Embed Size (px)
Citation preview

Technical Appendix
National Theatres ProjectReportNovember 2006
© Crown copyright 2007
This document is also available on the Scottish Executive website:www.scotland.gov.uk
Astron B49732 1/07
Further copies are available fromBlackwell’s Bookshop53 South BridgeEdinburghEH1 1YS
Telephone orders and enquiries0131 622 8283 or 0131 622 8258
Fax orders0131 557 8149
Email [email protected]

Scottish Executive, Edinburgh 2007
Technical Appendix
National Theatres ProjectReportNovember 2006

National Theatres Projectii
© Crown copyright 2007
ISBN: 978-0-7559-5322-6
Scottish ExecutiveSt Andrew’s HouseEdinburghEH1 3DG
Produced for the Scottish Executive by Astron B49732 1-07
Published by the Scottish Executive, January 2007
Further copies are available fromBlackwell’s Bookshop53 South BridgeEdinburghEH1 1YS
The text pages of this document are printed on recycled paper and are 100% recyclable

Contents
INTRODUCTION 2
APPENDIX A: Glossary and Definitions 4
APPENDIX B: Balanced Scorecard 19
APPENDIX C: Mandatory Scorecard 22
APPENDIX D: Measure Definitions 23
APPENDIX E: Reporting Framework 25
APPENDIX F: Pilot Management Reports 26
APPENDIX G: Pilot Scorecard 29
APPENDIX H: Pilot Analysis - Hours Breakdown 30
APPENDIX I: Pilot Analysis - Session Duration 31
APPENDIX J: Pilot Analysis - Patient Pathway 32
APPENDIX K: Pilot Analysis - Surgical & Anaesthetic Times 33
APPENDIX L: Capability Scoping 35
APPENDIX M: Capability Template 45
Contents 1

National Theatres Project2
Introduction
The objective of the National Theatres Project (NTP)is to achieve Best Value for theatre services byappropriately increasing patient throughput, therebyusing resources more productively and efficiently.
The purpose of this Technical Appendix is to providefurther detail to the main report on the project workundertaken and to give examples of analysis andinvestigation of findings from the use of the balancedscorecard approach to comparative performance.
Summary of Supporting InformationIn June 2005 the National Theatres Project agreedthe following activities with the NationalBenchmarking Project Board:
• a national theatres glossary with agreed definitionsto be drawn up and implemented
• a minimum standard dataset to be agreed acrossScotland
• development of routes for ensuring localaccountability
• evaluation of existing/available theatre systems.
Glossary and Definitions
A draft Glossary and Definitions was produced inconjunction with the Service. Where there wasalready agreement from existing national bodies onspecific definitions, these were incorporated. Whereno such agreement existed, definitions were agreedby a wide group of theatre users and wherenecessary amended following consultation (nationalevents and Board visits).
This draft was progressed through the NationalClinical Dataset Development Programme Board andhas been subject to a full formal consultation processwith a view to implementation in 2007.
A summary of terms and definitions appears asAppendix A.
Minimum Dataset
A National Data Points Day was held in August 2005with stakeholders from across the Service todetermine the information required in order tomanage theatres effectively. A theatre servicesbalanced scorecard which covers strategic andoperational indicators was produced from the outputof the day. This scorecard has been subsequentlyrefined and further developed with a focus on patientoutcomes and clinical governance matters with awide range of Service input from across Scotland.
The latest draft balanced scorecard, and some noteson the potential application of the balancedscorecard in a theatres context can be found inAppendix B.
A subset of these indicators have been proposed asmandatory national indicators to be collected byBoards from 2007/08 onwards. These are shown inAppendix C, while Appendix D provides moredetailed definitions of the measures.
Scorecard Pilots
Following development of the balanced scorecard,two pilot implementations tested:
• the use of the balanced scorecard to monitor andmanage continuous improvement in theatres
• accountability and responsibility structures toachieve ownership and control of the theatrecapacity and improvement in theatre services.
Appendix E shows an outline reporting framework,and examples of the management reports developedduring the pilots can be found in Appendix F.
Data from the pilots was used to populate thebalanced scorecard as far as possible. Thispopulated scorecard forms Appendix G. Where datacould be extracted from an existing theatre system,much of the scorecard could be populated with

Introduction 3
relative ease. Where a manual system was in place itwas not possible to populate as much of thescorecard. Accordingly two full pilot site scorecardcomparisons were not able to be generated as onlyone site had a comprehensive electronic theatresystem with the other pilot site providing manualreturns for pilot reporting.
Following completion of the pilots, the data collectedwas analysed and effective ways of representing thisinformation were explored. Appendices H to Killustrate these.
Capability Scoping
During March to July 2006 visits were made to allmainland Health Boards. The purpose of these was to:
• carry out a detailed assessment of currentlyavailable local theatres information
• evaluate existing theatres system implementations
• validate and assess nationally collected theatresdata
• seek Board input to the National Theatres Projectand balanced scorecard development
• communicate the purpose and objectives of theNational Theatres Project to Health Boards andinterested staff.
The detailed findings from the capability scopingare contained in Appendix L and the templateused to structure the visits can be found inAppendix M.

National Theatres Project4
GENERIC DATA ITEMS
CHI Number The Community Health Index (CHI) is a population register, which is used in Scotland for
health care purposes. The CHI number uniquely identifies a person on the index.
Person Birth Date The date on which a person was born or is officially deemed to have been born, as
recorded on the Birth Certificate.
Associated Associated Professionals are those individuals who are involved with the client/patient in
Professionals a professional capacity, e.g. consultant, social worker, occupational therapist, etc.
Associated The recognised professional group to which the care professional belongs and in which
Professional Group they are employed.
Health Record A Patient Health Record Identifier is a code (set of characters) used to uniquely identify a
Identifier patient within a health register or a health records system, e.g. PAS.
APPENDIX A: Glossary and Definitions
Operating Theatres Data Standards
PATIENT DETAILS
ASA status The ASA PS classification globally assesses the degree of “sickness” or “physical state”
prior to selecting the anaesthetic or prior to performing surgery.
Code P1: A normal healthy patient.
Code P2: A patient with mild systemic disease.
Code P3: A patient with severe systemic disease.
Code P4: A patient with severe systemic disease that is a constant threat to life.
Code P5: A moribund patient who is not expected to survive without the operation.
Code P6: A declared brain-dead patient whose organs are being removed for donor
purposes.

Appendix A: Glossary and Definitions 5
PATIENT DETAILS (Contd)
NCEPOD category NCEPOD classification categorizes the urgency of the patient’s intervention.
Code 01: Immediate: Life, limb or organ saving intervention. Resuscitation simultaneous
with surgical treatment. The target time to theatre is within minutes of decision taken to
operate. E.g. Rupture aortic aneurysm, major trauma to abdomen or thorax, fracture with
major neurovascular deficit, etc.
Code 02: Urgent: Acute onset or deterioration of conditions that threaten life, limb or
organ survival.
Sub code A: Intervention within 6 hours: the target time to theatre is within
6 hours of decision to operate and normally once resuscitation is complete.
Sub code B: Intervention within 24 hours: the target time to theatre is within
24 hours of decision to operate and normally once resuscitation is complete.
Code 03: Expedited: Stable patient requiring early intervention for a condition that is not
an immediate threat to life, limb or organ survival. Target time to theatre is within days of
decision to operate.
Code 04: Elective: Surgical procedure planned or booked in advance of routine
admission to hospital. Target time to theatre is planned. Encompasses all conditions not
classified as immediate, urgent or expedited.

National Theatres Project6
OPERATING ENVIRONMENT
Operating room type The type and setting of the room in a hospital where an interventional procedure
codeable in OPCS4 takes place.
Code 01: Category 1: Main theatre suite Sub code A: Operating theatre
Sub code B: Anaesthetic room
Sub code C: Recovery room
Sub code D: Procedure room
Code 02: Category 2: Sub code A: Satellite or isolated theatre
Sub code B: Day theatres
Code 03: Category 3: Sub code A: Endoscopy Suite
Sub code B: Radiology
Sub code C: Cardiac Catheterisation Lab
Sub code D: Procedure room
Sub code E: Pain clinic
Code 04: Category 4: Sub code A: ICU
Sub code B: A & E
Sub code C: Wards
Code 98: Other: Any other location not included in the above.
Operating session type The type of period of operating time allocated to a consultant.
Code 01: Scheduled:
Sub code A: Planned: Periods of theatre time allocated to a consultant,
usually on a regular basis, in which the consultant or a member of the firm
can perform operations, the majority of which have been arranged
beforehand. The maximum duration of a scheduled session is a notional
half-day.
Sub code B: Emergency: Periods of time allocated to a consultant on a
regular basis for patients whose visit to the operating theatre were not
foreseen but take place as a result of illness or a complication requiring an
urgent operation. The maximum duration of a scheduled session is a notional
half-day, e.g. trauma sessions/sessions sometimes locally known as CEPOD
sessions.
Code 02: Unscheduled: Periods of time allocated to one or more consultants outside
scheduled sessions allocated to a consultant and used by that consultant or one of the
same main specialty, for specific Theatre Case, usually at short notice.
Operating list type The type of published list, which consists of a set of patients who are to be operated on
in a session. The list documents the patients and the details of their impending operation.
Code 01: Elective: An operating list that comprises solely elective cases.
Code 02: Emergency: An operating list that comprises solely emergency cases.

Appendix A: Glossary and Definitions 7
OPERATING ENVIRONMENT (Contd.)
Specialty of session The specialty of the consultant to whom the operating session has been allocated.
A specialty is defined as a division of medicine or dentistry covering a specific area of
clinical activity and identified within one of the Royal Colleges or Faculties.
Code A1: General Medicine
Code A2: Cardiology
Code A7: Dermatology
Code A9: Gastroenterology
Code AA: Genitourinary Medicine
Code AM: Palliative Medicine
Code AQ: Respiratory Medicine
Code C1: General Surgery
Code C12: Vascular Surgery
Code C3: Anaesthetics
Code C4: Cardiothoracic Surgery
Code C41: Cardiac Surgery
Code C42: Thoracic Surgery
Code C5: Ear, Nose & Throat
Code C6: Neurosurgery
Code C7: Ophthalmology
Code C8: Trauma and Orthopaedics
Code C9: Plastic Surgery
Code CA: Paediatric Surgery
Code CB: Urology
Code D3: Oral Surgery
Code F2: Gynaecology
Code F3: Obstetrics
Code G1: General Psychiatry
Code H1: Clinical Radiology
Code R11: Surgical Podiatry
Code 98: Other, specify
To be determined, no existing codes at present:Dental Surgery
Maxillofacial
Interventional Radiology

National Theatres Project8
OPERATING ENVIRONMENT (Contd.)
Operating hours The hours during which the procedure was performed.
Code 01: Office hours: 08:00 hrs to 17:59 hrs Monday to Friday.
Code 02: Out of hours: 18:00 hrs to 07:59 hrs Monday to Friday and all day Saturday
and Sunday.
Time of day/night The period during which the procedure was carried out.
Code 01: Daytime: 08:00 – 17:59 hours.
Code 02: Evening: 18:00 – 23:59 hours.
Code 03: Night: 00:00 – 07:59 hours.
Operating times The combined date and time of an event.
Allocated start time of list/session: Time when the anaesthetist is scheduled to take
charge of the (first) patient in preparation for anaesthesia.
Actual start time of list/session: Time when the anaesthetist actually takes charge of the
(first) patient in preparation for anaesthesia.
Allocated finish time of list/session: The time when the anaesthetist is scheduled to hand
over the care of the last patient to recovery staff.
Actual finish time of list/session: The time when the anaesthetist actually hands over the
care of the last patient to recovery staff.
Sub-data items - adapted from the National Theatres Project:
Planned hours of list/session: The difference between the allocated start time of
list/session and allocated finish time of list/session.
List run time: The time difference between the actual list/session start time and the actual
list/session finish time.
List under run: When the list run time is less than the planned hours of list/session. The
term, as used in the Acute Hospital Portfolio, does not necessarily mean the list finished
early, as it might have started late.
List over run: When the list run time exceeds the planned hours of list/session. The term,
as used in the Acute Hospital Portfolio, does not necessarily mean the list finished late,
as it might have started early.

Appendix A: Glossary and Definitions 9
OPERATING ENVIRONMENT (Contd.)
Reason for An explanation of why an operating list or session did not take place as planned.
cancellation of Code 01: Public holidaylist/session Code 02: Cancelled by surgeon/main operator: Sub code A: Planned leave
Sub code B: Sick leave
Sub code C: On call
Sub code Z: Other reason
Code 03: Cancelled by anaesthetic department: Sub code A: Planned leave
Sub code B: Sick leave
Sub code C: Skill mix
Sub code Z: Other reason
Code 04: Theatre Staff: Sub code A: Sick leave
Sub code B: Skill mix
Sub code Z: Other
Code 05: Training/Continuing Professional Development
Code 06: Maintenance
Code 07: Equipment failure/unavailable
Code 08: Administrative error
Code 09: No ward beds
Code 10: No High Dependency Unit beds available
Code 11: No Intensive Care Unit beds available
Code 98: Other reason for cancellation
Code 99: Not known
Reason for late start An explanation for the theatre list/session starting later than its allocated start.
of list/session Late start: When the actual start time of list/session is later than the allocated start time
of list/session.
Code 01: Porter not available
Code 02: Patient arrived late to hospital
Code 03: Patient not fasted
Code 04: Patient not ready in ward
Code 05: Patient not consented
Code 06: Staff not available to accompany the patient
Code 07: Investigations or x-rays missing
Code 08: Blood not available
Code 09: Intrusion of other specialty or emergency
Code 10: Anaesthetist delayed

National Theatres Project10
OPERATING ENVIRONMENT (Contd.)
Reason for late startof list/session Code 11: Surgeon/main operator delayed
(Contd.) Code 12: Theatre staff delayed
Code 13: Anaesthetic assistant delayed
Code 14: Theatre not adequately staffed
Code 15: Theatre not ready
Code 16: Equipment failure/unavailable
Code 98: Other
Code 99: Not known
Reason for late finish An explanation for the list finishing later than its allocated finish time.
of list/session Late finish: When the actual finish time of list/session is later than the allocated
finish time of list/session.
Code 01: Late start of list/session
Code 02: Unexpectedly difficult procedure
Code 03: Difficult or unexpected anaesthetic problem
Code 04: Intrusion of other specialty
Code 05: Intrusion of other emergency
Code 06: Delayed availability of recovery facilities
Code 07: Delayed availability of High Dependency Unit facilities
Code 08: Delayed availability of Intensive Care Unit facilities
Code 09: List overbooked
Code 10: Equipment failure/unavailable
Code 98: Other
Code 99: Not known

Appendix A: Glossary and Definitions 11
THEATRE PROCESSES AND OPERATIVE PROCEDURES
Specialty of procedure The specialty of the consultant who is responsible for the patient’s care. A specialty is
defined as a division of medicine or dentistry covering a specific area of clinical activity
and identified within one of the Royal Colleges or Faculties.
Code A1: General Medicine
Code A2: Cardiology
Code A7: Dermatology
Code A9: Gastroenterology
Code AA: Genitourinary Medicine
Code AM: Palliative Medicine
Code AQ: Respiratory Medicine
Code C1: General Surgery
Code C12: Vascular Surgery
Code C3: Anaesthetics
Code C4: Cardiothoracic Surgery
Code C41: Cardiac Surgery
Code C42: Thoracic Surgery
Code C5: Ear, Nose & Throat
Code C6: Neurosurgery
Code C7: Ophthalmology
Code C8: Trauma and Orthopaedics
Code C9: Plastic Surgery
Code CA: Paediatric Surgery
Code CB: Urology
Code D3: Oral Surgery
Code F2: Gynaecology
Code F3: Obstetrics
Code G1: General Psychiatry
Code H1: Clinical Radiology
Code R11: Surgical Podiatry
Code 98: Other, specify
To be determined, no existing codes at present:Dental Surgery
Maxillofacial
Interventional Radiology

National Theatres Project12
THEATRE PROCESSES AND OPERATIVE PROCEDURES (Contd.)
Type of theatre case An indication of the type of patient visit to the operating theatre to undergo one or more
operative procedures.
Code 01: Scheduled: Includes scheduled or elective cases where the operation was
planned in advance.
Code 02: Unscheduled: Where the operation was unexpected or could not be planned
in advance.
Sub code A: Emergency
Sub code B: Revisit to theatre: When it was necessary for the patient to be
referred to theatre for a further operation/procedure as a result of
complication(s) related to a previous operation/procedure undertaken during
the same episode of care.
Management intent Whether or not the patient's attending clinician expects, at the time of booking, that the
patient will be admitted and discharged on the same calendar day, or discharged on a
subsequent date.
Code 00: None: Where no decision has been taken.
Code 01: Inpatient: Where the patient is expected to be discharged on a subsequent
date following the procedure.
Code 02: Day case: Where the patient is expected to be discharged on the same
calendar day after the procedure.
Code 03: Extended recovery: Where patients are admitted, operated on and stay for one
night post-operatively in a hospital facility (overall stay up to 23 hours). (International
Association for Ambulatory Surgery.)
Code 99: Not known.
Dates and times of The combined date and time of an event.
theatre processes Date and time of booking: The combined date and time at which the theatre team were
and operative notified that the patient required a procedure in theatre.
procedures Time patient sent for: The time that the theatre team sent the request for the patient to
be brought to the operating theatre department.
Time patient arrived in theatre premises: The time that the patient actually arrived in the
operating theatre premises.
Time into anaesthetic room: The time at which the patient was brought into the
anaesthetic room.
Start time of anaesthesia: The time of start of the anaesthetic procedure where this takes
place either in the operating theatre or in the anaesthetic room.
Time into theatre: The time at which the patient is transferred from the anaesthetic room
into theatre.
Start time of procedure: The time of commencement of the procedure regardless of
whether an anaesthetic is given or not. This should be ‘knife to skin’ or equivalent.
It does not include positioning, with the exception of manipulation of fractures.

Appendix A: Glossary and Definitions 13
THEATRE PROCESSES AND OPERATIVE PROCEDURES (Contd.)
Dates and times of Finish time of procedure: The time at which the procedure was finished and any
theatre processes dressings applied.
and operative Time patient entered recovery: The time at which the patient was transferred into the
procedures (Contd.) recovery area.
Time patient ready to leave recovery: The time at which the patient was assessed as
meeting the discharge criteria of the recovery room.
Time patient actually left recovery: The time at which the patient actually left the recovery room.
Operative procedure An indication of whether or not the intended operative procedure was performed.
performed indicator Code 01: Procedure performed.
Code 02: Patient anaesthetised but procedure not performed.
Code 03: Procedure cancelled.
Code 99: Not known.
Reason operative An explanation for an operative procedure not having taken place as planned.procedure not Code 01: Secretarial error.performed Code 02: Cancelled by patient:
Sub code A: Unable to attend
Sub code B: No longer wishes procedure
Sub code C: Did not attend – reason not known
Sub code Z: Other
Code 03: Cancelled by surgeon/main operator:
Sub code A: procedure not required
Sub code B: Patient not prepared
Sub code C: Surgeon/main operator not available
Sub code Z: Other
Code 04: Cancelled by anaesthetist:
Sub code A: Patient not fit
Sub code B: Patient not prepared
Sub code C: Anaesthetist not available (Sickness)
Sub code D: Anaesthetist not available (Skill mix)
Sub code Z: Other

National Theatres Project14
THEATRE PROCESSES AND OPERATIVE PROCEDURES (Contd.)
Reason operative Code 05: Cancelled by theatre management:
procedure not Sub code A: Staff not available (Sickness)
performed (Contd.) Sub code B: Staff not available (Skill mix)
Sub code C: Equipment not available
Sub code D: Intervention by emergency case
Sub code E: Intervention by priority case
Sub code F: Lack of theatre time
Sub code Z: Other
Code 06: Cancelled by hospital:
Sub code A: No ward bed bed available
Sub code C: No Intensive Care Unit bed available
Sub code D: Administrative error
Sub code Z: Other
Code 07: Preoperative guidance not followed.
Code 98: Other reason for cancellation.
Code 99: Not known.

Appendix A: Glossary and Definitions 15
HEALTHCARE PROFESSIONALS
Associated An indication of the role carried out by each professional. Professionals are those
Professional Role individuals who are involved with the client/patient in a professional capacity.
(Operating theatres)Code 01: Consultant responsible for care: Consultant who carries clinical responsibility
for a patient’s healthcare during an episode.
Code 02: Operating surgeon/main operator (Main operating clinician): Clinician
performing the procedure.
Code 03: Surgical first assistant (First operating assistant): An individual who assists
the operating surgeon in performing the procedure.
Code 04: Assistant surgeon (Additional operating assistant): Any other individual (in
addition to the first assistant) who assists the operating surgeon/clinician in
performing the procedure.
Code 05: Supervising surgeon/clinician: Surgeon/clinician supervising the procedure.
Code 06: Main anaesthetist: Medical practitioner responsible for the administration of
anaesthesia/sedation.
Code 07: Assistant anaesthetist: Medical practitioner assisting the main anaesthetist in
the administration of anaesthesia/sedation.
Sub Code A: Medical practitioner
Sub Code B: Non-medical practitioner
Code 08: Supervising anaesthetist: Anaesthetist supervising the anaesthetic procedure.
Code 09: Anaesthetic assistant: Non-medical person assisting the anaesthetist(s) in
the administration of anaesthesia/sedation.
Code 10: Scrub practitioner: Registered practitioner responsible for the preparation
and handling of instrumentation, swabs, needles, etc. during a surgical
procedure.
Code 11: Circulating practitioner: Practitioner assisting the scrub practitioner.
Code 12: Recovery room practitioner: Registered practitioner responsible for care of
patient during recovery from procedure.
Code 13: Radiographer
Code 98: Other: Includes medical and nursing students, medical trainees, medical
representatives, AHP trainees or any other observers.

National Theatres Project16
HEALTHCARE PROFESSIONALS (Contd.)
Associated The grade of the associated professional in the operating theatre.
Professional Grade(Operating theatres) Attributes: Associated Professional Status - Permanent
Locum
Temporary
Agency
Bank
Code 01: Consultant
Code 02: Associate Specialist
Code 03: Staff Grade
Code 04: Seamless training grade
Sub code A: Year 1
Sub code B: Year 2
Sub code C: Year 3
Sub code D: Year 4
Sub code E: Year 5
Sub code F: Year 6
Sub code G: Year 7
Sub code H: Year 8
Code 05: Specialist Registrar year 1-4
Code 06: Senior House Officer
Code 07: Foundation Year 2 (Senior House Officer 1)
Code 08: Foundation Year 1 (Pre-Registration House Officer)
Code 09: Nurse: bands 2-8
Code 10: Operating Department Practitioner
Code 11: Operating Department Assistant
Code 12: Physicians assistant - anaesthesia
Code 13: Surgical Practitioner
Code 98: Other
Level of surgical/ Where a non-consultant is involved this indicates the level of supervision in place and
clinical supervision the location or whereabouts of the supervising consultant/clinician.
Code 00: No supervision
Code 01: Operating room environment:
Sub code A: Present in operating room - Scrubbed
Sub code B: Present in operating room - Not scrubbed
Sub code C: In operating department but not in operating room
Code 02: Office
Code 03: Home
Code 98: Other

Appendix A: Glossary and Definitions 17
HEALTHCARE PROFESSIONALS (Contd.)
Level of anaesthetic Where a non-consultant is involved this indicates the level of supervision in place and
supervision the location or whereabouts of the supervising consultant anaesthetist.
Code 00: No supervision
Code 01: Operating room environment:
Sub code A: Present in operating room
Sub code B: In operating department but not in operating room
Code 02: Office
Code 03: Home
Code 98: Other
SOURCE AND DESTINATION PATIENT
Source of admission The originating location within the hospital from where the patient was brought to theatre.
to operating theatreCode 01: Inpatient ward: Local identifiers may include ward numbers, names, etc.
Code 02: Day bed unit
Code 03: Emergency care unit
Code 04: A&E
Code 05: High Dependency Unit
Code 06: Intensive Care Unit: Synonyms include Critical Care Unit (Adult/Paediatric),
Intensive Therapy Unit, etc.
Code 07: Admissions unit
Code 98: Other source
Intended destination The planned or intended location to which the patient is to be sent from the operating
from operating theatre/recovery area.
theatre/recoveryCode 01: Inpatient ward: Local identifiers may include ward numbers, names etc.
Code 02: Day bed unit
Code 03: Emergency care unit
Code 04: Extended recovery unit: Where patients are admitted, operated on and stay for
one night post-operatively in a hospital facility (overall stay up to 23 hours). (International
Association for Ambulatory Surgery.)
Code 05: High Dependency Unit
Code 06: Intensive Care Unit: Synonyms include Critical Care Unit (Adult/Paediatric),
Intensive Therapy Unit, etc.
Code 07: Transfer to other hospital
Code 08: Home
Code 98: Other destination

National Theatres Project18
SOURCE AND DESTINATION PATIENT (Contd.)
Actual destination The actual location to which the patient was sent from the operating theatre/recovery.
from operatingtheatre/recovery Code 01: Inpatient ward: Local identifiers may include ward numbers, names, etc.
Code 02: Day bed unit
Code 03: Emergency care unit
Code 04: Extended recovery unit: Where patients are admitted, operated on and stay for
one night post-operatively in a hospital facility (overall stay up to 23 hours). (International
Association for Ambulatory Surgery.)
Code 05: High Dependency Unit
Code 06: Intensive Care Unit: Synonyms include Critical Care Unit (Adult/Paediatric),
Intensive Therapy Unit, etc.
Code 07: Transfer to other hospital
Code 08: Home
Code 09: Mortuary
Code 98: Other destination

Appendix B 19
National• Cost of idle capacity• Direct cost per case (case mix adjusted)• Total cost per head population (adjusted for
cross-boundary flow) and by theatre level
LocalFinancial measures are currently thought to be lessuseful at local level
Financial
National• Deaths• Cancellations
Local• Cancellations• Complaints• Resource unavailability• Deaths• Critical Care• Time in recovery• Risk management episodes• Length of stay outliers• Surgical re-admissions• Waiting list efficiency ratio• Theatre delays• Re-operation within the same admission• Sickness abscence• % emergency procedures at night
Patient/Quality
National• Surgical theatre hours• Anaesthetic theatre hours• Downtime• Utilisation• Case-mix adjusted throughout• Elective/non-elective mix
Local• Available theatre time• Allocated theatre hours• Actual theatre hours• Procedural theatre hours• Surgical theatre hours• Anaesthetic theatre hours• Turnover time• Case-mix adjusted throughput• Elective/non-elective mix• Over-runs• Under-runs• Late-starts• Cancelled sessions• Delayed discharges (from Recovery)
Efficiency
National• Information capture
Local• Theatre staff compliance ratio• Development of new ways of working• PDPs (learning/development)• Utilisation of theatre information• Level of dataset capture• Role within capacity planning• Level of supervised training procedures• Level of unsupervised training procedures
Future/Capability
APPENDIX B: Balanced ScorecardNational Theatres Project – Balanced Scorecard3rd October 2006

National Theatres Project20
A balanced scorecard can be produced for each(elliptical) interface on the diagram. As the scorecardbecomes more high level the level of detail and arequirement for individual identifiers becomes less.
1) At an individual level the scorecard should collateall the procedures carried out by one individual(nurse, surgeon or anaesthetist) to populate theindividual’s personal dataset. This information shouldbe in a format using the definitions for the nationaldataset and be exportable to existing operation logs,the scorecard forming the event log for the individual.Colleges (Anaesthesia and Surgical) have alreadydefined formats and datasets for these reports towhich can be added data about theatre utilisation,start, finish times, etc. from the collated personaldata. By providing feedback on the dataset availablethis will encourage local ownership and verificationthus ensuring buy-in and data quality at a local level.The information can be validated through use in theappraisal process and link in to any national auditprocesses. By incorporating all the items from thenational scorecard (and any specialty standards) theindividual will be able to set their performance incontext. This is key to any working system.
2) The theatre level scorecard will collate all datafor that theatre. This dataset will contain moremanagerial factors (start and finish times,utilisation, etc.) and will be used to managetheatre capacity. A typical dataset for managerialpurposes can be derived from the nationaltheatres audits by the Audit Commission andadvice and rules to utilise the data arising can befound in these reports. The top-level informationon utilisation, etc. can be used to comparetheatres within the suite.
3) The hospital level scorecard takes all of theindividual theatre datasets and distils the datatowards the Board dataset. In performing thisprocess local comparisons on critical incidents andperformance can be used to change practice locallyat an early stage if necessary.
4) The Board level scorecard has progressivelyfewer indicators however the basis of the scorecardis the detail contained in the local scorecards. Anyoutlying information can be tracked through thesystem.
Individual
Hospital
Board
Scotland
BoardScorecard
HospitalScorecard
TheatreScorecard
Individual Event Log(Nurse, Surgeon,Anaesthetist)
Specific condition/procedure review and standardSpecific
Condition/Operation
Application of the Balanced Scorecard

Appendix B 21
5) At a national level it is important that theinformation is easily understood by the public (whowill be seeking reassurance that the system isworking safely and efficiently) and is concise.Comparison of the Board data at a national level willset the standard for Scotland.
It is clear from previous attempts to produce a globalfigure for theatre activity that it is very case-mixdependant. Case-mix adjustment is complex and notalways accurate. Efficiency figures should beapplicable across the board and quality measuresunequivocal.
To provide performance data for individual specialtydepartments it is suggested that relevant professionaladvisory groups be asked to produce a basket ofprocedures that occur in sufficient numbers and haveconsistent profiles of care in terms of length ofanaesthetic, operation, grade of surgeon andanaesthetist, outcome and at a Board level populationbased incidence of procedure. This approach hasbeen in place and is successful for hip fractures.
Each specialty should identify one major procedureand one day case procedure together with a further“developing” procedure.

National Theatres Project22
Mandatory Indicators
Opportunity cost of unused hours
Comparative cost of theatres activity
Financial
Risk management episodes
Surgical re-admissions
Theatre delays
Cancellations
Deaths/10,000 patients
% emergency procedures at night
Patient/Quality
Unutilised hours/Allocated hours
Over-runs/Allocated hours
Under-runs/Allocated hours
Procedural time/Actual hours
Operative time/Allocated hours
% cancelled sessions
Late start hours/Allocated hours
% emergency cases in planned sessions
Efficiency
Information quality
% dataset captured
Use of theatres information
Development of new ways of working
Future/Capability
APPENDIX C: Mandatory Scorecard

Appendix D: Measure Definitions 23
The contents of the square brackets within the textcross-reference these definitions with Appendix A.
Opportunity cost of unused hours: the costassociated with the number of patients who couldhave been operated upon during unutilised time:unutilised hours divided by 3.5, multiplied by theaverage number of patients per session for theBoard, multiplied by the average cost per patient.
Comparative cost of theatres activity: Cost pertheatre hour.
Allocated hours: total theatre time allocated to eachsession holder and specialty. Allocated hours are thedifference between the session allocated start timeand the session allocated finish time [Operatingtimes].
Unutilised hours: the difference between allocatedhours and actual hours as a percentage of allocatedhours. Actual hours are the difference between thesession actual start time and the session actual finishtime [Operating times].
Over-runs: the number of over-run hours as apercentage of allocated hours. An over-run occurswhen the actual session length exceeds the plannedsession length [Operating times]. Only over-runs ofmore than 30 minutes will be included.
Under-runs: the number of under-run hours as apercentage of allocated hours. An under-run occurswhen the planned session length exceeds actualsession length [Operating times]. Only under-runs ofmore than 45 minutes will be included.
Procedural time: procedural hours are the time fromstart of anaesthetic to time of exiting the operatingroom [Dates and times of theatre processes andoperative procedures].
Operative time: the difference between the starttime of the procedure and the finish time of theprocedure [Dates and times of theatre processes andoperative procedures].
Cancelled sessions: the percentage of allocatedsessions unused due to cancellation by the holder[Reason for cancellation of list/session].
Late starts: the number of hours lost due to latestarts as a percentage of allocated hours. A late startoccurs when the list actual start time exceeds theplanned start time [Reason for late start oflist/session]. Only late starts of more than 5 minuteswill be included.
Emergency cases: the number of emergency cases[NCEPOD category: 01, 02] carried out withinplanned sessions as a percentage of the totalnumber of cases carried out within planned sessions[Operating session type: 01A].
Risk management episodes: the number of riskmanagement episodes per 1000 procedures.
Surgical re-admissions: the number of surgicalpatients re-admitted for surgery within 28 days as apercentage of total number of patients.
Theatre delays: the average number of minutes lostper session due to delays, e.g. no porter, patient notready. Only delays of more than 5 minutes will beincluded.
Cancellations: percentage of elective patientswhose procedure is cancelled within 10 working daysof due date for operation [Reason operativeprocedure not performed].
Deaths: the number of deaths in theatre per 10,000patients [Actual destination from operating theatre/recovery: 09].
APPENDIX D: Measure Definitions

National Theatres Project24
% emergency procedures at night: thepercentage of emergency [NCEPOD category: 01,02] procedures carried out between 00:00 and 07:59[Time of day/night].
Information quality: an assessment High, Mediumor Low of the quality of theatres information available.The criteria for assessment are shown in sections5.3, 5.4 and 5.5 of the main report.
Dataset capture: the proportion of the mandatoryindicators available.
Use of theatre information: an assessment High,Medium or Low as to the effective use of theatresinformation.
New ways of working: an assessment High,Medium or Low as to the degree of innovation andextent to which new ways of working are beingadopted. The criteria for assessment are shown insection 5.7 of the main report.
It is proposed to further develop and test RiskManagement and Quality Assurance measuresthrough the National Theatres Implementation Group(NTIG). This work will also include development oftraining measures:
Supervised training: the number of supervisedtraining procedures carried out as a percentage oftotal procedures. A supervised training procedureoccurs when the main operator [Associatedprofessional role: 02] is a trainee [Associatedprofessional grade: 04-06], and a consultant[Associated professional grade: 01] is present –scrubbed or not scrubbed [Level of surgical/clinicalsupervision: 01/A or 01/B].
Unsupervised training: the number ofunsupervised training procedures carried out as apercentage of total procedures. An unsupervisedtraining procedure occurs when the main operator[Associated professional role: 02] is a trainee[Associated professional grade: 04-06], and there isno consultant present [Level of surgical/clinicalsupervision: neither 01/A nor 01/B].
Efficiency and Patient/Quality indicators will bereported at session holder, specialty, hospitaland Board level. Indicators will be reported forscheduled (planned and emergency) andunscheduled sessions.
NTIG will produce a detailed specification foreach of the above measures prior tocommencement of data collection.

Appendix E: Reporting Framework 25A
PP
EN
DIX
E:R
epo
rtin
gF
ram
ewo
rk
By
Boa
rd/S
ite/T
heat
reTy
pe/T
eam
/Indi
vidu
al/C
linic
ian
Thea
tres
Vari
ance
Sp
ecia
lty
Vari
ance
Ana
lysi
s
Pro
ced
ural
Vari
ance
-C
ompa
rativ
eco
stof
thea
tres
activ
ity
-O
ppor
tuni
tyco
stof
unus
edho
urs
Cos
t
Mix
Volu
me
Cos
t
Pat
ient
Volu
me
-U
nutil
ised
hour
s/A
lloca
ted
hour
s-
Late
star
thou
rs/A
lloca
ted
hour
s-
%C
ance
lled
sess
ions
-Tu
rnov
ertim
e-
Ope
rativ
etim
e-
Ove
r-ru
ns/A
lloca
ted
hour
s-
Und
er-r
uns/
Allo
cate
dho
urs
-%
Em
erge
ncy
case
sin
plan
ned
sess
ions
-P
roce
dura
ltim
e-
Ana
esth
etic
time
-O
pera
tive
time
-Tu
rnov
ertim
e-
Rec
over
ytim
e
-P
roce
dura
ltim
e-
Ana
esth
etic
time
-O
pera
tive
time
-Tu
rnov
ertim
e-
Rec
over
ytim
e
-D
eath
spe
r10
,000
patie
nts
-C
ance
llatio
ns-
Thea
tre
dela
ys-
Sur
gica
lre-
adm
issi
ons
-R
isk
man
agem
ente
piso
des
-%
emer
genc
ypr
oced
ures
atni
ght
As
Leve
l1-
Dea
ths
per
10,0
00pa
tient
s-
Re-
adm
issi
ons
-R
isk
man
agem
ente
piso
des
-In
form
atio
nqu
ality
-%
data
setc
aptu
red
-U
seof
thea
tre
info
rmat
ion
-D
evel
opm
ento
fnew
way
sof
wor
king
EFF
ICIE
NC
Y
PATI
EN
T/Q
UA
LITY
FUTU
RE
CO
ST
Leve
l1–
Ove
rall
The
atre
Ap
pen
dic
esF,
G,H
Leve
l2–
Sp
ecia
lty
Ap
pen
dic
esF,
ILe
vel3
–P
roce
dur
eA
pp
end
ices
J,K

National Theatres Project26
Hours Breakdown
Actual Procdrl Surg Anaesth Turnover Procdrl
Percentage Breakdown
Surg Anaesth OtherOther Turnover
B+F C+D+E A-B H+I+JHospital AC8: Orthopaedics
Session holder: 92 66.4 88.2 33.5 11.8 42.9 -21.8 133 50 18 65 -33
Session holder: 96 53.6 51.0 31.4 11.0 8.6 2.6 95 59 20 16 5
Session holder: 155 54.7 51.6 33.2 9.5 8.9 3.1 94 61 17 16 6
Session holder: 227 33.2 30.9 20.7 5.4 4.8 2.3 93 62 16 15 7
Session holder: 242 42.0 41.0 26.8 6.4 7.8 0.9 98 64 15 19 2
Session holder: 254 52.6 49.7 33.6 10.1 6 2.9 95 64 19 12 5
Session holder: 306 26.7 26.8 13.7 6.4 6.7 -0.1 100 51 24 25 0
Session holder: 1136 99.8 107.0 61.7 15.1 30.2 -7.2 107 62 15 30 -7
Session holder: 1147 96.9 94.2 59.9 19.0 15.3 2.7 97 62 20 15 3
Session holder: 1228 97.2 94.4 59.6 20.8 14 2.8 97 61 21 15 3
Session holder: 1420 13.8 12.8 7.9 2.5 2.4 1.0 93 57 18 18 7
Session holder: 1857 9.4 9.5 6.3 2.2 1 -0.1 101 67 23 11 -1
Session holder: 2646 79.2 81.2 44.6 15.4 21.2 -2.0 103 56 19 28 -3
Total 725.4 738.3 432.7 135.5 170.1 -12.9 102 60 19 23 -2
C9: Plastic Surgery
Session holder: 52 6.5 7.1 3.5 0.0 3.6 -0.6 109 54 0 55 -9
Session holder: 63 4.8 3.1 2.9 0.0 0.2 1.8 64 61 0 3 36
Session holder: 200 18.8 25.3 12.6 1.6 11.1 -6.5 134 67 8 59 -34
Session holder: 1108 124.0 124.6 83.1 0.4 41.1 -0.6 101 67 0 34 -1
Total 154.2 160.1 102.1 2.0 56 -5.9 104 66 1 37 -4
CB: Urology
Session holder: 86 12.0 11.1 7.2 1.3 2.6 1.0 92 60 10 22 8
Session holder: 172 97.5 117.2 58.9 6.0 52.3 -19.7 120 60 6 54 -20
Session holder: 2409 6.6 11.8 4.8 0.6 6.4 -5.3 180 73 9 98 -80
Session holder: 2603 40.3 52.1 27.1 3.5 21.5 -11.8 129 67 9 53 -29
Total 156.3 192.1 98.0 11.3 82.8 -35.8 123 63 7 53 -23Report version 1.0 31 August 2006
APPENDIX F: Pilot Management ReportsNational Theatres Project – Benchmarking Pilot Board XHours Usage Analysis(Elective Sessions Only)Period: 01/02/2006 to 30/04/2006
A B C D E F G H I J K
Appendix F: Pilot Management Reports 27
Over-Runs
Sessions No. %AverageDuration(Hours)
No. %
Under-Runs
AverageDuration(Hours)
Hospital BUrology 72 18 25 1.5 45 63 1.5
Plastic Surgery 2 0 0 0.0 2 100 1.2
Minor Ops 7 0 0 0.0 7 100 1.3
Cardiology 5 0 0 0.0 5 100 2.0
Community Dental 7 1 14 1.0 6 86 1.3
Vascular 2 0 0 0.0 2 100 0.8
E N T 76 14 18 1.3 46 61 1.6
General Surgery 79 33 42 1.3 43 54 1.7
Gynaecology 10 0 0 0.0 9 90 1.6
Kids Dental 5 0 0 0.0 5 100 1.5
Max Fax 6 3 50 1.6 0 0 0.0
Oral Surgery 22 5 23 1.6 13 59 1.3
Orthopaedics 40 14 35 1.2 22 55 1.7
Renal 5 0 0 0.0 5 100 1.4
Total 338 88 26 1.3 210 62 1.6
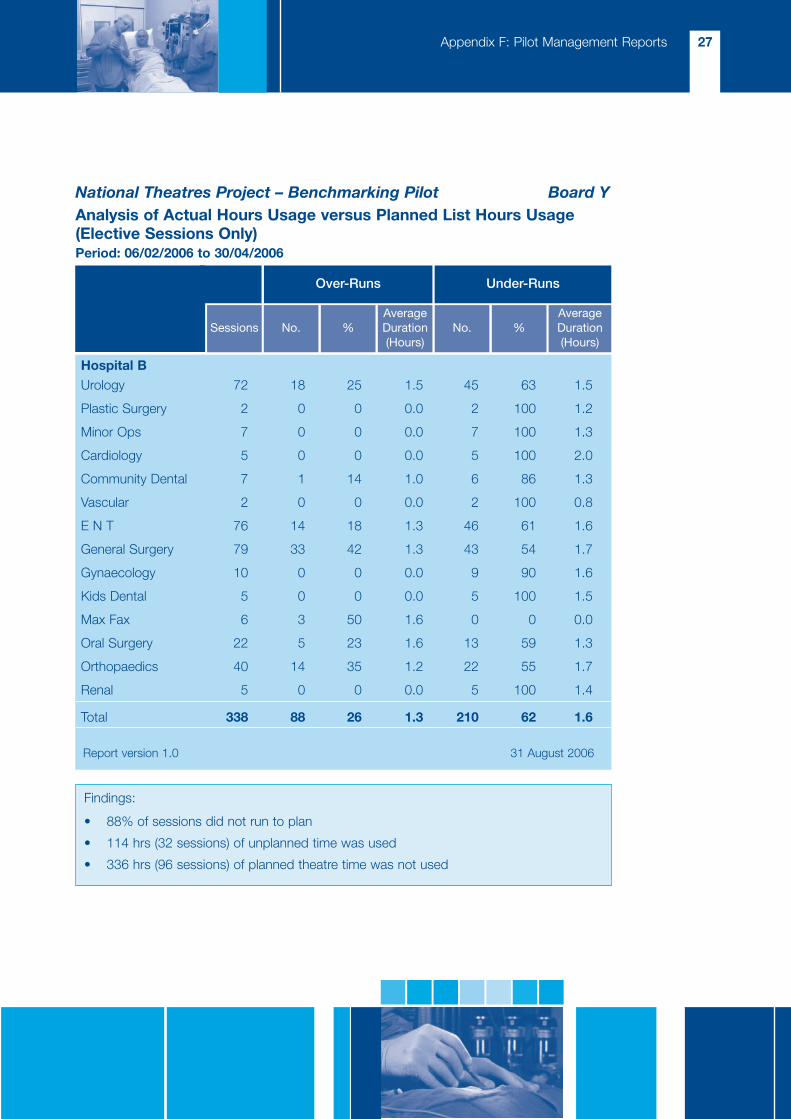
National Theatres Project – Benchmarking Pilot Board YAnalysis of Actual Hours Usage versus Planned List Hours Usage(Elective Sessions Only)Period: 06/02/2006 to 30/04/2006
Report version 1.0 31 August 2006
Findings:
• 88% of sessions did not run to plan
• 114 hrs (32 sessions) of unplanned time was used
• 336 hrs (96 sessions) of planned theatre time was not used

National Theatres Project28
Patient cancelled
PatientsNumber
Cancellations
%
Patientcancelled
PatientDNA
Theatrecancelled
Surgeon/anaesth
cancelled
Hospitalcancelled
Noreason
supplied
Hospital CA1 General Medicine 223 36 16 7 23 1 4 1 0
C1 General Surgery 257 23 9 5 8 0 4 2 4
C8 Orthopaedics 303 25 8 7 7 0 11 0 0
CB Urology 239 32 13 11 15 0 4 1 1
D3 Oral Surgery 6 1 17 0 0 0 1 0 0
Total 1,028 117 11 30 53 1 24 4 5
Cancellations Analysis
Period: 01/02/2006 to 30/04/2006
National Theatres Project – Benchmarking Pilot (Contd.) Board X
Report version 1.0 31 August 2006

Appendix G: Pilot Scorecard 29
APPENDIX G: Pilot Scorecard
Board X Hospital B
Patient/QualityCancellations % 13 7
Complaints No 2
Resource unavailability hrs lost
Deaths per 1000 pats 0.1 0.4
Critical care % 0.4 0.0
Time in recovery Avg (Mins) 38 –
Risk management episodes No 21
Length of stay outliers %
Surgical re-admissions per 1,000
Waiting list efficiency ratio
Theatre delays % 2 –
Re-operation within the same admission No
EfficiencyAvailable theatre time hrs 13,671 3,780
Allocated threatre hours hrs 11,767 –
Actual theatre hours hrs 8,601 1,098
Procedural theatre hours % 101 87
Surgical theatre hours % 59 65
Anaesthetic theatre hours % 14 21
Turnover time hours % -1 14
Case-mix adjusted throughput per theatre 1,136 1,180
Elective/emergency/unplanned mix % Elective 81 87
Over-runs (sessions) % 12 26
Under-runs (sessions) % 50 62
Late starts (sessions) % 79 71
Cancelled sessions % 14 21
Delayed discharges (from Recovery) No
Scheduled Utilisation = Allocated Hours
=11,767
X 100 = 86%Available Hours 13,671
Actual Utilisation =*Actual Theatre Hours Worked X 100
=8,601
= 73%Allocated Hours 11,767
*(Allocated Hours + Over-run Hours – Under-run Hours – Cancelled Sessions)

National Theatres Project30A
PP
EN
DIX
H:P
ilot
Ana
lysi
s–
Ho
urs
Bre
akd
ow
n
13,6
71
Ava
ilab
leH
ours
11,7
671,
904
Allo
cate
dH
ours
Una
lloca
ted
Hou
rs
Act
ualH
ours
Use
d
8,02
9
Use
d
3,73
8
Unu
sed
Use
d
952
1,14
51,
640
85
Late
star
tsE
arly
Fini
shes
Can
celle
dS
essi
ons
Ear
lyS
tart
sLa
teFi
nish
es
487
8,60
1
Use
d(8
029)
Unu
sed
3,73
8
Pro
cedu
ralT
ime
=A
naes
thet
icTi
me
+S
urgi
calT
ime
+O
ther
(8,7
00)
(1,1
69)
(5,0
54)
(2,3
78)
Ove
r-ru
ns
356
1,88
11,
640
Und
er-r
uns
Can
celle
dS
essi
ons
Can
celle
dS
essi
ons
(572
)
Turn
over
time
(-99
)
572
Tim
esar
ein
hour
s.
Ana
lysi
sba
sed
onth
epe
riod
1st
Febr
uary
2006
to30
thA
pril
2006
,ele
ctiv
ese
ssio
nson
ly.
Ava
ilabl
eho
urs
isa
theo
retic
alm
axim
umba
sed
ontw
o3.
5ho
urs
sess
ions
per
wee
kday
for
the
abov
epe
riod
for
alls
igni
fican
tth
eatr
elo
ci(c
hild
ren’
sth
eatr
e,de
ntal
thea
tre,
DS
Upr
oced
ure
room
s,D
SU
thea
tres
,gyn
aeco
logy
thea
tres
,mat
erni
tyth
eatr
es,m
ain
thea
tres
and
endo
scop
yro
om).
Pro
cedu
ralt
ime
isde
fined
asin
toan
aest
hetic
toin
tore
cove
ry.I
tis
ther
efor
epo
ssib
lefo
rtu
rnov
ertim
e(th
edi
ffere
nce
betw
een
actu
altim
ean
dpr
oced
ural
time)
tobe
nega
tive
–ne
xtpa
tient
goes
into
anae
sthe
ticbe
fore
the
prev
ious
one
goes
into
reco
very
.
An
over
-run
isa
sess
ion
whe
reth
eac
tual
dura
tion
exce
eded
the
plan
ned
dura
tion
(irre
spec
tive
ofpl
anne
dan
dac
tual
star
tan
den
dtim
es),
sim
ilarly
anun
der-
run
isa
sess
ion
whe
reth
eac
tual
dura
tion
isle
ssth
anth
epl
anne
ddu
ratio
n.
Bo
ard
X
No
tes

Appendix I: Pilot Analysis – Session Duration 31
AP
PE
ND
IXI:
Pilo
tA
naly
sis
–S
essi
on
Dur
atio
nT
heat
reS
essi
ons
,Und
er-R
uns
and
Ove
rR
uns
Bo
ard
X,O
pht
halm
olo
gy,
01/0
2/20
06to
30/0
4/20
06
-100-80
-60
-40
-20020406080100
Session holder 43
Session holder 44
Session holder 97
Session holder 184
Session holder 264
Session holder 1033
Session holder 1983
%Under-Runs%Over-Runs
444
444
333
888
Not
es:
(1)–
Und
er-R
uns
are
only
calc
ulat
edif
they
are
over
45m
ins.
(2)–
Ove
r-R
uns
are
only
calc
ulat
edif
they
are
over
30m
ins.
Ove
r-R
uns
Ove
r-R
uns
Boa
rdX
Und
er-R
uns
Und
er-R
uns
Boa
rdX
1U
nder
-Run
sar
eon
lyca
lcul
ated
ifth
eyar
eov
er45
min
utes
.2
Ove
r-R
uns
are
only
calc
ulat
edif
they
are
over
30m
inut
es.
3N
ote
that
the
sess
ion
hold
eris
not
nece
ssar
ilyth
ese
ssio
nus
er.
No
tes

National Theatres Project32
AP
PE
ND
IXJ:
Pilo
tA
naly
sis
–P
atie
ntP
athw
ayP
atie
ntP
athw
ay–
Cat
arac
tS
urg
ery,
Bo
ard
X
Gra
de
of
Ana
esth
etis
tn
%
No
Ana
esth
etis
t56
376
Ass
ocia
teS
pec
ialis
t66
9
Con
sulta
nt38
5
SP
R29
4
SH
O20
3
Med
ical
Stu
den
t11
1
LSTF
GR
D4
1
PTG
DP
30
Not
reco
rded
10
HO
10
LCO
NS
10
Ca
nc
ella
tio
ns
Th
ere
wer
en
oca
nce
llatio
ns
reco
rded
for
cata
ract
surg
ery.
Th
ere
wer
e7
37
case
sfo
rca
tara
ctsu
rger
y
Des
tinat
ion
Th
ed
estin
atio
nfo
ral
l73
7p
atie
nts
was
aS
tan
dar
dW
ard
De
lays
Th
ere
wer
e2
3ca
tara
cto
per
atio
ns
del
ayed
(3%
of
the
tota
l).
Re
aso
n
No
po
rter
avai
lab
le1
3P
atie
nt
no
tre
ady
10
Gra
de
of
Sur
geo
nn
%
Con
sulta
nt37
150
SP
R24
233
SH
O11
516
Med
ical
Stu
den
t4
1
STF
DO
C4
1
Not
reco
rded
10
Sen
tfo
r-
Arr
ival
An
aest
het
icst
art
-In
toth
eatr
e
Su
rger
yst
art
-S
urg
ery
end
Into
reco
very
-O
ut
of
reco
very
Me
an
tim
em
inu
tes
(Sta
nd
ard
De
via
tio
n)
05
10
15
20
25
30
35
40
45
50
55
60
65
8(4
)
8(8
)
18
(14
)
8(6
)
11
(7)
4(4
)
4(7
)
Arr
ival
-A
nae
sth
etic
star
t
Into
thea
tre
-S
urg
ery
star
t
Find
ing
s
•30
%of
time
issu
rgic
altim
e•
26%
oftim
eis
pre
par
atio
nan
dan
aest
hesi
a
•38
%of
time
isd
own
time
•w
ide
varia
tion
inan
aest
hetic
star
t-
into
thea
tre
•w
ide
varia
tion
insu
rgic
altim
e
•w
ide
varia
tion
intim
efo
rin
toan
dou
tof
reco
very
Su
rger
yen
d-
Into
reco
very

Appendix K: Pilot Analysis 33
AP
PE
ND
IXK
:Pilo
tA
naly
sis
–S
urg
ical
&A
naes
thet
icT
imes
Sur
gic
alT
ime
for
Cat
arac
tO
per
atio
nsb
yS
urg
eon
Bo
ard
Y,30
/01/
2006
to28
/04/
2006
(Ele
ctiv
ep
roce
dur
eso
nly)
1C2C
3NC
5C6C
7NC
8NC
9NC
10C
11C
12N
C
Sur
geon
IDan
dgr
ade
(C=
Con
sulta
nt,N
C=
Non
-con
sulta
nt)
Sur
geon
IDan
dgr
ade
1C2C
3NC
5C6C
7NC
8NC
9NC
10C
11C
12N
C
No.
ofca
ses
5153
3755
523
1613
4052
10
70 60 50 40 30 20 10 0
Surgicaltime (mins)

National Theatres Project34
Ana
esth
etic
Tim
efo
rH
ipR
epla
cem
ent
by
Ana
esth
etis
tB
oar
dX
,01/
02/2
006
to30
/04/
2006
(Ele
ctiv
ep
roce
dur
eso
nly)
Ana
esth
etis
tID
Ana
esth
etis
tID
and
grad
e(C
=C
onsu
ltant
,NC
=N
on-c
onsu
ltant
)38
C47
C48
C93
C12
3C12
9C15
2C18
1C22
1C29
1NC
293C
354N
C10
20C
1109
NC
No.
ofca
ses
91
102
27
35
44
43
141
1132
C11
39C
1140
NC
1143
C11
54C
1182
NC
1196
C12
22C
1226
C12
27C
1625
NC
1685
NC
1858
NC
2012
NC
No.
ofca
ses
63
54
21
52
77
92
11
2053
NC
2272
NC
2312
NC
2653
NC
2685
NC
2694
NC
2697
NC
2767
NC
2793
NC
2825
NC
2826
NC
No.
ofca
ses
11
31
11
12
19
1
80 60 40 20 0
38C
47C
48C
93C
123C
129C
152C
181C
221C
291NC
293C
354NC
1020C
1109NC
1132C
1139C
1140NC
1143C
1154C
1182NC
1196C
1222C
1226C
1227C
1625NC
1685NC
1858NC
2012NC
2053NC
2272NC
2312NC
2653NC
2685NC
2694NC
2697NC
2767NC
2793NC
2825NC
2826NC
Anaesthetic time (mins)AP
PE
ND
IXK
:(C
ont
d.)

Appendix L: Capability Scoping 35
Nationally Reported DataA number of common themes emerged regarding theinformation published in the annual Scottish HealthService Costs (Cost Book):
• In most Boards, theatres hours information iscollected either manually or through existingTheatre Management Systems and provided toFinance who combine with correspondingfinancial information.
• In a number of Boards, there was uncertainty asto how Finance sourced theatre hours statistics.
• There were general concerns over the quality ofthe published data, these primarily related toconsistency of definitions, inaccuracies in thenumbers of theatres per site, and capture of localprocedures.
• Cost book submissions prepared by Finance arenot validated by theatres personnel.
Other issues/concerns related to:
• the clarity of cost book definitions
• the prescriptive nature of cost bookrequirements
• the potential skewing of financial statistics bywaiting list initiative funding.
Comments on how to improve nationally reporteddata consisted of a mixture of common themes andmore detailed data-related suggestions. The mainthemes comprised:
• the need for clear and consistent definitions
• improved liaison with Finance, including validationof figures.
In some Boards, it was recognised that improvedlocal reporting capability was required.
There were a number of suggestions on how toimprove the value and accuracy of the data reported,as well as thoughts on potentially useful additionalinformation:
Improvement:
• separation of used/unused theatres
• separation of emergency and elective theatres
• reporting at site and specialty level
• identification of CEPOD, out of hours, etc.
• improvements in quality of coding
• a facility for local managers to provide asupporting commentary to identify assumptionsmade relating to their submissions.
Useful additional data:
• cost per case for standard procedures
• more robust utilisation statistics
• the extent to which pre-operative assessment isused
• use of capacity within the private sector
• available funded capacity by site and specialty
• education and training statistics
• staffing statistics.
National Theatres MetricsAn early piece of work by the National TheatresProject involved combining Cost Book informationwith SMR01 activity data to derive a number ofBoard level theatres metrics. These were reviewed aspart of the scoping visits.
On the whole Boards felt that the metrics derivedwould be potentially useful subject to the accuracy ofthe underlying Cost Book data. Again consistency ofdefinitions was a key issue.
APPENDIX L: Capability Scoping

Local InformationBoards across Scotland are moving towards real-time theatres information capture via a variety of TheatreManagement Systems, with several Boards implementing systems in recent months. There are however still anumber of mainland and island Boards which do not yet have systems.
National Theatres Project36
A number of factors and concerns were raisedrelating to the use and interpretation of the metrics:
• Potential inconsistencies in the types of theatreincluded and their impact on utilisation, e.g.emergency theatres will reduce utilisation figuresand these should be excluded or reportedseparately
• The need to handle endoscopy activity on aconsistent basis
• Some Boards felt that the use of 41 hours pertheatre as a capacity measure was either too highor too blunt a statistic
• Cost book statistics assume a 52 week year,which will understate utilisation for theatresrun/funded for shorter periods
• Using SMR01 “Procedure not done” will under-report cancellations
• Figures would be more use by site and specialty
• Cost per procedure information would be betterby specialty
• The impact of teaching sessions on throughput
• Post-operative infection ratios would be moreuseful if based on inpatient activity only
• Grouping together DGH and Teaching hospitalswould be useful.
Systems in Use
Board System Vendor/In-house Updating Comments
(Former) Argyll and Clyde ORSOS* Per-Se Real-time Inverclyde RH using Galaxyas at March 2006
Ayrshire and Arran RES-Q RES-Q Real-timeBorders Sapphire Newgate Technology Real-time Expected to go live September 2006Dumfries and Galloway Sapphire Newgate Technology Real-timeFifeForth Valley Sapphire Newgate Technology Real-timeGolden JubileeGrampian Stopped using Galaxy in 2000
ORSOS Per-Se Real-timeGreater Glasgow TIS In-house Real-time
Meditech Real-time Meditech theatre moduleintegrated with HISS
Highland TheatreMan Tri-Soft Real-time Not BroadfordLanarkshire ORMIS iSOFT Real-time
ORSOS Per-SeLothian
Pets In-house St. John’s Hospital onlyTayside In-house Manual data capture
* Implementation ongoing at time of visit
Moving toreal-time

Appendix L 37
For Boards with systems, data is typically captured using a combination of touch screen and keyboard inputs. In one case, information is recorded manually and then entered into the Theatre Management System. It iscommon for surgeons and anaesthetists to add information to the system (operation note, procedure codes, ASAgrading information), but this does not happen in all Boards. Submitted information is usually verified, and can beamended if necessary. Within Boards without systems, manual data collection allows at least some key theatreperformance information to be provided, e.g. hours, cancelled sessions, cancelled patients, utilisation, etc.
Existing Systems – Support and Ease of Use
Board System Support Ease of Use
(Former) Argyll and Clyde ORSOS Standard upgrades. User group. Users confident about using in liveQuality - patchy to-date. environment.
Ayrshire and Arran RES-Q Annual license provides very basic System quite basic and lacksbasic support. validation facilities.
Borders Sapphire Standard upgrades. Very intuitive.Dumfries and Galloway Sapphire Two upgrades per year. User No major problems.
group. Quality – no problems.Forth Valley Sapphire Standard upgrades. Quality – Easy to use but some issues.
variable.ORSOS Periodic updates. Per-Se help desk.
Quality – pretty reliable.Greater Glasgow
TIS In-house. Quality – excellent.Meditech Major upgrades every two years. Relatively easy to use.
Highland TheatreMan Optional periodic upgrades. Fairly intuitive to use, few issues.Quality – okay.
Lanarkshire ORMIS Quarterly releases. User Group. No problems – easy to use.Quality – fine to-date.
Lothian ORSOS Input time consuming, user interfacePets requires improvement.
Tayside In-house support. Very happy with system.
On the whole, staff are happy with thesystems.
National Theatres Project38
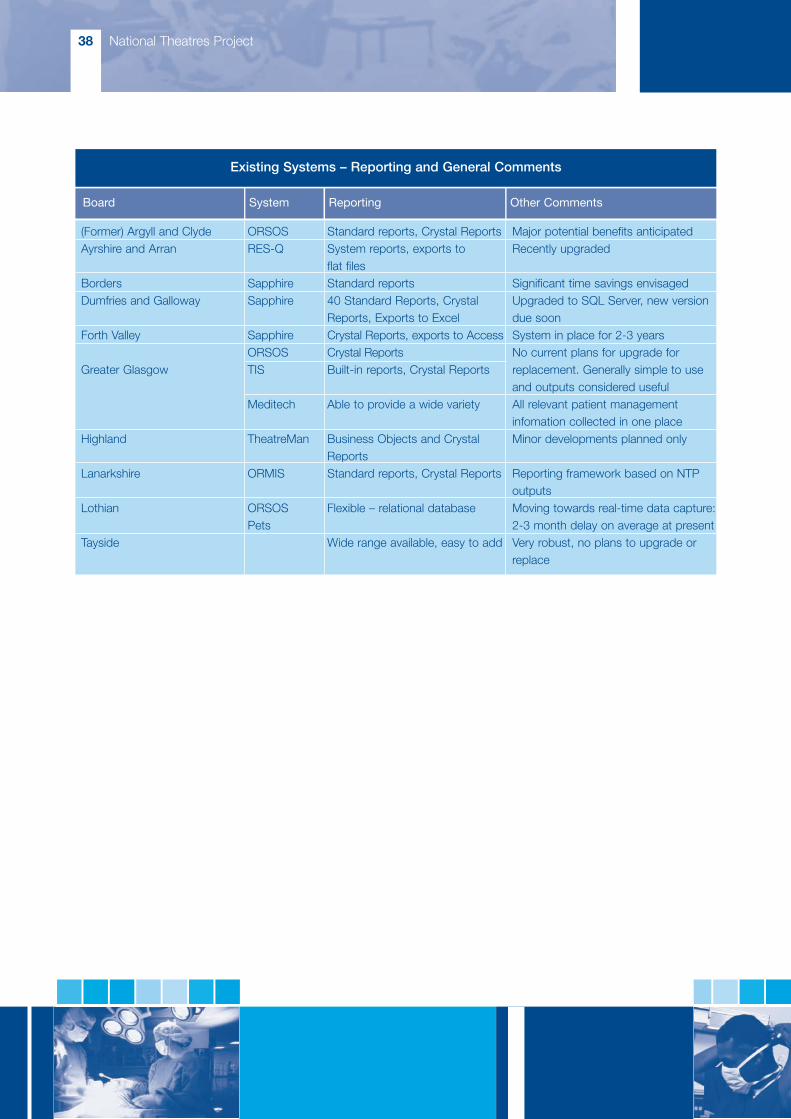
Existing Systems – Reporting and General Comments
Board System Reporting Other Comments
(Former) Argyll and Clyde ORSOS Standard reports, Crystal Reports Major potential benefits anticipatedAyrshire and Arran RES-Q System reports, exports to Recently upgraded
flat filesBorders Sapphire Standard reports Significant time savings envisagedDumfries and Galloway Sapphire 40 Standard Reports, Crystal Upgraded to SQL Server, new version
Reports, Exports to Excel due soonForth Valley Sapphire Crystal Reports, exports to Access System in place for 2-3 years
ORSOS Crystal Reports No current plans for upgrade forGreater Glasgow TIS Built-in reports, Crystal Reports replacement. Generally simple to use
and outputs considered usefulMeditech Able to provide a wide variety All relevant patient management
infomation collected in one placeHighland TheatreMan Business Objects and Crystal Minor developments planned only
ReportsLanarkshire ORMIS Standard reports, Crystal Reports Reporting framework based on NTP
outputsLothian ORSOS Flexible – relational database Moving towards real-time data capture:
Pets 2-3 month delay on average at presentTayside Wide range available, easy to add Very robust, no plans to upgrade or
replace

Appendix L 39
Reporting and AccountabilityThere are huge differences in the nature and level oftheatres performance reporting between Boards inScotland. This can vary from Boards where regularperformance reporting is not currently required, toBoards where reports covering a range of keyindicators are circulated widely around theatre usersand managers.
Reports produced include:
• utilisation reports
• cancelled sessions
• patient cancellations
• theatre activity
• over-runs, under-runs and late starts
• log books
• audit reports.
In addition, theatre information is used to:
• support ad hoc analyses
• provide baselines
• develop business cases
• report performance against specific targets
• provide comparisons
• support research activities
• validate data for national returns.
Reporting is typically a combination of weekly andmonthly outputs. Report distribution and theatreaccountability can include:
• Theatre Users
• Clinical Groups
• Anaesthetic Management Teams
• Surgical Management Teams
• Theatre Service Managers
• Clinical Service Managers
• Heads of Service
• Clinical Directors
• Medical Directors
• General Managers
• Performance Review/Management
• Specialty Management
• Directorate Managers
• Divisional Managers
• Senior Management Team
• Executive Directors
• Operating Division Chief Executives.
In at least one Board, Theatre Management Systemoutputs are displayed on notice-boards with plans toinclude the information on the intranet.

National Theatres Project40
Minimum DatasetThe table below gives a high-level indication of the availability of the dataset required to produce the draftbalanced scorecard across Boards with Theatre Management Systems.
Sessional – by holder, specialty and siteAvailable theatre hoursAllocated sessions/hours:
- booked start time (first patient into anaesthesia)- actual start time- booked end time (last patient into recovery)- actual end time- cancellation - plus reason and notice period
ProceduralDate and locationSession holderOperating surgeonMain anaesthetistOperation type
- Emergency (usually within 1 hour) NCEPOD 1- Urgent (within 6 hours) NCEPOD 2a- Urgent (within 24 hours) NCEPOD 2b- Scheduled (within 3 weeks) NCEPOD 3- Elective NCEPOD 4
Time into anaestheticStart time of anaesthesiaTime into theatreStart time of procedureTime operation completedTime into exit roomTime into recoveryTime ready to leave recoveryTime out of recoveryDelays - reason and durationDestination (DSU, Ward, HDU, ICU, Mortuary, Transfer)Cancellation - plus reasonSpecialtyOPCS4 code(s)
Other information – by specialty and holder/surgeonAdvance hospital cancellation of procedure - date and reasonComplaintsTheatre hours lost to resource unavailability, e.g. equipment failure, staff shortageRisk management episodesSurgical re-admissions (within a specified period)Re-operation within the same admission
Dark Blue – high coverage Lilac – medium coverage Light Blue – low coverage

Appendix L 41
Glossary and DefinitionsFor terms relating to the derivation of the minimumdataset, relatively little disagreement was foundbetween the proposed national definitions andcurrent Board practice (for Boards where there was aTheatre Management System in use).
There were two notable exceptions:
• list finish time
• operating time
and in each of these cases at least several Boardswere working to different definitions.
Use of Theatres InformationThe final sections of the capability scoping visitslooked at the use of theatres information withinBoards (with or without an implemented system), inthree parts:
• What information is required?
• How is information used in capacity planning andoperations management?
• How do Boards manage theatres within thecontext of the “whole system”?
Required Information
As well as highlighting the “usual” theatres indicators,e.g. cancellations, utilisation of sessions, utilisationwithin sessions, throughput, start and finish times,etc., a number of other potential requirements werehighlighted. In particular, the need for individual datato support log books, job planning and appraisals.Other requirements included:
• surgical rates
• implant tracking
• costs per procedure
• times per procedure
• patient journey
• case-mix analysis
• bed utilisation
• re-operation rates
• surgical infection rates
• patient risk assessment
• operation records
• audit.
Capacity Planning and Operations Management
There was tremendous variety between Boards in theuse of theatres information to support these activities.In many Boards, such work tended to be restricted toone-off analyses for specific purposes, often as aconsequence of the limitations of the theatresinformation currently available.
Capacity reports, monthly capacity plans and/ormeetings were highlighted by a number of Boards,and the need to improve capability and awareness inthis area was also recognised. Several Boards areusing or developing capacity planning models. Theimpact of anaesthetist availability has also been thefocus of attention in a couple of Boards, and in oneinstance this has led to the development andsuccessful implementation of an anaesthetist rostersystem.
Whole System
Again, this is an area where the level of activity varieswidely. A significant number of Boards currentlyundertake little work in this area, but are seeking toaddress this. Much of the work that is undertaken isof an ad hoc nature and again effort has beenconstrained by data issues.
In some Boards, whole system issues are addressedthrough Performance Management, or throughrelevant stakeholder groups.
Of the whole system related activities currently takingplace, much of this is focussed on bed requirements.

National Theatres Project42
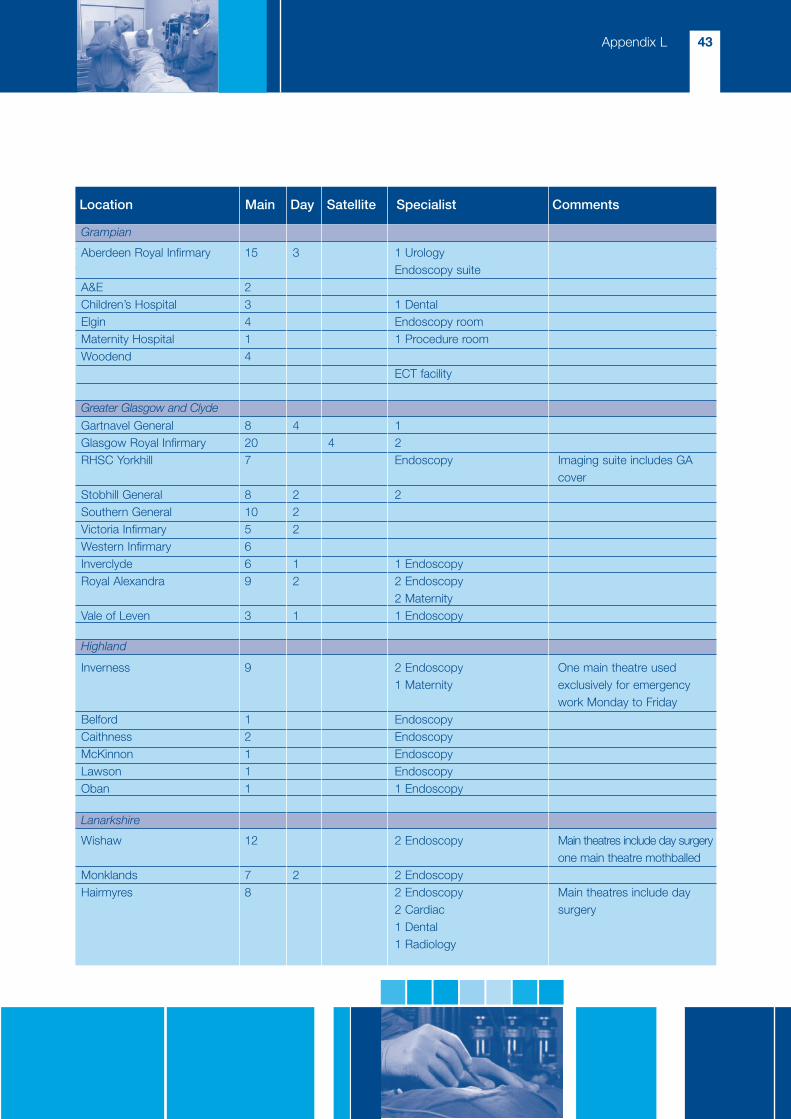
Location Main Day Satellite Specialist Comments
Annex: Theatre Facilities by Site
Arran 12 Specialist
Ayr 5 3 2 Endoscopy2 Urology procedure roomsAnaesthetic procedure room
Ayrshire Central 2 ObstetricsCrosshouse 8 4 4 Endsocopy
Borders General 5 1 1 Endoscopy One main theatre is A&E, oneis exclusively Obstetrics
Dumfries 6 1 Ophthalmology One main theatre is dedicated1 Obstetric 24-hour emergency, two areEndoscopy designated day surgery
Garrick 1
Queen Margaret Hospital 8 1 Cataract1 Dental
Victoria Hospital 6 1 Dental One further main theatremothballed
Forth Park Maternity 1 Gynaecology1 Obstetrics
St. Andrews Memorial One main theatre mothballed
Falkirk 5 3 Endoscopy Main theatres include daysurgery, no emergency
Stirling 5 3 1 Endoscopy Main theatres include one forCEPOD and one for Trauma.One satellite theatre is forObstetrics
8 Endoscopy Six main theatres and twoOphthalmology treatment rooms in use. Main4 Treatment rooms theatres include day surgery
Ayrshire and Arran
Borders
Dumfries and Galloway
Fife
Forth Valley
Golden Jubilee
Appendix L 43
Location Main Day Satellite Specialist Comments
Aberdeen Royal Infirmary 15 3 1 UrologyEndoscopy suite
A&E 2Children’s Hospital 3 1 DentalElgin 4 Endoscopy roomMaternity Hospital 1 1 Procedure roomWoodend 4
ECT facility
Gartnavel General 8 4 1Glasgow Royal Infirmary 20 4 2RHSC Yorkhill 7 Endoscopy Imaging suite includes GA
coverStobhill General 8 2 2Southern General 10 2Victoria Infirmary 5 2Western Infirmary 6Inverclyde 6 1 1 EndoscopyRoyal Alexandra 9 2 2 Endoscopy
2 MaternityVale of Leven 3 1 1 Endoscopy
Inverness 9 2 Endoscopy One main theatre used1 Maternity exclusively for emergency
work Monday to FridayBelford 1 EndoscopyCaithness 2 EndoscopyMcKinnon 1 EndoscopyLawson 1 EndoscopyOban 1 1 Endoscopy
Wishaw 12 2 Endoscopy Main theatres include day surgeryone main theatre mothballed
Monklands 7 2 2 EndoscopyHairmyres 8 2 Endoscopy Main theatres include day
2 Cardiac surgery1 Dental1 Radiology
Grampian
Greater Glasgow and Clyde
Highland
Lanarkshire

National Theatres Project44
Location Main Day Satellite Specialist Comments
New Royal Infirmary 12 4 8 Three mothballedEye Pavillion 3Western General 6 1 5Roodlands 2St. John’s 9 4Lauriston 1RHSC 5
Stracathro 3 2 EndoscopyPerth 5 2 2 Plus, one day surgery
treatment room. One satellitetheatre is mothballed
Ninewells 12 2 1 Ophthalmology Main theatres include 1 twin.Maternity theatre and Plust two day surgeryemergency room treatment rooms. Off-siteDental suite ECT facilities. Dental HospitalPaediatric theatre (sedation only)
Lothian
Tayside
Appendix M: Capability Template 45
APPENDIX M: Capability Template
CAPABILITY SCOPING
Board:
Primary Contact
Name:
Position:
Telephone/E-mail:
Planning
Extract baseline information:
Cost Book 2003/04 & 2004/05
National metrics 2003/04 & 2004/05
Identify specific data issues
Forward Requirements Summary to Primary Contact
Visits
Preliminary – NTP, introduction, background and information pack:
Datapoints Day Background Document
Draft Glossary and Definitions
Balanced Scorecard
Pilot Framework

National Theatres Project46
Mechanism for Feedback
Number of Theatres
Site Main Day Satellite Specialist
Key Theatres Contacts (for inclusion in NTP distribution list)
Name Role e-mail

Appendix M 47
Nationally Held Data
Review of 2003/04 and 2004/05 baselines:
Are the figures reasonable, are the metrics potentially useful, general comments?
Specific data issues and resolution:
Sourcing of nationally reported data
Sources of activity and cost data
Issues and risks
Quality of data, ease to obtain, etc.

National Theatres Project48
Potential improvement
(Including what information is useful, and what additional information would be useful)
Local information
1. Collection of local information
Process and issues, flowchart of process

Appendix M 49
Theatres System
For recent/ongoing implementations – request ITT and evaluation documents
System:
Vendor details (or in-house):
Software environment:
Purchase arrangements:
Support arrangements
Supported by, cost, SLA, quality of support, enhancements and upgrades
Ease of use
User comments on user-friendliness of system, like and dislikes
Reporting
Range and content of reports available, ability to define and configure reports

National Theatres Project50
Implications of revised definitions and dataset
Ability to add and revise data fields, are there cost and operational implications
General comments
Existing plans for upgrade or replacement, major features and/or deficiencies, overall user assessment ofsystem.
2. Timeliness of information
Average delay between activity and recording:
Information added at a later date and average delay

Appendix M 51
3. Range and content of reports available
Reports if no Theatres System, or those produced outwith the Theatres Sytstem
Use of reports, who uses them and how are they used to drive improvement and/or corrective action
4. Data fields collected
Field list and definitions, input forms, etc.(Any source providing all fields available)
If not readily available, request and/or obtain contact details for provider

National Theatres Project52
Minimum DatasetMany of the theatres scorecard measures can be calculated from the sessional and procedural datapointslisted below. The remaining measures have been detailed separately.
Avail (Y/N) SourceSessional – by holder, specialty and siteAvailable theatre hoursAllocated sessions/hours:
- booked start time (first patient into anaesthesia)- actual start time- booked end time (last patient into recovery)- actual end time- cancellation – plus reason and notice period
ProceduralDate and locationSession holderOperating surgeonMain anaesthetistOperation type
- Emergency (usually within 1 hour) NCEPOD 1- Urgent (within 6 hours) NCEPOD 2a- Urgent (within 24 hours) NCEPOD 2b- Scheduled (within 3 weeks) NCEPOD 3- Elective NCEPOD 4
Time into anaestheticStart time of anaesthesiaTime into theatreStart time of procedureTime operation completedTime into exit roomTime into recoveryTime ready to leave recoveryTime out of recoveryDelays - reason and durationDestination (DSU, Ward, HDU, ICU, Mortuary, Transfer)Cancellation - plus reasonSpecialtyOPCS4 code(s)
Other information - by specialty and holder/surgeonAdvance hospital cancellation of procedure - date and reasonComplaintsTheatre hours lost to resource unavailability, e.g. equipment failure, staff shortageRisk management episodesSurgical re-admissions (within a specified period)Re-operation within the same admission
OtherLength of stay outliers (see note 1)Waiting list efficiency ratio (see note 2)

Appendix M 53
Notes:
1. Individual cases compared with a historical analysis based on length of stay, specialty, and OPCS4 code(s).
2. Ratio of throughput to demand. Requires throughput and snapshots of opening and closing waiting list sizeover a period of time by specialty.
Definitions
For comparison against the draft Glossary and Definitions
Definition Description of any difference in definitionElective Emergency Operating theatreConsultant responsible for care Operating surgeon Supervising surgeon Surgical first assistant Assistant surgeons Main anaesthetist Supervising anaesthetist Assistant anaesthetist Specialty - consultant/patientDestination on leaving theatreList start time List finish timeList run timeList under-runList over-runPatient procedure hoursPlanned hoursOperating timeTurnover timeTime of bookingTime patient sent forTime patient arrived in theatre suiteTime into anaesthetic roomStart time of anaesthesia Time into theatreStart time of procedureTime operation completedTime into recoveryTime ready to leave recoveryTime actually left recovery
National Theatres Project54
5. Data quality and issues
Comments on general quality of data, issues, data validation, matching data to costs, etc.
6. Health Board view on local theatres data
Information found to be useful, data gaps and information that would be useful
Extent to which theatres information is used in capacity planning (inc. demand and demand forecasting,e.g. OP referrals, emergency), decision making and operations management

Appendix M 55
7. Whole Systems View
How do Board anticipate/accommodate “whole system” two-way interactions:Consultant/Doctor sessions (e.g. theatre v. outpatients); Surgical beds; Length of stay;Occupancy; ICU beds; HDU beds
Visit Details
Location:
Date:
Board Representatives:
NTP Representatives:
Document History

Technical Appendix
National Theatres ProjectReportNovember 2006
© Crown copyright 2007
This document is also available on the Scottish Executive website:www.scotland.gov.uk
Astron B49732 1/07
Further copies are available fromBlackwell’s Bookshop53 South BridgeEdinburghEH1 1YS
Telephone orders and enquiries0131 622 8283 or 0131 622 8258
Fax orders0131 557 8149
Email [email protected]