Embed Size (px)
Citation preview

ToolkitforimplementingtheNamasteCareprogrammeforpeoplewithadvanceddementialivingincarehomes
MinStacpoole
DrAmandaThompsell
DrJoHockley
1
AcknowledgementsThetoolkitowesitsexistencetoProfessorJoyceSimardwhodevelopedtheNamasteCareprogrammeandinspiredusandmanyothersacrosstheworldtoworktoimprovethecareofpeoplewithadvanceddementiaattheendoftheirlives.Weoweagreatdebttoherworkwhichwehaveusedasabasisforthismanual.ProfessorLadislavVolicerwasatowerofstrengththroughoutourresearchstudyandhasmadevaluablecontributionstothistoolkit.WewouldalsoliketothankHelenScottwhowasimmenselyhelpfulineditingthetoolkit,andKimberlyStJohnwhocontributedtothe‘tools’.
CopyrightCopyright©StChristopher’s2016.ThistoolkithasbeenwrittentosupporttheintroductionoftheNamasteCareprogrammeandisfreetodownloadandreproduce.ThetoolkitiscopyrightandweaskthatyouacknowledgeStChristopher’swhenyouusethematerials.Publishedin2016byStChristopher’s,51-59LawrieParkRoad,LondonSE266DZwww.stchristophers.org.uk
2
Contents
IntroductiontotheNamasteCareprogramme 3
Section1:Advanceddementia 7
Section2:End-of-lifecareforpeoplewithdementia 12
Section3:Person-centredcareandtheNamasteCareprogramme 16
Section4:Leadingthechange 21
Section5:GettingreadyfortheNamasteCareprogramme 32
Section6:Communicatingwithrelatives:the‘familymeeting’ 37
Section7:TheNamasteCareprogramme 45
Section8:Achievingcomfortandpleasure 58
Section9:Developing,evaluatingandsustainingNamasteCare64
References 74
3
Introduction‘Youmatterbecauseyouareyouandyoumattertotheendofyourlife,andwewillhelpyounotonlytodiepeacefullybuttoliveuntilyoudie.’
DameCicelySaunders,founderofthemodernhospiceandpalliativecaremovementThistoolkitaimstohelpyouandyourcarehomeusetheNamasteCareprogrammetogive excellent care to your residentswith dementia, especially in the later stages oftheirillness.
Aswellasbeingkeptwellfed,cleanandcomfortable,peoplewithadvanceddementianeed to feel loved and they need to express themselves and be recognized asindividuals. They need care that enhances their quality of life. However, anAlzheimer’s Society survey found thatonly41%of relatives consider that their lovedoneswithdementialivingincarehomesenjoyagoodqualityoflife1.Peoplewithadvanceddementiabecomevery frail as thebrain shutsdownand theyoftenfinditdifficulttocommunicateandinteractwithotherpeople.Thismeansthatthey are no longer engaging in the conventional group activities of the care home.Care home staff can find it difficult to make the lives of residents with advanceddementia enjoyable and meaningful, despite their good intentions. People withadvanced dementia living in care homes sometimes spend long hours alone in theirrooms,orasleepinan‘activity’theycannolongertakepartin.InanotherAlzheimer’sSocietystudy2theaverageinteractionbetweenaresidentwithadvanceddementiaandcarehomestaff,notincludingtimespentingivingpersonalcareorhelpingwithmeals,
wasobservedtolastonlytwominutes.
TheNamasteCareprogrammeNamasteCareisastructuredprogramme,developedbyJoyceSimardintheUSA3,thatintegrates compassionate nursing care with individualised activities for people withadvanceddementiainagroupsetting.‘Namaste’isanIndiangreetingwhichmeans‘tohonour the spirit within’. The care programme is multi-dimensional, includingphysical,sensoryandemotionalelements. ThepurposeofNamasteCareistogivecomfortandpleasuretopeoplewithadvanceddementiathroughsensorystimulation,especiallytheuseoftouch.NamasteCareincreasesthelengthoftimethatcarehomestaff spend engaging and connecting with residents with advanced dementia andprovides a possible solution to meeting the sensory and emotional needs of theseresidents,andenrichingtheirqualityoflife.Theprogrammeisconductedsevendaysaweek,fortwohoursinthemorningandtwohours in the afternoon, but does not require additional staff, or space, or expensiveequipment. Namaste gives a structure to the ‘empty time’ when residents withadvanced dementia are not engaged in personal care or mealtimes. The NamastesessionsarerunbyaNamasteCareworkerwhoisamemberofthecarestaffteamand
4
aredeliveredinadesignatedplacewithinthecarehome,protectedfrominterruptionsandmadehomelyandattractive,sothatthereisacalmatmosphere.Thecoreelementsoftheprogrammeare:o ‘Honouringthespiritwithin’: theguidingprincipleofNamasteCare isarespectful
andcompassionateapproachtoindividualswithadvanceddementia.
o Thepresenceofothers:Namasteresidentsarebroughttogetherasasocialgroupwith a dedicatedNamaste Careworker, so each resident feels ‘included’ in theircommunity.
o Comfort and pain management: comfortable seating and painassessment/management are the essential first step towards enabling Namasteresidentstorelax,engageandexpresshowtheyfeel.
o Sensory stimulation: the programme incorporates stimulation of the five senses(touch,hearing,sight,smell,taste).Music,colour,therapeutictouchandmassage,aromatherapy oils and food treats are all part of themulti-sensory environmentcreatedintheNamasteroom.
o Meaningfulactivity:inNamaste,personalcareisprovidedasameaningfulactivity,eventhoughtheNamasteresidentswillusuallyhavehadtheirmorningwash.Thefocus is on pleasure rather than personal hygiene. Hands and face are gentlywashedwithawarmflannelandpatteddrywithasofttowel.Moisturisingcreamsare applied and the Namaste Care worker uses this opportunity to make eyecontact,andtalkaffirmativelywiththeresident.Handsandfacewashingispartofeveryone’slifeexperienceandusuallyresultsinasenseofwell-being.TheNamasteCareworkerwillexplore individualwishesandpreferencesandadaptactivitiestomeetpeople’sneeds.
o Lifestory:knowledgeoftheresident’slifestoryiskeytoadaptingtheprogramme
ofactivitiesandinterventionssothattheyaremeaningfulforeachperson.
o Food treats and hydration: the Namaste Care worker offers drinks and foodthroughout thesession (beingmindfulofanyswallowingdifficulties).Thiscreatesextra opportunities to improve hydration and nutrition and contribute to theresidents’healthandwell-being
o Careworkereducation:careworkersinvolvedinNamasterequireeducationaboutdementiaandallaspectsofthecareprogramme.Thecareworkersneedsupporttofeelconfident.
o Familymeetings: holding a familymeeting when a resident is going to start theNamasteCareprogrammecreatesa furtherbondbetweenthefamily/friendsandthe care staff, opening up the conversation about end-of-life care. Families areencouragedtotakepartintheNamastesessionswhentheyvisit.
5
o Careofthedyingandafter-deathcare:thecarethatresidentsenjoyintheNamaste
Care programme can be transferred to the bedroomwhen the person is unwell,andwhentheyaredying.
o Afterdeathreflection:dedicatingtimetorememberingaresidentaftertheirdeath
supports the care staff emotionally. Reflecting on what went well, and anydifficulties,providesanopportunityforcarestafftolearnfromtheexperienceandimprovethecaretheygivetoresidentswhentheyaredying.
None of these core elements are anything new in dementia care. However, what isdifferent is thatNamastebringspeoplewithadvanceddementia together ina singlecareprogrammethatprovidescompanyandstimulationonaregularbasis.St Christopher’s Hospice and the South London and Maudsley Trust evaluated theeffectsofNamasteCareonthequalityoflifeofpeoplewithadvanceddementiainfivecare homes in South London.We found that Namaste Care reduced the severity ofresidents’behaviouralsymptoms,suchasagitationandaggression,aswellaslethargy4.It also led to increased satisfactionamong familymemberswho foundvisitingeasierbecausetheirlovedonewasmorecontent.Thefamilyappreciatedtheeffortsthattheysaw care staff making to meet the needs of the person they love. Some familymembersjoinedinwithNamasteCarealongsidethecarehomestaff.Carehomestaffalsofoundtheprogrammerewardingandfeltmoresatisfiedwiththeirwork5.‘ThebiggestthingNamastehasgivenmeisadifferentfocuswhenvisitingmum.Formanyyearsnowmumhasn'tbeenabletocommunicatewithusandconversationhasbeenonesidedwhichisdifficultandattimessheappearedtobarelyrealiseIwasthere.Inowknowtodootherthingsaswellastalktomum,likeshowheroldphotos,brushherhair,feedhertreats,andmoisturiseherfaceandhands.ThismakesspendingtimewithhereasierandIfeelI'mmakingmoreofaconnectionwithherandadifferenceinherlife.’
(Emailfromthedaughterofaresident)
AimsofthetoolkitWewanttosharewhatwelearnedfromsettinguptheNamasteCareprogrammeinavarietyofUKcarehome,andsupportyouandothercarehomestofindnewwaysofworkingandprovidingcareforpeoplewithadvanceddementiathatmeetstheirpsycho-socialandspiritualneeds.WewanttoprovideapracticalguidetointroducingNamasteCareintoUKcarehomes.Thetoolkithasbeendesignedtohelpeveryoneworkingwithinthecarehome—(fromthecarehomemanagertothemaintenancestaff)—understandandsupporttheNamasteCareprogramme.Thewholeteamneedstobeinvolvedinmakingthecareprogrammeworkandeveryonecanenjoyjoiningin.
6
Wehopethatthetoolkitandtheaccompanyingworkshopwillenableyouto:
• UnderstandthepurposeoftheNamasteCareprogrammeanditsbenefitsforpeoplewithadvanceddementia,familiesandfriends,andcarehomestaff
• Communicatethevisiontothewholecarehometeam• Leadchangeinthewaythecarehometeamworkswithpeoplewithdementia
andtheirfamilies• IntroduceandestablishtheNamasteCareprogrammeinyourcarehome• DevelopastrategytoevaluateandsustaintheNamasteCareprogrammein
yourcarehome.
7
SectionOne
Advanceddementia
Sectionaim:
• Todescribetheadvancedstagesofdementiainordertohelpyou:o SelectresidentswhowillbenefitfromNamasteCareo UnderstandwhythisgroupofpeopleneedsNamasteCareo Recognisetheneedtoplanend-of-lifecareforresidents
withadvanceddementia
AdvanceddementiaDementia isanumbrellatermusedtodescribeanumberofdifferentdiseasesofthebrain, including Alzheimer’s disease, vascular dementia, mixed dementia, dementiawithLewybodies, fronto-temporaldementiaandmanyothers.Alzheimer’sdisease isthemostcommontypeofdementia.Itcausesabnormalfunctionandeventualdeathofselectednervecellsinthebrain5.Whilsttheprogressionofsymptomsisuniqueforeverypersonwithdementia,asthedisease progresses, people generally tend to lose memories, become immobile andcompletely dependent for all activities of living, and gradually are less able to usemeaningful speech. People with advanced dementia can also experience distressingsymptomsduetodepression,socialwithdrawal,agitation,resistivenesstocare(whichsometimesseemslikeaggressiontocarers),swallowingdifficulties,recurrentinfectionsandpneumonia6,7,8.Painisalsocommoninfrailolderpeoplewithdementiaandoftengoesunrecognized.This isbecausepeoplewithadvanceddementiaareoftenunabletelltheircarersthattheyareinpain9,10,11.Inthelaterstagesofthedisease,unlikeintheearlierstages,peoplewithdementiaarenotabletoparticipateactivelyinmostgroupactivities,e.g.aquizorasing-along.Theycanthereforebecomeincreasinglyisolatedwithinthecarehomeenvironmentbecausestaffareunsurehowtoengagetheminmeaningfulactivities12.
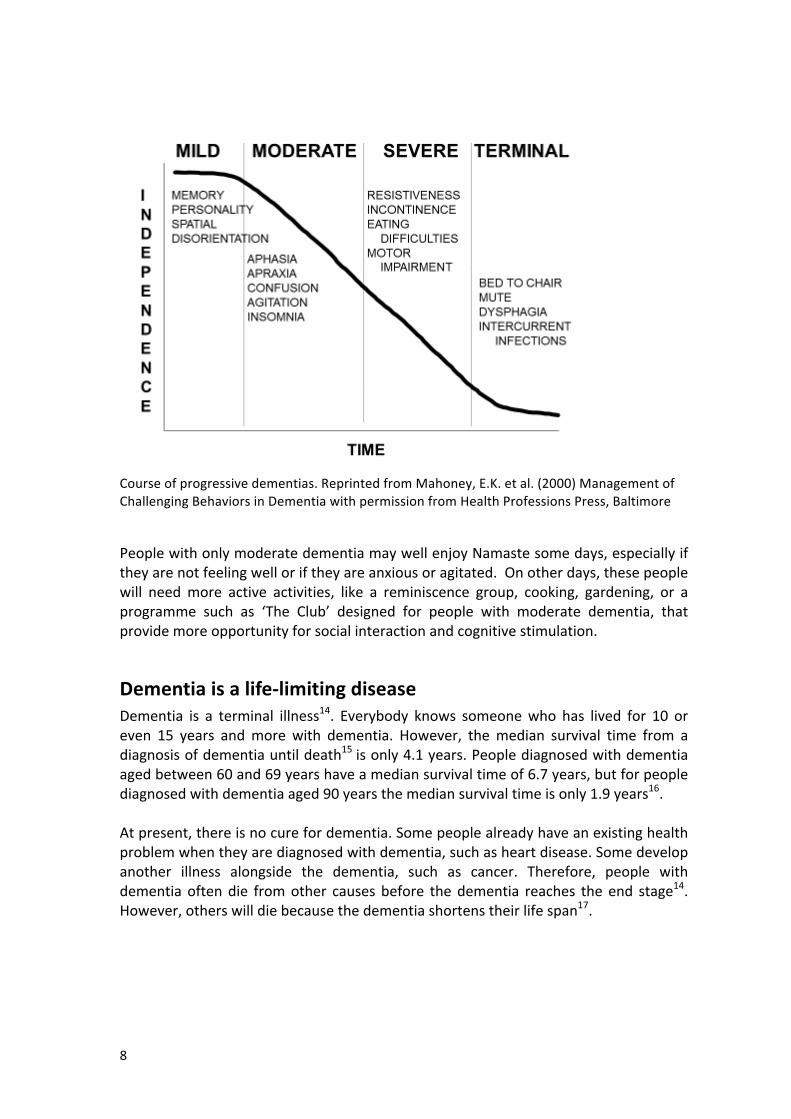
TrackingtheprogressofdementiaItisusefultotryandworkoutwhatabilitiesthepersonwithdementiahassothatyoucanworkouthowbesttoengagetheminactivitiesandenhancetheirqualityoflife.Asnoteverybodywithdementiaexperiencesthesamesymptomsorprogressesthroughthe disease at the same rate, there are assessment scales that can be used to helprecognisewhatstageapersonhasreachedintheirdementia,forexample,theClinicalDementiaRatingScale13.NamasteCarewillespeciallybenefitresidentswhohavereachedthestageofseveredementiaandterminaldementia.
8
Courseofprogressivedementias.ReprintedfromMahoney,E.K.etal.(2000)ManagementofChallengingBehaviorsinDementiawithpermissionfromHealthProfessionsPress,Baltimore
PeoplewithonlymoderatedementiamaywellenjoyNamastesomedays,especiallyiftheyarenotfeelingwelloriftheyareanxiousoragitated.Onotherdays,thesepeoplewill needmore active activities, like a reminiscence group, cooking, gardening, or aprogramme such as ‘The Club’ designed for people with moderate dementia, thatprovidemoreopportunityforsocialinteractionandcognitivestimulation.
Dementiaisalife-limitingdiseaseDementia is a terminal illness14. Everybody knows someonewho has lived for 10 oreven 15 years andmore with dementia. However, themedian survival time from adiagnosisofdementiauntildeath15 isonly4.1years.Peoplediagnosedwithdementiaagedbetween60and69yearshaveamediansurvivaltimeof6.7years,butforpeoplediagnosedwithdementiaaged90yearsthemediansurvivaltimeisonly1.9years16.Atpresent,thereisnocurefordementia.Somepeoplealreadyhaveanexistinghealthproblemwhentheyarediagnosedwithdementia,suchasheartdisease.Somedevelopanother illness alongside the dementia, such as cancer. Therefore, people withdementia oftendie fromother causes before thedementia reaches the end stage14.However,otherswilldiebecausethedementiashortenstheirlifespan17.
9
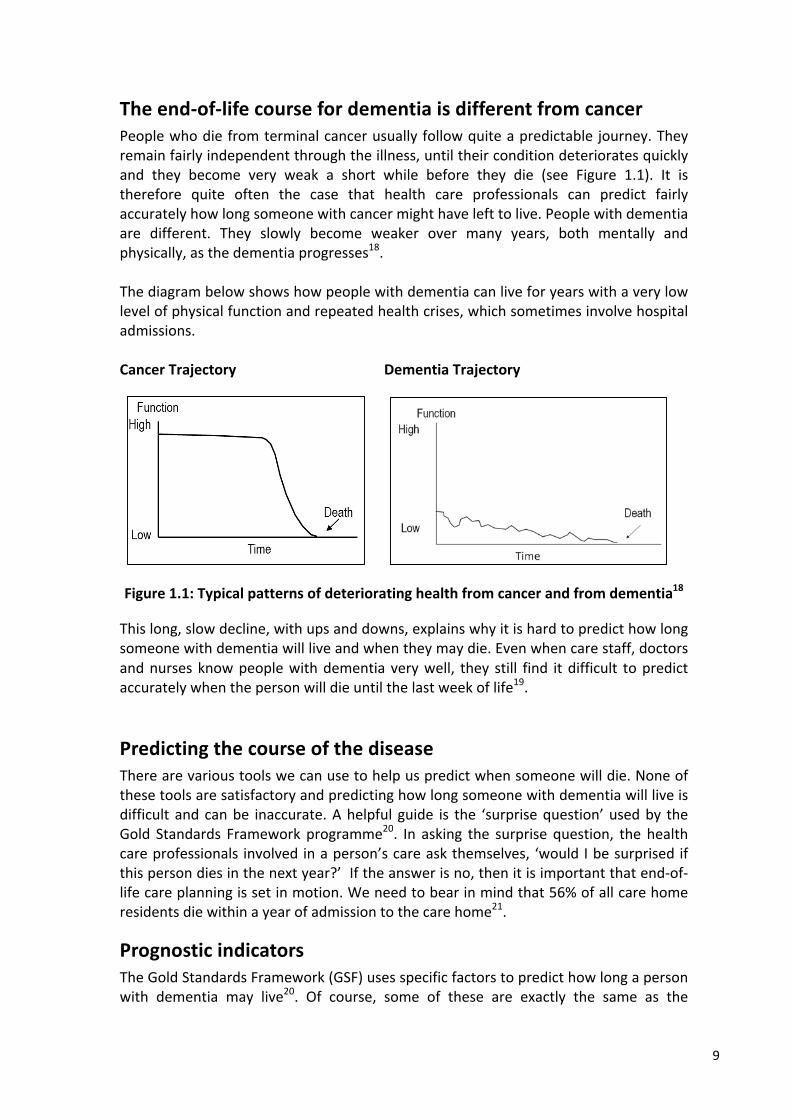
Theend-of-lifecoursefordementiaisdifferentfromcancerPeoplewhodiefromterminalcancerusuallyfollowquiteapredictable journey.Theyremainfairlyindependentthroughtheillness,untiltheirconditiondeterioratesquicklyand they become very weak a short while before they die (see Figure 1.1). It istherefore quite often the case that health care professionals can predict fairlyaccuratelyhowlongsomeonewithcancermighthavelefttolive.Peoplewithdementiaare different. They slowly become weaker over many years, both mentally andphysically,asthedementiaprogresses18.Thediagrambelowshowshowpeoplewithdementiacanliveforyearswithaverylowlevelofphysicalfunctionandrepeatedhealthcrises,whichsometimesinvolvehospitaladmissions.CancerTrajectoryDementiaTrajectory
Figure1.1:Typicalpatternsofdeterioratinghealthfromcancerandfromdementia18Thislong,slowdecline,withupsanddowns,explainswhyitishardtopredicthowlongsomeonewithdementiawillliveandwhentheymaydie.Evenwhencarestaff,doctorsandnursesknowpeoplewithdementia verywell, they still find itdifficult topredictaccuratelywhenthepersonwilldieuntilthelastweekoflife19.
PredictingthecourseofthediseaseTherearevarioustoolswecanusetohelpuspredictwhensomeonewilldie.Noneofthesetoolsaresatisfactoryandpredictinghowlongsomeonewithdementiawillliveisdifficult andcanbe inaccurate.Ahelpful guide is the ‘surprisequestion’usedby theGold Standards Framework programme20. In asking the surprise question, the healthcareprofessionals involvedinaperson’scareaskthemselves, ‘wouldIbesurprised ifthispersondiesinthenextyear?’Iftheanswerisno,thenitisimportantthatend-of-lifecareplanningissetinmotion.Weneedtobearinmindthat56%ofallcarehomeresidentsdiewithinayearofadmissiontothecarehome21.
PrognosticindicatorsTheGoldStandardsFramework(GSF)usesspecificfactorstopredicthowlongapersonwith dementia may live20. Of course, some of these are exactly the same as the
10
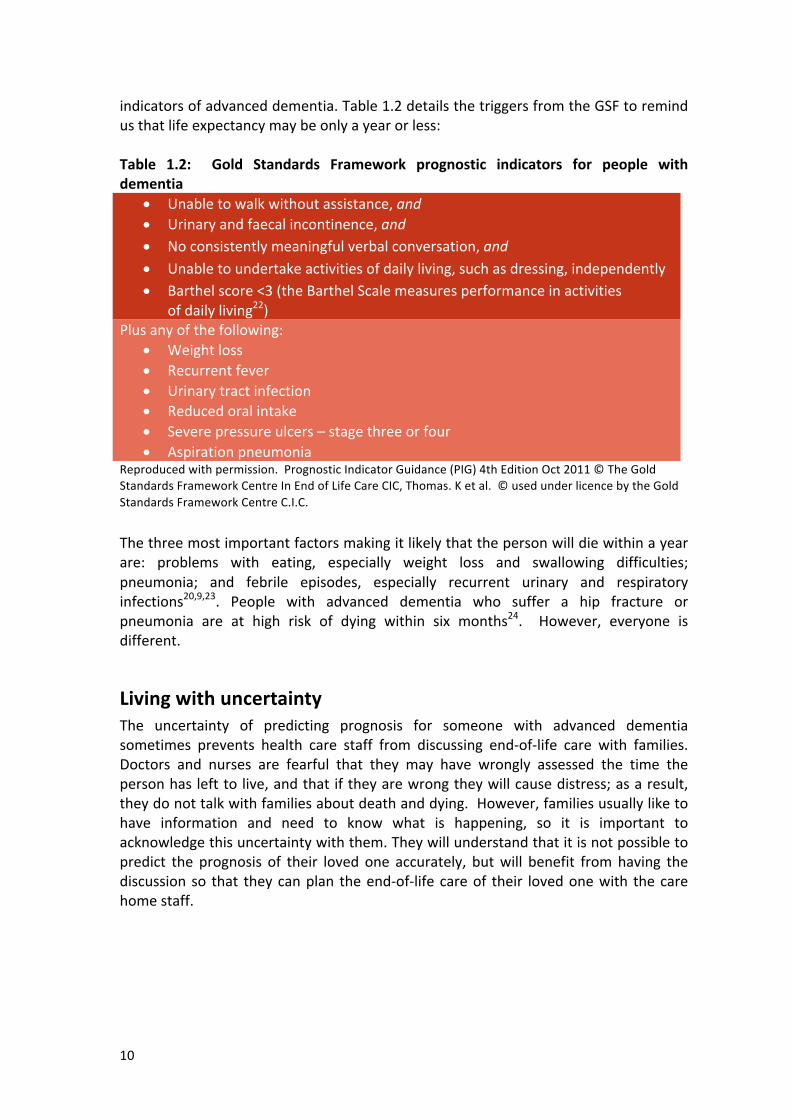
indicatorsofadvanceddementia.Table1.2detailsthetriggersfromtheGSFtoremindusthatlifeexpectancymaybeonlyayearorless:Table 1.2: Gold Standards Framework prognostic indicators for people withdementia
• Unabletowalkwithoutassistance,and• Urinaryandfaecalincontinence,and• Noconsistentlymeaningfulverbalconversation,and• Unabletoundertakeactivitiesofdailyliving,suchasdressing,independently• Barthelscore<3(theBarthelScalemeasuresperformanceinactivities
ofdailyliving22)Plusanyofthefollowing:
• Weightloss• Recurrentfever• Urinarytractinfection• Reducedoralintake• Severepressureulcers–stagethreeorfour• Aspirationpneumonia
Reproducedwithpermission.PrognosticIndicatorGuidance(PIG)4thEditionOct2011©TheGoldStandardsFrameworkCentreInEndofLifeCareCIC,Thomas.Ketal.©usedunderlicencebytheGoldStandardsFrameworkCentreC.I.C.Thethreemostimportantfactorsmakingitlikelythatthepersonwilldiewithinayearare: problems with eating, especially weight loss and swallowing difficulties;pneumonia; and febrile episodes, especially recurrent urinary and respiratoryinfections20,9,23. People with advanced dementia who suffer a hip fracture orpneumonia are at high risk of dying within six months24. However, everyone isdifferent.
LivingwithuncertaintyThe uncertainty of predicting prognosis for someone with advanced dementiasometimes prevents health care staff from discussing end-of-life care with families.Doctors and nurses are fearful that they may have wrongly assessed the time thepersonhaslefttolive,andthat iftheyarewrongtheywillcausedistress;asaresult,theydonottalkwithfamiliesaboutdeathanddying.However,familiesusuallyliketohave information and need to know what is happening, so it is important toacknowledgethisuncertaintywiththem.Theywillunderstandthatitisnotpossibletopredict the prognosis of their loved one accurately, butwill benefit fromhaving thediscussionso that theycanplan theend-of-life careof their lovedonewith thecarehomestaff.

11
Recognisingtheneedtoplanend-of-lifecareforresidentswhoarepartoftheNamasteCaregroupAll the peoplewith dementiawho benefit from theNamaste Care programme havereached the stage in theirdementiawhen it is important for the carehome tohavediscussionsaboutend-of-lifecarewiththefamilies.Itisalwaysaswelltoplanfortheworstandhopeforthebest.
12
SectionTwo
End-of-lifecareforpeoplewithdementia
Sectionaims:
• Todescribewhatismeantby‘agooddeath’• Toexplainwhyapalliativecareapproach isneededtocare forsomeonewith
advanceddementia
Thiswillhelpyou:
• Understand why preparing for end-of-life care is important for peoplewithdementia
• Provide information about end-of-life care thatwill be useful in theNamasteCarefamilymeetings
End-of-lifecareThe Government’s End of Life Care Strategy25 promotes good end-of-life care foreveryoneintheUK,includingpeoplewithdementia.TheStrategysuggeststhat,whileeveryoneisdifferent,formostofus‘agooddeath’willinvolve:
• Beingtreatedasanindividual,withdignityandrespect• Beingwithoutpainandothersymptoms• Beinginfamiliarsurroundings• Beinginthecompanyofclosefamilyand/orfriends.
The National Dementia Strategy6 set a goal that by 2014, anyone diagnosed withdementiawouldbeabletosay,‘Iexpectagooddeath.Iamconfidentthatmyend-of-lifewisheswillbemet’.
End-of-lifecareforpeoplewithdementiaSadly,peoplewithdementiaaremorelikelytohaveapoorexperienceofcareattheendoftheirlivesthanotherpeople.Thepresenthealthcaresystemisnotmeetingthechallengeofenablingpeoplewithdementiatodiewell.In2012,formercarers,currentcarersandpeoplewithdementiawereinterviewedbytheAlzheimer’sSocietytofindoutabouttheirexperienceofend-of-lifecare forpeoplewithdementia.Thereport26foundthatpeoplewithdementiaoftenexperiencepainandotherphysicaldiscomfortsduring the last stages of their illness. Many people with dementia die in hospitaldespitetheirownwishtodieathomeorintheircarehome.
13
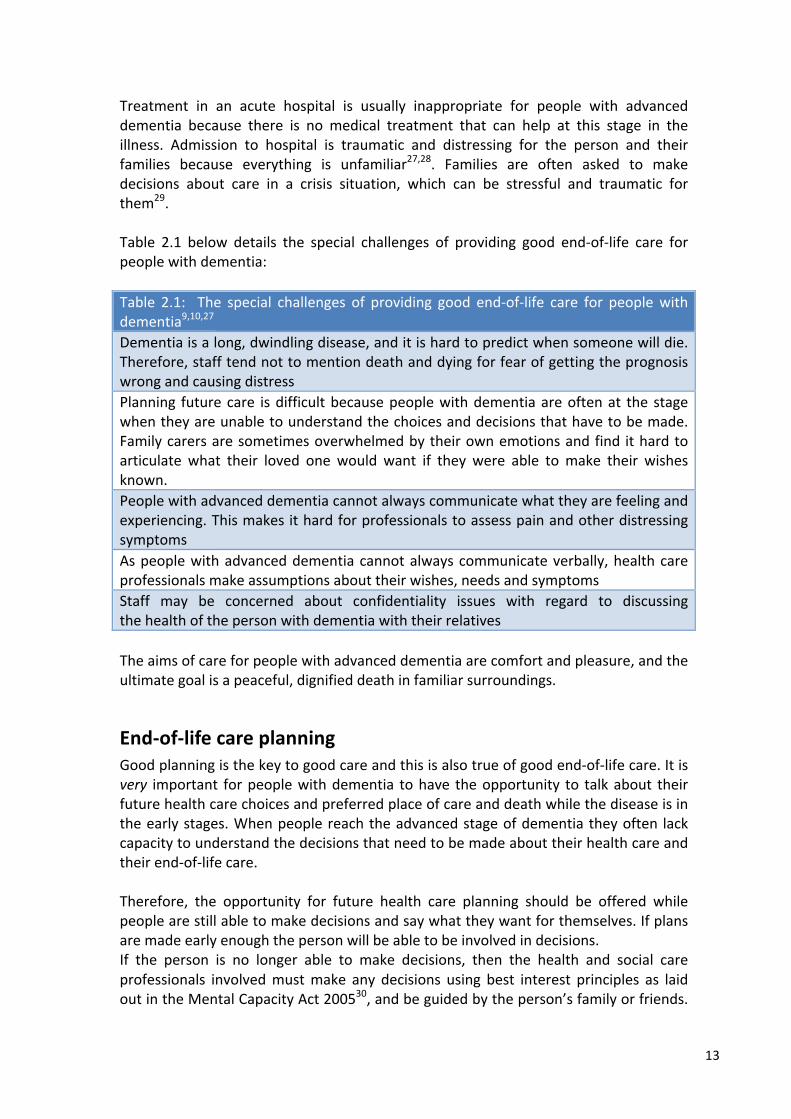
Treatment in an acute hospital is usually inappropriate for people with advanceddementia because there is no medical treatment that can help at this stage in theillness. Admission to hospital is traumatic and distressing for the person and theirfamilies because everything is unfamiliar27,28. Families are often asked to makedecisions about care in a crisis situation, which can be stressful and traumatic forthem29. Table 2.1 below details the special challenges of providing good end-of-life care forpeoplewithdementia:Table 2.1: The special challenges of providing good end-of-life care for peoplewithdementia9,10,27Dementiaisalong,dwindlingdisease,anditishardtopredictwhensomeonewilldie.Therefore,stafftendnottomentiondeathanddyingforfearofgettingtheprognosiswrongandcausingdistressPlanning futurecare isdifficultbecausepeoplewithdementiaareoftenat the stagewhentheyareunabletounderstandthechoicesanddecisionsthathavetobemade.Familycarersaresometimesoverwhelmedbytheirownemotionsandfind ithardtoarticulate what their loved one would want if they were able tomake their wishesknown.Peoplewithadvanceddementiacannotalwayscommunicatewhattheyarefeelingandexperiencing.ThismakesithardforprofessionalstoassesspainandotherdistressingsymptomsAspeoplewithadvanceddementiacannotalwayscommunicateverbally,healthcareprofessionalsmakeassumptionsabouttheirwishes,needsandsymptomsStaff may be concerned about confidentiality issues with regard to discussingthehealthofthepersonwithdementiawiththeirrelativesTheaimsofcareforpeoplewithadvanceddementiaarecomfortandpleasure,andtheultimategoalisapeaceful,dignifieddeathinfamiliarsurroundings.
End-of-lifecareplanningGoodplanningisthekeytogoodcareandthisisalsotrueofgoodend-of-lifecare.Itisvery important forpeoplewithdementia tohave theopportunity to talkabout theirfuturehealthcarechoicesandpreferredplaceofcareanddeathwhilethediseaseisintheearlystages.Whenpeoplereachtheadvancedstageofdementiatheyoften lackcapacitytounderstandthedecisionsthatneedtobemadeabouttheirhealthcareandtheirend-of-lifecare.Therefore, the opportunity for future health care planning should be offered whilepeoplearestillabletomakedecisionsandsaywhattheywantforthemselves.Ifplansaremadeearlyenoughthepersonwillbeabletobeinvolvedindecisions.If the person is no longer able to make decisions, then the health and social careprofessionals involvedmustmake any decisions using best interest principles as laidoutintheMentalCapacityAct200530,andbeguidedbytheperson’sfamilyorfriends.
14
TheMentalCapacityAct2005providesaframeworkfordecisionstobemadebyothersintheperson’sbestinterests.
TheWorldHealthOrganization’sdefinitionofpalliativecare
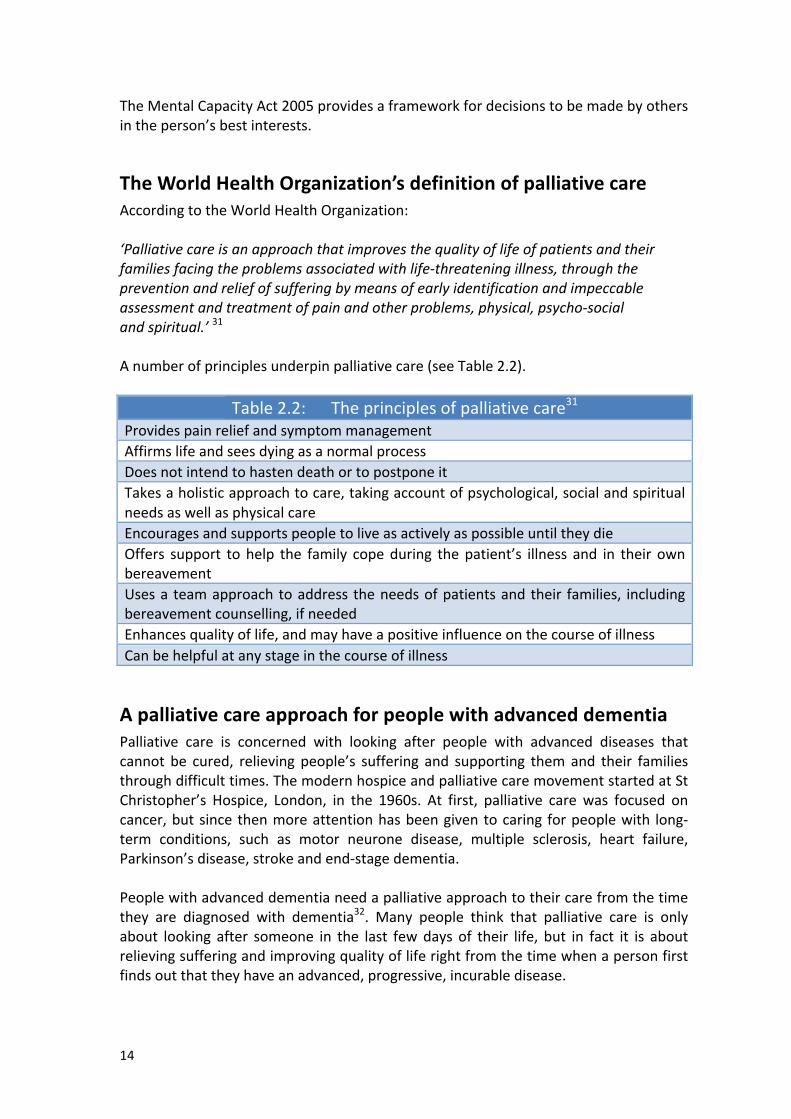
AccordingtotheWorldHealthOrganization:‘Palliativecareisanapproachthatimprovesthequalityoflifeofpatientsandtheirfamiliesfacingtheproblemsassociatedwithlife-threateningillness,throughthepreventionandreliefofsufferingbymeansofearlyidentificationandimpeccableassessmentandtreatmentofpainandotherproblems,physical,psycho-socialandspiritual.’31Anumberofprinciplesunderpinpalliativecare(seeTable2.2).
Table2.2:Theprinciplesofpalliativecare31ProvidespainreliefandsymptommanagementAffirmslifeandseesdyingasanormalprocessDoesnotintendtohastendeathortopostponeitTakesaholisticapproachtocare,takingaccountofpsychological,socialandspiritualneedsaswellasphysicalcareEncouragesandsupportspeopletoliveasactivelyaspossibleuntiltheydieOffers support tohelp the family copeduring thepatient’s illness and in their ownbereavementUsesa teamapproachtoaddress theneedsofpatientsandtheir families, includingbereavementcounselling,ifneededEnhancesqualityoflife,andmayhaveapositiveinfluenceonthecourseofillnessCanbehelpfulatanystageinthecourseofillness
ApalliativecareapproachforpeoplewithadvanceddementiaPalliative care is concerned with looking after people with advanced diseases thatcannot be cured, relieving people’s suffering and supporting themand their familiesthroughdifficulttimes.ThemodernhospiceandpalliativecaremovementstartedatStChristopher’s Hospice, London, in the 1960s. At first, palliative carewas focused oncancer,butsincethenmoreattentionhasbeengiventocaring forpeoplewith long-term conditions, such as motor neurone disease, multiple sclerosis, heart failure,Parkinson’sdisease,strokeandend-stagedementia.Peoplewithadvanceddementianeedapalliativeapproachtotheircarefromthetimethey are diagnosed with dementia32. Many people think that palliative care is onlyabout looking after someone in the last fewdays of their life, but in fact it is aboutrelievingsufferingandimprovingqualityofliferightfromthetimewhenapersonfirstfindsoutthattheyhaveanadvanced,progressive,incurabledisease.
15
Apalliativecareapproachincludesacceptingthatdementiaisalife-limitingillnessandmakingplanstoensurethatwhenthepersonisreadytodie,theydiecomfortablyandpeacefully33.ApalliativecareapproachtopeoplewithadvanceddementiaisaveryimportantpartoftheNamasteCareprogramme.
‘Howpeopledieremainsinthememoriesofthosewhoremainbehind’DameCicelySaunders,founderofthemodernhospiceandpalliativecaremovement.
16
SectionThree
Person-centredcareandtheNamasteCareprogramme
Sectionaims:
• Toconsiderthemotivationforhumanbehaviour• Todescribeperson-centredcare• Tooutlinethemostimportantemotional,spiritualandsocialneeds
ofpeoplewithdementia• ToshowhowtheNamasteCareprogrammecanhelpincorporatetheconcept
ofperson-centredcareintopractice.
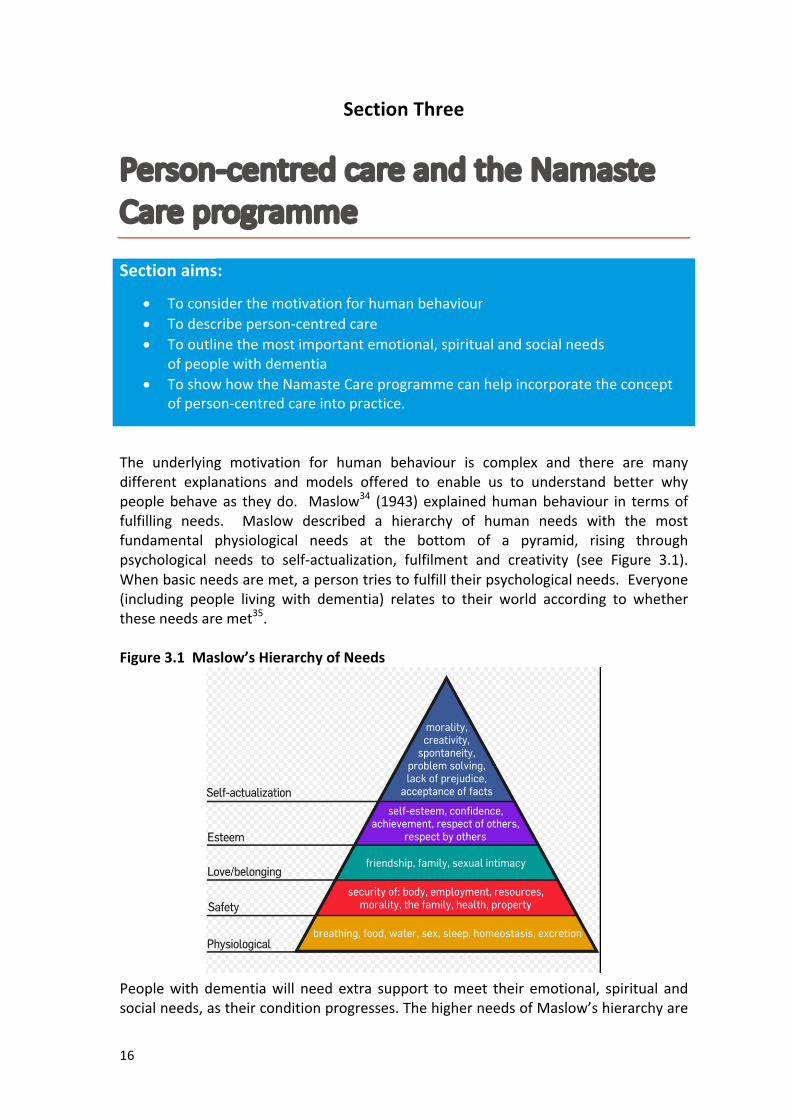
The underlying motivation for human behaviour is complex and there are manydifferent explanations and models offered to enable us to understand better whypeoplebehaveas theydo. Maslow34 (1943)explainedhumanbehaviour in termsoffulfilling needs. Maslow described a hierarchy of human needs with the mostfundamental physiological needs at the bottom of a pyramid, rising throughpsychological needs to self-actualization, fulfilment and creativity (see Figure 3.1).Whenbasicneedsaremet,apersontriestofulfilltheirpsychologicalneeds.Everyone(including people living with dementia) relates to their world according to whethertheseneedsaremet35.Figure3.1Maslow’sHierarchyofNeeds
Peoplewith dementiawill need extra support tomeet their emotional, spiritual andsocialneeds,astheirconditionprogresses.ThehigherneedsofMaslow’shierarchyare
17
similartothepsychologicalandsocialneedsidentifiedbyTomKitwood36inhisperson-centredphilosophyofdementiacare.Person-centredcare isaphilosophicalapproachtodementiacare,pioneeredbyTomKitwood36in1997,andremainsthefoundationforexcellentdementiacareintheUK.TheNationalInstituteforHealthandCareExcellence’s32qualitystandardfordementiacare recognises thataperson-centredapproach isessential todeliveringhigh-qualitycareforpeoplewithallstagesofdementia.Thissectionofthetoolkitsetsouttheprinciplesofperson-centredcareonwhichtheNamasteCareprogrammeisbased.
Person-centredcareWearealluniqueandeachoneofushasindividualcharacteristics,responses,feelings,thoughts,beliefsandexperiences.Thisiswhatgivesusoursenseof‘self’.Thesenseofselfisgenerallyequatedwiththeideaof‘personhood’.Person-centredcareseekstosupportandmaintain‘personhood’36.TheNamasteCareprogrammeismotivatedbytheintentionto‘honourthespiritwithin’thepersonwithdementia at the stagewhen they areno longer able to communicate their thoughtsand feelings. ‘Honouring the spirit within’ mirrors Kitwood’s philosophy of person-centredcare.Dementiacanundermineaperson’ssenseofself,whichinturncanlowertheirsenseofself-worth,andmakethemfeelthattheyareaburden37.Someoftheproblemswithdementiaare createdbyotherpeopleand thenegativeways inwhich theyperceivethepersonwithdementia.Kitwooddescribedthenegativewaysinwhichotherpeople(howeverunwittingly)candemoraliseapersonwithdementiaandcausethemtobecomesociallyexcluded.Thenegativeelementsofthis‘malignantsocialpsychology’canbeseeninTable3.1below
Table3.1:Theelementsof‘malignantsocialpsychology’36
Disempowerment ObjectificationInfantilisation IgnoringIntimidation ImpositionLabelling WithholdingStigmatisation AccusationOutpacing DisruptionInvalidation DisparagementBanishment Treachery
18
JoyceSimard,thecreatorofNamasteCare,wrote:v Elizabethis84yearsold.
ShehaslivedwithAlzheimer’sdiseaseforthepasteightyears.Shenolongerwalks,sometimesshemakessoundsbutmostofherdayisspentinbed;shebecomesinvisible.
v Johnhasdementiaandis‘parked’infrontofthenurse’sstationforhoursatatime.Heoccasionallycriesoutbutnoonecanunderstandwhy.Ifhecannotbecalmed,heisputbackinhisroom;hebecomesinvisible.
v Emma,JuliaandHarryareunabletoparticipateactivelyinanyoftheactivityprogrammesoffered.Theyaretakentoa‘dayroom’wheretheystareblanklyatatelevisionset;theyaresilentandbecomeinvisibleasstaffrushtohelpmorevocalresidents.
Residentslikethesearetypicalofthousandsofnursinghomeresidentswithadvanceddementiawhoarewellcaredformedically,givenmedication,vitalstaken,groomed,changed,fedandbathed.Isthisqualityoflife?Arewemeetingspiritualandsocialneeds?Areweprovidingmeaningfulactivitiesforthepersonwithadvanceddementia?Whoislisteningtotheirsilentcries?
Takenfrom:Simard38(2007)Kitwood36 outlined approaches that enhance ‘personhood’, namely ‘positive personwork’(seeTable3.2).Theelementsof‘positivepersonwork’areasfollows:Table3.2:Coreelementof‘positivepersonwork’
Experienceofthepersonwithdementia36
Recognition Experiencesasenseof‘belonging’Negotiation FeelingofbeingincontrolCollaboration FeelingofbeinginpartnershipwithothersPlay Imaginativeexpression.Recognitionofthe‘innerchild’.Sensoryexploration Opportunitytoexploreself-awarenessandself-discovery
throughsensoryexperiencesCelebration Celebratingspecialoccasions,butalsocelebratingevery
moment,experiencingjoywithothersRelaxation Nosenseofbodytensionandasenseofsafety
andsecurityValidation Theperson’sfeelingsareacknowledgedandhonouredHolding Feelingofbeingsafe,secureandsupportedGiving Experienceofvalueandworthinanenvironmenttowhich
thepersonisacontributorFacilitation OpportunitiesforpersonalgrowthCreation Opportunityandabilitytoexpressselfcreativelythrough
actionsandemotions
19
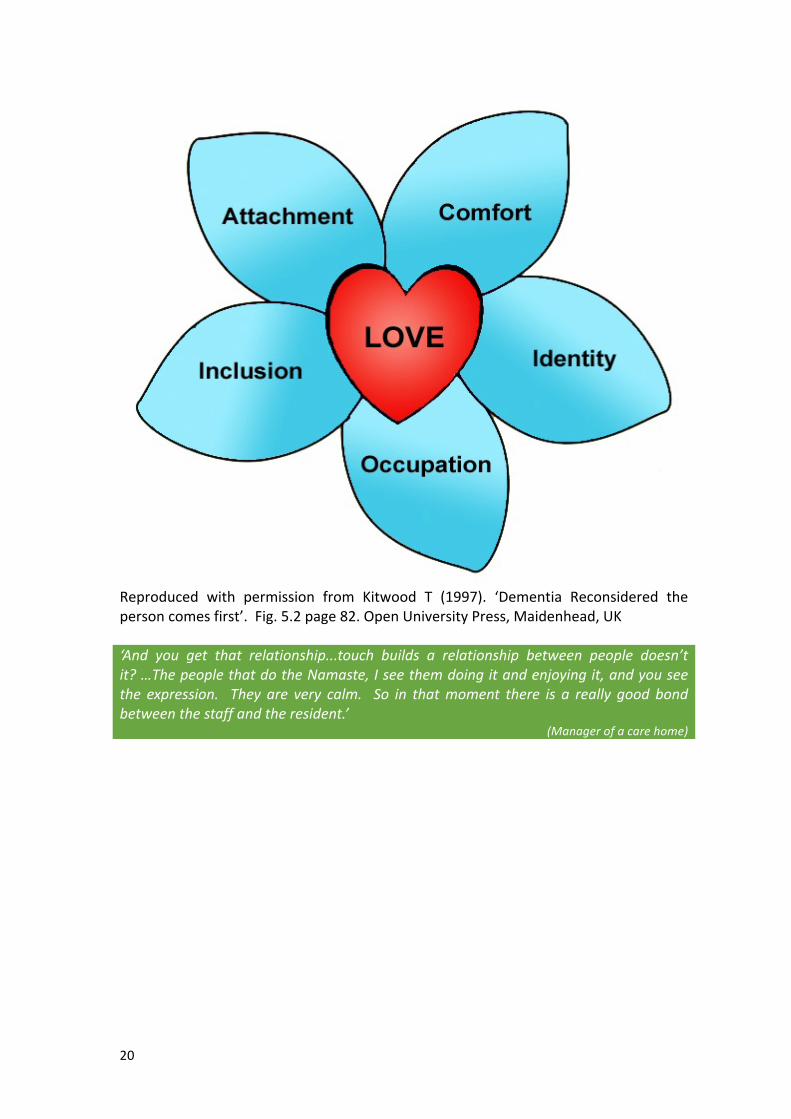
TomKitwood’sfundamentalbeliefwasthatpeoplewithdementianeedtofeelasenseofcontrolandpurpose,andthatwhenwereachoutsomebodywillbethere36.AccordingtoTomKitwood,peoplewithdementianeed:
• Attachment:tofeellovedandsafe• Comfort:tobephysicallyandmentallyrelaxedandnottobeinpain• Identity:toberespectedasauniqueindividualandhaveasenseofself-worth• Occupation:tousetheirtimemeaningfullyandnottobebored• Inclusion:tohavecompanionshipandfeelpartoftheworld,nottobelonelyor
excluded.Unlessthesefundamentalneedsaremet,itisimpossibleforpeoplewithdementiatofunctionasaperson.Person-centred care is about seeing the ‘ME’ in deMEntia36. Good dementia careinvolves loving-kindness. It isabout thepersonwithdementiahavingan identityandbeing understood. In order to give ‘loving-kindness’ you need to get to know thepersonbehindthedementiabyfindingoutabouttheir lifestory.Whentheperson isknown,theirbehaviourcanbeunderstoodmoreeasilyandthecareworkerwillbeabletoformrelationshipswiththepersonmoreeasily36,39.NamasteCarehasbeenstructuredtomeetthehumanneeds identifiedbyKitwood’s‘Flower of Need’36 (see Figure 3.2) - attachment, comfort, identity, occupation andinclusion.Itisawayofsupportingandstimulatingstafftoprovideperson-centredcareand engage in ‘positive person work’ with people with advanced dementia in carehomes.‘Themainpsychologicalneedsofpeoplewithdementia’.Peoplewithadvanceddementiaoftenfeelbored,lonelyandhelplessasaresultoftheeffectsoftheirillness.Theyneedtofeelthattheyarepartofthedailylifeofthecarehomeandthat theyhaverelationshipswiththecarehomestaff40.Namastecanhelpcarehomesgiveresidentswithadvanceddementia,whoaresociallywithdrawnandnolongerabletobenefitfromgroupactivities,apositiveexperienceofcare.Atthesametime,theprogrammecanhelpbuildcloserrelationshipswithfamilymembers,whocanalsobeinvolvedintheNamasteCaresessions3.
20
Reproduced with permission from Kitwood T (1997). ‘Dementia Reconsidered thepersoncomesfirst’.Fig.5.2page82.OpenUniversityPress,Maidenhead,UK‘And you get that relationship...touch builds a relationship between people doesn’tit?…ThepeoplethatdotheNamaste,Iseethemdoingitandenjoyingit,andyouseethe expression. They are very calm. So in thatmoment there is a really good bondbetweenthestaffandtheresident.’
(Managerofacarehome)
21
SectionFour
Leadingthechange
Sectionaims:
• TohighlighttheimportanceofmanagerialsupportandleadershiptothesuccessfulimplementationoftheNamasteCareprogramme
• TodescribetherolesoftheNamasteCarecoreteammembers• ToexplaintheimportanceofteamworkfortheNamasteCareprogramme• ToshowthatNamasteCaredoesnotrequireextrastafforspace,butanewwayof
working
TheNamaste Care programme and this toolkit are based on best practice dementiacareandbestpracticeend-of-lifecare.TheNamasteCareprogrammedoesnotrequireextrastaff,orspaceorexpensiveequipment.However,itdoesmeanchangingthewayinwhicheverybodywithin thecarehomeworks.Tomake thechangehappen, thereneedstobewillingnesstochange.Changerequiresgoodleadershipandteamwork.
LeadershipThecarehomemanagerandseniormanagement(e.g.regionalmanagers,thecompanydirectors,ortheowners)needtoshowcommitmenttointroducingNamasteCareandprovidingthebestpossiblequalityof lifeforresidents. Everyoneworking inthecarehomeneeds toknowthat theorganisation is committed to introducing theNamasteCareprogrammeforthebenefitoftheirresidents.The manager/clinical lead needs to be highly involved during both the preparationphaseandthefirstweeksofsettingupthecareprogramme.ItisimportanttosettimeasideandmaketheNamasteCareprogrammeapriority.Unless there is commitment fromeverybodyat all levels there is a real risk that theNamasteCareprogrammewillnothappentwiceadaysevendaysaweek.Strongandeffectiveleadershipisneededtoestablishtheprogrammeandsustainthechangeovertime.
ChoosingtheNamasteCarecoreteamThemanagermustchoosetwoorthreeindividualswhoareenthusedbyNamasteandexperienced and committed to dementia care. These individuals will run the dailyNamasteCareprogrammeandprovideleadershipatgroundlevelforthecarestaff.Thecore teammembers couldbenursesor careworkers, but theymustbepeoplewhocommandtherespectofthecarestaff.Coreteammemberscouldbecalled‘Namaste
22
Champions’,andwillbeinvolvedwithplanningandorganisingthecareprogrammeateverystage.ThecoreteamneedstobestaffmemberswhoWANTtodothiswork,asopposedtojustbeingtoldtodoit!
Everybodyneedstobe‘onboard’For Namaste Care to be introduced successfully, everyone in the care home mustunderstand why the Namaste Care programme is being introduced and see thebenefitsthatNamasteCarecanbringtoresidentsandthecarehome.Inourevaluation,wefoundthat‘topdown’decisionsmadebymanagerswereunlikelytobringaboutchangeunlessallthemembersoftheteamwereonboard.Theenergytomakethechangehappenneededtocomefromboththetopandthebottomoftheorganisation4.ThismeansexplainingtheNamasteCareprogrammetoeveryoneworking inthecarehome right from the start. Table 4.1 details what ALL staff need to know aboutNamasteCare.Table 4.1: What everyone needs to know about the Namaste Careprogramme
• Theoverallaimistoprovidequalityoflifetotheendoflifeforresidentswithadvanceddementia
• NamasteCarefocusesonmeetingtheemotionalandsocialneedsofthepeoplewhoaremostdisabledbydementia
• NamasteCareisbasedaroundsensoryexperience:music,massage,colour,tasteandscents
• Dementiaisaterminalillnessandacutehospitalcarehaslittletoofferpeopleinthelaterstagesofdementiawhoarebestcaredforinthecarehome
• Forpeoplewithadvanceddementiatheaimsoftheirtreatmentarecomfortandpleasureandthefinalgoalofcareisapeacefuldignifieddeathinthecarehome
• NamasteCaredependsupontheinvolvementandcommitmentofeverymemberofthecarehometeam.
CommunicatingthevisionWithinthecarehomeIn the first weeks of the programme, the most important goal of the care homemanager/clinicalleadistowinthe‘heartsandminds’ofthecarestaff.Itisvitalthatallmembersofthecarestaffandthewidercarehometeamunderstandwhatisplannedandhowresidentswillbenefit(seeTable4.2).
23
Table4.2:BenefitsofNamasteCareforresidents4
Inourresearchstudy,wefoundthatresidentstakingpartintheNamasteCareprogramme:ExperiencedanoverallreductionintheseverityofbehaviouralsymptomswhichwassustainedovertimeWerestimulatedtobemorealertandresponsive,andengagedmoreactivelywithothersWererelaxedandbecamelessagitatedastheyexperiencedacalmeratmosphereandapproachtocareEnjoyeddifferentelementsofthecareprogramme,e.g.massage,music,birdsong,life-likedollsoranimals,foodtreatsandimprovedhydrationetc.Hadregular,structured,one-to-onetimewithacareworkerandwereofferedtherapeutictouchandtheopportunitytoconnectandcommunicateandexpressemotion.Severalresidentswhoscarcelyspokebecamemoreverbal.
Anexampleofapositiveexperienceisthat, inonecarehome,onthefirstdayoftheNamaste Care programme, a daughter satwith hermother and gently rubbed handcreamintohermother’shand.Weturnedroundandfoundthedaughterintears.Weaskedheranxiouslywhyshewasupset,andshesaid,‘Mumjuststrokedmyhandback,and that’s the first time she has done somethingmotherly forme for ever somanyyears’.
ReluctanceandresistanceInitially,carestaffmayfind itdifficult toacceptchange,ortobelieve it ispossibletoimplementtheNamasteCareprogrammeinthecarehome.Issuessuchasnothavingenough resources, time, staff or space need to be addressed from the start. Bepreparedforcarestafftosay:• “ThereisnotenoughtimetodoNamaste,wearetoobusy”–thesamenumberof
carestaffarelookingafterthesamenumberofpeople,sothisisnotmorework.• “There is already toomuch work without bringing in anything new” –Namaste
meetstheresidents’needs,andthatisourwork.• “This isnothingnew”– that is true,butwhat isnew is to focusonpeoplemost
disabled by dementia, bringing them together as a group and giving themstructuredengagement/activity• “We are doing all this already” –Are you really? Think of one of your own
residentsreflectonwhattheydothroughtheday.• “The activity co-ordinators should be doing this” – Activity co-ordinators
cannot provide individualised activity for everyone in the care home single-handed! Engagingresidents inactivities is theroleofALLstaff. Activityco-ordinatorscanbeawonderfulresourceandsourceofsupportfortheNamastecareworkersalongsidethisotherwork.
• “We give wonderful care anyway” – does your wonderful care include thisgroupofresidents?Whatexactlyareyoudoingforthem?
24
Thenursesmaysay:
• “This is not clinical care” – but aNamaste session will provide informationaboutwhetheranindividualis inpain,whethertheyareeatinganddrinkingnormally,anunderstandingoftheirmoodandbehaviourandconsciouslevel.Thisinformationisclinicallyimportant.
• “We have too many responsibilities to get involved with Namaste” – theresidents’well-beingisaprimaryresponsibility.
• “Namaste is the job of the careworkers”–without support from thenursesNamasteislikelytofail
• “Itwillbeveryexpensive”–youwillseefromthepagesbelowthatNamasteisaffordable.
None of these negative statements are true and they should be challengedimmediately,becauseactive support fromeverybody in thecarehome isneeded forNamasteCaretoflourish.Ifpossible,tryandtakescepticalstafftoseeNamasteCarein action in another care home because ‘seeing is believing’ and they may becomepowerfulchampions.This toolkit aims to provide answers to the common objections of staff to NamasteCare.
Anexercisetogetpeopleonboard
It isusefultoreflecton individualresidents inyourcarehome,anddiscusswithstaffwhat theyaredoingat themoment toenhancetheseresidents’qualityof life.Thinkaboutwhethermorecouldbeachieved ifNamasteCare is implementedandthere isstructuredtimetofocusonengagementandpleasurableactivity.
Seeingisbelieving
IfyoucanarrangeavisitforthecoreteamandkeystafftoanotherhomethatisalreadyrunningaNamasteCareprogramme,youwillfindthatstaffwilllatchontotheideamorequickly.Encouragingstafftocontributeideaswillhelptoengagethemwiththeproject.Carehomesarefulloftalentedandcreativepeople.Onceyoustart theprogrammeandstaffmembersseethebenefits for residentsandfeelthebenefitsforthemselves,thenmanyofthedifficultieswillstarttomeltaway.Below (see Box 4.1) are comments made by participants having implemented theNamasteCareprogramme.
25
Box4.1:Commentsmadebyparticipantsinourresearchstudy4
‘Ithinkitdoesmakeadifference,especiallywhenyourubthecreamintotheirhandsandthat.Theyseemto,Heatherseemstocomealive,kindof,shewakesup.’
(Husband)‘Youwashandbaththem,dressthem.ButbeinginNamaste,you’reactually,onceyoudothemassageontheirhandsandfeet,thepatientopeningtheirhandsandyoucanactuallyseethepalmoftheirhands;itmakesyoufeel,“God,it’sthefirsttimeI’veactuallyseenthepalmofthisperson’shand.’
(Nurse)‘Phyllishasneversmiled,Iworkherefor16yearsandshehadneversmiled.She’salwaysbeenaseriousperson,nevergetsmilefromPhyllis.NoweverythingyousaytoPhyllis,is“Hee,hee,hee”.She’slaughing,she’shappy.’
(Careworker)‘Frommymother’spointofview,andpeopleatthatlevel,Ithinkithasbeenwonderful.Sheismuchmorehealthynow.Idon’tknowwhy,butsheisdifferent.Sheismorealiveeventhoughshecan’tdoanythingforherselfatall.’
(Daughter)‘Andtheywerejustsittingthere.Whenyouseetheireyes,bytouchingandthefivesenses,theyarelightingupandtheylookwell.Tolookatthem,theyreallylookwell.Evenveryillpatientsarelookingmuchbetter.’
(Nurse)
WinningoverthewidercarehometeamActivityorganiserswillhaveakeyroleinsupportingcarestafftoruntheNamasteCareprogramme,buteveryoneemployedbythecarehomeneedstoplayaroleinNamaste.Kitchen, laundry,maintenanceandadministrative staffoftenhaveclose relationshipswithresidents.TheyneedtoknowthattheywillplayapracticalpartinsupportingtheNamaste Care programme and bringing a better quality of life to residents withadvanceddementia.EveryoneinthecarehomeneedstoknowthattheircontributiontotheNamasteCareprogrammeisvalued.
FamiliesandfriendsIntroducingNamasteCarewillinevitablychangethewaythecarehomeworks.Itisbestpracticetoinvolverelativesinanychangeswhichmayaffecttheirfamilymember.Astheroutineofthecarehomechangesitishelpfultohavetheunderstandingandco-operationoffamiliesandfriends.Itisthereforeimportanttoholdarelatives’meetingtoexplaintheNamastecareprogrammetoallrelatives,notonlythosewhohaveafamilymemberlikelytobenefitfromthecareprogramme.
Itisalsoimportantthatwhenfamilymemberscometovisit,theyknowtheyarewelcometobepartofNamaste,andiftheyfeelcomfortablecombingthehairofthe
26
persontheycarefor,orofferingahandmassageoradrinktheyareinvitedtodothosethings.IftheywishtotaketheirlovedoneoutoftheNamasteroomandvisitawayfromthegroupactivitytheyarewelcometodothis.
Trytoenlistthehelpandsupportofrelativesfromtheoutset.
Themulti-professionalteamandcarehomevisitorsEveryone who visits the care home professionally needs to understand the changesthat are being introduced and the reasons for introducing the Namaste Careprogramme, e.g. the GP, communitymental health team, community palliative careteam, local ministers of religion and volunteers. Ideally, it is best to talk about theprogrammeinperson.However, itmaybethata letteroremail istheeasiestwaytocommunicatewiththemall.It is vital that everyone (care staff, family members, visiting professionals e.g. GP)understandstheNamasteCareprogrammesothattheycansupportyourwork.
ChoosingtherighttimetostartThecarehomeneeds tobe ready forchange. Themanagerandcarestaffmembersneed to feel confident that they are already giving their residents good health andsocial care. Theyhave to feel ready to takeon the challengeof findingnewwaysofworking thatwill helppeoplewith advanceddementia to connectmore closelywithothersandexperiencecomfortandpleasureeveryday.When implementing the Namaste Care programme, staffing levels should be at anormallevelforthecarehome.Ifyourcarehomeisunder-staffed,orifyourstaffareintheprocessof introducinganotherimprovementincare, itwillbedifficulttobringabout the necessary changes in order to implement the Namaste Care programmeproperly.It isnotagood idea tostartNamasteCarewhileothermajororganisationalchangesare going on. It is also not a good idea to start over a holiday period when staffmembers are likely to be away and there is less time to build up continuity.Managementsupportiscrucial,especiallyinthefirstfewweekswhiletheprogrammeisestablished. Ifcarestaffarenotengagingwiththeproject it isworthdelayingandtakingtimetogaintheirsupport,becausecommitmentfromeverybodyisthesecretofsuccess.Make sure care staff knowwhatdocumentation youhave chosenand feel confidentusing it. In particular care staff need to be confident in actually undertaking a painassessmentandusingapainassessmenttool(seeSectionEight).Ifyouhavepaintedaroom,makesurethesmellofpainthasgonebeforeyoubringtheresidentsinforNamaste.
27
Make sure thecore teamand thekey leaderswithin thehomeareworkingallweekwhenyoustartyourNamasteCareprogramme.
UsingtimedifferentlyRe-organisingstaffingtomaketimeforNamasteCare
Withinmostcarehomes,onanyparticularday,careworkershaveanassignmentof4–8 people at different stages of dementia with different needs and levels ofdependency.WhenyouarerunningaNamasteCareprogramme,theallocationofstaffto residents remains the same in themorning until the residents have been helpedwiththeirpersonalcareneedsandhavehadbreakfast.Allhandsondeck–helpingresidentsgettoNamasteOncemost residents have had their breakfast andmorningwash, then theNamasteCareworker for the shift goes to setup theNamaste room.Once the room is readyshe/he tells colleagues that Namaste is open. The next fifteen minutes are veryimportantbecauseeveryavailableperson, includingthemanagerandthecleaners, isneeded tohelpbring theNamaste residents to the room.TheNamasteCareworkerwill be there to greet residents as they arrive. This ensures that each individual isrecognizedwithrespectandaffectionatthestartofthesession.SharingtheworkForthenexttwohourstheNamasteCareworkerstaysintheNamasteroom,engagingwiththeNamasteresidents.TheNamastegroupconsistsofatleastthesamenumberof residents as the average care worker’s allocation, i.e. 4 – 8. The difference fromusualcareisthattheNamasteCareworkerisnowcaringforagroupofpeoplewhoareall in the later stages of dementia. Sometimes theNamaste Careworker looks aftermore residents than theaverageallocation,because theNamasteCare residents aregenerally immobile,andsomeofthemwillbeasleepattimes. InmostNamastecarehomes, the other care workers and nurses enjoy coming into the Namaste roombecause they find the atmosphere pleasant and relaxing, and they enjoy interactingwithresidents.Meanwhile, other care staff remaining on the floor will continue working with theothermoreable residents,usuallyengaging them inactivities that suit theirphysicalandcognitiveabilities....We have found that care homemanagers organise staffing in several differentwayswhen implementing the Namaste Care programme. These are detailed in Box 4.2below.

28
GroupactivitiesforpeoplewithmoderatedementiaIdeally, at this timeofday,other groupactivities areprovided forpeoplewithmoremoderatedementia,egreminiscence,orcognitivestimulation,orgardeningetc..Thesesessionswillprobablybeorganisedbytheactivityco-ordinator.Inthiswaytherearetwosupervisedgroupsofresidentsonthefloor,andoneortworesidentswhomaybeunwell in their rooms and one or twowhomay choose not to be involved in eithergroup.InhomeswhereNamasteCareisofferedeachdaythereareveryfewresidentswhoarenotengagedinmeaningfulactivity.
LunchtimeWhentheprogrammeclosesbeforelunch,thecarestaffareallneededagaintobringtheNamasteCareresidentsoutoftheroomtobemadereadyforlunch.TheNamasteCareworker thanks each resident for attending the session and says goodbye, thenbriefly tidies up and joins the other care workers. The same numbers of staff arethereforeavailabletohelpwithtoiletingandlunch.TheNamasteroomre-opensafterlunch at 2 pm or 3 pm, according to the care home’s routine, and once again theNamaste Champion (this may be another member of staff now) looks after a fullassignmentof4-8residents.
Box4.2:DifferentwaysoforganisingstaffingfortheNamasteCareprogramme
v InsomecarehomestheNamasteChampionsruntheprogrammeeveryday.
Thishastheadvantageofcontinuity.However,othercareworkersneedtogainexperienceandskillstotakeoveriftheNamasteChampionisonholiday,orworkingnightsorsick.Also,weekendshavetobecoveredbecauseNamasteCareisasevendaysaweekprogramme.
7daysaweekand4hoursadayistheoptimalschedulefortheNamasteCareprogramme,butifyoucannotmanagethisatfirstyoushouldnotbeputoffstarting.Asacarehomeyouhavetodecideonthefrequencyyoucancommitto,andthenbuildtowardsafullprogramme.
v Inothercarehomes,carestafftakeitturnsrunningtheprogramme,onemaytaketheprogrammeinthemorningandanotherintheafternoon.IntheUSAthereisanassistedlivingorganisationwhereallstaffwantedtobeapartoftheprogramsotheyrotateevery30minutes!
v Eachcarehomemustworkoutwhatpatternworksbestforthemselves.
v Ideally,aprogrammeofgroupactivitiesforpeoplewithmoderatetoadvanceddementiaisrunningsimultaneouslywiththeNamasteCareprogramme.
29
SupportfromthewidercarehometeamInorder toachieve thebestpossiblecare for residentswithadvanceddementia, thecare homemanager needs to involve every team in the care home. Quality of caredependsoncleaners,kitchenstaff, laundryworkersandadministrationaswellastheclinical care staff who are directly involved in care (see Box 4.3). If all the teamscontributetotheprogrammethenanyextrawork involved isspreadrightacrosstheorganisation.
Box4.3:Sharingtheloadwiththewidercarehometeam
v Inonecarehometheactivityco-ordinatorsetuptheNamasteroomwhiletheNamasteCareworkerwentforabreakbeforebeginningthecareprogramme.
v InanothercarehomethenursesetuptheNamasteroomafterfinishing
themedicationroundsothattheNamasteCareworkercouldhaveabreakbeforestartingNamaste.
v Thekitchenstaffcanhelpbyputtingtogetheratrayortrolleyofdrinks,waterandachoiceofjuice,andpreparingfoodtreatsfortheNamasteprogramme,e.g.orangesegments,piecesofbanana,orpureedfruitsforpeoplewithswallowingdifficulties.TheNamastecoreteamcantalkwiththecookandthekitchenstafftocreatevarietyandchoice,e.g.onedayicecream,anotherdayyoghurtsmoothiesorcake.Thetypeoffoodwilldependuponeachresident’sswallowingability.
v Laundrystaffcansupportstaffwithwashingtheextratowels/faceclothsusedinNamaste,andkeepingtheroomsupplied.
v Maintenancestaffcanhelpwithjobssuchasfittingupablindtodiffusebrightdaylight,advisingaboutnaturallighting,orsettingupspeakersforthemusicsystem.
v EveryonecanplayapartandeveryoneshouldbeencouragedtospendatleasttwentyminutesinaNamastesessionsothattheyunderstandwhatisgoingon.
FindingaNamastespaceinyourcarehomeThe most important feature of the Namaste room is the constant presence of theNamasteCareworker.Remember,‘Ifthereisnoonethere,itisnotNamaste’.Everythingthat isdone intheNamasteCareprogrammeisdone ‘tohonourthespiritwithin’.Everydecisionyoumakeabouttheenvironmentofthecareprogrammeshouldreflectthisfundamentalphilosophy.
30
TheperfectNamasteroomIdeally,NamasteCarehas adesignated room,whereeverything canbe left inplace,supplies canbe lockedawayafter the sessionand there isnodangerofmoreactiveresidents going into the roomand damaging growing plants or fragile ornaments bymistake (seeBox4.4).However, if there isno separate room, thenaNamaste spacecanstillbecreated.Itmaybeascreened-offareainaloungeorthediningroom.Theenvironment must be made ‘special’, i.e. welcoming and homely, with natural orslightly dimmed lighting, attractive scents, such as lavender from an aromatherapydiffuser,andwithsoftmusicplaying.Thereshouldbeaslittledistractionaspossible.
Box4.4:IntheperfectNamasteroomtherewillbe:Awindowlookingoveragarden AbirdtableoutsideAdoortotheoutside AmusicsystemandavarietyofmusicADVDplayerandappropriateDVDs AnaromatherapydiffuserAnaromatherapydiffuserRecliningchairs
BeautifulpicturesGrowingplants
Ornamentsfromthepast AcupboardthatcanbelockedAfridge AsinkwithrunningwaterAsmoothiemaker Curtainsorblinds
CreatingyourNamastespace:YoumayneedtobequitecreativeabouthowyousetuptheroomorspacetoprovideaNamasteCareprogramme(seeBox4.5).
Box4.5:Usingspacecreatively
v Onecarehomehadjustoneloungeandmostresidentshadtoeatinthat.ItsonlyoptionwastocreateaNamastespaceatoneendoftheroom.Thestaffrearrangedthefurniture,paintedthewallspinkandhungacurtain,whichtheydrewwhentherewasaNamastesession.
v Inanothercarehomethemanagerhadalargeoffice.ShemovedoutintoasmalleroneandtheroomwastransformedintoaNamasteroomwithalickofpaintandsomepictures.
v Anotherhomehadalargediningroomthatwasemptyexceptatmealtimes;thiswas‘dressed’immediatelyafterbreakfastwithsomecolourfulwallhangingsandflowers.
v In the USA, a care home started its Namaste Care programme in an emptyresident’sroom.
31
Howeveryouorganisethespace,youwillneed:• Aspacethatcanbeprotectedfrompeoplewalkingthroughandcausing
adisturbance• Acommittedteamwhowillusetheirimaginationtocreateahomely,
welcomingatmosphere• Amusiccentre• Ameansofscentingtheroom• Tofindawaytobringthenaturalworldinside• Storage.
SeeChapter5formoredetailedinformationaboutessentialsupplies.
MakingithappenIfyouareonlyrelyingononeparticularpersontoruntheNamastesessionitwillnotwork.Onepersoncannotbearoundeverydayofeveryweek.Therefore,itisimportanttohaveseveral staffmemberswhocanrunNamastesessions.TheNamastesessionsmustbe‘officially’allocatedontherota.Itisalsoimportantthatyouallocatepeoplewhoareenthusiasticandconfident to runtheNamastesessions.WeallhaveuniqueskillsandsomeofyourstaffwillbebettersuitedtodoingNamastethanothers.Overtime,everymemberofstaffwillbeabletoruntheNamasteCaresession.
Themanagermust protect and support the core teammemberswhile theNamasteCareprogrammeisbeingestablished,e.g.notputtingthemonnightduty,orsendingthem on escort duty. Ideally, for the best chance of success, during the initialimplementationphase, themanager/clinical leadneeds tobepresent at the start ofeachsession,andtoengagewitheveryaspectoftheprogramme.We have found that the Namaste Care programme enables you to use time moreproductively.InBox4.6belowwesummarisethis.
Box4.6:Usingtimeproductively
Inmanyofthecarehomeswehavevisited,youcanoftenfindacareworkersittinginthelounge,duringthemorningorafternoon,lookingafteragroupofresidentsandmakingsuretheyaresafe.Oftenthecareworkerisfillingoutfluidchartsorsomeotherpaperwork,butnotinter-actingwithresidentsTheNamasteCareprogrammeusesthiscareworker’stimedifferently.Insteadof‘minding’residents,theNamasteCareworkerengageswithresidentswithadvanceddementiaandprovidesappropriatesensorystimulationandone-to-onetimeinagroup.ThemorefreedomthattheNamasteCareworkershave,themoretheywilldevelop
ideasthemselves.FamilymembersoftenenjoytakingpartinNamasteandsometimessupplyideasandskillsandmaterial.
32
SectionFive
GettingreadyfortheNamasteCareprogramme
Sectionaims:
• TohighlightwhatneedstobedonetogetNamasteCarestartedOnce you have decided to implement the Namaste Care programme in your carehome,youneedtoprepare–makingcertaindecisionsandpreliminaryorganisations.
Decisions• Decideonabudget(evenifyoudecideyouhavenothingtospend—thatwill
thenbeclear)
• Choosethecoreteam(encouragethemtoreadTheEnd-of-LifeNamasteCare™ProgramforPeoplewithDementia3)
• WiththecoreteamchooseaspacefortheNamasteCareprogramme.
PreliminaryorganisingforNamastebycarehomemanager• Explain theNamaste Care programme at staffmeetings and, for example, at
handovermeetings
• Put upnotices/posters in the care home announcing the introduction of theNamasteCareprogrammeandaprovisionalstartdate.
• Meetwith/writetoGPsandotherrelevantoutsideprofessionalsandagenciestoinformthemthatyouarecommencingtheprogramme
• Setuparelatives’meetingtoinformthemaboutchanges
• WiththecoreteamlistthebasicequipmentfortheNamasteCareroom
• Reviewresidentswithkeyworkerstoestablishwhichresidents fulfil theGoldStandards Framework criteria19 for end-stage dementia and would thereforebenefitfromattendingtheNamasteCaresessions
• Makesuretherearesuitablechairs(seeBox5.2)–aNamasteCareprogrammecannotworkwithresidentssittinguncomfortably
• Makesureessential suppliesare ready (seeBox5.1). Youcanalwaysmakea‘wishlist’(seeBox5.3)thatpeoplemightdonateto
• SetarealisticdatetostarttheNamasteCareprogramme.
33
Box5.2:Essentialequipmentandsupplies4(N.B.Mostofthesewillbeavailableinthecarehomealready)
v Comfortablechairsv MusicsystemandCDs(orMP3playeranddownloads)v Anaromatherapydiffuser(oraplasticspraybottlewithdistilledwateranda
dropoflavenderessentialoil)v Attractivecolouredrug/blanketforeachresidentv A‘washbag’,orziplockedbagforeachNamasteresidentcontainingtheirown
brushandcomb,facecreamandhandcream,nailclippers,emeryboard,lipbalm,etc.
v Drinkingcupsthatcanbelabeled,ordisposablecupsandamarkerpenv Faceclothsandtowelsv Alargestoragebagforeachresident,e.g.aplasticzipbagtokeeparugand/or
pillowandperhapsalife-likedolloranimalv Arummagebagwithsilky,tweedy,velvetyscrapsofmaterial,bubblewrap,etc.v Twotothreeportable(preferablyfolding)chairsfortheNamasteCareworker
andforvisitorsv Handsanitizer,rubbishbagsv Boxoftissuesforrunnynosesv Laundrybagsandglovesincaseofaccidentsv NamasteCareworkerhasavisiblenamebadgewiththeirfirstnameinlarge
fontv Welcomesign(onecarehomehasanoticethatsays,‘Pleasecomeinquietly
andgently’.
Box5.1:Seating
Peoplewithadvanceddementiaoftenneedspecialchairsbecausetheyareusuallyfrailandimmobile,andoftenhavecontractedlimbs.
Havingachairwithwheelsisparticularlyhelpfulbecauseitmeansthepersondoesnotbecome ‘bedbound’ and can spend the day in comfort and move around the carehome.Thesechairsarehoweverspecialistequipmentandveryexpensive.
Itisthereforeimportantforyoutoassesswhetheryouthinkthechairtheresidentisinisthemostsuitableoneforthem(oftenthecarehomehasavarietyofchairs);itmaywellbethereisamoresuitableonebutifnotdoseekadvice.Peoplewithdementiainprivate care homes are entitled to assessment of their seating needs by an NHSoccupationaltherapist.
RequestinganO.T.assessmentisthefirststeptowardsgettingappropriateseatingforsucharesident.
Sorting out the funding for an appropriate chair can causedelay so beloware somepossibleothersolutions:
o SometimestheNHSsuppliesasuitablechair
34
o Sometimestheresidenthastheirownfundso Sometimesrelativeswillbuyacomfortablechairo Thefamilyandthecarehomecansharethecostontheunderstandingthatthe
carehomekeepsthechairwhentheresidentdieso Sometimescarehomeshavechairstheyhaveboughtorinheritedo There are charitable trusts that will contribute to the cost of specialist
equipmentforsickpeopleo Ifthefinancespermit,considerincludingthecostofonenewrecliningchairin
yourNamastebudget.o Considerfundraisingforachaire.g.coffeemorning,raffleetc.
Box5.3:WishlistforNamasteequipment(N.B.Maybeavailableinthecarehome,orperhapssomeonewoulddonate,
orraisemoneyforfunds)
v Atrolleyforequipmentforthesessionandtotakeequipmenttoaresident’sroom
v Greenplantsv Oneortwolife-likedollsv Life-likecatsanddogsv Life-likesingingbirdsv Afridgeforfoodtreatsv Picturebooksv Poetrybooksv Avarietyofessentialoilsv Tambourineandrainmakerv Picturesandornamentsv ADVDplayerandappropriatefilmswithascreentoshowthemv Footspa
Jobsforcoreteam
• Checkaroundthecarehomeforalreadyavailableequipmentandsupplies(seeBox5.1)
• Askcolleaguesandvisitorsforscrapsofmaterial,etc.forarummagebox.• Check out your colleagues’ skills. For example, does anyone have training in
aromatherapyormassage?Doesanyonehaveabeautifulsingingvoice?Doesanyonehaveagardenfromwhichtheycouldbringflowers?
• Collect supplies for each individual resident (see Box 5.2). Use their ownsuppliesanddiscussthiswithfamily/friendsatthefamilymeeting(seeSectionSix).
• WhenyouhavedecidedwheretoruntheNamasteCareprogramme,preparethe space. Itmay need a lick of paint, or youmay need to create a screen.Allocate roles to teammembers and check your equipment and storage and
35
that the music player is working before you confirm the starting date forNamaste.
• Makeawelcomesign.Box5.1:Generalsupplies
• Pillowsforpositioning• Blankets/rugs/quilts
(colourful)• Facecloths• Bowlsinwhichtosoakhands• Towels• Aqueouscreamfor
moisturisingskin• Cottonbuds• Hypoallergenicoilfor
massage• Soapdispenser/handsanitiser• Glovesandlaundrybagsin
caseofaccidents
• Disposablewipes
Box5.2:PersonalsuppliesforNamasteresidentsAclearlynamedbagcontaining
• Hairbrushandcomb• Nailclippers• Emeryboard• Facecream• Lipbalm• Itemssuppliedbythefamily,
e.g.perfumeandmakeupforwomen,aftershaveformen
Alargebagsuchasadrycleaningbagtokeeptheblanketand,forexample,alife-likeanimal.
DocumentationThe manager and the core team must decide how to document the Namaste Careprogramme.Suggestionsfordocumentationinclude:
• Arecordofattendance• Apersonalprofileforeachresident• Documentinganyrisks• Allergies• Concernsaboutinfection• Informationaboutconditionssuchasdiabetes• Swallowingdifficulties• Sensoryimpairments,e.g.poorsight,wearsglasses,orpoorhearinginoneear• Concernsaboutbehaviour,e.g.maytrytoeatinediblethings• A‘sensory’biographyoflikesanddislikes• Favouritemusic• Foods/tastes• Scents• Doesthepersonlikehugsandtouch?
36
• Doesthepersonrespondtocolourorenjoylookingatpictures?• A folder containing a recordof activities for eachof the residents takingpart
andtheirresponsestodifferentsensoryexperiences.• A non-verbal pain assessment scalewhich staff in the care home understand
howtouse(seeSectionEight)Once potential residents have been selected for Namaste, it is important that themanagersetsupameetingwithindividualfamily/friendstoexplainwhyNamasteCarewillbesuitablefortheirrelative(seeSectionSix).Finally,thecarehomemanagershouldfilloutaNamasteCarechecklisttobesurethateverythingisinplacetostarttheNamasteCareprogramme.
37
SectionSix
The‘familymeeting’:communicatingwithrelatives
Sectionaims:• ToofferguidanceforholdingaNamastefamilymeetingwiththeresident’s
family/closefriends• toinformfamilyabouttheroleofNamasteCareinhelping
tomaintainthequalityoflifeofpeoplewithadvanceddementia• Toaskthefamily’shelpwithcreatinga‘sensorybiography’,e.g.theperson’s
favouritemusic• Toexplaintheimportanceofplanningend-of-lifecareatthisstage• Tohighlighttheimportanceofdiscussingissuessuchasadvancedecisionsto
refusetreatmentandcardiopulmonaryresuscitationWhenyouhaveassessedthataresidentwouldbenefitfromNamasteCareyouneedtoset up a ‘family meeting’ to explain the change in care to family/friends. GoodcommunicationwithrelativesiskeytothesuccessofNamasteCare.The familymeeting isheld to learn fromthe familyandengagewith them in findingwaystobringpleasureandtriggermemoriesfortheirfamilymember.Thismeetingisalso anopportunity to acknowledge the resident’s deterioration fromdementiawithfamily/friendsinthepositivecontextofofferingmoreappropriatecare.Thediscussionabout how to provide quality of life can open up conversations about maintainingqualityoflifetotheendoflifeandplanningend-of-lifecare.Themainpurposesofthe‘familymeeting’areto:IntroducetheconceptofNamasteCare
• Discusswithrelatives/friendsthatitisfelttheresident’sconditionisprogressing.
• Explainthattheresidentisnolongerabletotakeanactivepartinconventionalcarehomeactivities.
• DescribetheNamasteCareprogrammeandinformrelatives/friendsthatNamasteCareisaninterventionthathasbeenshowntobenefitresidentswithadvanceddementiae.g.byreducingisolation,agitation,andanxietyandpromotingengagementandcommunication.
• Learnmorefromrelatives/friendsabouttheirlovedone’slifestory,andanymeaningfulactivitiesandsourcesofcomfortandpleasurethatthefamilyfeelwouldbenefitthemduringthecareprogramme,e.g.whatmusicisassociatedwithpleasurableeventsintheresident’slife,andwhatperfumesoraftershaves
38
theresidentmaylikeandwhichmaytriggermemories.Youcanthinkofthisascompilinga‘sensorybiography’.
• Encouragerelatives/friendstoparticipateintheNamasteCareprogrammeandsharecarestaffmembers’effortstoconnectwiththepersonwithdementia.
Preparerelatives/friendsthattheirlovedone’sconditionisworsening
• Thismeetinggivesyouanopportunitytoexplainthat,evenatthislatestageindementia,peoplehaveasenseofselfandareabletoengageemotionallywithothers.Family/friendsandhealthcareprofessionalsshouldconcentrateonmaintainingqualityoflifetotheendoflife.
• Highqualityend-of-lifecareneedsplanning,andanend-of-lifecareplanneedstobeagreedupon.
• Preparetherelatives/friendsforloss.• Discusstheburdensandbenefitsofacutemedicalinterventions(discussions
mayencompassissuessuchascardiopulmonaryresuscitationandpreferredplaceofcareanddeath),andexplainthatcomfortandpleasurearetheaimsofcareatthisstageinthedementiatrajectory
• Establishthegoalofapeaceful,dignifieddeathinfamiliarsurroundingsatthecarehome.
Youmaynotachievealltheaimssetoutaboveinthisfirstmeeting.Nevertheless,itisimportant to start the conversation about end-of-life care while the person withdementiaisnotimminentlydying,becauseitallowstimeforthefamilytoadjusttotheideaoflosingtheirlovedone.Givethefamilyachancetogoawayandthink,talkwithfriends and look thingsupon the internetor speakwith their ownGP. Then, invitethemtocomebackforanothermeetingtotalkthroughthestepsthatneedtobetakentoensurethepersontheylovehasapeaceful,dignifieddeathcaredforbypeoplewhoknowthemwell.Ifyoualreadyknowtheresident’sfamilywellandhavealreadyexploredtheirthoughtsandpreferencesaroundend-of-lifecarefortheirlovedone,thenthismeetingwillbeachance to check that nothing has changed and everything is in place to ensure apeaceful,dignifieddeathinthecarehomee.g.thesignedDNaCPRorderandanend-of-lifecareplan.Having a face to face meeting rather than a telephone discussion is best practicebecausewhenyoumeetwiththefamilyyouwillbemoreawareofanydistressandyouwill be able to able to pick up on non-verbal communication which is lost over thephone.Ifyoufeel thata familymember is inneedofsupport thenyoucanrefer themforacarer’sneedsassessmentwhichisprovidedforintheCareAct41(2014).
PreparingforthemeetingIt is essential to invite to thismeeting relativeswho are involved in the care of theresident, or friendswhomay bemore involvedwith the resident than actual familymembers.Clearly,ifthereisaLastingPowerofAttorneyforHealthandWelfare,that
39
personshouldbeinvited. Themeetingcanbearrangedwhenthefamily/friendsvisittheirlovedone,orbytelephoning/sendinganinvitationlettertotherelevantpersonorpeopleinvolved.Confirming themeetingwith the relatives/friendsa fewdaysbefore it isdue to takeplaceisveryhelpful.Intheinterestsofgoodcommunication,itisalsobestpracticetoensurethatallstaffmembersareawarethatthemeetingishappening.Itisimportanttoprepareproperlyandrespectfullyforthemeeting.Forexample,thereneeds to be enough staff onduty, and, if possible, aNamasteCareworkerwho canattend aswell as themanager, or a senior nurse. You should try to arrange a quietspace/roomforthemeetingwherethere isnotelephoneandwheretherewillbenointerruptionsfrompeoplecominginandout.Makesurethereareenoughchairsandifpossiblearrangeforteaandcoffeewhichhelpscreatearelaxingatmosphere.Remembertoplansufficienttimeforthemeeting.
OutlineofdiscussioncontentIntroductionItishelpfultobeginbycheckingiftherelativeshaveanyconcernsorqueries.Askthemhowtheyfeeltheirfamilymember/friendhasbeenoverthepastfewmonths.Remindthem that if anything is said that theydonotunderstand then they should interruptandaskforanexplanation.Box6.1givessomeusefulsuggestions.
Box6.1:CommunicationsuggestionsØ Howdoes[nameofresident]seemtoyou?Ø Haveyounoticedanychangesin[name’s]condition?Ø Wefeelthat[name]islessabletodothingsthanpreviously?(trytogivean
exampleofchangeintheindividual)……Wouldyouagree?Ø Dementiaisaprogressivedisease,inthatthepersonwithdementia,
overtime,graduallybecomeslesswell.Ø Thesignsthatthedementiaisprogressingincludelossofappetiteanddifficulty
swallowing,difficultywalkingwithouthelp,moreinfections,increasingdifficultieswithtalkingandinteractingwithotherpeople.Again,trytorelatethistochangesthefamilymayhaveseenintheirfamilymember
Ø Suchsymptomsindicatetousthat[name]maybeenteringthefinalstagesoflife.Itisofcoursedifficulttoknowjusthowlongsomeonehaslefttolive,aseveryoneisdifferent.[Name]mayhaveafewmonths,orevenyears.Thereisalsothepossibilitythat[name]haslessthanafewmonths.Wedon’tknowbutwewillbemonitoringthemcloselyandwillofcoursekeepinregularcontactwithfamily.
InformationabouttheNamasteCareprogrammeThe family/friends need to be informed (if they do not already know) that the carehome offers Namaste Care to residentswith advanced dementia, and that NamasteCarewillhelpstaffmembersengagewithresidentsandprovidepleasantexperiences.Explain that theprogrammealso ensures that their lovedonewithdementiawill be
40
closely monitored for pain and distress, while at the same time theirhydration/nutritionwillbeimprovedasstaffmembersconcentrateongivingfluidsandappropriatefoodduringthesessions.Bringingupthetopicoftheresident’sdeteriorationThismeetingisachancetotalkwiththefamily/friendsabouttheprogressionoftheirrelative’sdementiaandsupport themtoacknowledge thatdementia isa life-limitingcondition.Itisimportanttoexplainthatitisdifficulttopredictexactlywhensomebodywill deteriorate and how quickly. Thismay be the first time the family have spokenabout their relative’s end-of-life care. It may be the first time they have faced theprospectofthepersontheylovedying.A relativemayask ‘how longhasmymother/fathergot to live?’ Besure toexplainthatpredictingwhensomeoneislikelytodieisparticularlydifficultandunreliableforpeople with dementia. Be careful to talk in terms of months, or weeks, or days,whichever is appropriate;neveraparticularnumber. If youareasked topredict say,“we are looking in terms of months/weeks”, not ‘a month’ or ‘two weeks’. It isimportantthatyoureassurethemthatyouwillbemonitoringthepersoncloselyandiftheir condition deteriorates youwould let them know immediately. This is a usefulopportunity to check contactdetails for the relativesare correctand findout if theywouldwanttobecalledovernightiftherewasasuddendeterioration,oriftheywouldprefertobecalledinthemorning.
Thismeetingencouragesthefamilytothinkaboutthethingsthatmattertotheirlovedonetowardstheendoflife,aswellasanypersonalgoalsofcareandpreviouswishesthatthepersonmayhavewrittendownwhiletheywereableThe family could be asked to consider what they feel their loved one, if they couldexpressaview,wouldliketohappenatthetimeoftheirdeath,e.g.wheretheywouldliketodie,whetheritisthoughttheywouldlikecertainmusictobeplaying,andwhotheywouldliketobepresent.Thisisanopportunitytodiscusswhatthefamily/friendsknowabouttheirlovedone’spreviousconcernsandwishes;whetherthepersoneverspokewiththemaboutwhattheywouldwishtohappenwhentheyweredying.StatementsofwishesandpreferencesThe family need to understand that a statement ofwishes and preferences is not alegally binding document but will be used by health care professionals to guidedecisions.Noonecandemandaparticulartreatmentifthemedicalteamfeelitwouldnot be in the person’s best interest to undergo such treatment. An example of thiswouldbeifapersonwithterminalcanceronlyhadafewdaysorhourslefttoliveandthefamilyrequestedanothertrialchemotherapy. Thedutyofthemedicalteamistoact in the person’s best interest. Therefore, if the medical consultant judged thetreatmentwould be futile andwould cause the person additional distress then theywouldrefusethefamily’srequest42.Belowaresomeinformationandsuggestionsthatmightbehelpfulwhendiscussingfuturecare(seeBox6.2)
41
LastingPowerofAttorneyforHealthandWelfareA person with capacity to make decisions about their future care may choose toappoint a Lasting Power of Attorney for Health and Welfare and give this personresponsibility formaking future decisions on their behalf in the event that they lackcapacity. This is a legal process and a Lasting Power of Attorney documentmust beregisteredwiththeOfficeofthePublicGuardian.WhenthepersonappointsaLastingPowerofAttorney theycanchoosewhetherornot toallow thatperson tohave thepower to make decisions about life-sustaining treatments. If there is a registeredlastingpowerofattorney forhealth, then there isa legal requirement for thehealthandsocialcareteamtoconsultwiththemabouthealthissues,eveniftheclinicalteamsee another friendor relativemoreoften than thepersonwhohas lastingpowerofattorney.Box6.2:Communicationsuggestionstohelpwhendiscussingfuturecare
• Althoughwecannotbecertainhowlong[name]haslefttolive,wefindthatitisgoodpracticetopreparefortheendphaseoftheirlifewhileatthesametimehopingforthebest.Forexample,itmaybeusefulatthisstagetostartthinkingaboutwhereyouthink[name]wouldliketobecaredforuntiltheend.
• Inourexperience,itismuchbetterforapersonwithadvanceddementiatoremaininfamiliarsurroundings.Hospitalscanbeverydistressingforpeoplewithdementia,becausetheyareverynoisyandbusyplaces.
• Ourmainaimistoensurethat[name]iskeptcomfortableatalltimesandthatwehonouranyrequeststheymayhavemadeaboutwhattheywouldliketohappenwhentheydie.Didtheyevertalktoyouaboutthis?
• Althoughweallhopethatyourlovedonewillbewithusforawhileyet,itwouldbeveryusefultodiscusshowyouwouldlikeustocarefor[name]whenthetimecomes.Forexample,itisveryimportantforsomefamiliestobepresentwiththepersontheylovewhentheyaredying.
MakingdecisionswhenpeoplelackcapacitytomakedecisionsforthemselvesTheMentalCapacityAct200530
ThefirstprincipleoftheMentalCapacityAct2005isthatsomeoneshouldbeassumedto have capacity to make their own decisions. When a person has dementia, thisassumptionneedstobetested.The Mental Capacity Act requires the judgement about whether a person lackscapacity,andifsowhattodoaboutit,tobemadeatthetimethemedicaldecisionhastobemade.However,oftenatthepointacrisisoccurs, itmaybedifficult toconsulteverybodywhoshouldbeconsulted.Itisbestpractice,therefore,toplanahead.Amentalcapacityassessmentshouldbeundertakentoestablishwhethertheresidentisabletounderstandandretaininformationforlongenoughtoweighuptherisksandbenefitsofadecisionandcommunicatethedecisiontheymake. Ideally,peoplewithdementiashouldmakeprovisionfortheirend-of-lifecarewishestobemetintheearly
42
stagesofthediseasewhiletheyhavecapacity.Peopleinthelaterstagesofdementiawill not have the capacity to make the necessary decisions to ensure they have adignifiedandpeacefuldeath.IftheresidenthasnotappointedaLastingPowerofAttorneyforHealthorWelfare,ormade an advance decision to refuse treatment, then the responsibility for makingdecisionsabouttheresident’scarelieswithhealthandsocialcareprofessionals.Healthand social care professionals are bound to act in thebest interests of a personwholackscapacitytoactontheirownbehalf.Almost invariablythehealthandsocialcareprofessionalswillbeguidedintheirdecisionmakingbythefamily/friendsofthepersonbecausethefamilyhavetheperson’sbestinterestsatheart,andknowwhatmatteredtothem,andwhatthepersonmighthavechosenforthemselves.AbestinterestsmeetingIn cases of people who are unable to make their own decisions, end-of-life caredecisionsneed tobe informedbyabest interestsmeeting. Inorder toarriveat thebestpossibleoutcomeforthepersonand,asfaraspossible,toactasthepersonwouldwish in the circumstances, the best interests meeting must involve the person’sfamily/friends, and any legally required representative as laid out in the MentalCapacityAct,alongwiththehealthandsocialcareprofessionalswhoknowthepersonbest. It is essential that everyone involved has a full understanding of all the issuesinvolved.Whendecisions about health care are discussed, health care staffmust beinvolved. Ina carehome itwill usuallybe theGPwho takes the lead,butnot inallcases.Ifabestinterestsmeetingisheld,itisimportanttodocumentwhowaspresent,whatthedecisionwas,whattheargumentswereforandagainstthedecision,andthenattheendseewhatdecisionthosepresentfeltwouldbeintheperson’sbestinterest.AdvancedecisionstorefusetreatmentInthemeeting,it is importanttoaskaboutanyadvancedecisiontorefusetreatmentthat thepersonwithdementiamayhavemade.This issuecanoftenbe forgottenonadmissiontothecarehome.Althoughatreatmentcannotbedemanded,apersonmaystatetheirwishestorefuseaspecificmedicaltreatmentinadvance.Forexample,inthecaseofapersonwantingto die at home, they could state that they only want comfort measures to beimplementedanddonotwanttobetransferredtohospitalforactivetreatment,suchasartificialnutritionorrespiratorysupport.Thetreatmentsthat thepersonwantstorefuseneedtobeclearlystatedinanadvancedecisiontorefusetreatmentdocument,and thedocument should specify the circumstances inwhich itwouldbe applicable.Suchadocument is legallybinding ifsignedandwitnessedandwaswrittenatatimewhen the person had capacity (TheNational Council for Palliative Care andNationalEndofLifeCareProgramme42,2009).
43
Topicstobediscussedwiththefamiliesofpeoplewithadvanceddementiainordertopreparethemfordeteriorationintheconditionoftheirrelative,andguidefuturedecision-makingThe followingquestions canprovideuseful information toguidedecisions relating totheend-of-lifecareofapersonwithadvanceddementia:
• Howcanweensurethatanyknownwishesofthispersoncanbefollowed?• Willthispersonbenefitfromcardiopulmonaryresuscitation?• Willthispersonbenefitfromartificialnutritionorhydration?• Underwhatcircumstanceswillthispersonbenefitfromhospitaladmission?
The person’s wishes should guide the care they are given. Cardiopulmonaryresuscitation, artificial hydration and nutrition and other treatments cannot bedemandedbythefamily,andshouldbegivenonlyiftheseniorclinicianinvolved(inacarehomethisisusuallytheGP)believesthatatreatmentisinthebestinterestsofthepatient.
Helpfulfactswhichyoumaywishtorefertowhenansweringrelatives’questions.Cardiopulmonaryresuscitation
Cardiopulmonaryresuscitationisanemergencyproceduretorestoretheheartbeatofapersoninthecaseofacardiacarrestwherethereisnoheartbeat.Itinvolvesinflatingthelungswithamaskortubeinsertedintothewindpipe,regularlypressingdownveryfirmlyonthechestandsometimesusingelectricshockstotrytocorrecttherhythmoftheheart.
Thepersonconducting thediscussionmustbesensitive to the fact thatwhenhavingdiscussionsaboutcardiopulmonaryresuscitation,relativesfeelthatbysaying‘no’toittheyareactuallylettingtheirlovedonedie.Therefore,itisimportantthattherelativesare awareof the full facts before giving a viewas towhat their relativewouldhavewanted. Successful resuscitation (i.e. the person recovers enough to leave hospital),onlyoccursinoneineightpeoplewithalltypesofillness.Elderlypeoplewithchronicillnessonlyhaveanaveragesurvivaloflessthanfivepercent;forpeoplewithadvancedillness, survival rates are often less than one per cent43. There has never been asuccessful resuscitation attempt following an unwitnessed cardiac arrest in a carehome44.Forelderly residentswithdementia, it isusuallynot in theirbest interests toopt forresuscitationas,intheeventofacardiacarrest,itwouldmeantransferringthepersontohospitalasanemergencywiththeveryhigh likelihoodthattheywoulddie inthatenvironment.
44
Whenresidentswithdementiareachtheendoftheirlives,itisbetterforthemtodieanaturaldeath,inthesurroundingstheyknow,andwiththepeopletheylove.ArtificialnutritionForpeoplewithadvanceddementia,thereisnoevidencethatartificialfeedingthroughanasogastrictubeorapercutaneousendoscopicgastrostomy(PEG)tube(atubethatgoesdirectlyintothestomach)hasanybenefit45.Ithasbeenfoundthat:
• Lengthoflifeisnotextended• Weightlossisnothalted• Complicationssuchaspressureulcersarenotprevented• Thepersonislikelytopullanytubeout• Thepersonlosesthecomfortoffoodandone-to-onecontactwiththeperson
whofeedsthem.ArtificialhydrationWhenpeoplearedyingtheyarenotabletomaintainhydration.Peopledyingwith,forexample,cancer,whoareabletodescribehowtheyfeelwhentheyaredying, rarelydescribethirstastheybecomemoredehydrated,althoughtheydocomplainofhavingadrymouth.Ifapersonwithadvanceddementiastopseating,drinkingandswallowingbecause they are dying, there will be no benefit in transferring them to hospital torehydratethemwith intravenous fluids. Givinggoodregularmouthcarerelieves thedrymouthjustaswell46.HospitaladmissionHospital admission is distressing for patients and families24,27,28. Hospital admissionrarelybenefitspeoplewithadvanceddementia:
• Theyarefourtimesmorelikelytodieduringtheadmissionthansomeonewithoutdementia
• Theyreceiveinadequatesymptommanagement,especiallyofpain• Theyarelesslikelythanotherterminallyillpatientstobereferredforspecialist
palliativecare.
45
SectionSeven
TheNamasteCareprogramme
Sectionaim:• TooutlinethepracticalpreparationsforNamasteCare• TodescribewhatisinvolvedinNamasteCaresessions
o Toconsidertheeffectsofsensorystimulationonbehaviourandcommunication
o Toprovideexamplesofcomfortmeasures,appropriatesensorystimulationandmeaningfulactivities
The sooner you startNamaste Care the better, so that your residents can enjoy thebenefitsofthecareprogramme.Youwillcontinuetodevelopyourprogrammeasyougoalong.SettinguptheNamasteroom,makingasensoryenvironmentforpeoplewithadvanceddementiaYou will find very helpful advice in ‘How toMake a Sensory Room for People withDementia’47,whichisavailableasafreedownloadfromtheinternet.Thisguidebookofferssuggestionsforcreatinganageappropriatemulti-sensoryenvironment.Youwillfindevidencebasedguidanceonmakingthespaceyouchoosefeelcomfortable,safe,meaningfulandfamiliarforpeoplewithdementia.Box 7.1: Understanding the world through our senses, sight, sound,touch,taste,smellandmovementWe all need stimulation to understand the world around us. We learn about oursurroundings through our senses: sight, touch, smell, taste, sound and movement.Sensorydeprivationhasdeeplynegativeeffectsonhealthandwellbeing.Whenthereis toomuch stimulationpeople canbecomeoverwhelmed. Mosthealthypeopleareabletomakeadjustmentstotheirenvironment,orwithinthemselves, inordertogetonwithlifeandfunctionwell.Peoplewith dementiawho have impaired physical and cognitive abilities often havelittlecontrolovertheirenvironment,sotheyneedsupporttofindalevelofstimulationthat fits theirneeds. If there isvery little stimulation,withnothingmuchhappeningand nothing to do, then many people will sleep to pass the time away, but somebecome anxious and agitated. Some people with dementia become agitated andanxiouswhentheenvironmentisoverstimulating,whileothersmayrespondtoover-stimulationby‘switchingoff’andwithdrawing.In the multi-sensory environment of the Namaste Care session, the Namaste Careworker tries to help each individual to relax. Namaste Care can help people withdementiawhoarefeelingagitated,anxiousandtensetounwindandfeelcalm.These
46
peopleareoftenexhaustedandthereleaseoftensionmaymeanthattheyfallasleepinNamaste.0ther people with dementia protect themselves from the complexity and over-stimulationoftheirsurroundingsbywithdrawingintosleepandlethargy.InNamasteCarethemulti-sensoryenvironmentreducesdistractionsandallowsthesepeople to set aside some of their defences and to ‘wake up’ in Namaste sessions.Peoplewhoaregenerallyunresponsiveand lethargicmaystart to interactmorewithotherpeopleandtheenvironment,perhapstheyrespondtothemusic,orperhapsthetouchoftheNamasteCareworkerencouragesthemtomakeeyecontactortospeak.
LightingLighting inNamaste shouldbenatural. Soft lighting reduces the shadowsandmakeseveryonelookbetter.Wall lampswithsoftbulbscreateahomelyatmosphere.Brightoverheadlightscouldbedimmedwithadimmerswitch,orwithaspecial lampshade.Youmayneedablind to filterbright sunlight. Somecarehomeshave specialbubbletubelamps.Theseareanattractivefeaturebuttheyarenotessential.
MusicMusichasthepowertounlockmemoriesandemotionsinallofus.ItisacornerstoneoftheNamasteCareprogrammeandtheNamasteCareworkershouldthinkcarefullyabout the music for the day. During each session she/he needs to observe howindividualresidentsrespondtoparticularpiecesofmusic.Atthestartoftheday,soft,gentle,classicalmusicmaybeeffective.Eventhoughthemusicisgentle,youmayneedtoplayitquiteloudlybecausemanyresidentshavepoorhearing. If themusic can be heard outside the Namaste space, other residentsmaywalkintoseewhatishappeningandmaydecidetostayforawhile.If youplaymusic continuously,people stophearing it. So, afterabout fortyminutes,have tenminutesof silencebefore starting themusicagain.Relaxationmusic,whichhasaslowrhythm,canslowtheheartbeatandhelpthebodytorelax.Forachange,youcanputona recordingofbirdsongorwaveson theseashore.Alwaysnotice ifaresidentappearstoenjoyorbemovedbyanymusicyouplay.Musictriggersmemories.Themusictheresidentslovedwhentheywereyoungermayhave strong associations for them. When family members have told you whatparticular music was associated with a positive experience for their relative, whichparticularsingersorsongswereplayedatsignificantevents,youcantryplayingthemintheNamastesession.Itisthenimportanttoobservewhethertheresident’squalityof attention and engagement changes and to notice the effect of themusic on theotherresidentsinthegroup.If apieceofmusicmakes someone sad,offer themcomfort and supportbutdonotimmediatelystopplayingthemusic.Thepersonmayhavebeenbottlingupemotions

47
andthemusicenablesthemtobeintouchwiththeirfeelingsandexpressthem.Youshouldthinkcarefullyaboutwhen/whethertoplaythatpieceofmusicagain.LivelymusictowardstheendofthesessionpreparestheresidentforthechangefromthecalmNamaste roomto thebustleof thecarehomeand themealahead. Dancemusic, for example, can make the transition easier and helps to ensure Namasteresidentsfeelawakeandreadyforthemeal.
ScentingtheroomScenting the room immediately creates the sense of somewhere ‘special’. Lavenderand lemon balm have been shown to reduce anxiety, depression and agitation inpeople with dementia and both essential oils are generally safe to use If you haveaccesstoanaroma-therapistyouwillbeabletoexploreusingarangeoffragrances.If youhaveanelectricaromatherapydiffuser,youcanput theoil into thecontainer,switch it onand the roomwill be scented. If youdonothaveadiffuser, put two tothreedropsofessentialoilintowaterinanironingspraybottleandspraytheroom.Also, importantly,whenusingaromatherapyoils, youmustbeawareof the safetyissues involved, particularly for residents and staff. The care home should have apolicyfortheiruseandstorage.Essentialoilsarechemicallycomplexandshouldbeusedwithcaution.Ifthereissomeoneinthecarehomewitharomatherapytraining,nowisthetimetomakeuseofher/hisskillsandknowledge.DoNOTusescentedcandles!NursingsuppliesYouwillneedfacecloths,towelsandwashbowlsathand.Youwillalsoneedsuppliesofaqueous cream and Q-tips, disposable wipes, hand sanitiser and gloves (in case ofaccidents,notforroutinecare!).
DrinksandfoodtreatsDrinksTryandarrange for thekitchentobringa trolleywitha jugofwaterandachoiceofjuices, e.g. orange and cranberry. Each Namaste resident must have an individuallymarkedcup.Itmaybeeasiesttousepapercupsandamarkerpen.Youwillalsoneedstraws. There should be ‘thickener’ on the trolley for anyone with swallowingdifficulties. The needs of residents with swallowing difficulties must be identified intheirNamasteCarepersonalprofiles,andtherightamountofthickenerforaquantityoffluidmustbeknownbytheNamasteCareworkerFoodtreatsPeoplewithdementiaoftenhaveasweettooth,whichisagoodwaytoincreasetheircalorieintake.Fruitisusuallywell-received,especiallyorangeslices,pineapplechunks,banana slicesor strawberries in the summer.Abowlofpureed fruit forpeoplewith
48
swallowingdifficultiesisimportant.Asmoothiemakerwouldbeverybeneficial.Otherexamples of food treats are small pieces of bread and butter and honey,marshmallows,cakeandicecream.Itisveryhelpfulifthecarehomemanagerensurestheunitisgenerouslystaffedforthefirst twoweeks of the Namaste Care programme. As highlighted previously, if at allpossible, themanager/most seniormemberof staff should aim tobepresent at thestartof the first fewsessions.This sendsoutamessageofcommitmentandensuresthatthecrucialtimewhenresidentsarebroughttoNamasterunssmoothly.Carestaffwillsoonadjusttothechangeandgetthehangofthenewroutine.Thestaffallocation forNamasteneedstobeclearlymarkedonthedutyrotasothateveryone knows who will be responsible for the Namaste sessions on each shift,includingtheweekends.The timingofyourcarehomesessionwilldependuponyour routine,e.g.what timebreakfast is served and what time lunch is ready. You should aim for the Namastemorningsessiontorunfortwohoursinthemorningandtwohoursintheafternoon.
PreparingfortheNamasteCaresessionTheNamasteCareworkershouldhaveabreakassoonasshe/hehasfinishedhelpingresidentswithbreakfasts,especiallyifshehasbeenworkingsince07.00hrs.Shethenprepares the Namaste space or room: this involves putting on music, scenting theroom, adjusting the lighting, preparing a trolley with supplies such as face flannels,towels,massageoilandhandsanitizer,ensuringthedrinksandfoodtreatsareready.Ithelpsthecareteamiftheactivityco-ordinatorcanassistwithsettinguptheroom.IfNamasteistotakeplaceinanareaofthediningroom,itshouldbescreenedoffduringthepreparationsoasnottodisturbresidentswhiletheyareeatingtheirbreakfast.Before each session commences, it is important that the Namaste Care workerbecomesfamiliarwiththedocumentationandisawareofanyrisksassociatedwiththeresidentswhowillbepartof theprogramme,e.g. swallowingdifficultiesor theneedforadiabeticdiet.When the Namaste space is ready, the Namaste Care worker will hang up the‘WelcometoNamasteCare’sign,andtellher/hiscolleaguesthatNamasteisopening.
Bringing,greetingandsettlingresidentsOncetheroomisready,allavailablestaffshouldspendthenextfifteenminutestakingall the Namaste Care residents to the Namaste room and helping to settle themcomfortably.
49
A vital part of the care programme is for the Namaste Care worker to greet eachresidentbynameandwelcomethemtotheNamasteroom/space.Eachresidentmustberecognisedwithrespectasanindividualperson,andatouchorhugwillusuallybeappreciated. The person with dementia will recognise that something different ishappening.NamebadgeTheNamasteCareworker should introduceher/himselfevery session and should bewearinganamebadgeinalargefontthatresidentscanread.ComfortTheNamasteCareworkerand the careworkerwhobrings the resident to the roommake the resident comfortable in an easy chair. It often takes two people to getsomebody comfortable, so the escort stays until the resident they have brought issettled.Ifthereisnorecliningchairtheresidentmayneedsmallpillowsandperhapsafootstoolforsupport.Nooneshouldsitinawheelchairunlessithasbeenindividuallydesignedfortheperson.Afterpositioningtheresident,theNamasteCareworkertuckstheresidentupwiththeresident’sownblanket/quilt.Theblankets/quiltsTuckingablanketoverthekneesoftenseemstobecomfortingandhelpspeoplefeelsafe.Also,forresidentswhoareabletogetup,havingablankettuckedaroundtheirkneesisacueforthemtostayinthechair.Immobileresidentsoftenfeelthecoldandaregladofextrawarmth,even insummer,butbecarefulthepersondoesn’tgettoohotTheblanket/quiltandpillowsshouldbereservedfortheindividual,labelledandkeptina named storage bag so that there is no ‘sharing’ and cross-infection. The blanketsshouldonlybewashedwhennecessarysotheykeepfluffyandsoft.PainassessmentSettlingtheresidentsistheidealtimetoassessthemfordiscomfortandpain.Signsofdiscomfort include whether the resident flinched or moaned when they moved,whether it was difficult to position them comfortably and whether they lookcomfortable.There isnopoint inworkingtoengagetheresident inactivity iftheyare inpain.SeeSection Eight for information re pain assessment tools. If the Namaste Care workerassesses that the resident is in pain, she/he should involve the nurse to ensure theresident’spainisappropriatelymanaged.
FoodtreatsanddrinksAlmost all residents with advanced dementia are at risk of malnutrition anddehydration. Good hydration is a key factor in keeping a person with advanceddementiahealthyandenablingthemtofightinfection.Whenpeoplearerelaxedtheyaremoreinclinedtoeatanddrink.Snackingisagoodwaytoputonweight.
50
Assoonasaresidenthasbeensettled,theNamasteCareworkershouldofferthemadrink.Peoplearemorelikelytoeatanddrinkwellwhentheyarerelaxedandenjoyingthemselves.Therefore,offeringfrequentdrinksandtemptingpeoplewithfoodtreatsthroughoutthesessionisapriority.Labellingthecupsisagoodwaytopreventgivingonepersonsomeoneelse’sdrink.In Namaste, the care worker can take advantage of spending long periods withresidentswithadvanceddementiabyhelping them to take sips and swigsof adrinkand to eat the food treats whenever they are awake and receptive. People withadvanceddementiatendtosleepalot.Thecareworkershouldtouchthemgentlyandthepersonwill usuallywakeup. If theydonot, the careworkermoves to thenextperson,butthenmaycomebackin15minutestoseeifthefirstresidentisreadyforcare.
MeaningfulactivityPersonalcare
Everyoneofus,almosteverydayofourlives,washesourhandsandfaceandbrushesourhair.Weusuallyfeelbetteronceitisdoneand,ifwehavetimetonotice,weenjoytheprocess.Forpeoplewhosememoryhasrecededfarintothepast,personalcarewillstillbeaconstantfeatureoftheirlifeexperience.GoingtobepamperedataspahasalwaysbeenaluxuryandtheaimoftheNamastesession is to capture that enjoyable experience. The personal care that is given inNamasteCare isdifferent fromthecarethat isgiventoresidentswhencareworkershelpthemwiththeirmorninghygieneneeds.
Individualisedcare-anexamplefromourexperience5
OnemanstartedtoprayaloudthefirsttimehecameintotheNamasteroomandhadhisfeetwashed.Hehadneverprayedlikethisbeforethoughhehadbeenatthecarehomeformonths,indeedhecommunicatedverylittleandwasoftenresistivetocare.Whenthecareworkerstoldhisdaughterwhathadhappened,shethoughthardandrememberedthatfootwashinghadbeenpartofthechurchritualinhishomecountry.
Thisresidenthadcleanfeetandwellcaredfornails;however,Namastecreatedaspecialatmosphere.TheNamastecareworkerwaswashinghisfeetgentlyandherintentionwastosootheandcomforthimratherthanmakehimclean.Thegentlefootwashingwithoutglovestriggeredreminiscenceandopenedaspiritualwindowforthisman.
WheneverpossibletheNamasteCareworkerwouldspendtimewashingthisresident’sfeetinNamastesessions.
NoglovesinNamasteNoglovesarewornduringNamasteCare.Thereisnoneedtowearglovesforpersonalcareunlessthereisariskofinfectionorthecareworkerhastocomeintocontactwith
51
bodyfluids.Takingglovesoffallowsforcloserskintoskincontactbetweenresidentsandcareworkers.HandsandfacewashwithawarmfaceclothThisshouldbealuxuriousexperiencefortheresidentandenjoyedbythecareworker.The aim is pleasure not cleanliness. The flannel should be hot/warm and ideally thetowelshouldbewarmedontheradiator (orwithahairdryer). Ifa residenthashandcontractures, then soaking theirhands,andmakingagentlewaterfallover themwilloftenallowthemusclestorelaxandthehandtoopenuplikeaflower.Theresident’shandsandfacemustthenbepatteddrywithawarm,fluffytowel.WhiletheNamasteCareworkerisgivingpersonalcareshe/heshouldconsciouslymakeeyecontactwiththeresidentandtalkappreciativelyandaffirmingly,e.g.thankingtheresident for thepleasureof theircompany,praisingbrighteyes, fineskin,ora lovelysmile.This isalsoachancetotalkabouttheresident’spast,usingexamplesfromthelifestorysuppliedbythefamily.
TouchTouch is a fundamental means of human communication and is probably the mostimportantelementoftheNamasteCareprogramme.Weallneedtouchaspartofourlifelongneedtobecaredfor,nurtured,valued,and,mostimportantly,loved.However,whenpeopleareelderlyorsick,theycanbecomestarvedoftouch.One-to-onecontactwithotherpeople is known tobe themostpowerful stimulus toengagement for people in the late stages of dementia48. Touch may involve juststrokingsomeone’shandorhairoritmaybeahandrubormassage(seetherapeutictouchhandout).Evensomethingassimpleasgentlybrushingsomeone’shaircanbeapleasurableandmeaningfulexperience.Inourevaluationstudy,wefoundthatmanyofourNamasteresidentsrespondedtotouchbygivingthecareworkerahandrubinreturnorreachingouttothem5.Theexperienceoftouchwasmutualinthatthecareworkerswere engaging in therapeutic touch ‘with’ the residents not just ‘for’ them,andbothenjoyedtheexperience.Nursesandcarerstouchthepeopletheycareforeveryday,butusuallywhiledoingatask, e.g. washing and dressing. In Namaste Care touch is used purposefully toconnectandcommunicatewiththeresidentandtoexpressaffectionandreassurance.Therapeutic touchhasbeen shown to improvenutritional intake, relieveanxiety andagitationandpromotecalmingandcherishingeffectsonpeoplewithdementia49.
Ifaresidentdoesnotliketouchthenthismustberespected.However,itisimportanttotryandfindotherwaystocommunicatewiththatperson.So,wheneveryonehasbeengreetedandsettledandhashada‘Namastewash’,ahandmassagemaybethebestformofmeaningfulactivityformanypeople.
52
Life-likedollsAftera livingperson,babyoranimal, thenextmostpowerful stimuluswithwhich toengageapersonwithdementiaisasimulatedperson,babyoranimal.Thisexplainsthepoweroflife-likedollstotransformthelifeofpeoplewithdementia.Ifawomanoraman formsanattachmentwitha life-likedoll, then thismayallay theiranxietiesandgivethemafocusfortheirloveandlongingtogivecareratherthanjustreceivecare;itmayalsogivethemasenseofcontrol.Aswitheveryactivity,knowingtheperson’slifestoryiscrucial.Forexample,apersonmaynothavehadchildren,mayhave lostababyorneverbeenabletohaveachild,andthereforeababymighthavenegativeassociations.Giving a doll to an adult is potentially problematic. It can be seen as infantilising orpatronising theperson. Itwouldbeunwise to try ‘doll therapy’withoutdiscussing itfirstwiththefamily.Itmayalsohelptogivethefamilywritteninformationaboutdolltherapy50.Ifthefamilychoosestoexplorewhethertheirrelativewillbenefitfromadoll(oradogor cat if that seems more appropriate), then a doll should be introduced to theresident.Thereshouldbenoattempttotrickthepersonintobelievingitisarealbaby.The doll shouldNOT be one that cries orwets itself! Ideally, the doll should have aslightsmile,andeyesthatclosewhenitislaidflatandopenwhenitsitsup.Thedollshouldbeintroducedasadoll,orperhapsleftbesidetheresidentsotheycanchoosetointeractwithitornot.Ifthepersonchoosestobelievethedollislife-like,thenthiscomesfromtheirownimagination,orperhapstheirneed.N.B. It is importanttohandlethedoll respectfully,e.g.notholding itbythefeetandswingingitontothetopofthecupboard,asthiscancausedistresstothepersonwhoisengagingwithitSimilarly, life-like cats and dogs can be a great source of comfort and pleasure topeople who have enjoyed animals all their lives. The same precautions should befollowed for life-likeanimalsas for life-likedolls. Introducinga life-likepet shouldbediscussedwithrelativesandthereshouldbenoattempttodeceivetheresident.Ifa residenthasadollor life-likeanimal theyenjoy, this shouldbegiven to themassoonastheyarriveintheNamastesession.Itmaybethattheygetsomuchpleasurefrom the doll/animal that it stays with them and is not just used in the Namastesession.Ifhoweverthedolloranimaldoesnotaccompanythematalltimes,itshouldbestoredintheirownbagwiththeirblanket/pillows.
OtheractivitiestostimulateNamasteCareresidentsAfterpersonalcareandahandmassageresidentswithadvanceddementiamaydozeoff.Themorningrush,beingwashedanddressedandhavingbreakfastcanbetiringforalltheresidents.Therefore,anapisnaturalandbeneficial.Residentswhoareagitated

53
and find Namaste Care relaxing may sleep, which will provide themwith relief andrespitefromtheiragitation.However, a room full of sleeping residents is not the aim of Namaste Care. TheNamaste Care worker should aim to engage people’s interest and attention withstimulating activities. For some this will just be enabling them to experience apleasant/interestingsensation.Whenintroducinganyactivity,takingtimetoexplainanddemonstratetotheresidentwhat the activity is about, is more likely to result in a positive response from theresident.RummageboxRummage boxes containing a collection of materials of different textures (e.g. silk,velvet, tweed, bubble wrap) can be brought to the resident who can explore andexperiencethevarioustextures.Iftheresidentisenjoyingtouchingthematerials,theymayliketostroketheirfaceandhandswiththem.Iftheresidentisnotinterested,therummageboxshouldbetakenelsewhere.MusicalinstrumentsThe Namaste Care worker can show the resident a tambourine or rainmakerinstrument,demonstratehowitworksandusesmilesandnodstoshowappreciationand enjoyment when it is played. Try to help them focus their attention on theinstrument.Iftheyarenotinterestedgiveup,butiftheylikeitleaveitwiththem.Youmaybeabletosupportthemtousethe instrumentbymovingyourhandswiththeirhands.MemoryboxA resident’s personal memory box provides an opportunity for the Namaste Careworkertositwiththeresidentandtalkaboutwhatiscontainedwithinit,reminiscingaboutthepas.Handlingfamiliarobjectscansometimestriggerreminiscence.ReadingaloudPoetryislikemusic;itlingersinthebrainandisoftenapowerfulemotionalexperience.Readingaloudmayhavebeenafamiliaractivityfortheresidentinthepast,andmanyolder people learned poems by heart at school, and nursery rhymes at home.Sometimes it can be hard to keep up a flow of conversationwhen the personwithdementia isunable toanswer. Readingaloudenables the careworker to keepupaflowoflanguagewhichmaybestimulatingorsoothingfortheperson.RangeofmovementGentlemovement tomusic is fun (dancing!), and creates a connection between theresidentandthecareworker. It isalsogoodfortheresident’scirculation,supplenessandmobility.
54
GettingactivebeforelunchTwenty minutes before residents have to leave Namaste Care in order to be madereadyforlunch,theNamasteCareworkerneedstomakesurethateveryoneisawakeandalertfortheirmeal.Playlighter,brightermusicThis is a good time to play residents’ favourite tunes, such as dancemusic or showtunesfromthe1940sand1950s.Choosesomethingrousingandcheerful.Initiate‘fun’activitiesBlowbubbles,tossaballoon,wearasillyhat,singanddance.BringtheworldintotheroomSeasonalflowersareaperfectwaytotryandorientatepeopletothetimeofyear.Forexample,abasinofgrassthathasbeenrecentlymownorautumnleavesorsnowcanallhelptoorientatethepersontothetimeofyear.Passingaroundasmallsofttoybirdthatchirpswhenpressedcanbringpleasure(fromtheRoyalSocietyfortheProtectionofBirdswww.rspb.org.uk).ClosingthesessionAtthecloseofthesessionothercareworkerswillcometotakeresidentsaway. TheNamasteCareworkermustsaygoodbyetoeachresidentinturn,usingtheirname,andthankingthemforcomingtotheNamastesession.TheNamasteCareworkermustthencompletetheattendanceformandtheNamasteactivitiesrecordforeachresidentatthesession.Anythingremarkablemaybewritteninthediary,or intheresident’snotes.TheNamasteCareworkerwilltidyupandgetready for theafternoon sessionbefore joining the restof the care staff tohelpwithlunch.
TheafternoonsessionThetimingoftheafternoonsessiondependsuponthecarehomeroutine.Somecarehomes reopen the Namaste room at 2 pm, while others like to start the afternoonsessionat3pm.Someresidentsneed to reston thebedafter lunchwhereasothersneedtolieonthebedratherthansitbecauseofskinproblems.Ifresidentsaresleepyintheafternoon,thenatleastinNamaste,whentheywake,therearepeoplearoundthem.The afternoon session follows a similar pattern to the morning session, but withdifferent activities. For example, foot soaking and foot rubs can replace the handmassageand,ifthereistime,nailcareand/orhaircarecanbeperformed.TheafternoonmayalsobeatimeforanatureDVDoranoldmusical.Thesessionwillclosewithalivelygoodbyetoeachindividual.AsummaryoftheNamasteCaredayisoutlinedbelow.
55
VisitorsOtherresidentsmay‘dropin’andvisittheNamastesession.AllshouldbewelcomedandiftheyarewillinggivenaNamasteexperience.Anyresidentmaybenefitfromthepeacefulatmosphereandthesensoryapproach,especiallyiftheyareanxious.Familyvisitors/friendsarealwayswelcomeintheNamasteroom,butiftheyprefertovisit their relative somewhere else in the care home, then that should be arranged.Familyvisitorsusuallyenjoythecareprogrammeandmeetingotherrelatives,andtheyshouldallbeencouragedtojoininwiththeactivities.Theywillquicklysensethattheatmosphere in Namaste is peaceful and calm and will understand the need to talkquietly.OthermembersofthecarestaffarealsowelcomeintheNamasteroomandshouldbeencouraged to participate in the programme’s activities. They must respect theatmosphereintheroomandtheintention‘tohonourthespiritwithin’eachpersonintheroom,i.e.resident,stafforrelative.
ProtectingtheNamastespaceThemanager’s authority is needed to protect theNamaste space. Namaste needs acalmandpeacefulatmosphere, verydifferent fromthe restof thecarehomewhereeveryone is rushing around trying to get things done. There should be no avoidableinterruptions to Namaste, careworkers and nurses should be respectful of the careprogramme and try not to disturb the group unnecessarily. If staff need to go inwithoutstayingtojointhegroup,theyshouldtrytokeeptheirvoicesdownandnottodisrupttheatmosphere.Box6.1givesanoverviewofamorningandanafternoonNamastesession.Thesearesuggestionsforatypicalday.Itisalwaysimportanttoindividualisethescheduleandbeflexible.Seasonalchanges,staffchangesandresidentchangesmustberespectedandtheschedulereorganised.
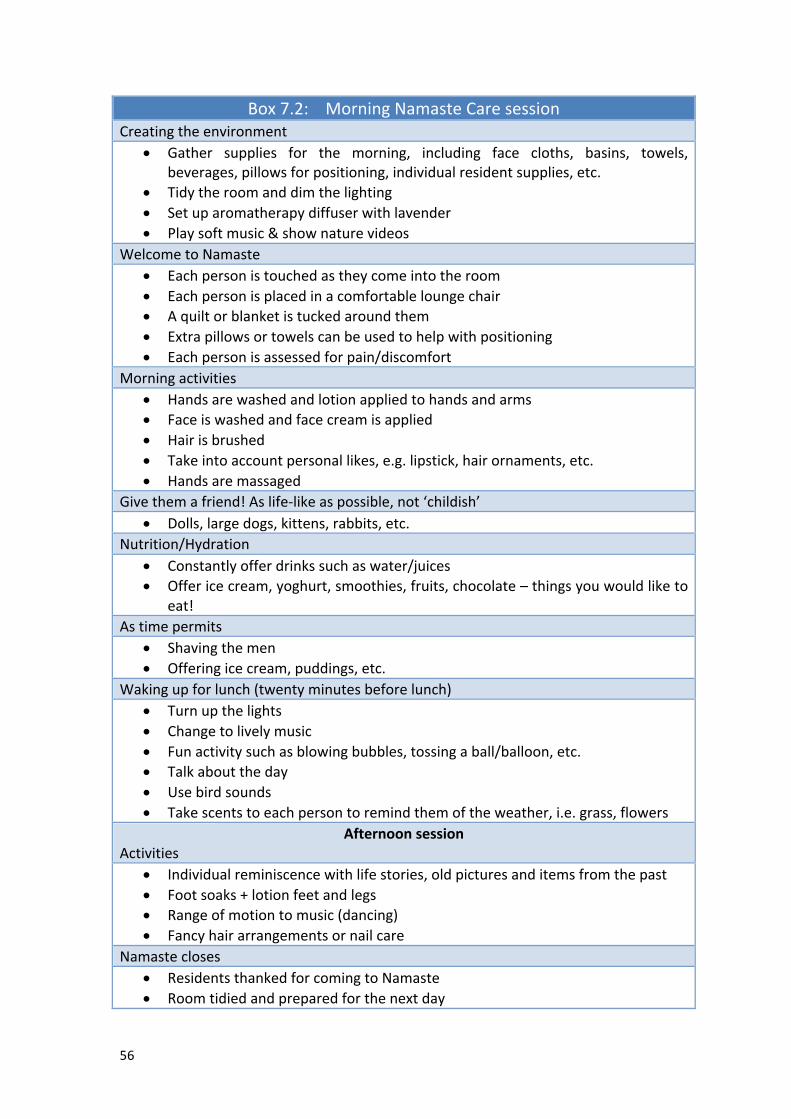
56
Box7.2:MorningNamasteCaresessionCreatingtheenvironment
• Gather supplies for the morning, including face cloths, basins, towels,beverages,pillowsforpositioning,individualresidentsupplies,etc.
• Tidytheroomanddimthelighting• Setuparomatherapydiffuserwithlavender• Playsoftmusic&shownaturevideos
WelcometoNamaste• Eachpersonistouchedastheycomeintotheroom• Eachpersonisplacedinacomfortableloungechair• Aquiltorblanketistuckedaroundthem• Extrapillowsortowelscanbeusedtohelpwithpositioning• Eachpersonisassessedforpain/discomfort
Morningactivities• Handsarewashedandlotionappliedtohandsandarms• Faceiswashedandfacecreamisapplied• Hairisbrushed• Takeintoaccountpersonallikes,e.g.lipstick,hairornaments,etc.• Handsaremassaged
Givethemafriend!Aslife-likeaspossible,not‘childish’• Dolls,largedogs,kittens,rabbits,etc.
Nutrition/Hydration• Constantlyofferdrinkssuchaswater/juices• Offericecream,yoghurt,smoothies,fruits,chocolate–thingsyouwouldliketo
eat!Astimepermits
• Shavingthemen• Offeringicecream,puddings,etc.
Wakingupforlunch(twentyminutesbeforelunch)• Turnupthelights• Changetolivelymusic• Funactivitysuchasblowingbubbles,tossingaball/balloon,etc.• Talkabouttheday • Usebirdsounds• Takescentstoeachpersontoremindthemoftheweather,i.e.grass,flowers
AfternoonsessionActivities
• Individualreminiscencewithlifestories,oldpicturesanditemsfromthepast• Footsoaks+lotionfeetandlegs• Rangeofmotiontomusic(dancing) • Fancyhairarrangementsornailcare
Namastecloses• ResidentsthankedforcomingtoNamaste• Roomtidiedandpreparedforthenextday
57
Namasteintheresident’sroomWhenaresidentisunwell
NamastecanbetakentopeopleintheirownroomswhentheyareunabletocometotheNamastesession,e.g.iftheyareunwell.AtrolleycangofromroomtoroomwithaportableCDplayer,somemoisturisingcreamand,forexample,asingingbirdtoengagetheresidentorwhateverisknowntopleasethem.IfaresidentisdistressedNamasteCarewilloftensoothesomeonewho isagitatedordistressed. Ifaperson isnot copingwith beingwith other people in theNamaste session, then tryingmusic,fragrance and therapeutic touch in their own room may enable them to relax andbecome calm. It may be possible to accustom the person to Namaste Care andgraduallyintroducethemtothegroup.WhenaresidentisdyingWhenaresidentisdying,theNamasteCareworkercanbringthemusicandfragrancetheyenjoyedinNamastetotheirroomandallpersonalcarecanbegivenasagentle,pleasurable experience. Family can be shown how to do hand massage and mouthcare,ifthatisappropriate,becauseinvolvementinphysicalcareisoftenbeneficialtofamily/friends. Religious items may be comforting to the resident as well as thefamilies.Religiousmusicthatwaspartofwhateverchurchtheybelongedtomightbeappropriate. When someone is dying, ‘honouring the spirit within’ is the guidingprincipleoftheircareAfter-deathcare‘Honouringthespiritwithin’continuesbeyondthemomentofdeath.Careworkerswillprovide the same respectful, lovingcare for thebodyof thepersonwhohasdiedastheydidforthelivingperson.Ideally,whentheperson’sbodyisfinallytakenfromthecarehome,acareworkerwillwalkwiththemoutofthehometothefuneraldirector’svehicle,sothatthepersonisaccompanieduntiltheyfinallyleavethecarehome.CommunicatingnewsofthedeathPlacingaframedphotographofthepersonwhohasdiesinthehallwayisarespectfulwayofcommunicatingnewsofthedeathtovisitorsandstaffwhohavebeenoffduty.Ofcourse,youmustseekthepermissionofthefamilyforthis.AfterdeathreflectionThedeathofacarehomeresidentisoftenfeltdeeplybythecarestaff,andfollowingthedeathofaNamasteresidentthereshouldbeanafterdeathmeeting/debrief.Thisisanopportunitytoreflectonthelifeofthepersonwhohasdiedandthefeelingsofloss staffmaybeexperiencing. It isalsoanopportunity to reflectonhowthedeathwas managed. What went well? What didn’t go so well? What could be donedifferently another time? What could be learned? And what could be changed toimprovepractice?

58
SectionEight
Achievingcomfortandpleasure
Sectionaims:• ToexplaintheroleofpainrecognitionandmanagementintheNamasteCare
programmeo Todescribetheuseofascaleforassessingpaininpeoplewhoareunableto
communicatetheirpain• Tohighlighttheneedforawarenessofdepressioninpeoplewithadvanced
dementia• Todescribetheuseofascaleforassessingdepressioninpeoplewithadvanced
dementiawhoareunabletocommunicateclearly.If someone is in pain then they cannot be comfortable! Quality of life is almostimpossibletoachieveifsomeoneisindistress.Therefore,assessingandmanagingpainanddistressisanecessarypartoftheNamasteCareprogramme.Thissectiondealswithpainanddepression,whicharetwocommonreasonsforpeoplewithdementiatofeeluncomfortableandtobeunabletoenjoypleasurableactivities.However, if someone with dementia appears distressed and agitated, it is alsoimportanttorememberothersimplecausesofphysicaldistresssuchasbeingtoohotorconstipated.
PainUntreated pain can have a major impact on the quality of life of people withdementia51. Common causes of pain in people with dementia include arthritis,neuropathiesandpressureulcers52.Assessingsymptomsisparticularlydifficultinpeoplewithadvanceddementiawhoareunable to communicate their distress verbally. There is evidence24 that pain is oftenneglected in people with dementia because the person often does not ask for painrelief,andbecausetheymayexpresstheirpaininunusualways,e.g.throughagitationorwithdrawal.Aswellasthesechallenges,there isamisconceptionthatpeoplewithdementia do not experience pain in the same way as people withoutdementia9,11,24,53,55..Effective management of pain can lead to significant improvement in symptoms ofagitationand/oraggressioninresidentswithdementia.Itshouldnotbeassumedthatthe behavioural and psychological symptoms of agitated residents are relatedexclusivelytotheirdementia55.
59
TheNamasteCareworkers,whospendhoursatatimewithresidentswithadvanceddementia,areintheperfectpositiontoobserveforsignsandsymptomsindicatingpainanddistress.
AssessmentofpainIthasbeenfoundthatmanycareworkersdonotknowhowtoassesspaininsomeonewithadvanceddementia55,56.Itisbestpracticetousepain-assessmentscalesaspartofanoverallpain-managementstrategyforresidentswithinthecarehome.Usingapainassessment scale has been shown to help care workers detect pain and increasesrecognitionofpaincomparedwithnotusingapainassessmentscale.Thereare severalpain-assessment scales that canbeused forpeoplewithadvanceddementia who are unable to communicate their pain. No pain-assessment scale isperfect. You should introduce the one that you feel would work best for your careworkers.Includingstaffinthedecision-makingprocesswillhelptoensurethattheyarecommittedtoitsuse.Examples of well-constructed, reliable pain-assessment scales include the PainAssessment in Advanced Dementia Scale (PAINAD)57, the Doloplus-258, and the PainAssessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC)59 ,and the Abbey Pain Scale60. The assessment scales usually require care workers toassessresidentsduringmovementandwhencarryingoutpersonalcareorprocedures,becausethesearethetimeswhenresidentstendtoexperiencemorepain.AnoverviewofthePainAssessmentinAdvancedDementiaScale(PAINAD)isprovidedbelow.PainAssessmentinAdvancedDementiaScale(PAINAD)57
PAINAD is quick and simple to use and helps to educate staff about the types ofbehaviourthatmayindicatethatresidentsareinpain.PAINAD has been developed for use with people who are unable to use self-reportmethods to describe pain, e.g. people who are cognitively impaired and unable tocommunicate. Itcoversfivebehavioural items(seeBox8.1),whichareeachassessedandscoredduringperiodsofactivity,e.g.whenrepositioning,walkingortransferring.Thebehavioural itemsare scored from0–3andscores foreachof the five itemsareaddedtogetherforatotalnumericalscore.
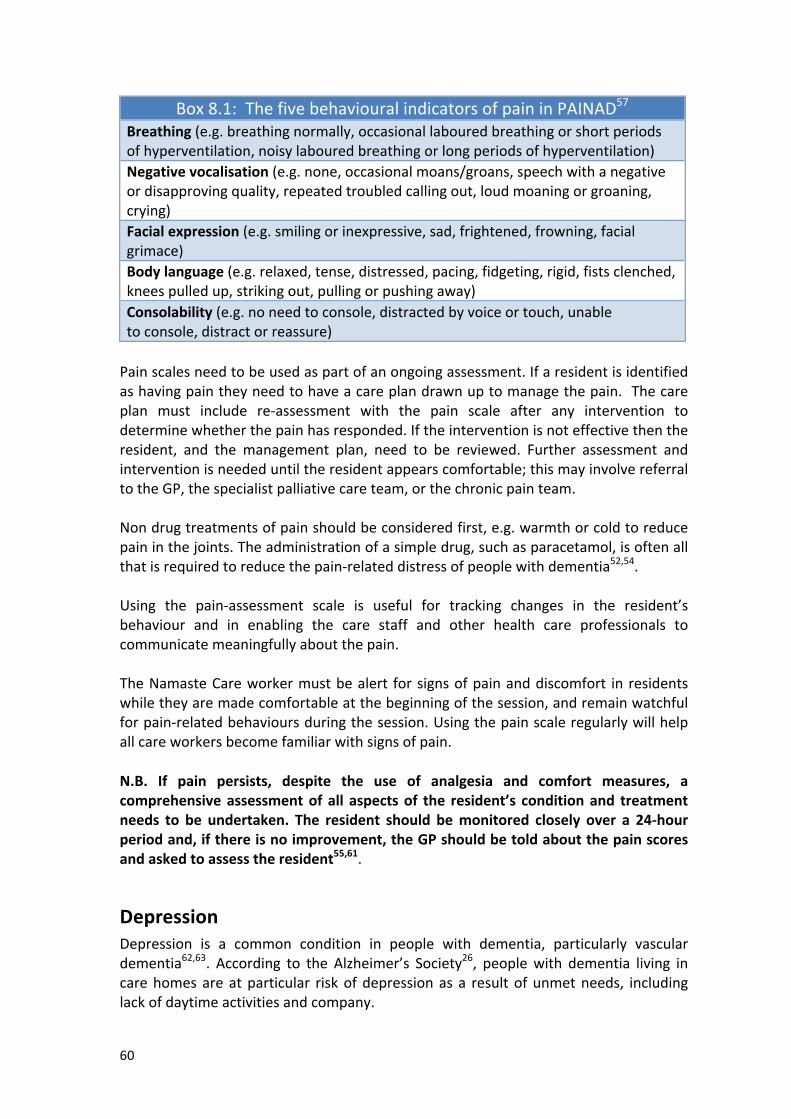
60
Box8.1:ThefivebehaviouralindicatorsofpaininPAINAD57
Breathing(e.g.breathingnormally,occasionallabouredbreathingorshortperiodsofhyperventilation,noisylabouredbreathingorlongperiodsofhyperventilation)Negativevocalisation(e.g.none,occasionalmoans/groans,speechwithanegativeordisapprovingquality,repeatedtroubledcallingout,loudmoaningorgroaning,crying)Facialexpression(e.g.smilingorinexpressive,sad,frightened,frowning,facialgrimace)Bodylanguage(e.g.relaxed,tense,distressed,pacing,fidgeting,rigid,fistsclenched,kneespulledup,strikingout,pullingorpushingaway)Consolability(e.g.noneedtoconsole,distractedbyvoiceortouch,unabletoconsole,distractorreassure)Painscalesneedtobeusedaspartofanongoingassessment.Ifaresidentisidentifiedashavingpaintheyneedtohaveacareplandrawnuptomanagethepain.Thecareplan must include re-assessment with the pain scale after any intervention todeterminewhetherthepainhasresponded.Iftheinterventionisnoteffectivethentheresident, and the management plan, need to be reviewed. Further assessment andinterventionisneededuntiltheresidentappearscomfortable;thismayinvolvereferraltotheGP,thespecialistpalliativecareteam,orthechronicpainteam.Nondrugtreatmentsofpainshouldbeconsideredfirst,e.g.warmthorcoldtoreducepaininthejoints.Theadministrationofasimpledrug,suchasparacetamol,isoftenallthatisrequiredtoreducethepain-relateddistressofpeoplewithdementia52,54.Using the pain-assessment scale is useful for tracking changes in the resident’sbehaviour and in enabling the care staff and other health care professionals tocommunicatemeaningfullyaboutthepain.TheNamasteCareworkermustbealert forsignsofpainanddiscomfort in residentswhiletheyaremadecomfortableatthebeginningofthesession,andremainwatchfulforpain-relatedbehavioursduringthesession.Usingthepainscaleregularlywillhelpallcareworkersbecomefamiliarwithsignsofpain.N.B. If pain persists, despite the use of analgesia and comfort measures, acomprehensiveassessmentofall aspectsof the resident’s conditionand treatmentneeds to be undertaken. The resident should bemonitored closely over a 24-hourperiodand,ifthereisnoimprovement,theGPshouldbetoldaboutthepainscoresandaskedtoassesstheresident55,61.
DepressionDepression is a common condition in people with dementia, particularly vasculardementia62,63. According to the Alzheimer’s Society26, peoplewith dementia living incarehomesareatparticular riskofdepressionasa resultofunmetneeds, includinglackofdaytimeactivitiesandcompany.
61
Depressioncanbedifficulttoassess,especiallyifresidentshavemoderatetoadvanceddementia and have difficulties communicating63. Therefore, carers need to becomemore aware of the causes and signs and symptoms of depression. There are manypossible causes of depression in both people with and without dementia63. Theseinclude:
• Geneticpredispositiontodepression• Pasthistoryofdepression.• Effectsofcertainillnesses(i.e.thereisanincreasedriskofdementiain
Parkinson’sDisease)• Side-effectsofmedication• Bereavement• Lackofactivities,leadingtofeelingsofboredomandaimlessness• Lackofsocialsupportorsocialisolation• Traumaticorupsettingevents
Depressionaffectspeopleindifferentwaysandtodifferentdegrees.Someofthemorecommon signs and symptoms of depression seen in older people include thefollowing62,63:
• Lossofappetiteandweightloss• Tirednessorlossofenergy• Achesandpainsthatappeartohavenophysicalcause• Sleepdisturbance(e.g.earlymorningwakening)• Difficultyconcentrating,understanding,rememberingormakingsimple
decisions• Lossofengagement,interestorpleasureinactivitiesthatwereonceenjoyed• Feelingsofisolation• Deteriorationinfunction• Achangeinmood(i.e.moreirritableordistressed)• Increasedanxiety,restlessnessandagitation• Feelingsoflowself-esteem,worthlessnessorundueguilt• Thoughtsofdeathandsuicide• Agitation.
Some of these symptoms are very similar to some of the symptoms experienced bypeoplewithdementia,which increasesthedifficultycarestaffcanfind inrecognisingclinicaldepressionintheirresidentswithdementia.However,ifcarestaffobservethatapersonwithdementiaseemstofinditevenharderthanusualtorememberthings,orisevenmorewithdrawn,orbecomesmoreanxiousor irritable particularly in the morning, then they should consider the possibility ofdepression, once they have ruled out a physical cause such as infection or the sideeffects of drugs. Depressionmay alsoworsen behavioural symptoms in peoplewithdementia, presenting as irritability, problems sleeping or refusal to eat. In the laterstagesofdementia,depression tends toshow itself in the formofdepressive ‘signs’,suchasearlymorningwaking,reducedsocialengagementandweightloss62,63,65.
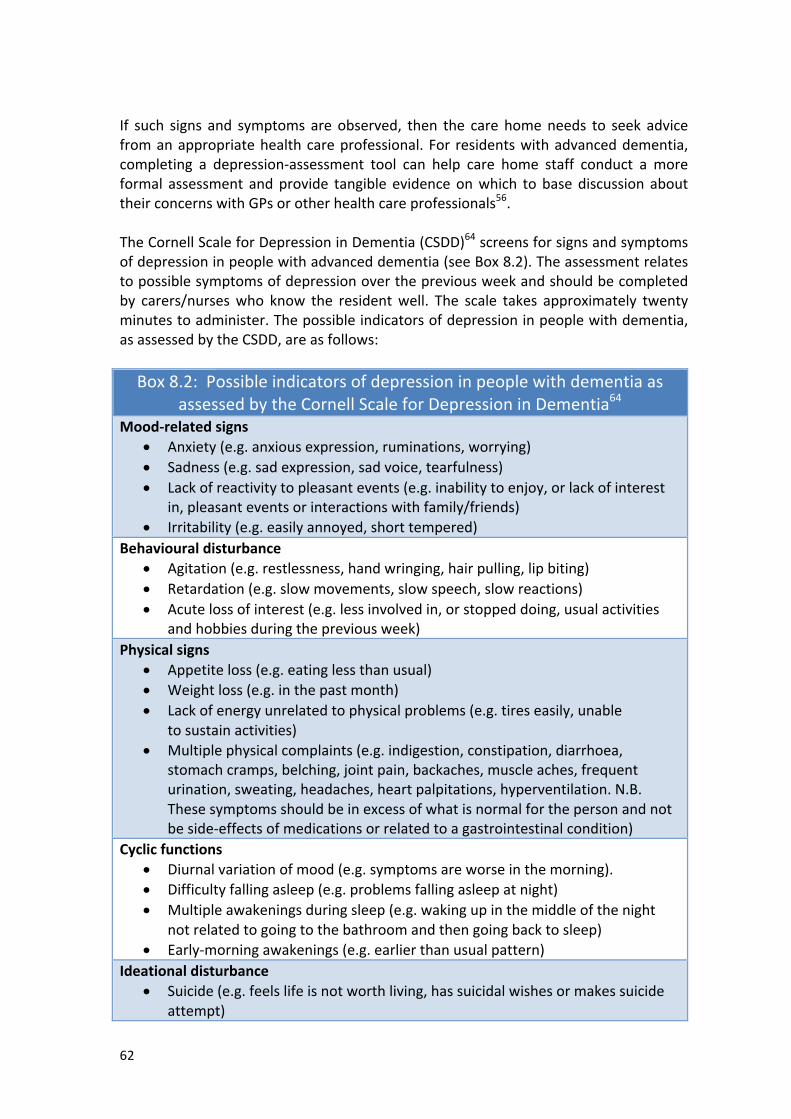
62
If such signs and symptoms are observed, then the care homeneeds to seek advicefromanappropriatehealthcareprofessional.For residentswithadvanceddementia,completing a depression-assessment tool can help care home staff conduct a moreformal assessment andprovide tangible evidenceonwhich tobasediscussion abouttheirconcernswithGPsorotherhealthcareprofessionals56.TheCornellScaleforDepressioninDementia(CSDD)64screensforsignsandsymptomsofdepressioninpeoplewithadvanceddementia(seeBox8.2).Theassessmentrelatestopossiblesymptomsofdepressionoverthepreviousweekandshouldbecompletedby carers/nurseswho know the residentwell. The scale takes approximately twentyminutestoadminister.Thepossibleindicatorsofdepressioninpeoplewithdementia,asassessedbytheCSDD,areasfollows:Box8.2:Possibleindicatorsofdepressioninpeoplewithdementiaas
assessedbytheCornellScaleforDepressioninDementia64
Mood-relatedsigns• Anxiety(e.g.anxiousexpression,ruminations,worrying)• Sadness(e.g.sadexpression,sadvoice,tearfulness)• Lackofreactivitytopleasantevents(e.g.inabilitytoenjoy,orlackofinterest
in,pleasanteventsorinteractionswithfamily/friends)• Irritability(e.g.easilyannoyed,shorttempered)
Behaviouraldisturbance• Agitation(e.g.restlessness,handwringing,hairpulling,lipbiting)• Retardation(e.g.slowmovements,slowspeech,slowreactions)• Acutelossofinterest(e.g.lessinvolvedin,orstoppeddoing,usualactivities
andhobbiesduringthepreviousweek)Physicalsigns
• Appetiteloss(e.g.eatinglessthanusual)• Weightloss(e.g.inthepastmonth)• Lackofenergyunrelatedtophysicalproblems(e.g.tireseasily,unable
tosustainactivities)• Multiplephysicalcomplaints(e.g.indigestion,constipation,diarrhoea,
stomachcramps,belching,jointpain,backaches,muscleaches,frequenturination,sweating,headaches,heartpalpitations,hyperventilation.N.B.Thesesymptomsshouldbeinexcessofwhatisnormalforthepersonandnotbeside-effectsofmedicationsorrelatedtoagastrointestinalcondition)
Cyclicfunctions• Diurnalvariationofmood(e.g.symptomsareworseinthemorning).• Difficultyfallingasleep(e.g.problemsfallingasleepatnight)• Multipleawakeningsduringsleep(e.g.wakingupinthemiddleofthenight
notrelatedtogoingtothebathroomandthengoingbacktosleep)• Early-morningawakenings(e.g.earlierthanusualpattern)
Ideationaldisturbance• Suicide(e.g.feelslifeisnotworthliving,hassuicidalwishesormakessuicide
attempt)
63
• Self-depreciation(e.g.self-blame,poorself-esteem,feelingsoffailure)• Pessimism(e.g.anticipatestheworst)• Moodcongruentdelusions(e.g.delusionsofpoverty,illness,orloss,perceives
illnessaspunishment)The usual treatment for depression is psychological therapies in combination withantidepressants.Takingpartinpsychologicaltherapiesmaybedifficultforpeoplewithmoreadvanceddementia. However, other strategies include increasing the amount of time spentparticipating in activities that the person enjoys and planning regular activities withotherpeople,becausesocial isolationcanmakedepressionworse. Ithasbeen foundthat residentswith dementia express happiness over seven timesmoreoftenduringstructuredrecreationaltimethanduringunstructuredtime66.The Namaste Care programme can help to both reduce the risk of residents withadvanced dementia developing depression andmanage depression in residentswhohavedepression.
64
SectionNine
Developing,evaluatingandsustainingNamasteCare
Sectionaims:
• TosuggestwaystodevelopandsustaintheNamasteCareprogrammewithinyourcarehome
• TodescribethechallengestotheNamasteCareprogrammeyoumaymeetinyourcarehomeandsomewaysofovercomingthem
• TosuggesthowbesttoevaluatetheeffectsoftheNamasteCareprogrammeonyourresidentswithadvanceddementia.
‘Growing’theNamasteCareprogrammewithinyourcarehomeDailysupportandsupervisionTheoverall aimof this toolkit is to help youmakeNamaste Care a key part of dailyroutineatthecarehome.ThemanagerorleadnurseshouldvisittheNamastesessionsdailytoensurethatresidentsareenjoyingthesessionandtooffertheNamasteCareworker support. The manager/nurse should ensure that residents are comfortablyseated, the Namaste Care worker is wearing the large font name badge, music isplaying,andtheroomlooksattractiveandcolourfulandisscented.TheNamasteCareChecklistwillhelpyou.The manager/nurse should also check that the Namaste Care worker is busy andoccupied with residents, there is hand sanitiser in the room, residents have theirpossessions stored individually to prevent cross-infection, and the food treats arecoveredwhentheyarenotbeingused.WeeklymeetingsWhile the Namaste Care programme is being introduced, weeklymeetings with theNamaste core teamwill help themanager and the Namaste Champions succeed. Inthesemeetings, everybodyneeds to reportonprogress andanyproblems thathavearisen.Themeetingshouldfocusonwhatisworkingwell,whatisnotworkingwellandhowthingscanbeimproved.Thesemeetingsareencouragingandmotivatingforstaff.It isespecially importanttotackleanyconcernsfromcarehometeammemberswhoareopposedtochangingpracticeandintroducingNamaste.Plansneedtobemadeforthefollowingweek.Responsibilitiesfordifferentaspectsofthecareprogrammeshouldbesharedoutandreviewedatthenextweek’smeeting.The team needs to work out strategies for managing some of the challenges (seebelow) thatarise in theearlydaysof introducing thecareprogramme.ThemeetingsarealsoatimetoreflectontheimpactoftheNamasteCareprogrammeonindividual
65
residents and the care home as awhole. It isworthwhile asking family and visitingprofessionalsforfeedback.Theweeklymeetingsshouldcontinueforas longastheteamfindsthemuseful;thentheycanbecomefortnightlyandthenmonthly.MonthlyNamastechecklistsandmonthlyNamastemeetingsBefore the monthly meeting, the nurse manager should go through the Namastechecklist, to ensure that the care programme is on course. The boxes that are notticked need to be discussed at themonthlymeeting, sorted out and prioritised. Forexample,ifelectricequipmentneedstobechecked,thatmustbeapriority,butifthereisnoDVDplayer,thatissomethingforlong-termplanning.Aftertheprogrammehasstarted, itmaybehelpfultofocusondifferentelementsofNamaste (seethe introductiontothis toolkit)oneata time. Forexample,youcouldfocusoncomfortandlookathowcomfortableyoucanmakeeachresident.Thismightinvolvelookingatseating,orfindingsuitablecushionstosupportaperson’shead,oracontractured limb. Youmightthinkabout looseningtightclothingorremovingshoesduringNamaste.Warmingtowelscanenhancethesenseofcomfortafterawashoramassage. Pain assessment will also be considered under this topic, and this mayinvolveateachingsessionforcareworkersonusingapainassessmentscale.OnceNamasteiswellestablished,monthlymeetingswillprimarilybeaboutdevelopingthe care programme for individual residents, extending the range of activitiesundertakenandmakingtheprogrammemoreflexible.ReflectingwiththecarestaffThemanagerneedstokeeptheNamasteCareprogrammeatthetopoftheagendaforallteammeetingsinthefirstfewmonthsandmustsupportstafftoreflectonchangesinpractice.Reflectingonchangesinpracticeisanimportantpartofcreatingchange.Itis importantforstafftoseeandfeelthebenefitsfortheirresidents.Therefore,everymemberofstaffshouldspendatleasttwentyminutesinaNamastesessionduringthefirstmonthofimplementation.It is important to address any concerns raised by staff as soon as possible beforemisconceptionsandrumoursarise.ScepticalstaffareoftenthosewhohavetheleastunderstandingofNamasteCare, so it isespecially important toensure theyattendasessionandlearnfromexperience.Itisessentialtomakesurethesuccessstoriesaboutchangeinindividualresidentsarepassedontoallmembersofstaffwithinthecarehome.WritingamissionstatementWriting a mission statement for the Namaste Care programme (see Boxes 9.1; 9.2)involvesaskingstafftoputtheirobservations, ideasandbeliefsaboutthebenefitsofNamasteCareintowords.Theexercisebuildsonreflectiveworkandhelpstoembedthechange.Theprocessofrecognizingandarticulatingthepositivechangesseenwith
66
Namastehelpseveryonetovaluethecareprogramme.ThemissionstatementshouldcapturewhatstaffvalueintheNamasteCareprogramme.Atateammeetingitisimportanttoinformallthestaffthatyouareplanningtowriteamission statement for the Namaste Care programme in your care home. You couldshowthemtheexampleofaNamasteCaremissionstatementinJoyceSimard’sbook3,as well as the two examples below that were written by UK care homes that havealreadyimplementedNamasteCare.Youcouldstartbyaskingeveryonefortheir impressionsofNamasteCareandwritingdownwhattheysayonaflipchart.Copydownthewordstheyuseandkeepthem.Putup a notice in the office and ask everyone to write downwhat they like and valueaboutNamaste.Sitdownwith theNamastecore teamandstart toput togetheramissionstatementusing the thoughts andwords of your own team. Take this draft back to thewholeteamfortheircommentsandfurthercontributions.Thengobacktothecoreteamandrepeattheprocessuntilyouhaveamissionstatementthateveryonecansignuptoandofwhichtheyfeelproud.Themissionstatementisespeciallyusefulforinformingnewstaff,relativesandvisitorsabouttheNamasteCareprogrammeandexplainingthebenefitsforresidents,staffandrelatives.YoucouldframethemissionstatementandhangitintheNamasteroom.
Box9.1:MissionstatementfortheNamasteCareprogrammeatAmberleyLodgeNursingHome
AtAmberleyLodgeweembraceNamasteandwhatitstandsforNamasteCareisadeepexpressionofrespectanddignitythatrecognisesthequalityofpeoplewithadvancedementiaItisaglowinglightofcompassionthathonoursthespiritwithinWebelievethatthespiritineachindividuallivesregardlessofphysicalandcognitivestatusOuraimisto:
Ø Treateveryindividualinauniqueway,recognisingtheirindividualdifferences,and
Ø Nurtureeachpersonthroughlovingtouchandmeaningfulactivitiesinthepresenceofothers
Wefocusoncomfort,wellbeingandqualityoflifeWebelieveNamasteCarecanbegivenanywhereinthehomeWedoeverythinginourpowertomaketheirpassinggentleandpeacefulatthetimeofendoflifeandsurroundedbypeoplewhocare
67
Box9.2:MissionstatementfortheNamasteCareprogrammeatLakesideNursingHome
AtLakesideNursingHomewerecognisethatourresidentswithadvanceddementiaareallpeoplelikeourselves,andwewanttogivethemthecarewewouldwantintheirsituation.TheNamasteCareprogrammeenablesustoreachouttoeachotherthroughlovingtouch,meaningfulactivitiesandthepresenceofothers.Wewantourresidentstofeelathomeandtofeelthattheyarelovedandrespected.Wewantthemtobecomfortable,calmandpeacefulandwewilltrytomakepleasureandenjoymentpartoftheireverydayexperience.WorkingtogetherasateammeansthatresidentsintheNamasteCareprogrammereceiveexcellenthealthcarewithaholisticapproachfocusingoncomfortandqualityoflife.Wealsobelievethatlastdaysarepreciousandtheteamwillmakeeveryefforttoensurethatwhenourresidentsdietheirpassingispeacefulanddignifiedandthattheyaresurroundedbypeoplewhocare.
ChallengesStaffshortages
Staff shortages are the most common challenge to the Namaste Care programme.Whensomebodyisoffsickorhashadtogoonescortdutyunexpectedly,staffmaysay,‘We can’t doNamaste because of the staff shortage’. Nobody says, ‘Wewon’t havelunch because there’s a staff shortage’, or ‘Wewon’t give outmedications becausethere’sastaffshortage’. Peoplewithadvanceddementianeedemotional interactionand sensory stimulation every day – Namaste meets social, emotional and sensoryneeds.ThesituationcanbeovercomebythedeterminationofthestafftoinvolvethemselvesintheNamastesessions.However,staffhavetobelieveinthevalueofthesessions.IfthereislackofcommitmentthenNamasteisnotgoingtohappen.Strategyforcopingwithstaffshortages
• Askmembersofthewidercarehometeam(e.g.themanageroradministrativestaff)tostepinforshortperiods,e.g.twentyminutesatatime,toreleasetheNamasteCareworkerifshe/heisdesperatelyneededsomewhereelseforashorttime
• IfthepersonwhoisfillinginisnotamemberofthecareteamtheycanprovideapresenceintheNamasteroomandthereisnoreasonwhytheycannotputhandlotiononsomeone’shand,brushhair,changethemusicandchatwithresidents
• ConsiderincreasingthenumberofresidentsintheNamastesessionsothatmorepeoplearelookedafterinthegroup.
68
The psycho-social and spiritual needs of residents with advanced dementia are asimportant as their physical needs, and keeping the Namaste Care programme goingshouldbeseenasapriority.
ChallengeResidentswithadvanceddementiawhodon’tsettleinaNamasteCaresessionInevitablytherewillbetheoccasionalresidentwhodoesnotsettlewhentheyarefirsttakentotheNamastesessions.Somepeoplearetooagitated,distressedoranxioustositdown,evenforamoment,othersmaybenoisyanddisruptivesothattheydestroyeveryoneelse’speace.Strategy
• TrytobringtheseresidentstoNamastesessions.YouwillbesurprisedattheresponseofthoseresidentswhoyourstaffwilltellyouwillcauseissuesintheNamasteroom,orwhostafffeelwillnotlikeit.
• TheNamasteChampionshouldtrytofindactivitieswithwhichtoengagethepersonbyreferringtotheirlifestoryandaskingadvicefromthefamilyandcareworkers.
• IfsomeoneisdisruptivefortenminutesthentheyshouldbetakenoutoftheNamasteroomsothesessionisnotruinedfortheothers.
• TheNamasteChampionshouldfindatimetodoone-to-oneworkwiththispersonintheirownroom.
• JustbecausesomeonedidnotappeartolikeNamastethefirsttime,doesnotmeantheyshouldnottryitagain.
• OftenpeoplebecomegraduallyaccustomedtoNamasteandbuildupthelengthoftimetheyspendinthecareprogramme.
ChallengeInvolvingfamiliesfromtheoutsetFamilies and friends can be a great source of support for Namaste. Family visitorsusuallyenjoycoming intotheNamasteroom,andthepraisetheygivetostaffwhenthey realize what they are doing is beneficial for staff morale. However, iffamilies/friendsarenot involvedwiththecareprogrammefromtheoutsetthentheymay not let their loved ones go into the Namaste sessions. This is a waste of thisinvaluableresource.
ChallengeUsingNamastefamilymeetingstothefullInthefamilymeetings,sometimesstaffonlyexplainabouttheNamastesessionsanddonotusetheopportunitytohelpfamily/friendsunderstandthatthepersontheylovehas advanced dementia, and therefore has limited life expectancy. Failure tounderstandthatapersonwithadvanceddementiaisinthelaststagesoftheirlifecanleadtoaseriesofcrisisdecisionsforthefamilywhentheperson’sconditioninevitably
69
deteriorates.Familymisunderstandingofthesituationoftenleadstothepersonbeingadmittedinappropriatelytohospital.Whenfamilymembershavehadtimetoreflect,theyareoftenunhappythattheydidnot fully understand the situation and wish they had been given the relevantinformationaboutendoflifecare
ChallengeNotindividualisingactivitiesThe aim of Namaste is always to enrich quality of life for residents with advanceddementia. However, if the care given is not based on the individual’s own specificneeds and does not reflect their unique life history, then it is not based in a trulyperson-centredapproachand is less likely to improvetheperson’squalityof life.Forexample, someonemight respondwith great pleasure to theperfume sheused as ayoungwoman,buthaveaverylimitedresponsetootherfragrances.
ChallengeAfternoonNamastesessionsCarehomesappeartohavemoredifficultyestablishingtheNamasteCareprogrammeintheafternoonsthan inthemornings.Thereasonsforthisarevaried.Forexample,staffaremore tiredafter themorningwork, lunchbreaksneed tobecovered in theafternoon, a number of residents may need to rest on the bed for a period in theafternoonbecause theyhave skinproblemsorbecause theyareunwellor very frail,andoftenresidentsaresleepyintheafternoons.However, to be fully effective for residents with advanced dementia, the gentlerelaxation and stimulation of Namaste must occupy a substantial part of their day.Residents with dementia are more likely to be agitated towards evening, and theNamastesessioncreatesawelcomecalm.Strategy
• AdaptthetimingoftheafternoonNamastesessiontosuityourcarehomeroutine
• ForthosewhoareunabletocometotheNamastesession,takeNamaste(music,touch,scents,tastes,colour)totheresidents’rooms
• Themanager/shiftleaderneedstovisiteachsessionintheafternoonuntiltheroutineembeds.OnceNamasteisembeddedintheafternoonroutine,carestaffwillenjoytheafternoonsessionsasmuchasthemorningsessions.Also,asresidentsaregroupedtogetherandarerelaxed,theafternoonsessionsdonotincreasetheworkload
• Rememberthatevenifresidentsaresleepy,iftheyfallasleepinNamastetherewillbesomeonewiththemwhentheywake
• Challengestafftocreateadifferentexperienceintheafternoons,perhapsworkingonlifestoriesand/orreadingaloudtothewholegroup.Creatinga
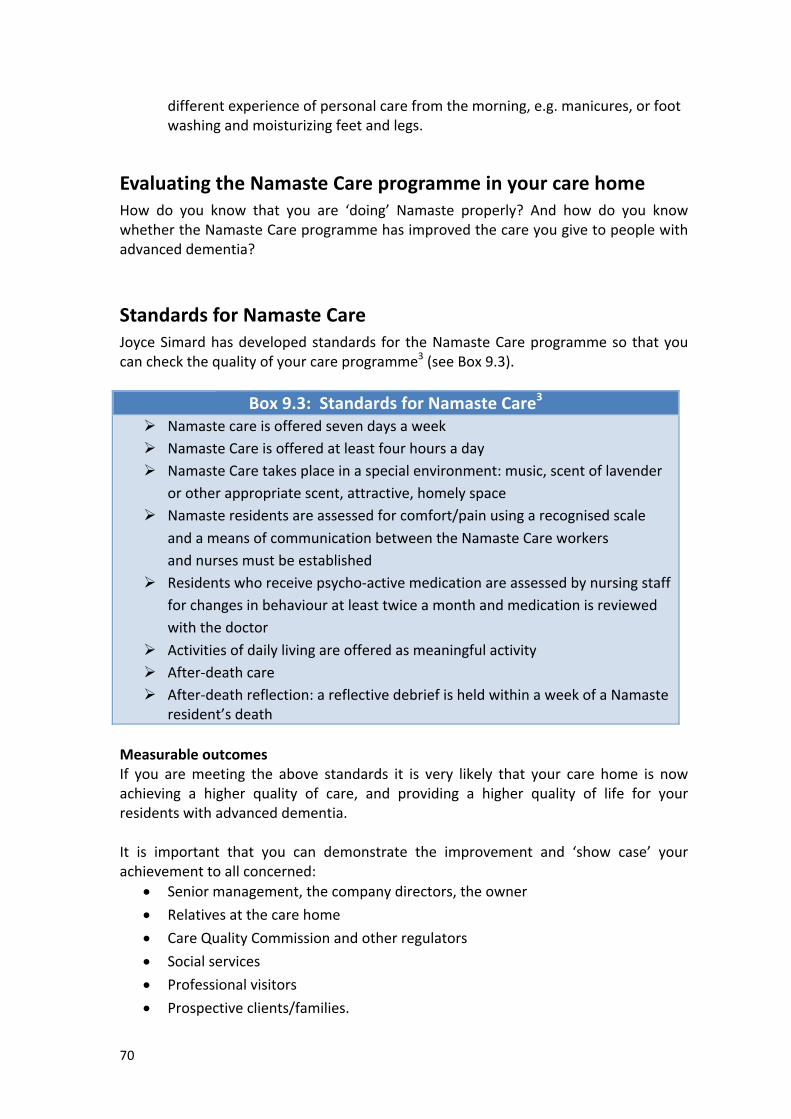
70
differentexperienceofpersonalcarefromthemorning,e.g.manicures,orfootwashingandmoisturizingfeetandlegs.
EvaluatingtheNamasteCareprogrammeinyourcarehomeHow do you know that you are ‘doing’ Namaste properly? And how do you knowwhethertheNamasteCareprogrammehasimprovedthecareyougivetopeoplewithadvanceddementia?
StandardsforNamasteCareJoyceSimardhasdevelopedstandards for theNamasteCareprogrammeso thatyoucancheckthequalityofyourcareprogramme3(seeBox9.3).
Box9.3:StandardsforNamasteCare3
Ø NamastecareisofferedsevendaysaweekØ NamasteCareisofferedatleastfourhoursadayØ NamasteCaretakesplaceinaspecialenvironment:music,scentoflavender
orotherappropriatescent,attractive,homelyspaceØ Namasteresidentsareassessedforcomfort/painusingarecognisedscale
andameansofcommunicationbetweentheNamasteCareworkersandnursesmustbeestablished
Ø Residentswhoreceivepsycho-activemedicationareassessedbynursingstaffforchangesinbehaviouratleasttwiceamonthandmedicationisreviewedwiththedoctor
Ø ActivitiesofdailylivingareofferedasmeaningfulactivityØ After-deathcareØ After-deathreflection:areflectivedebriefisheldwithinaweekofaNamaste
resident’sdeathMeasurableoutcomesIf you aremeeting the above standards it is very likely that your care home is nowachieving a higher quality of care, and providing a higher quality of life for yourresidentswithadvanceddementia.It is important that you can demonstrate the improvement and ‘show case’ yourachievementtoallconcerned:
• Seniormanagement,thecompanydirectors,theowner• Relativesatthecarehome• CareQualityCommissionandotherregulators• Socialservices• Professionalvisitors• Prospectiveclients/families.
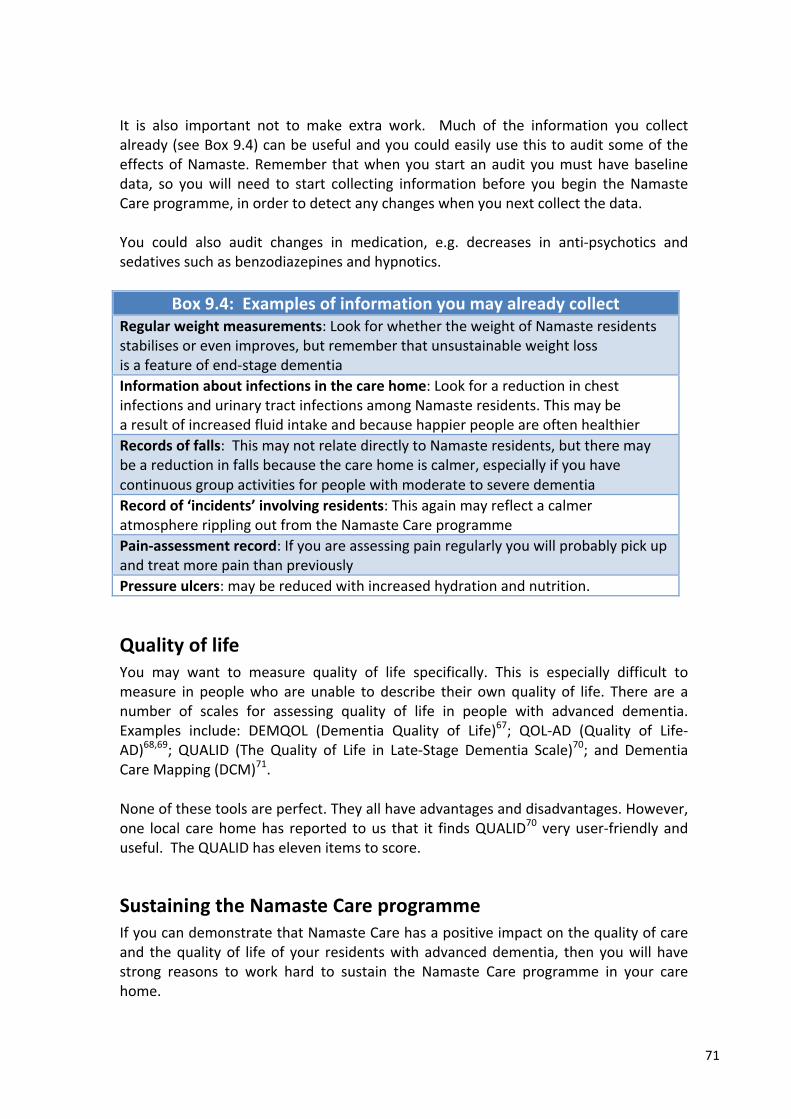
71
It is also important not to make extra work. Much of the information you collectalready(seeBox9.4)canbeusefulandyoucouldeasilyusethistoauditsomeoftheeffectsofNamaste.Remember thatwhenyoustartanaudityoumusthavebaselinedata, so youwill need to start collecting information before you begin theNamasteCareprogramme,inordertodetectanychangeswhenyounextcollectthedata.You could also audit changes in medication, e.g. decreases in anti-psychotics andsedativessuchasbenzodiazepinesandhypnotics.
Box9.4:ExamplesofinformationyoumayalreadycollectRegularweightmeasurements:LookforwhethertheweightofNamasteresidentsstabilisesorevenimproves,butrememberthatunsustainableweightlossisafeatureofend-stagedementiaInformationaboutinfectionsinthecarehome:LookforareductioninchestinfectionsandurinarytractinfectionsamongNamasteresidents.ThismaybearesultofincreasedfluidintakeandbecausehappierpeopleareoftenhealthierRecordsoffalls:ThismaynotrelatedirectlytoNamasteresidents,buttheremaybeareductioninfallsbecausethecarehomeiscalmer,especiallyifyouhavecontinuousgroupactivitiesforpeoplewithmoderatetoseveredementiaRecordof‘incidents’involvingresidents:ThisagainmayreflectacalmeratmosphereripplingoutfromtheNamasteCareprogrammePain-assessmentrecord:IfyouareassessingpainregularlyyouwillprobablypickupandtreatmorepainthanpreviouslyPressureulcers:maybereducedwithincreasedhydrationandnutrition.
QualityoflifeYou may want to measure quality of life specifically. This is especially difficult tomeasure in peoplewho are unable to describe their ownquality of life. There are anumber of scales for assessing quality of life in people with advanced dementia.Examples include: DEMQOL (Dementia Quality of Life)67; QOL-AD (Quality of Life-AD)68,69; QUALID (The Quality of Life in Late-Stage Dementia Scale)70; and DementiaCareMapping(DCM)71.Noneofthesetoolsareperfect.Theyallhaveadvantagesanddisadvantages.However,one local carehomehas reported tous that it findsQUALID70 veryuser-friendlyanduseful.TheQUALIDhaselevenitemstoscore.
SustainingtheNamasteCareprogrammeIfyoucandemonstratethatNamasteCarehasapositiveimpactonthequalityofcareand thequalityof lifeof your residentswithadvanceddementia, thenyouwill havestrong reasons to work hard to sustain the Namaste Care programme in your carehome.
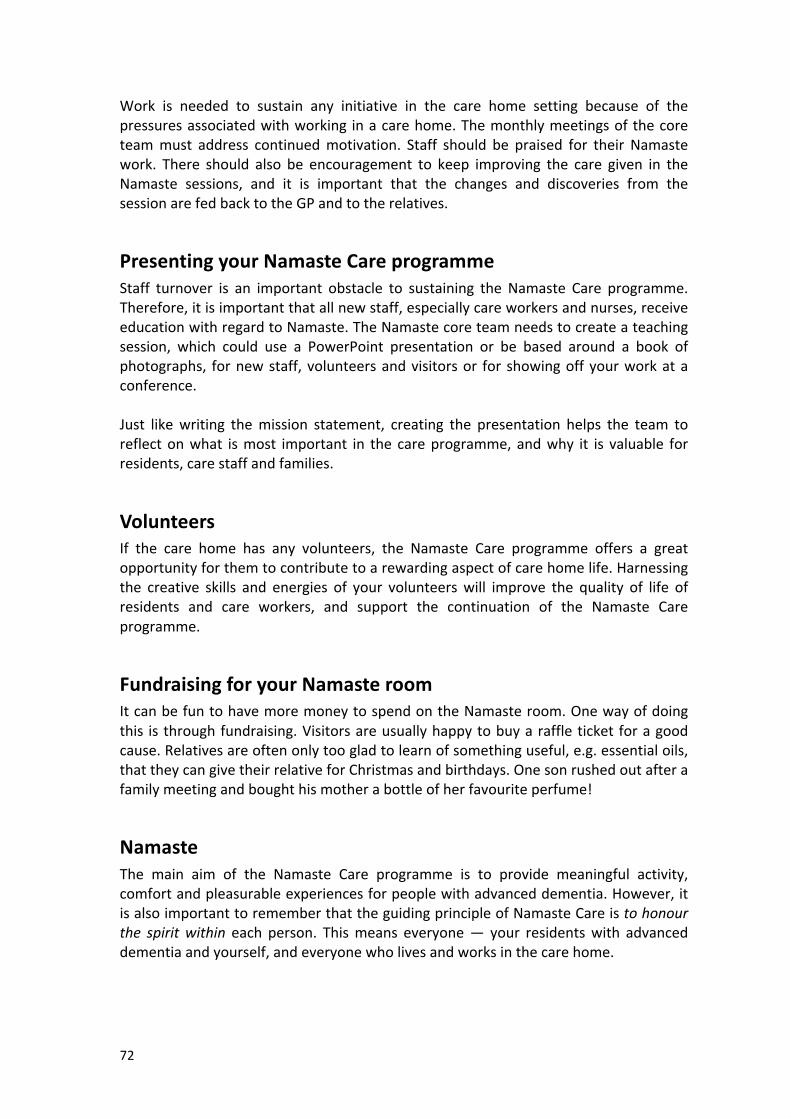
72
Work is needed to sustain any initiative in the care home setting because of thepressuresassociatedwithworking inacarehome.Themonthlymeetingsofthecoreteammust address continuedmotivation. Staff should be praised for their Namastework. There should also be encouragement to keep improving the care given in theNamaste sessions, and it is important that the changes and discoveries from thesessionarefedbacktotheGPandtotherelatives.
PresentingyourNamasteCareprogrammeStaff turnover is an important obstacle to sustaining the Namaste Care programme.Therefore,itisimportantthatallnewstaff,especiallycareworkersandnurses,receiveeducationwithregardtoNamaste.TheNamastecoreteamneedstocreateateachingsession, which could use a PowerPoint presentation or be based around a book ofphotographs, fornewstaff, volunteersandvisitorsor for showingoffyourworkataconference.Just likewriting themission statement, creating the presentation helps the team toreflectonwhat ismost important in the careprogramme,andwhy it is valuable forresidents,carestaffandfamilies.
VolunteersIf the care home has any volunteers, the Namaste Care programme offers a greatopportunityforthemtocontributetoarewardingaspectofcarehomelife.Harnessingthe creative skills and energies of your volunteerswill improve the quality of life ofresidents and care workers, and support the continuation of the Namaste Careprogramme.
FundraisingforyourNamasteroomItcanbefuntohavemoremoneytospendontheNamasteroom.Onewayofdoingthis is throughfundraising.Visitorsareusuallyhappytobuyaraffleticketforagoodcause.Relativesareoftenonlytoogladtolearnofsomethinguseful,e.g.essentialoils,thattheycangivetheirrelativeforChristmasandbirthdays.Onesonrushedoutafterafamilymeetingandboughthismotherabottleofherfavouriteperfume!
NamasteThe main aim of the Namaste Care programme is to provide meaningful activity,comfortandpleasurableexperiencesforpeoplewithadvanceddementia.However,itisalsoimportanttorememberthattheguidingprincipleofNamasteCareistohonourthe spiritwithin each person. Thismeans everyone— your residentswith advanceddementiaandyourself,andeveryonewholivesandworksinthecarehome.
73
Feel proudofwhat you are trying to do andwhat youhave achieved. Encourage allmembersof the team to valueand respect colleagueswhoareworking to the sameends.Whenpeoplearedoingagoodjob,praisethem.Namasteshouldbringfunandenergy intotheworkenvironment.However, itcanonlybesuccessful if teamwork isgoodandeveryteammemberisrespectfulofoneanother.Oncecarestaffhave learnt fromtheirexperiences in theNamastesessions, theywilltake new skills into theirwork outsideNamaste. Care staff and nurseswill find thatusing lovingtouchandaslowgentleapproachtoeverycontactwithresidentsmakeslifemucheasierforeveryone.Familieswillappreciatetheeffortsmadefortheirlovedones. The calm of the Namaste room should start to flow under the door and intoeverypartofthecarehome.In the downloadable resources listed below the toolkit youwill find ‘tools’, e.g. theNamaste Care Programme Checklist, suggestions for documentation which you canadapt,templatelettersetc.,whichcanhelpyousetuptheNamasteCareprogrammeinyourcarehome.You can read accounts of care homes that have successfully set up a Namaste Careprogrammeinthearticlesreferencedbelow.
Namaste!
74
References:
1. Alzheimer’sSociety.LowExpectations:AttitudesonChoice,CareandCommunityforPeoplewithDementiainCareHomes.London:Alzheimer’sSociety;2013.Accessedfrom:https://www.alzheimers.org.uk/site/scripts/download_info.php?downloadID=1024[09.12.2015]
2. Alzheimer’sSociety.HomefromHome:aReportHighlightingOpportunitiesforImprovingStandardsofDementiaCareinCareHomes.London:Alzheimer’sSociety;2007.https://www.google.co.uk/?gws_rd=ssl#q=2.%09Alzheimer%E2%80%99s+Society.++Home+from+Home:+a+Report+Highlighting+Opportunities+for+Improving+Standards+of+Dementia+Care+in+Care+Homes.+London:+Alzheimer%E2%80%99s+Society%3B+[09.12.2015]
3. Simard J.TheEnd-of-LifeNamasteCare™Program forPeoplewithDementia.2ndedn.Baltimore,Maryland:HealthProfessionsPress;2013.SimardJ.
4. StacpooleM.,HockleyJ.,ThompsellA.,SimardJ.&VolicerL.(2015)TheNamaste
Careprogrammecan reducebehavioural symptoms in carehome residentswith
advanceddementia.InternationalJournalofGeriatricPsychiatry7,702-709.
5. StacpooleM,ThompsellA,HockleyJ,SimardJ,VolicerL.TheNamasteCareProgrammeforPeoplewithAdvancedDementiaattheEndofTheirLives:anActionResearchStudyinSixCareHomeswithNursing.Finalstudyreport.Availablefrom:www.stchristophers.org.uk/care-homes[accessed30thJanuary2013].
6. TheDepartmentofHealth.LivingWellwithDementia:aNationalDementiaStrategy.London:TheStationeryOffice;2009.https://www.gov.uk/government/publications/living-well-with-dementia-a-national-dementia-strategy[09.12.2015]
7. SIGN.ManagementofPatientswithDementia:aNationalClinicalGuideline.ScottishIntercollegiateGuidelinesNetwork:Edinburgh;2006.
8. KvernoKS,RabinsPV,BlassDM,HicksKL,BlackBS.Prevalenceandtreatmentofneuropsychiatricsymptomsinadvanceddementia.JournalofGerontologicalNursing.2008;34(12):8–15.
9. MitchellSL,TenoJM,KielyDK,etal.Theclinicalcourseofadvanceddementia.NewEnglandJournalofMedicine.2009;361(16):1529–38.
10. SampsonEL,RitchieCW,LaiR,RavenPW,BlanchardMR.Asystematicreviewofthescientificevidencefortheefficacyofapalliativecareapproachinadvanceddementia.InternationalPsychogeriatrics.2005;17(1):31–40.
11. SchrederE,OostermanJ,SwaabDetal.Recentdevelopmentsinpainindementia.BritishMedicalJournal.2005;30(7489):461–4.
75
12. SampsonEL.Frailtyanddementia:commonbutcomplexcomorbidities.Aging&MentalHealth.2012;16(3):269–72.
13. MorrisJCClinicalDementiaRating:AReliableandValidDiagnosticandStagingMeasureforDementiaoftheAlzheimerType.InternationalPsychogeriatrics.1997;9Suppl1:173-6;discussion177-8.
14. JolleyD.Anintroductiontothedementias:aclinicalview.In:HughesJC,Lloyd-WilliamsM,SachsGA(eds)SupportiveCareforthePersonwithDementia.Oxford:OxfordUniversityPress;11–20;2010.
15. XieJ,BrayneC,MatthewsFE.Survivaltimesinpeoplewithdementia:analysisfrompopulationbasedcohortstudywith14yearfollow-up.BritishMedicalJournal.2008;336:258–62.
16. RaitG,WaltersK,BottomleyC,PetersenI,IliffeS,NazarethI.Survivalofpeoplewithclinicaldiagnosisofdementiainprimarycare:cohortstudy.BritishMedicalJournal.2010;341:c3584.doi:10.1136/bmj.c3584.
17. NationalEndofLifeCareIntelligenceNetwork.DeathsfromAlzheimer’sDisease,DementiaandSenilityinEngland.November2010.Leicester:NationalEndofLifeCareIntelligenceNetwork;2010.Accessedfrom:http://www.endoflifecare-intelligence.org.uk/resources/publications/deaths_from_alzheimers[22.12.2015]
18. LynnJ,AdamsonDM.LivingWellattheEndofLife.AdaptingHealthCaretoSeriousChronicIllnessinOldAge.Washington:RandHealth;2003.
19. MitchellSL,MillerSC,TenoJM,DavisRB,ShafferML.TheAdvancedDementiaPrognosticTool(ADEPT):ariskscoretoestimatesurvivalinnursinghomeresidentswithadvanceddementia.JournalofPain&SymptomManagement.2010;40(5):639–651.Availablefrom:doi:10.1016/j.jpainsymman.2010.02.014.[Accessed:13February2014].
20. ThomasK.TheGSFPrognosticIndicatorGuidance.(4thedn.)Shrewsbury:GSFCentreCIC;2011.Accessedfrom:http://www.goldstandardsframework.org.uk/cd-content/uploads/files/General%20Files/Prognostic%20Indicator%20Guidance%20October%202011.pdf
21. KinleyJ,HockleyJ,StoneSetal.TheprovisionofcareforresidentsdyinginUKnursingcarehomes.AgeandAging.2013;16October:doi:10.1093/ageing/aft158
22. MahoneyF.BarthelD.Functionalevaluation:theBarthelIndex.MarylandStateMedicalJournal.1965;14(February):61–5.
23. BoschX,FormigaF,CuerpoS,TorresB,RosónB,López-SotoA.Aspirationpneumoniainoldpatientswithdementia.Prognosticfactorsofmortality.EuropeanJournalofInternalMedicine.2012;23(8):720–6.
24. MorrisonRS,SiuAL.Survivalinend-stagedementiafollowingacuteillness.JournaloftheAmericanMedicalAssociation.2000;284(1):47–52.
76
25. DepartmentofHealth.EndofLifeCareStrategy:PromotingHighQualityCareforallAdultsattheEndofLife.London:TheStationeryOffice;2008.
26. Alzheimer’sSociety.MyLifeUntiltheEnd:DyingWellWithDementia.London:Alzheimer’sSociety;2012.https://www.alzheimers.org.uk/endoflife[Accessedon26.01.2016]
27. Sampson EL, Gould V, Lee D, Blanchard MR. Differences in care received bypatientswithandwithoutdementiawhodiedduringacutehospitaladmission:aretrospectivecasenotestudy.AgeandAgeing.2006;35(2):187–9.
28. Alzheimer’sSociety.2009).CountingtheCost.CaringforPeoplewithDementiaonHospitalWards.London:Alzheimer’sSociety.https://www.alzheimers.org.uk/site/scripts/download.php?type=downloads&fileID=787.[Accessed26.01.2016]
29. SampsonEL,Thuné-BoyleI,KukkastenvehmasR,JonesL,TookmanA,KingM,BlanchardMR.Palliativecareinadvanceddementia:amixedmethodsapproachforthedevelopmentofacomplexintervention.BMCPalliativeCare.2008;7(8).Availablefrom:http://bmcpalliatcare.biomedcentral.com/articles/10.1186/1472-684X-7-8[Accessed:04.02.2016]
30. MentalCapacityAct2005.Availablefrom:www.legislation.gov.uk/ukpga/2005/9/contents[Accessed:26/01/2016]
31. World Health Organization. WHO Definition of Palliative Care. Geneva: WHO;2002.
32. National Institute for Health and Care Excellence. NICE Clinical Guideline 42.Dementia:SupportingPeopleWithDementiaandTheirCarersinHealthandSocialCare.London:NationalInstituteforHealthandCareExcellence;200.
33. van der Steen JT, Radbruch L, Hertogh CM et al. White paper defining optimalpalliative care in older people with dementia: a Delphi study andrecommendations from the European Association for Palliative Care. PalliativeMedicine.2013:4July.Availablefrom:doi:10.1177/0269216313493685.
34. Maslow, A. H. (1943). A Theory of Human Motivation. Psychological Review,50(4),370-96.(Accessed10.02.2016)
35. Scholzel-DorenbosC,MeeusenE,OldeRikkertM.(2010).Integratingunmetneedsintodementiahealth-relatedqualityofliferesearchandcare:IntroductionoftheHierarchyModelofNeedsinDementia.Aging&MentalHealth,14(1),pages 113-119
36. Kitwood T. Dementia Reconsidered: the Person Comes First. Buckingham: OpenUniversityPress;1997.
37. SabatSR.TheExperienceofAlzheimer’sDisease—LifeThroughaTangledVeil.Oxford:BlackwellPublishers;2001.
38. SimardJ.Silentandinvisible;nursinghomeresidentswithadvanceddementia.JournalofNutrition,Health&Aging.2007;11(6):484–8.
39. SabatSR.Maintainingtheselfindementia.In:HughesJC,Lloyd-WilliamsM,SachsGA,eds.SupportiveCareforthePersonwithDementia.Oxford:OxfordUniversity
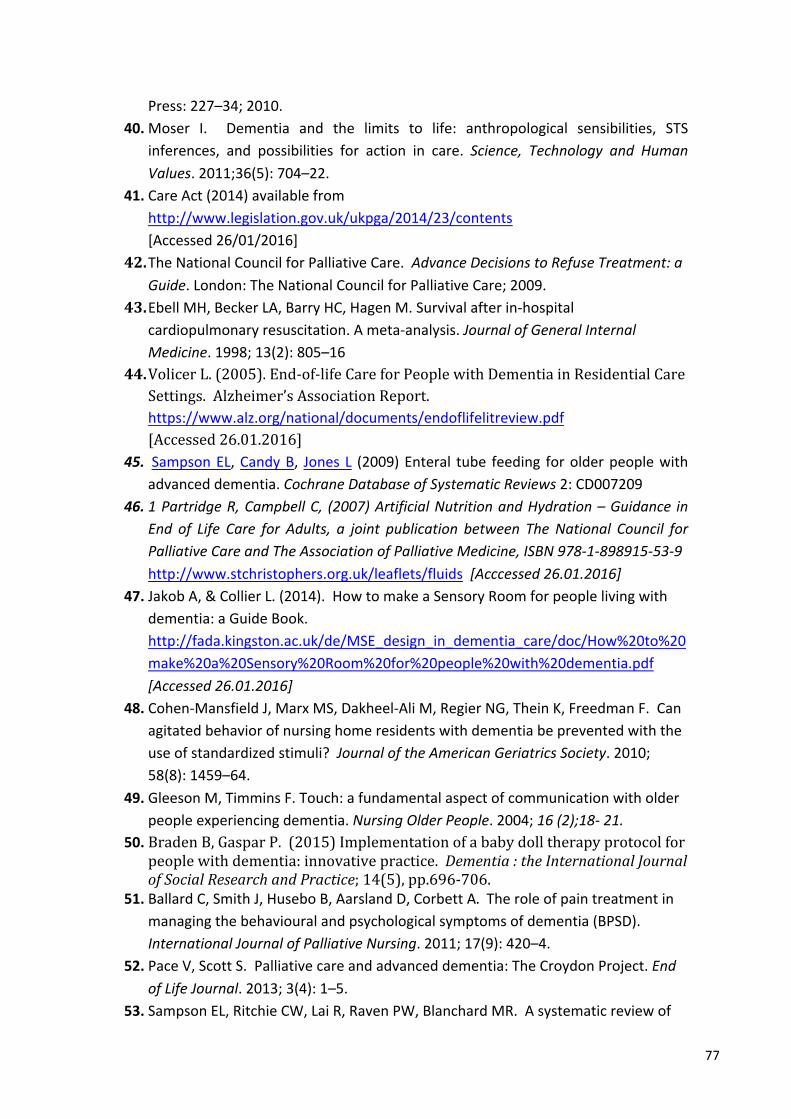
77
Press:227–34;2010.40. Moser I. Dementia and the limits to life: anthropological sensibilities, STS
inferences, and possibilities for action in care. Science, Technology and HumanValues.2011;36(5):704–22.
41. CareAct(2014)availablefromhttp://www.legislation.gov.uk/ukpga/2014/23/contents[Accessed26/01/2016]
42. TheNationalCouncilforPalliativeCare.AdvanceDecisionstoRefuseTreatment:aGuide.London:TheNationalCouncilforPalliativeCare;2009.
43. EbellMH,BeckerLA,BarryHC,HagenM.Survivalafterin-hospitalcardiopulmonaryresuscitation.Ameta-analysis.JournalofGeneralInternalMedicine.1998;13(2):805–16
44. VolicerL.(2005).End-of-lifeCareforPeoplewithDementiainResidentialCareSettings.Alzheimer’sAssociationReport.https://www.alz.org/national/documents/endoflifelitreview.pdf[Accessed26.01.2016]
45. SampsonEL,CandyB, JonesL (2009)Enteral tube feeding forolderpeoplewithadvanceddementia.CochraneDatabaseofSystematicReviews2:CD007209
46. 1PartridgeR,CampbellC, (2007)ArtificialNutritionandHydration–Guidance inEnd of Life Care for Adults, a joint publication between TheNational Council forPalliativeCareandTheAssociationofPalliativeMedicine,ISBN978-1-898915-53-9http://www.stchristophers.org.uk/leaflets/fluids[Acccessed26.01.2016]
47. JakobA,&CollierL.(2014).HowtomakeaSensoryRoomforpeoplelivingwithdementia:aGuideBook.http://fada.kingston.ac.uk/de/MSE_design_in_dementia_care/doc/How%20to%20make%20a%20Sensory%20Room%20for%20people%20with%20dementia.pdf[Accessed26.01.2016]
48. Cohen-MansfieldJ,MarxMS,Dakheel-AliM,RegierNG,TheinK,FreedmanF.Canagitatedbehaviorofnursinghomeresidentswithdementiabepreventedwiththeuseofstandardizedstimuli?JournaloftheAmericanGeriatricsSociety.2010;58(8):1459–64.
49. GleesonM,TimminsF.Touch:afundamentalaspectofcommunicationwitholderpeopleexperiencingdementia.NursingOlderPeople.2004;16(2);18-21.
50. BradenB,GasparP.(2015)Implementationofababydolltherapyprotocolforpeoplewithdementia:innovativepractice.Dementia:theInternationalJournalofSocialResearchandPractice;14(5),pp.696-706.
51. BallardC,SmithJ,HuseboB,AarslandD,CorbettA.Theroleofpaintreatmentinmanagingthebehaviouralandpsychologicalsymptomsofdementia(BPSD).InternationalJournalofPalliativeNursing.2011;17(9):420–4.
52. PaceV,ScottS.Palliativecareandadvanceddementia:TheCroydonProject.EndofLifeJournal.2013;3(4):1–5.
53. SampsonEL,RitchieCW,LaiR,RavenPW,BlanchardMR.Asystematicreviewof
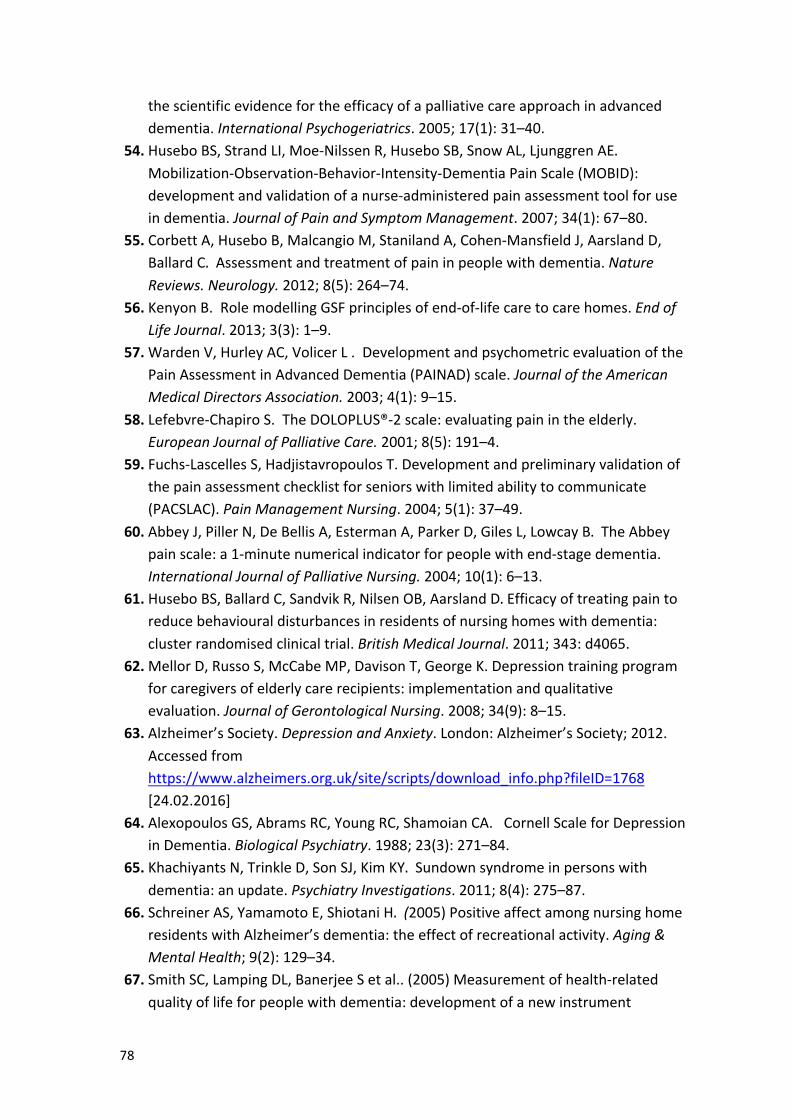
78
thescientificevidencefortheefficacyofapalliativecareapproachinadvanceddementia.InternationalPsychogeriatrics.2005;17(1):31–40.
54. HuseboBS,StrandLI,Moe-NilssenR,HuseboSB,SnowAL,LjunggrenAE.Mobilization-Observation-Behavior-Intensity-DementiaPainScale(MOBID):developmentandvalidationofanurse-administeredpainassessmenttoolforuseindementia.JournalofPainandSymptomManagement.2007;34(1):67–80.
55. CorbettA,HuseboB,MalcangioM,StanilandA,Cohen-MansfieldJ,AarslandD,BallardC.Assessmentandtreatmentofpaininpeoplewithdementia.NatureReviews.Neurology.2012;8(5):264–74.
56. KenyonB.RolemodellingGSFprinciplesofend-of-lifecaretocarehomes.EndofLifeJournal.2013;3(3):1–9.
57. WardenV,HurleyAC,VolicerL.DevelopmentandpsychometricevaluationofthePainAssessmentinAdvancedDementia(PAINAD)scale.JournaloftheAmericanMedicalDirectorsAssociation.2003;4(1):9–15.
58. Lefebvre-ChapiroS.TheDOLOPLUS®-2scale:evaluatingpainintheelderly.EuropeanJournalofPalliativeCare.2001;8(5):191–4.
59. Fuchs-LascellesS,HadjistavropoulosT.Developmentandpreliminaryvalidationofthepainassessmentchecklistforseniorswithlimitedabilitytocommunicate(PACSLAC).PainManagementNursing.2004;5(1):37–49.
60. AbbeyJ,PillerN,DeBellisA,EstermanA,ParkerD,GilesL,LowcayB.TheAbbeypainscale:a1-minutenumericalindicatorforpeoplewithend-stagedementia.InternationalJournalofPalliativeNursing.2004;10(1):6–13.
61. HuseboBS,BallardC,SandvikR,NilsenOB,AarslandD.Efficacyoftreatingpaintoreducebehaviouraldisturbancesinresidentsofnursinghomeswithdementia:clusterrandomisedclinicaltrial.BritishMedicalJournal.2011;343:d4065.
62. MellorD,RussoS,McCabeMP,DavisonT,GeorgeK.Depressiontrainingprogramforcaregiversofelderlycarerecipients:implementationandqualitativeevaluation.JournalofGerontologicalNursing.2008;34(9):8–15.
63. Alzheimer’sSociety.DepressionandAnxiety.London:Alzheimer’sSociety;2012.Accessedfromhttps://www.alzheimers.org.uk/site/scripts/download_info.php?fileID=1768[24.02.2016]
64. AlexopoulosGS,AbramsRC,YoungRC,ShamoianCA.CornellScaleforDepressioninDementia.BiologicalPsychiatry.1988;23(3):271–84.
65. KhachiyantsN,TrinkleD,SonSJ,KimKY.Sundownsyndromeinpersonswithdementia:anupdate.PsychiatryInvestigations.2011;8(4):275–87.
66. SchreinerAS,YamamotoE,ShiotaniH.(2005)PositiveaffectamongnursinghomeresidentswithAlzheimer’sdementia:theeffectofrecreationalactivity.Aging&MentalHealth;9(2):129–34.
67. SmithSC,LampingDL,BanerjeeSetal..(2005)Measurementofhealth-relatedqualityoflifeforpeoplewithdementia:developmentofanewinstrument
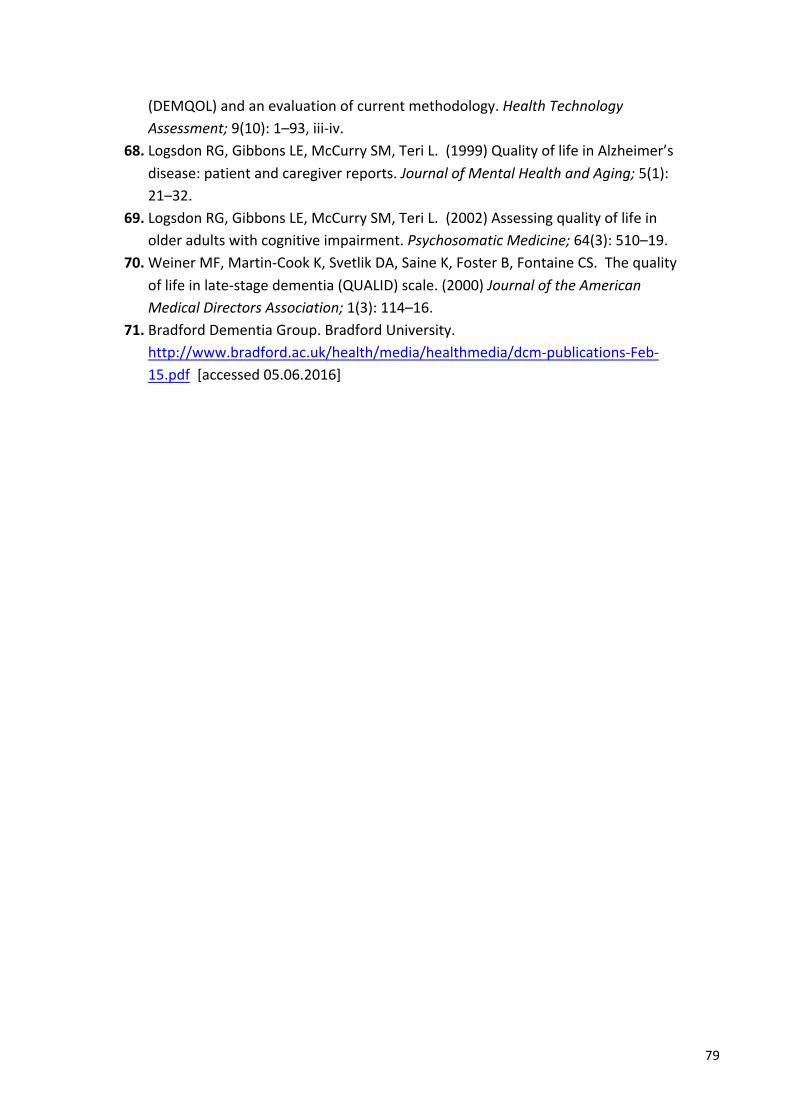
79
(DEMQOL)andanevaluationofcurrentmethodology.HealthTechnologyAssessment;9(10):1–93,iii-iv.
68. LogsdonRG,GibbonsLE,McCurrySM,TeriL.(1999)QualityoflifeinAlzheimer’sdisease:patientandcaregiverreports.JournalofMentalHealthandAging;5(1):21–32.
69. LogsdonRG,GibbonsLE,McCurrySM,TeriL.(2002)Assessingqualityoflifeinolderadultswithcognitiveimpairment.PsychosomaticMedicine;64(3):510–19.
70. WeinerMF,Martin-CookK,SvetlikDA,SaineK,FosterB,FontaineCS.Thequalityoflifeinlate-stagedementia(QUALID)scale.(2000)JournaloftheAmericanMedicalDirectorsAssociation;1(3):114–16.
71. BradfordDementiaGroup.BradfordUniversity.http://www.bradford.ac.uk/health/media/healthmedia/dcm-publications-Feb-15.pdf[accessed05.06.2016]