Embed Size (px)
Citation preview

Natural History of Human Immunodeficiency Virus Disease in Perinatally
710 PEDIATRICS Vol. 97 No. 5 May 1996
Infected Children: An Analysis From the Pediatric Spectrum of DiseaseProject
Huiman X. Barnhart, PhD,* M. Blake Caldwell, MD4 Pauline Thomas, MD,� Laurene Mascola, MD,IIIdith Ortiz, MD,�IJ Ho-Wen Hsu, MD,# Joann Schulte, DO,’� Robert Parrott, MD4�
Yvonne Maldonado, MD,� Robert Byers, PhD4 and the
Pediatric Spectrum of Disease Clinical Consortiumil II
ABSTRACT. Objective. To describe the progressionof human immunodeficiency virus (HIV) diseasethrough clinical stages from birth to death among a largenumber of perinatally infected children.
Methods. The Pediatric Spectrum of Disease (PSD)project, coordinated by the Centers for Disease Controland Prevention (CDC), has conducted active surveillancefor HIV disease since 1988 in seven geographic regions.PSD data are collected from medical and social servicerecords every 6 months through practitioners at eachparticipating hospital clinic. We analyzed data from pen-natally HIV-infected children born between 1982 and1993. The natural history of HIV disease was divided intofive progressive stages using the clinical categories in theCDC 1994 pediatric HIV classification system: stage N,no signs or symptoms; stage A, mild signs or symptoms;stage B, moderate signs or symptoms; stage C, severesigns or symptoms; and stage D, death. A five-stageMarkov model was fitted to the PSD data. To comparethe estimates from the PSD project with the publishedestimates, we also fitted an alternative Markov modelusing acquired immunodeficiency syndrome (AIDS;1987 case definition) in place of stage C and also calcu-lated standard Kaplan-Meier estimates.
Results. A total of 2148 perinatally HIV-infected chil-dren were included in the analysis. The estimated meantimes spent in each stage were: N, 10 months; A, 4months; B, 65 months; and C, 34 months. We estimatedthat a child born with HIV infection has a 50% (95%
confidence interval [CII, 40%-60%) chance of severesigns or symptoms developing by 5 years of age and a75% (95% CI, 68%-82%) chance of surviving to 5 years ofage. For a child in stage B, there is a 60% (95% CI,49%-71%) chance of severe signs or symptoms develop-ing within the next 5 years and a 65% (95% CI, 56%-73%)chance of surviving 5 more years. The estimated meantime from birth to stage C was 6.6 (95% CI, 5.7-7.5) years,
From the *Depa�ent of Biostatistics, Rollins School of Public Health,Emory University, and �Division of HIV/AIDS, Centers for Disease Control
and Prevention, Atlanta, Georgia; §New York City Department of Health;
ilLos Angeles Department of Health Services; #{182}PuertoRico Department ofHealth, San Juan; #Massachusetts Department of Public Health, Jamaica
Plain; **�e,�s Department of Health, Austin; �Children’s National Medical
Center, Washington, DC; and 55Stanford University, Stanford, California.
I, IlMembers of the Pediatric Spectrum of Disease Clinical Consortium arelisted in “Acknowledgments.”
Received for publication Apr 17, 1995; accepted Oct 2, 1995.
Reprint requests to (H.X.B.) Department of Biostatistics, Rollins School of
Public Health, Emory University, Atlanta, GA 30322.
PEDIATRICS (ISSN 0031 4005). Copyright © 1996 by the American Acad-
emy of Pediatrics.
and the estimated mean survival time from birth was 9.4(95% CI, 8.1-10.7) years. From the alternative Markovmodel, the estimated mean time from birth to AIDS was4.8 (95% CI, 4.5-5.2) years.
Conclusion. Markov modeling using the revised pe-diatric classification system allowed us to describe thenatural history of HIV disease in children before diag-nosis of AIDS. On average, children progress to moder-ate symptoms in the second year of life and then remainmoderately symptomatic for more than half of their ex-pected lives, underscoring their need for clinical carebefore the onset of AIDS. The results from the Markovmodel are useful in family counseling, health care plan-fling, and clinical trial designs. Pediatrics 199697:710-716; pediatric HIV and AIDS, natural history, Markovmodel.
ABBREVIATIONS. HIV, human immunodeficiency virus; AIDS,acquired immunodeficiency syndrome; PSD, Pediatric Spectrumof Disease; CDC, Centers for Disease Control and Prevention; LIP,lymphoid interstitial pneumonia; CI, confidence interval.
Initial reports of the clinical manifestations of hu-man immunodeficiency virus (HIV) infection in pen-natally infected children described a rapidly progres-sive disease with short survival.”2 However, becausethese observations were made early in the epidemicon small numbers of children whose HIV infectionhad been ascertained because of their severe illness,they were biased toward including HIV-infectedchildren with the most rapidly progressive disease.Later descriptions were more comprehensive, be-cause larger numbers of children had been observed,the duration of follow-up was longer, and the devel-opment of HIV antibody testing allowed asymptom-
atic infected children to be included.3 As a result,
recent estimates of the time to acquired immunode-ficiency syndrome (AIDS) and death in peninatallyH1V-infected children are much longer than the ii-tial estimates.
Until recently, no systematic method for descnib-ing the course of HIV infection in children was avail-able. The 1987 dassification system for HP/-infectedchildren categorized HP/-related diseases but wasnot designed to describe disease progression.4 How-ever, the 1994 revision of this classification systemallows children to be classffied into mutually exclu-sive categories based on severity of disease. With this
by guest on July 2, 2020www.aappublications.org/newsDownloaded from

ARTICLES 711
new classification system and more cumulative fob-low-up time, an even more accurate description ofthe course of pediatric HIV infection, especially dun-ing the early stages, is now possible.
An accurate understanding of the timing of theprogression of HIV infection in children has impor-tant clinical, research, and public health benefits. Forclinicians, such knowledge contributes to prognosticinformation that can be communicated to patientsand their families. For researchers designing clinicaltrials, knowledge of the rates of occurrence of van-ous defined stages of disease assists in calculatingsample sizes and planning trial durations. For healthplanners, the length of each stage of disease is im-
pontant for estimating the resource needs of HIV-infected children.
A description of the progression of pediatric HIVdisease through the clinical stages can be developed
from clinical data. Ideally, the clinical data wouldcome from prospective clinical observations. How-ever, most prospective clinical series have limitednumbers of children under observation. The Pediat-ric Spectrum of Disease (PSD) project has collectedlongitudinal clinical data from more than 2000 HIV-infected children born to HP/-infected mothers.These children were diagnosed at various ages andfollowed for varying lengths of time. The Mankovmodel can be used to model these longitudinal datato describe the progression of HIV disease. Thismethod complements prospective cohort studies byestimating progression times based on larger num-bens of infected children using the newly designedclassification system. In addition, the Markov modelis uniquely suited to estimating progression time,because even in prospective studies, the exact time ofdevelopment of signs and symptoms that indicateprogression to a more severe stage is not preciselyknown and is dependent on the frequency of medicalevaluations. For example, documentation of liverand spleen enlargement moves a child from no-signson symptoms stage to the mild-signs and symptomsstage. However, the precise age at which the childentered the mild-signs and symptoms stage is oftennot known (it occurred at some point in time be-tween the two clinical evaluations). Therefore, theage at transition between disease stages is best esti-mated by mathematical models.
In this article, we describe the age-specific naturalhistory of HIV disease from birth to death amongchildren enrolled in the PSD project. To best describethe course of HIV disease among these lange num-bers of HP/-infected children, we applied Markovmodeling techniques that are specifically suited formodeling short portions of individual disease histo-ries and for evaluating transitions between clinicalstages, such as those in the new classification system.
METHODS
PSD Project
The PSD project has conducted active surveillance for HIVinfection and perinatal HIV exposure among children in sevengeographic regions: Los Angeles County, New York City, three
cities in Texas, Massachusetts, Washington, DC, Puerto Rico, andthe San Francisco Bay area. In most sites, the surveillance is
population based, enrolling essentially all children who have been
clinically identified as HIV exposed or infected in those geo-
graphic areas. In New York City and Washington, DC, the sur-veillance is hospital based, enroffing only children identified in thepartidpating hospitals and their associated clinics. The projectstarted in 1988, but all children born after January 1, 1976, who
were HIV infected or HIV exposed and who had been seen at oneof the participating institutions were eligible for inclusion in thePSD project.
Children eligible for enrollment are identified through practi-tioners at each partidpating hospital clinic. Study personnel visit
these institutions on a regular basis to collect data on childreneligible for the project. All available inpatient and outpatientmedical records on each child are abstracted at the initial evalua-tion. Records on each enrolled child are then reviewed every 6months.
Data are collected on standard forms and entered into a Centersfor Disease Control and Prevention (CDC)-designed software sys-tem at each site. Each participating site is responsible for estab-lishing a provider-specific data management plan, compatiblewith local status, which ensures strict confidentiality of all medicalrecords, surveillance registries, data collection forms, and com-puter files. Detailed data collection instructions and intensivetechnical support help ensure uniformity in data abstractionacross sites. The information collected on each child includesdemographic characteristics, mode of HIV exposure, diseases in-dicative of AIDS4 and other HP/-related conditions included in thePublic Health Service pediatric HIV classification system,5 labora-tory data, treatment for HJV infection, prophylaxis and treatmentof opportunistic infections, and date and cause of death if the childdied.
Data for Analysis
All data collected through year-end 1993 on children born since1982 were included in the analysis. Children born before 1982were excluded to avoid biases; HIV infection was not recognizedin children until 1982, and short-term survivors born before 1982would have been missed. The analysis presented here uses
months of age as the smallest time unit, because the dates ofsymptoms were collected only by month and year of occurrence.
Classification System
The CDC’s 1994 revised pediatric HIV classification systemcategorizes children by clinical status and CD4 T-lymphocytecount.5 We used these clinical categories to define the stages ofdisease. The clinical categories are: N, no signs or symptoms; A,
mild signs or symptoms; B, moderate signs or symptoms; and C,severe signs or symptoms (see “Appendix”). All AIDS-definingconditions in the CDC 1987 definition are included in category C,
except lymphoid interstitial pneumonia (LIP), which is less severeand associated with longer survival when compared with otherAIDS-defining illnesses. LIP is classified in category B. The cate-gories are mutually exclusive, and once a child has met the criteriafor a more severe category, that child is not reclassified in a less
severe category, even if the signs or symptoms resolve.
Markov Models
The natural history of HIV infection in perinatally infectedchildren can be considered as a progression of stages from birth todeath. Markov models have been successfully used to describeprogression of adults through stages of HIV infection6� and otherdiseases, including cancer.’215 The natural history of HIV diseasein perinatally infected children was divided into five progressive
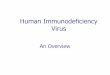
stages; clinical categories N, A, B, and C were defined by the HIVclassification system and a fifth stage, D (death), was included asthe final stage. Using the methods of Longini et al,6 we fit afive-stage Markov model to the PSD data. Like the classificationsystem, the model allowed children to progress when they met thecriteria for the next category but not to regress when signs orsymptoms improved. Figure la depicts the progressive stages;stage-specific rates of transition (hazard rates) are represented byA. We assumed that all children were in stage N at birth, because
perinatally infected children rarely have signs or symptoms ofHIV infection at birth.16 This Markov model assumed that everyinfected child moved to stage A, then to stage B, then to stage C,and finally to stage D in sequence as the disease progressed.
by guest on July 2, 2020www.aappublications.org/newsDownloaded from

N A B C D
(a)
p M ,#{216} M ,� M �#{216}�
Natural History of Pediatric HIV Disease
712 HP�’ PROGRESSION IN PERINATALLY INFECTED CHILDREN
Fig 1. a, five-stage Markov model.N, indicates no signs or symptoms;
A, mild signs or symptoms; B,
moderate signs or symptoms; C,
severe signs or symptoms; and D,
death. b, alternative five-stageMarkov model using AIDS as astage.
EIiII:i:�A1 � .‘�2 � “3 #{149}KIIIiII::��
N A B without LIP
(b)
C or LIP (AIDS) D
However, all stages may not have been observed because of thetiming of medical evaluations and the rate of disease progression.
In addition, the time of the observation may not be the exact time
when the child entered the stage. Thus, the data required models,such as Markov models, that were capable of estimating both thetime of entry and the time of exit for a stage and, hence, the time
spent in each stage.To compare the results from the PSD data with published data,
an alternative five-stage Markov model was also fit to the PSDdata (Fig Ib). By placing LIP with category C rather than categoryB, the revised category (C including LIP) in this model becomesidentical to the 1987 AIDS case definition. In addition, we alsocalculated Kaplan-Meier estimates for time from birth to diagnosisof AIDS, time from birth to death, and time from diagnosis ofAIDS to death.
RESULTS
Clinical data from 2148 perinatally HIV-infectedchildren born between 1982 and 1993 were indudedin the analyses. Of these children, 11% were white,45% were African-American, 41% were Hispanic,and 3% had other or unrecorded race or ethnicity.The mother’s risk of HIV transmission was sexualcontact in 30%, injected drug use in 40%, and other orunrecorded risk in 30%. Of the children included inthe analysis, 36% were from New York City, 16%were from Puerto Rico, 13% were from Massachu-setts, 10% were from Los Angeles, 9% were fromWashington, DC, 9% were from Texas, and 7% werefrom San Francisco. One hundred twenty-four (6%)of the children were born in 1982 and 1983,247(12%)were born in 1984 and 1985, 386 (18%) were born in1986 and 1987, 521 (24%) were born in 1988 and 1989,609 (28%) were born in 1990 and 1991, and 261 (12%)were born in 1992 and 1993. At year-end 1993, 458(21%) had died, 357 (17%) were in stage C, 1157(54%) were in stage B, 143 (7%) were in stage A, and33 (2%) were in stage N. The mean age of livingchildren at the time of the most recent clinical eval-uation was 50 (median, 43) months. The mean age atdeath for the children who had died was 32 (median,23) months. Three hundred forty-eight (16%) chil-dren died in the first 4 years of life, and 876 (41%)survived beyond 4 years of age. Thus, substantially
more children have less rapidly progressive disease,and the resulting model primarily reflects this pop-ulation.
Table I displays the number of paired observa-tions for every two consecutive observation times(including birth). The months between the two con-secutive observation times range from I to 127months, with a median of 6 months. These numbers,together with the observation times, contributed tothe estimate of transition time from one stage to thenext stage. Of the 2148 HIV-infected children whobegan in stage N at birth, 2115 (98%) were observedin other stages (row N, columns A-D) at some time.The largest frequency in Table I is row B, column B,which indicates that many children remained instage B for several observations without progressingto stage C or D. Relatively small numbers in row Ashow that many children progressed to stages Bthrough D quickly without being observed in stageA. Of the 458 deaths observed, 388 (85%) occurred inchildren with severe signs or symptoms at previousobservations (row C, column D).
The estimated mean and median times spent ineach stage from the five-stage Markov model aregiven in Table 2. The estimated mean times spent instages N and A were relatively short (10 and 4months, respectively), and the time spent in stage Bwas the longest (mean, 65 months). Table 3 showsthe estimated mean and median times from the be-ginning of stages N, A, and B to the beginning of
TABLE 1.Consecutive 0
Number of Observed Paired Stages for Every Twobservation Times (Induding the Time of Birth)
From Stage To Stage Total
N A B C D
NABC
Total
559 255 1396 461 3 2674. . . 307 101 9 2 419. . . . . . 3638 275 65 3978
. . . . . . . . . 1583 388 1971559 562 5135 2328 458 9042
by guest on July 2, 2020www.aappublications.org/newsDownloaded from

ARTICLES 713
TABLE 2. Mean and Median Times Spent in Each Stage
Stage Mean
Mo (yr)
Time
95% CI
Median
Mo (yr)
Time
95% CI
N 10 (0.9) 9-11 7 (0.6) 6-7A 4(0.3) 3-4 3(0.2) 2-3B 65 (5.4) 60-70 45 (3.8) 42-48
C 34 (2.8) 31-37 24 (2.0) 21-26
TABLEFrom th
3. Estimated Mean and Median Te Beginning of Each Stage
lines to Stage
From Mean Time to C Median Time to C Proportion ofStage
mo (yr) 95% CI mo (yr)C Within 5 yr
(95% CI)
N 79 (6.6) 5.7-7.5 60 (5.0) 0.50(0.40-0.60)
A 69 (5.7) 4.9-6.6 49 (4.1) 0.58 (0.47-0.69)B 65 (5.4) 5.1-5.8 45 (3.8) 0.60 (0.49-0.71)
stage C. The estimated mean time from birth (stageN) to stage C was 6.6 years (95% confidence interval[CI], 5.7-7.5 years). We estimated that a child withHIV infection has a 50% chance of severe signs orsymptoms developing by 5 years of age. For childrenwho have just entered stage B, the chance of severesigns or symptoms developing in the next 5 years is60%.
Table 4 shows the estimated mean and mediansurvival times from the beginning of each stage. For
a child with perinatally acquired HIV infection, themean survival time (birth to death) was estimated as9.4 years (95% CI, 8.1-10.7 years), and the probabilityof surviving to 5 years of age was 75%. For childrenwith moderate signs or symptoms (stage B), the es-
timated mean time from stage B to death was 8.2years. For a child with severe signs or symptoms, theestimated mean time from stage C to death was 2.8years (95% CI, 2.5-3.1 years), and the chance of sur-viving 5 years was 17%.
In the alternative five-stage Markov model withAIDS in place of stage C (Fig ib), the AIDS incuba-tion period was the time from birth (stage N) to stageC including LIP. The estimated mean times spent ineach stage were 10 months for stage N, 4 months forstage A, 44 months (3.7 years) for stage B not includ-ing LIP, and 54 months (4.5 years; 95% CI, 4.1-4.9years) for the AIDS stage. The estimated median timefrom AIDS to death was 3.1 years. From the cumu-lative distribution of the AIDS incubation period, weestimated that the mean AIDS incubation period was58 months on 4.8 years (95% CI, 4.5-5.2 years; me-dian, 3.8 years).
For comparison, we also computed estimates fromthe Kaplan-Meier method using the same data. Theestimated median survival time was 10.9 years. Thisestimate is biased, because no death was observedafter 10.9 years, and the 95% CI is not available.However, the estimated probability of surviving 5years was P = .76 (95% CI, .74-.78). The median timeto AIDS was estimated as 4.9 years (95% CI, 4.2-5.5years). We used 943 children with AIDS to estimatethe survival time from AIDS. The median time fromAIDS to death was 3.1 years (95% CI, 2.7-3.7 years).
Subgroup analyses were performed to address
C
possible biases. We first selected infected childrenborn between 1986 and 1989 to exclude those chil-dren born before the HIV enzyme-linked immu-nosorbent assay was developed and to avoid biasesresulting from short follow-up times. A total of 907infected children were included in subgroup 1. Toaddress possible case ascertainment bias, subgroup 2
consisted of the 1171 children enrolled from the pop-ulation-based project sites (ie, excluding New York
City and Washington, DC). The third subgroup con-tained the 486 children who were included in bothsubgroups 1 and 2. Table 5 gives the estimated meantimes spent at each stage as well as the times frombirth to stage C, mean survival times, AIDS incuba-tion periods, and mean survival times from AIDS.The estimates from the subgroup analyses were sim-ilar to the estimates from the analyses that includedall 2148 children.
DISCUSSION
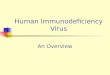
We have used a staged Markov model to describethe age-specific natural history of HIV disease inpeninatally infected children from birth to death (Fig2). Several authors have advocated using the Markovmodel over other methods, such as the Kaplan-Meienmethod, to analyze data on the natural history ofHIV.6� First, the Markov model allows the progres-sion of a disease through different stages to be ex-amined and, therefore, provides a comprehensiveview of the disease process. Second, in contrast to theKaplan-Meier method, the Markov model can handle
data in which the exact transition times among stagesare not known (right, left, or interval censored).Therefore, the Mankov model can use incompletelongitudinal data on short portions of individualdisease histories more efficiently than can theKaplan-Meien method. However, when applyingboth methods to the PSD data, the estimates weresimilar.
Because this analysis is the first to use the 1994revised classification system with Mankov modelingto assess clinical progression among HP/-infectedchildren, it is important to examine the validity andpotential biases of the data and the model. The pri-many limitation of this Markov model was its as-sumption that children moved through the clinicalstages in sequence, which may not be true for somechildren. A more complex model, which allows chil-dren to jump over one or more clinical stages, isbeing developed. The potential biases in the data aremore numerous. Our analyses used data obtained byreviewing the medical records of all HP/-infected
TABLE 4. Estimated Mean andthe Beginning of Each Stage
Median S urvival Times From
From Mean Survival Time Median ProportionStage Survival
Time
mo (yr)
Surviving atLeast 5 yr
#{176}mo (yr) 95% CI
N 113 (9.4) 8.1-10.7 96 (8.0) 0.75 (0.68-0.82)A 103 (8.6) 7.2-9.9 85 (7.1) 0.67(0.61-0.74)B 99 (8.2) 6.9-9.6 81 (6.8) 0.65 (0.56-0.73)C 34 (2.8) 2.6-3.1 23 (1.9) 0.17(0.10-0.24)
by guest on July 2, 2020www.aappublications.org/newsDownloaded from

0 1014Birth
113Death
TABLE 5. Subgroup Analyses: Mean Times in Stages and Between Stages
714 HIV PROGRESSION IN PERINATALLY INFECTED CHILDREN
Stages Subgroup I
(n = 9#{216}7)*
Subgroup 2
(n = 1171)*
Subgroup 3
(n = 486)*
mo (yr) 95% CI
All
(n = 2148)
mo (yr) 95% CI mo (yr) 95% CI mo (yr) 95% CI
N 11 (0.9) 10-12 9 (0.7) 8-10 10 (0.8) 10-11 10 (0.9) 10-11A 5 (0.4) 4-5 3 (0.3) 3-4 3 (0.3) 3-4 4 (0.3) 3-4
B 61 (5.1) 55-67 61 (5.1) 56-67 55 (4.6) 48-62 65 (5.4) 60-70
C 33 (2.8) 29-37 32 (2.7) 28-36 32 (2.7) 27-37 34 (2.8) 31-37N to C 77 (6.4) 56-97 73 (6.1) 58-89 69 (5.7) 42-96 79 (6.6) 68-90
N to D 110 (9.2) 81-139 105 (8.8) 82-128 101 (8.4) 61-141 113 (9.4) 97-128N to AIDS 55 (4.6) 48-61 61 (5.1) 52-70 54 (4.5) 38-70 58 (4.8) 54-62
AIDS to D 52 (4.3) 45-58 44 (3.7) 39-49 44 (3.7) 37-51 54 (4.5) 48-59
* Subgroup I includes all infected children born between 1986 and 1989; subgroup 2 is the population-based group that includes all
infected children born between 1982 and 1993 excluding New York and Washington, DC; subgroup 3 comprises infected children whoare included in both subgroups I and 2.
children at the seven sites born from 1982 to 1993.Because the capability for serologic diagnosis of HWwas limited before 1985, only symptomatic mothersand their children were identified during this period.We found that most of the deaths among youngerchildren occurred among those born recently. Thisfinding suggests that HP/-related deaths at an early
�age were not captured among children born early inthe epidemic. Furthermore, one study site (NewYork City) did not systematically enroll children whodied before the study began. In addition, childrenborn in the early years of the epidemic may haveentered the study at older ages, because data collec-tion for the project began in 1988. Although all med-ical records of these children were examined, theirdisease status was not observed every 6 months. Inour analyses, children born earlier contribute moreinformation for disease progression at later ages, andchildren born recently contribute more informationfor disease progression at early ages. A potential biasmay be present if infected children born earlier pro-gressed differently than the children born more re-cently. For example, children born before the wide-spread availability of prophylaxis for Pneumocystis
carinhi pneumonia, antiretroviral therapy, and othervarious advances in treatment for opportunistic in-fections may have progressed more rapidly thanchildren born more recently.
Another source of bias in these data is incompletecase ascertainment. HP/-infected children born tomothers not tested for HIV are generally not identi-fled until either the mother or the child becomessymptomatic. Therefore, the PSD data are potentiallybiased toward more symptomatic children. Last, thetime interval of data abstraction introduces a poten-tial bias. Because the mean times spent in stages Nand A are relatively short (10 and 4 months, respec-tively), and the data are collected in 6-month inter-vabs, the estimates of the ages at transition from
stages N to A and A to B may be less precise than theones from stages B to C and C to D. As a result, the
confidence bounds from the Markov model mayoverestimate our true confidence.
The subgroup analyses address these issues. Theestimated times spent in each stage and betweenstages are very similar among the four groups. Thesubgroup analyses reassure us that the analyses us-mg all children born between 1982 and 1989 are notsubstantially affected by the biases discussed. We
postulate, specifically, that the children under carebefore routine use of effective therapies may haveprogressed differently. However, they contribute asmall portion of the data used to fit the model and donot distort the estimate. Thus, the results of the anal-yses using all 2148 children are more reliable becausethe sample size is larger.
In the past several years, both statisticians’7 andclinicians’8’19 have observed that HP/-infected chil-dren fall into two distinct groups. The first group issmaller and has a more rapid disease course than thesecond group, but both groups have more rapidprogression than adults. Auger and colleagues,17 us-ing a mixture model of two Weibull distributions,estimated that the median time to AIDS was 4months for the first group and 6.1 years for thesecond group. In our analysis, 16% of the childrendied in the first 4 years of life (short-term survivors),41 % survived beyond 4 years of age (long-term sun-vivons), and 43% are alive at ages younger than 4years and may be short or long-term survivors. Do-scribing disease progression in two distinct popula-tions of HP/-infected children using the Markovmodel will require modeling the mixture of twoMarkov processes. The method for this modelingprocess has not been described but is currently beingdeveloped. However, the population that we ana-lyzed has a larger number of long-term survivorsthan short-term survivors. We estimated that 72% of
I AIDS
� B � C
58 79
Time in months
Fig 2. Estimated mean age of transition between clinical stages for children with perinatal HIV infection.
by guest on July 2, 2020www.aappublications.org/newsDownloaded from

ARTICLES 715
the children represented in our data were long-termsurvivors. Thus, the resulting estimates of diseaseprogression in this population will approximate thedisease progression in the long-term survivor popu-lation more closely than in the short-term survivorpopulation.
These estimates provide prognostic informationfor children classified using the revised pediatricclassification system. Based on the single Markovmodel that we used, a peninatally infected childwould remain in stage N until 10 months of age andwould be in stage A for 4 more months. A childentering stage B has a 60% chance of severe diseasedeveloping (stage C) in the next 5 years and anexpected survival of 8.2 more years. Some childrenmay have passed directly from stage N to stage B or,more likely, from stage A to stage C. Our modelassumed that they passed through the intermediatestage but were not observed in that stage. Many ofthese children are probably members of the short-term survival group and await modeling of the twoMarkov processes for a more accurate description.
Our findings are consistent with reported clinicalobservations. The Italian Register for HP/3 observedthat some signs or symptoms had developed in76.6% of infected children by I year of age, comparedwith our estimate of 68.8%. They estimated that the5-year survival was 75%,20 which is identical to ourestimate. For French children, Blanche et al18 found acomparable 5-year survival of 65%. Furthermore,they estimated that 48% of perinatally infected chil-dren died within 3 years of diagnosis of AIDS, whichis the same as our estimate. The prospective Euro-
pean Collaborative Study21 estimated that 40% ofinfected children were in stage C by 4 years of age,and that 72% were alive at 5 years of age. Theseestimates are dose to our estimates of 40% in stage Cby 4 years of age and 75% alive at 5 years of age.However, they estimated that a higher proportion ofinfected children would be in stage C or dead by I
year of age, possibly because of a larger portion ofshort-term survivors in their study than in the PSDstudy.
In contrast, we found more rapid disease progres-sion in children when compared with a similarMarkov model performed in a cohort of adults.Longini et al9 estimated that adults remained asymp-tomatic for 4.4 years and AIDS developed after 9.8 to15 years.
In conclusion, Markov modeling using the re-vised pediatric classification system allowed us to
describe the natural history of HP/ disease in pen-natally HIV-infected children more comprehen-sively. Although considerable information hasbeen published on progression to AIDS and sur-vival, the results from the Markov model provideinformation on progression before diagnosis ofAIDS as well as the transition rates from each
stage. Furthermore, these estimates enhance theaccuracy and completeness of the description ofthe disease progression because they are based on
a larger population of children and have morecumulative follow-up times than found in previ-ously published clinical studies. In our population
with approximately 72% long-term survivors, chil-dren progress to moderate symptoms in the second
year of life and then remain moderately symptom-atic for more than half of their expected lives,
underscoring their need for clinical care before theonset of AIDS. The results have several important
benefits for clinicians and health care planners.First, they provide data that clinicians can use to
counsel families by predicting the age-specific din-ical course of HIV-infected children. Second, the
estimated times spent in each disease stage andprogression rates between stages assist clinical ne-
searchers in calculating sample sizes and accrualrates for clinical trials. Third, these estimates also
can be used to project future resource needs for
HIV-infected children.
ACKNOWLEDGMENTS
This research was supported by contracts and collaborativeagreements from the Division of HIV/AIDS at the US Centers forDisease Control and Prevention.
We thank Ira Longini, Scott Clark, and Glen Satten for helpfuldiscussions, John Lancaster for data assistance, and CatherineWilfert and R. J. Simons for their assistance in writing the manu-script.
Members of the Pediatric Spectrum of Disease Clinical Consor-tium:
Massachusetts: Principal Investigator, Ho-Wen Hsu, MD; Bay-state Medical Center, Barbara Stechenberg, MD; Boston Children’sHospital, Kenneth McIntosh, MD; Boston City Hospital, StephenPelton, MD; New England Medical Center, Cody Meissner, MD;Massachusetts Department of Social Services, Suzanne Tobin, RN;Massachusetts General Hospital, Mark Pasternack, MD; and Uni-versity of Massachusetts Medical Center, John Sullivan, MD.
Los Angeles: Principal Investigator, Laurene Mascola, MD; Ce-dars-Sinai Medical Center, Philip Brunell, MD; Harbor General-UCLA Medical Center, Carol Berkowitz, MD; Huntington Hospi-tal, Nadia Ewing, MD; Kaiser Permanent Medical Groups; LAC-USC Medical Center, Andrea Kovacs, MD; Los Angeles Children’sHospital, Joseph Church, MD; Martin Luther King Jr GeneralHospital, Steve Taylor, MD; Memorial Medical Center of LongBeach, Audra Deveilds, MD; and UCLA Medical Center, YvonneBryson, MD.
San Francisco: Principal Investigator, Yvonne Maldonado,MD; Children’s Hospital Medical Center of Northern Califor-nia, Ann Petru, MD; Santa Clara Valley Medical Center, Cathe-rine Albin, MD; Stanford University School of Medicine,Charles Prober, MD; and University of California San Francisco,Diane Wara, MD.
New York City: Principal Investigator, Pauline Thomas, MD;Albert Einstein College of Medicine, Arye Rubinstein, MD; Bronx-
Lebanon Hospital Center, Geniveve Lambert, MD; Bronx Mimic-ipal Hospital Center, Ruth Stein, MD; Harlem Hospital Center,Elaine Abrams, MD, and Susan Champion, MD; Kings County
Hospital, Herman Mendez, MD; Montefiore Medical Center andNorth Central Bronx Hospital Center, Nathan Litman, MD, andDonna Futterman, MD; SUNY-Health Science Center, Senih
Fikrig, MD; and The New York Hospital-Cornell Medical Center,Joseph Cervia, MD, and Margaret Hilgartner, MD.
Washington, DC: Principal Investigator, Robert Parrott, MD;Children’s National Medical Center, Tamara Rakusan, MD; DCGeneral Hospital, Yvette Reid, MD; and Howard University Hos-pital, Antoine Fomafod, MD.
Texas: Principal Investigator, Joann Schulte, MD; Baylor Col-lege of Medicine, Houston, Mark Kline, MD; Children’s MedicalCenter, Dallas, Janet Squires, MD; and University of Texas Health
Science Center, San Antonio, Terence Doran MD, PhD.Puerto Rico: Principal Investigator, Idith Ortiz, MD; Bayamon
Regional Medical Center, David Garcia-Trias, MD; Caguas Re-gional Hospital, Jose Vazquez Julia, MD; San Juan City Hospital,
Ingrid Mendez, MD; and University of Puerto Rico, ClementeDiaz, MD.
by guest on July 2, 2020www.aappublications.org/newsDownloaded from

APPENDIX REFERENCES
716 HI\’ PROGRESSION IN PERINATALLY INFECTED CHILDREN
Revised Pediatric Clinical Pediatric HIV Classification
Category N: Not Symptomatic
Children with no signs or symptoms considered theresult of HIV infection or with only one of the
conditions listed in category A.
Category A: Mildly Symptomatic
Children who have two or more of the conditionslisted below but none of the conditions listed in
categories B and C.
Lymphadenopathy (>0.5 cm at more than two sites;bilateral is considered one site);
Hepatomegaly;Splenomegaly;Dermatitis;
Panotitis; andRecurrent or persistent upper respiratory infection,
sinusitis, or otitis media.
Category B: Moderately Symptomatic
Children who have symptomatic conditions otherthan those listed for categories A and C that areattributed to HP/ infection. Examples of condi-
tions in clinical category B include, but are notlimited to:
Anemia (<8 g/dL), neutropenia (<1000/mm3), or
thrombocytopenia (<100 000/mm3) persisting for
more than 30 days;Bacterial meningitis, pneumonia, on sepsis (single
episode);Candidiasis, oropharyngeal (thrush), persistent (>2
months) in a child older than 6 months of age;Cardiomyopathy;Cytomegabovirus infection, with onset before I
month of age;Diarrhea, recurrent or chronic;Hepatitis;Herpes simplex virus stomatitis, recurrent (more
than two episodes within I year);Herpes simplex virus bronchitis, pneumonitis, on
esophagitis with onset before I month of age;Herpes zoster (shingles) involving at least two dis-
tinct episodes or more than one dermatome;Leiomyosarcoma;
LIP or pulmonary lymphoid hyperplasia complex;
Nephropathy;Nocardiosis;Persistent varicella zosten;Persistent fever for more than I month;Toxoplasmosis, onset before I month of age; andVaricella, disseminated (complicated chickenpox).
Category C: Severely Symptomatic
Children who have any condition listed in the 1987survefflance case definition for AIDS, with the ex-
ception of LIP.
1. Rogers MF, Thomas PA, Starcher ET, Noa MC, Bush fl, Jaffe HW.Acquired immunodeficiency syndrome in children: report of the Cen-
ters for Disease Control national survefflance, 1982 to 1985. Pediatrics.
1987;79:1008-1014
2. Scott GB, Hutto C, Makuch RW, et al. Survival in children with pen-
natally acquired human immunodeficiency virus type I infection. N
Engi I Med. 1989321:1791-1796
3. Tovo PA, de Martino M, Gabioano C, et al. Prognostic factors andsurvival in children with perinatal HIV-1 infection. Lancet. 1992;339:1249-1253
4. Centers for Disease Control and Prevention. Classification system for
human immunodeficiency virus (HP!) infection in children under 13
years of age. MMWR. 198736:225-235
5. Centers for Disease Control and Prevention. 1994 revised classification
system for HP! infected children (<13 years old). MMWR. 1994;43(RR-
12):1-10
6. Longini IM, Clark WS, Byers RH, et al. Statistical analysis of the
stages of HIV infection using a Markov model. Stat Med. 1989;8:
831-843
7. Longini IM, Jr. Clark WS, Gardner LI, Brundage JF. The dynamics of
CD4+ T-lymphocyte decline in HIV-infected individuals: a Markovmodeling approach. I Acquir Immune Defic Syndr Hum Refrovirol. 1991;
4:1141-1147
8. Longini IM, Jr. Clark WS, Karon JM. Effect of routine use of therapy in
slowing the clinical course of human immunodeficiency virus (HIV)
infection in a population-based cohort. Am I Epidemiol. 1992;137:
1229-1240
9. Longini IM, Jr. Byers RH, Hessol NA, Tan WY. Estimating the stage-
specific numbers of HP! infection using a Markov model and back-
calculation. Stat Med. 1992;11:831-843
10. Longini IM,Jr, Clark WS, Satten GA, Byers RH, KaronJ. Staged Markovmodels based on CD4+ T-lymphocytes for the natural history y of HIV
infection. In: Isham V, Medley G, eds. Models for Infectious Human
Diseases: Their Structure and Relation to Data. London: Cambridge Uni-versity Press; 1995:429-449
11. Gentleman R, Lawless JF, LindseyJC, Yan Y. Multi-state Markov mod-
els for analyzing incomplete disease history data with ifiustrations for
HIV disease. Stat Med. 1994;13:805-821
12. Gail MH. Evaluating serial cancer marker studies in patients at risk of
recurrent disease. Biometrics. 198137:67-78
13. Kay R. A Markov model for analyzing cancer markers and disease
states in survival studies. Biometrics. 1986;42:855-865
14. KalbfleischJD, Lawless LF, Voilmer NM. Estimation in Markov models
from aggregate data. Biometrics. 198339:907-919
15. Lagakos SW, Sommer CJ, Zelen M. Semi-Markov models for partially
censored data. Biometrika. 1978;65:311-317
16. Blanche 5, Rouzioux C, Moscato MLG, at al. A prospective study of
infants born to women seropositive for human immunodeflciency virus
type I. N Engi J Med. 1989320:1643-1648
17. Auger I, Thomas PA, de Gruttola V, et al. Incubation periods for
pediatric AIDS patients. Nature. 1988336:575-577
18. Blanche 5, Tardieu M, Duliege AM, at al. Longitudinal study of 94
symptomatic infants with perinatally acquired human immunodefi-
ciency virus infection: evidence for a bimodal expression of clinical and
biological symptoms. Am 1 Dis Child. 1990;144:1210-1215
19. Duliege AM, Messiah A, Blanche 5, Tardieu M, Griscelli C, Spira A.
Natural history of human immunodeficiency virus type I infection in
children: prognostic value of laboratory tests on the bimodal progres-
sion of the disease. Pediatr Infect Dis J. 1992;11:630-.635
20. Italian register for HIV infection in children. Features of children peri-
natally infected with HIV-1 surviving longer than 5 years. Lancet. 1994;
343:191-195
21. The European Collaborative Study. Natural history of vertically
acquired immunodeficiency virus-I infection. Pediatrics. 1994;94:
815-819
by guest on July 2, 2020www.aappublications.org/newsDownloaded from

1996;97;710Pediatrics Pediatric Spectrum of Disease Clinical Consortium
Ho-Wen Hsu, Joann Schulte, Robert Parrott, Yvonne Maldonado, Robert Byers and Huiman X. Barnhart, M. Blake Caldwell, Pauline Thomas, Laurene Mascola, Idith Ortiz,
Children: An Analysis From the Pediatric Spectrum of Disease ProjectNatural History of Human Immunodeficiency Virus Disease in Perinatally Infected
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/97/5/710including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlentirety can be found online at: Information about reproducing this article in parts (figures, tables) or in its
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 2, 2020www.aappublications.org/newsDownloaded from

1996;97;710Pediatrics Pediatric Spectrum of Disease Clinical Consortium
Ho-Wen Hsu, Joann Schulte, Robert Parrott, Yvonne Maldonado, Robert Byers and Huiman X. Barnhart, M. Blake Caldwell, Pauline Thomas, Laurene Mascola, Idith Ortiz,
Children: An Analysis From the Pediatric Spectrum of Disease ProjectNatural History of Human Immunodeficiency Virus Disease in Perinatally Infected
http://pediatrics.aappublications.org/content/97/5/710the World Wide Web at:
The online version of this article, along with updated information and services, is located on
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 1996 by thebeen published continuously since 1948. Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
by guest on July 2, 2020www.aappublications.org/newsDownloaded from