Embed Size (px)
Citation preview

1
NationalInstituteonDrugAbuse(NIDA)
MedicationstoTreatOpioidUseDisorder
LastUpdatedJune2018https://www.drugabuse.gov

2
TableofContents
MedicationstoTreatOpioidUseDisorder
Overview
Howdomedicationstotreatopioidusedisorderwork?
Howeffectivearemedicationstotreatopioidusedisorder?
Whataremisconceptionsaboutmaintenancetreatment?
Whatisthetreatmentneedversusthediversionriskforopioidusedisordertreatment?
WhatistheimpactofmedicationforopioidusedisordertreatmentonHIV/HCVoutcomes?
Howisopioidusedisordertreatedinthecriminaljusticesystem?
Ismedicationtotreatopioidusedisorderavailableinthemilitary?
Whattreatmentisavailableforpregnantmothersandtheirbabies?
HowMuchDoesOpioidTreatmentCost?
Isnaloxoneaccessible?
References

3
Overview
Anestimated2.1millionpeopleintheUnitedStateshadasubstanceusedisorderrelatedtoprescriptionopioidpainmedicinesin2016. However,onlyafractionofpeoplewithprescriptionopioidusedisordersreceivespecialtytreatment(17.5percentin2016). Overdosedeathslinkedtothesemedicineswerefivetimeshigherin2016than1999. Thereisnowalsoariseinheroinuseandheroinusedisorderassomepeopleshiftfromprescriptionopioidstotheircheaperstreetrelative;626,000peoplehadaheroinusedisorderin2016,andmorethan15,000Americansdiedofaheroinoverdosein2016. Besidesoverdose,consequencesoftheopioidcrisisincludearisingincidenceofinfantsborndependentonopioidsbecausetheirmothersusedthesesubstancesduringpregnancy andincreasedspreadofinfectiousdiseases,includingHIVandhepatitisC(HCV),aswasseenin2015insouthernIndiana.
EffectivepreventionandtreatmentstrategiesexistforopioidmisuseandusedisorderbutarehighlyunderutilizedacrosstheUnitedStates.AninitiativeoftheSecretaryofHealthandHumanServices(HHS) beganin2015toaddressthecomplexproblemofprescriptionopioidandheroinuse.In2017,HHSannouncedfiveprioritiesforaddressingtheopioidcrisis:
1. improvingaccesstotreatmentandrecoveryservices
2. promotinguseofoverdose-reversingdrugs
3. strengtheningourunderstandingoftheepidemicthroughbetterpublichealthsurveillance
4. providingsupportforcutting-edgeresearchonpainandaddiction
5. advancingbetterpracticesforpainmanagement
Effectivemedicationsexisttotreatopioidusedisorder:methadone,buprenorphine,andnaltrexone.Thesemedicationscouldhelpmanypeoplerecoverfromopioidusedisorder,buttheyremainhighlyunderutilized.Fewerthanhalfofprivate-sectortreatmentprogramsoffermedicationsforopioidusedisorders,andofpatientsinthoseprogramswhomightbenefit,onlyathird
1
1
2
1,3
4,5
6
7
9

4
actuallyreceiveit. OvercomingthemisunderstandingsandotherbarriersthatpreventwideradoptionofthesetreatmentsiscrucialfortacklingtheproblemofopioidusedisorderandtheepidemicofopioidoverdoseintheUnitedStates.
9

5
Howdomedicationstotreatopioidusedisorderwork?
OpioidAgonistsandPartialAgonists(MaintenanceMedications)
Studiesshowthatpeoplewithopioidusedisorderwhofollowdetoxificationwithcompleteabstinenceareverylikelytorelapse,orreturntousingthedrug. Whilerelapseisanormalsteponthepathtorecovery,itcanalsobelifethreatening,raisingtheriskforafataloverdose.11Thus,animportantwaytosupportrecoveryfromheroinorprescriptionopioidusedisorderistomaintainabstinencefromthosedrugs.Someoneinrecoverycanalsousemedicationsthatreducethenegativeeffectsofwithdrawalandcravingswithoutproducingtheeuphoriathattheoriginaldrugofabusecaused.Forexample,theFDArecentlyapprovedlofexidine,anon-opioidmedicinedesignedtoreduceopioidwithdrawalsymptoms.Methadoneandbuprenorphineareothermedicationsapprovedforthispurpose.
Methadoneisasyntheticopioidagonistthateliminateswithdrawalsymptomsandrelievesdrugcravingsbyactingonopioidreceptorsinthebrain—thesamereceptorsthatotheropioidssuchasheroin,morphine,andopioidpainmedicationsactivate.Althoughitoccupiesandactivatestheseopioidreceptors,itdoessomoreslowlythanotheropioidsand,inanopioid-dependentperson,treatmentdosesdonotproduceeuphoria.Ithasbeenusedsuccessfullyformorethan40yearstotreatopioidusedisorderandmustbedispensedthroughspecializedopioidtreatmentprograms.
Buprenorphineisapartialopioidagonist,meaningthatitbindstothosesameopioidreceptorsbutactivatesthemlessstronglythanfullagonistsdo.Likemethadone,itcanreducecravingsandwithdrawalsymptomsinapersonwithanopioidusedisorderwithoutproducingeuphoria,andpatientstendtotolerateitwell.Researchhasfoundbuprenorphinetobesimilarlyeffectiveasmethadonefortreatingopioidusedisorders,aslongasitisgivenatasufficientdoseandforsufficientduration. TheU.S.FoodandDrugAdministration(FDA)approvedbuprenorphinein2002,makingitthefirstmedicationeligibletobe
10
12
13

6
prescribedbycertifiedphysiciansthroughtheDrugAddictionTreatmentAct.Thisapprovaleliminatestheneedtovisitspecializedtreatmentclinics,therebyexpandingaccesstotreatmentformanywhoneedit.Additionally,theComprehensiveAddictionandRecoveryAct(CARA),whichwassignedintolawinJuly2016,temporarilyexpandseligibilitytoprescribebuprenorphine-baseddrugsformedication-assistedtreatment(MAT)toqualifyingnursepractitionersandphysicianassistantsthroughOctober1,2021.Buprenorphinehasbeenavailableforopioidusedisorderssince2002asatabletandsince2010asasublingualfilm. TheFDAapproveda6-monthsubdermalbuprenorphineimplantinMay2016andaonce-monthlybuprenorphineinjectioninNovember2017.Theseformulationsareavailabletopatientsstabilizedonbuprenorphineandwilleliminatethetreatmentbarrierofdailydosingforthesepatients.(Alsosee"Whataremisconceptionsaboutmaintenancetreatment?")
OpioidAntagonists
Naltrexoneisanopioidantagonist,whichmeansthatitworksbyblockingtheactivationofopioidreceptors.Insteadofcontrollingwithdrawalandcravings,ittreatsopioidusedisorderbypreventinganyopioiddrugfromproducingrewardingeffectssuchaseuphoria.Itsuseforongoingopioidusedisordertreatmenthasbeensomewhatlimitedbecauseofpooradherenceandtolerabilitybypatients.However,in2010,aninjectable,long-actingformofnaltrexone(Vivitrol ),originallyapprovedfortreatingalcoholusedisorder,wasFDA-approvedfortreatingopioidusedisorder.Becauseitseffectslastforweeks,Vivitrol isagoodoptionforpatientswhodonothavereadyaccesstohealthcareorwhostrugglewithtakingtheirmedicationsregularly.
Becauseeachmedicationworksdifferently,atreatmentprovidershoulddecideontheoptimalmedicationinconsultationwiththeindividualpatientandshouldconsiderthepatient’suniquehistoryandcircumstances.
14
®
®

7
Howeffectivearemedicationstotreatopioidusedisorder?
Abundantevidenceshowsthatmethadone,buprenorphine,andnaltrexoneallreduceopioiduseandopioidusedisorder-relatedsymptoms,andtheyreducetheriskofinfectiousdiseasetransmissionaswellascriminalbehaviorassociatedwithdruguse. Thesemedicationsalsoincreasethelikelihoodthatapersonwillremainintreatment,whichitselfisassociatedwithlowerriskofoverdosemortality,reducedriskofHIVandHCVtransmission,reducedcriminaljusticeinvolvement,andgreaterlikelihoodofemployment.
Methadone
Methadoneisthemedicationwiththelongesthistoryofuseforopioidusedisordertreatment,havingbeenusedsince1947.Alargenumberofstudies(someofwhicharesummarizedinthegraphbelow)supportmethadone'seffectivenessatreducingopioiduse.AcomprehensiveCochranereviewin2009comparedmethadone-basedtreatment(methadonepluspsychosocialtreatment)toplacebowithpsychosocialtreatmentandfoundthatmethadonetreatmentwaseffectiveinreducingopioiduse,opioiduse-associatedtransmissionofinfectiousdisease,andcrime. Patientsonmethadonehad33percentfeweropioid-positivedrugtestsandwere4.44timesmorelikelytostayintreatmentcomparedtocontrols. Methadonetreatmentsignificantlyimprovesoutcomes,evenwhenprovidedintheabsenceofregularcounselingservices; long-term(beyond6months)outcomesarebetteringroupsreceivingmethadone,regardlessofthefrequencyofcounselingreceived.
15
15
12,16–20
12
18,19,21
22,23

8
Buprenorphine
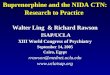
Buprenorphine,whichwasfirstapprovedin2002,iscurrentlyavailableintwoforms:alone(Probuphine ,Sublocade™,Bunavail )andincombinationwiththeopioidreceptorantagonistnaloxone(Suboxone ,Zubsolv ).Bothformulationsofbuprenorphineareeffectiveforthetreatmentofopioidusedisorders,thoughsomestudieshaveshownhighrelapseratesamongpatientstaperedoffofbuprenorphinecomparedtopatientsmaintainedonthedrugforalongerperiodoftime.
® ®
® ®
24
Source:Kakkoetal.,2003

9
ASwedishstudycomparedpatientsmaintainedon16mgofbuprenorphinedailytoacontrolgroupthatreceivedbuprenorphinefordetoxification(6days)followedbyplacebo. Allpatientsreceivedpsychosocialsupports.Inthisstudy,thetreatmentfailurerateforplacebowas100percentvs.25percentforbuprenorphine.Morethantwoopioid-positiveurinetestswithin3monthsresultedincessationoftreatment,sotreatmentretentionwascloselyrelatedtorelapse.Ofpatientsnotretainedintreatment,therewasa20percentmortalityrate.
Meta-analysisdeterminedthatpatientsondosesofbuprenorphineof16mgperdayormorewere1.82timesmorelikelytostayintreatmentthanplacebo-treatedpatients,andbuprenorphinedecreasedthenumberofopioid-positivedrugtestsby14.2percent(thestandardizedmeandifferencewas-1.17).
Tobeeffective,buprenorphinemustbegivenatasufficientlyhighdose(generally,16mgperdayormore).Sometreatmentproviderswaryofusingopioidshaveprescribedlowerdosesforshorttreatmentdurations,leadingtofailureofbuprenorphinetreatmentandthemistakenconclusionthatthemedicationisineffective.
25
13,25,26
13,27

10
MethadoneandBuprenorphineCompared
Methadoneandbuprenorphineareequallyeffectiveatreducingopioiduse.AcomprehensiveCochranereviewcomparingbuprenorphine,methadone,andplacebofoundnodifferencesinopioid-positivedrugtestsorself-reportedheroinusewhentreatingwithmethadoneorbuprenorphineatmedium-to-highdoses.
Notably,flexibledoseregimensofbuprenorphineanddosesofbuprenorphineof6mgorbelowarelesseffectivethanmethadoneatkeepingpatientsintreatment,highlightingtheneedfordeliveryofevidence-baseddosingregimensofthesemedications.
Naltrexone
Naltrexonewasinitiallyapprovedforthetreatmentofopioidusedisorderinadailypillform.Itdoesnotproducetoleranceorwithdrawal.Poortreatmentadherencehasprimarilylimitedthereal-worldeffectivenessofthisformulation. Asaresult,thereisinsufficientevidencethatoralnaltrexoneisaneffectivetreatmentforopioidusedisorder. Extended-releaseinjectablenaltrexone(XR-NTX)isadministeredoncemonthly,whichremovestheneedfordailydosing.Whilethisformulationisthenewestformofmedicationforopioidusedisorder,evidencetodatesuggeststhatitiseffective.
Thedouble-blind,placebo-controlledtrialthatwasmostinfluentialingettingXR-NTXapprovedbytheFDAin2010foropioidusedisordertreatmentshowedthatXR-NTXsignificantlyincreasedopioidabstinence.TheXR-NTXgrouphad90percentconfirmedabstinentweekscomparedto35percentintheplacebogroup.TreatmentretentionwasalsohigherintheXR-NTXgroup(58percentvs.42percent),whilesubjectivedrugcravingandrelapsewerebothdecreased(0.8percentvs.13.7percent). ImprovementintheXR-NTXgroupwassustainedthroughoutanopenlabelperiodoutto76weeks. ThesedatawerecollectedinRussia,andadditionalstudiesarerequiredtodetermineifeffectivenesswillbesimilarintheUnitedStates.
BuprenorphineandNaltrexoneCompared
13
13
28
29
28,30
31
32
33

11
ANIDAstudyshowedthatoncetreatmentisinitiated,abuprenorphine/naloxonecombinationandanextendedreleasenaltrexoneformulationaresimilarlyeffectiveintreatingopioidusedisorder.Becausenaltrexonerequiresfulldetoxification,initiatingtreatmentamongactiveopioiduserswasmoredifficultwiththismedication.However,oncedetoxificationwascomplete,thenaltrexoneformulationhadasimilareffectivenessasthebuprenorphine/naloxonecombination.

12
Whataremisconceptionsaboutmaintenancetreatment?
Becausemaintenancemedications(methadoneandbuprenorphine)arethemselvesopioidsandareabletoproduceeuphoriainpeoplewhoarenotdependentonopioids,manypeoplehaveassumedthatthisformoftreatmentjustsubstitutesanewsubstanceusedisorderforanoldone.Thisbeliefhasunfortunatelyhinderedtheadoptionoftheseeffectivetreatments.Inthepast,evensomeinpatienttreatmentprogramsthatwereotherwiseevidence-baseddidnotallowpatientstousethesemedications,infavorofan"abstinenceonly"philosophy.
Althoughitispossibleforindividualswhodonothaveanopioidusedisordertogethighonbuprenorphineormethadone(see"Whatisthetreatmentneedversusthediversionriskforopioidusedisordertreatment?"),thesemedicationsaffectpeoplewhohavedevelopedahightolerance(see"OpioidTolerance")toopioidsdifferently.Atthedosesprescribed,andasaresultoftheirpharmacodynamicandpharmacokineticproperties(thewaytheyactatopioidreceptorsitesandtheirslowermetabolisminthebody),thesemedicationsdonotproduceaeuphorichighbutinsteadminimizewithdrawalsymptomsandcravings(see"MechanismsofOpioidDependence").Thismakesitpossibleforthepatienttofunctionnormally,attendschoolorwork,andparticipateinotherformsoftreatmentorrecoverysupportservicestohelpthembecomefreeoftheirsubstanceusedisorderovertime.
Theultimateaimcanbetoweanoffthemaintenancemedication,butthetreatmentprovidershouldmakethisdecisionjointlywiththepatientandtaperingthemedicationmustbedonegradually.Itmaytakemonthsoryearsinsomecases.Justasbodytissuesrequireprolongedperiodstohealafterinjuryandmayrequireexternalsupports(e.g.,acastandcrutchesorawheelchairforabrokenleg),braincircuitsthathavebeenalteredbyprolongeddruguseandsubstanceusedisordertaketimetorecoverandbenefitfromexternalsupportsintheformofmedication.Incasesofseriousandlong-termopioidusedisorder,apatientmayneedthesesupportsindefinitely.

13
In2005,methadoneandbuprenorphinewereaddedtotheWorldHealthOrganization'slistofessentialmedicines,definedasmedicinesthatare"intendedtobeavailablewithinthecontextoffunctioninghealthcaresystemsatalltimesinadequateamounts,intheappropriatedosageforms,withassuredquality,andatapricetheindividualandthecommunitycanafford."
OpioidTolerance
Peoplewhotakeopioidsforlongperiodsoftimetypicallydeveloptolerance,astateinwhichmoreofthedrugisneededtoproducethesameeffect.Receptordesensitizationanddownregulationaremolecularprocessesthatcausetolerance.Inpeoplewithopioidusedisorder,thebrainiscontinuallyexposedtohighlevelsofopioidsaswellasdopamine,whichisreleasedintherewardcircuitfollowingopioidreceptoractivation.Braincellsrespondtothisbyreducingtheirresponsetoreceptoractivationandbyremovingopioidanddopaminereceptorsfromthecellmembrane,resultinginfewerreceptorsthatcanbeactivatedbythedrug. Thesemechanismsresultinalessenedresponsetothedrug,sohigherdosesarerequiredtoelicitthesameeffect.Thisopioidtoleranceisthereasonthatpeoplewithopioidusedisorderdonotexperienceeuphoriceffectsfromtherapeuticdosesofbuprenorphineormethadone,whilepeoplewithoutopioidusedisorderdo. Itisalsothereasonwhypeopleareatincreasedriskofoverdosewhenrelapsingtoopioiduseafteraperiodofabstinence:Theylosetheirtolerancetothedrugwithoutrealizingit,sotheynolongerknowwhatdoseofthedrugtheycansafelytolerate.
34,35
36,37
38,39

14
MechanismsofOpioidDependence
Thesustainedactivationofopioidreceptorsthatresultsfromopioidusedisorderandcausestolerancealsocauseswithdrawalsymptomswhentheopioiddrugsleavethebody.Drugwithdrawalsymptomsareoppositetothesymptomscausedbydrugtaking.Inthecaseofopioids,theyincludeanxiety,jitters,anddiarrhea. Avoidanceofthesenegativesymptomsisonereasonthatpeoplekeeptakingopioids,andintheearlystagesoftreatment,medicationssuchasmethadoneandbuprenorphinereducewithdrawalsymptoms.
40
Opioidreceptoractivity.Heroin(redline)activatesopioidreceptorsfullyandquickly.Methadone(blue)isalsoafullagonist,buttheactivationismuchslowerandlongerlasting.Buprenorphine(green)activatesthereceptorspartially,withasimilartimecoursetomethadone.Naltrexone(purple)isanopioidreceptorantagonistandthereforepreventsreceptoractivation.Sources:Cruciani&Knotkova,2013;Goodmanetal.,2006
41,42

15
Whatisthetreatmentneedversusthediversionriskforopioidusedisordertreatment?
Likeotheropioidmedications,buprenorphineandmethadonearesometimesdivertedandmisused.However,mostdatasuggestthatthemajorityofbuprenorphineandmethadonemisuse(usewithoutaprescription)isforthepurposeofcontrollingwithdrawalandcravingsforotheropioidsandnottogethigh.Amongallopioidagonistmedications,methadoneandbuprenorphinetogethermakeup15percentofdiversionreports,whileoxycodoneandhydrocodoneareresponsiblefor67percent. Naltrexone,anopioidantagonistusedtotreatopioidaddiction,doesnotcauseeuphoriceffectsandisnotadiversionrisk.
DiversionRiskofBuprenorphine
Bothbuprenorphineandbuprenorphine/naloxoneformulationscaninterferewiththeeffectsoffullopioidagonists,suchasheroin,andcanprecipitatewithdrawalinindividualswithopioiddependence.TwoU.S.surveysofpeoplewithopioidusedisorderfoundthatamajorityofthosewhousedillicitbuprenorphinereportedthattheyuseditfortherapeuticpurposes(i.e.,toreducewithdrawalsymptoms,reduceheroinuse,etc.). Ninety-sevenpercentreportedusingittopreventcravings,90percenttopreventwithdrawal,and29percenttosavemoney. Illicituseofbuprenorphinedecreasedasindividualshadaccesstotreatment. Theminorityproportionofpeoplewhousebuprenorphineillicitlytogethigh(rangingfrom8to25percent) hasbeenshowntodecreaseovertime,whichcouldsuggestthatpeopleabandonthisgoalaftertheyexperiencethedrug’sbluntedrewardingeffects. Indeed,patientsintreatmentforopioidusedisorderrarelyendorsebuprenorphineastheprimarydrugofmisuse.
Whilethereissomeriskassociatedwithmisuseofbuprenorphine,theriskofharms,suchasfataloverdose,aresignificantlylowerthanthoseoffullagonistopioids(oxycodone,hydrocodone,heroin). Overdosesandrelateddeaths
43
44,45
45
45
45,46
46
47
39,51

16
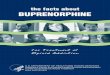
dooccurbutareusuallytheresultofcombinationwithotherrespiratorydepressantdrugssuchasbenzodiazepinesoralcohol.Emergencydepartment(ED)visitsinvolvingbuprenorphineincreasedfrom3,161in2005to30,135visitsin2010asavailabilityofthedrugincreased(buprenorphinewasfirstapprovedin2002);butEDvisitsforbuprenorphineremainsignificantlylesscommonthanthoseforotheropioids. Fifty-twopercent,or15,778visits(seeleftbarchartbelow),wererelatedtononmedicalusein2010;59percentofthesevisitsinvolvedadditionaldrugs(seerightbarchartbelow).
52
53,54
Emergencydepartment(ED)visitsinvolvingbuprenorphineincreasedasdrugavailabilityincreased,butEDvisitsforbuprenorphinearefarlesscommonthanthoseforotheropioids.

17
DiversionRiskofMethadone
Methadonediversionisprimarilyassociatedwithmethadoneprescribedforthetreatmentofpainandnotforthetreatmentofopioidusedisorders.Opioidtreatmentprogramsarerequiredtomaintainandimplementadiversioncontrolplan;theytypicallyrequirepatientstocomeindailytoreceivetheirmedicationandstrictlymonitortake-homedoses.Inaddition,evidencesuggeststhatthediversionthatdoesoccurisassociatedwithalackofaccesstomedication. Inonesurvey,givingmethadoneawaywasidentifiedasthemostcommonformofmethadonediversion, whichalignswithotherfindingsthat80percentofpeoplewhoreportdivertingmethadonedidsotohelpotherswhomisusedsubstances. Amongthoseusingillicitmethadone,themostcommonreasonwasamissedmedicationpick-up.
Methadone,asafullopioidagonistthatismetabolizedslowly,posesagreaterriskofoverdosethanbuprenorphine.In2010,65,945EDvisitsinvolvednonmedicaluseofmethadone. However,methadonethatisdispensedforuseasapainreliever,notasansubstanceusedisordermedication,isthemain
Source:CBHSQ,2011
48
49
48,50
50
53
55

18
sourceofthemethadoneinvolvedinoverdosedeaths.55

19
WhatistheimpactofmedicationforopioidusedisordertreatmentonHIV/HCVoutcomes?
InjectiondruguseisstillaprimarydriveroftheHIV/AIDSepidemicacrosstheworld. ArecentexampleisthesmallcommunityofAustin,Indiana,where170newHIVinfectionsoccurredinthe8monthsbetweenNovember2014andJune2015amongpeoplemisusingtheprescriptionopioidpainrelieveroxymorphone(Opana )viainjection. Peoplewhoinjectdrugsfrequentlysharetheirneedlesandotherinjectionequipment,enablingvirusessuchasHIVandhepatitisC(HCV)tospreadbetweenpeople.
MedicationsforopioidusedisordertreatmentcanreducetransmissionofHIVandHCVbyreducingriskbehaviorsinpeoplewhoinjectdrugsandcanimproveHIV-andHCV-relatedoutcomesbytreatingthosenotengagedininjectionopioidusewhomightotherwisetransitiontoinjection,linkingthosewithHIV/HCVinfectiontoappropriatetreatment, andimprovingadherencetoHIV/HCVtreatment. TheseimprovementsdependonaccessibilityofmedicationsforopioidusedisordertopeoplewhoneeditandcoordinatingmedicationdeliverywithHCV/HIVscreeningandtreatment.
Treatmentwithmethadoneorbuprenorphineisassociatedwithreducedinjectiondruguseriskbehaviors.Meta-analyseshaveshownareductioninriskbehaviorsincludinga32to69percentreductioninillicitopioiduse,a20to60percentreductionininjectiondruguse,anda25to86percentreductioninsharingofinjectionequipment. Treatmentwithextended-releasenaltrexonealsoreducedHIVriskbehaviorscomparedtoplacebo.
MethadoneandbuprenorphinetreatmentarealsoassociatedwithlowerHCVinfectionratesinyoungadultswhoinjectdrugs,whileothertreatmentsanddetoxificationalonearenot. MethadonetreatmentisassociatedwithlowratesofcontractingHCVoverall, withmathematicalmodelingsuggestingthatitcanprevent22.6newHCVinfectionsper100treatedpeoplewhoengagedininjectiondruguse,peryear. MethadonetreatmentalsoreducesbothHIV
56
® 6
57,58
59,60
61,62
31
63
64
65,66

20
riskbehaviorsandHIVinfection,withbetteroutcomesforpeoplewhoinjectdrugswhoareintreatment(3.5percentcontractingHIVvs.22percent),andbetteroutcomesforlongertreatmentdurationandforcontinuous(versusinterrupted)treatment.
AstudycomparingtheeffectsofmethadoneandbuprenorphinetreatmentonHIVriskfrominjectionbehaviorsandHIVriskfromsexualbehaviorsshowedequalandsignificantreductionsinriskyinjectionbehaviors.Riskysexualbehaviorswerereducedinbothmaleandfemalemethadonepatientsbutwerehigherinmalepatientsonbuprenorphine.
MitigatingFactors
ThereareseveralknowninteractionsbetweenmedicationsusedtotreatHIVorHCVandbothmethadoneandbuprenorphine. Thesecouldrequireanadjustmentofdosageorrevisionofthetreatmentplan,andhighlighttheneedforintegratedcare.Forexample,somepatientsarereluctanttobeginhighlyactiveantiretroviraltherapy(HAART)becauseofworriesthatitwillinterferewiththeirmethadonetreatment,sotreatmentprovidersshouldconsiderrevisedmethadonedosesforthesepatients.
ContractingHCVwhileonmethadoneisassociatedwithcontinuedinjectiondruguse. SomestudieshaveshownmethadonedetoxificationalonetobeassociatedwithincreasedratesofcontractingHIV,soongoingtreatmentwiththismedicationiskeytoreducingtransmissionofviralinfection.
PossibilityofDualTherapeuticPotential
OnerecentreportdemonstratesthepotentialofbuprenorphinetocounteractaneuroinflammatoryprocessthatisinvolvedinHIV-associatedneurocognitivedisorders,suggestingthatbuprenorphinecouldpotentiallybesimultaneouslytherapeuticforopioidusedisorderandHIV. OpioidusedisordermedicationsarealsoassociatedwithincreasedadherencetoHAARTforthetreatmentofHIV. SomeprovidershesitatetotreatHCVinpeoplewhoinjectdrugs,butanaltrexoneimplantationclinicshowedratesofsustainedvirologicresponseintheirpatientsthatwerecomparabletoclinicstreatingnon-injection-
67–69
70
71,72
72
73
74
75,76
59,60
77

21
drug-usingpatients.
77

22
Howisopioidusedisordertreatedinthecriminaljusticesystem?
Opioidusedisordersarehighlyprevalentamongcriminaljusticepopulations.AccordingtodatafromtheU.S.DepartmentofJustice,approximatelyhalfofstateandfederalprisonersmeetcriteriaforsubstanceusedisorder. Evenso,therehasbeenreticenceincriminaljusticesettingstousingmethadone,buprenorphine,andnaltrexonetotreatopioidusedisorder.Innationalsurveys,utilizationofthesemedicationsisverylowincriminaljusticesettings,includingdrugcourts, jails, andprisons. Thus,opioidusedisordergoeslargelyuntreatedduringperiodsofincarceration,andopioiduseoftenresumesafterrelease.
Aformerinmate’sriskofdeathwithinthefirst2weeksofreleaseismorethan12timesthatofotherindividuals,withtheleadingcauseofdeathbeingafataloverdose. Overdosesaremorecommonwhenapersonrelapsestodruguseafteraperiodofabstinenceduetolossoftolerancetothedrug.Onestudyfoundareductioninpost-incarcerationdeathsfromoverdoseamongindividualswhohadreceivedmedicationforopioidusedisorderincorrectionalfacilities. Untreatedopioidusedisordersalsocontributetoareturntocriminalactivity,reincarceration,andriskybehaviorcontributingtothespreadofHIVandhepatitisBandCinfections(see"WhatistheimpactofmedicationforopioidusedisordertreatmentonHIV/HCVoutcomes?").
TheWorldHealthOrganization’sGuidelinesforthePsychosociallyAssistedPharmacologicalTreatmentofOpioidDependencerecommendsthatincarceratedindividualsshouldreceiveadequatehealthcareandthatopioidwithdrawal,agonistmaintenanceandnaltrexonetreatmentshouldallbeavailableinprisonsettings,andprisonersshouldnotbeforcedtoacceptanyparticulartreatment."
Manystatescurrentlydonotofferappropriateaccesstoorutilizemedicationstotreatopioidusedisorderamongarresteesorinmateseventhoughresearchhasshownmanybenefitsofincorporatingmedication-assistedtreatmentintocriminaljusticetreatmentprograms.Inmateswhoreceivebuprenorphine
78
79 80 81
82
83
84
85

23
treatmentpriortoreleasearemorelikelytoengageintreatmentaftertheirreleasethaninmateswhoonlyparticipateincounseling. Participantswhoengageinmethadonetreatmentandcounselinginprisonaremorelikelytoentercommunity-basedmethadonetreatmentcentersaftertheirrelease(68.6percent)thanthosereceivingonlycounseling(7.8percent)orthoseincounselingandreferredtoatreatmentcenter(50percent).
Inonestudy,inmateswhobeganbuprenorphinetreatmentwhileincarceratedengagedinpost-releasetreatmentsooner,averaging3.9daysafterrelease,comparedto9.2daysforparticipantsreferredtotreatmentpost-release. Theywerealsolikelytostayintreatmentlongeriftheywereinitiatedintreatmentpriortorelease(20.3weeksonaverage)thaniftheybegantreatmentaftertheirrelease(13.2weeks).
Inmateswhoparticipateinmethadonetreatmentandcounselingwhileinprisonarelesslikelytotestpositiveforillicitopioidsatonemonthfollowingtheirrelease(27.6percent)comparedtothosewhoonlyreceivecounseling(62.9percent)andthosewhoreceivecounselingandareferraltoatreatmentcenter(41percent).
Arandomizedcontrolledtrialwaspublishedin2016,comparingprison-initiatedextended-releasenaltrexone(XR-NTX)treatmenttostandardcounselingprotocolsforpreventionofopioidrelapse.Duringthetreatmentphase,relapsewassignificantlylowerinthegroupreceivingXR-NTX(43percentvs.64percent).TheXR-NTXgroupalsoexperiencednooverdoseevents,whilethereweresevenoverdoseeventsinthecontrolgroup.
Asurveyofcommunitycorrectionagents’viewsonusingmedicationstotreatopioidusedisordershowedthatmorefavorableattitudestowardmedicationuseareassociatedwithgreaterknowledgeabouttheevidencebaseforthesemedicationsandgreaterunderstandingofopioidusedisorderasamedicaldisorder. Organizationallinkagebetweencorrectionalstakeholdersandcommunitytreatmentproviders,alongwithtrainingsessions,canbeaneffectivewaytochangeperceptionsandincreaseknowledgeabouttheefficacyofthesemedications,andcanincreasetheintentwithincorrectionalfacilitiestoreferindividualswithopioidusedisordertotreatmentthatincorporates
87
19
84
84
19
88
89
86

24
medications.
Amechanismtoreducerecidivismanddivertnonviolentoffendersfromtraditionaljailandprisonsettingsisthedrugtreatmentcourtmodel,whichprovidestreatmentservicesincombinationwithjudicialsupervision. Still,resistancetomedicationspersistseveninthisareaofthecriminaljusticesystem;asurveypublishedin2013reportedthat50percentofdrugcourtsdidnotallowagonisttreatmentforopioidusedisorderunderanycircumstances.In2015,theOfficeofNationalDrugControlPolicyannouncedthatstatedrugcourtsreceivingfederalgrantsmustnot:1)denyanyappropriateandeligibleclientforthetreatmentdrugcourtaccesstotheprogrambecauseoftheiruseofFDA-approvedmedicationsthatisinaccordancewithanappropriatelyauthorizedprescription;or2)mandatethatadrugcourtclientnolongerusemedicationsaspartoftheconditionsofthedrugcourtifsuchamandateisinconsistentwithamedicalpractitioner’srecommendationorprescription.
86
90
79
91

25
Ismedicationtotreatopioidusedisorderavailableinthemilitary?
Ratesofprescriptionopioidmisusearehigheramongservicemembersthanamongcivilians. Surveyresultssuggestdruguseamongreturningsoldiersisoftenacopingstrategytotreatarousalsymptomsofpost-traumaticstressdisorder. Returningmilitarypersonnelalsoexperiencehigherratesofchronicpainandrelatedmedicaluseofopioidpainrelieverscomparedtothecivilianpopulation.Thesedatacollectivelysuggestanunmetneedfortheassessment,management,andtreatmentofbothchronicpainandopioidusedisorderinthispopulation.
TheVeteransHealthAdministration(VHA)acknowledgesthattreatmentwithopioidagonists(methadoneorbuprenorphine)isthefirst-linetreatmentforopioidusedisorderandrecommendsitforallopioid-dependentpatients.Notably,a2015revisionoftreatmentguidelinesfortheU.S.DepartmentofVeteranAffairsandU.S.DepartmentofDefenseshiftedtowardallowingthesemedicationsasatreatmentoptionforactivedutymilitarymembers. Still,onlyaboutaquarterofpatientswithanopioidusedisordertreatedatVHAfacilitiesreceivemedication. BarrierstoopioidagonistmedicationamongVHAprovidersincludelackofperceivedpatientinterest,stigmatowardthepatientpopulation,andlackofeducationaboutopioidagonisttreatment.
Inthepast,lackofinsurancecoverageforopioidagonistmedicationswasabarrierforuseamongactivedutymilitary;however,asof2013,TRICAREincludedcoverageforthesemedications,anda2016modificationofTRICAREregulationincludedprovisionsforexpandedcoverageofopioidusedisordertreatment. Thisexpandedcoverageremovedannualandlifetimelimitationsonsubstanceusedisordertreatmentallowedforoffice-basedopioidtreatment,andestablishedopioidtreatmentprogramsasanewlyrecognizedcategoryofinstitutionalproviderunderTRICARE.
92
93
94
95
96
97
98

26
Whattreatmentisavailableforpregnantmothersandtheirbabies?
Parallelingthelargerecentincreasesinopioiduse,usedisorder,andoverdose,theincidenceofbabiesborndependentonopioids(neonatalabstinencesyndrome,orNAS)asaresultofthemother’sopioiduseduringpregnancyhasalsogreatlyincreased. IncidenceofNASrosenearlyfivefoldbetween2000and2012; thisincreasewasassociatedwithincreasesintheprescriptionofopioidstopregnantwomenforpain,whichdoubledbetween1995and2009.
Untreatedopioidusedisorderduringpregnancycanhavedevastatingeffectsonthefetus.Thefluctuatinglevelsofopioidsinthebloodofmothersmisusingopioidsexposethefetustorepeatedperiodsofwithdrawal, whichcanalsoharmthefunctionoftheplacentaandincreasetheriskof:
fetalgrowthrestriction
placentalabruption
pretermlabor
fetalconvulsions
intrauterinepassageofmeconium
Source:Toliaetal.,2015
5
4
99,100
101
101
101
101
101
101
102

27
fetaldeath
Inadditiontothesedirectphysicaleffects,otherriskstothefetusinclude:
untreatedmaternalinfectionssuchasHIV
malnutritionandpoorprenatalcare
dangersconferredbydrug-seekinglifestyle,includingviolenceandincarceration
MethadoneandBuprenorphineastheStandardofCareforOpioidUseDisorderinPregnancy
Tolessenthenegativeeffectsofopioiddependenceonthefetus,treatmentwithmethadonehasbeenusedforpregnantwomenwithopioidusedisordersincethe1970sandhasbeenrecognizedasthestandardofcaresince1998.Recentevidence,however,suggeststhatbuprenorphinemaybeanevenbettertreatmentoption.
Bothmethadoneandbuprenorphinetreatmentduringpregnancy:
stabilizefetallevelsofopioids,reducingrepeatedprenatalwithdrawal
improveneonataloutcomes
increasematernalHIVtreatmenttoreducethelikelihoodoftransmittingthevirustothefetus
linkmotherstobetterprenatalcare
Ameta-analysisshowedthat,comparedtosingle-dosemethadonetreatment,buprenorphineresultedin:
10percentlowerincidenceofNAS
shorterneonataltreatmenttime(anaverageof8.4daysshorter)
102
103
104
102,104
102,103
105
101,106
104
102–104
102,104

28
loweramountofmorphineusedforNAStreatment(anaverageof3.6mglower)
highergestationalage,weight,andheadcircumferenceatbirth
DatafromtheNIDA-fundedMaternalOpioidTreatment:HumanExperimentalResearchstudyshowsimilarbenefitsofbuprenorphine. Still,methadoneisassociatedwithhighertreatmentretentionthanbuprenorphine. Divideddosingwithmethadonehasbeenexploredasawaytoreducefetalexposuretowithdrawalperiods,andrecentdatashowlowlevelsofNASinbabiesborntomotherstreatedwithdivideddosesofmethadone. Largercomparisonstudiesareneededtodetermineifsplitmethadonedosingforopioidusedisordersinpregnancyisassociatedwithbetteroutcomes.
NASstilloccursinbabieswhosemothershavereceivedbuprenorphineormethadone,butitislessseverethanitwouldbeintheabsenceoftreatment.ResearchdoesnotsupportreducingmaternalmethadonedosetoavoidNAS,asthismaypromoteincreasedillicitdruguse,resultinginincreasedrisktothefetus.
105
107
105
108
109
101
Source:Jonesetal.,2010

29
HowMuchDoesOpioidTreatmentCost?
Althoughthepriceforopioidtreatmentmayvarybasedonanumberoffactors,recentpreliminarycostestimatesfromtheU.S.DepartmentofDefensefortreatmentinacertifiedopioidtreatmentprogram(OTP)provideareasonablebasisforcomparison:
methadonetreatment,includingmedicationandintegratedpsychosocialandmedicalsupportservices(assumesdailyvisits):$126.00perweekor$6,552.00peryear
buprenorphineforastablepatientprovidedinacertifiedOTP,includingmedicationandtwice-weeklyvisits:$115.00perweekor$5,980.00peryear
naltrexoneprovidedinanOTP,includingdrug,drugadministration,andrelatedservices:$1,176.50permonthor$14,112.00peryear
Toputthesecostsintocontext,itisusefultocomparethemwiththecostsofotherconditions.AccordingtotheAgencyforHealthcareResearchandQuality,annualexpendituresforindividualswhoreceivedhealthcareare$3,560.00forthosewithdiabetesmellitusand$5,624.00forkidneydisease.
Itisalsoimportanttorememberthecostsassociatedwithuntreatedopioidusedisorders,includingcostsassociatedwith:
criminaljustice
treatingbabiesborndependentonopioids
greatertransmissionofinfectiousdiseases
treatingoverdoses
injuriesassociatedwithintoxication(e.g.,druggeddriving)
lostproductivity
98
110

30
Theamountpaidfortreatmentofsubstanceusedisordersisonlyasmallportionofthecoststhesedisordersimposeonsociety.AnanalysissuggestedthatthetotalcostsofprescriptionopioidusedisordersandoverdosesintheUnitedStateswas$78billionin2013.Ofthat,only3.6percent,orabout$2.8billion,wasfortreatment.111

31
Isnaloxoneaccessible?
Naloxoneisanopioidantagonistthatcanreverseanopioidoverdose.Naloxoneaccessincreasedbetween2010and2014,with:
morethanthreetimesthenumberoflocalsitesprovidingnaloxone(from188to644)
nearlythreetimesthenumberoflaypersonsprovidednaloxonekits(from53,032to152,283)
a94percentincreaseinstates(from16to30),includingWashington,DC,withatleastoneorganizationprovidingnaloxone
morethan2.5timesthenumberofoverdosereversalsreported(from10,171to26,463)
Naloxoneprescriptionsdispensedfromretailpharmaciesincreasednearlytwelvefoldbetweenthefourthquarterof2013andthesecondquarterof2015.
Moststateshavepassedlawstowidentheavailabilitytonaloxoneforfamily,friends,andotherpotentialbystandersofoverdose.
8
112

32
Naloxonehasbecomewidelyusedbyemergencymedicalproviders,withall50statesandtheDistrictofColumbia,Guam,andPuertoRicocertifyingandapprovingemergencymedicalservicepersonnelattheparamedicleveltoadministernaloxone.Onestepfurther,emergencymedicaltechnicians(EMTs)wereexplicitlypermittedtoadministernaloxonein12ofthese53jurisdictions(23percent—California,Colorado,DistrictofColumbia,Massachusetts,Maryland,NewMexico,NorthCarolina,Ohio,Oklahoma,RhodeIsland,Virginia,andVermont)asofNovember2013.Becausenon-paramedicEMTsaretypicallythefirstandsometimesonlysourceofemergencycare,providingauthorizationandtrainingforthemtoadministernaloxoneisapromisingstrategytoreduceoverdosedeaths.
Afteranaloxonetrainingsession,amajorityofpoliceofficersreportedthatitwouldnotbedifficulttousenaloxoneatthesceneofanoverdose(89.7percent)andthatitwasimportantthatotherofficersbetrainedtousenaloxone(82.9percent).
EffectsofNaloxoneDistribution
113
114

33
Overdoseeducationandnaloxonedistribution(OEND)hasbeenshowntoincreasethereversalofpotentiallyfataloverdoses;onestudyshowedopioidoverdosedeathratestobe27to46percentlowerincommunitieswhereOENDwasimplemented. Among4,926peoplewhousedsubstancesandparticipatedinOENDinMassachusetts,373(7.6percent)reportedadministeringnaloxoneduringanoverdoserescue,withfewdifferencesinbehaviorbetweentrainedanduntrainedoverdoserescuers. AnaloxonedistributionstudyinSanFranciscoreportedthat11percentofparticipantsusednaloxoneduringanoverdose;of399overdoseeventswherenaloxonewasused,89percentwerereversed. Briefeducationissufficienttoimprovecomfortandcompetenceinrecognizingandmanagingoverdose.Prospectivestudiesareneededtodeterminetheoptimalleveloftrainingandwhethernaloxonerescuekitscanmeetthestandardforbecomingavailableoverthecounter.
Inaprobabilisticanalysis,naloxonedistributionprogramswereshowntopreventoverdosedeaths,increasequality-adjustedlifeyears(QALYs)andbehighlycost-effective.Naloxonedistributionwaspredictedtoprevent6percentofoverdosedeaths,1forevery227naloxonekitsdistributed.Costeffectiveness,undermarkedlyconservativepredictions,wasmeasuredtobe$14,000.00perQALY,wellwithinthestandardfavorablerangeofcost-benefitratios(under$50,000.00perQALY).
Criticsofnaloxonedistributionhaveclaimedthatitcouldleadtoanincreaseinriskyopioiduse,butastudyinMassachusettsshowedratesofopioid-relatedemergencydepartmentvisitsandhospitaladmissionswerenotsignificantlydifferentincommunitieswithloworhighimplementationofOENDprograms.
115
116
117
118
116
119
115

34
References
1. SubstanceAbuseCenterforBehavioralHealthStatisticsandQuality.Resultsfromthe2016NationalSurveyonDrugUseandHealth:DetailedTables.SAMHSA.https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2016/NSDUH-DetTabs-2016.htm.PublishedSeptember7,2017.AccessedMarch7,2018.
2. RuddRA,AleshireN,ZibbellJE,GladdenRM.IncreasesinDrugandOpioidOverdoseDeaths--UnitedStates,2000-2014.MMWRMorbMortalWklyRep.2016;64(50-51):1378-1382.doi:10.15585/mmwr.mm6450a3.
3. RuddRA,SethP,DavidF,SchollL.IncreasesinDrugandOpioid-InvolvedOverdoseDeaths-UnitedStates,2010-2015.MMWRMorbMortalWklyRep.2016;65(5051):1445-1452.doi:10.15585/mmwr.mm655051e1.
4. PatrickSW,DavisMM,LehmannCU,LehmanCU,CooperWO.Increasingincidenceandgeographicdistributionofneonatalabstinencesyndrome:UnitedStates2009to2012.JPerinatolOffJCalifPerinatAssoc.2015;35(8):650-655.doi:10.1038/jp.2015.36.
5. ToliaVN,PatrickSW,BennettMM,etal.IncreasingincidenceoftheneonatalabstinencesyndromeinU.S.neonatalICUs.NEnglJMed.2015;372(22):2118-2126.doi:10.1056/NEJMsa1500439.
6. ConradC,BradleyHM,BrozD,etal.CommunityOutbreakofHIVInfectionLinkedtoInjectionDrugUseofOxymorphone--Indiana,2015.MMWRMorbMortalWklyRep.2015;64(16):443-444.
7. U.S.DepartmentofHealthandHumanServices,OfficeoftheAssistantSecretaryforPlanningandEvaluation.OpioidAbuseintheU.S.andHHSActionstoAddressOpioid-DrugRelatedOverdosesandDeaths.ASPE.https://aspe.hhs.gov/pdf-report/opioid-abuse-us-and-hhs-actions-address-opioid-drug-related-overdoses-and-deaths.PublishedNovember23,2015.AccessedMay11,2017.
8. WheelerE,JonesTS,GilbertMK,DavidsonPJ,CentersforDiseaseControlandPrevention(CDC).OpioidOverdosePreventionProgramsProvidingNaloxonetoLaypersons-UnitedStates,2014.MMWRMorbMortalWklyRep.2015;64(23):631-635.

35
9. KnudsenHK,AbrahamAJ,RomanPM.Adoptionandimplementationofmedicationsinaddictiontreatmentprograms.JAddictMed.2011;5(1):21-27.doi:10.1097/ADM.0b013e3181d41ddb.
10. BartG.Maintenancemedicationforopiateaddiction:thefoundationofrecovery.JAddictDis.2012;31(3):207-225.doi:10.1080/10550887.2012.694598.
11. DavoliM,BargagliAM,PerucciCA,etal.Riskoffataloverdoseduringandafterspecialistdrugtreatment:theVEdeTTEstudy,anationalmulti-siteprospectivecohortstudy.AddictAbingdonEngl.2007;102(12):1954-1959.doi:10.1111/j.1360-0443.2007.02025.x.
12. MattickRP,BreenC,KimberJ,DavoliM.Methadonemaintenancetherapyversusnoopioidreplacementtherapyforopioiddependence.CochraneDatabaseSystRev.2009;(3):CD002209.doi:10.1002/14651858.CD002209.pub2.
13. MattickRP,BreenC,KimberJ,DavoliM.Buprenorphinemaintenanceversusplaceboormethadonemaintenanceforopioiddependence.CochraneDatabaseSystRev.2014;(2):CD002207.doi:10.1002/14651858.CD002207.pub4.
14. SubstanceAbuseandMentalHealthServicesAdministration.ClinicalGuidelinesfortheUseofBuprenorphineintheTreatmentofOpioidAddiction:ATreatmentImprovementProtocolTIP40.SubstanceAbuseandMentalHealthServicesAdministration;2004.https://www.ncbi.nlm.nih.gov/books/NBK64245/pdf/Bookshelf_NBK64245.pdf.AccessedMay11,2017.
15. TheAmericanSocietyofAddictionMedicine.AdvancingAccesstoAddictionMedications.http://www.asam.org/docs/default-source/advocacy/aaam_implications-for-opioid-addiction-treatment_final.AccessedMay11,2017.
16. YancovitzSR,DesJarlaisDC,PeyserNP,etal.Arandomizedtrialofaninterimmethadonemaintenanceclinic.AmJPublicHealth.1991;81(9):1185-1191.
17. VanichseniS,WongsuwanB,ChoopanyaK,WongpanichK.AcontrolledtrialofmethadonemaintenanceinapopulationofintravenousdrugusersinBangkok:implicationsforpreventionofHIV.IntJAddict.1991;26(12):1313-

36
1320.
18. SchwartzRP,HighfieldDA,JaffeJH,etal.Arandomizedcontrolledtrialofinterimmethadonemaintenance.ArchGenPsychiatry.2006;63(1):102-109.doi:10.1001/archpsyc.63.1.102.
19. KinlockTW,GordonMS,SchwartzRP,O’GradyK,FitzgeraldTT,WilsonM.Arandomizedclinicaltrialofmethadonemaintenanceforprisoners:resultsat1-monthpost-release.DrugAlcoholDepend.2007;91(2-3):220-227.doi:10.1016/j.drugalcdep.2007.05.022.
20. DolanKA,ShearerJ,MacDonaldM,MattickRP,HallW,WodakAD.ArandomisedcontrolledtrialofmethadonemaintenancetreatmentversuswaitlistcontrolinanAustralianprisonsystem.DrugAlcoholDepend.2003;72(1):59-65.
21. SchwartzRP,KellySM,O’GradyKE,GandhiD,JaffeJH.Randomizedtrialofstandardmethadonetreatmentcomparedtoinitiatingmethadonewithoutcounseling:12-monthfindings.AddictAbingdonEngl.2012;107(5):943-952.doi:10.1111/j.1360-0443.2011.03700.x.
22. SeesKL,DelucchiKL,MassonC,etal.Methadonemaintenancevs180-daypsychosociallyenricheddetoxificationfortreatmentofopioiddependence:arandomizedcontrolledtrial.JAMA.2000;283(10):1303-1310.
23. GruberVA,DelucchiKL,KielsteinA,BatkiSL.Arandomizedtrialof6-monthmethadonemaintenancewithstandardorminimalcounselingversus21-daymethadonedetoxification.DrugAlcoholDepend.2008;94(1-3):199-206.doi:10.1016/j.drugalcdep.2007.11.021.
24. FiellinDA,SchottenfeldRS,CutterCJ,MooreBA,BarryDT,O’ConnorPG.Primarycare-basedbuprenorphinetapervsmaintenancetherapyforprescriptionopioiddependence:arandomizedclinicaltrial.JAMAInternMed.2014;174(12):1947-1954.doi:10.1001/jamainternmed.2014.5302.
25. KakkoJ,SvanborgKD,KreekMJ,HeiligM.1-yearretentionandsocialfunctionafterbuprenorphine-assistedrelapsepreventiontreatmentforheroindependenceinSweden:arandomised,placebo-controlledtrial.LancetLondEngl.2003;361(9358):662-668.doi:10.1016/S0140-6736(03)12600-1.

37
26. FudalaPJ,BridgeTP,HerbertS,etal.Office-basedtreatmentofopiateaddictionwithasublingual-tabletformulationofbuprenorphineandnaloxone.NEnglJMed.2003;349(10):949-958.doi:10.1056/NEJMoa022164.
27. MacDonaldK,LambK,ThomasML,KhentiganW.BuprenorphineMaintenanceTreatmentofOpiateDependence:CorrelationsBetweenPrescriberBeliefsandPractices.SubstUseMisuse.2016;51(1):85-90.doi:10.3109/10826084.2015.1089905.
28. NunesEV,KrupitskyE,LingW,etal.TreatingOpioidDependenceWithInjectableExtended-ReleaseNaltrexone(XR-NTX):WhoWillRespond?JAddictMed.2015;9(3):238-243.doi:10.1097/ADM.0000000000000125.
29. MinozziS,AmatoL,VecchiS,DavoliM,KirchmayerU,VersterA.Oralnaltrexonemaintenancetreatmentforopioiddependence.CochraneDatabaseSystRev.2011;(4):CD001333.doi:10.1002/14651858.CD001333.pub4.
30. KrupitskyE,NunesEV,LingW,GastfriendDR,MemisogluA,SilvermanBL.Injectableextended-releasenaltrexone(XR-NTX)foropioiddependence:long-termsafetyandeffectiveness.AddictAbingdonEngl.2013;108(9):1628-1637.doi:10.1111/add.12208.
31. KrupitskyE,NunesEV,LingW,IlleperumaA,GastfriendDR,SilvermanBL.Injectableextended-releasenaltrexoneforopioiddependence:adouble-blind,placebo-controlled,multicentrerandomisedtrial.LancetLondEngl.2011;377(9776):1506-1513.doi:10.1016/S0140-6736(11)60358-9.
32. SyedYY,KeatingGM.Extended-releaseintramuscularnaltrexone(VIVITROL®):areviewofitsuseinthepreventionofrelapsetoopioiddependenceindetoxifiedpatients.CNSDrugs.2013;27(10):851-861.doi:10.1007/s40263-013-0110-x.
33. JacksonH,MandellK,JohnsonK,ChatterjeeD,VannessDJ.Cost-EffectivenessofInjectableExtended-ReleaseNaltrexoneComparedWithMethadoneMaintenanceandBuprenorphineMaintenanceTreatmentforOpioidDependence.SubstAbuse.2015;36(2):226-231.doi:10.1080/08897077.2015.1010031.
34. WorldHealthOrganization.ProposalfortheInclusionofBuprenorphineintheWHOModelListofEssentialMedicines.;2004.

38
http://www.who.int/substance_abuse/activities/buprenorphine_essential_medicines.pdfAccessedMay11,2017.
35. WorldHealthOrganization.ProposalfortheInclusionofMethadoneintheWHOModelListofEssentialMedicines.WorldHealthOrganization;2004.http://www.who.int/substance_abuse/activities/methadone_essential_medicines.pdf.AccessedMay11,2017.
36. WilliamsJT,IngramSL,HendersonG,etal.Regulationofµ-opioidreceptors:desensitization,phosphorylation,internalization,andtolerance.PharmacolRev.2013;65(1):223-254.doi:10.1124/pr.112.005942.
37. AlloucheS,NobleF,MarieN.Opioidreceptordesensitization:mechanismsanditslinktotolerance.FrontPharmacol.2014;5:280.doi:10.3389/fphar.2014.00280.
38. WalshSL,JuneHL,SchuhKJ,PrestonKL,BigelowGE,StitzerML.Effectsofbuprenorphineandmethadoneinmethadone-maintainedsubjects.Psychopharmacology(Berl).1995;119(3):268-276.
39. HighlightsofPrescribingInformation:SUBOXONE®.February2017.https://www.suboxone.com/content/pdfs/prescribing-information.pdf.AccessedMay11,2017.
40. KostenTR,GeorgeTP.Theneurobiologyofopioiddependence:implicationsfortreatment.SciPractPerspect.2002;1(1):13-20.
41. CrucianiRA,KnotkovaH,eds.HandbookofMethadonePrescribingandBuprenorphineTherapy.NewYork:Springer-Verlag;2013.
42. BruntonLL,LazoJS,ParkerKL,eds.Goodman&Gilman’sThePharmacologicalBasisofTherapeutics.11thed.
43. U.S.DepartmentofJusticeDrugEnforcementAdministration,OfficeofDiversionControl.NationalForensicLaboratoryInformationSystem(NFLIS)2013AnnualReport.https://www.nflis.deadiversion.usdoj.gov/DesktopModules/ReportDownloads/Reports/NFLIS2013AR.pdfAccessedMay11,2017.
44. BazaziAR,YokellM,FuJJ,RichJD,ZallerND.Illicituseofbuprenorphine/naloxoneamonginjectingandnoninjectingopioidusers.JAddictMed.2011;5(3):175-180.doi:10.1097/ADM.0b013e3182034e31.

39
45. Schuman-OlivierZ,AlbaneseM,NelsonSE,etal.Self-treatment:illicitbuprenorphineusebyopioid-dependenttreatmentseekers.JSubstAbuseTreat.2010;39(1):41-50.doi:10.1016/j.jsat.2010.03.014.
46. CiceroTJ,SurrattHL,InciardiJ.Useandmisuseofbuprenorphineinthemanagementofopioidaddiction.JOpioidManag.2007;3(6):302-308.
47. CiceroTJ,EllisMS,SurrattHL,KurtzSP.Factorscontributingtotheriseofbuprenorphinemisuse:2008-2013.DrugAlcoholDepend.2014;142:98-104.doi:10.1016/j.drugalcdep.2014.06.005.
48. JohnsonB,RichertT.Diversionofmethadoneandbuprenorphinefromopioidsubstitutiontreatment:astaffperspective.JPsychoactiveDrugs.2014;46(5):427-435.doi:10.1080/02791072.2014.960109.
49. JohnsonB,RichertT.DiversionofmethadoneandbuprenorphinebypatientsinopioidsubstitutiontreatmentinSweden:prevalenceestimatesandriskfactors.IntJDrugPolicy.2015;26(2):183-190.doi:10.1016/j.drugpo.2014.10.003.
50. DuffyP,MackridgeAJ.Useanddiversionofillicitmethadone–underwhatcircumstancesdoesitoccur,andpotentialrisksassociatedwithcontinueduseofothersubstances.JSubstUse.2014;19(1-2):48-55.doi:10.3109/14659891.2012.734539.
51. SoykaM.Newdevelopmentsinthemanagementofopioiddependence:focusonsublingualbuprenorphine-naloxone.SubstAbuseRehabil.2015;6:1-14.doi:10.2147/SAR.S45585.
52. CenterforBehavioralHealthStatisticsandQuality(CBHSQ).DrugAbuseWarningNetwork:2011:SelectedTablesofNationalEstimatesofDrug-RelatedEmergencyDepartmentVisits.Rockville,MD:SubstanceAbuseandMentalHealthServicesAdministration;2013.
53. SubstanceAbuseandMentalHealthServicesAdministration.DrugAbuseWarningNetwork,2011:NationalEstimatesofDrug-RelatedEmergencyDepartmentVisits.https://www.samhsa.gov/data/sites/default/files/DAWN2k11ED/DAWN2k11ED/DAWN2k11ED.pdfPublishedMay2013.AccessedMay12,2017.
54. SubstanceAbuseandMentalHealthServicesAdministration,CenterforBehavioralHealthStatisticsandQuality(CBHSQ).TheDAWNReport:

40
EmergencyDepartmentVisitsInvolvingBuprenorphine.SubstanceAbuseandMentalHealthServicesAdministration;2013.AccessedMay12,2017.
55. CentersforDiseaseControlandPrevention(CDC).Vitalsigns:riskforoverdosefrommethadoneusedforpainrelief-UnitedStates,1999-2010.MMWRMorbMortalWklyRep.2012;61(26):493-497.
56. MetzgerDS,DonnellD,CelentanoDD,etal.ExpandingsubstanceusetreatmentoptionsforHIVpreventionwithbuprenorphine-naloxone:HIVPreventionTrialsNetwork058.JAcquirImmuneDeficSyndr1999.2015;68(5):554-561.doi:10.1097/QAI.0000000000000510.
57. PerlmanDC,JordanAE,UuskulaA,etal.AninternationalperspectiveonusingopioidsubstitutiontreatmenttoimprovehepatitisCpreventionandcareforpeoplewhoinjectdrugs:Structuralbarriersandpublichealthpotential.IntJDrugPolicy.2015;26(11):1056-1063.doi:10.1016/j.drugpo.2015.04.015.
58. OtiashviliD,PiralishviliG,SikharulidzeZ,KamkamidzeG,PooleS,WoodyGE.Methadoneandbuprenorphine-naloxoneareeffectiveinreducingillicitbuprenorphineandotheropioiduse,andreducingHIVriskbehavior--outcomesofarandomizedtrial.DrugAlcoholDepend.2013;133(2):376-382.doi:10.1016/j.drugalcdep.2013.06.024.
59. MaltaM,StrathdeeSA,MagnaniniMMF,BastosFI.Adherencetoantiretroviraltherapyforhumanimmunodeficiencyvirus/acquiredimmunedeficiencysyndromeamongdrugusers:asystematicreview.AddictAbingdonEngl.2008;103(8):1242-1257.doi:10.1111/j.1360-0443.2008.02269.x.
60. BatkiSL,GruberVA,BradleyJM,BradleyM,DelucchiK.Acontrolledtrialofmethadonetreatmentcombinedwithdirectlyobservedisoniazidfortuberculosispreventionininjectiondrugusers.DrugAlcoholDepend.2002;66(3):283-293.
61. GowingL,FarrellMF,BornemannR,SullivanLE,AliR.OralsubstitutiontreatmentofinjectingopioidusersforpreventionofHIVinfection.CochraneDatabaseSystRev.2011;(8):CD004145.doi:10.1002/14651858.CD004145.pub4.
62. GowingLR,HickmanM,DegenhardtL.MitigatingtheriskofHIVinfectionwithopioidsubstitutiontreatment.BullWorldHealthOrgan.2013;91(2):148-

41
149.doi:10.2471/BLT.12.109553.
63. TsuiJI,EvansJL,LumPJ,HahnJA,PageK.AssociationofopioidagonisttherapywithlowerincidenceofhepatitisCvirusinfectioninyoungadultinjectiondrugusers.JAMAInternMed.2014;174(12):1974-1981.doi:10.1001/jamainternmed.2014.5416.
64. NolanS,DiasLimaV,FairbairnN,etal.TheimpactofmethadonemaintenancetherapyonhepatitisCincidenceamongillicitdrugusers.AddictAbingdonEngl.2014;109(12):2053-2059.doi:10.1111/add.12682.
65. PelesE,SchreiberS,RadosV,AdelsonM.LowriskforhepatitisCseroconversioninmethadonemaintenancetreatment.JAddictMed.2011;5(3):214-220.doi:10.1097/ADM.0b013e31820e13dd.
66. AlavianSM,MirahmadizadehA,JavanbakhtM,etal.EffectivenessofMethadoneMaintenanceTreatmentinPreventionofHepatitisCVirusTransmissionamongInjectingDrugUsers.HepatMon.2013;13(8):e12411.doi:10.5812/hepatmon.12411.
67. HallinanR,ByrneA,AminJ,DoreGJ.HepatitisCvirusincidenceamonginjectingdrugusersonopioidreplacementtherapy.AustNZJPublicHealth.2004;28(6):576-578.
68. GibsonDR,FlynnNM,McCarthyJJ.EffectivenessofmethadonetreatmentinreducingHIVriskbehaviorandHIVseroconversionamonginjectingdrugusers.AIDSLondEngl.1999;13(14):1807-1818.
69. MetzgerDS,WoodyGE,McLellanAT,etal.Humanimmunodeficiencyvirusseroconversionamongintravenousdrugusersin-andout-of-treatment:an18-monthprospectivefollow-up.JAcquirImmuneDeficSyndr.1993;6(9):1049-1056.
70. WoodyGE,BruceD,KorthuisPT,etal.HIVriskreductionwithbuprenorphine-naloxoneormethadone:findingsfromarandomizedtrial.JAcquirImmuneDeficSyndr1999.2014;66(3):288-293.doi:10.1097/QAI.0000000000000165.
71. BruceRD,MoodyDE,AlticeFL,GourevitchMN,FriedlandGH.AreviewofpharmacologicalinteractionsbetweenHIVorhepatitisCvirusmedicationsandopioidagonisttherapy:implicationsandmanagementforclinicalpractice.ExpertRevClinPharmacol.2013;6(3):249-269.

42
doi:10.1586/ecp.13.18.
72. MaasB,KerrT,FairbairnN,MontanerJ,WoodE.PharmacokineticinteractionsbetweenHIVantiretroviraltherapyanddrugsusedtotreatopioiddependence.ExpertOpinDrugMetabToxicol.2006;2(4):533-543.doi:10.1517/17425255.2.4.533.
73. ZhouW,WangX,ZhouS,etal.HepatitisCseroconversioninmethadonemaintenancetreatmentprogramsinWuhan,China.AddictAbingdonEngl.2015;110(5):796-802.doi:10.1111/add.12836.
74. MacArthurGJ,MinozziS,MartinN,etal.OpiatesubstitutiontreatmentandHIVtransmissioninpeoplewhoinjectdrugs:systematicreviewandmeta-analysis.BMJ.2012;345:e5945.
75. CarvalloL,LopezL,CheF-Y,etal.BuprenorphinedecreasestheCCL2-mediatedchemotacticresponseofmonocytes.JImmunolBaltimMd1950.2015;194(7):3246-3258.doi:10.4049/jimmunol.1302647.
76. FittingS,ZouS,El-HageN,etal.OpiateaddictiontherapiesandHIV-1Tat:interactiveeffectsonglial[Ca ]i,oxyradicalandneuroinflammatorychemokineproductionandcorrelativeneurotoxicity.CurrHIVRes.2014;12(6):424-434.
77. JeffreyGP,MacQuillanG,ChuaF,etal.HepatitisCviruseradicationinintravenousdrugusersmaintainedwithsubcutaneousnaltrexoneimplants.HepatolBaltimMd.2007;45(1):111-117.doi:10.1002/hep.21470.
78. MumolaCJ,KarbergJC.BureauofJusticeStatisticsSpecialReport:DrugUseandDependence,StateandFederalPrisoners,2004.U.S.DepartmentofJustice,OfficeofJusticePrograms;2006.https://www.bjs.gov/content/pub/pdf/dudsfp04.pdf.AccessedMay11,2017.
79. MatusowH,DickmanSL,RichJD,etal.MedicationassistedtreatmentinUSdrugcourts:resultsfromanationwidesurveyofavailability,barriersandattitudes.JSubstAbuseTreat.2013;44(5):473-480.doi:10.1016/j.jsat.2012.10.004.
80. FiscellaK,MooreA,EngermanJ,MeldrumS.Jailmanagementofarrestees/inmatesenrolledincommunitymethadonemaintenanceprograms.JUrbanHealthBullNYAcadMed.2004;81(4):645-654.doi:10.1093/jurban/jth147.
2+

43
81. NunnA,ZallerN,DickmanS,TrimburC,NijhawanA,RichJD.MethadoneandbuprenorphineprescribingandreferralpracticesinUSprisonsystems:resultsfromanationwidesurvey.DrugAlcoholDepend.2009;105(1-2):83-88.doi:10.1016/j.drugalcdep.2009.06.015.
82. BinswangerIA,SternMF,DeyoRA,etal.Releasefromprison–ahighriskofdeathforformerinmates.NEnglJMed.2007;356(2):157-165.doi:10.1056/NEJMsa064115.
83. GreenTC,ClarkeJ,Brinkley-RubinsteinL,etal.PostincarcerationFatalOverdosesAfterImplementingMedicationsforAddictionTreatmentinaStatewideCorrectionalSystem.JAMAPsychiatry.February2018.doi:10.1001/jamapsychiatry.2017.4614
84. ZallerN,McKenzieM,FriedmannPD,GreenTC,McGowanS,RichJD.Initiationofbuprenorphineduringincarcerationandretentionintreatmentuponrelease.JSubstAbuseTreat.2013;45(2):222-226.doi:10.1016/j.jsat.2013.02.005.
85. WorldHealthOrganization.GuidelinesforthePsychosociallyAssistedPharmacologicalTreatmentofOpioidDependence.WorldHealthOrganization;2009.http://www.who.int/substance_abuse/publications/opioid_dependence_guidelines.pdf.AccessedMay11,2017.
86. FriedmannPD,WilsonD,KnudsenHK,etal.Effectofanorganizationallinkageinterventiononstaffperceptionsofmedication-assistedtreatmentandreferralintentionsincommunitycorrections.JSubstAbuseTreat.2015;50:50-58.doi:10.1016/j.jsat.2014.10.001.
87. GordonMS,KinlockTW,SchwartzRP,FitzgeraldTT,O’GradyKE,VocciFJ.Arandomizedcontrolledtrialofprison-initiatedbuprenorphine:prisonoutcomesandcommunitytreatmententry.DrugAlcoholDepend.2014;142:33-40.doi:10.1016/j.drugalcdep.2014.05.011.
88. LeeJD,FriedmannPD,BoneyTY,etal.Extended-releasenaltrexonetopreventrelapseamongopioiddependent,criminaljusticesysteminvolvedadults:rationaleanddesignofarandomizedcontrolledeffectivenesstrial.ContempClinTrials.2015;41:110-117.doi:10.1016/j.cct.2015.01.005.
89. MitchellSG,WilletJ,MonicoLB,etal.Communitycorrectionalagents’viewsofmedication-assistedtreatment:Examiningtheirinfluenceontreatment

44
referralsandcommunitysupervisionpractices.SubstAbuse.2016;37(1):127-133.doi:10.1080/08897077.2015.1129389.
90. BrownRT.Systematicreviewoftheimpactofadultdrug-treatmentcourts.TranslResJLabClinMed.2010;155(6):263-274.doi:10.1016/j.trsl.2010.03.001.
91. SubstanceAbuseandMentalHealthServicesAdministration.GrantstoExpandSubstanceAbuseTreatmentCapacityinAdultandFamilyDrugCourts:RequestforApplications(RFA)No.TI-15-002.2015.http://www.samhsa.gov/sites/default/files/grants/doc/ti-15-002.doc.
92. NationalInstituteonDrugAbuse.SubstanceAbuseintheMilitary.https://www.drugabuse.gov/publications/drugfacts/substance-abuse-in-military.PublishedMarch1,2013.AccessedMay11,2017.
93. ShipherdJC,StaffordJ,TannerLR.PredictingalcoholanddrugabuseinPersianGulfWarveterans:whatroledoPTSDsymptomsplay?AddictBehav.2005;30(3):595-599.doi:10.1016/j.addbeh.2004.07.004.
94. ToblinRL,QuartanaPJ,RiviereLA,WalperKC,HogeCW.ChronicpainandopioiduseinUSsoldiersaftercombatdeployment.JAMAInternMed.2014;174(8):1400-1401.doi:10.1001/jamainternmed.2014.2726.
95. U.S.DepartmentofVeteranAffairs.A/DoDClinicalPracticeGuidelinefortheManagementofSubstanceUseDisorders.2015.https://www.healthquality.va.gov/guidelines/MH/sud/VADoDSUDCPGRevised22216.pdfAccessedMay11,2017.
96. OlivaEM,TraftonJA,HarrisAHS,GordonAJ.TrendsinopioidagonisttherapyintheVeteransHealthAdministration:issupplykeepingupwithdemand?AmJDrugAlcoholAbuse.2013;39(2):103-107.doi:10.3109/00952990.2012.741167.
97. GordonAJ,KavanaghG,KrummM,etal.FacilitatorsandbarriersinimplementingbuprenorphineintheVeteransHealthAdministration.PsycholAddictBehavJSocPsycholAddictBehav.2011;25(2):215-224.doi:10.1037/a0022776.
98. U.S.DepartmentofDefense,OfficeoftheSecretary.TRICARE;MentalHealthandSubstanceUseDisorderTreatment.FederalRegister.https://www.federalregister.gov/documents/2016/09/02/2016-21125/tricare-

45
mental-health-and-substance-use-disorder-treatment.PublishedSeptember2,2016.AccessedMay11,2017.
99. EpsteinRA,BoboWV,MartinPR,etal.Increasingpregnancy-relateduseofprescribedopioidanalgesics.AnnEpidemiol.2013;23(8):498-503.doi:10.1016/j.annepidem.2013.05.017.
100. PatrickSW,DudleyJ,MartinPR,etal.Prescriptionopioidepidemicandinfantoutcomes.Pediatrics.2015;135(5):842-850.doi:10.1542/peds.2014-3299.
101. KaltenbachK,BerghellaV,FinneganL.Opioiddependenceduringpregnancy.Effectsandmanagement.ObstetGynecolClinNorthAm.1998;25(1):139-151.
102. TheAmericanCollegeofObstetriciansandGynecologists,TheAmericanSocietyofAddictionMedicine.OpioidUseandOpioidUseDisorderinPregnancy.TheAmericanCollegeofObstetriciansandGynecologists;2017.https://www.acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Obstetric-Practice/Opioid-Use-and-Opioid-Use-Disorder-in-Pregnancy.AccessedMarch30,2018.
103. Effectivemedicaltreatmentofopiateaddiction.NationalConsensusDevelopmentPanelonEffectiveMedicalTreatmentofOpiateAddiction.JAMA.1998;280(22):1936-1943.
104. SubstanceAbuseandMentalHealthServicesAdministration.Medication-AssistedTreatmentforOpioidAddictioninOpioidTreatmentPrograms.TreatmentImprovementProtocol(TIP)Series43.SubstanceAbuseandMentalHealthServicesAdministration;2005.https://www.ncbi.nlm.nih.gov/books/NBK64164/pdf/Bookshelf_NBK64164.pdf.AccessedMay11,2017.
105. BroglySB,SaiaKA,WalleyAY,DuHM,SebastianiP.Prenatalbuprenorphineversusmethadoneexposureandneonataloutcomes:systematicreviewandmeta-analysis.AmJEpidemiol.2014;180(7):673-686.doi:10.1093/aje/kwu190.
106. KandallSR,DoberczakTM,JantunenM,SteinJ.Themethadone-maintainedpregnancy.ClinPerinatol.1999;26(1):173-183.
107. JonesHE,KaltenbachK,HeilSH,etal.Neonatalabstinencesyndromeafter

46
methadoneorbuprenorphineexposure.NEnglJMed.2010;363(24):2320-2331.doi:10.1056/NEJMoa1005359.
108. McCarthyJJ,LeamonMH,WillitsNH,SaloR.Theeffectofmethadonedoseregimenonneonatalabstinencesyndrome.JAddictMed.2015;9(2):105-110.doi:10.1097/ADM.0000000000000099.
109. Fajemirokun-OdudeyiO,SinhaC,TuttyS,etal.Pregnancyoutcomeinwomenwhouseopiates.EurJObstetGynecolReprodBiol.2006;126(2):170-175.doi:10.1016/j.ejogrb.2005.08.010.
110. AgencyforHealthcareResearchandQuality.MeanExpensesperPersonwithCareforSelectedConditionsbyTypeofService:UnitedStates,2014.MedicalExpenditurePanelSurveyHouseholdComponentData.2016.https://meps.ahrq.gov/mepsweb/survey_comp/household.jsp.AccessedMay11,2017.
111. FlorenceCS,ZhouC,LuoF,XuL.TheEconomicBurdenofPrescriptionOpioidOverdose,Abuse,andDependenceintheUnitedStates,2013.MedCare.2016;54(10):901-906.doi:10.1097/MLR.0000000000000625.
112. JonesCM,LuriePG,ComptonWM.IncreaseinNaloxonePrescriptionsDispensedinUSRetailPharmaciesSince2013.AmJPublicHealth.2016;106(4):689-690.doi:10.2105/AJPH.2016.303062.
113. DavisCS,SouthwellJK,NiehausVR,WalleyAY,DaileyMW.Emergencymedicalservicesnaloxoneaccess:anationalsystematiclegalreview.AcadEmergMedOffJSocAcadEmergMed.2014;21(10):1173-1177.doi:10.1111/acem.12485.
114. RayB,O’DonnellD,KahreK.Policeofficerattitudestowardsintranasalnaloxonetraining.DrugAlcoholDepend.2015;146:107-110.doi:10.1016/j.drugalcdep.2014.10.026.
115. WalleyAY,XuanZ,HackmanHH,etal.OpioidoverdoseratesandimplementationofoverdoseeducationandnasalnaloxonedistributioninMassachusetts:interruptedtimeseriesanalysis.BMJ.2013;346:f174.
116. Doe-SimkinsM,QuinnE,XuanZ,etal.Overdoserescuesbytrainedanduntrainedparticipantsandchangeinopioiduseamongsubstance-usingparticipantsinoverdoseeducationandnaloxonedistributionprograms:aretrospectivecohortstudy.BMCPublicHealth.2014;14:297.

47
doi:10.1186/1471-2458-14-297.
117. EnteenL,BauerJ,McLeanR,etal.OverdosepreventionandnaloxoneprescriptionforopioidusersinSanFrancisco.JUrbanHealthBullNYAcadMed.2010;87(6):931-941.doi:10.1007/s11524-010-9495-8.
118. BeharE,SantosG-M,WheelerE,RoweC,CoffinPO.Briefoverdoseeducationissufficientfornaloxonedistributiontoopioidusers.DrugAlcoholDepend.2015;148:209-212.doi:10.1016/j.drugalcdep.2014.12.009.
119. CoffinPO,SullivanSD.Cost-effectivenessofdistributingnaloxonetoheroinusersforlayoverdosereversal.AnnInternMed.2013;158(1):1-9.doi:10.7326/0003-4819-158-1-201301010-00003.