Embed Size (px)
Citation preview
National Standard SNOMED CT subset for Diagnostic Imaging
procedures and the relationship to local 'Order Catalogues'
Ian ArrowsmithNHS Connecting for Health
Royal College of Radiologists PACS and Teleradiology Special Interest Group
20th April 2005
Structure of presentation
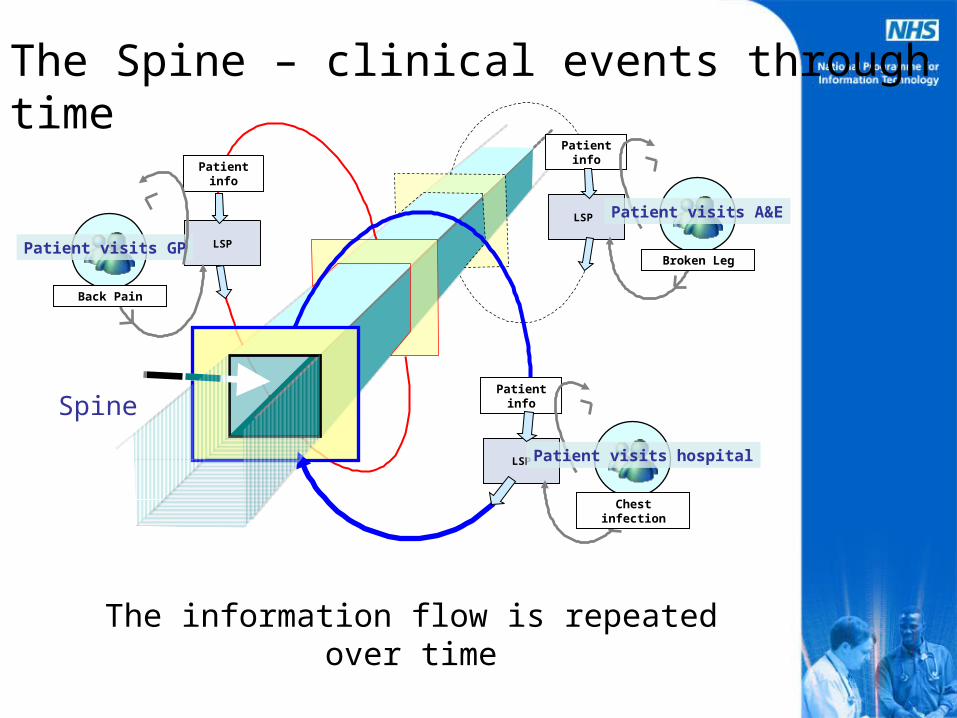
• The need for a National Standard – The NHS Care Record Service ‘Spine’
• The National Subset of DI procedures– Principles
• Relationship to local/cluster order catalogues
• Management arrangements
The NHS Care Record Service ‘Vision’
• The “Continuity of Care Record”– The NHS Care Record Spine is a universally
accessible (to those with an authority to view) repository of Health Care information for every person in England.
– The content of the record can be thought of as the minimum information required by a clinician when seeing a patient for the first time in the absence of a referral from a clinical colleague. That is not to say that the record will only be used in unplanned and emergency situations.
LSP
Patient info
Broken Leg
Patient visits A&E
Patient info
LSP
Back Pain
Patient visits GP
LSP
Patient info
Chest infection
Patient visits hospital
Spine
The Spine – clinical events through time
The information flow is repeated over time
SNOMED CT
• All structured clinical information will be represented in the NCRS using SNOMED Clinical Terms® and will be communicated to and from the Spine using HL7 v3 messages
• It is therefore essential that Diagnostic Imaging procedures are represented effectively in SNOMED CT and that the terminology is used consistently throughout the NHS CRS
Subsets
• A SNOMED CT subset is a collection of terminology, selected and grouped for a particular purpose. A subset may be composed of anything from a single component to the entire set of concepts, descriptions or relationships - and are commonly needed for: – Data quality improvement– Message field validation– Simplified data entry and retrieval– Elimination of ‘noise’
The National SNOMED CT Subset of DI procedures
• A comprehensive set of DI procedure descriptions to ensure Nationally consistent recording of all DI procedures undertaken in the NHS using the mandated terminology
• Expressed simply as the modality, the body site and, where necessary, the laterality (some notable exceptions)
Principles
• Descriptions should be clear and unambiguous both within and outside the DI business domain
• Descriptions should represent clinical activity and not administrative functions
Modalities
• X-Ray (includes Mammography)• US scan (includes Obstetric ultrasound)• CT• MRI (includes Magnetic resonance
angiography)• Radionuclide Study (includes single
photon emission computed tomography)• Fluoroscopy (includes angiography)• DEXA scan ?
Example descriptions and user-friendly alternatives
Arterial Stent Renal Fluoroscopic angiography of renal
artery and insertion of stent
Right ventriculogramFluoroscopic angiography of right
cardiac ventricle
HysterosalpingogramFluoroscopy of uterus and
fallopian tubes
Exceptions
• Barium follow through
• CT leg length measurement
• High Resolution CT of lungs
• Radionuclide gastric emptying study– Plus many more Nuclear medicine
procedures
Current status
• Delivery end of this week• Review by workshop attendees (2
weeks)• Revision of list (1 week)• Changes effected in SNOMED CT (?
by summer 2005)• Formal release ( ? by autumn 2005)
Existing ‘order catalogues’
• Current situation– Development of cluster-wide lists
• Including an RCR approved one
– Other local lists in service provider departments
– GP systems (Read codes)– National subset
Issues• There are very few systems which currently have the capability
of SNOMED CT encoding directly and it will be many years before all systems enable this.
• Some LSP’s, in conjunction with their sub-contractors and local health communities have developed catalogues ahead of, and therefore inconsistent with, the emergent nationally agreed subset principles
• Any new arrangements must not cause detriment to existing information flows
• Replacement Radiology systems are being procured to support the roll-out of PACS which are not required to integrate with the common NCRS architecture in the short term.
• Different levels of granularity/specificity are required at different points in the requesting/reporting workflow.
• Mapping automatically from a less detailed coding scheme to a more detailed one is generally not considered acceptable where the relationship is not a logical one-to-one map. Whether receiving requests or reports, receiving systems which cannot process incoming data are therefore expected to deprecate the content to text unless there is a degree of manual intervention.
Resolution
• With specific reference to the domains of DI and pathology it has been decided that NPfIT will allow mapping between the local code lists and the National Standard subsets for population of the relevant fields in the NPfIT HL7v3 messages.
• In the requesting systems however, the local term instances will be exact lexical equivalents to descriptions in the national Standard Subset so although a translation will occur (from READ to SNOMED CT) this will be a one-to-one relationship.
For requesting in an inter-organisational environment and for populating messages
• Requesters will only be allowed to order from the list of descriptions in the National Standard list (even though they may be represented in a different coding scheme eg Read codes).
• These descriptions will be lexically equivalent where possible with the items in the National subset. Where this is not possible (due to term length constraints for instance) then the local description must have a mapping to a single entry in the National subset.
• On receipt of the request by the service provider system, business rules may be utilised to translate the procedure/investigation from the National standard list to the local equivalent or it may simply be deprecated to text.
• Responsibility for the accuracy of this process and the creation of any mapping tables lies with the local health community representatives in conjunction with the system supplier
For reporting in an inter-organisational environment and for populating messages
• In service provider systems, where a concept does not exist in the National list, the local form should be mapped to the closest approximation from the list with any additional clinically significant information provided in the original text/code fields in the report message. This is only permitted in the case of outgoing communication from service providers.
• On eventual receipt of the report, the original requesting system may utilise business rules to translate the result or it may simply be deprecated to (structured) text. Responsibility for the accuracy of this process and the creation of any mapping tables lies with the local health community representatives in conjunction with the system supplier.
• The system supplier will provide evidence that any mapping tables utilised for mapping from service provider descriptions to the National subset (for outgoing messages) or to the National subset from local descriptions (for incoming messages) are technically robust as part of the accreditation process
• On creation of the result within the diagnostic service provider system, the local coding instance will be mapped to the NPfIT mandated representation for communication to requester and PSIS
• Interactions within the Local Service Provider environment, i.e. internal Order Comms between Hospital departments, may utilise the local code and local textual description
For reporting in an inter-organisational environment and for populating messages
Example - requesting
• Patient is complaining of knee pain and GP believes this may be due to arthritic changes and requests a ‘left knee X-ray’. GP enters search string which returns a selection of national catalogue post co-ordinated expression for direct selection, i.e. is coding using SNOMED CT and national catalogue eg Left knee X-ray
• The GP validates the message content and sends the request message via TMS to service provider
• The message is received at service provider system and is mapped according to locally designed business rules or by manual entry to the local order catalogue entry to the term ‘Left knee X-ray – osteoarthritis protocol’ (local code = 0003)
Example - reporting
• Patient attends, examination is performed and subsequently reported and the report message is sent to PSIS and to the requester.
• The entry for ‘Left knee X-ray – osteoarthritis protocol’ is translated through the use of locally created mapping tables to the equivalent National standard list entry which in this case is Left knee X-ray for population of the message
• The report message is received by the GP system and the procedure item is either rendered on the screen (and subsequently manually coded) or processed by the system and translated back into the Read code/term
Migration guidance
• The catalogues should be adopted over as many organisations and as wide a geographical area as possible
• Where possible, real descriptions from SNOMED CT should be incorporated in the local order catalogue (not necessarily the preferred term)
• With particular respect to DI, it is recommended that the Radiology Descriptors and short codes catalogue that has been developed after wide consultation, and has been approved by the Royal College of Radiologists, be adopted for all existing and new non-SNOMED CT enabled NPfIT Cluster RIS systems - these are in the process of being mapped to the National Standard list
• A professionally led, responsive management mechanism for the national catalogues will be established
Further information
http://www.connectingforhealth.nhs.uk/technical/standards/