan08 A M 63 8 52 18 DLF\ IP\ SP\ PT scan14 B F 63 01 68 17 IP\ SP\ DLF\ AT\ BG scan07 A M 51 09 62 13 thalamus scan4 B F 53 01 53 19 BG chart7 A F 32 05 62 19 OF\ LF\ MF\ SP\ BG scan8 A M 59 01 60 07 DLPF\ DLF\ IP\ AT\ PT scan
05 B M 35 01 86 07 Normalb scan19 C F 43 09 78 07 DLPF\ DLF scan29 A M 69 01 098 03 BG scan1 B M 54 00 77 02 DLF scan
06 B M 51 01 48 02 OF\ MF\ IP scan17 A F 31 05 64 02 IP\ SP scan13 B M 65 5 65 01 Normalb CT report2 B M 39 00 60 7 BG scan
01 B M 47 00 093 5 MCA\ ACA CT report16 B M 28 NA 72 5 IC\ insula scan02 C F 52 01 81 1 − not scannedb
03 C M 36 02 NA 1 SP\ IP CT report04 B M 56 8 000 1 PT scan10 A F 36 7 77 1 − not scannedb
18 A F 14 00 NA 0 DLPF\ DLF\ IP\ SP\ AT\ PT scan
aDLPF�dorsolateral prefrontal\ DLF�dorsolateral frontal\ OF�orbital frontal\ MF�mesial frontal\ IP�inferior parietal\ SP�superiorparietal\ AT�anterior temporal\ PT�posterior temporal\ IC�internal capsule\ CS�centrum semiovale\ WM�white matter\ BG�basal ganglia\MCA�middle cerebral artery\ ACA�anterior cerebral artery[
bclinical presentation consistent with RCVA[
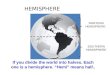
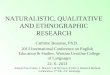
Fig[ 0\ which shows the untransformed means#[ Therewas also a signi_cant group×condition interaction "F"2\015#�2[2#[ Planned contrasts were carried out on thesolo conditions "0 vs 1#\ the dual conditions "2 vs 3# andthe solo vs dual conditions "0 and 1 vs 2 and 3#[ Results\shown in Table 5\ reveal that the group×condition inter!action was present in two of the three contrasts[ Relativeto controls\ the RCVA group was adversely a}ected byhaving to perform two tasks compared to one "contrast(2 in Table 5#\ as well as by having to perform two taskswith drawer search\ compared to without it "contrast(1#[
The contrast involving Solo!Basic and Solo!Dis!tractors "(0 in Table 5# yielded non signi_cant maine}ect and group×condition interaction[ Thus\ based onthis analysis\ there is no evidence that subjects| behaviorwas a}ected by the addition of distractors to the solotask "but see below#[
Returning to the main analysis\ we found that whileform did not emerge as a main e}ect\ it did qualify the
expression of the group×condition interaction justreported^ that is\ the three way interaction including formwas statistically reliable "F"5\015#�1[6#[ Close inspectionof the data revealed that this was due to the fact that thetoast!making task "{{make a slice of toast with butter andjam||# proved especially easy^ in each form\ the con!dition"s# involving toast making\ whether solo or dual\yielded fewer errors than expected for that condition[
2[0[3[ Comparison with CHI patientsHaving shown that a tendency to commit errors is a
feature of right hemisphere damage\ we next sought todetermine whether this manifests in ways similar to whatwas previously reported for CHI[ The previous studyð28Ł utilized test and scoring procedures identical to thecurrent procedures[ The 29 CHI subjects were selectedfrom an inpatient rehabilitation service using the sameminimal criteria[ Compared to the RCVA patients "Table0#\ the CHI patients were younger "Mn[ age 20[2#\ dis!proportionately male "n�10#\ and clinically less severe

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð55 46
Fig[ 0[ Mean number of errors "with standard error bars# for the RCVA group "n�29# and control group "n�07# on each of the four conditions ofthe MLAT\ collapsed across forms[
Table 5Results of planned contrasts
Contrast E}ect F p
Conditions 0 vs 1 main ³0[9 ×9[49interaction ³0[9 ×9[49
Conditions 2 vs 3 main 4[9 ³9[94interaction 3[3 ³9[94
0¦1 vs 2¦3 main 17[1 ³9[990interaction 4[2 ³9[94
Main�main e}ect of condition^ interaction�condition×group[
"Mn[ FIM�78[8^ t"45#�2[0#[ Only one of the CHI hadneglect as assessed by NIH stroke scale[ On the MLAT\CHI patients made signi_cantly fewer errors than RCVA"Mn[ 09[9^ SD 00[6\ compared with Mn[ 19[7\ SD 03[8for RCVA^ t"45#�2[03#[
As clinical severity correlates strongly with error rate\this group di}erence in error rate could conceivablyreduce to the greater severity of the RCVA group[ To seeif this is so\ and to see whether the two patient groupsresponded similarly to the conditions manipulation\ wecarried out a repeated measures analysis of covarianceon transformed error scores\ using FIM score as thecovariate[ As before\ the within subjects factor was con!dition\ and the between factors were form and group"RCVA\ CHI#[
As expected\ the e}ect of FIM on error rate was highlysigni_cant "F"0\35#�12[2#[4 Before adjusting for FIM\
4 In contrast\ age as a covariate was not found to be signi_cant "F"0\37#�1[0#\ despite the fact that age and error scores were signi_cantlycorrelated for the RCVA group[
we determined that the interactions involving FIM andthe between factors did not approach signi_cance"p×9[09#\ that is\ that the assumption of parallelism waswarranted ð08Ł[ We then deleted these interaction termsfrom the model and found that the main e}ect for groupwas signi_cant "F"0\40#�6[2#[ Thus\ the di}erencebetween the two patient groups persists after we stat!istically control for FIM[
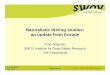
The analysis produced the expected main e}ect of con!dition "F"2\042#�3[3#^ but more importantly\ there wasno suggestion of a condition×group interaction "F³0#[Figure 1 "top# shows the breakdown of means with thedata transformed\ as they were in the ANCOVA^ Fig[ 1"bottom# shows the untransformed data[ It is evident thatthe pattern across conditions is very similar for the twogroups\ except that the RCVA group shows a greater risein error score in condition 3 "Dual!Search#\ which is moreapparent in the untransformed means[5
2[1[ Error patterns
Schwartz et al[ ð28Ł found that the modal error type forCHI patients was omission "27) of all errors#\ followedby sequence "19)#\ and action addition "01)#[ Objectsubstitutions accounted for 8) of the errors[ Com!parable analysis performed on the RCVA data yielded asimilar ranking "Table 6#] omissions "37)# followed by
5 The ANCOVA was repeated using the raw "untransformed# means\and there\ too\ the condition×group interaction did not approachsigni_cance "F³0#[ It should be said\ however\ that when Schwartz etal[ ð28Ł analyzed just the data from CHI and age!matched controls\ thecontrast for conditions 2 vs 3 was not signi_cant for either main e}ector condition×group interaction[

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð5547
Fig[ 1[ Performance across the four conditions of the MLAT is shown for the RCVA patients from the present study "n�29# and the CHI patientsreported in Schwartz et al[ ð28Ł "n�29#[ The top graph shows the means "and standard error bars# for the dependent variable under the square roottransform used in the analysis of variance[ The bottom graph shows the untransformed data[
sequence "08)#\ action additions "7)# and object sub!stitutions "6)#[
For the control subjects\ omission was not the pre!dominant error type\ although these did account for 5 ofthe 18 errors committed "10)#[ In Schwartz et al[ ð28Ł\omissions accounted for only 0 of the 25 errors "2)#committed by the neurologically intact control group"n�07#[ Those controls were age matched to CHI\ hencesubstantially younger than the controls in the presentstudy[
Using a standardized error rate measure which con!trolled for the number of error opportunities\ Schwartzet al[ ð28Ł found that the CHI group|s standardized ratefor omissions was signi_cantly higher than the stan!dardized rates for sequence errors and object substi!tutions\ and that only omissions varied signi_cantlyacross conditions[ We next investigated whether thesee}ects would hold as well for the RCVA group[
To compute the standardized rate measure * rate per099 opportunities * we take the number of errors of a

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð55 48
Table 6Error frequencies\ expressed as proportions of all errors
Controls "n�07# RCVA "n�29#
Omission 9[10 9[36Sequence 9[09 9[08Object substitution 9[13 9[96Action Addition 9[13 9[97Gesture substitution 9[92 9[90Spatial Misorientation 9[96 9[95Spatial Mis!estimation 9[99 9[93Tool omission 9[92 9[90Quality 9[99 9[96
Total number of errors for the control group was 18 and for the rightCVA "RCVA# group it was 514[
given type committed by the subject\ divide it by thenumber of opportunities that exist for that error type inthat condition\ and multiply by 099[ We estimate theerror opportunities by simply counting up the number ofexemplars listed on the coding sheet\ restricting ourselvesto those error types for which the sheets provide anexhaustive listing of unique exemplars "omissions\ objectsubstitutions\ and a subset of sequence errors "antici!pation:omissions^ reversals#\ hereafter denoted as{{sequence||[
Table 7 shows the RCVA group|s mean standardizedrates for these three error types\ broken down bycondition[ As we had previously found for CHI\ theomissions continue to predominate over the other errortypes even with opportunities controlled in this way[
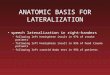
For a closer comparison with CHI\ we carried out arepeated measures ANOVA with standardized error rateas the dependent variable[ We found that the group factorinteracted signi_cantly with error type "F"1\005#�4[6#but not with condition "F³0#[ In post hoc analysis ofthe group×error type interaction\ the standardized errorrate for RCVA exceeded CHI for omissions "t"47#�5[96^p�9[901# and {{sequence|| "t�5[9^ p�9[906#\ but notobject substitutions "t�1[34^ p×9[09# "see Fig[ 2#[ "Note]critical value of p is 9[906[# Evidence presented below
Table 7Standardized error rates "errors per 099 opportunities# for the right CVA "RCVA# group
Type of error Condition 0 Condition 1 Condition 2 Condition 3 M SE"Solo!Basic# "Solo!Distractors# "Dual!Basic# "Dual!Search#
M SE M SE M SE M SE
Omission 06[1 4[1 08[9 3[8 12[6 4[4 29[0 4[7 11[4 1[6{{Sequence|| 5[0 1[9 5[2 1[1 2[0 9[6 4[9 0[2 4[0 9[7Obj[ subst[ 0[9 9[4 5[2 0[7 0[7 9[7 0[0 9[5 1[5 9[5
7[0 1[9 09[4 1[9 8[5 1[0 01[0 1[3
suggests that this may relate to the way in which severityimpacts the di}erent error types[
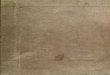
The ANOVA also produced a signi_cant con!dition×error type interaction "F"5\ 237#�3[0#[ As in theearlier CHI study\ the e}ect of condition was signi_cantfor omissions "F"0\ 063#�00[2#\ but not for {{sequence||"F³0# or object substitution "F�0[3^ p×9[19# "see Fig[3#[ The omission e}ect was further subject to plannedcontrasts] within the Dual conditions\ omissions occurredat higher rates in Dual!Search\ compared with Dual!Basic "F�00[2#[ And within the Solo conditions\ therewas a trend toward higher rates in Solo!Distractors\ com!pared with Solo!Basic "F�1[8^ p�9[98#[ These e}ectswere present in both CHI and RCVA groups\ as shownin Fig[ 4\ and as supported by the absence of a three!wayinteraction "F"5\ 237#�0[1^ p×9[19[#[
When Schwartz et al[ ð28Ł looked at how standardizederror rates for the three error types varied across theindividual CHI subjects\ it turned out that the omissionrate was highly correlated with severity\ as measured bothby error score and by FIM[ The correlations for the othererror types were lower or not statistically reliable[ Table8 show how these correlations compare in CHI vs RCVA[For the most part\ the data pattern in much the sameway for the two groups^ in particular\ the correlationbetween omissions and severity is very strong[
Table 8 also sheds light on the _nding\ reported above\that there was a group di}erence in standardized errorrate for omissions and {{sequence|| but not for objectsubstitutions] RCVA are more clinically severe\ andomissions and {{sequence|| correlate more strongly withseverity than do substitutions[
3[ Discussion
Results from study 0 show that an unselected groupof acute\ right hemisphere stroke patients was seriouslyimpaired\ relative to a neurologically intact controlgroup\ in executing familiar tasks of everyday life in thecontext of the MLAT[ The RCVA group made moreerrors on all conditions of the MLAT\ but the di}erence

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð5559
Fig[ 2[ Means "and standard error bars# of the standardized error rate "errors per 099 opportunities# for object substitution\ omission\ and {{sequence||errors[ The data presented are from the RCVA patients from the present study "n�29# and the CHI patients reported in Schwartz et al[ ð28Ł "n�29#[{{sequence|| comprises anticipation\ anticipation:omission\ and reversal errors[
Fig[ 3[ Mean "and standard error bars# of the standardized error rate "errors per 099 opportunities# for RCVA and CHI groups combined "n�59#\illustrating the condition×error type interaction[ CHI data are from Schwartz et al[ ð28Ł[
was greater on the more complex\ dual task conditions\and especially the dual condition with drawer search[
Nearly half of all the errors committed by the RCVAgroup involved omission of a key step[ The prevalence ofomissions does not reduce to di}erences in opportunitiesfor the major error types[ The comparison of stan!dardized error rate * which controls for opportunities *con_rmed the basic e}ect] mean rate for omissions was
four times that of {{sequence|| and eight times that ofobject substitutions[
These _ndings from the RCVA group were very similarto what we had previously observed in a group of recover!ing CHI patients ð28Ł[ And the way that the two patientgroups responded to the conditions manipulation wasalso very similar[ In analyses of mean error scores andstandardized error rates\ we found reliable condition

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð55 50
Fig[ 4[ Mean "and standard error bars# of the standardized error rate for omissions "omissions per 099 opportunities#\ broken down by MLATcondition[ CHI data are from Schwartz et al[ ð28Ł[
Table 8Comparison of correlations in right CVA "RCVA# and closed head injury "CHI#
Variables Pearson r Signi_cance level of testfor di}erence
RCVA group "n�29# CHI group "n�29#
Omissions and error score 9[74����� 9[84����� ��{{Sequence|| and error score 9[60����� 9[48���� n[s[Obj[subst[ and error score 9[26�� 9[20� n[sOmissions and FIM −9[38��� −9[43��� n[s[{{Sequence|| and FIM −9[47���� −9[94 "n[s[# ��Obj[ subst[ and FIM −9[17 "n[s[# −9[15 "n[s[# n[s[
n[s[ not signi_cant "p×9[09#[� 9[09×p×9[94��p³9[94[���p³9[90[����p³9[990[�����p³9[9990[CHI data are from Schwartz et al[ ð28Ł[
e}ects\ but no group×condition interactions[ Theabsence of interaction is especially notable in the stan!dardized error rate analyses\ where it emerged that thecondition e}ect was reliable only for omissions[ That is\complicating the solo tasks by adding distractors\ or thedual tasks by adding drawer search\ encouraged omis!sions speci_cally\ and this was true for both patientgroups[
In both CHI and RCVA studies\ we found that FIM\a widely used measure of clinical severity\ strongly pre!dicted overall error scores[ As FIM scores were worse forthe RCVA group\ it follows that their errors scores werehigher\ as well[ But the group di}erence was found to
persist in an analysis of covariance which statisticallycontrolled for FIM[ Thus\ it appears that right hemi!sphere damages confers greater vulnerability to errors^but how this vulnerability manifests across error typesand across conditions is basically the same in the twopatient groups[
Before discussing how these _ndings relate to theresource hypothesis\ it is useful to consider what role\ ifany\ hemispatial neglect played in the performance ofthe RCVA group[ While this study was not speci_callydesigned to answer this question\ we did perform somerelevant post hoc analyses\ summarized here under study1[

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð5551
4[ Study 1
Recall that 04 of the 14 patients assessed on the"expanded# stroke scale demonstrated neglect to somedegree[ These 04 were among the most clinically severein our sample[ "Mean FIM score is 56[8 compared to 64[8for the sample as a whole[# And\ as expected from thestrong correlation between FIM and error score\ theywere among the highest error producers[ "Mean numberof errors is 18[8\ compared to 19[7 for the sample as awhole#[
In some of these patients\ left!side neglect had amarked and obvious in~uence on error production[ Thisis illustrated in the following scenarios\ which are takenfrom two patients assessed as having neglect]
Pt[ W[M["FIM�57# * condition 3 "Dual!Search# forthis patient involved wrapping a gift and preparing aletter[ W[M[ did not look toward the left at any pointduring the task\ and\ consequently\ did not use the gift"a doll#\ gift box\ letter\ or stamps located on the left[Searching through the drawer\ he found the bag ofdecorative bows and the masking tape\ and proceededto tape the bag shut "an action addition#[ He thensealed the empty envelope "anticipation:omission#\and announced that he was _nished "omissions for thesteps of tearing the stamp from the roll and applyingit to the envelope#[
Pt[ P[S[ "FIM�098# * condition 1 "Solo!Distractors#for this patient required making a piece of toast withbutter and jam[ He began the task looking to the right\where he encountered the bag of bread\ along with ahot plate!the distractor for toaster "located on the left#[P[S[ placed the slice of bread onto the hot plate andwaited\ all the while checking for heat "the hot platewas not plugged in#[ He expressed dissatisfaction withthe lack of progress\ and visually searched the table\eventually turning toward the left and at one pointlooking directly at the toaster[ But at no point did heacknowledge his error or attempt to correct it[
We carried out several analyses to determine whetherthe spatial in~uence on errors was statistically reliablewithin and across subjects[
4[0[ Methods
4[0[0[ SubjectsFrom the original RCVA group "n�29#\ we further
analyzed the data from those patients who had stan!dardized rates of omissions "omissions per 099 oppor!tunities# greater than 9 but less than 099\ and who hadbeen assessed on the neglect item of the NIH stroke scale[There were 06 such patients[ Ten of the 06 earned a scoreindicative of neglect[ Mean FIM scores of these neglectand non!neglect patients did not di}er "t"03#�0[6\p�9[73#[ Seven of the 09 neglect patients had cortical
lesions that included "n�5# or were restricted to "n�0#the right frontal lobe[ Of the 6 non!neglect patients\ onehad cortical lesions that included the frontal lobe\ 4 hadright subcortical lesions\ and one was missing anatomicaldata[
4[0[1[ Procedures and resultsPerformance of the {{primary|| toast\ present\ and
lunchbox tasks in the Solo!Distractors\ Dual!Basic\ andDual!Search conditions was analyzed[ Three analyseswere performed which focused on the region of space inwhich action errors occurred[
In the _rst analysis\ each object of the primary taskwas given a single code indicating whether the object wasused at any point during the task or omitted throughout[Object location was assigned on the basis of the object|sinitial placement in the MLAT array[ Across the threeprimary tasks\ there were 09 objects in left hemispace and01 objects in right hemispace[ The locations of used andomitted objects were tallied for each subject and for eachsubgroup "neglect^ non!neglect#[
The ten neglect patients used 46 of the 099 objects "09objects×09 subjects# located in left hemispace\ and 84 ofthe 019 objects in right hemispace "Chi Square�01[4\Fisher|s Exact p�9[9993#[ The seven nonneglect patientsused 45 of the 69 objects in left hemispace\ and 54 of the73 objects in right hemispace "Chi Square�9[58\ Fisher|sExact p�9[73#[
In the second analysis\ each primary task was dividedinto a number of steps\ and a score assigned to each ofthe objects relevant to each step[ Objects were scoredas {{used||\ {{omitted||\ or {{unavailable||[ {{Unavailable||scores refer to occasions on which object"s# could not beused due to a prior omission[ For example\ a patient whofailed to open the juice bottle received an {{omitted|| scorefor the {{opens juice bottle|| step and an unavailable scorefor the following step\ {{juice into thermos||[ To avoidover!penalizing subjects for omitting unavailable objects\steps with such scores were dropped from further analy!sis[
We next coded the {{on!line|| locations of objects usedand omitted at each step[ Speci_cally\ we coded theobjects for their location relative to the subject|s torsoat the time the step was relevant[ This permitted us toaccommodate object and subject movements during thecourse of the task[ {{Midline|| denotes the region boundedby the subject|s shoulders\ while {{right hemispace|| and{{left hemispace|| denote those regions lateral to the rightand left shoulder\ respectively[ The instances of objectomission and object use in the left and right hemispacewere tallied[
For the neglect patients\ the ratio of used to not!usedleft objects was 72]81\ whereas the ratio for right objectswas 108]34 "Chi Square�50[8\ p³9[9990#[ The neglectpatients were thus signi_cantly more likely to fail to useobjects in left hemispace[ In contrast\ for the nonneglect

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð55 52
patients the ratio of used to not!used left objects was095]17 and the ratio for right objects was 093]20 "ChiSquare�9[75\ Fisher|s exact p�9[66#[ Five of the 09neglect patients were signi_cantly more likely to fail touse objects in left hemispace "Chi Square ×09[5\ p³9[90for each of the _ve subjects#\ whereas none of the non!neglect patients showed a signi_cant di}erence betweeninstances of object use in left vs right hemispace "pr9[19for all subjects#[
In the third analysis\ we assessed whether object sub!stitution errors\ in particular\ were conditioned by spatialfactors[ Using the same on!line position coding as wasused in analysis 1\ we determined the active hemispace inwhich target "substituted!for# objects were located[ Forexample\ a left!sided substitution was scored when\ in the{{bread into toaster|| step\ a subject used the hot!plate"on the right# instead of the toaster located in the lefthemispace[
The 09 neglect patients made 04 substitution errors inwhich the correct target object was in left hemispace\ vsonly one substitution in which the target object was inright hemispace[ In contrast\ the substitution errors ofthe nonneglect patients were evenly divided between leftsided and right sided objects "1 and 2 substitutions\respectively#[
4[1[ Discussion
The analyses performed to assess the in~uence of spa!tial factors on errors lead to the same unambiguous con!clusion] omission and substitution errors of patients withneglect\ but not those without neglect\ are conditionedby the hemispace in which relevant objects are located[Neglect patients as a group "and several individual pati!ents\ as well# were more likely to omit left sided objectsand to use objects on the right[ In addition to providingempirical support for a well!known clinical phenomenon\this _nding validates the simple clinical assessment weused to categorize neglect and non!neglect patients[ "Seeunder description of stroke scale assessment#[
While the hemispatial placement of objects clearlyin~uenced the performance of neglect patients\ these pat!ients also committed many errors that could not be attri!buted to left!sided unawareness[ For example\ the _rstanalysis unearthed 34 instances in which neglect patientsfailed to use target objects in right action space[ Thirty!two of these represent pure instances of right!sided objectuse failure\ in that nothing on the left was required forthe step to be completed[ Eight of the 09 neglect patientscontributed at least one pure right!sided object use fail!ure[
The occurrence of right!side omissions in left neglectpatients has been observed before\ in paper!and!penciltests for neglect ð09\ 02\ 20\ 36Ł[ While this may indicatethat the right hemisphere is specialized for distributingattention to both ipsilateral and contralateral space ð36Ł\
an alternative possibility is that right!side omissions sig!nal a non!spatial attentional de_cit that coincides withneglect ð20Ł[
In keeping with the latter view\ the neglect patients inthis study also made many errors in which the targetobjects were not neglected but rather used inap!propriately\ or in which something extra or excessive wasdone[ Examples include cutting or tearing too small apiece of wrapping paper or aluminum foil to cover thetarget item^ reading or writing on the prepared letter^perseveratively opening and closing the drawer or lunch!box^ and adding extra items to the lunchbox "e[g[\ jar ofapplesauce#[
Data from the nonneglect RCVA patients furtherimplicates an additional factor besides neglect in the gen!esis of action errors[ Six of the 6 nonneglect patientsexamined in study 1 performed outside the control rangefor their form[ Furthermore\ the types of errors theymade were similar to neglect patients at comparable levelsof severity[ The following scenario from a nonneglectpatient illustrates this point[
Pt[ M[W[ "FIM 098# * While performing pre!sent¦letter with search "condition 3#\ this patientpacked an empty gift box "omission for inserting gift#^wrote on the prepared envelope "action addition#^ andfailed to insert the letter into the envelope or seal it"omission for each step#[ In the toast¦co}ee condition"condition 2#\ he omitted the toasting step[
5[ General discussion
Study 0 showed that RCVA patients as a group areimpaired in the performance of naturalistic action tasksand that their performance has much in common with agroup of recovering CHI patients[ These _ndings are aswe predicted\ based upon two premises] that errors ofaction in CHI arise on account of reduced resourcecapacity^ and that reduced capacity is a reliable conse!quence of right hemisphere damage[ We will examineeach of these premises[
The notion that the brain makes available a limited!capacity pool of resources for enhancement of cognitiveoperations has a long and controversial history ð0\ 07\ 19\37Ł[ Schwartz et al[ ð28Ł invoked the resource constructto account for what appeared to be a continuum betweencontrol subjects and patients at di}erent levels of severity[On the MLAT\ control subjects made errors at low rates\and their errors were primarily commissions[ Mild CHIpatients made similar errors and at comparable rates\ onthe MLAT[ However\ on a more challenging extensionof this test\ named the {{1×2|| because it involved thethree primary tasks performed twice\ they producedmany more errors than controls and showed a greatertendency to make omissions[ More severe CHI patientsmade numerous omissions even on the MLAT and their

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð5553
commission errors were more frequent\ and often more~agrant\ than the controls and the milder patients[
The appearance of a continuum of behavior whichencompasses neurologically intact subjects at one endargues against de_cit!based accounts of the phenomenain question[ According to Schwartz et al[ ð28Ł\ the preva!lence of omissions\ compared to commission errors\ andtheir greater sensitivity to task and patient factors\ alsoundermines most de_cit!based accounts\ in particular\those that feature supervisory attention\ workingmemory\ or top!down response selection[ Any of thesede_cits would be expected to increase the vulnerability todata!driven errors and other errors of commission[
The arguments presented in Schwartz et al[ support anon!speci_c basis for errors in CHI^ however\ they donot make a positive case for limited resource capacity[Indeed\ a number of other general constructs could beinvoked * e}ort\ arousal\ alertness\ motivation\ and vig!ilance\ among others * so long as these are seen toconnote active processes "i[e[\ under volitional control#\governed in part by task and environmental demands[6
All of these interrelated constructs have been impli!cated in the right hemisphere syndrome[ The evidenceincludes enhanced susceptibility to dual task interference"relative to left hemisphere patients# ð8Ł\ low galvanic skinresponses in response to mild electrical stimulation ð03Ł\di.culty maintaining alertness in uncued reaction timetasks ð14Ł^ and the tendency to miss stimuli in ipsilesional\as well as contralesional\ space "see above#[ From ourperspective\ the implication of these _ndings is thatRCVA patients as a group should be highly vulnerableto errors of action^ and the evidence from study 0 bearsthis out[
Of course\ the presence of hemispatial neglect alsoconfers a vulnerability to errors\ and study 1 con_rmedthat spatial factors in~uenced the performance of theRCVA patients diagnosed as having neglect[ We argued\however\ that neglect\ by itself\ could not explain all the_ndings[ It explains neither the occurrence of errors inRCVA without neglect nor the occurrence of non!spatialerrors in those with neglect[ These lines of evidence impli!cate an additional factor\ besides neglect\ in the genesisof errors[
According to the present hypothesis\ this additionalfactor is reduced capacity[ Reduced capacity and spatial
6 The process must be volitional to account for the fact that humanagents can and do control the likelihood of action errors by expendinggreater e}ort\ paying closer attention\ slowing down\ and altering theenvironment ð07\ 16Ł[ The same appears to be true for the controlsubjects studied by Schwartz et al[ ð28Ł[ Their per task error rate washigher for the solo conditions of the MLAT than it was for the dualconditions and for the more complex {{1×2|| test\ cited above[ Thepresumption is that as the task demands increase\ these neurologicallyintact subjects expend more resources "e}ort\ motivation\ etc[# and\consequently\ are less likely to err[
neglect may have an additive in~uence] if we designate thedegree and manner of performance decrement associatedwith capacity loss as c and that associated with neglectas n\ then the total performance decrement in neglectpatients equals the sum of c¦n[ In RCVA patients with!out neglect\ the contribution of n is presumed to be neg!ligible\ and the same is true for recovering CHI patients[But now consider the strong similarities that were shownbetween the CHI and RCVA groups\ both in theirresponse to the conditions manipulation and in the pat!tern of errors they produced[ If the performance dec!rement in CHI is given by c and RCVA by c¦n\ thesimilarities are puzzling\ unless the contribution of n issmall\ relative to c[
One way to meet this requirement is to allow for inter!action between reduced capacity and neglect[ Thus\ ifneglect patients partially compensate for the hemispatialde_cit by utilizing resource capacity in scanning leftwardand acting in left hemispace\ this could have the e}ect ofdecreasing the contribution of n\ perhaps at the expenseof c[ Under this interaction scenario\ the capacity limi!tation is key to the breakdown of naturalistic actionproduction in RCVA\ notwithstanding the evident con!tribution of neglect[
There is some independent evidence for the interactionscenario[ Robertson and Frasca ð29Ł showed that thedegree of left!sided unawareness manifest on standardneglect tasks could be shown to increase under dual taskchallenge\ even where the secondary task was linguistic\and not visuospatial[ This implicates a general!purpose\limited capacity resource as a factor in left!sided neglect[Another study found that when left!neglect patients weretrained to maintain a heightened level of alertness\ theyshowed signi_cant reduction in the degree of neglect ð23Ł[Robertson ð18Ł reviewed these and other neglect studiesfrom the perspective of the PosnerÐPeterson theory ofattention ð15Ł and concluded that chronic left neglectrepresents the interaction of a spatial attentional de_cit\which is lateralized\ and a non!spatial\ arousal:sustainedattention de_cit\ which is not lateralized[ The arou!sal:sustained attention de_cit in~uences the expression ofneglect by\ among other things\ limiting the degree towhich patients learn and implement compensatory mech!anisms ð18\ 22Ł[
There is much overlap between our account and Rob!ertson|s "see also Heilman and colleagues| arousal!atten!tion model ð03\ 04\ 06Ł#[ The di}erence turns on the natureof the hypothesized non!lateralized de_cit^ Robertson|saccount implicates an attention controller\ which evi!dence suggests is served by the circuitry of the right fron!tal lobe ð12\ 38Ł[ Our evidence suggests that naturalisticaction breakdown does not localize to the frontal lobes"recall that here\ and in Schwartz et al[ ð28Ł pres!ence:absence of frontal involvement does not add to theprediction of error scores beyond clinical severity[# Nor\as we have recently found\ does its presentation in CVA

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð55 54
vary greatly with the side of lesion ð6Ł[ Along with theother evidence for non!speci_city\ the negative local!ization _ndings implies to us that the problem lies not inthe attention controller but rather in the resources itcontrols[
Returning to the theme of rehabilitation with whichwe began this paper\ we note that the theoretical pro!posals put forth here have testable implications for therehabilitation of neglect patients[ Thus\ assume it is truethat general purpose attentional resources are utilized byneglect patients in a compensatory manner\ and thatreduced capacity sets limits on what can be accomplished[Focusing these patients| attention to the left side of actionspace by means of anchoring or alerting techniques mightin~uence where and how resources are deployed\ but itshould not enhance capacity[ Consequently\ a decreasein left!sided object!use errors might well come at theexpense of right!sided and non spatial errors[ Such atrade!o} has\ on occasion\ been observed "Robertsonð17Ł^ also Charles Butters\ personal communication\ May\0886#[
Acknowledgements
This research is supported by a grant from the NationalInstitute for Neurological Diseases and Stroke "(RO0NS20713#[
References
ð0Ł Allport A[ Attention and control] Have we been asking the wrongquestions< Attention and Performance XIV] A Silver Jubilee\ MITPress\ Cambridge\ 0882[
ð1Ł Baars BJ "ed[# Experimental Slips and Human Error] Exploring theArchitecture of Volition[ Plenum Press\ New York\ NY\ 0881[
ð2Ł Boyd TM\ Sautter W[ Route!_nding] A measure of everydayexecutive functioning in the head injured adult[ Applied CognitivePsychology 0882^6]060Ð070[
ð3Ł Brott THP\ Adams J\ Olinger CP\ Marler JR\ Barsan WG\ BillerJ\ Spilker J\ Holleran R\ Eberle R\ Hertzberg V\ Rorick M\Moomaw CJ\ Walker M[ Measurements of acute cerebral infarc!tion] A clinical examination scale[ Stroke 0878^19]753Ð769[
ð4Ł Buxbaum LJ\ Schwartz MF\ Carew TG[ The role of semanticmemory in object use[ Cognitive Neuropsychology 0886^03]108Ð143[
ð5Ł Buxbaum LJ\ Schwartz MF\ Coslett HB\ Carew TG[ Everydayaction and praxis in callosal apraxia[ Neurocase 0884^0]2Ð06[
ð6Ł Buxbaum LJ\ Schwartz MF\ Montgomery MW[ Ideationalapraxia and naturalistic action[ Cognitive Neuropsychology\ inpress[
ð7Ł Cooper R\ Shallice T\ Modelling the selection of routine action]Exploring the criticality of parameter values[ In Proceedings of the08th Annual Conference of the Cognitive Science Society\ eds ShaftoMG\ Langley\ P[ Lawrence Erlbaum\ Mahway\ NJ\ 0886\ pp[ 020Ð025[
ð8Ł Coslett HB\ Bowers D\ Heilman K[ Reduction in cerebral acti!vation after right hemisphere stroke[ Neurology 0876^26]846Ð851[
ð09Ł Gainotti G\ Giustolisi L\ Nocentini U[ Contralateral and ipsi!lateral disorders of visual attention in patients with unilateral brain
damage[ Journal of Neurology\ Neurosurgery and Psychiatry0889^42]311Ð315[
ð00Ł Glisky EL\ Schacter DL\ Tulving E[ Learning and retention ofcomputer!related vocabulary in memory!impaired patients]Method of vanishing cues[ Journal of Clinical and ExperimentalNeuropsychology 0875^7]182Ð201[
ð01Ł Guide for the Use of the Uniform Data Set for Medical Rehabili!tation "Adult FlM#\ Version 3[9[ State University of New York atBu}alo\ Bu}alo\ NY\ 0882[
ð02Ł Halligan PW\ Burn JP\ Marshall JC\ Wade DT[ Visuo!spatialneglect] Qualitative di}erences and laterality of cerebal lesion[Journal of Neurology\ Neurosurgery and Psychiatry 0881^44]0959Ð0957[
ð03Ł Heilman KM\ Schwartz HD\ Watson KT[ Hypoarousal in patientswith the neglect syndrome and emotional indi}erence[ Neurology0867^17]118Ð121[
ð04Ł Heilman KM\ Valenstein E[ Frontal lobe neglect in man[ Neuro!logy 0861^11]559Ð553[
ð05Ł Heilman KM\ Van Den Abell T[ Right hemispheric dominancefor mediating cerebral activation[ Neurology 0868^06]204Ð210[
ð06Ł Heilman KM\ Watson KT[ Mechanisms underlying the unilateralneglect syndrome[ In Advances in Neurology\ eds Weinstein EA\Friedland RP\ Vol 04[ Raven Press\ New York City\ 0866\ pp[ 82Ð095[
ð07Ł Kahneman D[ Attention and Effort[ Prentice!Hall\ EnglewoodCli}s\ NJ\ 0862[
ð08Ł Kleinbaum DG\ Kupper LL[ Applied Regression Analysis andOther Multivariable Methods[ Wadsworth\ Belmont\ CA\ 0867[
ð19Ł Navon D[ Resources Ð A theoretical soup stone<[ PsychologicalReview 0873^80]105Ð123[
ð10Ł Norman DA[ Categorization of action slips[ Psychological Review0870^77]0Ð04[
ð11Ł Norman DA\ Shallice T[ Attention to action] Willed and AutomaticControl of Behavior[ Center for Human Information Processing"Technical Report No[ 88#[ "Reprinted in revised form in Con!sciousness and Self!Regulation\ eds Davidson RJ\ Schwartz GE\Shapiro D[ University of California\ New York\ 0875\ pp[ 0Ð07[
ð12Ł Pardo JV\ Fox PT\ Raichle ME[ Localization of a human systemfor sustained attention by positron emission tomography[ Nature0880^238]50Ð53[
ð13Ł Pocock SJ[ Clinical Trials] A Practical Approach[ John Wiley\ NewYork\ 0872[
ð14Ł Posner MI\ Inho} AW\ Friedrich FJ\ Cohen A[ Isolating atten!tional systems] A cognitive!anatomical analysis[ Psychobiology0876^04]096Ð010[
ð15Ł Posner MI\ Peterson SE[ The attention system of the human brain[Annual Review of Neuroscience 0889^02]14Ð31[
ð16Ł Reason JT\ Mycielska K[ Absent minded< The Psychology ofMental Lapses and Everyday Errors[ Prentice!Hall\ EnglewoodCli}s\ NJ\ 0871[
ð17Ł Robertson IH[ Anomalies in the lateralisation of omissions inunilateral left neglect] Implications for an attentional theory ofneglect[ Neuropsychologia 0878^16]046Ð054[
ð18Ł Robertson IH[ The relationship between lateralised and non!lateralised attentional de_cits in unilateral neglect[ In UnilateralNeglect] Clinical and Experimental Studies\ eds Robertson IH\Marshall JC[ Lawrence Erlbaum Assoc[\ Hove\ 0882\ pp[ 146Ð167[
ð29Ł Robertson IH\ Frasca R[ Attentional load and visual neglect[International Journal of Neuroscience 0881^51]34Ð45[
ð20Ł Robertson IH\ Halligan PW\ Bergego C\ Ho�mberg V\ PizzamiglioL\ Weber E\ Wilson BA[ Right neglect following right hemispheredamage< Cortex 0883^29]088Ð102[
ð21Ł Robertson IH\ Manly T\ Andrade J\ Baddeley BT\ Yiend J[{{Oops;||^ Performance correlates of everyday attentional failuresin traumatic brain injured and normal subjects[ Neuropsychologia0886^24]636Ð647[
ð22Ł Robertson IH\ Ridgeway V\ Green_eld E\ Parr A[ Motor recovery

M[F[ Schwartz et al[:Neuropsycholo`ia 26 "0888# 40Ð5555
after stroke depends on intact sustained attention] A 1!year follow!up study[ Neuropsychologia 0886^00]0Ð5[
ð23Ł Robertson IH\ Tegner R\ Tham K\ Lo A\ Nimmo!Smith I[ Sus!tained attention training for unilateral neglect] Theoretical andrehabilitation implications[ Journal of Clinical and ExperimentalNeuropsychology 0884^06]305Ð329[
ð24Ł Robertson IH\ Ward A\ Ridgeway V\ Nimmo!Smith I[ Test ofEveryday Attention[ Thames Valley Test Company\ Flempton\0883[
ð25Ł Schwartz MF[ Re!examining the role of executive functions inroutine action production[ Annals of the New York Academy ofSciences 0884^658]210Ð224[
ð26Ł Schwartz\ MF\ Buxbaum LJ[ Naturalistic action[ In Apraxia] TheNeuropsychology of Action\ eds Rothi LJG\ Heilman KM[Psychology Press\ East Sussex\ 0886\ pp[ 158Ð178[
ð27Ł Schwartz MF\ Mayer NH\ Fitzpatrick!DeSalme EJ\ MontgomeryMW[ Cognitive theory and the study of everyday action disordersafter brain damage[ Journal of Head Trauma Rehabilitation0882^7]48Ð61[
ð28Ł Schwartz MF\ Montgomery MW\ Buxbaum LJ\ Lee SS\ CarewTG\ Coslett BH\ Ferraro M\ Fitzpatrick!DeSalme E\ Hart T\Mayer N[ Naturalistic action impairment in closed head injury[Neuropsychology 0886^01]02Ð17[
ð39Ł Schwartz MF\ Montgomery MW\ Fitzpatrick!DeSalme EJ\Ochipa C\ Coslett HB\ Mayer NH[ Analysis of a disorder ofeveryday action[ Cognitive Neuropsychology 0884^01]752Ð781[
ð30Ł Schwartz MF\ Reed ES\ Montgomery MW\ Palmer C\ Mayer NH[The quantitative description of action disorganization after brain
damage] A case study[ Cognitive Neuropsychology 0880^7]270Ð303[
ð31Ł Shallice T[ From Neuropsychology to Mental Structure[ CambridgeUniversity Press\ Cambridge\ 0877[
ð32Ł Shallice T\ Burgess PW[ De_cits in strategy application followingfrontal lobe damage in man[ Brain 0880^003]616Ð630[
ð33Ł Shallice T\ Burgess PW[ The domain of supervisory processes andthe temporal organization of behaviour[ Transactions of the RoyalSociety 0885^240]0394Ð0301[
ð34Ł Shallice T\ Burgess PW\ Schon F\ Baxter DM[ The origins ofutilization behavior[ Brain 0878^001]0476Ð0487[
ð35Ł Stuss DT\ Shallice T\ Alexander MP\ Picton TW[ A multi!disciplinary approach to anterior attentional functions[ Annals ofthe New York Academy of Sciences 0884^658]080Ð101[
ð36Ł Weintraub S\ Mesulam M[ Right cerebral dominance in spatialattention[ Further evidence based on ipsilateral neglect[ Archivesof Neurology 0876^33]510Ð514[
ð37Ł Wickens CD[ Processing resources in attention[ In Varieties ofAttention\ eds Parasuraman R[\ Davies DR[ Academic Press\Orlando\ 0873\ pp[ 52Ð091[
ð38Ł Wilkins AJ\ Shallice T\ McCarthy R[ Frontal lesions and sustainedattention[ Neuropsychologia 0876^14]248Ð254[
ð49Ł Wilson BA\ Alderman N\ Burgess PW\ Emslie H\ Evans JJ[ BADS]Behavioural Assessment of the Dysexecutive Syndrome[ ThamesValley Test Co[\ Bury St[ Edmunds\ 0885[
ð40Ł Wilson BA\ Cockburn J\ Baddeley AD[ The Rivermead BehaviouralMemory Test[ Thames Valley Test Company\ Bury St[ Edmunds\0874[