Embed Size (px)
Citation preview
National Strength andConditioning Association:Strength and ConditioningProfessional Standardsand Guidelines
STRENGTH AND CONDITIONINGPROFESSIONAL STANDARDS ANDGUIDELINES: OVERVIEW
The Strength & Conditioning profes-sion has come to a defining moment.The profession involves the combinedcompetencies of sport/exercise science,administration, management, teachingand coaching. Its practitioners must alsocomply with various laws and regula-tions while responding to instances ofpotential injury, and related claims andsuits. This creates remarkable chal-lenges, and requires substantial experi-ence, expertise and other resourcesto effectively address them, especiallyin multi-sport (e.g., collegiate andscholastic) settings.
Ample resources are available in someof these settings. In many others, how-ever, they are not. Budgets, equipment,facilities and staff are often limited(or lacking altogether), with a resultingmismatch between the participants’demand for safe and effective programsand services, and the institution’s pro-vision of them. It is important forStrength & Conditioning practitionersand their employers to understand thatthis standard of care is a shared duty;the institution and individual are thusjointly responsible for fulfilling it.
Collectively, these issues are the driv-ing forces behind this project.
The purpose of the NSCA Strength &Conditioning Professional Standards &Guidelines project is to help identifyareas of risk exposure, increase safetyand decrease the likelihood of injuriesthat might lead to claims, and ultimatelyimprove the standard of care beingoffered. This document is intended tobe neither rigid nor static. On the con-trary, the need for discretion and insightis a fundamental theme throughout; andthe information presented here will berevised periodically as the professioncontinues to evolve. It is hoped thatStrength & Conditioning practitionersand the institutions employing themwillmutually benefit from applying thisinformation, and in turn significantlyenhance the quality of services andprograms provided to their participants.
NOTICE
This document is intended to providerelevant practice parameters forStrength & Conditioning professionalsto utilize when carrying out theirresponsibilities in providing servicesto athletes or other participants. Thestandards and guidelines presentedhere are based on published scientificstudies, pertinent statements from
other associations, analysis of claims,and a consensus of expert views.However, this information is not a sub-stitute for individualized judgment orindependent professional advice.
Neither the NSCA nor the contrib-utors to this project assume any dutyowed to third parties by those reading,interpreting or implementing this in-formation. When rendering servicesto third parties, these standards andguidelines cannot be adopted foruse with all participants without exer-cising independent judgment and de-cision-making based on the Strength &Conditioning professional’s individualtraining, education and experience.Furthermore, Strength & Conditioningpractitioners must stay abreast of newdevelopments in the profession so thatthese standards and guidelines mayevolve to meet particular service needs.
Neither the NSCA nor the contrib-utors to this project, by reason ofauthorship or publication of this doc-ument, shall be deemed to be engagedin practice of any branch of profes-sional discipline (e.g., medicine, phys-ical therapy, law). Strength &Conditioning practitioners utilizingthis information are encouraged toseek and obtain such advice, if neededor desired, from licensed professionals.
VOLUME 31 | NUMBER 5 | OCTOBER 2009 Copyright � National Strength and Conditioning Association14

INTRODUCTION
SCOPE OF PRACTICE
The responsibilities and professionalscope of practice for Strength &Conditioning professionals can besubdivided into two domains (58):‘‘Scientific Foundations’’ and ‘‘Practical/Applied’’. Each of these involves cor-responding activities, responsibilitiesand knowledge requirements (refer toAppendices A & B):
Scientific Foundations.� Exercise Sciences (Anatomy, Exer-cise Physiology, Biomechanics, etc)
� Nutrition
Practical/Applied.� Program Design� Exercise Technique� Organization & Administration� Testing & Evaluation
DUTIES & CONCEPTS
Strength & Conditioning practitionershave duties to provide an appropriatelevel of supervision and instruction inorder to meet a reasonable standard ofcare, and to provide and maintain a safeenvironment for the participants undertheir supervision. These duties alsoinvolve informing users of risks inherentin and related to their activities, andpreventing unreasonable risk or harmresulting from ‘‘negligent instruction orsupervision’’(28,29,36). Greenwood &Greenwood (Chapter 21 [pp. 543-568]of Essentials Of Strength Training &Conditioning (7)) summarize the fol-lowing key liability concepts for theStrength & Conditioning professional:� Assumption of risk: voluntarily par-ticipation in activity with knowledgeof the inherent risk(s). Athleticactivities, including Strength & Con-ditioning, involve certain risks. Par-ticipants must be informed of therisks of activity, and required to signa statement to that effect.
� Responsibility, duty or obligation:Strength & Conditioning professio-nals have a duty to the participantsthey serve to take reasonable steps toprevent injury, and to act prudentlywhen an injury occurs (12).
� Standard of care: what a prudent andreasonable person would do undersimilar circumstances. A Strength &Conditioning professional is expectedto act according to his/her educa-tion, training and certification status(e.g., CSCS, NSCA-CPT, CPR, andFirst Aid).
� Negligence: failure to act as a reason-able and prudent person wouldunder similar circumstances. Fourelements must exist for a Strength &Conditioning professional to befound liable for negligence: duty,breach of duty, proximate cause, anddamages (65). Simply stated, aStrength & Conditioning professionalis negligent if he/she is proven to havea duty to act, and to have failed to actwith the appropriate standard of care,proximately causing injury or damagesto another person.
Standards vs. Guidelines.It is important to distinguish between‘‘standards’’ and ‘‘guidelines’’ becauseeach term has different legal implica-tions (19,83):� Standard: a required procedure thatprobably reflects a duty or obligationfor standard of care (note that thestandard statements in this docu-ment utilize the word ‘‘must’’). Thestandards set forth in this documentmay ultimately be recognized as alegal standard of care to be imple-mented into the daily operations ofStrength & Conditioning programsand facilities.
� Guideline: a recommended operat-ing procedure formulated and de-veloped to further enhance thequality of services provided (notethat the guideline statements in thisdocument utilize the word‘‘should’’). Guidelines are not in-tended to be standards of practiceor to give rise to legally definedduties of care, but in certain circum-stances they could assist in evaluat-ing and improving services rendered.
While the publication of this documentdoes not amount to a determination ofthe standard of care to be applied ina particular case, it is presumed, that
the standards stated herein may begiven authoritative weight.
Published Standards of Practice =Potential Duties.Proof of duty or standard of care can bedetermined in various ways, one ofwhich is from standards of practicepublished by professional associationsand organizations. Published standardsof practice can be used particularly tohelp determine whether a person wasnegligent in carrying out his/her duties(19), where they are generally recognizedas being indicative of widely acceptedpractices. Some courts examining theseissues in negligence cases have ruled thatviolations of such professional standardsconstitute a breach of duty.
If properly adopted and applied, pub-lished standards of practice can mini-mize liability exposures associated withnegligence, and thereby serve as a shieldfor those who comply with them. Theycan also be used as a sword againstthose who do not comply with them,potentially increasing liability risksassociated with negligence (19). Thekey issue in this regard appears to bethe practitioner’s consistent applicationof established standards of practice inthe provision of daily service. Forexample, if his/her conduct is provento be consistent with accepted stand-ard(s), it will be difficult to show breachof duty, thereby providing greater pro-tection against negligence. If his/herconduct is not proven to be consistentwith accepted standard(s), however, itmay be easier for the injured party toshow breach of duty by failure to followsuch standards, which can lead toa ruling of negligence.
TYPES OF STANDARDS
In addition to standards for desiredoperational practices published byprofessional organizations such as theNSCA, there are also standards fortechnical/physical specifications pub-lished by independent organizations suchas the AMERICAN SOCIETY FORTESTING & MATERIALS (ASTM) orU.S. CONSUMER PRODUCTSAFETY COMMISSION (CPSC).These are briefly described below:
Strength and Conditioning Journal | www.nsca-lift.org 15

Operational Practices.Established standards of care can beused to gauge a practitioner’s pro-fessional competence by comparinghis/her actual conduct with writtenbenchmarks of expected behavior. Inaddition to the standards and guide-lines from allied professional organiza-tions such as the AMERICANCOLLEGE OF SPORTS MEDICINE(8,23,83), AMERICAN HEART AS-SOCIATION (8,52) and NATIONALATHLETIC TRAINERS’ ASSOCIA-TION (73) referenced in this docu-ment, the following associations havealso published standards of practice:� AEROBICS & FITNESS ASSOCI-ATION OF AMERICA. ExerciseStandards & Guidelines. VenturaCA: AFAA, 1995.
� AMERICAN ACADEMY OF PE-DIATRICS. Strength Training byChildren and Adolescents. Pediatrics2008 121: 835-840. http://aappolicy.aappublications.org/cgi/search
� AMERICAN PHYSICAL THER-APYASSOCIATION. Guide to Phys-ical Therapist Practice (2nd Edition).Alexandria VA: APTA, 2001.
� AMERICAN PHYSICAL THER-APYASSOCIATION. Administrationof physical therapy services. Alexan-dria VA: APTA, 2001. http://www.apta.org/AM/Template.cfm?Section=Policies_and_Bylaws&CONTENTID=33912&TEMPLATE=/CM/ContentDisplay.cfm
� NATIONAL ASSOCIATION FORSPORT & PHYSICAL EDUCA-TION. National Physical EducationStandards (3rdEdition). ColumbusOH:McGraw-Hill Higher Education, 1995.
� NATIONAL ASSOCIATION FORSPORT & PHYSICAL EDUCA-TION.National Standards for AthleticCoaches. Reston VA: NASPE, 1995.
� NATIONAL ATHLETIC TRAIN-ERS’ ASSOCIATION BOARDOF CERTIFICATION. Standards ofProfessional Practice. Dallas TX: NA-TA, 2000. http://www.bocatc.org/index.php?option=com_content&task=view&id=51&Itemid=54
� PRESIDENT’S COUNCIL ONPHYSICAL FITNESS AND
SPORTS. Youth Resistance Training.Research Digest 4(3): 1-8, 2003.http://www.fitness.gov/Reading_Room/Digests/Digest-September2003.pdf
Technical/Physical Specifications.Technical/physical specifications rele-vant to the Strength & Conditioningprofession have been published by theCPSC (e.g., ‘‘Prevent Injuries to Chil-dren From Exercise Equipment’’;CPSC Document #5028) and ASTM(3,4). The former organization alsooperates the National Electronic InjurySurveillance System (NEISS), a surveil-lance and follow-back system that gath-ers data from hospital emergencydepartments to provide timely informa-tion on consumer injuries associated withcertain products or activities. Some of thisdata has been used to research weighttraining injuries, as will be addressed inthe Injury Trends, Litigations & Standardof Care Load discussion.
STANDARDS OF PRACTICE ASTHEY APPLY TO RISKMANAGEMENT
Risk management is a proactive ad-ministrative process that helps mini-mize liability, as well as decrease thefrequency and severity of injuries andsubsequent claims (18). It may not bepossible to eliminate all risk of injuryand liability exposure in Strength &Conditioning settings; however, it canbe effectively minimized by imple-menting risk management strategies.The Strength & Conditioning coordi-nator is ultimately responsible for riskmanagement, but all practitionersshould be involved in the variousaspects of the process. Eickhoff-Shemek (20) proposes a 4-step pro-cedure (adapted from Head & Horn(33)) for applying standards of practiceto the risk management process:
1. Identify and select standards of practice,as well as all applicable laws. Becauseso many standards of practice arepublished by various organizations,it is challenging for the Strength &Conditioning professional to beaware of all of them, and determinewhich ones are appropriate when
implementing the risk managementplan. In terms of participant safety,the most conservative or stringentstandards in a given industry shouldgenerally be used.
2. Develop risk management strategiesreflecting standards of practice and allapplicable laws. This step involveswriting procedures describing spe-cific responsibilities and/or dutiesthat staff would carry out in partic-ular situations. The proceduresshould be written clearly, succinctly,and without excessive detail (toomuch detail may not allow theflexibility practitioners need in par-ticular situations, and make imple-mentation of those strategiesdifficult or impractical). Once thewritten procedures are finalized,they should be included in the staffpolicies and procedures manual.
3. Implement the risk management plan.Implementation of the risk manage-ment plan primarily involves stafftraining to ensure that the practi-tioner’s daily conduct will be con-sistent with written policies andprocedures, standards of practice,and applicable laws. The policiesand procedures manual should beused in conjunction with the initialtraining of new employees, as wellas during regular in-service trainingwhere all employees practice a par-ticular (e.g., emergency) procedure.It is also important to explain to staffwhy it is essential to carry out suchduties appropriately.
4. Evaluate the risk management plan.Like the law, standards of practiceare not static and need to beupdated periodically to reflectchange. The risk management planshould be formally evaluated at leastannually, as well as after eachincidence of accident or injury todetermine whether emergency pro-cedures were performed correctlyand what could be done to preventa similar incident in the future.
LIABILITY EXPOSURE IN THESTRENGTH & CONDITIONINGPROFESSION
While each Strength & Conditioningprogram and facility is unique, the
VOLUME 31 | NUMBER 5 | OCTOBER 200916
Standards and Guidelines

NSCA Professional Standards & Guide-lines Task Force has identified nine (9)areas of potential liability exposure, asdelineated below. It is important to notethat they are interrelated. For example,proper instruction and supervision isassociated with personnel qualifications,as well as facility layout and schedulingissues. Noncompliance in any area cantherefore affect others, and in turncompound the risk of liability exposure.Furthermore, the Strength & Condi-tioning practitioner and his/her em-ployer share the corresponding dutiesand responsibilities.
Collectively within these liability ex-posure areas, eleven (11) standards andthirteen (13) guidelines for Strength &Conditioning practitioners have fur-ther been identified (these are pre-sented in the next section of thisdocument). These standards andguidelines are intended to serve as anauthoritative and unbiased source forprofessional guidance. The rationalefor each is summarized below.
1. Pre-participation Screening &Clearance.A physical examination is imperativefor all participants prior to participatingin a Strength & Conditioning program(preferably conducted by a licensedphysician). This should include a com-prehensive health and immunizationhistory (as defined by current guide-lines from the CENTERS FORDISEASE CONTROL & PREVEN-TION), as well as a relevant physicalexam, part of which includes an ortho-pedic evaluation. Some type of cardio-vascular screening, as discussed below,is also recommended. The Strength &Conditioning professional does notneed a copy of the results, but mustrequire a signed statement verifyingproof of medical clearance to partici-pate. Participants who are returningfrom an injury or illness, or who havespecial needs, must also be requiredto show proof of medical clearanceprior to beginning or returning to aStrength & Conditioning program.
Currently there are no universally ac-cepted standards for screening
participants; nor are there approvedcertification procedures for health careprofessionals who perform such ex-aminations. However, a joint Pre-participation Physical Evaluation TaskForce of five organizations (AMERI-CAN ACADEMY OF FAMILY PHY-SICIANS, AMERICAN ACADEMYOF PEDIATRICS, AMERICANMEDICAL SOCIETY FOR SPORTSMEDICINE, AMERICAN ORTHO-PAEDIC SOCIETY FOR SPORTSMEDICINE, and AMERICANOSTEOPATHIC ACADEMY OFSPORTS MEDICINE) has publisheda widely accepted monograph includ-ing detailed instructions on performinga pre-participation history and physicalexam, determining clearance for par-ticipation, and a medical evaluationform to copy and use for eachexamination (64). Additionally, theAMERICAN HEART ASSOCIA-TION and AMERICAN COLLEGEOF SPORTS MEDICINE have pub-lished statements on pre-participationscreening for those involved in fitness-related activities (8,52). Relevant pointscan be summarized as follows:
� Educational institutions have an ethi-cal, medical and possible legal obligationto implement cost-efficient, pre-partici-pation screening strategies (includinga complete medical history and physicalexamination), and thereby ensure thathigh school and college athletes are notsubject to unacceptable risks. Supportfor such efforts, especially in largeathletic populations, is mitigated bycost-efficiency considerations, prac-tical limitations, and an awarenessthat it is not possible to achieve zerorisk in competitive sports.
� Pre-participation athletic screeningshould be performed by a properlyqualified health care provider with therequisite training, medical skills, andbackground to reliably perform a physi-cal examination, obtain a detailed car-diovascular history, and recognize heartdisease. A licensed physician is pre-ferred, but an appropriately trainedregistered nurse or physician assis-tant may be acceptable under certaincircumstances in states where non-
physician health care workers arepermitted to perform pre-participa-tion screening. In the latter situation,however, a formal certification pro-cess should be established to dem-onstrate expertise in performingcardiovascular examinations.
� A complete and careful personal andfamily medical history and physicalexamination designed to identify (orraise suspicion of ) cardiovascular riskfactors known to cause sudden death ordisease progression is the best availableand most practical approach to screeningpopulations of competitive sports partic-ipants. Such screening is an obtain-able objective, and should bemandatory for all participants. Ini-tially a complete medical historyand physical examination should beperformed before participation inorganized high school athletics(grades 9-12). An interim historyshould be obtained in interveningyears. For collegiate athletes, a com-prehensive personal/family historyand physical examination should beperformed by a qualified examinerinitially upon entering the institu-tion, before beginning training andcompetition. Screening should berepeated every two years thereafterunless more frequent examinationsare indicated; and an interim historyand blood pressure measurementshould be obtained each subsequentyear to determine whether anotherphysical examination, and possiblefurther testing, is required (e.g., dueto abnormalities or changes in med-ical status).
� Health appraisal questionnaires shouldbe used before exercise testing and/ortraining to initially classify participantsby risk for triage and preliminarydecision-making. Following the initialhealth appraisal (and medical con-sultation and/or supervised exercisetest, if indicated), participants can befurther classified for exercise trainingon the basis of individual character-istics. When a medical evaluation/recommendation is advised or re-quired, written and active commu-nication between facility staff andthe participant’s personal physician
Strength and Conditioning Journal | www.nsca-lift.org 17

or health care provider is stronglyrecommended. Furthermore, partic-ipants should be educated aboutthe importance of obtaining a pre-participation health appraisal andmedical evaluation/recommendation(if indicated), as well as the potentialrisks incurred without obtainingthem.
2. Personnel Qualifications.Qualified and knowledgeable person-nel must be hired in order to properlysupervise and instruct participantsutilizing Strength & Conditioning fa-cilities and equipment. A three-pronged approach is recommended.
First, the Strength & Conditioningpractitioner should acquire expertise,and have a degree from a regionallyaccredited college/university in one ormore of the topics comprising the‘‘Scientific Foundations’’ domain iden-tified in the Certified Strength &Conditioning Specialist� (CSCS�)Examination Content Description (58)(i.e. exercise/anatomy, biomechanics,physiology, nutrition; Appendix A), orin a relevant subject (e.g., exercise/sport pedagogy, psychology, motorlearning, training methodology, kinesi-ology). Note that the NSCA’s Educa-tional Recognition Program has beendeveloped to recognize institutions ofhigher learning that meet such require-ments; and also helps to identify aneducational career path for theStrength & Conditioning profession.Likewise, practitioners should make anongoing effort to acquire knowledgeand competence in the content areasoutside their primary area of expertise.In 2004, Commission on Accreditationof Allied Health Education (CAAHEP)began accrediting programs in exercisescience and exercise physiology (http://www.coaes.org/accreditedprograms.html), so if the practitioner is unableto attend an NSCA-ERP institution,training in an accredited programin exercise science or exercisephysiology will ensure that the ‘‘Sci-entific Foundations’’ are thoroughlycovered.
Second, certifications offered throughprofessional organizations with con-tinuing education requirements as wellas a code of ethics (e.g., the NSCA’sCSCS� credential; Appendix B) areavailable to Strength & Conditioningpractitioners interested in acquiringthe necessary competencies. Anotheroption is the NSCA’s Fly Soloprogram (http://www.nsca-lift.org/Fly%20Solo%20Program/default.shtml),endorsed by the National High SchoolAthletic Coaches Association. De-pending on the practitioner’s specificduties, responsibilities, and interests,relevant certifications offered by othergoverning bodies, such as USAWeight-lifting, may also be appropriate.
Third, a Strength & Conditioningpractitioner’s knowledge and skill de-velopment can be enhanced by apply-ing the ‘‘performance team’’ concept(i.e. aligning a staff comprised ofqualified professionals with interde-pendent expertise and shared leader-ship roles; Appendix C) (43,44). Thescope of practice for the Strength &Conditioning profession has expandedand diversified to the point where it isvery challenging, and often unrealisticfor each individual to acquire pro-ficiency in all areas. Furthermore, theproductivity of a hierarchical (single-leader) work group can be significantlyimproved by applying the teammodel to staffing; and the same teamdynamics that augment the group’seffectiveness also tend to enhanceindividual members’ learning and skillacquisition (43).
3. Program Supervision & Instruction.It has been estimated that 80% of allcourt cases concerning athletic injuriesdeal with some aspect of supervision(12). Although serious accidents arerare in supervised exercise programs,the liability costs associated with in-adequate or lax supervision are veryexpensive; and the plaintiff’s recoveryrate in such negligence lawsuits isalmost 56% (54). The main causes ofthese incidents are poor facility main-tenance, defective equipment, and in-adequate instruction or supervision.The importance of staffing is readily
apparent in each circumstance. Forexample, Rabinoff (66) reviewed 32litigations arising from negligent weighttraining supervision, and found thatthree issues were raised by the plaintiff’sattorneys in each case: poor instruction(or instructor qualifications); lax/poorsupervision; and failure to warn ofinherent dangers (in the equipment,facility, or exercise). The standard ofcare used in each case cited in theRabinoff investigation was based uponstatements established by the NSCA,ACSM or AAHPERD. A prevalenttrend in these litigations is the issue of‘‘professional instructor qualifications,’’i.e. appropriate degrees, recognizedcertifications, training, experience, andcontinuing education (refer to item 2,and Appendices A & B).
Participants in a Strength & Condi-tioning facility must be properly su-pervised and instructed at all times toensure maximum safety, especiallybecause of the athletic, skillful natureof many activities implemented inStrength & Conditioning programs,in accordance with the dynamic cor-respondence (74) and practice speci-ficity (69,70) principles. Bucher &Krotee (12) recommend the followingcardinal principles of supervision:
� Always be there.� Be active and hands-on.� Be prudent, careful, and prepared.� Be qualified (e.g., accredited degree,CSCS, CPR, First Aid).
� Be vigilant.� Inform participants of safety andemergency procedures.
� Know participants’ health status.� Monitor and enforce rules andregulations.
� Monitor and scrutinize theenvironment.
In addition to the physical presenceof qualified professionals duringStrength & Conditioning activities,effective instruction and supervisioninvolves a range of practical considera-tions (5,7,16,35,36,38,49):� A clear view of all areas of thefacility, or at least the zone beingsupervised by each practitioner andthe participants in it (this issue is
VOLUME 31 | NUMBER 5 | OCTOBER 200918
Standards and Guidelines

related to facility design and layout,i.e. equipment placement with re-spect to visibility, versatility andaccessibility; refer to item 4)
� The practitioner’s proximity to thegroup of participants under his/hersupervision, (i.e. the ability to seeand communicate clearly with oneanother; and quick access to partici-pants in need of immediate assis-tance or spotting)
� The number and grouping of partic-ipants, (i.e. to make optimal use ofavailable equipment, space and time)
� The participants’ age(s), experiencelevel(s)and need(s)
� The type of program being con-ducted, (i.e. skillful/explosivefree-weight movements vs. guided-resistance exercises, and correspond-ing need for coaching and spotting)
In theory, Strength & Conditioningactivities should be scheduled to dis-tribute activity throughout the day, andthereby promote an optimal trainingenvironment (refer to Appendix D forbasic guidelines on calculating spaceneeds). Even with careful planning,however, most facilities have times ofpeak usage (e.g., as a result of teampractices and participants’ class sched-ules). Beyond a certain point, it is im-practical to simply spread Strength &Conditioning activities over a widerrange of times in order to maintain anacceptable professional-to-participantratio. The central issue is to accom-modate peak usage times by providingadequate facilities and qualified staff,such that all participants are properlyinstructed and supervised (refer to item2) (31,38,50,83). Furthermore, propertechniques, movement mechanics andsafety should be emphasized in orderto minimize injury risk and liabilityexposure (refer to Section 3 [Chapters13-14] of Essentials of Strength Train-ing & Conditioning (7) as well as theNSCA position statements (15,22,40,61,76,86,87) summarized in Appendix E).Likewise, instructional methods, pro-cedures, and progressions that areconsistent with accepted professionalpractices should be utilized (1,7,10,15,21,22,24–27,31,32,39,40,42,45–47,55,59,62,69-72,74–76,78–82,84–89).
While reasonable steps should be takento make optimal use of the Strength &Conditioning facility and staff, a poten-tial mismatch between availableresources and demand for programsand services exists in many institutionsduring times of peak usage. Asexplained below in the Injury Trends,Litigations & Standard of Care Loaddiscussion, the combined effects of ex-plosive growth in collegiate/scholasticathlete participation (especially amongfemales), corresponding liability expo-sures, and equal opportunity/accesslaws create a standard of care loadand liability challenge for Strength &Conditioning practitioners and theiremployers. A two-pronged approachcan thus be recommended.
First, Strength & Conditioning activi-ties should be planned, and the re-quired number of qualified staff shouldbe present, such that recommendedguidelines for minimum average floorspace allowance per participant (100ft2), professional-to-participant ratios(1:10 junior high school, 1:15 highschool, 1:20 college), and number ofparticipants per barbell or trainingstation (up to 3) are applied duringpeak usage times (5,7,38,42). In idealcircumstances, this corresponds to oneStrength & Conditioning practitionerper 3-4 training stations and/or 1,000ft2 area (junior high school); 5 trainingstations and/or 1,500 ft2 area (highschool); or 6-7 training stations and/or2,000 ft2 area (college), respectively.Professional discretion can be used toadjust these guidelines with respect tothe practical considerations discussedabove.
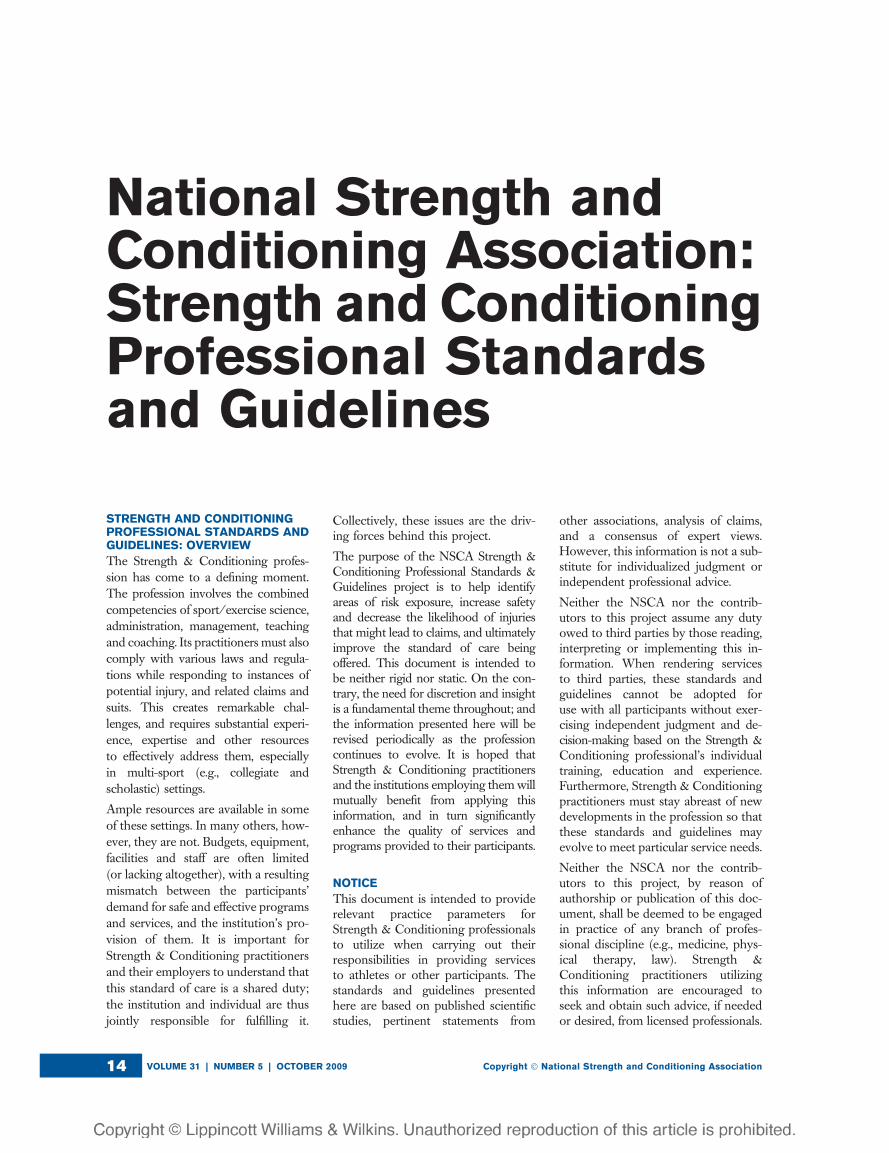
Second, Strength & Conditioning prac-titioners and their employers shouldwork together toward a long-term(e.g., 3-5 yr) goal of matching theprofessional-to-participant ratio inthe Strength & Conditioning facilityto each sport’s respective coach-to-athlete ratio. This is relatively straight-forward in collegiate settings where theNCAA limits the number of coachesper sport in Division I (NCAADivisionI Manual, Bylaw 11.7; updated annu-ally), and also provides sports
participation data (refer to AppendixF; note that coach-to-athlete ratiosfor individual-event sports are lowerthan those for team sports) (56). Inthe absence of similar information inother (e.g., scholastic) settings, suchdeterminations can be made on anindividual institution basis; or possiblyaccording to trends within a district,division or state.
4. Facility & Equipment Set-Up, Inspec-tion, Maintenance, Repair & Signage.In some cases, Strength & Conditioningprofessionals are involved in all phases offacility design and layout. Perhaps morecommonly, however, they assume re-sponsibility for an existing facility, inwhich case the opportunities to plan ormodify it may be limited. In either case,the Strength & Conditioning practi-tioner and his/her employer are jointlyresponsible for maximizing the safety,effectiveness and efficiency of the facility,such that the allotted space and time canbe put to optimal use (refer to Green-wood [Chapter 21, pp. 543-568] inEssentials Of Strength Training & Con-ditioning (7) as well as the table oncalculating equipment space needs inAppendix D).
The Strength & Conditioning profes-sional should establish written policiesand procedures for equipment/facilityselection, purchase, installation, set-up,inspection, maintenance and repair.Safety audits and periodic inspectionsof equipment, maintenance, repair andstatus reports should all be included.Manufacturer-provided user’s manuals,warranties and operating guides, aswell as other relevant records (e.g.,pertaining to equipment selection,purchase, installation, set-up, inspec-tion, maintenance and repair; refer toitem 6), should be kept on file andfollowed regarding equipment opera-tion and maintenance (12).
The Strength & Conditioning profes-sional should understand the conceptof ‘‘product liability’’, which refers tothe legal responsibilities of a productmanufacturer and/or vendor if a personsustains injury or damage due primarilyto a defect or deficiency in design or
Strength and Conditioning Journal | www.nsca-lift.org 19

manufacturing (9). While this issueapplies to manufacturers and vendors,there are actions and/or behaviorsthat can increase the Strength &Conditioning professional’s responsi-bility, consequently putting him/her atrisk for claims. The following stepsshould be taken to minimize liabilityexposures caused by Strength & Con-ditioning equipment: (12,16,48)� Buy equipment exclusively fromreputable manufacturers, and becertain that it meets existing stand-ards and guidelines for professional/commercial (not home) use.
� Use equipment only for the purposeintended by the manufacturer; donot modify it from the condition inwhich it was originally sold unlesssuch adaptations are clearly desig-nated and instructions for doing so areincluded in the product information.
� Post any signage provided by themanufacturer on (or in close prox-imity to) the equipment.
� Do not allow unsupervised partic-ipants to utilize equipment.
� Regularly inspect equipment fordamage and wear that may placeparticipants at risk for injury.
5. Emergency Planning & Response.An emergency response plan is a writ-ten document that details the properprocedures for caring for injuriesthat may occur to participants duringactivity (refer to Appendix G forsample guidelines for the collegiateenvironment). While all Strength &Conditioning facilities should havesuch a document, it is important toappreciate that the document itselfdoes not save lives. Indeed, it may offera false sense of security if it is notbacked up with appropriate trainingand preparedness by astute, profes-sional staff. Therefore, all personnel inStrength & Conditioning facilities must:� Know the emergency response planand the proper procedures for deal-ing with an emergency (i.e. locationof phones, activating emergencymedical services, designated person-nel to care for injuries, ambulanceaccess, and location of emergencysupplies).
� Review and practice emergencypolicies and procedures regularly(i.e. at least quarterly).
� Maintain current certification inguidelines for cardiopulmonary re-suscitation and automated externaldefibrillator (CPR-AED) as estab-lished by the AMERICAN HEARTASSOCIATION & INTERNA-TIONAL LIAISON COMMITTEEON RESUSCITATION (2). Severalorganizations, such as the AmericanHeart Association, the Red Cross,the National Safety Council, andSt. John Ambulance, offer acceptablecertifications. First Aid training andcertification may also be necessary ifSports Medicine personnel such asan ATC or MD are not immediatelyavailable.
� Adhere to universal precautions forpreventing exposure to and trans-mission of blood-borne pathogens,as established by the CENTERSFOR DISEASE CONTROL &PREVENTION (14) and OCCUPA-TIONAL SAFETY & HEALTHADMINISTRATION (60).
6. Records & Record Keeping.Documentation is fundamental to themanagement of Strength & Condition-ing programs and facilities. In additionto developing and maintaining a poli-cies and procedures manual (refer toEpley [Chapter 22, pp. 569-588] inEssentials Of Strength Training &Conditioning (7)), a variety of recordsshould be kept on file: (12)� Manufacturer provided user’s man-uals, warranties and operatingguides; and equipment selection,purchase, installation, set-up, inspec-tion, maintenance and repair records
� Personnel credentials� Professional standards andguidelines
� Safety policies and procedures, in-cluding a written emergency re-sponse plan (refer to item 5;Appendix G)
� Training logs, progress entries and/or activity instruction/supervisionnotes
� Injury/incident reports, pre-partici-pation medical clearance, and return
to participation clearance docu-ments (after the occurrence of aninjury, illness, change in health statusor an extended period of absence) foreach participant under theirsupervision
� In collegiate and scholastic settings,athletes are required to sign protec-tive legal documents (e.g., informedconsent, agreement to participate,waiver; refer to Appendix H) cover-ing all athletically-related activities,including Strength & Conditioning;however in other settings, theStrength & Conditioning profes-sional should consider having par-ticipants sign such legal documents.
Medical records should be kept on fileas long as possible in the event ofan injury claim. Statutes of limitations(i.e. the time in which individuals mayfile a lawsuit) vary from state to state,so it is a good practice to maintain filesindefinitely or consult with a legalauthority (37). As is the case withother organizational and administra-tive tasks, adequate staff are necessaryto properly keep and maintain suchrecords.
7. Equal Opportunity & Access.Federal, state, and possibly local lawsand regulations prohibit discriminationor unequal treatment (e.g., according torace, creed, national origin, gender,religion, age, handicap/disability orother such legal classifications) in mostorganizations, institutions and profes-sions. For example, practitioners em-ployed in federally-funded educational(i.e. collegiate or scholastic) settingsmust comply with civil rights statutesincluding Title IX of the EducationAmendments of 1972, which mandatesgender equity in providing opportunityand access to athletic facilities, pro-grams and services. The Strength &Conditioning professional must obeythe letter and spirit of these laws whenworking with participants as well asstaff.
8. Participation in Strength & Condi-tioning Activities by Children.Resistance training can be an
VOLUME 31 | NUMBER 5 | OCTOBER 200920
Standards and Guidelines

important component of youth fitness,health promotion and injury preven-tion. Such programs are safe whenproperly designed and supervised; andcan increase children’s strength, motorfitness skills, sports performance, psy-chosocial well-being and overall health(22,23). Indeed, many of the benefitsassociated with adult Strength &Conditioning activities are attainableby prepubescent and adolescent par-ticipants who participate in age-specific training. However, it is impor-tant for the Strength & Conditioningpractitioner to take certain precautionswith children.
In a 20-year retrospective review ofweight training injuries that wereevaluated and/or treated in U.S. hos-pital emergency departments (basedon NEISS data from the U.S. CON-SUMER PRODUCT SAFETY COM-MISSION), Jones et al.(41) found analarming incidence of injuries to youngchildren. Children ,7 years of age arealmost 6 times more likely to be injuredthan those .15 years of age, with themajority (80%) resulting from playingwith or around weight training equip-ment in the home. The CPSC esti-mates that about 8,700 children ,5years of age are injured each year withexercise equipment (e.g., include sta-tionary bicycles, treadmills, and stairclimbers), with an additional 16,500injuries per year to children 5-14 yearsof age (‘‘Prevent Injuries to ChildrenFrom Exercise Equipment’’; CPSCDocument #5028). This has clearimplications regarding the importanceof supervising children in these agegroups, and exposing them to suchequipment or facilities. In support ofthis, Malina (51) reported that esti-mated injury rates were 0.176, 0.053,and 0.055 per 100 participant-hours inthe programs examined in resistancetraining investigations in pre- andearly-pubertal youth. Twenty-two re-ports were examined and the inves-tigations employed high levels ofsupervision and low instructor toparticipant ratios, which was thoughtto be the reason for the extremely lowinjury rates.
Another area of potential injury concernfor children and pubescents/adolescents is the use of max testing(1RM). While Faigenbaum and others(22,23) have shown max testing to besafe in these age groups, it is empha-sized that maintaining technique iscritical. A multi-rep max (e.g., 3-5RM) may even be preferred to a1RM in certain situations, especiallywhere training age (i.e. number of yearsexperience in resistance training) is lessthan 3-4 years or physical developmentis behind what is expected for thechronological age. Nonetheless, atten-tion to NSCA-prescribed guidelines (7)for lifting technique should always befollowed.
9. Supplements, Ergogenic Aids &Drugs.The issue of using ergogenic aids,including nutritional supplements anddrugs, is complicated by several factors.First, dietary supplements are regulatedas foods rather than drugs according tothe Dietary Supplement Health &Education Act of 1994. Consequently,many people have concerns regardingquality control/assurance and possibleconsequences for consumers. Strength& Conditioning practitioners are oftenapproached for advice on nutrition andsupplementation, and therefore shouldbe aware of the following:� The FEDERAL TRADE COM-MISSION has primary responsibilityfor advertising claims. Simply stated,advertising for any product, includ-ing dietary supplements must betruthful, substantiated, and notmisleading.
� The U.S. FOOD &DRUGADMIN-ISTRATION has primary responsi-bility for product labeling claims.The legislation enforced by thisagency includes current goodmanufacturing practice regulations,and selected portions of the FederalFood, Drug & Cosmetic Act relatedto dietary supplements. Note thatthe U.S. Pharmacopeia & NationalFormulary, which establishesmanufacturing practices for nutri-tional supplements (i.e. standardsfor identity, strength, quality, purity,
packaging, labeling and storage), iscited as a primary resource in thislegislation.
A second complicating factor is thatthe boundaries between dietary sup-plements, drugs and conventionalfoods are not clear. This is especiallyproblematic for competitive athletesand coaches, because such productsmay contain substances that arebanned by one or more sport govern-ing bodies despite the manufacturer’sor vendor’s use of terms such as‘‘herbal’’, ‘‘legal’’, ‘‘natural’’, ‘‘organic’’,‘‘safe and effective’’, etc. Furthermore,supplement manufacturers are con-stantly developing new products withdifferent combinations of ingredients,making it more challenging to identifythose that may be problematic.
A third factor is that banned substancepolicies and procedures, testing proto-cols, and related rules and regulationsdiffer among sport governing bodies(e.g., MLB, NBA, NCAA, NFL, NHL,USOC). Therefore, a compound that islegal according to one governing bodymay be illegal according to another.Furthermore, Strength & Conditioningpractitioners at NCAA member insti-tutions need to be aware of Bylaw16.5.2.2: ‘‘An institution may provideonly non-muscle-building nutritionalsupplements to a student-athlete atany time for the purpose of providingadditional calories and electrolytes,provided the supplements do notcontain any NCAA banned substan-ces.’’ The NCAA Committee on Com-petitive Safeguards & Medical Aspectsof Sports has subsequently developedlists of permissible vs. non-permissiblenutritional supplements*, althoughthese will probably change as themarket continues to evolve and newproducts are evaluated.
*Note: According to the legislativeassistance section of the August 14,2000 NCAANews (vol. 37 no. 7; p. 24),there is an error on p. 209 of the 2000-01 NCAA Division I Manual. Thesecond sentence should read: ‘‘Permis-sible non-muscle-building nutritionalsupplements are identified accordingto the following classes: carbohydrate/
Strength and Conditioning Journal | www.nsca-lift.org 21

electrolyte drinks, energy bars, carbo-hydrate boosters, and vitamins andminerals.’’
INJURY TRENDS & STANDARD OFCARE LOAD: EFFECTS OF RISINGATHLETIC PARTICIPATION
The lack of qualified instruction andsupervision can be identified, eitherdirectly or indirectly, as a causativefactor in the available information oninjuries and litigations associated withweight training. In some cases this isclearly documented (41,67), while inothers it can be inferred. For example,the relatively high coach-to-athleteratio (and corresponding standard ofcare) in Olympic-style weightlifting isa likely reason for the low incidence ofinjury in this sport despite its technicaland athletic nature (30,77). Based onthe collective information summarizedbelow, it is difficult to overemphasizethe fundamental importance of quali-fied staffing in fulfilling the institution’sand Strength & Conditioning profes-sional’s shared legal duties for safety,supervision and standard of care.
Collegiate Settings.Year-round Strength & Conditioningactivities are now the rule rather thanthe exception in collegiate athleticprograms. According to NCAA dataon student-athlete participation (56),the overall number of participantsincreased 66% (from 231,445 to384,742) between 1981-82 and2004-05. Of special interest are thechanges in female participation duringthis period. The relative increase inwomen’s participation was 156% (from64,390 to 164,998) as compared with32% for men (from 167,055 to219,744); whereas absolute growthwas two-fold higher.
The total number of, and time ofparticipation in, athletically-related ac-tivities has also expanded accordingly.While desirable in terms of prepara-tion, the allowance of nontraditionalseasons, off-season skill instruction,and year-round Strength & Condition-ing activities increases each student-athlete’s liability exposure and potentialfor injury, as well as the corresponding
standard of care load placed on supportstaff. The NATA recently publisheda detailed overview of injury incidencein collegiate athletics, and found thatit has risen sharply and consistentlywith the increase in participants andexposures (73). The potential liabilityissues for Strength & Conditioningprofessionals and their employers arefurther compounded by the explosiverise in female participation, and lawsmandating equal opportunity andaccess to athletic programs, services,and facilities (refer to item 7).
Scholastic Settings.The sheer number of high schoolathletes, and growing emphasis onyear-round Strength & Conditioningactivities in scholastic settings, presentsa tremendous challenge in terms ofdemand for standard of care, and ac-companying liability exposure. Student-athlete participation in organized highschool sports increased 65.1% (fromless than 4 million to over 6.5 million)between 1971 and 1999-2000 (57).Of special interest are the changes infemale participation during this period.The relative increase in girls’ partici-pation was 810% (from about 0.3million to 2.7 million) as comparedwith 5% for boys (from about 3.7million to 3.9 million); whereas abso-lute growth was more than twelve-foldhigher.
As is the case in collegiate settings, thecombination of increasing participa-tion in athletic activities (especiallyamong females), a corresponding risein liability exposures, and laws man-dating equal opportunity and accesscreates a standard of care load — andchallenge in terms of legal duties — forStrength & Conditioning practitionersand their employers (refer to item 7).
Other Populations.Reeves et al. (67) performed a study ofNEISS data in 1986 and observed that,while serious injuries are relatively rare,an estimated 43,400 weight traininginjuries were evaluated/treated in hos-pital emergency departments out ofa total of 5.6 million visits for all sports.
By comparison, emergency room visitsfor weight training injuries in 1995totaled 56,400 out of more than 5.4million visits for all sports, representinga 9-year increase of approximately 30%.
Studies examining the incidence andtypes of weight training injury reportvarying injury rates, but similar distri-butions of injury types. Brown &Kimball (11) found that 39.4% ofcompetitive adolescent powerlifterssustained injuries in training, with aninjury rate of 0.0027 per 100 hours ofparticipation. In contrast, Risser et al.(68) observed that only 7.6% of ado-lescent football players in a supervisedweight training program sustainedinjuries. Zemper (90) found onlya 0.3% rate of weight training injuriesin a 4-year study of college footballplayers participating in supervisedtraining. While risk-factor studies ofacute weight training injuries are lack-ing, recognized contributing factorsinclude poor technique, lack of super-vision, skeletal immaturity, and steroidabuse (11, 53, 67a,68). Some of thesefactors are confirmed in the NSCA (22)and ACSM (23) published statementson youth resistance training. Chronicweight training injuries, on the otherhand, have been attributed to excessiveweight training and improper trainingtechniques (67b). Each of these factorscan be positively influenced withqualified instruction.
Jones et al. (41) conducted a 20-yearretrospective review of NEISS data onweight training injuries that wereevaluated and/or treated in U.S. hos-pital emergency departments fromOctober 1978 through December1998. An estimated 980,173 injuriesrelated to weight training activity orequipment occurred nationwide duringthe study period, representing a 35%increase over 20 years (note that thepopulation increased by 20% duringthe same period). While adolescent/young adult males (15-24 years old)-had the highest reported incidence ofinjury, alarming increases in injury ratewere reported for females and oldermales, most likely because of growingparticipation in these groups. Boys
VOLUME 31 | NUMBER 5 | OCTOBER 200922
Standards and Guidelines

(5-14 years old) were the only groupreporting a decline in injury rate. Themost common recorded venues ofinjury were the home (40.2%), sportsor recreation sites (17.8%) and school(9.4%). Based on available reports, themost common causes of injury appearto be unsafe behavior (63%), equip-ment malfunction (37%), lack of super-vision (30%) and inattention (10%).Once again, these factors can bepositively influenced with qualifiedinstruction and supervision.
Weight training injuries seem to beassociated with various methods (e.g.,bodybuilding, powerlifting, Olympic-style weightlifting, fitness/recreationalweight training) and equipment (e.g.,free weights, machines). Of these,explosive types of training and free-weight apparatus are often incorrectlybelieved to be inherently more dan-gerous than other methods. Hamill(30) conducted a survey of sport injuryrates in 13-16 year old school children,and found that the injury rate inweightlifting (0.0017 per 100 hours) iseven lower than that for weighttraining (0.0035 per 100 hours); andthat each of these injury rates weremuch lower than those observed forother, more popular sports (e.g., bas-ketball 0.03; football 0.10; gymnastics0.044; athletics 0.57). Stone et al. (77)reviewed the research literature oninjury potential and safety aspects ofOlympic-style weightlifting move-ments, and concluded that injuriesrelated to competitive weightliftingare neither excessive nor serious whencompared to other sports. Calhoon &Fry (13) analyzed weightlifting injuryreports at the U.S. Olympic TrainingCenters over a 6-year period, andfound that elite weightlifters’ injuriesare strains, tendinitis or sprains typicalof acute (59.6%) or chronic (30.4%)overuse or inflammation, rather thanrecurrences or complications. Therewere no indications of the traumaticproblems commonly observed in othersports. Injury rates were calculated tobe 3.3 per 1000 hours of weightliftingexposure, and the recommended num-ber of training days missed for most
(90.5%) injuries was one day. Theseauthors concluded that weightliftinginjury patterns and rates are similar tothose reported for other sports andactivities.
1. PRE-PARTICIPATIONSCREENING & CLEARANCE
STANDARD 1.1
Strength & Conditioning professionalsmust require participants to undergohealth care provider screening andclearance prior to participation, inaccordance with instructions specifiedby the AAFP-AAP-AMSSM-AOSSM-AOASM Pre-participation PhysicalEvaluation Task Force (64), the AHA& ACSM (8,52), as well as relevantgoverning bodies and/or their constit-uent members (e.g., the NCAA (63) forcollegiate athletes; state legislatures, orindividual state high school athleticassociations/districts for scholasticathletes). In most cases in the collegiateathletics environment, the AthleticTraining staff is involved in this processalong NATA guidelines. In recreationalactivity programs, Strength & Condi-tioning professionals must require par-ticipants to undergo pre-participationscreening and clearance in accordancewith AHA & ACSM recommenda-tions (8,52). For children, the clearancedecision must include a determinationor certification that the child hasreached a level of maturity allowingparticipation in such activities as ad-dressed in the ‘‘Participation inStrength & Conditioning Activitiesby Children’’ standards statement (re-fer to item 8).
GUIDELINE 1.1
Strength & Conditioning professionalsshould cooperate with a training par-ticipant’s health care providers at alltimes, and provide service in the par-ticipant’s best interest according to in-structions specified by such providers.
2. PERSONNEL QUALIFICATIONS
GUIDELINE 2.1
The Strength & Conditioning practi-tioner should acquire a bachelor’s ormaster’s degree from a regionallyaccredited college or university
(verification by transcript or degreecopy) in one or more of the topicscomprising the ‘‘Scientific Foun-dations’’ domain identified in theCertified Strength & ConditioningSpecialist� (CSCS�) ExaminationContent Description (58) (AppendixA), or in a relevant subject. An ongoingeffort should also be made to acquireknowledge and skill in the othercontent areas.
GUIDELINE 2.2
The Strength & Conditioning practi-tioner should achieve and maintainprofessional certification(s) with con-tinuing education requirements anda code of ethics, such as the CSCS�
credential offered through the NSCA(Appendix B). Depending on thepractitioner’s scope of activities, re-sponsibilities, and knowledge require-ments, relevant certifications offered byother governing bodies may also beappropriate.
GUIDELINE 2.3
The productivity of a Strength &Conditioning staff, as well as learningand skill development of individualmembers, should be enhanced byaligning a performance team com-prised of qualified practitioners withinterdependent expertise and sharedleadership roles (Appendix C). Oncethe team is assembled, respectiveactivities and responsibilities from the‘‘Practical/Applied’’ domain identifiedin the Certified Strength & Condition-ing Specialist� (CSCS�) ExaminationContent Description 58 (Appendix A),as well as appropriate liaison assign-ments, should be delegated accordingto each member’s particular ‘‘ScientificFoundations’’ expertise.
3. PROGRAM SUPERVISION &INSTRUCTION
STANDARD 3.1
Strength & Conditioning programsmust provide adequate and appropriatesupervision with well-qualified andtrained personnel, especially duringpeak usage times. To achieve maxi-mum health, safety, and instruction,Strength & Conditioning professionalsmust be present during Strength &
Strength and Conditioning Journal | www.nsca-lift.org 23

Conditioning activities; have a clearview of the entire facility (or at least thezone being supervised by each practi-tioner) and the participants in it; bephysically close enough to the partic-ipants under their supervision to beable to see and clearly communicatewith them; and have quick access tothose in need of spotting or assistance.
STANDARD 3.2
In conjunction with appropriate safetyequipment (e.g. power racks), attentivespotting must be provided for partici-pants performing activities where freeweights are supported on the trunkor moved over the head/face (referto Earle & Baechle [Chapter (14),pp. 325-376] in Essentials Of StrengthTraining & Conditioning (7)).
GUIDELINE 3.1
Strength & Conditioning activitiesshould be planned, and the requisitenumber of qualified staff (refer toitem 2) should be available such thatrecommended guidelines for minimumaverage floor space allowance perparticipant (100 ft2), professional-to-participant ratios (1:10 junior highschool, 1:15 high school, 1:20 college),and number of participants per barbellor training station (3) are achievedduring peak usage times (5,7,38,42).Younger participants, novices or spe-cial populations engaged in suchStrength & Conditioning activitiesshould be provided with greater su-pervision (refer to item 8). Strength &Conditioning practitioners and theiremployers should work togethertoward a long-term goal of matchingthe professional-to-participant ratio inthe Strength & Conditioning facilityto each sport’s respective coach-to-athlete ratio (e.g., refer to Appendix F).
4. FACILITY & EQUIPMENT SET-UP,INSPECTION, MAINTENANCE,REPAIR & SIGNAGE
STANDARD 4.1
Exercise devices, machines and equip-ment, including free weights, mustbe assembled, set up and placed inactivity areas in full accordance withmanufacturer’s instructions, tolerancesand recommendations; and with
accompanying safety signage, instruc-tion placards, notices and warningsposted or placed according to ASTMstandards (3,4) so as to be noticed byusers prior to use. In the absence ofsuch information, professionals mustcomplete these tasks in accordancewith authoritative information avail-able from other sources.
STANDARD 4.2
Prior to being put into service, exercisedevices, machines or free weights mustbe thoroughly inspected and tested byStrength & Conditioning professionalsto ensure that they are working andperforming properly, and as intendedby the manufacturer.
STANDARD 4.3
Exercise machines, equipment andfree weights must be inspected andmaintained at intervals specified bymanufacturers. In the absence ofsuch specifications, these items mustbe regularly inspected and maintainedaccording to the Strength & Condi-tioning practitioner’s professionaljudgment.
STANDARD 4.4
Exercise devices, machines, equipmentand free weights which are in need ofrepair, as determined by regular in-spection or as reported by users, mustbe removed from service and taken outof use until serviced and repaired; andbe re-inspected and tested to ensurethat they are working and performingproperly before being returned to ser-vice. If such devices are involved inincidents of injury, legal advisors or riskmanagers must be consulted for adviceprior to service/repair or destruction.
GUIDELINE 4.1
Strength & Conditioning professionalsand their employers should ensure thatfacilities are appropriate for Strength &Conditioning activities. Factors to bereviewed and approved prior to activ-ity include, but are not limited to,floor surface, lighting, room tempera-ture and air exchange (refer to Green-wood [Chapter 21, pp. 543-568] inEssentials Of Strength Training &Conditioning (7)).
GUIDELINE 4.2
Manufacturer provided user’s manuals,warranties and operating guides shouldbe preserved and followed (refer toitem 6).
GUIDELINE 4.3
All equipment, including free weights,should be cleaned and/or disinfectedregularly as deemed necessary by staff.Users should be encouraged to wipedown skin-contact surfaces aftereach use.
5. EMERGENCY PLANNING &RESPONSE
STANDARD 5.1
Strength & Conditioning professionalsmust be trained and certified in currentguidelines for cardiopulmonary resus-citation (CPR) established by AHA/ILCOR (2); as well as universal pre-cautions for preventing disease trans-mission established by the CDC (14)and OSHA (60). First Aid training/certification is also necessary if SportsMedicine personnel (e.g., MD or ATC)are not immediately available duringStrength & Conditioning activities.New staff engaged in Strength &Conditioning activities must complywith this standard as soon as possibleafter employment.
STANDARD 5.2
Strength & Conditioning professionalsmust develop a written, venue-specificemergency response plan to deal withinjuries and reasonably foreseeableuntoward events within each facility.The plan must be posted at strategicareas within each facility, and practicedand rehearsed at least quarterly. Theemergency response plan must beinitially evaluated (e.g., by facility riskmanagers, legal advisors, medical pro-viders and/or off-premise emergencyresponse agencies) and modified asnecessary at regular intervals. As partof the plan, a readily accessible andworking telephone must be immedi-ately available to summon on-premiseand/or off-premise emergency re-sponse resources.
GUIDELINE 5.1
The components of a written andposted emergency response plan
VOLUME 31 | NUMBER 5 | OCTOBER 200924
Standards and Guidelines

should include: planned access to aphysician and/or emergency medicalfacility when warranted, including aplan for communication and trans-portation between the venue and themedical facility; appropriate and nec-essary emergency care equipment on-site that is quickly accessible; and athorough understanding of the person-nel and procedures associated with theplan by all individuals (e.g., refer toAppendix G).
6. RECORDS & RECORD KEEPING
GUIDELINE 6.1
In conjunction with written policiesand procedures, Strength & Condi-tioning professionals should developand maintain various records includ-ing: manufacturer-provided user’smanuals, warranties and operatingguides; equipment selection, purchase,installation, set-up, inspection, mainte-nance and repair records; personnelcredentials; professional standards andguidelines; safety policies and proce-dures, including a written emergencyresponse plan (refer to item 5); traininglogs, progress entries and/or activityinstruction/supervision notes; injury/incident reports, pre-participationmedical clearance, and return to par-ticipation clearance documents. Insettings where participants are nototherwise required to sign protectivelegal documents (e.g., informed con-sent, agreement to participate, waiver;refer to Appendix H) covering allathletically related activities, theStrength & Conditioning professionalshould have such legal documentsprepared for participants under his/hersupervision. These records should bepreserved and maintained for a periodof time determined by professionallegal advice and consultation.
7. EQUAL OPPORTUNITY &ACCESS
STANDARD 7.1
Strength & Conditioning professionalsand their employers must providefacilities, training, programs, servicesand related opportunities in accor-dance with all laws, regulations and
requirements mandating equal oppor-tunity, access and non-discrimination.Such federal, state and possibly locallaws and regulations apply to mostorganizations, institutions and profes-sionals. Discrimination or unequaltreatment based upon race, creed,national origin, sex, religion, age, handi-cap/disability or other such legalclassifications is generally prohibited.
8. PARTICIPATION IN STRENGTH &CONDITIONING ACTIVITIES BYCHILDREN
GUIDELINE 8.1
Children under seven (7) years of ageshould not be permitted to engage inStrength & Conditioning activitieswith free weights or exercise devices/machines in facilities designed for useby adults and adolescents, and shouldbe denied access to such training areas.Other forms of Strength & Condition-ing activities may be beneficial for suchchildren, and should be recommendedaccording to the practitioner’s pro-fessional judgment, and with a greaterdegree of instruction and supervisionthan that supplied to adolescents andadults. Children participating in suchactivities should be cleared as specifiedin the NSCA’s ‘‘Standard for Pre-participation Screening & Clearance’’(refer to item 1).
GUIDELINE 8.2
Children between seven (7) and four-teen (14) years of age who havereached a level of maturity allowingparticipation in specified Strength &Conditioning activities, as determinedand certified by their medical careprovider (or by the Strength & Con-ditioning professional acting in concertwith a child’s medical care provider),and after clearance for participation asspecified in the NSCA’s ‘‘Standard forPre-participation Screening & Clear-ance’’ (refer to item 1), should beindividually assessed by the Strength& Conditioning professional in con-junction with the child’s parent(s)/guardian(s)/custodian(s) and healthcare provider(s)to determine if suchchildren may engage in such activitiesin areas containing free weights and
exercise devices/machines generallyused by adults and older children. Ifso permitted, such activities should bedeveloped and implemented accordingto the practitioner’s professional judg-ment, in conjunction with the child’shealth care provider(s), and with agreater degree of instruction and super-vision than that supplied to adolescentsand adults.
GUIDELINE 8.3
Children fourteen (14) years of age andolder who, according to the Strength &Conditioning practitioner’s profes-sional judgment, have reached a levelof maturity allowing them to engage inspecified Strength & Conditioningactivities (provided they have beencleared for participation as specifiedin the NSCA’s ‘‘Standard for Pre-participation Screening & Clearance’’;refer to item 1), may engage in suchactivities in areas containing freeweights and exercise devices/machinesgenerally used by adults, and with agreater degree of instruction andsupervision than that supplied to adultpopulations while training.
9. SUPPLEMENTS, ERGOGENICAIDS & DRUGS
STANDARD 9.1
Strength & Conditioning professionalsmust not prescribe, recommend orprovide drugs, controlled substancesor supplements that are illegal, pro-hibited, or harmful to participants forany purpose including enhancing ath-letic performance, conditioning orphysique. Only those substances thatare lawful and have been scientificallyproven to be beneficial, or at least notharmful, may be recommended orprovided to participants by Strength& Conditioning professionals, and onlyto individuals age 18 or above.
APPENDIX A. STRENGTH &CONDITIONING PRACTITIONERDEFINITION
In 1996, and again in 2004,the NSCA Certification Depart-ment (www.nsca-cc.org) and its
Strength and Conditioning Journal | www.nsca-lift.org 25

examination service (APPLIED MEA-SUREMENT PROFESSIONALS)conducted a Job Analysis study withthe purpose of surveying the activi-ties, responsibilities, and knowledgerequirements of a Certified Strength &Conditioning Specialist� (CSCS�).The results were used to describethe job activities of the CSCS insufficient detail to provide a basis forthe development of a professional,job-related certification examinationthat will certify S&C specialists ascompetent professionals. An earlystep in the process was to createa ‘‘practitioner definition’’. Essen-tially, this definition is a job de-scription that establishes the legaland professional scope of practiceof the appropriate activities ofa CSCS (refer to Appendix B): (6,7).
Certified Strength & Condi-tioning Specialists are professionalswho practically apply foundationalknowledge to assess, motivate, edu-cate, and train athletes for theprimary goal of improving sportperformance. They conduct sport-specific testing sessions, designand implement safe and effectivestrength training and conditioningprograms, and provide guidance forathletes in nutrition and injury pre-vention. Recognizing their area ofexpertise is separate and distinctfrom the medical, dietetic, athletictraining, and sport coaching fields,Certified Strength & ConditioningSpecialists consult with and referathletes to these professionals whenappropriate.
The CSCS Job Analysis studyevaluated the results of a question-naire sent to 1,020 randomly selec-ted NSCA members who wereCSCS-certified as of October1996. Respondents were asked toassign an importance to 112 tasksthat a CSCS typically performs onthe job. From this data, the NSCA’sCSCS Job Analysis Committee de-termined the inclusion criteria of thetasks (5 of the original 112 wereexcluded), the distribution of taskswithin each CSCS exam domain andits subcategories, as well as distri-bution of the exam question type (i.e.recall, application, and analysis)
within each domain and its subca-tegories. The document resultingfrom the CSCS Job Analysis studyis the ‘‘CSCS Examination ContentOutline’’ (refer to the abbreviatedsummary below), which forms thebasis for the Certified Strength &Conditioning Specialist (CSCS) Ex-amination Content Description (58),an exam preparation resource avail-able through the NSCA. The 2004questionnaire was sent to 770employers of certified individualsand the new results were used tochange the format of the exam, withmore emphasis placed on the prac-tical/applied section.
CSCS� EXAMINATION CONTENTOUTLINE
Adapted from: CertifiedStrength & Conditioning Specialist
�
(CSCS�) Examination Content De-
scription (59)
Scientific Foundations.I. Exercise Sciences (57 questions)
A. Develop training programsthat demonstrate an under-standing of human musclephysiology.
B. Develop training programsthat demonstrate an under-standing of human neuromus-cular adaptations.
C. Develop training programsthat demonstrate an under-standing of the basic princi-ples of human biomechanicswith respect to exercise selec-tion, execution, and sportperformance.
D. Develop training programsthat demonstrate an under-standing of human bone, mus-cle, and connective tissueadaptations.
E. Develop training programsthat demonstrate an under-standing of human bioenerget-ics and metabolism.
F. Develop training programs thatdemonstrate an understandingof human neuroendocrineresponses.
G. Develop training programsthat demonstrate an under-standing of human cardio-
pulmonary anatomy andphysiology.
H. Develop training programsthat demonstrate an under-standing of acute and chronicphysiological responses andadaptations to aerobic andanaerobic exercise.
I. Develop training programs thatdemonstrate an understandingof the anatomical, physiologi-cal, and biomechanical differ-ences of athletes.
J. Use sport psychology techni-ques to enhance the trainingand/or performance of anathlete.
K. Explain the effects, risks, andalternatives of various perfor-mance-enhancing substancesand methods.
II. Nutrition (23 questions)A. Explain nutritional factors af-
fecting health andperformance.
B. Explain the techniques to ma-nipulate food choices and train-ing methods to maximizeperformance.
C. Recognize signs, symptoms,and behaviors associated witheating disorders.
D. Recognize the nature of anathlete’s nutritional status anddetermine the appropriate-ness of a referral to a regis-tered dietician or relatednutritional professional.
III. New ‘‘untried’’ questions (10 non-scored questions)
Practical/Applied.I. Program Design (40 questions)
A. Design training programs thatmaximize performance by pre-scribing various training meth-ods and modes based uponan athlete’s health status,strength and conditioning lev-els, and training goals.
B. Design training programs thatmaximize performance by se-lecting exercises based uponan athlete’s health status,strength and conditioning lev-els, and training goals.
C. Design training programs thatmaximize performance by
VOLUME 31 | NUMBER 5 | OCTOBER 200926
Standards and Guidelines

applying the principles of exer-cise order based upon anathlete’s health status, strengthand conditioning levels, andtraining goals.
D. Design training programs thatmaximize performance by de-termining and prescribing ap-propriate loads/resistances(including heart rate guide-lines)based upon an athlete’shealth status, strength andconditioning levels, and train-ing goals.
E. Design training programs thatmaximize performance by de-termining and prescribing ap-propriate volumes (defined assets x reps) based upon anathlete’s health status, strengthand conditioning levels, andtraining goals.
F. Design training programs thatmaximize performance by de-termining and prescribing ap-propriate work/duration andrest periods and training fre-quencies based upon an ath-lete’s health status, strengthand conditioning levels, andtraining goals.
G. Design training programs thatmaximize performance by uti-lizing the principles ofperiodization.
H. Design training programs thatmaximize performance and/ordecrease injury susceptibilityby prescribing exercises todevelop and/or maintain mus-cular balance between antag-onistic muscles, musclegroups, and/or body parts.
I. Communicate with the athleticmedicine staff and/or medicalprofessional to coordinate therehabilitation/reconditioningof an athlete.
II. Exercise Techniques (39 questions)A. Describe and instruct flexibility
exercises.B. Describe and instruct condi-
tioning exercises.C. Describe and instruct plyo-
metric exercises.D. Describe and instruct strength/
power training exercises.
E. Describe and instruct spottingprocedures.
III. Organization & Administration (11questions)
A. Establish policies and proce-dures associated with the day-to-day operation of thestrength and conditioningfacility.
B. Determine the layout of thefacility for effective use of timeand space.
C. Maintain equipment and facil-ity to provide a safe trainingenvironment.
IV. Testing & Evaluation (20 questions)A. Select and administer appro-
priate tests to maximize testreliability and validity.
B. Evaluate and identify the sig-nificance of testing results.
V. New ‘‘untried’’ questions (10 non-scored questions)
APPENDIX B. CERTIFIEDSTRENGTH & CONDITIONINGSPECIALIST
�(CSCS
�)
The CSCS certification examprogram was initiated in 1985 toidentify individuals who possess theknowledge and skills to design andimplement safe and effectiveStrength & Conditioning programs.This certification program encour-ages a higher level of competenceamong practitioners, which in turn,raises the quality of strength trainingand conditioning programs to ath-letes by those who are CSCS-certified.
The CSCS educates andtrains primarily athletes in properstrength training and conditioningpractices. These professionals area diverse group; however, the pri-mary practitioners are Strength &Conditioning coaches, athletic train-ers, and physical therapists. CSCSprofessionals work in a variety ofenvironments, including high school,college, university and professionalinstitutions, Sports Medicine clinics,health and fitness clubs, corporatewellness centers, and in professionalsports. Competencies assessed inthe four-hour CSCS examinationwere determined via a national task
analysis conducted by an indepen-dent professional examination ser-vice. Thus, Strength & Conditioningprofessionals identified the compe-tency areas. Every step in the pro-cess leading to the development ofvalid certification exams met theNCCA’s stringent guidelines. Pass/fail rates and reliability statistics arepublished annually. The NSCA’sCertification Exam Program is theonly fitness-related certification pro-gram to provide public disclosure ofthis information.
Writers of the exams includerenowned practitioners, researchers,educators, and psychometricians.While there are many certificationprograms associated with physicaltraining, the CSCS certification ex-amination program was the firstspecifically designed to assess thecompetencies of those who strengthtrain and condition athletes.
ACCREDITATION
In 1993 the NSCA certifica-tion exam program became the first,and is still accredited by the es-teemed NATIONAL COMMISSIONFOR CERTIFYING AGENCIES*.The rigorous CSCS and NSCACertified Personal Trainer� (NSCA-CPT) examinations are the mostchallenging in the industry.*Note: The NCCA is the accredita-tion body of the NATIONAL ORGA-NIZATION FOR COMPETENCYASSURANCE, a non-profit non-gov-ernment agency that promotes ex-cellence in competency assurancefor practitioners in all occupationsand professions. The NCCA meas-ures the ability of certifying organ-izations in any industry to accuratelydiscriminate between qualified andunqualified professionals. To earnNCCA recognition, a credentialingbody must demonstrate an ability todevelop and administer psychomet-rically sound examinations that ef-fectively discriminate betweenqualified and unqualified professio-nals through a series of criteria,including:� The certifying organization is non-profit; and is responsible for alldecisions pertaining to certifica-tion and recertification (including,
Strength and Conditioning Journal | www.nsca-lift.org 27

but not limited to, examinationcontent, eligibility requirements,grievance and disciplinary poli-cies, setting fees, program opera-tion, etc.) without being subject toapproval by any other body.
� The examination is developedfrom job analysis data gatheredfrom a national study.
� Pass/fail rates and reliability sta-tistics are a matter of publicrecord.
� Examination development involvesqualified professionals, such ascontent experts and psychometri-cians with expertise in examdevelopment.
CSCS EXAMINATION FORMAT
To earn the CSCS credential,candidates must either pass a rigor-ous written examination or computerbased exam that consists of twosections. Candidates are alloweda maximum time of four hours tocomplete this examination process.A candidate must pass both sec-tions to be CSCS-certified (and mayretake any section not passed). Thefirst section, referred to as ‘‘Scien-tific Foundations’’, consists of 90multiple-choice questions in theareas of:� Exercise Sciences (Anatomy, Ex-ercise Physiology, Biomechanics)
� NutritionThe second section, ‘‘Practi-
cal/Applied’’, consists of 120 multi-ple-choice questions, 40 of whichinvolve viewing a videotape andanswering questions associatedwith the exercises, muscles and/orjoints shown. The areas coveredinclude:� Basic & Advanced ProgramDesign
� Exercise Technique� Organization & Administration� Testing & Evaluation
CONTINUING EDUCATIONPROGRAM
The purpose of having con-tinuing education as part of a certifi-cation program is to encouragecertificants to stay abreast of evolv-ing knowledge and skills in theprofession, and, in doing so, topromote the ongoing competency
of those who are certified. In order toremain certified, the NSCA requireseach certificant to do the followingto remain certified:� Complete six (6.0) CEUs or a pro-rated amount of CEUs if certifiedwithin the three-year reportingperiod.
� Submit a completed CEU Report-ing Form and recertification fee.
� Maintain documentation of activi-ties listed on the CEU ReportingForm.
NSCA Code of Ethics forCertificant: With the credibility pos-sessed by the CSCS and NSCA-CPT examinations comes the re-sponsibility to ensure the integrity ofthe credentials awarded. The Codeof Ethics of the NSCA was estab-lished to make its certificants, CSCSand NSCA-CPT, aware of the stand-ards of ethical behavior that shouldbe followed in the practice of theirprofession (strength training andconditioning and personal training).The Code presents fundamentalstandards of behavior that all certif-icants should strive to achieve. Itserves to increase ethical sensitivityand judgment, strengthen supportfor certificants’ moral courage andsharpen their sense of identity as anintegral part of the NSCA and itscontinued success.
The NSCA is committed tocertifying individuals who demon-strate the knowledge and skillsnecessary to design and implementsafe and effective strength trainingand conditioning and personal train-ing practices. The NSCA also be-lieves that continuing educationencourages individuals to stayabreast of evolving knowledge andskills, and, in doing so, promotestheir ongoing competency. Thisphilosophy implies that the respon-sibility of its certificants is not limitedto the well being of the athletesand/or clients, but also to society ingeneral and the reputation of othersin their field; with the overall goalbeing an improvement of health andwell being for all.
The NSCA is dedicated tomaintaining a high standard forcertificants. The following Code of
Ethics assures that CSCS andNSCA-CPT certificants are awareof the standards of ethical behaviorthat should be followed in thepractice of their profession. Certifi-cants shall:1. Respect the rights, welfare, and
dignity of all individuals.2. Strive to provide equal and fair
treatment to all individuals andnot discriminate against anyone.
3. Provide and maintain a safe andeffective training environment.
4. Comply with all general laws ofthe land including, but not limitedto, applicable business, employ-ment and copyright laws.
5. Accept responsibility for the useof sound judgment when workingwith their clientele.
6. Respect the confidentiality oftheir clientele while remainingaccountable.
7. Refer their clientele to more qual-ified fitness, medical, or healthprofessionals when appropriate.
8. Remain current on practical andtheoretical foundations throughcontinuing education activities.
9. Avoid engaging in any behavior orform of conduct that would con-stitute a conflict of interest oractions that adversely reflect onthe profession or the NATIONALSTRENGTH & CONDITIONINGASSOCIATION.
10. Strive to safeguard the public byreporting violations of this Codeof Ethics.
APPENDIX C. STRENGTH &CONDITIONING PERFORMANCETEAM DEVELOPMENT
Katzenbach & Smith (43) de-fine a team as ‘‘a small number ofpeople with complementary skillswho are committed to a commonpurpose, performance goals, andapproach for which they hold them-selves mutually accountable.’’Teams are preferable to single-leader groups when there is a needfor collective work products (i.e. mul-tiple skills, judgments and experien-ces) by members working togetherin real time, shifting leadershiproles, and mutual as well as indi-vidual accountability. In contrast,
VOLUME 31 | NUMBER 5 | OCTOBER 200928
Standards and Guidelines

single-leader/hierarchical workgroups are appropriate when thesum of independent workers’ con-tributions is adequate, singularrather than shared leadership iseffective, task(s) and correspondingsolution(s) are familiar, workers’skills can be applied productivelywithout interaction (other than shar-ing information), and speed andefficiency have priority over extraperformance results (43,44).
Extraordinarily demandingchallenges are the driving forcesbehind high-performance teams.Common features of such teamsinclude: (43,44)� Members are committed to a clearmission, common approach, col-laboration, and mutual account-ability and responsibility.
� Expectations and goals are highbut achievable, and performanceevaluation is based on results.
� Roles are interdependent; leader-ship is shared; abilities, experien-ces, expertise, knowledge, skills
and talents are complementary;contribution, participation and in-fluence are balanced.
� Effective task performance is fa-cilitated by encouraging and re-warding creativity, innovation andrisk taking in all decision making orproblem solving activities.
When aligning a Strength &Conditioning staff, the performanceteam concept can be applied byhiring practitioners with expertiseand formal education in one or moreof the topics comprising the ‘‘Sci-entific Foundations’’ domain (58)(Appendix A) or a related subject.Once the team is assembled, corre-sponding activities and responsibil-ities comprising the ‘‘Practical/Applied’’ domain (58) (AppendixA), as well as liaison assignments,can be delegated. In addition toexploiting greater collective exper-tise, this approach provides eachpractitioner with an opportunity toaugment knowledge and skill acqui-sition in areas outside of his/her
specialty. The Strength & Condition-ing coordinator is still ultimatelyresponsible for overseeing all as-pects of the program, and for de-termining appropriate utilization ofassociates/assistants in the provision of safe,effective and efficient service. Spe-cific duties and responsibilities canbe assigned according to specialtyareas or subdisciplines, in much thesame way a sport coaching stafftypically has offensive/defensive co-ordinators, liaison assignments, etc.Table C is an example of how toalign a Strength & Conditioningperformance team.
APPENDIX D. STRENGTH &CONDITIONING FACILITYSCHEDULING
See Table D.
APPENDIX E. STRENGTH &CONDITIONING TRAINING PLANDEVELOPMENT
A detailed discussion of de-veloping a Strength & Conditioning
Table CSample strength and conditioning performance team
Scientific FoundationsEducation/Expertise
Practical & AppliedActivities/Responsibilities Liaison Assignment(s)
Exercise/Sport Anatomy;Biomechanics
Exercise Technique; Testing & Evaluation;Rehabilitation & Reconditioning*
Exercise & Sport Science Faculty;Team Coaches; Sports Medicine Team
Exercise/Sport Physiology Program Design; Testing & Evaluation Exercise & Sport Science Faculty;Team Coaches
Exercise/Sport Nutrition Nutritionist Exercise & Sport Science Faculty
Exercise/Sport Pedagogy Program Design; Exercise Technique;Organization & Administration
Exercise & Sport Science Faculty;Athletic Administration
Exercise/Sport Psychology;Motor Learning
Exercise Technique; Rehabilitation &Reconditioning*
Exercise & Sport Science Faculty;Sports Medicine Team
Training Methodology Program Design; Organization &Administration
Exercise & Sport Science Faculty;Athletic Administration
Kinesiology; Physiotherapy;Sports Medicine
Rehabilitation & Reconditioning* Sports Medicine Team
*One area to carefully consider is that of a Rehabilitation & Reconditioning specialist, i.e. a member of the performance team who worksspecifically with injured/modified athletes to reduce risk of re-injury and facilitate return to full activity (Potach & Grindstaff )[Chapter 20, pp 523-540] in Essentials Of Strength Training & Conditioning (7). Due to such athletes’ increased need for care, it is impractical, especially during peakusage times, for Strength & Conditioning professionals to work with injured or modified participants while simultaneously instructing/supervisinglarger groups. In some situations, the Strength & Conditioning and Sports Medicine facilities are adjacent (or shared), with natural crossover inrespective activities and responsibilities. In many others, however, they are separated; and there is an opportunity to improve interaction andcommunication, and resulting provision of care for injured/modified athletes. In either case, the Rehabilitation & Reconditioning specialist wouldbe an appropriate choice for liaison between the Strength & Conditioning and Sports Medicine staff.
Strength and Conditioning Journal | www.nsca-lift.org 29

training plan is beyond the scopeof this project. For more specificinformation on program design,the Strength & Condition-ing practitioner should refer toSection 4 (Chapters 15–20) ofEssentials of Strength Training &Conditioning (7) as well as theNSCA position linked below. Addi-tional information on fundamentaltraining principles and their prac-tical implications is also avail-able through other resources(1,7,10,15,21,22,24–27,31,32,39,40,42,45–47,55,59,62,69–72,74–76,78–82,84–89).
NSCA Position StatementSummaries
[http://www.nsca-lift.org/Publications/posstatements.shtml]
Basic Guidelines for theResistance Training of Athletes(61)
Strength Training ForFemale Athletes (40)
The Squat Exercise inAthletic Conditioning (15)
Anabolic-Androgenic Ste-roid (AAS)Use By Athletes (87)
Explosive Exercises &Training (76)
Explosive/Plyometric Ex-ercises (86)
Youth Resistance Training(22)
APPENDIX F. NCAA DIVISION IATHLETE-TO-COACH RATIOS
See Tables F1–F3.
APPENDIX G. EMERGENCY CARE &PLANNING
Source: Guideline 1f [pp. 16–17], NCAA Sports Medicine Hand-book (63)
EMERGENCY CARE
Reasonable attention to allpossible preventive measures willnot eliminate sports injuries. Eachscheduled practice or contest of aninstitution-sponsored intercollegiateathletics event, as well as out-of-season practices and skills sessions,should include an emergency plan.
Like student-athlete welfare in gen-eral, a plan is a shared responsibilityof the athletics department; admin-istrators, coaches and medical per-sonnel who should all play a role inthe establishment of the plan, pro-curement of resources and under-standing by all parties. Componentsof such a plan should include:1. The presence of a person quali-
fied and delegated to renderemergency care to a strickenparticipant;
2. The presence or planned accessto a physician for prompt medicalevaluation of the situation, whenwarranted;
3. Planned access to a medicalfacility, including a plan for com-munication and transportationbetween the athletics site andthe medical facility for prompt med-ical services, when warranted.Access to a working telephoneor other telecommunicationsdevice, whether fixed or mobile,should be assured;
Table DCalculations for space needs. Source: Greenwood (Chapter 21 [pp. 543-568], Essentials of
strength training & conditioning (7))
Area Examples Formula
Prone/supine exercises Bench press; Lying tricepsextension
Actual weight bench length (6-8 ft.) + safety spacecushion of 3 ft. multiplied by suggested user space forweight bench width of 7 ft. + safety cushion of 3 ft.
Example: If using a 6 ft. long weight bench for the benchpress exercise (6 ft. + 3 ft.) x (7 ft. + 3 ft.) = 90 ft2.
Standing exercises Bicep curl; Upright row Actual bar length (4-7 ft.) + double-wide safety spacecushion of 6 ft. multiplied by suggested user spacefor standing exercise width of 4 ft.
Example: If using a 4 ft. curl bar for the bicep curlexercise (4 ft. + 6 ft.) x (4 ft.) = 40 ft2.
Standing exercises from rack Back squat; Shoulder press Actual bar length (5-7 ft.) + double-wide safety spacecushion of 6 ft. multiplied by suggested user space forstanding exercise from a rack width of 8-10 ft.
Example: If using a 7 ft. Olympic bar for the backsquat exercise (7 ft. + 6 ft.) x (10 ft.) = 130 ft2.
Olympic lifting area Power clean Lifting platform length (typically 8 ft.) + perimeterwalkway safety space cushion of 4 ft. multipliedby lifting platform width (typically 8 ft.) + perimeterwalkway safety space cushion of 4 ft.
Example: (8 ft. + 4 ft.) x (8 ft. + 4 ft.) = 144 ft2.
VOLUME 31 | NUMBER 5 | OCTOBER 200930
Standards and Guidelines
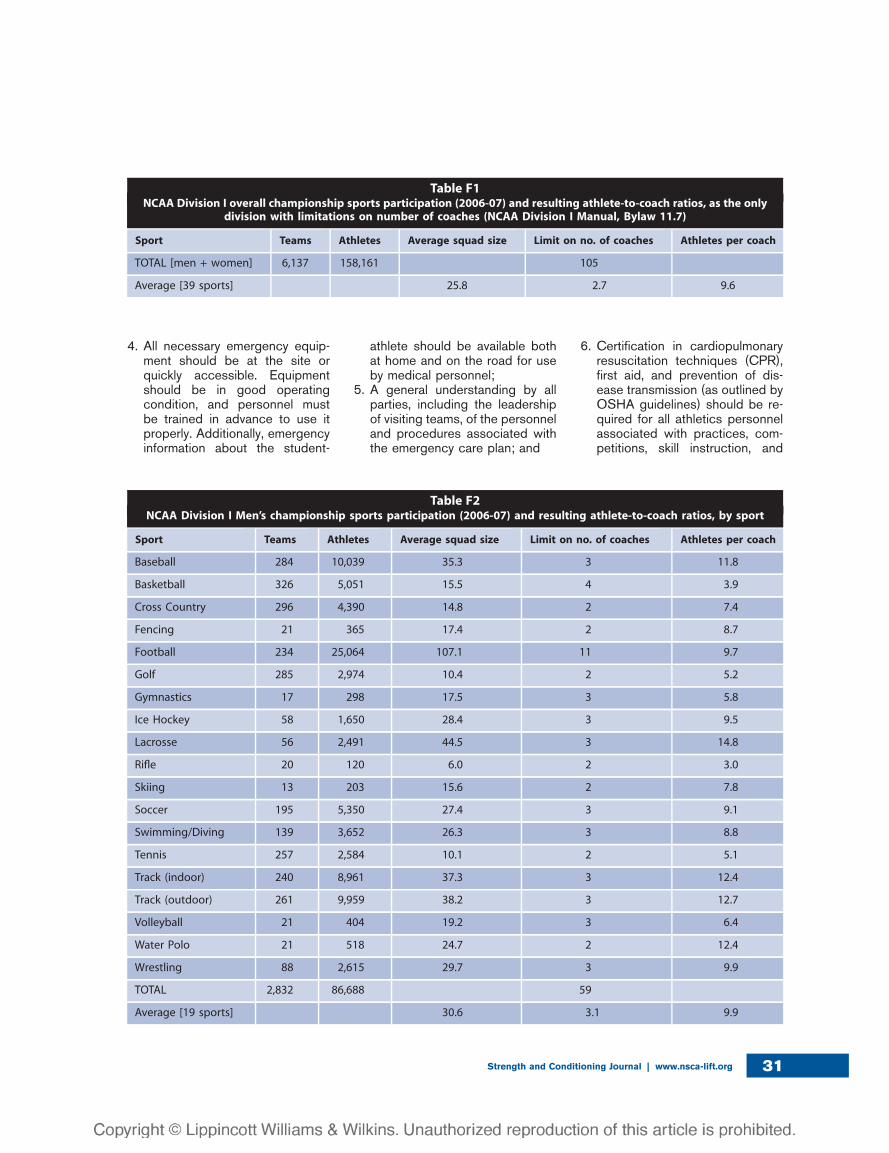
4. All necessary emergency equip-ment should be at the site orquickly accessible. Equipmentshould be in good operatingcondition, and personnel mustbe trained in advance to use itproperly. Additionally, emergencyinformation about the student-
athlete should be available bothat home and on the road for useby medical personnel;
5. A general understanding by allparties, including the leadershipof visiting teams, of the personneland procedures associated withthe emergency care plan; and
6. Certification in cardiopulmonaryresuscitation techniques (CPR),first aid, and prevention of dis-ease transmission (as outlined byOSHA guidelines) should be re-quired for all athletics personnelassociated with practices, com-petitions, skill instruction, and
Table F1NCAA Division I overall championship sports participation (2006-07) and resulting athlete-to-coach ratios, as the only
division with limitations on number of coaches (NCAA Division I Manual, Bylaw 11.7)
Sport Teams Athletes Average squad size Limit on no. of coaches Athletes per coach
TOTAL [men + women] 6,137 158,161 105
Average [39 sports] 25.8 2.7 9.6
Table F2NCAA Division I Men’s championship sports participation (2006-07) and resulting athlete-to-coach ratios, by sport
Sport Teams Athletes Average squad size Limit on no. of coaches Athletes per coach
Baseball 284 10,039 35.3 3 11.8
Basketball 326 5,051 15.5 4 3.9
Cross Country 296 4,390 14.8 2 7.4
Fencing 21 365 17.4 2 8.7
Football 234 25,064 107.1 11 9.7
Golf 285 2,974 10.4 2 5.2
Gymnastics 17 298 17.5 3 5.8
Ice Hockey 58 1,650 28.4 3 9.5
Lacrosse 56 2,491 44.5 3 14.8
Rifle 20 120 6.0 2 3.0
Skiing 13 203 15.6 2 7.8
Soccer 195 5,350 27.4 3 9.1
Swimming/Diving 139 3,652 26.3 3 8.8
Tennis 257 2,584 10.1 2 5.1
Track (indoor) 240 8,961 37.3 3 12.4
Track (outdoor) 261 9,959 38.2 3 12.7
Volleyball 21 404 19.2 3 6.4
Water Polo 21 518 24.7 2 12.4
Wrestling 88 2,615 29.7 3 9.9
TOTAL 2,832 86,688 59
Average [19 sports] 30.6 3.1 9.9
Strength and Conditioning Journal | www.nsca-lift.org 31
Strength & Conditioning. Newstaff engaged in these activitiesshould comply with these ruleswithin six months of employment.
EMERGENCY PLAN EXAMPLETEMPLATE
Acknowledgment.The following emergency plan
template was developed by RonCourson (Director of Sports Medi-cine, University of Georgia; Chair,NATA College/University AthleticTrainers’ Committee) and the Uni-versity of Georgia Sports Medicinestaff. This document provides a start-ing point for institutional
development of individualized emer-gency plans for all athletics activities(Source: Guideline 1a [pp. 6–7],NCAA Sports Medicine Handbook(63)).
Emergency situations mayarise at any time during athleticevents. Expedient action must betaken in order to provide the bestpossible care to the athletes ofemergency and/or life threateningconditions. The development andimplementation of an emergencyplan will help ensure that the bestcare will be provided. Athletic or-ganizations have a duty to developan emergency plan that may beimplemented immediately when
necessary and to provide appropri-ate standards of health care to allsports participants. As athletic in-juries may occur at any time andduring any activity, the Sports Med-icine team must be prepared. Thispreparation involves formulation ofan emergency plan, proper coverageof events, maintenance of appropri-ate emergency equipment and sup-plies, utilization of appropriateemergency medical personnel, andcontinuing education in the area ofemergency medicine. Hopefully,through careful pre-participationphysical screenings, adequate med-ical coverage, safe practice andtraining techniques and other safety
Table F3NCAA Division I Women’s championship sports participation (2006-07) and resulting athlete-to-coach ratios, by sport
Sport Teams Athletes Average squad size Limit on no. of coaches Athletes per coach
Basketball 325 4,744 14.6 4 3.6
Bowling 28 249 8.9 2 4.4
Cross Country 321 5,203 16.2 2 8.1
Fencing 26 403 15.5 2 7.8
Field Hockey 78 1,732 22.2 3 7.4
Golf 228 1,994 8.7 2 4.4
Gymnastics 65 1,109 17.1 3 5.7
Ice Hockey 33 828 25.1 3 8.4
Lacrosse 79 2,145 27.2 3 9.1
Rifle 27 171 6.3 2 3.2
Rowing 86 5,441 63.3 3 21.1
Skiing 14 215 15.4 2 7.7
Soccer 300 7,703 25.7 3 8.6
Softball 268 5,193 19.4 3 6.5
Swimming/ Diving 189 5,014 26.5 3 8.8
Tennis 304 2,838 9.3 2 4.6
Track (indoor) 289 10,591 36.6 3 12.2
Track (outdoor) 301 10,789 35.8 3 11.9
Volleyball 313 4,476 14.3 3 4.8
Water Polo 31 635 20.5 2 10.2
TOTAL 3,305 71,473 53
Average [20 sports] 21.6 2.6 8.3
VOLUME 31 | NUMBER 5 | OCTOBER 200932
Standards and Guidelines

avenues, some potential emergen-cies may be averted. However,accidents and injuries are inherentwith sports participation, and properpreparation on the part of the SportsMedicine team will enable eachemergency situation to be managedappropriately.
Components of the Emergency Plan.There are three basic components
of this plan: emergency personnel,communication, and equipment.1. Emergency Personnel. With ath-
letic association practice andcompetition, the first responderto an emergency situation istypically a member of the SportsMedicine staff, most commonlya certified athletic trainer. A teamphysician may not always bepresent at every organized prac-tice or competition. The type anddegree of Sports Medicine cov-erage for an athletic event mayvary widely, based on such fac-tors as the sport or activity, thesetting, and the type of training orcompetition. The first responderin some instancesmay be a coachor other institutional personnel.Certification in cardiopulmonaryresuscitation (CPR), first aid, pre-vention of disease transmission,and emergency plan review isrequired for all athletics person-nel associated with practices,competitions, skills instruction,and Strength & Conditioning.
2. Emergency Communication.Communication is the key toquick delivery of emergency carein athletic trauma situations. Ath-letic trainers and emergencymedical personnel must worktogether to provide the bestpossible care to injured athletes.Communication prior to the eventis a good way to establishboundaries and to build rapportbetween both groups of profes-sionals. If emergency medicaltransportation is not available onsite during a particular sportingevent then direct communicationwith the emergency medical sys-tem at the time of injury or illnessis necessary. Access to a working
telephone or other telecommuni-cations device, whether fixed ormobile, should be assured. Thecommunications system shouldbe checked prior to each practiceor competition to ensure properworking order. A back-up com-munication plan should be ineffect should there be failure ofthe primary communication sys-tem. The most common methodof communication is a publictelephone. However, a cellularphone is preferred if available.At any athletic venue, whetherhome or away, it is important toknow the location of a workabletelephone. Pre-arranged accessto the phone should be estab-lished if it is not easily accessible.
3. Emergency Equipment. All nec-essary emergency equipmentshould be at the site and quicklyaccessible. Personnel should befamiliar with the function andoperation of each type of emer-gency equipment. Equipmentshould be in good operatingcondition, and personnel mustbe trained in advance to use itproperly. Emergency equipmentshould be checked on a regularbasis and rehearsed by emer-gency personnel. The emergencyequipment available should beappropriate for the level of train-ing for the emergency medicalproviders. It is important to knowthe proper way to care for andstore the equipment as well.Equipment should be stored ina clean and environmentally con-trolled area. It should be readilyavailable when emergency situa-tions arise.
Roles Within the Emergency Team.The development of an emer-
gency plan cannot be completewithout the formation of an emer-gency team. The emergency teammay consist of a number of healthcare providers including physicians,emergency medical technicians, cer-tified athletic trainers; student athletictrainers; coaches; managers; and,possibly, bystanders. Roles of theseindividuals within the emergency
team may vary depending on variousfactors such as the number ofmembers of the team, the athleticvenue itself, or the preference of thehead athletic trainer. There are fourbasic roles within the emergencyteam.1. Immediate Care of the Athlete.
The first and most important roleis immediate care of the athlete.The most qualified individual onthe scene should provide acutecare in an emergency situation.Individuals with lower credentialsshould yield to those with moreappropriate training.
2. Emergency Equipment Retrieval.The second role, equipment re-trieval, may be done by anyone onthe emergency team who isfamiliar with the types and loca-tion of the specific equipmentneeded. Student athletic trainers,managers, and coaches are goodchoices for this role.
3. Activation of the EmergencyMedical System. The third role,EMS activation, may be neces-sary in situations where emer-gency transportation is notalready present at the sportingevent. This should be done assoon as the situation is deemedan emergency or a life-threaten-ing event. Time is the mostcritical factor under emergencyconditions. Activating the EMSsystem may be done by anyoneon the team. However, the per-son chosen for this duty shouldbe someone who is calm underpressure and who communi-cates well over the telephone.This person should also befamiliar with the location andaddress of the sporting event.
Making The Call:s 911 (if available)s telephone numbers for local
police, fire department, andambulance service
Providing information:s name, address, telephone
number of callers number of athletess condition of athlete(s)s first aid treatment initiated by
first responder
Strength and Conditioning Journal | www.nsca-lift.org 33

s specific directions as neededto locate the emergency scene(‘‘come to south entrance ofcoliseum’’)
s other information as requestedby dispatcher
4. Direction of EMS to Scene. AfterEMS has been activated, thefourth role in the emergency teamshould be performed, that ofdirecting EMS to the scene.One member of the team shouldbe responsible for meeting emer-gency medical personnel as theyarrive at the site of the contest.Depending on ease of access,this person should have keys toany locked gates or doors thatmay slow the arrival of medicalpersonnel. A student athletictrainer, manager, or coach maybe appropriate for this role.
When forming the emergencyteam, it is important to adapt theteam to each situation or sport. Itmay also be advantageous to havemore than one individual assigned toeach role. This allows the emer-gency team to function even thoughcertain members may not always bepresent.
Transportation.Emphasis is placed at having an
ambulance on site at high risksporting events. EMS response timeis additionally factored in when de-termining on site ambulance cover-age. Ambulances may becoordinated on site for other specialevents/sports, such as major tourna-ments or Conference/NCAA re-gional or championship events.Consideration is given to the capa-bilities of transportation serviceavailable (i.e. Basic Life Support orAdvanced Life Support)and theequipment and level of trainedpersonnel on board the ambulance.In the event that an ambulance is onsite, there should be a designatedlocation with rapid access to the siteand a cleared route for entering/ex-iting the venue.
In the emergency evaluation,the primary survey assists the emer-gency care provider in identifyingemergencies requiring critical
intervention and in determiningtransport decisions. In an emer-gency situation, the athlete shouldbe transported by ambulance, wherethe necessary staff and equipment isavailable to deliver appropriate care.Emergency care providers shouldrefrain from transporting unstableathletes in inappropriate vehicles.Care must be taken to ensure that theactivity areas are supervised shouldthe emergency care provider leavethe site in transporting the athlete.
Conclusion.The importance of being properlyprepared when athletic emergenciesarise cannot be stressed enough. Anathlete’s survival may hinge on howwell trained and prepared athletichealth care providers are. It isprudent to invest athletic depart-ment ‘‘ownership’’ in the emergencyplan by involving the athletic admin-istration and sport coaches as wellas Sports Medicine personnel. Theemergency plan should be reviewedat least once a year with all athleticpersonnel, along with CPR and firstaid refresher training. Through de-velopment and implementation ofthe emergency plan, the athlete willhave the best care provided when anemergency situation does arise.
APPENDIX H. PROTECTIVE LEGALDOCUMENTS
Notes: This appendix providesgeneral legal information. Protectivelegal documents should not beadopted or used in any contextwithout individualized legal advice.The information in this appendix hasbeen adapted with permission froman article by JoAnn Eickhoff-Sche-mek, entitled ‘‘Distinguishing Pro-tective Legal Documents’’,published in the ACSM’s Journal ofHealth & Fitness (18).
TYPES OF PROTECTIVE LEGALDOCUMENTS
Institutions such as universi-ties/colleges and high schools oftenrequire athletes to read and signsome type of protective legal
document(s) prior to participationin athletically-related activities, includ-ing Strength & Conditioning. Thesedocuments can help protect theinstitution and its employees frompotentially costly legal claims andlawsuits. The law involving protectivelegal documents is quite complex,however, and understanding theirfunction and the specific legal protec-tion they provide is often confusing.
Several types of protectivelegal documents exist. Three thatare commonly used in the health/fitness field may be applicable inStrength & Conditioning settings:informed consent, agreement toparticipate, and waiver. Each pro-vides protection from liability arisingfrom certain types of claims that canoccur while participating in activities,as explained below.
CAUSES OF INJURY ASSOCIATEDWITH PHYSICAL ACTIVITY
Cotten & Cotton (17) describethree causes of injury are associatedwith physical activity: inherent risks,negligence, and extreme forms ofconduct.
Inherent Risks.As the term implies, these risks areinherent in the activity. Generally,injuries caused by inherent risks areaccidental in nature, not prevent-able, and no one’s fault. The in-formed consent and agreement toparticipate documents provide thebest possible protection for claimsarising from such injuries. Althoughactual sections and content of pro-tective documents vary (and dependupon state law), the following aregenerally included in informed con-sent and agreement to participatedocuments:
INFORMED CONSENT� Purpose of the activity� Risks of the activity*� Benefits of the activity� Confidentiality� Inquiries� Signatures
AGREEMENT TO PARTICIPATE� Nature of the activity� Possible consequences of injury*
VOLUME 31 | NUMBER 5 | OCTOBER 200934
Standards and Guidelines

� Behavioral expectations of theparticipant
� Condition of the participant� Concluding statement� Signatures� *Note: ‘‘assumption of risk’’language
� A section within each of thesedocuments is devoted to inform-ing the participant of the potentialrisks, including those inherent inthe activity. It is important that thissection carefully describes theserisks (e.g., types of accidents thatmight occur and the consequen-ces of these accidents), and thatthe language used is understand-able to the person who will besigning it. This provides an ‘‘as-sumption of risk’’ defense, i.e. theparticipant knew and fully under-stood the risks, appreciated therisks, and voluntarily assumedthem. In general, the law doesnot allow individuals to recovercompensation for injuries resultingfrom assumed risks.
Negligence.Injuries can be caused by negli-gence, i.e. failure to act as reason-able and prudent professional wouldact under the circumstances. Partic-ipants can be injured by negligentacts of the Strength & Conditioningstaff (e.g., failure to inspect/maintainexercise equipment, failure to pro-vide CPR or First Aid when needed).A waiver document, also calleda prospective release, provides thebest legal protection for claimsarising from injuries caused bynegligence. Once again, while theactual sections and content of suchdocuments vary depending on statelaw, waiver documents generallyinclude: exculpatory clause; descrip-tion of risks (‘‘assumption of risk’’language); indemnification language(may not be valid); severabilityclause; affirmation of legal capacity;and signatures.
The ‘‘exculpatory clause’’ isa key section within the waiverexplicitly stating that the participantreleases the Strength & Condition-ing facility for any liability associatedwith negligence by the facility or its
employees. This clause, which mustbe written very carefully to beenforceable, provides evidence thatthe participant gave up (waived)his/her right to file a negligenceclaims against the facility. However,the exculpatory clause does notprovide protection from lawsuitsarising from injuries due to inherentrisks; and an ‘‘assumption of risk’’section is often added to the waiverfor this purpose.
Extreme Forms of Conduct.Injuries can also be caused byextreme forms of conduct (oftenreferred to as gross negligence,willful and wanton conduct, or reck-less conduct). For example, if theStrength & Conditioning staff hadprior knowledge of an existing dan-ger or risk but took no correctiveaction to help prevent resultinginjuries, this failure to act couldconstitute an extreme form of con-duct. Generally, no documents canprovide legal protection for grosslynegligent or reckless conduct. A fewstates may allow the use of a waiverto protect from such conduct, butmost do not (17).
MAKING PROTECTIVE LEGALDOCUMENTS ENFORCEABLE
Protective legal documents,signed by participants prior to theirparticipation in Strength & Condi-tioning programs and services, canprovide a good defense for theStrength & Conditioning facility afteran injured participant files a claim orlawsuit. A variety of factors shouldbe considered in order for theseforms to be legally enforceable:(17,18,34).� A lawyer who is knowledgeableabout the law regarding protectivedocuments should review yourprotective legal documents tohelp ensure they are written prop-erly and reflect the law in yourstate.
� Informed consent and waiverdocuments are contracts, andcan only be signed by adultsbecause minors cannot enter intoa contract. �Agreement to partici-pate� documents are not
contracts, and therefore can besigned by adults as well as minors.
� The exculpatory clause used ina waiver is not allowed in aninformed consent or agreementto participate. If an exculpatoryclause is added to an agreementto participate for adults, it thenbecomes a waiver.
� The exculpatory clause used ina waiver is not enforceable inmedical or research settings, orin certain states (Virginia, Monta-na, Louisiana)where they areagainst public policy. In educa-tional settings such as a college/university, the general rule is thatwaivers are against public policyfor required activities but maybe enforceable for voluntaryactivities.
� Informed consent documentsused in medical settings must beadministered prior to a patienthaving any kind of medical pro-cedure. If the informed consent isnot written or administered prop-erly, the health care provider (andmedical facility)could be foundnegligent for not informing thepatient of particular risks. Thisalso applies in research settings,because subjects must be prop-erly informed of risks throughinformed consent (note that thispoint is applicable in Strength &Conditioning settings where ath-letes participate as human sub-jects in research studies).
� All documents must be adminis-tered properly. For example, par-ticipants should have ample timeto read them, and a knowledgeableemployee should verbally explainthe document to each participant.
� Protective documents must bestored in a secure place for theamount of time consistent with thestatue of limitations, which may beup to 4 years in some states.
The choice of document orcombination of documents to use isa very important decision. In situa-tions where Strength & Conditioningactivities are not covered in theemploying institution’s legal docu-mentation, Strength & Conditioningprofessionals should consult with
Strength and Conditioning Journal | www.nsca-lift.org 35

a qualified lawyer to assist withthese decisions and to review orwrite the documents prior to imple-mentation. These resources shouldbe shared with your lawyer whenhe/she reviews the drafts and makesthe final document revisions.
Written protective documentsprovide important evidence whena lawsuit occurs. For example, ifa Strength & Conditioning facility issued for negligence, but has evi-dence that the injured party signeda properly written and administeredwaiver, this document provides theevidence to have a claim dismissed.In this situation, the legal documentprotects the facility from a potentiallycostly negligence lawsuit.
NSCA PROFESSIONALSTANDARDS & GUIDELINES TASKFORCE
Contributors: (2009 version)N. Travis Triplett, PhD, CSCS*D,FNSCA (Chair); Chat Williams, MS,CSCS*D, NSCA-CPT*D; Patrick,McHenry, MS, CSCS*D, CP;Michael Doscher, MS, CSCS*D,CP. (2001 version), Steven Plisk,MS, CSCS (Chair); Mike Brass, MS,CSCS; JoAnn Eickhoff-Shemek, PhD;Boyd Epley, MEd, CSCS, FNSCA;David Herbert, JD; Joe Owens,MS, CSCS*D; David Pearson, PhD,CSCS*D; Dan Wathen, MS, ATC,CSCS*D, NSCA-CPT*D.
REFERENCES1. Ajan T., Baroga L. Weightlifting. Budapest:
INTERNATIONAL WEIGHTLIFTING
FEDERATION/Medicina Publishing House,
1988.
2. AMERICAN HEART ASSOCIATION in
collaboration with the INTERNATIONAL
LIAISON COMMITTEE ON
RESUSCITATION. Guidelines 2000 for
cardiopulmonary resuscitation and
emergency cardiovascular care:
international consensus on science.
Circulation 102(8)Supplement: August 22,
2000.
3. AMERICAN SOCIETY FOR TESTING &
MATERIALS. ASTM Standard Consumer
Safety Specification for Stationary Exercise
Bicycles: Designation F1250-89. West
Conshohocken PA: ASTM, 1989.
4. AMERICAN SOCIETY FOR TESTING &
MATERIALS. ASTM Standard
Specification for Fitness Equipment &
Fitness Facility Safety Signage & Labels:
Designation F1749-96. West
Conshohocken PA: ASTM, 1996.
5a. Armitage-Johnson S. Providing a safe
training environment: part I. Strength &
Conditioning 16(1): 64–65, 1994.
5b. Armitage-Johnson S. Providing a safe
training environment: part II. Strength &
Conditioning 16(2): 34, 1994.
6. Baechle T.R. National study produces
a new CSCS job description. Strength &
Conditioning 19(3): 64–65, 1997.
7. Baechle T.R., Earle R.W. (Editors)/
NATIONAL STRENGTH &
CONDITIONING ASSOCIATION.
Essentials of Strength Training &
Conditioning (3rd Edition). Champaign IL:
Human Kinetics, 2008.
8. Balady G. J., et al./AMERICAN HEART
ASSOCIATION & AMERICAN COLLEGE
OF SPORTS MEDICINE.
Recommendations for cardiovascular
screening, staffing and emergency policies
at health/fitness facilities. Circulation
97(22): 2283-2293, 1998; Medicine &
Science in Sports & Exercise 30(6): 1009–
1018, 1998.
9. Baley J.A., Matthews D.L. Law & Liability in
Athletics, Physical Education & Recreation.
Boston MA: Allyn & Bacon, 1984.
10. Behm D.G. Neuromuscular implications
and applications of resistance training.
Journal of Strength & Conditioning
Research 9(4): 264–274, 1995.
11. Brown E.W., Kimball R.G. Medical history
associated with adolescent powerlifting.
Pediatrics 72(5): 636–644, 1983.
12. Bucher C.A., Krotee M.L. Management of
Physical Education & Sport (11th Edition).
Boston MA: McGraw-Hill, 1998.
13. Calhoon G., Fry A.C. Injury rates and
profiles of elite competitive weightlifters.
Journal of Athletic Training 34(3): 232–
238, 1999.
14. CENTERS FOR DISEASE CONTROL &
PREVENTION/U.S. DEPARTMENT OF
HEALTH & HUMAN SERVICES.
Perspectives in disease prevention and
health promotion update: universal
precautions for prevention of transmission
of human immunodeficiency virus, hepatitis
B virus, and other blood-borne pathogens
in health-care settings. Morbidity &
Mortality Weekly Report 37(24): 377–388,
1988.
15. Chandler T.J., Stone M. H./NATIONAL
STRENGTH & CONDITIONING
ASSOCIATION. The squat exercise in
athletic conditioning: a position statement
and review of the literature. National
Strength & Conditioning Association
Journal 13(5): 51–60, 1991.
16. COALITION OF AMERICANS TO
PROTECT SPORTS. Sports Injury Risk
Management (2nd Edition). North Palm
Beach FL: CAPS, 1998.
17. Cotten D.J., Cotten M.B. Legal Aspects of
Waivers in Sport, Recreation & Fitness
Activities. Canton OH: PRC Publishing,
1997.
18. Eickhoff-Shemek J. Distinguishing
protective legal documents. ACSM’s
Health & Fitness Journal 5(3): 27–29,
2001.
19. Eickhoff-Shemek J. Standards of practice.
In: Cotten D., Wilde J. & Wlohan J.
(Editors), Law for Recreation & Sport
Managers (2nd Edition). Dubuque IA:
Kendall/Hunt Publishing, 2001; pp. 293–
302.
20. Eickhoff-Shemek J., Deja K.4 steps to
minimize legal liability in exercise programs.
ACSM’s Health & Fitness Journal4(4):
13–18, 2000.
21. Elliott B. (Editor) Training in Sport.
Chichester: John Wiley & Sons, 1999.
22. Faigenbaum A.D., Kraemer W. J., et al./
NATIONAL STRENGTH &
CONDITIONING ASSOCIATION. Youth
resistance training: position statement
paper and literature review. Strength
& Conditioning 18(6): 62–75,
1996.
23. Faigenbaum A.D., Micheli L. J./AMERICAN
COLLEGE OF SPORTS MEDICINE.
Current Comment from the American
College of Sports Medicine: Youth
Strength Training. Indianapolis IN: ACSM,
1998 http://www.acsm.org/pdf/
YSTRNGTH.pdf.
24. Fleck S.J., Kraemer W.J. Designing
Resistance Training Programs (2nd
Edition). Champaign IL: Human Kinetics,
1997.
25. Hakkinen K. Factors influencing trainability
of muscular strength during short term and
prolonged training. National Strength &
Conditioning Association Journal 7(2):
32–37, 1985.
26. Hakkinen K. Neuromuscular and hormonal
adaptations during strength and power
training: a review. Journal of Sports
Medicine & Physical Fitness 29(1): 9–26,
1989.
27. Hakkinen K. Neuromuscular adaptation
during strength training, aging, detraining
and immobilization. Critical Reviews in
VOLUME 31 | NUMBER 5 | OCTOBER 200936
Standards and Guidelines
Physical Rehabilitation & Medicine 6(3):
161–198, 1994.
28. Halling D.H. Liability considerations of the
strength and conditioning specialist.
National Strength & Conditioning
Association Journal 12(5): 57–60, 1990.
29. Halling D.H. Legal terminology for the
strength and conditioning specialist.
National Strength & Conditioning
Association Journal 13(4): 59–61, 1991.
30. Hamill B.P. Relative safety of weightlifting
and weight training. Journal of Strength &
Conditioning Research 8(1): 53-57, 1994.
31. Harre D. (Editor) Principles of Sports
Training. Berlin: Sportverlag, 1982.
32. Hartmann J., Tunnemann H. Fitness &
Strength Training. Berlin: Sportverlag,
1989.
33. Head G.L., Horn S. Essentials of Risk
Management: Volume I (3rd Edition).
Malvern PA: Insurance Institute of America,
1995.
34. Herbert D.L., Herbert W.G. Legal Aspects
of Preventive, Rehabilitative & Recreational
Exercise Programs (3rd Edition). Canton
OH: PRC Publishing, 1993.
35. Herbert D.L. Legal aspects of strength and
conditioning. National Strength &
Conditioning Association Journal 15(4):
79, 1993.
36. Herbert D.L. Supervision for strength and
conditioning activities. Strength &
Conditioning 16(2): 32–33, 1994.
37. Herbert D.L. A good reason for keeping
records. Strength & Conditioning 16(3):
64, 1994.
38. Hillmann A., Pearson D.R. Supervision: the
key to strength training success. Strength
& Conditioning 17(5): 67–71, 1995.
39. Hochmuth G. Biomechanics of Athletic
Movement. Berlin: Sportverlag, 1984.
40a. Holloway J.B., Gater D., Ritchie M., et al./
NATIONAL STRENGTH &
CONDITIONING ASSOCIATION.
Strength training for female athletes:
a position paper: part 1. National Strength
& Conditioning Association Journal 11(4):
43–55, 1989.
40b. Holloway J.B., Gater D., Ritchie M., et al./
NATIONAL STRENGTH &
CONDITIONING ASSOCIATION.
Strength training for female athletes:
a position paper: part 2. National Strength
& Conditioning Association Journal 11(5):
29–36, 1989.
41. Jones C.S., Christensen C., Young M.
Weight training injury trends: a 20-year
survey. Physician & Sportsmedicine 28(7):
61–72, 2000.
42. Jones L./U.S. WEIGHTLIFTING
FEDERATION. USWF Coaching
Accreditation Course: Club Coach Manual.
Colorado Springs CO: USWF, 1991.
43. Katzenbach J.R., Smith D.K. The Wisdom
of Teams. Boston MA: Harvard Business
School, 1993.
44. Katzenbach J.R., et al. Real Change
Leaders. New York NY: Times Books/
Random House, 1995; pp. 217–224.
45. Knowles M.S., Holton E.F., Swanson R.A.
The Adult Learner (5th Edition). Houston
TX: Gulf Publishing, 1998.
46. Komi P.V. Neuromuscular performance:
factors influencing force and speed
production. Scandinavian Journal of Sports
Science 1(1): 2–15, 1979.
47. Komi P.V. (Editor) Strength & Power in
Sport. Oxford: Blackwell Scientific
Publications, 1992.
48. Kroll W. Selecting strength training
equipment. National Strength &
Conditioning Journal 12(5): 65–70, 1990.
49a. Kroll B. Structural and functional
considerations in designing the facility:
part I. National Strength & Conditioning
Association Journal 13(1): 51–58, 1991.
49b. Kroll W. Structural and functional
considerations in designing the facility:
part II. National Strength & Conditioning
Association Journal 13(3): 51–57, 1991.
50. Kroll B. Liability considerations for strength
training facilities. Strength & Conditioning
17(6): 16–17, 1995.
51. Malina, R.M. Weight training in youth-
growth, maturation and safety: An
evidence-based review. Clinical Journal of
Sports Medicine 16(6): 478–487, 2006.
52a. Maron B. J., et al./AMERICAN HEART
ASSOCIATION. Cardiovascular
preparticipation screening of competitive
athletes. Circulation 94(4): 850-856,
1996; Medicine & Science in Sports &
Exercise 28(12): 1445–1452, 1996.
52b. Maron B. J., et al./AMERICAN HEART
ASSOCIATION. Cardiovascular
preparticipation screening of competitive
athletes: addendum. Circulation 97(22):
2294, 1998.
53. Mazur L.J., Yetman R.J., Risser W.L.
Weight-training injuries: common injuries
and preventative methods. Sports
Medicine 16(1): 57–63, 1993.
54. Morris G.A. Supervision-an asset to the
weightroom? Strength & Conditioning
16(2): 14–18, 1994.
55. Morrissey M.C., Harman E.A., Johnson M.J.
Resistance training modes: specificity and
effectiveness. Medicine & Science in
Sports & Exercise 27(5): 648–660,
1995.
56. NATIONAL COLLEGIATE ATHLETIC
ASSOCIATION. NCAA Sports
Participation Rates. Indianapolis IN: NCAA,
2000 http://www.ncaa.org/
participation_rates/..
57. NATIONAL FEDERATION OF
STATE HIGH SCHOOL ASSOCIATIONS.
NFHS Participation Survey: 1999-2000.
Indianapolis IN: NFHS, 2000
,http://www.nfhs.org/PDF/2000-01%20
NFHS%20Participation%20Survey.pdf..
58. NSCA CERTIFICATION Department.
Certified Strength & Conditioning
Specialist� (CSCS�) Examination Content
Description. Colorado Springs, CO: NSCA
Certification Department, 2009.
59. Newton R.U, Kraemer W.J. Developing
explosive muscular power: implications for
a mixed methods training strategy.
Strength & Conditioning 16(5): 20–31,
1994.
60. OCCUPATIONAL SAFETY & HEALTH
ADMINISTRATION/U.S. DEPARTMENT
OF LABOR. OSHA Regulations
(Standards - 29 CFR)1910. 1030: Blood-
Borne Pathogens. Washington DC:
OSHA, 1996 ,http://www.osha-slc.gov/
OshStd_data/1910_1030.html..
61. Pearson, D., Faigenbaum, A., Conley, M.,
Kraemer, W. J./ NATIONAL STRENGTH &
CONDITIONING ASSOCIATION. Basic
guidelines for the resistance training of
athletes. Strength & Conditioning Journal
22(4): 14–27, 2000.
62. Plisk S.S. Anaerobic metabolic
conditioning: a brief review of theory,
strategy and practical application. Journal
of Applied Sport Science Research 5(1):
22–34, 1991.
63. Potts K.A., Dick R.W. (Editors)/NATIONAL
COLLEGIATE ATHLETIC ASSOCIATION.
2000-01 NCAA Sports Medicine
Handbook (13th Edition). Indianapolis IN:
NCAA, 2000.
64. Preparticipation Physical Evaluation Task
Force/AMERICAN ACADEMY OF FAMILY
PHYSICIANS, AMERICAN ACADEMY OF
PEDIATRICS, AMERICAN MEDICAL
SOCIETY FOR SPORTS MEDICINE,
AMERICAN ORTHOPAEDIC SOCIETY
FOR SPORTS MEDICINE & AMERICAN
OSTEOPATHIC ACADEMY OF SPORTS
MEDICINE. Preparticipation Physical
Evaluation (2nd Edition). Minneapolis MN:
McGraw-Hill, 1996.
65. Rabinoff M.A. Weight room litigation:
what’s it all about? Strength &
Conditioning 16(2): 10–12, 1994.
Strength and Conditioning Journal | www.nsca-lift.org 37
66. Rabinoff M.A. 32 reasons for the strength,
conditioning, and exercise professional
to understand the litigation process.
Strength & Conditioning16(2): 20–25,
1994.
67a. Reeves R.K., Laskowski E.R., Smith J.
Weight training injuries: part 1:
diagnosing and managing acute
conditions. Physician & Sportsmedicine
26(2): 67–96, 1998.
67b. Reeves R.K., Laskowski E.R., Smith J.
Weight training injuries: part 2:
diagnosing and managing chronic
conditions. Physician & Sportsmedicine
26(3): 54–63, 1998.
68. Risser W.L., Risser J.M., Preston D.
Weight-training injuries in adolescents.
American Journal of Diseases of Children
144(9): 1015–1017, 1990.
69. Schmidt R.A., Lee T.D. Motor Control &
Learning (3rd Edition). Champaign IL:
Human Kinetics, 1999.
70. Schmidt R.A., Wrisberg C.A. Motor
Learning & Performance (2nd Edition).
Champaign IL: Human Kinetics, 1999.
71a. Schmidtbleicher D. Strength training: part
1: classification of methods. Science
Periodical on Research & Technology in
Sport (Physical Training/Strength) W4:
1–12, August 1985.
71b. Schmidtbleicher D. Strength training: part
2: structural analysis of motor strength
qualities and its application to training.
Science Periodical on Research &
Technology in Sport (Physical Training/
Strength) W4: 1–10, September 1985.
72. Schmolinsky G. (Editor) Track & Field.
Toronto: Sport Books Publisher, 1993.
73. Shultz S. J., et al./NATIONAL ATHLETIC
TRAINERS’ ASSOCIATION.
Recommendations & Guidelines for
Appropriate Medical Coverage of
Intercollegiate Athletics. Dallas TX: NATA,
2000 ,http://www.nata.org/downloads/
AMCIA Recs and Guides.pdf..
74. Siff M.C. Supertraining (5th Edition).
Denver CO: Supertraining Institute, 2000.
75. Stone M., O’Bryant H. Weight Training.
Minneapolis MN: Bellwether Press/
Burgess International Group, 1987.
76. Stone M. H./NATIONAL STRENGTH &
CONDITIONING ASSOCIATION. Position
statement: explosive exercises and training.
National Strength & Conditioning
Association Journal 15(3): 6–15, 1993.
77. Stone M.H., et al. Injury potential and safety
aspects of weightlifting movements. Strength
& Conditioning 16(3): 15–21, 1994.
78. Stone M.H., et al. Training to muscular
failure: is it necessary? Strength &
Conditioning 18(3): 44–48, 1996.
79. Stone M.H., Borden R.A. Modes and
methods of resistance training. Strength &
Conditioning 19(4): 18–24, 1997.
80. Stone M.H., et al. Athletic performance
development: volume load — 1 set vs.
multiple sets, training velocity and training
variation. Strength & Conditioning 20(6):
22–31, 1998.
81a. Stone M.H., et al. Periodization: effects of
manipulating volume and intensity: part 1.
Strength & Conditioning Journal 21(2):
56–62, 1999.
81b. Stone M.H., et al. Periodization: effects of
manipulating volume and intensity: part 2.
Strength & Conditioning Journal 21(3):
54-60, 1999.
82. Stone M.H., et al. Training principles:
evaluation of modes and methods of
resistance training. Strength &
Conditioning Journal 22(3): 65–76, 2000.
83. Tharrett S.J., Peterson J.A. (Editors)/
AMERICAN COLLEGE OF SPORTS
MEDICINE. ACSM’s Health/Fitness Facility
Standards & Guidelines (2nd Edition).
Champaign IL: Human Kinetics, 1997.
84. Tidow G. Aspects of strength training in
athletics. New Studies in Athletics 5(1):
93–110, 1990.
85. Viru A. Adaptation in Sports Training. Boca
Raton FL: CRC Press, 1995.
86. Wathen D./NATIONAL STRENGTH &
CONDITIONING ASSOCIATION. Position
statement: explosive/plyometric exercises.
National Strength & Conditioning
Association Journal 15(3): 16–19, 1993.
87. Wright J.E., Stone M. H./NATIONAL
STRENGTH & CONDITIONING
ASSOCIATION. Position statement:
anabolic-androgenic steroid use by
athletes. National Strength & Conditioning
Association Journal 15(2): 9–28, 1993.
88. Zatsiorsky V.M. Science & Practice of
Strength Training. Champaign IL: Human
Kinetics, 1995.
89. Zatsiorsky V.M. (editor) Biomechanics in
Sport. Oxford: Blackwell Science, 2000.
90. Zemper E.D. Four-year study of
weightroom injuries in a national sample of
college football teams. National Strength &
Conditioning Association Journal 12(3):
32–34, 1990.
VOLUME 31 | NUMBER 5 | OCTOBER 200938
Standards and Guidelines