Embed Size (px)
Citation preview

NATIONAL NEWBORN CARE
KEY FINDINGS
AND
RECOMMENDATIONS
Child Priorities Meeting
December 2014
N R Rhoda
Neonatal Care Improvement Advisor, NDOH - RMCH (DFID)
This presentation is provided on the South African Child Health Priorities Website as presented at the 5th Child Health Priorities Conference except
that potential patient identifying content has been removed except where part of corporate content. The association takes no responsibility for the
content of the presentation.
OUTLINE
• KEY FINDINGS
• RECOMMENDATIONS
• POST MDG Dec 2015 • WAY FORWARD
2

3
THE MATERNAL – FETAL - NEONATAL CONTINUUM
HOW TO REDUCE PERINATAL DEATHS • STRATEGIC MATERNAL NEONATAL HEALTH ACTIONS
1. High priority in government policies
2. Cost effective clinical interventions
3. Functional health system (access/skilled care)
4. Continuum of care
5. Community involvement
Neonatal Survival 3, Systematic scaling up of neonatal care in countries, Lancet , March 2005
• Integrate
– Data sets
– National ministerial reports
– Existing programmes within MCWH
– Global initiatives – CARMMA, ENAP
• Decentralize care
– Drainage areas
– Facility plans
– Continuum of care
– Community
INTEGRATE MATERNAL + NEWBORN HEALTH
•Continuum of care
•Healthy pregnancy = healthy newborn
•Provide Road map •“guideline for improving maternal and neonatal care” Dec 2012
•Integrate NCCEMD and NAPEMMCO recommendations •5 H’s + HHAPI-NeSS
INCLUDED IN (E)NAPs
6
ADDRESSING THE CONTINUUM OF CARE MATERNAL - CHILD CROSS CUTTING INTERVENTIONSENTIONS
• Family Planning
• BANC
• Maternity Waiting Homes
• Emergency services (dedicated ambulances)
• Child PIP - late neonatal deaths
• WBOTS
• ISHP
Continuum of care Kate Kerber et al, Lancet, Oct 2007
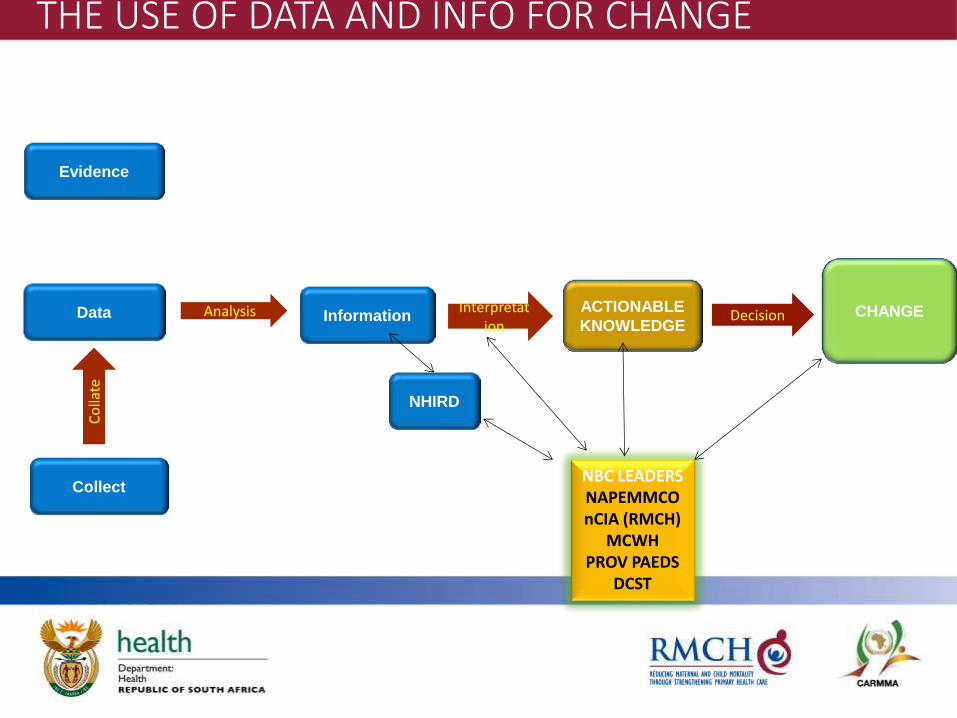
Data Information
ACTIONABLE
KNOWLEDGE CHANGE Analysis Interpretat
ion Decision
Evidence
Collect
Co
llate
NBC LEADERS NAPEMMCO nCIA (RMCH)
MCWH PROV PAEDS
DCST
NHIRD
THE USE OF DATA AND INFO FOR CHANGE
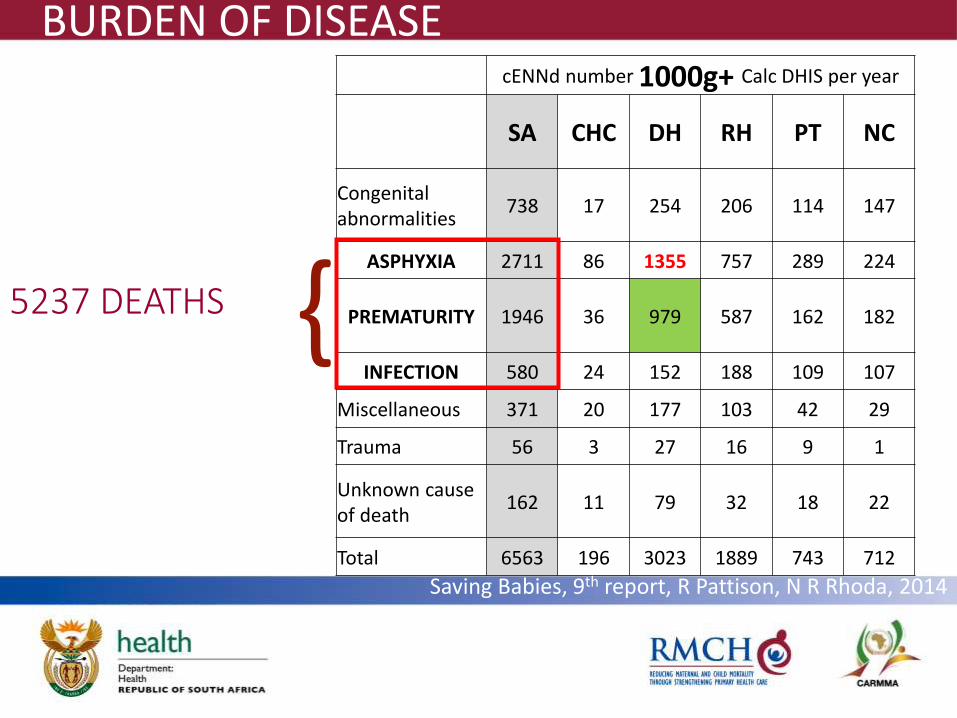
BURDEN OF DISEASE API = 5237 DEATHS 5237 DEATHS
cENNd number 1000g+ Calc DHIS per year
SA CHC DH RH PT NC
Congenital abnormalities
738 17 254 206 114 147
ASPHYXIA 2711 86 1355 757 289 224
PREMATURITY 1946 36 979 587 162 182
INFECTION 580 24 152 188 109 107
Miscellaneous 371 20 177 103 42 29
Trauma 56 3 27 16 9 1
Unknown cause of death
162 11 79 32 18 22
Total 6563 196 3023 1889 743 712
}
BURDEN OF DISEASE
Saving Babies, 9th report, R Pattison, N R Rhoda, 2014
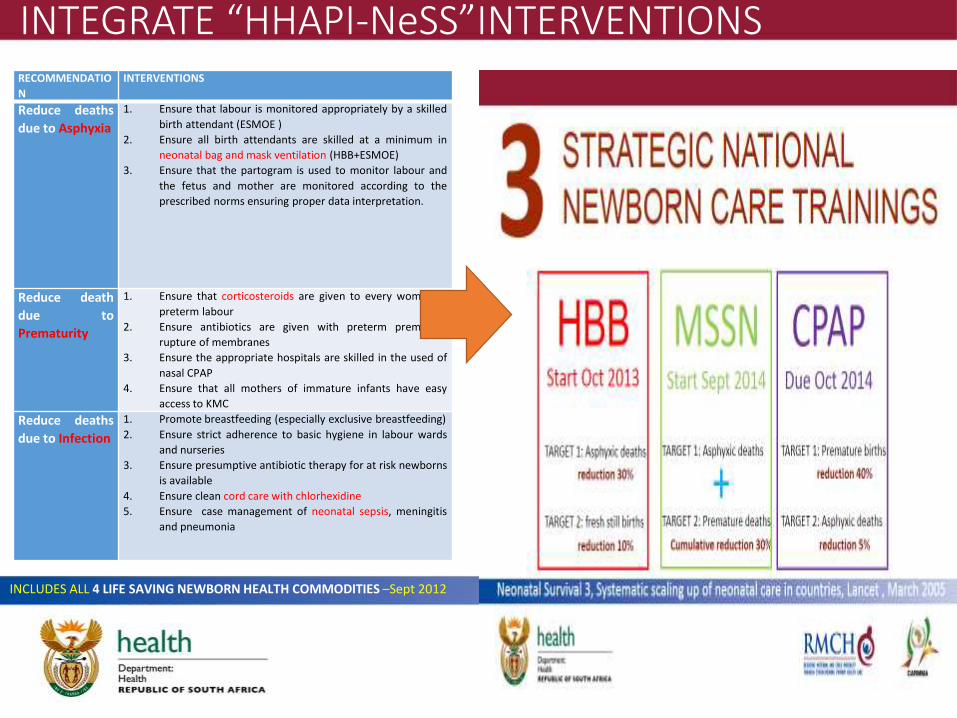
INTEGRATE “HHAPI-NeSS”INTERVENTIONS RECOMMENDATIO
N
INTERVENTIONS
Reduce deaths
due to Asphyxia
1. Ensure that labour is monitored appropriately by a skilled
birth attendant (ESMOE )
2. Ensure all birth attendants are skilled at a minimum in
neonatal bag and mask ventilation (HBB+ESMOE)
3. Ensure that the partogram is used to monitor labour and
the fetus and mother are monitored according to the
prescribed norms ensuring proper data interpretation.
Reduce death
due to
Prematurity
1. Ensure that corticosteroids are given to every women in
preterm labour
2. Ensure antibiotics are given with preterm premature
rupture of membranes
3. Ensure the appropriate hospitals are skilled in the used of
nasal CPAP
4. Ensure that all mothers of immature infants have easy
access to KMC
Reduce deaths
due to Infection
1. Promote breastfeeding (especially exclusive breastfeeding)
2. Ensure strict adherence to basic hygiene in labour wards
and nurseries
3. Ensure presumptive antibiotic therapy for at risk newborns
is available
4. Ensure clean cord care with chlorhexidine
5. Ensure case management of neonatal sepsis, meningitis
and pneumonia
INCLUDES ALL 4 LIFE SAVING NEWBORN HEALTH COMMODITIES –Sept 2012
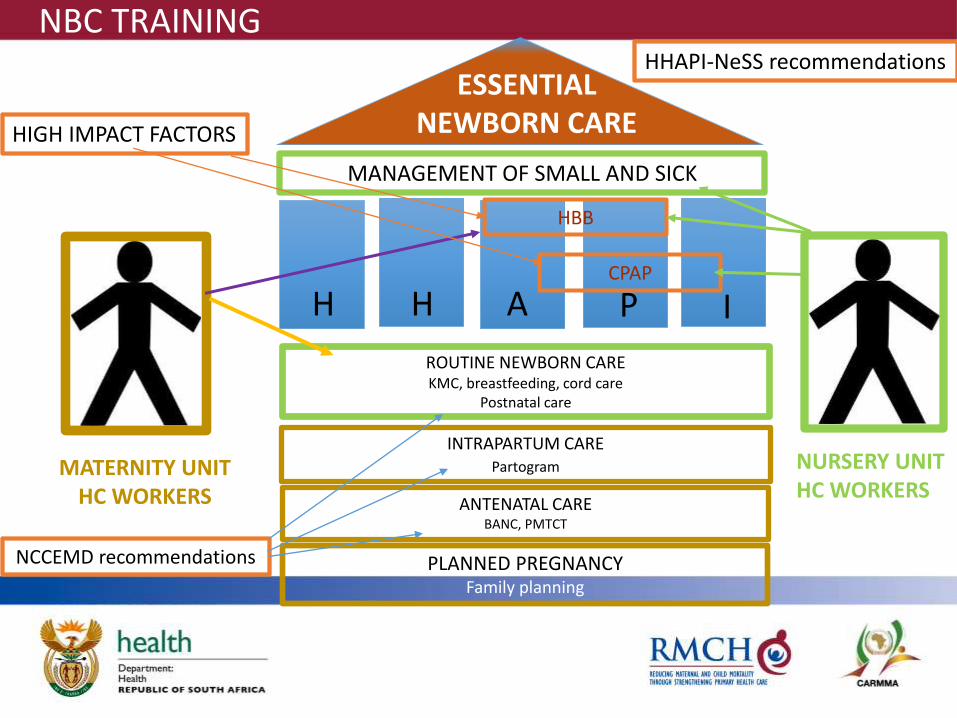
MANAGEMENT OF SMALL AND SICK
PLANNED PREGNANCY Family planning
ANTENATAL CARE BANC, PMTCT
ROUTINE NEWBORN CARE KMC, breastfeeding, cord care
Postnatal care
H A H P I
ESSENTIAL NEWBORN CARE
INTRAPARTUM CARE Partogram MATERNITY UNIT
HC WORKERS
NURSERY UNIT HC WORKERS
HBB
CPAP
HIGH IMPACT FACTORS
HHAPI-NeSS recommendations
NCCEMD recommendations
NBC TRAINING
HHAPI-NeSS • Improve the Health System for mothers and babies
• Improve the knowledge and skills of Health Care providers in maternal and neonatal care
• Reduce deaths due to Asphyxia
• Reduce death due to Prematurity
• Reduce deaths due to Infection
Implement interventions for each of the recommendation forms the basis of the newborn survival strategy (NeSS).
NB**The HHAPI-NeSS road map includes the
5 Hs for maternal health.
11
3 top causes of neonatal
deaths
SUGGESTIONS TO CHANGE APPROACH
• Models of care • NB *”No one size fits all!!”
• Use of analytical model List • Financial plan • % reduction in deaths
REF:PRICELESS REPORT
• Recommendations written in action style • Who facilitates • Who advocates • What is timeline and deadline
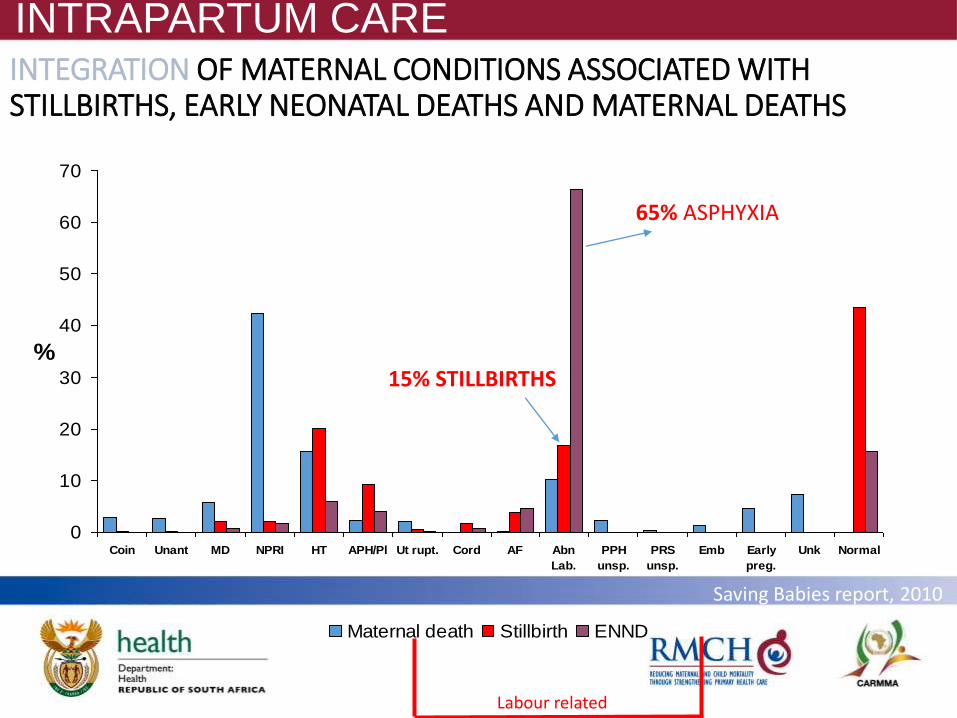
INTEGRATION OF MATERNAL CONDITIONS ASSOCIATED WITH STILLBIRTHS, EARLY NEONATAL DEATHS AND MATERNAL DEATHS
0
10
20
30
40
50
60
70
Coin Unant MD NPRI HT APH/Pl Ut rupt. Cord AF Abn
Lab.
PPH
unsp.
PRS
unsp.
Emb Early
preg.
Unk Normal
%
Maternal death Stillbirth ENND
Labour related
Saving Babies report, 2010
65% ASPHYXIA
15% STILLBIRTHS
INTRAPARTUM CARE
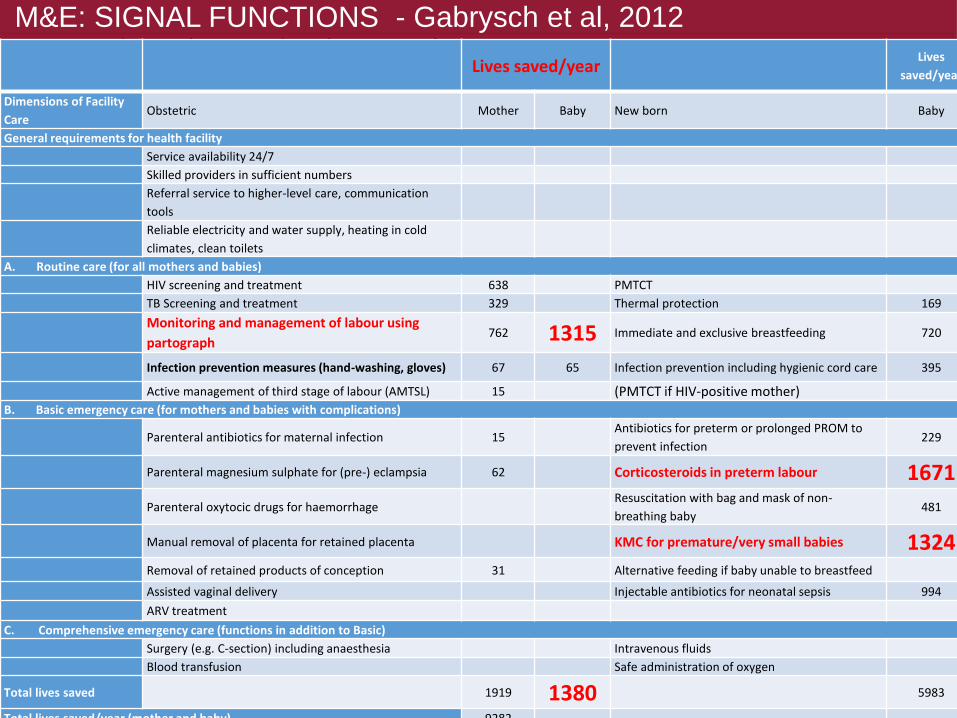
Essential Mother and Baby Care (EMoBaC) Lives saved/year
Lives
saved/year
Dimensions of Facility
Care Obstetric Mother Baby New born Baby
General requirements for health facility
Service availability 24/7
Skilled providers in sufficient numbers
Referral service to higher-level care, communication
tools
Reliable electricity and water supply, heating in cold
climates, clean toilets
A. Routine care (for all mothers and babies)
HIV screening and treatment 638 PMTCT
TB Screening and treatment 329 Thermal protection 169
Monitoring and management of labour using
partograph 762 1315 Immediate and exclusive breastfeeding 720
Infection prevention measures (hand-washing, gloves) 67 65 Infection prevention including hygienic cord care 395
Active management of third stage of labour (AMTSL) 15 (PMTCT if HIV-positive mother) B. Basic emergency care (for mothers and babies with complications)
Parenteral antibiotics for maternal infection 15 Antibiotics for preterm or prolonged PROM to
prevent infection 229
Parenteral magnesium sulphate for (pre-) eclampsia 62 Corticosteroids in preterm labour 1671
Parenteral oxytocic drugs for haemorrhage Resuscitation with bag and mask of non-
breathing baby 481
Manual removal of placenta for retained placenta KMC for premature/very small babies 1324 Removal of retained products of conception 31 Alternative feeding if baby unable to breastfeed
Assisted vaginal delivery Injectable antibiotics for neonatal sepsis 994
ARV treatment
C. Comprehensive emergency care (functions in addition to Basic)
Surgery (e.g. C-section) including anaesthesia Intravenous fluids
Blood transfusion Safe administration of oxygen
Total lives saved 1919 1380 5983
Total lives saved/year (mother and baby) 9282
M&E: SIGNAL FUNCTIONS - Gabrysch et al, 2012

KEY FINDINDS
KEY FINDINGS FOR 2ND TRIENNIAL REPORT (2010-13)
• The neonatal mortality rate for calendar year 2013 has stayed the same
• Highest neonatal death rates is in the weight category 1000g – 1999g
• Reduction in the data gap between DHIS and PPIP has improved
PPIP with quality of care assessments:
good Mpumalanga, N West, Free State, W Cape,
moderate Limpopo and Northern Cape
poor Eastern Cape, Gauteng and KwaZulu-Natal.
16
Data:
Causes of neonatal deaths:
• There is no change in the top three causes Asphyxia, Prematurity and Infections of neonatal deaths
• Unexplained stillbirth is the largest category of macerated stillbirths across all levels of care
• Intrapartum birth asphyxia is the most common category in fresh stillbirths in CHCs and district hospitals.
• Almost 50% of these deaths were thought to be probably preventable; the common problems being with fetal monitoring, use of the partogram and the second stage of labour.
17
At district level • District hospitals have the most deaths, most births and highest
mortality rates and perinatal care indices.
• Small but noticeable improvement in all indicators for districts hospitals when this saving babies report is compared to the 2010-11 Saving Babies report.
• On average one district hospital will deliver: • If 2000 deliveries / year then
• a live born baby between 1000g and 1999g once every 5 days • 12% (one in eight will be an early neonatal death).
• If 500 deliveries / year then: • they will deliver a live born between 1000g and 1999g every 20 days • two will die per year
18
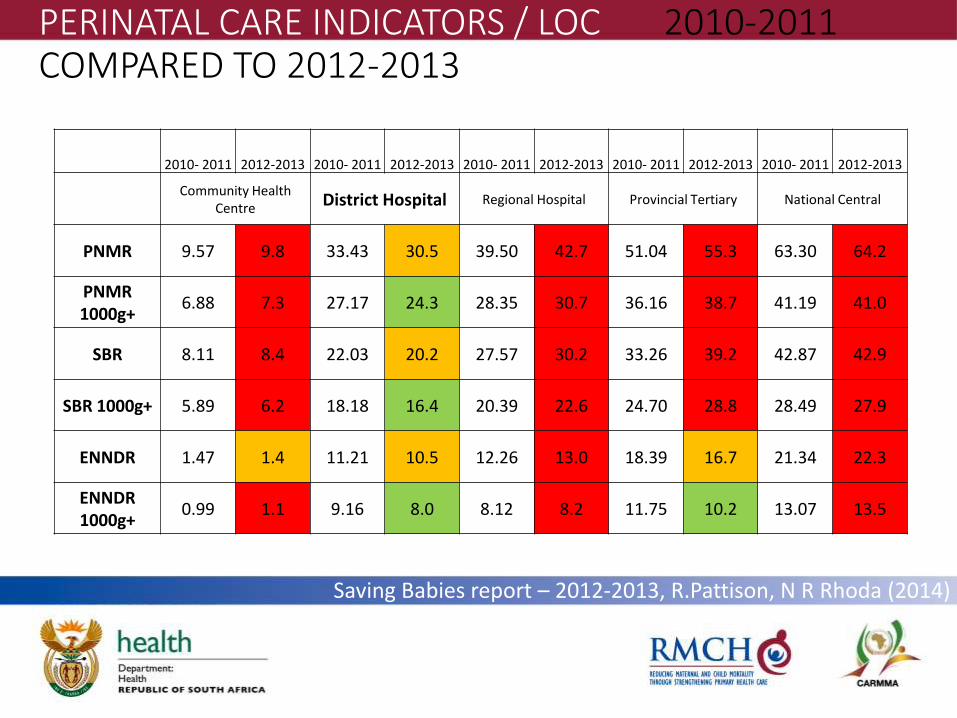
PERINATAL CARE INDICATORS / LOC 2010-2011 COMPARED TO 2012-2013
2010- 2011 2012-2013 2010- 2011 2012-2013 2010- 2011 2012-2013 2010- 2011 2012-2013 2010- 2011 2012-2013
Community Health
Centre District Hospital Regional Hospital Provincial Tertiary National Central
PNMR 9.57 9.8 33.43 30.5 39.50 42.7 51.04 55.3 63.30 64.2
PNMR 1000g+
6.88 7.3 27.17 24.3 28.35 30.7 36.16 38.7 41.19 41.0
SBR 8.11 8.4 22.03 20.2 27.57 30.2 33.26 39.2 42.87 42.9
SBR 1000g+ 5.89 6.2 18.18 16.4 20.39 22.6 24.70 28.8 28.49 27.9
ENNDR 1.47 1.4 11.21 10.5 12.26 13.0 18.39 16.7 21.34 22.3
ENNDR 1000g+
0.99 1.1 9.16 8.0 8.12 8.2 11.75 10.2 13.07 13.5
Saving Babies report – 2012-2013, R.Pattison, N R Rhoda (2014)
Avoidable causes
• Administrative associated causes- • Inadequate facilities were the most common avoidable
factor in spontaneous preterm labour • Deaths due to immaturity were thought to be probably
preventable if better neonatal facilities were available
• Patient associated • In almost one in five deaths which were unexplained
stillbirths the patient was reported as not responding to poor fetal movements
20
Avoidable causes
• Medical personnel associated: • Health care provider issues were relatively rarely reported,
but are significant in their nature.
• Unprofessional behaviour was found by doctors not responding to calls and lack of training also featured.
• In almost a third of babies dying due to complications of hypertension, hypertension was detected but NOT acted upon.
21
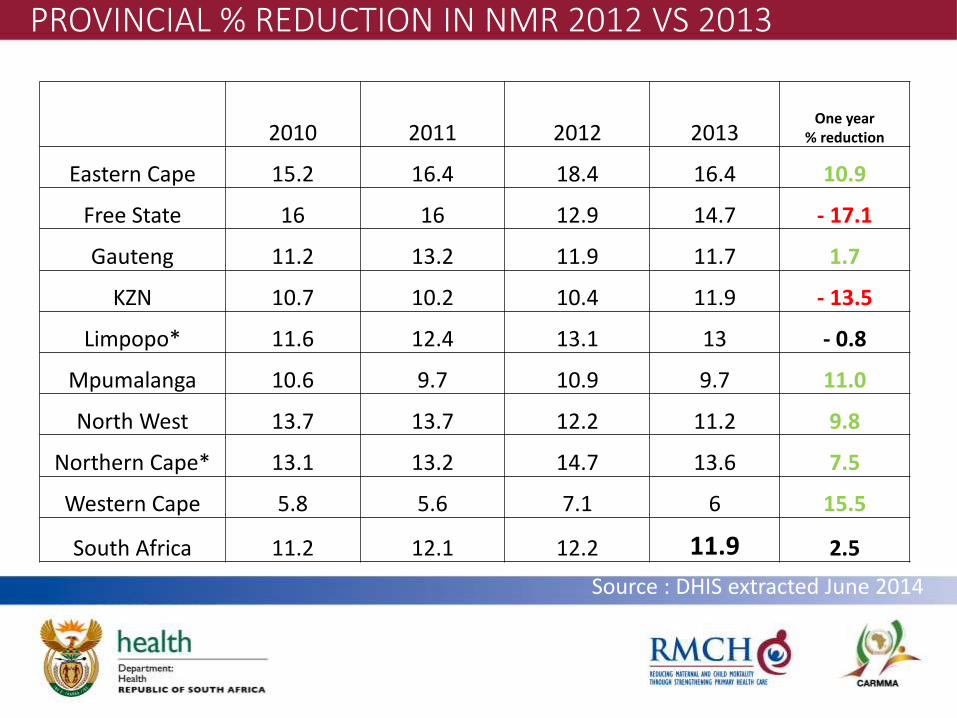
2010 2011 2012 2013 One year
% reduction
Eastern Cape 15.2 16.4 18.4 16.4 10.9
Free State 16 16 12.9 14.7 - 17.1
Gauteng 11.2 13.2 11.9 11.7 1.7
KZN 10.7 10.2 10.4 11.9 - 13.5
Limpopo* 11.6 12.4 13.1 13 - 0.8
Mpumalanga 10.6 9.7 10.9 9.7 11.0
North West 13.7 13.7 12.2 11.2 9.8
Northern Cape* 13.1 13.2 14.7 13.6 7.5
Western Cape 5.8 5.6 7.1 6 15.5
South Africa 11.2 12.1 12.2 11.9 2.5
PROVINCIAL % REDUCTION IN NMR 2012 VS 2013 PER PROVINCE DHIS
Source : DHIS extracted June 2014
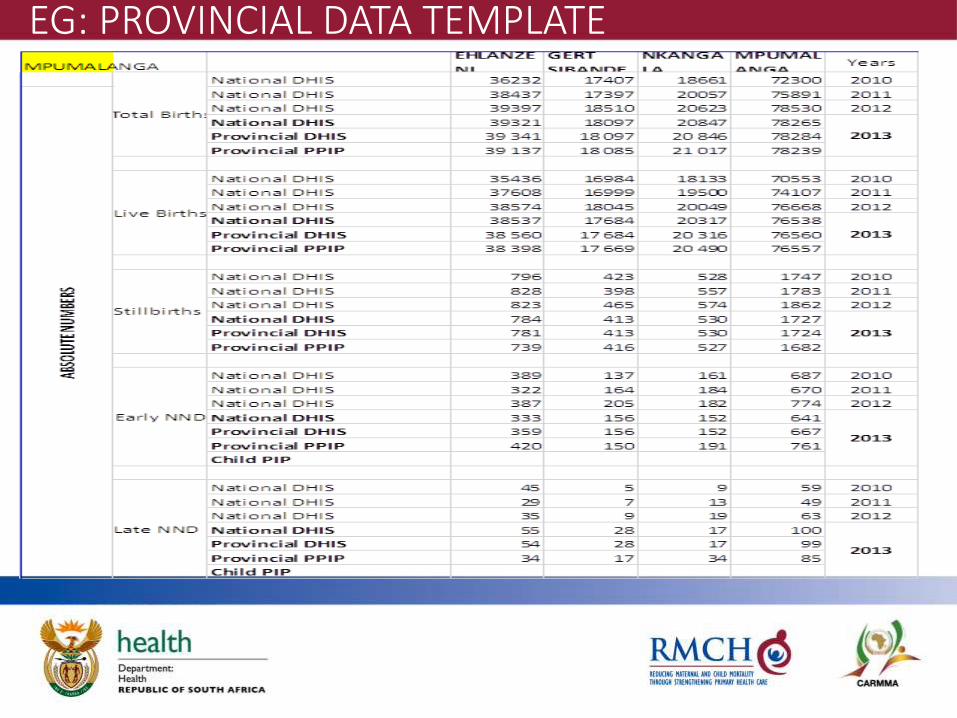
EG: PROVINCIAL DATA TEMPLATE

RECOMMENDATIONS
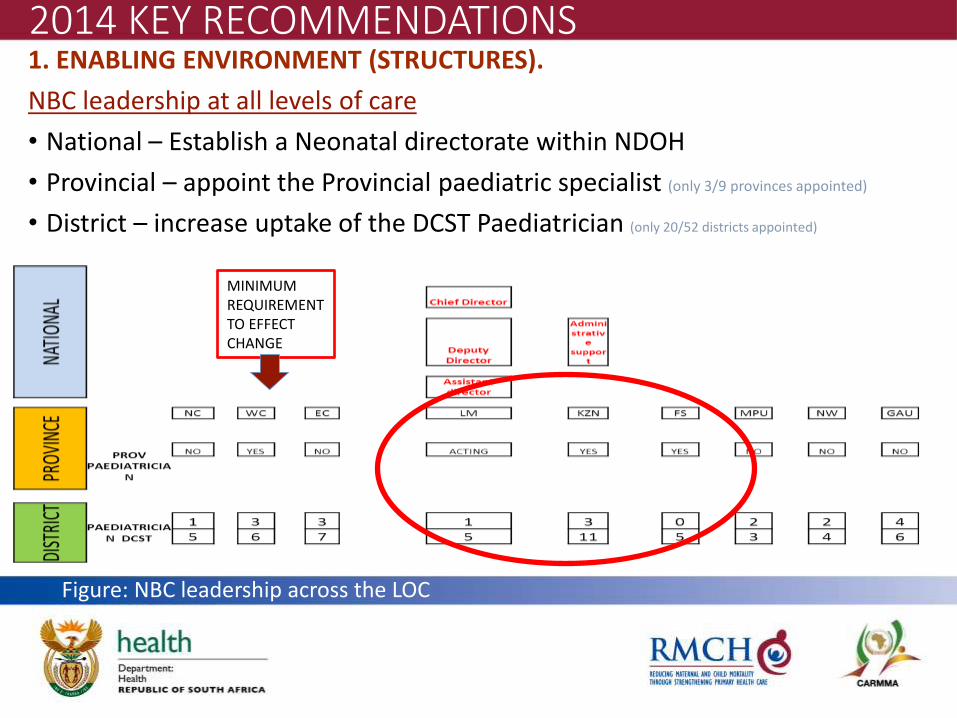
2014 KEY RECOMMENDATIONS 1. ENABLING ENVIRONMENT (STRUCTURES).
NBC leadership at all levels of care
• National – Establish a Neonatal directorate within NDOH
• Provincial – appoint the Provincial paediatric specialist (only 3/9 provinces appointed)
• District – increase uptake of the DCST Paediatrician (only 20/52 districts appointed)
Figure: NBC leadership across the LOC
MINIMUM REQUIREMENT TO EFFECT CHANGE
2014 KEY RECOMMENDATIONS
2. RESOURCES
2.1 Financial: Ring fence money for neonatal care (2012 recommendation)
2.2. Human:
2.2.1 Minimum requirements=Prov Paed + 50% Paed DCST
2.2.2 Appointment of a provincial data co-ordinator
3. CO-ORDINATED PLAN
3.1 National neonatal implementation and monitoring plan
3.2 Standardised Provincial plans
3.3 Strategic District plans -
3.4 Facility plans
2014 KEY RECOMMENDATIONS 4. TRAINING
4.1 Prioritise national roll out of newborn interventions in all districts
4.1.1.Reducing Asphyxia - increase coverage of HBB to 50% by March 2015.
4.1.2.Reducing Premature birth – “preterm package”: • Tocolytics to all mothers in Preterm labour
• Antenatal steroid use at PHC, CHC and DH especially
• CPAP implementation
• MSSN training in districts
4.1. 3 Reducing Infection prioritise hand washing
5. MONITORING AND EVALUATION
5.1 Standardised Provincial template across the country aligned with global Every Newborn Action Plan newborn care indicators
5.2 Neonatal Signal Functions should be incorporated into the DHPs
HHAPI-NeSS
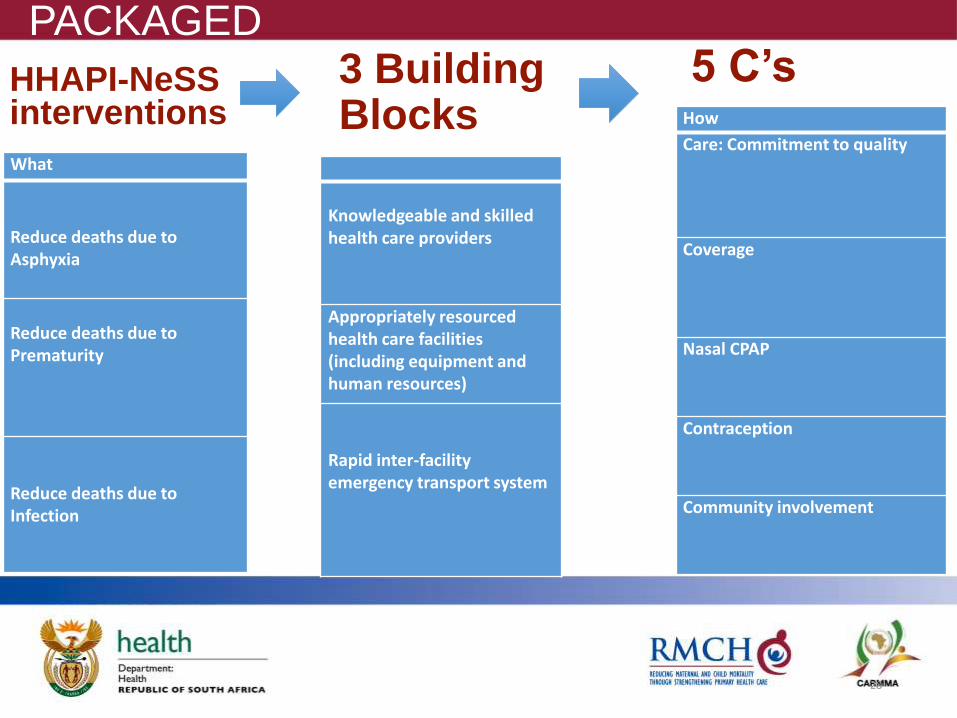
3 Building Blocks
Knowledgeable and skilled health care providers
Appropriately resourced health care facilities (including equipment and human resources)
Rapid inter-facility emergency transport system
28
How
Care: Commitment to quality
Coverage
Nasal CPAP
Contraception
Community involvement
5 C’s HHAPI-NeSS interventions
What
Reduce deaths due to Asphyxia
Reduce deaths due to Prematurity
Reduce deaths due to Infection
PACKAGED
29
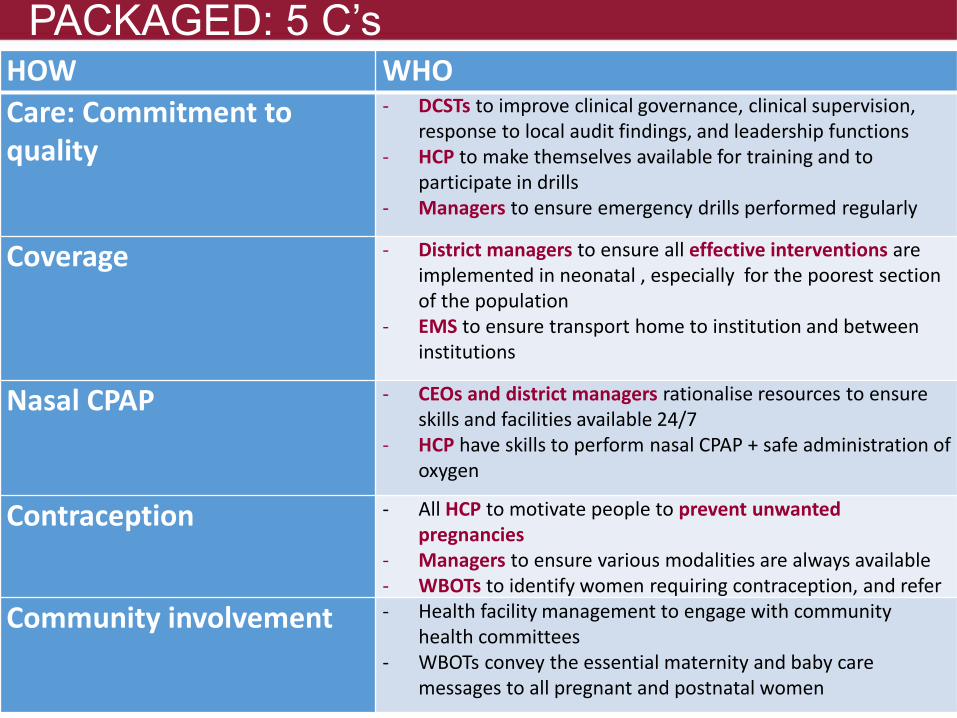
HOW WHO
Care: Commitment to quality
- DCSTs to improve clinical governance, clinical supervision, response to local audit findings, and leadership functions
- HCP to make themselves available for training and to participate in drills
- Managers to ensure emergency drills performed regularly
Coverage - District managers to ensure all effective interventions are implemented in neonatal , especially for the poorest section of the population
- EMS to ensure transport home to institution and between institutions
Nasal CPAP - CEOs and district managers rationalise resources to ensure skills and facilities available 24/7
- HCP have skills to perform nasal CPAP + safe administration of oxygen
Contraception - All HCP to motivate people to prevent unwanted pregnancies
- Managers to ensure various modalities are always available - WBOTs to identify women requiring contraception, and refer
Community involvement - Health facility management to engage with community health committees
- WBOTs convey the essential maternity and baby care messages to all pregnant and postnatal women
PACKAGED: 5 C’s
AIM
Post MDG
2035 global ENAP targets SBR<10
NMR<10
PNDSR PERINATAL DEATH SURVEILLANCE RESPONSE – AU conference, 2012
“EVERY FETUS COUNTS -20 000”
“EVERY NEWBORN COUNTS -12 000”
STILL BIRTHS (DHIS 2013: +20 000 deaths)
• Current interventions with impact
• ESMOE - • HBB - 10% reduction in fresh still births
Develop a National plan to reduce SBs (NAPEMMCO + NCCEMD)
WAY FORWARD 2015+
ACKNOWLEDGEMENTS
RMCH colleagues
NDOH - NHIRD/DHIS
NDOH - child directorate
NDOH - maternal directorate
PPIP – MRC Pretoria
Partners • ELMA
• UNICEF
• WHO
• PATH
• Limpopo University
• Save the Children
NAPEMMCO MEMBERS
• N R Rhoda (chair)
• N. Mzolo (KZN)
• M. Patrick (KZN –child PIP)
• T. Maphosa (MPU)
• N. Shipalana (LP)
• R. Pattison (secretariate)
• P. Cooper (GAU)
• S. Velaphi (GAU)
• OI. Adejayan (NW)
• A. Jassen (NC)
• M. Nazo (EC)
• H. Steinberg (FS)
• I. Els (WC)
• D. Bradshaw (MRC)

THANK YOU