Embed Size (px)
Citation preview

Bull World Health Organ 2018;96:173–184F | doi: http://dx.doi.org/10.2471/BLT.17.199414
Research
173
National policies on the management of latent tuberculosis infection: review of 98 countriesAnn Jagger,a Silke Reiter-karam,b Yohhei Hamadab & Haileyesus Getahunb
IntroductionTuberculosis is currently the leading infectious cause of death worldwide. The World Health Organization (WHO) End Tu-berculosis strategy aims to substantially reduce tuberculosis incidence by 90% and mortality by 95% compared with the 2015 baselines of 142 cases per 100 000 population and 5.3 to 19 cases per 100 000 (depending on human immunodefi-ciency virus (HIV) status), respectively1,2 Achieving this goal requires successful management of latent tuberculosis infec-tion, which serves as a reservoir for new tuberculosis cases.3 In high-income countries which already have a low incidence of tuberculosis, management of latent infection can contribute to elimination of the disease.4 A review of treatment regimens found that treatment of latent tuberculosis can reduce the risk of disease reactivation by 60% to 90%.5 A recent randomized controlled trial in a high tuberculosis burden country showed that the benefits of preventive treatment in people living with HIV can last for more than 5 years.6,7
The WHO recommends tailored latent tuberculosis infec-tion management based on tuberculosis burden and resource availability.8 Systematic testing and treatment for latent infec-tion is strongly recommended for people living with HIV and for children younger than 5 years who are household contacts of a pulmonary tuberculosis case, regardless of the country’s background tuberculosis burden or resource availability.9,10 In upper-middle or high-income countries, depending on low tuberculosis burden and availability of resources, systematic testing and treatment of latent tuberculosis is strongly recom-mended for certain other risk groups: adult household contacts of pulmonary tuberculosis cases; patients with silicosis; pa-
tients initiating anti-tumour necrosis factor treatment; patients on dialysis; and organ transplant recipients.11,12
Despite some progress, particularly over the last decade, the scale-up of tuberculosis preventive treatment remains suboptimal globally. The 161 740 children started on tuber-culosis preventive treatment in 2016 represented only 13% of the 1.3 million children estimated to be eligible for treat-ment.1 The total number of people living with HIV who were started on tuberculosis preventive treatment in 2016 was at least 1.3 million.1 Data for other risk groups are not available or very limited.
Barriers to scale-up of tuberculosis preventive treatment include the absence of national policies and a lack of monitor-ing and evaluation systems.13 Here we review national policy documents to identify differences in programmatic manage-ment of latent tuberculosis infection in high- and low-burden countries.
MethodsThe baseline for this descriptive policy review was the 216 countries and territories reporting data to the WHO Global Tuberculosis Programme (194 Member States and 22 asso-ciate Member States and territories). Based on the current WHO approach11 we divided countries into two groups: low burden and high burden. We defined low-burden countries as upper-middle or high-income countries with an estimated annual tuberculosis incidence of less than 100 cases per 100 000 population.11 High-burden countries were low- to lower-middle-income or other income countries with annual tuberculosis incidence of 100 or more cases
Objective To review policies on management of latent tuberculosis infection in countries with low and high burdens of tuberculosis.Methods We divided countries reporting data to the World Health Organization (WHO) Global Tuberculosis Programme into low and high tuberculosis burden, based on WHO criteria. We identified national policy documents on management of latent tuberculosis through online searches, government websites, WHO country offices and personal communication with programme managers. We made a descriptive analysis with a focus on policy gaps and deviations from WHO policy recommendations.Findings We obtained documents from 68 of 113 low-burden countries and 30 of 35 countries with the highest burdens of tuberculosis or human immunodeficiency virus (HIV)-associated tuberculosis. Screening and treatment of latent tuberculosis infection in people living with HIV was recommended in guidelines of 29 (96.7%) high-burden and 54 (79.7%) low-burden countries. Screening for children aged < 5 years with household tuberculosis contact was the policy of 25 (83.3%) high- and 28 (41.2%) low-burden countries. In most high-burden countries the recommendation was symptom screening alone before treatment, whereas in all low-burden countries it was testing before treatment. Some low-burden countries’ policies did not comply with WHO recommendations: nine (13.2%) recommended tuberculosis preventive treatment for travellers to high-burden countries and 10 (14.7%) for patients undergoing abdominal surgery.Conclusion Lack of solid evidence on certain aspects of management of latent tuberculosis infection results in national policies which vary considerably. This highlights a need to advance research and develop clear, implementable and evidence-based WHO policies.
a University of California Berkeley, School of Public Health, Berkeley, California, United States of America.b Global Tuberculosis Programme, World Health Organization, Avenue Appia 20, 1211 Geneva 27, Switzerland.Correspondence to Yohhei Hamada (email: [email protected]).(Submitted: 26 June 2017 – Revised version received: 17 December 2017 – Accepted: 18 December 2017 – Published online: 5 February 2018 )

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414174
ResearchNational policies on latent tuberculosis Ann Jagger et al.
per 100 000. Among the high-burden countries, we focused on the top 30 countries in terms of high burden of tuberculosis (both in terms of number of cases and incidence) and on the
top 30 countries in terms of high bur-den of HIV-associated tuberculosis. These countries account for most of the global burden of tuberculosis (9.1 out of 10.4 million cases, 88%) and
HIV-associated tuberculosis (0.91 out of 1.03 million, 88%).1 Because many countries feature in the top 30 of both lists, this produced a list of 35 target countries. Our approach resulted in
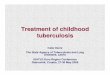
Fig. 1. Selection of countries for the review of national policies on management of latent tuberculosis infection
Countries and territories reporting data to the Global Tuberculosis Programme: 194 WHO Member States and 22 associate Member States and territories
113 high- and upper-middle income countries with an estimated annual tuberculosis incidence <100 per 100 000
68 policy documents obtained and included in the analysis
103 low- and lower-middle or other income countries with an estimated annual tuberculosis incidence ≥ 100 per 100 000
35 countries belonging to the 30 high tuberculosis or HIV-associated tuberculosis burden countries
30 policy documents obtained and included in the analysis
68 countries not belonging to the 30 high tuberculosis or HIV-associated
tuberculosis burden countries
45 policy documents on latent tuberculosis could not be obtained
5 policy documents on latent tuberculosis could not be obtained
HIV: human immunodeficiency virus.
Table 1. World Health Organization recommendations for the management of latent tuberculosis infection in low and high tuberculosis burden countries, October 2017
Tuberculosis burden classifica-tion
Risk groups defined Testing recommendations Diagnostic algorithms to exclude active tuberculosis
Treatment recommenda-tions
Low-burden countries
Strong recommendation: people living with HIV; adult and child household contacts of pulmonary tuberculosis cases; treatment with anti-tumour necrosis factor; organ transplantation; silicosis; end-stage renal disease Conditional recommendation: health-care workers; prisoners; immigrants from high-burden countries; illicit drug users; homeless people
Tuberculin skin test or interferon-gamma release assay
Symptomatic screening plus chest X-ray
6 months daily isoniazid; or 9 months daily isoniazid; or 3 months weekly rifapentine plus isoniazid; or 3–4 months daily isoniazid plus rifampicin; or 3–4 months daily rifampicin
High-burden countries
People living with HIV; children aged < 5 years; household contacts of pulmonary tuberculosis cases
Tuberculin skin test or interferon-gamma release assay not required. Tuberculin skin test encouraged for people living with HIV
Symptomatic screening alone
6 months daily isoniazid
HIV: human immunodeficiency virus. Sources: World Health Organization (WHO) Guidelines on the management of latent tuberculosis infection.11 WHO Recommendations for investigating contacts of persons with infectious tuberculosis in low- and middle-income countries.9 WHO Guidelines for intensified case-finding and isoniazid preventative therapy for people living with HIV in resource-constrained settings.10

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414 175
ResearchNational policies on latent tuberculosisAnn Jagger et al.
Table 2. Definitions of symptoms to exclude active tuberculosis before providing tuberculosis preventive treatment to adults and children living with human immunodeficiency virus (HIV) in countries with the highest burdens of tuberculosis or HIV-associated tuberculosis
Country Adults living with HIV Children living with HIV
Symptoms defined by WHO Additional symptoms or findings
Symptoms defined by WHO Additional symptoms or findings
Angola Current cough; fever; night sweats; weight loss
N/A Current cough; fever; weight loss or poor weight gain
Chest X-ray findings suggestive of tuberculosis
Bangladesh N/A N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
Fatigue, lethargy, neck mass, wheeze, ascites
Botswana N/A N/A N/A N/ACambodia Current cough; fever; night
sweats Fatigue; lethargy; wheeze; neck mass; abdominal mass; ascites
Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
Failure to thrive, enlarged lymph nodes
Cameroon Current cough; fever; night sweats; weight loss
N/A Current cough; fever; weight loss or poor weight gain
N/A
Central African Republic
Current cough; fever; night sweats; weight loss
N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
N/A
Democratic Republic of the Congo
Current cough; fever; night sweats; weight loss
N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
N/A
Ethiopia Current cough; fever; night sweats; weight loss
N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
N/A
Ghana N/A N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
Fatigue, lethargy, neck swelling, wheeze
India Current cough; fever; night sweats; weight loss
N/A N/A N/A
Indonesia Current cough; fever; night sweats; weight loss
Signs of extrapulmonary tuberculosis
N/A N/A
Kenya Current cough; fever; night sweats; weight loss
N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
Lethargy, less playful than usual
Lesotho Current cough; fever; night sweats; weight loss
N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
N/A
Malawi Current cough; fever; night sweats; weight loss
N/A Current cough; fever Failure to thrive, night sweats, malnutrition
Mozambique N/A N/A Current cough; fever; weight loss or poor weight gain
N/A
Myanmar Current cough; fever; night sweats; weight loss
N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
N/A
Namibia Current cough; fever; night sweats; weight loss
Chest pain; shortness of breath; haemoptysis; loss of appetite; diarrhoea; fatigue; enlarged lymph nodes
Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
Enlarged lymph nodes
(continues. . .)

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414176
ResearchNational policies on latent tuberculosis Ann Jagger et al.
a target of 148 countries (113 low-burden countries and 35 high-burden countries) for the study (Fig. 1).
We aimed to analyse each country’s or territory’s national guidelines on the management of tuberculosis, HIV, pae-diatric tuberculosis, latent tuberculosis infection and HIV-associated tuberculo-sis, and standard national operating pro-cedures for tuberculosis. We obtained documents by contacting WHO country offices or national programme manag-ers or by downloading them from the official website of the ministry of health or other national health organization.
We selected the information to be extracted a priori based on WHO recommendations for the manage-ment of latent tuberculosis infection (Table 1 and Table 2).9–11 We collected information on the following: (i) at-risk
populations targeted; (ii) recommended tests for latent tuberculosis infection; (iii) diagnostic algorithms to exclude active tuberculosis before starting treat-ment for latent tuberculosis infection; (iv) treatment regimens for latent tu-berculosis infection; and (v) presence of monitoring and evaluation systems for the management of latent tuberculosis infection. For high-burden countries, we focused the review only on people living with HIV and children younger than 5 years who have household contact with a tuberculosis case. One researcher collected and entered the data for all low-burden countries and another researcher for all high-burden countries using data extraction forms developed for the study.
Statistical analysis of the data was performed using GraphPad Prism
(GraphPad Software Inc., La Jolla, Unit-ed States of America) and STATA (Stata Corp LLC, College Station, USA) soft-ware. Where percentages are indicated, binary indicators (0,1) were created for the absence or presence of each policy item extracted. The means of those binary indicators corresponded to the percentage of countries addressing each policy item. The number and percentage of countries addressing each policy item were calculated and presented.
Results
Results of search
We obtained and analysed copies of policy documents from 98 countries (Table 3; available at: http://www.who.int/bulletin/volumes/96/3/17-199414).
Country Adults living with HIV Children living with HIV
Symptoms defined by WHO Additional symptoms or findings
Symptoms defined by WHO Additional symptoms or findings
Nigeria Current cough; fever; night sweats; weight loss
N/A N/A N/A
Pakistan Current cough; fever; night sweats; weight loss
N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
N/A
Papua New Guinea Current cough; night sweats; weight loss
N/A N/A N/A
Philippines Current cough; fever; night sweats; weight loss
N/A N/A N/A
Sierra Leone Current cough; fever; night sweats; weight loss
N/A N/A N/A
South Africa Current cough; fever; night sweats; weight loss
N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
Fatigue
Swaziland Current cough; fever; night sweats; weight loss
N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
N/A
Thailand N/A N/A N/A N/AUganda Current cough; fever; night
sweats; weight loss N/A N/A N/A
United Republic of Tanzania
Current cough; fever; night sweats; weight loss
N/A Fever; contact history with a tuberculosis case; weight loss or poor weight gain
N/A
Viet Nam Current cough; fever; night sweats; weight loss
N/A N/A N/A
Zambia Current cough; fever; night sweats; weight loss
N/A Current cough; fever; contact history with a tuberculosis case; weight loss or poor weight gain
N/A
Zimbabwe Current cough; fever; night sweats; weight loss
Haemoptysis N/A N/A
HIV: human immunodeficiency virus; N/A: data not available; WHO: World Health Organization. Notes: WHO recommended four-symptom algorithm for people living with HIV includes: current cough, fever, night sweats and weight loss for adults and current cough, fever, poor weight gain and contact history with a tuberculosis case for children.10
(. . .continued)

Ann Jagger et al. National policies on latent tuberculosisResearch
177Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414
For high-burden countries, we obtained guidelines from 30 of 35 (85.7%) high-burden countries. We were unable to retrieve any national policies pertaining to latent tuberculosis infection for Chad, Democratic People’s Republic of Korea, Guinea Bissau, Liberia and Congo. For guidelines obtained, publication year ranged between 2007 and 2016. We also included one draft guideline under review.
For low-burden countries, we were able to obtain policy documents from 68 of 113 (60.2%) countries, with a publica-tion year ranging from 2001 to 2015. The policy documents ranged from detailed policies focusing on latent tuberculosis infection to a brief mention of latent tuberculosis infection in a general tu-berculosis policy.
High-burden countries
Risk groups defined
Of the 30 high-burden countries for which guidelines were obtained, infor-mation on the management of latent tuberculosis infection among children with a household contact was available for 25 countries. In four countries the relevant tuberculosis guidelines could not be obtained and in one country the guidelines were written in local languages that we were not able to translate. All 25 countries followed WHO policy (Table 1) recommending treatment for children younger than 5 years with a household tuberculosis contact (Table 4); 17 of these specifically targeted contacts of smear-positive cases. India and Nigeria recommended preventive treatment for children under 6 years old with a house-hold contact. No policy recommended preventive treatment for contacts of a multidrug-resistant tuberculosis case.
For people living with HIV, 29 countries (96.7%) had recommenda-tions on tuberculosis preventive treat-ment; only Ghana did not provide any recommendations.
Testing recommendations
For children younger than 5 years with a household contact, 24/25 (96.0%) of the countries analysed did not have recommendations for testing for latent tuberculosis before starting preventive treatment. Only in the Philippines was a tuberculin skin test recommended, with the option to provide preventive treat-ment without testing when testing was
not available. To exclude active tuber-culosis before treatment of latent tuber-culosis, most countries (24/25, 96.0%) had a policy on symptomatic screening alone. Symptom-based algorithms to ex-clude active tuberculosis were defined in the guidelines of 12 countries (Table 2).
Of these, 11 countries included cough, fever and weight loss or poor weight gain in their algorithms. The presence of a va-riety of additional symptoms and signs were also specified: fatigue, wheeze, neck mass, abdominal mass, ascites, diarrhoea, loss of appetite and night
Table 4. Recommendations for management of latent tuberculosis infection in countries with the highest burdens of tuberculosis or HIV-associated tuberculosis
Indicator Total no. of countries reviewed
No. (%) following recommendation
Guidelines identified on testing and treatment of tuberculosis, with or without HIV
35 30 (85.7)
Latent tuberculosis infection treatment recommended for:
Children aged < 5 years with household tuberculosis contact
Yes 30 25 (83.3) Unknowna 30 5 (16.7)People living with HIV Yes 30 29 (96.7) No 30 1 (3.3)Recommended treatment regimens 6 months isoniazid monotherapy 30 18 (60.0)6–9 months isoniazid monotherapy 30 6 (20.0)Isoniazid monotherapy, other durations 30 5 (16.7)6 months isoniazid and 3 months rifampicin 30 1 (3.3)Monitoring and evaluation indicators Isoniazid preventive therapy for children aged < 5 years with household tuberculosis contact
30 4 (13.3)
Screening coverage among children aged < 5 years with household tuberculosis contact
30 7 (23.3)
Isoniazid preventive treatment coverage among HIV-infected people
30 18 (60.0)
Isoniazid preventive treatment reporting tool available 30 15 (50.0)Screening of children aged < 5 years old with household tuberculosis contact
Clinical examination only 30 24 (80.0)Clinical examination and tuberculin skin test 30 1 (3.3)Unknown 30 5 (16.7)Screening of HIV-infected people Adults Clinical examination only 30 26 (86.7) Clinical examination and tuberculin skin test 30 1 (3.3) Not defined 30 3 (10.0)Children aged > 12 months Clinical examination only 30 20 (66.7) Clinical examination and tuberculin skin test 30 1 (3.3) Clinical examination and chest X-ray 30 1 (3.3) Not defined 30 8 (26.7)
HIV: human immunodeficiency virus. a We could not obtain any relevant treatment guidelines for child contacts and we found no
recommendations in other available guidelines (4 countries) or the guidelines were written in a local language and we were unable to translate them with confidence (1 country).

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414178
ResearchNational policies on latent tuberculosis Ann Jagger et al.
sweats. The exclusion algorithm was not defined in the remaining countries.
For people living with HIV, 86.7% (26/30) of the high-burden countries analysed provided preventive treatment for latent tuberculosis without testing for infection. In South Africa the recom-mendation was for a tuberculin skin test before starting preventive treatment, but this was not specified by the remaining countries. The majority of the countries (20/30) applied the WHO four-symp-tom screening rule (current cough, fever, weight loss and night sweats) for ex-cluding pulmonary tuberculosis before starting preventive treatment (Table 2). Five countries specified a different set of symptoms and another five countries did not specify the symptoms to be used in the exclusion algorithm.
For children older than 12 months living with HIV, 66.7% (20/30) of high-burden countries had a recom-mendation for symptomatic screening alone before starting preventive treat-ment. Only India had a policy of doing a tuberculin skin test in addition to symptomatic screening before starting such treatment. In Angola, the recom-mendations were for chest radiography in addition to symptomatic screening. Only eight (26.7%) countries followed the WHO recommendation to exclude active tuberculosis based on poor weight gain, fever, current cough or contact his-tory with a tuberculosis case (Table 2).
Treatment recommendations
WHO recommends 6 months of iso-niazid monotherapy both for people living with HIV and children with a household contact in high-burden coun-tries (Table 1). Among the high-burden countries reviewed, the majority (18/30) of guidelines recommended 6 months of isoniazid monotherapy, while in six countries (Cambodia, Democratic Republic of Congo, Namibia, Thailand, Viet Nam and Zimbabwe) it was a course of 6‒9 months. Central African Republic had a policy of 3 months of rifampicin plus isoniazid, as well as 6 months of iso-niazid (Table 4). In Uganda and Pakistan recommendations were for an additional course of prolonged isoniazid treatment (12 and 36 months, respectively) for people living with HIV who have tuber-culosis contact history. In South Africa the recommendations were 6‒36 months of isoniazid treatment, depending on the
results and availability of tuberculin skin testing. In Malawi the policy was contin-uation of isoniazid treatment for those not receiving antiretroviral therapy but discontinuation once therapy is started.
Monitoring and evaluation indicators
Of the high-burden countries, only Ke-nya, Malawi, South Africa and Thailand had guidelines that defined indicators to evaluate the coverage of tuberculosis screening and preventive treatment among children younger than 5 years with a household contact. Most coun-tries (18/30) defined an indicator for coverage of preventive treatment in people living with HIV (Table 4). In 2017, 10 of these countries reported data to the Global tuberculosis report1 about the proportion of patients newly enrolled in HIV care who were provided with tuberculosis preventive treatment (Table 5). Fifteen countries included information on recording and reporting tools for isoniazid preventive treatment in their guidelines (Table 4).
Low-burden countries
Risk groups defined
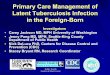
The risk groups strongly recommended by WHO to be targeted for latent tu-berculosis infection screening (Table 1) were included in the national latent tu-berculosis infection policies of between 19 (27.9%) and 54 (79.4%) of 68 low-burden countries (Fig. 2). Specifically, 28 countries (42.1%) had a recommen-dation to screen children younger than 5 years who are contacts of a tubercu-losis case. An additional 49 countries (70.1%) had recommendations to screen all contacts of a tuberculosis case, mak-ing no distinction between adults and children. For people living with HIV, the policy in 54 (79.4%) countries was to screen people living with HIV for latent tuberculosis infection and in 23 (33.8%) countries it was to screen im-munocompromised individuals, which includes people living with HIV.
In contrast, some of the condition-ally recommended categories (such as
Table 5. Tuberculosis preventive treatment for people newly enrolled in human immunodeficiency virus (HIV) care in countries with the highest burdens of tuberculosis or HIV-associated tuberculosis, 2016
Country No. (%) of people living with HIV who were newly enrolled in HIV carea
Indicator defined in national policyb
Total Provided with tuberculosis preven-
tive treatment
Diagnosed with active tubercu-
losis
Cambodia 3 193 631 (19.8) N/A YesEthiopia 36 761 19 244 (52.3) 2 165 (5.9) YesIndia 174 125 8 135 (4.7) 21 032 (12.1) NoIndonesia 36 294 877 (2.4) 9 792 (27.0) YesLiberia 4 528 390 (8.6) 1 219 (26.9) N/AMalawi 145 117 72 446 (49.9) 2 402 (1.7) YesMozambique 315 712 162 646 (51.5) N/A YesMyanmar 34 765 1 018 (2.9) 3 960 (11.4) YesNigeria 216 293 62 781 (29.0) 14 794 (6.8) YesPhilippines 5 966 2 938 (49.2) 1 645 (27.6) NoSierra Leone 17 843 3 609 (20.2) 1 627 (9.1) NoSouth Africa 751 620 385 932 (51.3) N/A YesSwaziland 138 016 21 320 (15.4) 2 342 (1.7) YesUnited Republic of Tanzania
49 351 4 202 (8.5) N/A Yes
Viet Nam 13 593 3 474 (25.6) N/A NoZimbabwe 168 968 123 846 (73.3) 9 176 (5.4) No
N/A: data not available.a Data are from the World Health Organization Global tuberculosis report.1 b Indicator for coverage of preventive treatment in people living with HIV was defined in the national policy.
Note: The table includes only the 16 countries that reported data on preventive treatment among people living with HIV in 2017.

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414 179
ResearchNational policies on latent tuberculosisAnn Jagger et al.
prisoners and illicit drug users; Table 1) were rarely mentioned in policies (Fig. 2). Notably, some countries in-cluded categories that are not recom-mended by the WHO; nine countries (13.2%) recommended tuberculosis preventive treatment for travellers to high tuberculosis burden countries and 10 (14.7%) for patients undergoing abdominal surgery.
Testing recommendations
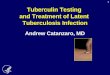
The WHO latent tuberculosis infection guidelines indicate that in low-burden countries either a tuberculin skin test or interferon-gamma release assay can be used for diagnosis (Table 1). Of the low-burden countries 33/68 (48.5%) had a recommendation to use tuberculin
skin testing as the primary screen-ing method compared with only 2/68 (2.8%) recommending interferon assay (Fig. 3). In 21 countries (30.8%), the policy was either tuberculin skin test or interferon assay as the primary method of screening. In addition, multiple poli-cies specified situations when using one test over the other was preferable. For example, in 21 (30.8%) countries the policy was that interferon assay should be used for individuals vaccinated with bacille Calmette–Guérin (BCG) and in 17 (25.0%) countries that interferon assay and tuberculin skin test should be used sequentially. For some countries, including Costa Rica and Uruguay, there were no explicit recommendations on methods of testing.
An algorithm for excluding active tuberculosis was specified in the poli-cies of 43 (63.2%) low-burden countries, although the content of that algorithm varied greatly from country to country. In Colombia, Ecuador and Uruguay the recommendation was only that active tuberculosis should be ruled out, with no mention of an exclusion algorithm. All other countries required at least a chest X-ray.
Treatment recommendations
The most commonly recommended treatments in low-burden countries were isoniazid for 6 months (55 coun-tries; 80.8%) or 9 months (55 countries, 80.8%) (Fig. 4), which is in line with the WHO guidelines on treatment of latent tuberculosis (Table 1). Alternative treatment options recommended by the WHO were also frequently mentioned in other policies, but to a lesser extent, ranging from 8 (11.7%) to 51 (75.0%) countries.
Monitoring and evaluation indicators
Monitoring and evaluation of latent tuberculosis infection screening was mentioned in the policies of 32 (47.1%) low-burden countries. Even among the countries that mentioned reporting requirements, those were often specific to active tuberculosis, and therefore the form may be inappropriate for latent tuberculosis infection.
DiscussionThis review identified that the majority of both high- and low-burden countries had a national policy that addressed la-tent tuberculosis infection management in people living with HIV and children younger than 5 years with a household contact. Clinical high-risk groups were also covered by most guidelines from low-burden countries. However, the content of the guidelines varied con-siderable across countries. For example, clear and standard algorithms for ex-cluding tuberculosis before treatment and latent tuberculosis infection testing were not available in many countries, and indicators for monitoring and evalu-ation were rarely defined. Guidelines are the first step in implementing the programmatic management of latent tu-berculosis infection, hence it is essential to provide clear and simple operational
Fig. 2. Compliance of national policies with World Health Organization guidelines on screening for latent tuberculosis infection among high-risk population groups in low-burden countries
Homeless peopleChildren aged <5 years with new tuberculosis infection
Patients with haematologic malignanciesIllicit drug users
Travellers to high tuberculosis burden countriesPatients with gastrectomy
Malnourished or underweight peoplePatients with diabetes
Patients with incomplete tuberculosis treatmentPatients with tuberculin skin test conversion
Patients with jejunoileal bypassPatients with radiographic evidence
Immigrants from high tuberculosis burden countriesPatients with end-stage renal disease
PrisonersPatients with silicosis
Immunocompromized (nonspecific) peoplePatients with head or neck carcinoma
Children aged <15 yearsOther occupational groups
Health-care workersOrgan transplant or blood transfusion recipients
Patients treated with anti-tumour necrosis factorPeople with a tuberculosis contact
People living with HIV infection
Risk
gro
ups
% of countries recommending screening0 10 20 30 40 50 60 70 80 90 100
Conditionally recommended by WHONot recommended by WHO
Strongly recommended by WHO
WHO: World Health Organization.Notes: WHO Guidelines on screening for latent tuberculosis infection11 are summarized in Table 1. Risk groups targeted by fewer than 3% of low-burden countries are not shown on the chart. The risk categories not shown are: people with harmful alcohol use; patients with incomplete tuberculosis treatment; elderly people; children born to tuberculosis-positive mothers; and tobacco smokers. The total number of countries analysed was 68.

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414180
ResearchNational policies on latent tuberculosis Ann Jagger et al.
guidance, including evidence-based standardized algorithms and a frame-work of monitoring and evaluation.14
The advantage of an evidence-based standardized algorithm was demon-strated by the WHO recommended four-symptom screening rule to exclude active tuberculosis before starting pre-ventive treatment for people living with HIV.10 This simple algorithm adds to the clarity of the policy and has resulted in a steep rise in implementation of isoniazid preventive treatment among people living with HIV in settings with a high prevalence of tuberculosis and low resources, reaching 1.3 million in 2016.1 Ensuring that guidelines and algorithms are simple can also facilitate their in-corporation into national guidelines. For example, seven out of 10 countries that had algorithms different from the WHO recommendation in a previous policy review15 have now adopted them (Cameroon, Lesotho, Nigeria, South Africa, Swaziland, United Republic of Tanzania and Viet Nam).
In contrast to the uptake of the screening algorithm for people living
with HIV, the corresponding screening algorithm for children was not taken up or defined in national policies. This could be due to the limited evidence about the effectiveness of the algorithm, as it was recommended largely based on expert opinion.16 Further research is needed to evaluate the performance of the algorithm and identify the optimal approach to exclude active tuberculosis in children before starting preventive treatment.
Consistent with our previous study,13 we found that the national policies and guidelines in the major-ity of low-burden countries addressed latent tuberculosis infection specifically or as part of the general tuberculosis policy. The Netherlands has revised its guidelines since the publication of the 2015 WHO latent tuberculosis infection guidelines,17 which are now mostly con-sistent with WHO recommendations. A similar revision by other countries would increase alignment between na-tional policies and WHO recommenda-tions. This could lead to more consistent and comprehensive latent tuberculosis
infection policies and pave the way for global monitoring and evaluation of the programmatic management of latent tuberculosis infection. Although it may be too early to evaluate the impact of such policy changes on tuberculosis incidence, it is a question that needs to be addressed in the future.
Tuberculin skin testing was the most frequently recommended diag-nostic tool. The test requires no labora-tory work and is comparably cheaper per unit test than interferon-gamma release assay. That may explain the overwhelming preference for the test over interferon assay in the policies of low-burden countries. Several coun-tries specified additional diagnostic algorithms, such as different tuberculin skin test cut-off points among specific risk groups, sequential use of the two tests, or use of interferon assay for BCG-vaccinated individuals. A system-atic review did not show a significant difference in the prediction of progres-sion to active tuberculosis between the two tests in head-to-head analysis.11 However, there were insufficient data on the predictive utility among specific populations. The diversity of policies across countries calls for more research in how to use interferon-gamma re-lease assay and tuberculin skin testing together among different risk groups based on the underlying tuberculosis epidemiology.
This policy review has limitations. First, determining the latest published guidelines was done through contact-ing national programmes, WHO of-fices and through extensive internet searches; however some policies may not have been identified. Even though latent tuberculosis infection monitor-ing and evaluation indicators may not have been defined in guidelines they may nevertheless exist within a coun-try’s national tuberculosis programme or other guidelines. These limitations might have led to misclassification of the findings. Second, a single person was responsible for reviewing policies, extracting relevant information and entering data within each group (high-and low-burden countries). While this provided internal consistency, the data collection may have been subject to reviewer bias.
Fig. 3. Recommendations for screening methods for latent tuberculosis infection in the national policies of low-burden countries
Interferon assay (primary)
Tuberculin skin test for repeat testing (e.g. contact investigation)
Interferon assay for outbreak investigation for children aged >5 years
Interferon assay for immunocompromised people
Sequential use of tuberculin skin test and interferon assay
Tuberculin skin test for contact investigation for children aged <5 years
Interferon assay for BCG-vaccinated people
Tuberculin skin test or interferon assay
Tuberculin skin test (primary)
Scre
enin
g m
etho
d fo
r lat
ent t
uber
culo
sis
% of countries recommending method0 10 20 30 40 50 60 70 80 90 100
BCG: bacille Calmette-Guérin; WHO: World Health Organization.Notes: World Health Organization guidelines are that either tuberculin skin test or interferon-gamma release assay can be used to screen for latent tuberculosis infection.11 Interferon assay refers to interferon-gamma release assay. The total number of countries analysed was 68.

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414 181
ResearchNational policies on latent tuberculosisAnn Jagger et al.
ملخصالسياسات الوطنية املتبعة للتعامل مع عدوى السل الكامنة: مراجعة شملت 98 بلًدا
الغرض مراجعة السياسات املتبعة للتعامل مع عدوى السل الكامنة يف البلدان التي تعاين من معدالت منخفضة لإلصابة بمرض السل
والبلدان التي تعاين من معدالت مرتفعة لإلصابة باملرض.العاملي للربنامج بيانات التي قدمت البلدان بتقسيم قمنا الطريقة إىل السل مرض بمكافحة واملعني العاملية الصحة ملنظمة التابع بلدان لدهيا معدالت منخفضة وأخرى تعاين من معدالت مرتفعة العاملية. وقد استناًدا ملعايري منظمة الصحة بالسل وذلك لإلصابة حددنا وثائق السياسات الوطنية للتعامل مع مرض السل الكامن اإللكرتونية واملواقع اإلنرتنت شبكة عىل البحث خالل من واالتصال العاملية الصحة ملنظمة الُقطرية واملكاتب للحكومات الشخيص مع مديري الربنامج. كام قمنا بإجراء حتليل وصفي يركز توصيات عن املتبعة السياسات يف احليود وحاالت الثغرات عىل
السياسات ملنظمة الصحة العاملية.113 بلًدا أصل من 68 بلًدا من وثائق عىل حصلنا النتائج السل مرض أو السل بمرض لإلصابة منخفضة معدالت لدهيا املصاحب لفريوس عوز املناعة البرشي )HIV(، كام حصلنا عىل 35 بلًدا تعاين من معدالت مرتفعة. 30 بلًدا من أصل وثائق من الكامنة لدى السل وقد وردت توصيات بفحص وعالج عدوى
املتبعة التوجيهية املبادئ املناعة البرشي يف املصابني بفريوس عوز لدى 29 بلًدا )بواقع 96.7 %( تعاين من ارتفاع معدالت اإلصابة معدالت لدهيا )% 79.7 )بواقع بلًدا 54 يف وكذلك باملرض، منخفضة لإلصابة باملرض. ونصت السياسات عىل وجوب إجراء أفراد العرضة لالتصال مع 5 سنوات فحص لألطفال دون عمر األرسة املصابني بمرض السل، وذلك يف 25 بلًدا )بنسبة 83.3 %( 28 بلًدا يف وكذلك باملرض لإلصابة مرتفعة معدالت من تعاين التوصيات لدهيا معدالت منخفضة. واقترصت )% 41.2 )بنسبة يف معظم البلدان التي تعاين من معدالت مرتفعة لإلصابة باملرض عىل جمرد إجراء فحص قائم عىل أعراض اإلصابة قبل العالج، يف حني أن البلدان التي لدهيا معدالت منخفضة لإلصابة تلتزم بإجراء االختبارات قبل العالج. وال تتوافق سياسات بعض البلدان التي الصحة منظمة توصيات مع لإلصابة منخفضة معدالت لدهيا العاملية؛ حيث أوصت تسعة بلدان )13.2 %( املسافرين إىل ابلدان باحلصول السل بمرض اإلصابة معدالت ارتفاع من تعاين التي عىل عالج وقائي للمرض، يف حني أوصت عرشة بلدان )14.7 %( باحلصول عىل العالج الوقائي للمرىض الذين خيضعون جلراحة يف
البطن.
In conclusion, our review identi-fied large variations across countries in their national tuberculosis policies. The differences are probably attributable to different country contexts and disease epidemiology and lack of consensus on some aspects of latent tuberculosis infection management. There are unique challenges associated with management of latent tuberculosis infection, such as exclusion of active tuberculosis, test-ing for latent tuberculosis infection and treatment initiation. It is therefore important to continue to develop clear, implementable and evidence-based WHO policies. An important compo-nent of such policies should be monitor-ing and evaluation, as this is essential to assess progress in the implementation and to make policy decisions. Lack of a monitoring and evaluation component in more than half of the national poli-cies presents a barrier to programmatic management of latent tuberculosis in-fection. ■
AcknowledgementsThe authors thank Fatima Kazi, Annabel Baddeley and all the programme manag-ers, WHO regional and country staff.
Competing interests: None declared.
Fig. 4. Compliance of national policies with World Health Organization guidelines on treatment of latent tuberculosis infection in low-burden countries
3 months twice weekly isoniazid + rifampicin
3 months weekly rifapentine + isoniazid
6 months rifampicin
6–9 months weekly isoniazid
12 months isoniazid
Special instructions for children
4 months isoniazid + rifampicin
3 months isoniazid + rifampicin
3–4 months rifampicin
9 months isoniazid
6 months isoniazid
Trea
tmen
t for
late
nt tu
berc
ulos
is
% of countries recommending treatment0 10 20 30 40 50 60 70 80 90 100
Not recommended by WHO
Recommended by WHO
WHO: World Health Organization.Notes: WHO guidelines on treatment of latent tuberculosis infection11 are summarized in Table 1. Special instructions for children refer to any policy recommendation for an alternative treatment or duration of treatment for children younger than 5 years. The total number of countries analysed was 68.

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414182
ResearchNational policies on latent tuberculosis Ann Jagger et al.
摘要潜伏性结核感染管理国家政策:对 98 个国家的回顾目标 回顾结核病低负担国家和结核病高负担国家在潜伏性结核感染上的管理政策。方法 我 们 根 据 世 界 卫 生 组 织 (WHO) 的 标 准 将向 WHO 全球结核病项目汇报数据的国家划分为结核病低负担国家和结核病高负担国家。我们通过在线搜索、政府网站、WHO 国家办事处和与项目管理者的个人沟通,确定了关于潜伏性结核感染管理的国家政策文件。我们进行了描述性分析,重点关注该国政策与 WHO 政策建议的差距和偏差。结果 在 113 个结核病低负担国家和 35 个结核病高负担国家中,我们分别获得了 68 个国家和 30 个国 家 的 结 核 病 或 人 类 免 疫 缺 陷 病 毒 (HIV) 相关 结 核 病 的 文 件。 在 29 个 结 核 病 高 负 担 国家 (96.7%) 和 54 个 (79.7%) 结核病低负担国家的指
导方针中,建议对 HIV 感染者进行潜伏性结核感染 的 筛 查 和 治 疗。25 个 (83.3%) 结 核 病 高 负 担 国家和 28 个 (41.2%) 结核病低负担国家的政策规定,对 5 岁以下、家中有结核病接触的孩子进行筛查。在大多数高负担国家,建议在治疗前单独进行症状筛查,而在全部低负担国家,则在治疗之前进行检测。一些低负担国家的政策不符合 WHO 建议 :其中有 9 项 (13.2%) 政策建议对准备去结核病高负担国家的游客进行结核病预防治疗,10 项 (14.7%) 建议患者接受腹部手术。结论 潜伏性结核感染管理的某些方面缺乏确凿依据,导致国家政策方面有很大差异。这突出了对推动研究,制定清晰、可执行和以证据为基础的 WHO 政策的需求。
Résumé
Politiques nationales pour la prise en charge de l’infection tuberculeuse latente: revue de 98 paysObjectif Passer en revue les politiques relatives à la prise en charge de l’infection tuberculeuse latente de pays faiblement ou fortement touchés par la tuberculose.Méthodes Nous avons séparé les pays qui transmettent des données au Programme mondial de lutte contre la tuberculose de l’Organisation mondiale de la Santé (OMS) selon qu’ils présentaient une charge de morbidité tuberculeuse faible ou élevée, suivant les critères de l’OMS. Nous avons trouvé les politiques nationales pour la prise en charge de la tuberculose latente grâce à des recherches en ligne, aux sites Internet des gouvernements, aux bureaux de l’OMS dans les pays et à des communications personnelles avec des responsables de programmes. Nous avons fait une analyse descriptive axée particulièrement sur les lacunes des politiques et leurs écarts des recommandations de l’OMS.Résultats Nous avons obtenu des documents de 68 pays sur 113 ayant une faible charge de morbidité tuberculeuse et de 30 pays sur 35 ayant les plus fortes charges de morbidité dues à la tuberculose ou à la tuberculose associée au virus de l’immunodéficience humaine (VIH). Le dépistage et le traitement de l’infection tuberculeuse latente chez les personnes vivant avec le VIH étaient recommandés dans les
directives de 29 pays (96,7%) à la charge de morbidité élevée et de 54 pays (79,7%) où cette charge était faible. Le dépistage des enfants de moins de 5 ans en contact familial avec la tuberculose était prévu dans 25 pays (83,3%) à la charge de morbidité élevée et dans 28 (41,2%) à la charge de morbidité faible. Dans la plupart des pays à la charge de morbidité élevée, seule la recherche des symptômes avant traitement était recommandée, tandis que tous les pays à la charge de morbidité faible recommandaient un dépistage avant traitement. Les politiques de certains pays à la charge de morbidité faible ne suivaient pas les recommandations de l’OMS: neuf (13,2%) recommandaient un traitement préventif contre la tuberculose pour les personnes se rendant dans des pays à la charge de morbidité élevée et 10 (14,7%) pour les patients subissant une chirurgie abdominale.Conclusion En l’absence de preuves solides concernant certains aspects de la prise en charge de l’infection tuberculeuse latente, les politiques nationales varient considérablement les unes des autres. Cela met en lumière la nécessité de faire progresser la recherche et, pour l’OMS, d’élaborer des politiques claires, applicables et fondées sur des éléments probants.
Резюме
Национальная политика по борьбе с латентной туберкулезной инфекцией: обзор 98 странЦель Провести обзор политики по борьбе с латентной туберкулезной инфекцией в странах с низким и высоким бременем туберкулеза.Методы На основе критериев ВОЗ авторы разделили страны, предоставляющие данные для Глобальной программы борьбы с туберкулезом Всемирной организации здравоохранения (ВОЗ), на несущие низкое и высокое бремя туберкулеза. Авторы
определили документы национальной политики по борьбе с латентным туберкулезом посредством онлайн-поиска, правительственных веб-сайтов, региональных бюро ВОЗ и личного общения с руководителями программ. Был проведен описательный анализ с упором на пробелы и отклонения от рекомендаций ВОЗ в политике.
االستنتاج يقود االفتقار إىل أدلة قوية بشأن بعض جوانب التعامل مع عدوى السل الكامنة إىل اعتامد سياسات وطنية متفاوتة بصورة بالبحث النهوض إىل احلاجة عىل الضوء ذلك ويسلط كبرية.
من األدلة عىل وقائمة للتنفيذ وقابلة واضحة سياسات وتطوير جانب منظمة الصحة العاملية.

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414 183
ResearchNational policies on latent tuberculosisAnn Jagger et al.
Результаты Были получены документы от 68 из 113 стран с низким бременем и от 30 из 35 стран с самым высоким бременем туберкулеза или вируса иммунодефицита человека (ВИЧ), связанного с туберкулезом. Скрининговое обследование и лечение латентной туберкулезной инфекции у людей с ВИЧ были рекомендованы в руководящих принципах 29 стран (96,7%) с высоким бременем и 54 стран (79,7%) с низким бременем туберкулеза. Скрининговое обследование детей в возрасте до 5 лет, находящихся в контакте с больными туберкулезом в бытовых условиях, проводился в рамках политики 25 стран (83,3%) с высоким бременем и 28 стран (41,2%) с низким бременем. В большинстве стран с высоким бременем туберкулеза перед началом лечения рекомендовано только скрининговое
обследование симптомов, тогда как во всех странах с низким бременем проводится тестирование. Политика некоторых стран с низким бременем не соответствовала рекомендациям ВОЗ: в девяти странах (13,2%) рекомендована профилактика туберкулеза для путешественников, выезжающих в страны с высоким бременем, и в 10 (14,7%) — для пациентов, перенесших абдоминальное хирургическое вмешательство.Вывод Отсутствие убедительных доказательств некоторых аспектов борьбы с латентной туберкулезной инфекцией приводит к значительным различиям в национальной политике. Это подчеркивает необходимость продвижения исследований и разработки четкой, реализуемой и основанной на фактических данных политики ВОЗ.
Resumen
Las políticas nacionales sobre el tratamiento de la infección de tuberculosis latente: análisis de 98 paísesObjetivo Analizar las políticas sobre el tratamiento de la infección de tuberculosis latente en países con niveles bajos y elevados de tuberculosis.Métodos Dividimos a los países que informan datos al Programa Global de Tuberculosis de la Organización Mundial de la Salud (OMS) en nivel de tuberculosis bajo y elevado, conforme a los criterios de la OMS. Identificamos los documentos de políticas nacionales sobre el tratamiento de la tuberculosis latente a través de búsquedas en línea, sitios web gubernamentales, sedes nacionales de la OMS y comunicación personal con los administradores del programa. Realizamos un análisis descriptivo enfocado en las desviaciones y los vacíos de las políticas con respecto a las recomendaciones de políticas de la OMS.Resultados Obtuvimos documentos de 68 de 113 países con nivel bajo y de 30 de 35 países con los niveles más elevados de tuberculosis o tuberculosis asociada con el virus de la inmunodeficiencia humana (VIH). En las pautas de 29 (96,7%) países con nivel elevado y 54 (79,7%) países con nivel bajo se recomendaron exámenes de detección y
tratamiento de la infección de tuberculosis latente en personas que viven con el VIH. La política de 25 (83,3%) países con nivel elevado y de 28 (41,2%) países con nivel bajo se basó en exámenes de detección en niños menores de cinco años de edad con contacto doméstico con tuberculosis. En casi todos los países con nivel elevado, la recomendación consistió únicamente en el examen de detección de los síntomas antes del tratamiento, mientras que, en todos los países con nivel bajo, esta consistió en pruebas antes del tratamiento. Las políticas de algunos países con nivel bajo no cumplen con las recomendaciones de la OMS: nueve (13,2%) recomendaron el tratamiento preventivo de la tuberculosis para viajeros que se dirijan a países con nivel elevado y 10 (14,7%) para pacientes que se sometan a una cirugía abdominal.Conclusión La falta de pruebas sólidas sobre ciertos aspectos del tratamiento de la infección de tuberculosis latente da lugar a políticas nacionales que varían considerablemente. Esto subraya la necesidad de realizar investigaciones avanzadas y desarrollar políticas de la OMS que sean claras, implementables y empíricas.
References1. Global tuberculosis report. Geneva: World Health Organization; 2017.2. Uplekar M, Weil D, Lonnroth K, Jaramillo E, Lienhardt C, Dias HM, et al.;
for WHO’s Global TB Programme. WHO’s new end TB strategy. Lancet. 2015 May 2;385(9979):1799–801. doi: http://dx.doi.org/10.1016/S0140-6736(15)60570-0 PMID: 25814376
3. Getahun H, Matteelli A, Chaisson RE, Raviglione M. Latent Mycobacterium tuberculosis infection. N Engl J Med. 2015 May 28;372(22):2127–35. doi: http://dx.doi.org/10.1056/NEJMra1405427 PMID: 26017823
4. Framework towards tuberculosis elimination in low-incidence countries. Geneva: World Health Organization; 2014.
5. Lobue P, Menzies D. Treatment of latent tuberculosis infection: An update. Respirology. 2010 May;15(4):603–22. doi: http://dx.doi.org/10.1111/j.1440-1843.2010.01751.x PMID: 20409026
6. Badje AD, Moh R, Gabillard D, Guehi C, Kabran M, Menan H, et al. Six-month IPT reduces mortality independently of ART in African adults with high CD4. Abstract Number: 78. In: Conference on Retroviruses and Opportunistic Infections, 13–16 February 2017, Seattle, United States of America. San Francisco: CROI Foundation; 2017.
7. Danel C, Moh R, Gabillard D, Badje A, Le Carrou J, Ouassa T, et al.; TEMPRANO ANRS 12136 Study Group. A trial of early antiretrovirals and isoniazid preventive therapy in Africa. N Engl J Med. 2015 Aug 27;373(9):808–22. doi: http://dx.doi.org/10.1056/NEJMoa1507198 PMID: 26193126
8. Getahun H, Matteelli A, Abubakar I, Hauer B, Pontali E, Migliori GB. Advancing global programmatic management of latent tuberculosis infection for at risk populations. Eur Respir J. 2016 May;47(5):1327–30. doi: http://dx.doi.org/10.1183/13993003.00449-2016 PMID: 27132266
9. Recommendations for investigating contacts of persons with infectious tuberculosis in low- and middle-income countries. Geneva: World Health Organization; 2012.
10. Guidelines for intensified case-finding and isoniazid preventative therapy for people living with HIV in resource-constrained settings. Geneva: World Health Organization; 2011.
11. Guidelines on the management of latent tuberculosis infection. Geneva: World Health Organization; 2015.
12. Getahun H, Matteelli A, Abubakar I, Aziz MA, Baddeley A, Barreira D, et al. Management of latent Mycobacterium tuberculosis infection: WHO guidelines for low tuberculosis burden countries. Eur Respir J. 2015 Dec;46(6):1563–76. doi: http://dx.doi.org/10.1183/13993003.01245-2015 PMID: 26405286
13. Hamada Y, Sidibe A, Matteelli A, Dadu A, Aziz MA, Del Granado M, et al. Policies and practices on the programmatic management of latent tuberculous infection: global survey. Int J Tuberc Lung Dis. 2016 Dec;20(12):1566–71. doi: http://dx.doi.org/10.5588/ijtld.16.0241 PMID: 27931330

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414184
ResearchNational policies on latent tuberculosis Ann Jagger et al.
14. Getahun H, Granich R, Sculier D, Gunneberg C, Blanc L, Nunn P, et al. Implementation of isoniazid preventive therapy for people living with HIV worldwide: barriers and solutions. AIDS. 2010 Nov;24 Suppl 5:S57–65. doi: http://dx.doi.org/10.1097/01.aids.0000391023.03037.1f PMID: 21079430
15. Gupta S, Granich R, Date A, Lepere P, Hersh B, Gouws E, et al. Review of policy and status of implementation of collaborative HIV-TB activities in 23 high-burden countries. Int J Tuberc Lung Dis. 2014 Oct;18(10):1149–58. doi: http://dx.doi.org/10.5588/ijtld.13.0889 PMID: 25216827
16. Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource-constrained settings. Geneva: World Health Organization; 2011.
17. Richtlijn behandeling latente tuberculose-infectie. Den Haag: KNVC Tuberculosis Foundation; 2015. Dutch. Available from: https://www.nvalt.nl/kwaliteit/richtlijnen/infectieziekten//Infectieziekten/KNCV%20Richtlijn%20Behandeling%20latente%20tuberculose-infectie%202015.pdf [cited 2018 Jan 5].

Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414 184A
ResearchNational policies on latent tuberculosisAnn Jagger et al.
Tabl
e 3.
Li
st o
f cou
ntrie
s and
terr
itorie
s inc
lude
d in
the
revi
ew o
f nat
iona
l pol
icies
on
the
man
agem
ent o
f lat
ent t
uber
culo
sis in
fect
ion
and
Wor
ld H
ealth
Org
aniz
atio
n re
com
men
datio
ns o
n tu
berc
ulos
is
Coun
try o
r ter
ritor
yW
HO re
gion
Coun
try g
roup
Data
sour
ce
Hig
h tu
berc
ulos
is b
urde
n co
untr
ies
Ango
laAF
RH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enNo
ta te
cnica
sobr
e as
mun
danc
as n
o di
agno
stico
e tr
etam
ento
da
infe
ccao
pel
o VI
H e
SIDA
em
Ang
ola
para
ad
ulto
s, ge
stan
tes,
adol
esce
ntes
e cr
ianc
as. L
uand
a: M
inist
erio
da
Saud
e, In
situt
o N
acio
nal d
e Lu
ta c
ontra
a
SIDA
; 201
4. R
otoc
olo
para
ava
liaçã
o e
segu
imen
to d
e en
ferm
agem
aos
pac
ient
es V
IH+. L
uand
a: M
inist
erio
da
Saud
e, In
situt
o N
acio
nal d
e Lu
ta c
ontra
a S
IDA;
201
4.
Bang
lade
shSE
AH
igh
tube
rcul
osis
burd
enNa
tiona
l gui
delin
es fo
r the
man
agem
ent o
f tub
ercu
losis
in ch
ildre
n. D
haka
: Nat
iona
l Tub
ercu
losis
Con
trol
Prog
ram
me,
Min
istry
of H
ealth
and
Fam
ily W
elfa
re; 2
012.
Nat
iona
l gui
delin
es o
f ant
iretro
vira
l the
rapy
, Ba
ngla
desh
. Dha
ka: N
atio
nal A
IDS/
STD
Pro
gram
me,
Dire
ctor
ate
Gen
eral
Hea
lth S
ervi
ces,
Min
istry
of H
ealth
an
d Fa
mily
Wel
fare
; 201
1.
Bots
wan
aAF
RH
igh
HIV
-ass
ocia
ted
tube
rcul
osis
burd
en
Bots
wan
a na
tiona
l HIV
and
AID
S tre
atm
ent g
uide
lines
. Gab
oron
e: M
inist
ry o
f Hea
lth; 2
012.
Tube
rcul
osis/
HIV
polic
y gui
delin
es. G
abor
one:
Min
istry
of H
ealth
; 201
1.Ca
mbo
dia
WPR
Hig
h tu
berc
ulos
is bu
rden
Na
tiona
l gui
delin
es fo
r dia
gnos
is an
d tre
atm
ent o
f tub
ercu
losis
in ch
ildre
n. P
hnom
Pen
h: N
atio
nal C
entre
for
Tube
rcul
osis
and
Lepr
osy
Cont
rol, M
inist
ry o
f Hea
lth; 2
008.
Sta
ndar
d op
erat
ing
proc
edur
es fo
r im
plem
entin
g th
e th
ree
I’s in
cont
inuu
m o
f car
e se
tting
s. Ph
nom
Pen
h: N
atio
nal C
entre
for H
IV/A
IDS
Der
mat
olog
y an
d ST
D
and
Nat
iona
l Cen
tre fo
r Tub
ercu
losis
and
Lep
rosy
Con
trol;
2010
. Ca
mer
oon
AFR
Hig
h H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
D
irect
ives
nat
iona
les d
e pr
even
tion
et d
e pr
ise e
n ch
arge
du
VIH
au C
amer
oun.
Yaou
ndé:
Min
istèr
e de
la
Sant
é; 2
015.
Gui
de te
chni
que
pour
les p
erso
nnel
s de
Sant
é. Ya
ound
é: P
rogr
amm
e N
atio
nal d
e Lu
tte c
ontre
la
Tube
rcul
ose,
Min
istèr
e de
la S
anté
; 201
2.
Cent
ral A
frica
n Re
publ
icAF
RH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enGu
ide
de p
rise
en ch
arge
de
la tu
berc
ulos
e de
l’adu
lte. B
angu
i: Pr
ogra
mm
e N
atio
nal d
e Lu
tte c
ontre
la
Tube
rcul
ose.
Min
istèr
e de
la S
anté
de
l’Hyg
iene
Pub
lique
et d
e la
Pop
ulat
ion;
201
6. G
uide
de
prise
en
char
ge
de la
tube
rcul
ose
de l’e
nfan
t. Ba
ngui
: Pro
gram
me
Nat
iona
l de
Lutte
Con
tre la
Min
istèr
e de
la S
anté
de
l’Hyg
iene
Pub
lique
et d
e la
Pop
ulat
ion;
201
6.
Dem
ocra
tic R
epub
lic o
f the
Co
ngo
AFR
Hig
h tu
berc
ulos
is an
d H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
Guid
e na
tiona
l de
prise
en
char
ge d
e l’in
fect
ion
a VI
H en
RD
C. K
insh
asa:
Pro
gram
me
Nat
iona
l de
Lutte
Con
tre
le V
IH/S
IDA
et le
s IST
s PN
LS; 2
013.
Gui
de d
e pr
ise e
n ch
arge
de
la co
-infe
ctio
n VI
H-tu
berc
ulos
e da
ns la
zone
de
sant
é. K
insh
asa:
Min
istèr
e de
la S
anté
Pub
lic; 2
012.
Et
hiop
iaAF
RH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enGu
idel
ines
for c
linica
l pro
gram
mat
ic m
anag
emen
t of t
uber
culo
sis, t
uber
culo
sis/H
IV a
nd le
pros
y in
Ethi
opia
. M
inist
ry o
f Hea
lth; 2
013.
Nat
iona
l gui
delin
es fo
r com
preh
ensiv
e HI
V pr
even
tion,
care
and
trea
tmen
t. Ad
dis
Abab
a: M
inist
ry o
f Hea
lth; 2
014.
Nat
iona
l chi
ldho
od tu
berc
ulos
is im
plem
enta
tion
guid
e. Ad
dis A
baba
: M
inist
ry o
f Hea
lth; 2
015.
Gh
ana
AFR
Hig
h H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
Gu
idel
ines
for d
iagn
osis
and
man
agem
ent o
f tub
ercu
losis
in ch
ildre
n. A
ccra
: Gha
na H
ealth
Ser
vice
; 201
2.
Guid
elin
es fo
r the
clin
ical m
anag
emen
t of t
uber
culo
sis a
nd H
IV co
-infe
ctio
n. A
ccra
: Gha
na H
ealth
Ser
vice
; 200
7.
Guid
elin
es fo
r ant
iretro
vira
l the
rapy
in G
hana
. Acc
ra: N
atio
nal H
IV/A
IDS/
STI C
ontro
l Pro
gram
me,
Min
istry
of
Hea
lth a
nd G
hana
Hea
lth S
ervi
ce; 2
008.
Indi
aSE
AH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enNa
tiona
l gui
delin
es o
n di
agno
sis a
nd tr
eatm
ent o
f pae
diat
ric tu
berc
ulos
is. N
ew D
elhi
: Cen
tral T
uber
culo
sis
Div
ision
, Dire
ctor
ate
Gen
eral
of H
ealth
Ser
vice
s, M
inist
ry o
f Hea
lth a
nd F
amily
Wel
fare
; 201
2. D
OTS-
plus
gu
idel
ines
. New
Del
hi: R
evise
d N
atio
nal T
uber
culo
sis C
ontro
l Pro
gram
me;
201
0.
Stan
dard
s for
tube
rcul
osis
care
in In
dia.
New
Del
hi: C
entra
l Tub
ercu
losis
Div
ision
, Dire
ctor
ate
Gen
eral
of
Hea
lth S
ervi
ces,
Min
istry
of H
ealth
and
Fam
ily W
elfa
re; 2
014.
In
done
siaSE
AH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enNa
tiona
l pol
icy o
n tu
berc
ulos
is/HI
V co
llabo
ratio
n [tr
ansla
ted]
. Jak
arta
: Min
istry
of H
ealth
; 201
5. Te
chni
cal
guid
elin
es o
n m
anag
emen
t of t
uber
culo
sis in
child
ren
[tran
slate
d]. J
akar
ta: M
inist
ry o
f Hea
lth; 2
013.
(con
tinue
s. . .
)

Ann Jagger et al.National policies on latent tuberculosisResearch
184B Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414
Co
untr
y or t
errit
ory
WHO
regi
onCo
untr
y gro
upDa
ta so
urce
Keny
aAF
RH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enNa
tiona
l ison
iazid
pre
vent
ativ
e th
erap
y sta
ndar
d op
erat
ing
proc
edur
e. N
airo
bi: M
inist
ry o
f Hea
lth; 2
015.
Gu
idel
ines
for m
anag
emen
t of t
uber
culo
sis a
nd le
pros
y in
Keny
a. N
airo
bi: M
inist
ry o
f Hea
lth; 2
013.
Leso
tho
AFR
Hig
h tu
berc
ulos
is an
d H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
Natio
nal g
uide
lines
for t
he th
ree
I’s (i
soni
azid
pre
vent
ive
ther
apy (
IPT)
inte
nsifi
ed ca
se fi
ndin
g (IC
F) a
nd in
fect
ion
cont
rol (
IC).
Mas
eru:
Gov
ernm
ent o
f Les
otho
; 201
1. N
atio
nal t
uber
culo
sis p
rogr
amm
e po
licy a
nd m
anua
l. M
aser
u: G
over
nmen
t of L
esot
ho; 2
007.
Mal
awi
AFR
Hig
h H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
Na
tiona
l tub
ercu
losis
cont
rol p
rogr
amm
e m
anua
l. Li
long
we:
Min
istry
of H
ealth
; 201
2. C
linica
l man
agem
ent o
f HI
V in
child
ren
and
adul
ts. L
ilong
we:
Min
istry
of H
ealth
; 201
4.M
ozam
biqu
eAF
RH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enGu
ia d
e tra
tam
ento
ant
iretro
vira
l e in
fecç
ões o
port
unist
as n
o ad
ulto
, ado
lesc
ente
grá
vida
e cr
ianç
a. M
aput
o:
Min
istro
da
Saúd
e; 2
014.
Mya
nmar
SEA
Hig
h tu
berc
ulos
is an
d H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
Guid
elin
es fo
r the
pro
gram
mat
ic m
anag
emen
t of t
uber
culo
sis/H
IV in
Mya
nmar
. Nay
pyid
aw: N
atio
nal
Tube
rcul
osis
Prog
ram
me
and
Nat
iona
l AID
S Pr
ogra
mm
e; 2
015.
Nam
ibia
AFR
Hig
h tu
berc
ulos
is an
d H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
Natio
nal g
uide
lines
for t
he m
anag
emen
t of t
uber
culo
sis. W
indh
oek:
Min
istry
of H
ealth
and
Soc
ial S
ervi
ces;
2011
. Nat
iona
l gui
delin
es fo
r HIV
pre
vent
ion
treat
men
t and
care
. Win
dhoe
k: M
inist
ry o
f Hea
lth a
nd S
ocia
l Se
rvic
es; 2
014.
Nig
eria
AFR
Hig
h tu
berc
ulos
is an
d H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
Natio
nal t
uber
culo
sis a
nd le
pros
y con
trol p
rogr
amm
e –
wor
ker’s
man
ual.
Abuj
a: D
epar
tmen
t of P
ublic
Hea
lth,
Fede
ral M
inist
ry o
f Hea
lth; 2
010.
Paki
stan
EMR
Hig
h tu
berc
ulos
is bu
rden
Na
tiona
l gui
delin
es fo
r the
cont
rol o
f tub
ercu
losis
in P
akist
an. I
slam
abad
: Nat
iona
l TB
Cont
rol P
rogr
amm
e,
Min
istry
of N
atio
nal H
ealth
Ser
vice
s, Re
gula
tion
and
Coor
dina
tion;
201
5.
Papu
a N
ew G
uine
aW
PRH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enNa
tiona
l tub
ercu
losis
man
agem
ent p
roto
col.
Port
Mor
esby
: Dep
artm
ent o
f Hea
lth, D
iseas
e Co
ntro
l Bra
nch,
N
atio
nal T
uber
culo
sis P
rogr
amm
e; 2
011.
Gui
delin
es fo
r HIV
care
and
trea
tmen
t in
Papu
a Ne
w G
uine
a. P
ort
Mor
esby
: Dep
artm
ent o
f Hea
lth; 2
009.
Ph
ilipp
ines
WPR
Hig
h tu
berc
ulos
is bu
rden
Na
tiona
l tub
ercu
losis
cont
rol p
rogr
amm
e: m
anua
l of p
roce
dure
s, 5t
h ed
ition
. Man
ila: D
epar
tmen
t of H
ealth
; 20
14.
Sier
ra L
eone
AFR
Hig
h tu
berc
ulos
is bu
rden
Tu
berc
ulos
is tre
atm
ent g
uide
lines
[dra
ft]. F
reet
own:
Min
istry
of H
ealth
and
San
itatio
n; 2
016.
Na
tiona
l ant
iretro
vira
l tre
atm
ent g
uide
lines
. Fre
etow
n: M
inist
ry o
f Hea
lth a
nd S
anita
tion;
201
5.So
uth
Afric
aAF
RH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enGu
idel
ines
for t
he m
anag
emen
t of t
uber
culo
sis in
child
ren.
Pre
toria
: Dep
artm
ent o
f Hea
lth, 2
013.
Na
tiona
l tub
ercu
losis
man
agem
ent g
uide
lines
. Pre
toria
: Dep
artm
ent o
f Hea
lth; 2
014.
Gu
idel
ines
for t
uber
culo
sis p
reve
ntiv
e th
erap
y am
ong
HIV
infe
cted
indi
vidu
als i
n So
uth
Afric
a. P
reto
ria:
Dep
artm
ent o
f Hea
lth; 2
010.
Na
tiona
l con
solid
ated
gui
delin
es fo
r the
pre
vent
ion
of m
othe
r-to-
child
tran
smiss
ion
of H
IV (P
MTC
T) a
nd th
e m
anag
emen
t of H
IV in
child
ren,
ado
lesc
ents
and
adu
lts. P
reto
ria: D
epar
tmen
t of H
ealth
; 201
4.Sw
azila
ndAF
RH
igh
HIV
-ass
ocia
ted
tube
rcul
osis
burd
en
Swaz
iland
inte
grat
ed H
IV m
anag
emen
t gui
delin
es. M
baba
ne: M
inist
ry o
f Hea
lth; 2
015.
Nat
iona
l pol
icy
guid
elin
es o
n TB
/HIV
colla
bora
tive
activ
ities
. Mba
bane
: Min
istry
of H
ealth
; 201
5.Th
aila
ndSE
AH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enCl
inica
l pra
ctice
s gui
delin
es o
f tub
ercu
losis
trea
tmen
t in
adul
ts. N
onth
abur
i: D
epar
tmen
t of T
uber
culo
sis,
Dep
artm
ent o
f Dise
ase
Cont
rol, M
inist
ry o
f Pub
lic H
ealth
; 201
3.
Uga
nda
AFR
Hig
h H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
M
inist
ry o
f hea
lth m
anua
l of t
he n
atio
nal t
uber
culo
sis a
nd le
pros
y pro
gram
me.
Kam
pala
: Min
istry
of H
ealth
; 20
10. T
he in
tegr
ated
nat
iona
l gui
delin
es o
n an
tiret
rovi
ral t
hera
py p
reve
ntio
n of
mot
her t
o ch
ild tr
ansm
issio
n of
HI
V in
fant
and
youn
g ch
ild fe
edin
g. K
ampa
la: M
inist
ry o
f Hea
lth; 2
012.
(. . .
cont
inue
d)
(con
tinue
s. . .
)

Ann Jagger et al. National policies on latent tuberculosisResearch
184CBull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414
Co
untr
y or t
errit
ory
WHO
regi
onCo
untr
y gro
upDa
ta so
urce
Uni
ted
Repu
blic
of T
anza
nia
AFR
Hig
h tu
berc
ulos
is an
d H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
Natio
nal g
uide
lines
for t
he m
anag
emen
t of t
uber
culo
sis in
child
ren.
Dar
es S
alaa
m: M
inist
ry o
f Hea
lth a
nd S
ocia
l W
elfa
re; 2
013.
M
anua
l for
the
man
agem
ent o
f tub
ercu
losis
and
lepr
osy.
Dar
es S
alaa
m: M
inist
ry o
f Hea
lth a
nd S
ocia
l Wel
fare
; 20
13. N
atio
nal p
olic
y gui
delin
es fo
r col
labo
rativ
e TB
/HIV
act
iviti
es. D
ar e
s Sal
aam
: Min
istry
of H
ealth
and
Soc
ial
Wel
fare
; 200
8. N
atio
nal g
uide
lines
for t
he m
anag
emen
t of H
IV a
nd A
IDS.
Dar
es S
alaa
m: M
inist
ry o
f Hea
lth a
nd
Soci
al W
elfa
re; 2
012.
Viet
Nam
WPR
Hig
h tu
berc
ulos
is bu
rden
D
iagn
osis,
trea
tmen
t, an
d pr
even
tion
of tu
berc
ulos
is [tr
ansla
ted]
. Han
oi: M
inist
ry o
f Hea
lth; 2
015.
Gui
delin
es
for H
IV/A
IDS
diag
nosis
and
trea
tmen
t. H
anoi
: Min
istry
of H
ealth
; 201
4. C
olla
bora
tive
prot
ocol
for T
B/HI
V di
agno
sis, t
reat
men
t and
case
man
agem
ent.
Han
oi: M
inist
ry o
f Hea
lth; 2
007.
Zam
bia
AFR
Hig
h tu
berc
ulos
is an
d H
IV-a
ssoc
iate
d tu
berc
ulos
is bu
rden
Natio
nal g
uide
lines
on
man
agem
ent o
f tub
ercu
losis
in ch
ildre
n. L
usak
a: M
inist
ry o
f Hea
lth, D
ivisi
on o
f Le
pros
y, Tu
berc
ulos
is an
d Lu
ng D
iseas
e; 2
013.
Zam
bia
cons
olid
ated
gui
delin
es fo
r tre
atm
ent a
nd p
reve
ntio
n of
HIV
infe
ctio
n. L
usak
a: M
inist
ry o
f Hea
lth a
nd M
inist
ry o
f Com
mun
ity D
evel
opm
ent,
Mot
her a
nd C
hild
H
ealth
; 201
4.
Zim
babw
eAF
RH
igh
tube
rcul
osis
and
HIV
-ass
ocia
ted
tube
rcul
osis
burd
enNa
tiona
l TB
guid
elin
es, 4
th e
ditio
n. H
arar
e: N
atio
nal T
uber
culo
sis C
ontro
l Pro
gram
me,
Min
istry
of H
ealth
an
d Ch
ild W
elfa
re; 2
010.
Nat
iona
l gui
delin
es fo
r TB/
HIV
co-m
anag
emen
t. H
arar
e: N
atio
nal H
IV/A
IDS
and
Tube
rcul
osis
Cont
rol P
rogr
amm
es. M
inist
ry o
f Hea
lth a
nd C
hild
Wel
fare
; 201
4.Lo
w-t
uber
culo
sis
burd
en
coun
trie
sAl
geria
AFR
Low
-tub
ercu
losis
bur
den
Mea
sure
de
prev
entio
n po
ur le
s suj
ets c
onta
ct. C
hapi
tre V
I. In
: La
prev
entio
n de
la tu
berc
ulos
e. Al
ger:
Min
istèr
e de
la S
anté
, de
la P
opul
atio
n et
de
la R
éfor
me
Hos
pita
lière
; 201
1Am
eric
an S
amoa
WPR
Low
-tub
ercu
losis
bur
den
Late
nt tu
berc
ulos
is in
fect
ion:
a g
uide
for p
rimar
y car
e pr
ovid
ers.
Atla
nta:
Uni
ted
Stat
es C
ente
rs fo
r Dise
ase
Cont
rol a
nd P
reve
ntio
n; 2
013.
An
tigua
and
Bar
buda
AMR
Low
tube
rcul
osis
burd
enCa
ribbe
an g
uide
lines
for t
he p
reve
ntio
n, tr
eatm
ent,
care
and
cont
rol o
f tub
ercu
losis
and
HIV
/TB.
Was
hing
ton:
Ca
ribbe
an H
IV/A
IDS
Regi
onal
Trai
ning
Net
wor
k; 2
010.
Ar
gent
ina
AMR
Low
tube
rcul
osis
burd
enPr
ogra
ma
naci
onal
de
cont
rol d
e la
tube
rcul
osis.
Nor
mas
técn
icas.
Buen
os A
ires:
Min
ister
io d
e Sa
lud
de la
N
ació
n; 2
013.
Arub
aAM
RLo
w tu
berc
ulos
is bu
rden
Carib
bean
gui
delin
es fo
r the
pre
vent
ion,
trea
tmen
t, ca
re a
nd co
ntro
l of t
uber
culo
sis a
nd H
IV/t
uber
culo
sis.
Was
hing
ton:
Car
ibbe
an H
IV/A
IDS
Regi
onal
Trai
ning
Net
wor
k; 2
010.
Au
stra
liaW
PRLo
w tu
berc
ulos
is bu
rden
CDNA
nat
iona
l gui
delin
es fo
r the
pub
lic h
ealth
man
agem
ent o
f tub
ercu
losis
. Can
berra
: Dep
artm
ent o
f Hea
lth;
2013
.Au
stria
EUR
Low
tube
rcul
osis
burd
enÖ
ster
reic
hisc
he le
itlin
ie zu
rtub
erku
lose
– u
mge
bung
sunt
ersu
chun
g. V
ienn
a: B
unde
smin
ister
ium
für
Ges
undh
eit;
2013
.Ba
ham
asAM
RLo
w tu
berc
ulos
is bu
rden
Tube
rcul
osis
cont
rol [
Inte
rnet
]. N
assa
u: M
inist
ry o
f Hea
lth; 2
011.
Barb
ados
AMR
Low
tube
rcul
osis
burd
enCa
ribbe
an g
uide
lines
for t
he p
reve
ntio
n, tr
eatm
ent,
care
and
cont
rol o
f tub
ercu
losis
and
HIV
/TB.
Was
hing
ton:
Ca
ribbe
an H
IV/A
IDS
Regi
onal
Trai
ning
Net
wor
k; 2
010.
Be
lgiu
mEU
RLo
w tu
berc
ulos
is bu
rden
Reco
mm
enda
tions
conc
erna
nt le
dep
istag
e ci
ble
et le
trai
tem
ent d
e l’in
fect
ion
tube
rcul
euse
late
nte.
Brus
sels:
Fo
ndat
ion
Cont
re L
es A
ffect
ions
Res
pira
toire
s et P
our L
’Edu
catio
n a
La S
ante
; 200
3.Be
lize
AMR
Low
tube
rcul
osis
burd
enCa
ribbe
an g
uide
lines
for t
he p
reve
ntio
n, tr
eatm
ent,
care
and
cont
rol o
f tub
ercu
losis
and
HIV
/TB.
Was
hing
ton:
Ca
ribbe
an H
IV/A
IDS
Regi
onal
Trai
ning
Net
wor
k; 2
010.
Be
rmud
aAM
RLo
w tu
berc
ulos
is bu
rden
Carib
bean
gui
delin
es fo
r the
pre
vent
ion,
trea
tmen
t, ca
re a
nd co
ntro
l of t
uber
culo
sis a
nd H
IV/T
B. W
ashi
ngto
n:
Carib
bean
HIV
/AID
S Re
gion
al Tr
aini
ng N
etw
ork;
201
0.
(. . .
cont
inue
d)
(con
tinue
s. . .
)

Ann Jagger et al.National policies on latent tuberculosisResearch
184D Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414
Co
untr
y or t
errit
ory
WHO
regi
onCo
untr
y gro
upDa
ta so
urce
Braz
ilAM
RLo
w tu
berc
ulos
is bu
rden
Man
ual d
e re
com
enda
coes
par
a o
cont
role
da
tube
rcul
ose
no B
razil
. Bra
sília
: Min
ister
io d
a Sa
lude
; 201
1.Br
unei
Dar
ussa
lam
WPR
Low
tube
rcul
osis
burd
enGu
idel
ines
for t
uber
culo
sis co
ntro
l in B
rune
i Dar
ussa
lam
. Ban
dar S
eri B
egaw
an: M
inist
ry o
f Hea
lth; 2
013.
Ca
nada
AMR
Low
tube
rcul
osis
burd
enCa
nadi
an tu
berc
ulos
is st
anda
rds,
7th
editi
on. O
ttaw
a: P
ublic
Hea
lth A
genc
y of
Can
ada;
201
4.
Chile
AMR
Low
tube
rcul
osis
burd
enNo
rmas
tecn
icas p
ara
el co
ntro
l y la
elim
inac
ion
de la
tube
rcul
osis.
San
tiago
: Pro
gram
a N
acio
nal p
ara
el
Cont
rol y
la E
limin
acio
n de
la Tu
berc
ulos
is; 2
014.
Ch
ina,
Hon
g Ko
ng S
peci
al
Adm
inist
rativ
e Re
gion
WPR
Low
tube
rcul
osis
burd
enGu
idel
ines
on
targ
eted
tube
rcul
in te
stin
g an
d tre
atm
ent o
f lat
ent t
uber
culo
sis in
fect
ion.
Hon
g Ko
ng:
Tube
rcul
osis
and
Ches
t Ser
vice
; 201
5 (la
st u
pdat
e on
31
Mar
ch 2
015)
. Co
lom
bia
AMR
Low
tube
rcul
osis
burd
enGu
ías d
e pr
omoc
ión
de la
salu
d y p
reve
nció
n de
enf
erm
edad
es e
n la
salu
d pú
blica
. Guí
a II:
Guí
a de
ate
nció
n de
la tu
berc
ulos
is pu
lmon
ar y
extra
pulm
onar
. Bog
otá:
Pro
gram
a de
Apo
yo a
la R
efor
ma
de S
alud
/PAR
S,
Min
ister
io d
e la
Pro
tecc
ión
Soci
al; 2
005.
Co
sta
Rica
AMR
Low
tube
rcul
osis
burd
enM
anua
l de
norm
as d
e at
enci
on y
vigi
lanc
ia p
ara
el co
ntro
l de
la tu
berc
ulos
is. S
an Jo
sé: P
rogr
ama
Nac
iona
l pa
ra e
l Con
trol d
e la
Tube
rcul
osis;
200
3.Cy
prus
EUR
Low
tube
rcul
osis
burd
enPr
olyp
si tis
met
ados
is fy
mat
iosis
se xo
rous
par
oxhs
yper
esio
n yg
eias
. [Pr
even
tion
of th
e tra
nsm
issio
n of
tu
berc
ulos
is to
hea
lth-c
are
faci
litie
s.] N
icos
ia: M
inist
ry o
f Hea
lth; 2
015.
Cz
echi
aEU
RLo
w tu
berc
ulos
is bu
rden
Vyhl
áška
473
/200
8 Sb
: Min
ister
stva
zdra
votn
ictv
í ze
dne
17 p
rosin
ce 2
008
o sy
stém
u ep
idem
iolo
gick
é bd
ělos
ti pr
o vy
bran
é in
fekc
e. [D
ecla
ratio
n 47
3/20
08 S
b by
the
Min
istry
of H
ealth
of 1
7 D
ecem
ber 2
008
on a
n ep
idem
iolo
gica
l ale
rt sy
stem
for s
elec
ted
infe
ctio
ns.]
Prag
ue: M
inist
ry o
f Hea
lth; 2
008.
D
omin
ican
Rep
ublic
AMR
Low
tube
rcul
osis
burd
enRe
glam
ento
tecn
ico p
ara
la p
reve
ncio
n y e
l con
trol d
e la
tube
rcul
osis.
San
to D
omin
go: M
inist
erio
de
Salu
d Pu
blic
a; 2
014.
Nor
mas
nac
iona
les p
ara
el co
ntro
l de
la tu
berc
ulos
is en
Rep
ublic
a D
omin
icana
. Ser
ie d
e no
rmas
na
cion
ales
no.
16.
San
to D
omin
go D
.N.: E
cret
aria
de
Esta
do d
e Sa
lud
Publ
ica
y As
isten
cia
Soci
al, P
rogr
ama
Nac
iona
l de
Cont
rol d
e la
Tube
rcul
osis;
200
3.Ec
uado
rAM
RLo
w tu
berc
ulos
is bu
rden
Man
ual d
e no
rmas
y pr
oced
imie
ntos
par
a el
cont
rol d
e la
tube
rcul
osis
en E
cuad
or. Q
uito
: Min
ister
io d
e Sa
lud
Publ
ica;
201
0.Fi
jiW
PRLo
w tu
berc
ulos
is bu
rden
Tube
rcul
osis
guid
elin
e. Su
va: N
atio
nal T
uber
culo
sis P
rogr
amm
e; 2
011.
Finl
and
EUR
Low
tube
rcul
osis
burd
enSu
ositu
s tub
erku
loos
in ko
ntak
tisel
vity
ksen
tote
utta
mise
ksi.
Hel
sinki
: Ter
veyd
en ja
hyv
invo
inni
n la
itos;
2011
. Fr
ance
EUR
Low
tube
rcul
osis
burd
enAv
is du
cons
eil s
uper
ieur
d’h
ygie
ne p
ubliq
ue d
e Fr
ance
sect
ion
mal
adie
s tra
nsm
issib
les.
Rela
tif a
u tra
itmen
t de
la tu
berc
ulos
e-in
fect
ion.
Par
is: D
irect
ion
Gen
eral
de
la S
anté
. Min
istèr
e de
la S
anté
, de
la F
amill
e et
des
Pe
rson
nes h
andi
capé
es; 2
003.
Fr
ench
Pol
ynes
iaW
PRLo
w tu
berc
ulos
is bu
rden
Guid
e pr
atiq
ue a
l’int
entio
n de
pro
fess
ione
ls de
sant
é. Pa
peet
e: D
irect
ion
de la
San
té, D
épar
tem
ent d
es
Prog
ram
mes
de
Prév
entio
n, P
rogr
amm
e Co
ntre
la Tu
berc
ulos
e; 2
011.
G
erm
any
EUR
Low
tube
rcul
osis
burd
enNe
w re
com
men
datio
ns fo
r con
tact
trac
ing
in tu
berc
ulos
is. S
tuttg
art:
Ger
man
Cen
tral C
omm
ittee
aga
inst
Tu
berc
ulos
is; 2
011.
Gree
ceEU
RLo
w tu
berc
ulos
is bu
rden
Fym
atio
si: a
po ti
dia
gnos
i sti
ther
apia
. [Tu
berc
ulos
is: fr
om d
iagn
osis
to th
erap
ies.]
Ath
ens:
Ellin
iki P
neum
olog
iki
Etai
ria; 2
012.
Gren
ada
AMR
Low
tube
rcul
osis
burd
enCa
ribbe
an g
uide
lines
for t
he p
reve
ntio
n, tr
eatm
ent,
care
and
cont
rol o
f tub
ercu
losis
and
HIV
/tub
ercu
losis
. W
ashi
ngto
n: C
arib
bean
HIV
/AID
S Re
gion
al Tr
aini
ng N
etw
ork;
201
0.
Irela
ndEU
RLo
w tu
berc
ulos
is bu
rden
Guid
elin
es o
n th
e pr
even
tion
and
cont
rol o
f tub
ercu
losis
in Ir
elan
d. D
ublin
: Hea
lth P
rote
ctio
n an
d Su
rvei
llanc
e Ce
ntre
; 201
0 [a
men
ded
2014
]. Isr
ael
EUR
Low
tube
rcul
osis
burd
enD.
Che
mto
b, A
. Lev
enth
al,Y.
Ber
low
itz,D
. Wei
ler-
Rave
ll. Th
e ne
w n
atio
nal t
uber
culo
sis c
ontro
l pro
gram
me
in
Israe
l, a c
ount
ry o
f hig
h im
mig
ratio
n. In
t J Tu
berc
Lung
Dis.
200
3 Se
p;7(
9):8
28–3
6. P
MID
:129
7166
5
(. . .
cont
inue
d)
(con
tinue
s. . .
)

Ann Jagger et al. National policies on latent tuberculosisResearch
184EBull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414
Co
untr
y or t
errit
ory
WHO
regi
onCo
untr
y gro
upDa
ta so
urce
Jam
aica
AMR
Low
tube
rcul
osis
burd
enCa
ribbe
an g
uide
lines
for t
he p
reve
ntio
n, tr
eatm
ent,
care
and
cont
rol o
f tub
ercu
losis
and
HIV
/tub
ercu
losis
. W
ashi
ngto
n: C
arib
bean
HIV
/AID
S Re
gion
al Tr
aini
ng N
etw
ork;
201
0.
Japa
nW
PRLo
w tu
berc
ulos
is bu
rden
Trea
tmen
t gui
delin
es fo
r lat
ent t
uber
culo
sis in
fect
ion.
Toky
o: P
reve
ntio
n Co
mm
ittee
and
the
Trea
tmen
t Co
mm
ittee
of t
he Ja
pane
se S
ocie
ty fo
r Tub
ercu
losis
; 201
3.
Mal
aysia
WPR
Low
tube
rcul
osis
burd
enM
anag
emen
t of t
uber
culo
sis, 3
rd e
ditio
n. P
utra
jaya
: Mal
aysia
Hea
lth Te
chno
logy
Ass
essm
ent S
ectio
n; 2
012.
M
alta
EUR
Low
tube
rcul
osis
burd
enPr
even
tion,
cont
rol a
nd m
anag
emen
t of t
uber
culo
sis: a
nat
iona
l stra
tegy
for M
alta
. Msid
a: In
fect
ious
Dise
ase
Prev
entio
n an
d Co
ntro
l Uni
t, M
inist
ry o
f Hea
lth; 2
012.
M
exic
oAM
RLo
w tu
berc
ulos
is bu
rden
Norm
a ofi
cial
Mex
icana
NO
M-0
06-S
SA2–
2013
, par
a la
pre
venc
ión
y con
trol d
e la
tube
rcul
osis.
Mex
ico
City
: Se
cret
aría
de
Salu
d; 2
013.
N
ethe
rland
sEU
RLo
w tu
berc
ulos
is bu
rden
Rich
tlijn
beh
ande
ling
late
nte
tube
rcul
ose-
infe
ctie
. The
Hag
ue: K
NCV
Tube
rcul
osis
Foun
datio
n; 2
015.
N
ew Z
eala
ndW
PRLo
w tu
berc
ulos
is bu
rden
Guid
elin
es fo
r tub
ercu
losis
cont
rol in
New
Zea
land
201
0. C
hapt
er 8
. Wel
lingt
on: M
inist
ry o
f Hea
lth; 2
010.
N
orw
ayEU
RLo
w tu
berc
ulos
is bu
rden
Tube
rkul
osev
eile
dere
n: 1
0. Fo
reby
ggen
de b
ehan
dlin
g av
late
nt tu
berk
ulos
e (L
TB).
Oslo
: Fol
kehe
lsein
stitu
ttet;
2010
. O
man
EMR
Low
tube
rcul
osis
burd
enST
OP
tube
rcul
osis.
Man
ual o
f tub
ercu
losis
cont
rol p
rogr
amm
e, 4t
h ed
ition
, Apr
il 200
7. M
usca
t: N
atio
nal
Tube
rcul
osis
Cont
rol P
rogr
amm
e D
epar
tmen
t of C
omm
unic
able
Dise
ase
Surv
eilla
nce
and
Cont
rol,
Dire
ctor
ate
Gen
eral
of H
ealth
Affa
irs, M
inist
ry o
f Hea
lth; 2
007.
Pa
lau
WPR
Low
tube
rcul
osis
burd
enLa
tent
tube
rcul
osis
infe
ctio
n: a
gui
de fo
r prim
ary c
are
prov
ider
s. At
lant
a: U
nite
d St
ates
Cen
ters
for D
iseas
e Co
ntro
l and
Pre
vent
ion;
201
3.Pa
nam
aAM
RLo
w tu
berc
ulos
is bu
rden
Norm
a na
cion
al p
ara
la p
reve
ncio
n y c
ontro
l de
la tu
berc
ulos
is. P
anam
a Ci
ty: M
inist
erio
de
Salu
d; ;
2015
.Po
land
EUR
Low
tube
rcul
osis
burd
enTu
berc
ulos
is m
anua
l: nat
iona
l tub
ercu
losis
pro
gram
me
guid
elin
es. W
arsa
w: N
atio
nal T
uber
culo
sis a
nd L
ung
Dise
ases
Res
earc
h In
stitu
te; 2
001.
Port
ugal
EUR
Low
tube
rcul
osis
burd
enTr
atam
ento
da
tube
rcul
ose
late
nte
revi
são
das n
orm
as. L
isbon
: Soc
ieda
de P
ortu
gues
a de
Pne
umol
ogia
; 201
4.Pu
erto
Ric
oAM
RLo
w tu
berc
ulos
is bu
rden
Late
nt tu
berc
ulos
is in
fect
ion:
a g
uide
for p
rimar
y car
e pr
ovid
ers.
Atla
nta:
Uni
ted
Stat
es C
ente
rs fo
r Dise
ase
Cont
rol a
nd P
reve
ntio
n; 2
013.
Sain
t Kitt
s and
Nev
isAM
RLo
w tu
berc
ulos
is bu
rden
Carib
bean
gui
delin
es fo
r the
pre
vent
ion,
trea
tmen
t, ca
re a
nd co
ntro
l of t
uber
culo
sis a
nd H
IV/t
uber
culo
sis.
Was
hing
ton:
Car
ibbe
an H
IV/A
IDS
Regi
onal
Trai
ning
Net
wor
k; 2
010.
Sa
int L
ucia
AMR
Low
tube
rcul
osis
burd
enCa
ribbe
an g
uide
lines
for t
he p
reve
ntio
n, tr
eatm
ent,
care
and
cont
rol o
f tub
ercu
losis
and
HIV
/tub
ercu
losis
. W
ashi
ngto
n: C
arib
bean
HIV
/AID
S Re
gion
al Tr
aini
ng N
etw
ork;
201
0.
Sain
t Vin
cent
and
the
Gren
adin
esAM
RLo
w tu
berc
ulos
is bu
rden
Carib
bean
gui
delin
es fo
r the
pre
vent
ion,
trea
tmen
t, ca
re a
nd co
ntro
l of t
uber
culo
sis a
nd H
IV/t
uber
culo
sis.
Was
hing
ton:
Car
ibbe
an H
IV/A
IDS
Regi
onal
Trai
ning
Net
wor
k; 2
010.
Sa
udi A
rabi
aEM
RLo
w tu
berc
ulos
is bu
rden
Saud
i gui
delin
es fo
r tes
ting
and
treat
men
t of l
aten
t tub
ercu
losis
infe
ctio
n. 2
010.
Join
t sta
tem
ent o
f the
Sa
udi T
hora
cic
Soci
ety,
the
Saud
i Soc
iety
of M
edic
al M
icro
biol
ogy
and
Infe
ctio
us D
iseas
es, t
he S
audi
As
soci
atio
n of
Pub
lic H
ealth
, and
the
Soci
ety
of F
amily
and
Com
mun
ity M
edic
ine.
Ann
Sau
di M
ed. 2
010
Jan-
Feb;
30(
1): 3
8–49
.Se
rbia
EUR
Low
tube
rcul
osis
burd
enGu
idel
ines
for e
xam
inin
g pe
rson
s in
cont
act w
ith tu
berc
ulos
is, la
tent
tube
rcul
osis
and
chem
opro
phyl
axis.
Pro
ject
“tu
berc
ulos
is co
ntro
l in S
erbi
a” [t
rans
late
d tit
le].
Belg
rade
: Min
istry
of H
ealth
; 201
1.
Seyc
helle
sAF
RLo
w tu
berc
ulos
is bu
rden
Natio
nal t
uber
culo
sis p
rogr
amm
e: cl
inica
l dia
gnos
is an
d m
anag
emen
t of t
uber
culo
sis, a
nd m
easu
res f
or it
s pr
even
tion
and
cont
rol.
Mon
t Fle
uri:
Com
mun
icab
le D
iseas
e Co
ntro
l Uni
t Sey
chel
les H
ospi
tal;
2013
. Si
ngap
ore
WPR
Low
tube
rcul
osis
burd
enA
guid
e on
infe
ctio
us d
iseas
es o
f pub
lic h
ealth
impo
rtan
ce in
Sin
gapo
re. S
inga
pore
: Min
istry
of H
ealth
; 201
1.
(. . .
cont
inue
d)
(con
tinue
s. . .
)

Ann Jagger et al.National policies on latent tuberculosisResearch
184F Bull World Health Organ 2018;96:173–184F| doi: http://dx.doi.org/10.2471/BLT.17.199414
Co
untr
y or t
errit
ory
WHO
regi
onCo
untr
y gro
upDa
ta so
urce
Sint
Maa
rten
(Dut
ch p
art)
AMR
Low
tube
rcul
osis
burd
enCa
ribbe
an g
uide
lines
for t
he p
reve
ntio
n, tr
eatm
ent,
care
and
cont
rol o
f tub
ercu
losis
and
HIV
/tub
ercu
losis
. W
ashi
ngto
n: C
arib
bean
HIV
/AID
S Re
gion
al Tr
aini
ng N
etw
ork;
201
0.
Spai
nEU
RLo
w tu
berc
ulos
is bu
rden
Guia
de
prac
tica
clin
ica so
bre
el d
iagn
ostic
o, e
l tra
tam
ient
o y l
a pr
even
cion
de
la tu
berc
ulos
is. G
uias
de
prac
tica
clin
ical e
n el
SNS
. Mad
rid: M
inist
erio
de
Sani
dad,
Pol
ica
Soci
al e
Igua
lidad
; 201
0.
Surin
ame
AMR
Low
tube
rcul
osis
burd
enCa
ribbe
an g
uide
lines
for t
he p
reve
ntio
n, tr
eatm
ent,
care
and
cont
rol o
f tub
ercu
losis
and
HIV
/tub
ercu
losis
. W
ashi
ngto
n: C
arib
bean
HIV
/AID
S Re
gion
al Tr
aini
ng N
etw
ork;
201
0.
Swed
enEU
RLo
w tu
berc
ulos
is bu
rden
Reko
mm
enda
tione
r för
pre
vent
iva
insa
tser
mot
tube
rkul
os: h
älso
kont
roll,
smitt
spår
ning
och
vacc
inat
ion.
St
ockh
olm
: Soc
ialst
yrel
sen;
201
2.Sw
itzer
land
EUR
Low
tube
rcul
osis
burd
enTu
berc
ulos
is in
Sw
itzer
land
. Ber
n: S
wiss
Fe
dera
l Offi
ce o
f Pub
lic H
ealth
; 201
2.Th
e fo
rmer
Yug
osla
v Re
publ
ic
of M
aced
onia
EUR
Low
tube
rcul
osis
burd
enD
iagn
osis
and
treat
men
t of l
aten
t tub
ercu
losis
infe
ctio
n. S
kopj
e: PH
I Ins
titut
e fo
r Lun
g D
iseas
e an
d Tu
berc
ulos
is; 2
009.
Tr
inid
ad a
nd To
bago
AMR
Low
tube
rcul
osis
burd
enCa
ribbe
an g
uide
lines
for t
he p
reve
ntio
n, tr
eatm
ent,
care
and
cont
rol o
f tub
ercu
losis
and
HIV
/tub
ercu
losis
. W
ashi
ngto
n: C
arib
bean
HIV
/AID
S Re
gion
al Tr
aini
ng N
etw
ork;
201
0.
Tuni
siaEM
RLo
w tu
berc
ulos
is bu
rden
Guid
e de
pris
e en
char
ge d
e la
turb
ecul
ose
en Tu
nisie
. Tun
is: D
irect
ion
des S
oins
de
Sant
é de
Bas
e, R
épub
lique
Tu
nisie
nne;
201
4;U
nite
d Ar
ab E
mira
tes
EMR
Low
tube
rcul
osis
burd
enM
anua
l of t
uber
culo
sis co
ntro
l. Ab
u D
habi
: Nat
iona
l Tub
ercu
losis
Con
trol P
rogr
amm
e; M
inist
ry o
f Hea
lth;
2010
. U
nite
d Ki
ngdo
mEU
RLo
w tu
berc
ulos
is bu
rden
Tube
rcul
osis.
NIC
E gu
idel
ines
[NG3
3]. L
ondo
n: N
atio
nal I
nstit
ute
for H
ealth
and
Car
e Ex
celle
nce;
201
6.
Briti
sh O
vers
eas T
errit
ory T
urks
an
d Ca
icos
Isla
nds
AMR
Low
tube
rcul
osis
burd
enCa
ribbe
an g
uide
lines
for t
he p
reve
ntio
n, tr
eatm
ent,
care
and
cont
rol o
f tub
ercu
losis
and
HIV
/tub
ercu
losis
. W
ashi
ngto
n: C
arib
bean
HIV
/AID
S Re
gion
al Tr
aini
ng N
etw
ork;
201
0.
Uni
ted
Stat
esAM
RLo
w tu
berc
ulos
is bu
rden
Late
nt tu
berc
ulos
is in
fect
ion:
a g
uide
for p
rimar
y car
e pr
ovid
ers.
Atla
nta:
Uni
ted
Stat
es C
ente
rs fo
r Dise
ase
Cont
rol a
nd P
reve
ntio
n; 2
013.
Uru
guay
AMR
Low
tube
rcul
osis
burd
enGu
ía N
acio
nal p
ara
el m
anej
o de
la Tu
berc
ulos
is. M
onte
vide
o: C
omisi
on H
onor
aria
par
a la
Luc
ha
Antit
uber
culo
sa y
Enf
erm
edad
es P
reva
lent
es; 2
016.
Uni
ted
Stat
es V
irgin
Isla
nds
AMR
Low
tube
rcul
osis
burd
enLa
tent
tube
rcul
osis
infe
ctio
n: a
gui
de fo
r prim
ary c
are
prov
ider
s. At
lant
a: U
nite
d St
ates
Cen
ters
for D
iseas
e Co
ntro
l and
Pre
vent
ion;
201
3.Ve
nezu
ela
(Bol
ivar
ian
Repu
blic
of
)AM
RLo
w tu
berc
ulos
is bu
rden
Dire
ctric
es p
ara
el d
espi
staj
e, di
agnó
stico
y tra
tam
ient
o de
la tu
berc
ulos
is en
pac
ient
es co
n in
dica
ción
de
tera
pias
bio
lógi
cas.
Cara
cas:
Min
ister
io d
el P
oder
Pop
ular
par
a la
Sal
ud, V
icem
inist
erio
de
Rede
s de
Salu
d Co
lect
iva
& D
irecc
ion
Gen
eral
de
Prog
ram
as d
e Sa
lud
Coor
dina
ción
Nac
iona
l de
Salu
d Re
spira
toria
; 201
0.
AFR:
Afri
can
Regi
on; A
IDS:
acq
uire
d im
mun
e de
ficie
ncy
synd
rom
e; A
MR:
Reg
ion
of th
e Am
eric
as; E
MR:
Eas
tern
Med
iterra
nean
Reg
ion;
EUR
: Eur
opea
n Re
gion
; HIV
: hum
an im
mun
odefi
cien
cy v
irus;
SEAR
: Sou
th-E
ast A
sia R
egio
n; TB
: tub
ercu
losis
; WHO
: W
orld
Hea
lth O
rgan
izatio
n; W
PR: W
este
rn P
acifi
c Re
gion
.
(. . .
cont
inue
d)