-
Research Article Open Access
Volume 1 • Issue 2 • 1000104OtolaryngolISSN:2161-119X
Otolaryngology an open access journal
Open AccessResearch Article
Szymczyk et al. Otolaryngol 2011, 1:2 DOI:
10.4172/2161-119X.1000104
IntroductionPostresection defect of the total lip, especially
when it is associated
with regional tissues i.e. cheek skin, floor of the mouth,
mandible, presents a real challenge for reconstructive surgeon. For
total lip recreation many different techniques can be considered.
Microvascular free tissue transfer is the latest major advance in
lower lip reconstructions and the main contributing factor in the
quality of life improvement. The modern techniques are able to
deliver well-vascularised tissues to allow closure of even most
complex and extended postresection defects. The aim of lip
restoration is to provide proper oral lining and external cheek
skin and to reconstruct oral competence. There are several issues
in lower lip reconstruction using microvascular tissues that must
be considered, including defect’s size, aesthetic units, support,
recreation of the vermillion and defects of associated tissues.
Among many certain donor sites the radial forearm free flap (RFFF)
has become a golden standard for majority of patients with total
lip postresection defects, especially in cases where the use of
local techniques may result in functional and/or aesthetic loss
[1].
RFFF provides thin, pliable fasciocutaneous tissue for intra-
and extra oral defects. This particular free flap is highly
reliable because of large diameter of its artery and veins. The
vascular pedicle is ideal with long vessels capable to reach the
opposite side of the neck if necessary [5]. That characteristic
makes it a useful one for lower face postresection defects
reconstruction.
Aim of the StudyThe aim of this paper is to present the group of
10 consecutive
patients with lower lip cancer, who underwent the RFFF
reconstruction to develop a precise, based on anatomical details,
plan of incorporating
*Corresponding author: Łukasz Krakowczyk, Department of
Oncological Surgery, Cancer Centre, M.C Sklodowska Memorial
Institute, Wybrzeże Armii Krajowej 15, Gliwice, Poland, E-mail:
[email protected]
Received June 06, 2011; Accepted November 03, 2011; Published
November 07, 2011
Citation: Szymczyk C, Maciejewski A, Wierzgoń J, Krakowczyk Ł,
Grajek M, et al. (2011) The Use of Radial Forearm Free Flap for
Total Lower Lip Reconstruction: The Analysis of 10 Consequentive
Cases and Quality of Life Evaluation. Otolaryngol 1:104.
doi:10.4172/2161-119X.1000104
Copyright: © 2011 Szymczyk C, et al. This is an open-access
article distributed under the terms of the Creative Commons
Attribution License, which permits unrestricted use, distribution,
and reproduction in any medium, provided the original author and
source are credited.
The Use of Radial Forearm Free Flap for Total Lower Lip
Reconstruction: The Analysis of 10 Consequentive Cases and Quality
of Life Evaluation Cezary Szymczyk, Adam Maciejewski, Janusz
Wierzgoń, Łukasz Krakowczyk*, Maciej Grajek, Piotr Jędrzejewski,
Mirosław Dobrut, Ryszard Szumniak, Rafał Ulczok and Stanisław
Półtorak
Department of Oncological Surgery, Cancer Centre, M.C Sklodowska
Memorial Institute, Wybrzeże Armii Krajowej 15, Gliwice, Poland
radial forearm free flap in lower lip reconstruction. Qualities
of life, mainly aesthetic and functional results are also
analyzed.
Material and MethodsMaterial: From March 2002 to December 2005,
10 consecutive
patients with squamous cell cancer of the lower lip, underwent
complex surgical treatment in the Dept. of Surgical Oncology in
Cancer Center MSC Memorial Institute, Gliwice, Poland. The only
eligible criterion was the use of radial forearm free flaps for
lower lip reconstruction. All reconstructive procedures were
performed at the time of resection. None of the patients underwent
second corrections.
There were 8 men and 2 women, and M:F ratio was 4:1. The average
age was 56 years. In whole group cancer was in advanced stage (T
3/4).
Methods: All patients underwent surgical resection of primary
tumor en block with regional neck nodes. Type of lymph nodes
AbstractBackground: Postresective defect of the total lip,
especially when associated with soft tissues of lower face
still
remains a challenge for adequate reconstruction. Among many
options microvascular free tissue transfer is the latest major
advance and the main contributing factor in the quality of life
improvement. The modern techniques are able to deliver
well-vascularised tissues which allow to reconstruct even most
complex and extended defects. The aim of lip restoration is to
provide proper oral lining and external cheek skin and to
reconstruct oral competence. There are several issues in lower lip
reconstruction using microvascular tissues that must be considered,
including defect’s size, aesthetic units, support, recreation of
the vermillion and defects of associated tissues. Among many
certain donor sites the radial forearm free flap (RFFF) has become
a golden standard for majority of patients with total lip
postressective defects.
Materials and Methods: The aim of this paper is to present the
group of 10 consecutive patients with lower lip cancer, where RFFF
was used for functional lower lip reconstruction, with analysis of
life quality. In the material the patient characteristics is
presented with the details of RFFF modifications according to the
type of lip suspension. Based on own QOL questionnaire, the
functional and aesthetic results were analysed.
Results: The results suggest that the careful and detailed
planning of the size, shape and type of lip suspension influence
both functional and aesthetic results. Static lip suspension for
defects limited to lower lip only is comparable to dynamic
suspension in cases where the defect is complex and extended.
Results of quality of life analysis may be a predictive factor
influencing the choice of individual flap modification including
the type of lip suspension
Conclusions: Our experience with free radial forearm free flap
for total lip reconstruction suggests that the careful and detailed
planning of the size, shape and type of lip suspension influence
both functional and aesthetic results.
Oto
lary
ngology: OpenAccess
ISSN: 2161-119X
Otolaryngology: Open Access
-
Citation: Szymczyk C, Maciejewski A, Wierzgoń J, Krakowczyk Ł,
Grajek M, et al. (2011) The Use of Radial Forearm Free Flap for
Total Lower Lip Reconstruction: The Analysis of 10 Consequentive
Cases and Quality of Life Evaluation. Otolaryngol 1:104.
doi:10.4172/2161-119X.1000104
Page 2 of 5
Volume 1 • Issue 2 • 1000104OtolaryngolISSN:2161-119X
Otolaryngology an open access journal
dissection was adequate to the stage of disease. In all cases
wide local resection were performed. Technique of the
reconstruction was chosen individually, based on type and
localization of postresection defect, general patient’s condition
and his expectations as well. In all cases radial fasciocutaneous
forearm free flap was chosen. Volume and location of soft tissue
loss directly forced the size and shape of skin paddle. The size of
skin island corresponded with the contour of the postresection
defect. In all cases a template duplicated the defect was made. The
extraoral defects varied from 18 to 45 cm2 and the intaoral were
between 15 and 30 cm2. In 3 cases the marginal mandibulectomy was
performed. In 7 cases the flap was harvested with the palmaris
longus tendon crossing the internal surface. In 4 cases the tendon
was sutured to the deep surface of the oral commissures and in
remaining 3 cases (were resection was more extended) it was
attached to the zygomatic arches.
In 4 cases the RFFF was associated with antebrachal sensitive
nerve which was anastomosed to menthal nerve stump. The detailed
characteristic of the material is presented in Table 1.
The vascular pedicle length varied from 10 to 16 cm. In 8 cases
arterial anastomoses were performed with facial artery end to end
and in remaining 2 with thyroid superior. In about 70% RFFF single
vein (concomitant) was connected with jugular internal or facial
vain and in the remaining 30% two veins were simultaneously
anastomized.
In all cases split-thickness skin grafts were used for donor
site closure (taken from the thigh). In 8 cases radial forearm free
flap was used alone (Figure 1a,b,2a,b) and in two cases the RFFF
was combined with fibula free flap due to mandible infiltration
(Figure 3a,b). In those cases osteoseptocutaeous free fibula was
able to reconstruct the segment of the mandible and its skin island
was used to recreate the oral vestibule and floor of the mouth.
Quality of life evaluation: There are still too little studies
on the QOL of patients after microvascular reconstructions for
lower lip cancer. This is the reason why we recently introduce the
routine practice to own questionnaire of functional and aesthetic
outcome after combined surgery (resection + reconstruction) for all
patients
PATIENT AGE TNMDEFECT SIZE (cm) ANASTOMOSES
LIP SUSPENSION REINNERVATIONEXTRAORAL INTRAORAL ARTERIAL
VENOUS
1 58 T4N1 8X4 6X4 RADIAL - FACIAL CONCOM. – JUG. INTPALMARIS
LONG. TEND. – ORAL COM -
2 45 T3N0 6X3 5X3 RADIAL - FACIAL CONCOM - FACIAL - -
3 67 T4NO 9X5 7X4 + MARG. MADIBULECTOMYRADIAL – THYROID SUP.
DOUBLE
PALMARIS LONG. TEND. – ZYG. ARCH
ANTEBR. – MENTHAL
4 61 T4N2 10X4 11X5 + MARG. MADIBULECTOMY RADIAL -
FACIALCONNECTION – JUG. INT.
PALMARIS LONG. TEND. – ZYG. ARCH
ANTEBR. – MENTHAL
5 42 TTN1 7X3 7X3 RADIAL - FACIAL CONNECTION – JUG. INT.PALMARIS
LONG. TEND. – ORAL COM -
6 57 T3N1 5X5 5X3 RADIAL - FACIAL CONCOM. – JUG. INT - -
7 53 T4N0 8X4 6X5 RADIAL – THYROID SUP.CONNECTION – JUG. INT
PALMARIS LONG. TEND. – ORAL COM -
8 69 T4N1 9X5 10X3 + MARG. MADIBULECTOMY RADIAL - FACIAL
DOUBLEPALMARIS LONG. TEND. – ZYG. ARCH
ANTEBR. – MENTHAL
9 65 T3N2 6X3 6X3 RADIAL - FACIAL CONCOM - FACIAL - -
10 46 T4N0 8X6 7X4 RADIAL - FACIAL CONNECTION - FACIALPALMARIS
LONG. TEND. - ORAL COM
ANTEBR. – MENTHAL
Table 1: Characteristic of the clinical material.
Table 2: QOL questionairre and results.
PATIENT DEFECT SIZE (cm2)QUALITY OF LIFE – AESTHETIC RESULT
QUALITY OF LIFE – FUNCTIONAL RESULTSymmetry Vermillon shape Lip
size & contour Scars status Lip mobility Oral closure
Articulation Presence of microstomia
1 56 1 0 1 1 0 1 1 12 33 1 1 1 0 1 1 1 13 73 0 0 1 1 1 1 1 14 95
0 1 0 1 0 0 1 15 42 1 1 1 1 1 1 0 16 40 1 1 1 1 1 1 1 17 62 1 0 0 0
0 1 1 18 75 1 0 0 1 0 1 1 19 36 1 1 1 1 1 1 1 110 70 0 0 0 1 0 1 1
1
Table 3: Aesthetic and functional results according to defect
size and type of lip suspension.
DEFECT SIZE LIP SUSPENSION
30 – 60(5 patients)>60(5 patients)
PALM. LONG. TENDON – ORAL COMMISURE (4 patients)
PALM. LONG. TENDON – ZYGOMATIC ARCH (3 patients)
NO SUSPENSION(3 patients)
AESTHETIC EFFECT 3,6 2 2,3 2,3 3,7FUNCTIONAL EFFECT 3,6 3 3 3
4
BOTH 7 5 5,3 5,3 7,7
-
Citation: Szymczyk C, Maciejewski A, Wierzgoń J, Krakowczyk Ł,
Grajek M, et al. (2011) The Use of Radial Forearm Free Flap for
Total Lower Lip Reconstruction: The Analysis of 10 Consequentive
Cases and Quality of Life Evaluation. Otolaryngol 1:104.
doi:10.4172/2161-119X.1000104
Page 3 of 5
Volume 1 • Issue 2 • 1000104OtolaryngolISSN:2161-119X
Otolaryngology an open access journal
reconstruction outcome, that means aesthetic and functional
results have been quantified using own Quality Of Life
Questionnaires. The questionnaire takes into account the impact of
surgical procedures on the QOL in relation to a radial forearm free
flap for lower lip reconstruction. Eight-item scale includes
measures of symmetry, vermillon shape, size and contour of the
recreated lip, the status of postoperative scars and functional
results such as: lip mobility, oral closure, articulation and
presence of the microstomia. Each parameter was considered as good
(1) or bad (0). Every patient answered once to this questionnaire,
i.e. 6 months after surgery (Table 2).
The patients are interviewed by the QOL Office (sociologists and
physiologists) independently of the treatment team. The present
analysis includes small number of cases which can be considered
only as a preliminary report.
ResultsIn the whole group of 10 patients tumor resection was
radical
and surgical margins were histopathologically negative.
Actuarial 12-months recurrence-free survival is 100%.
10 flaps were successfully transferred (100%). Two flaps were
explored within 24 hours after surgery, because of vein thrombosis
and two was salvaged. One patient developed postoperative fistula
in submandibular region which required surgical retreatment
with
(a)
(b)
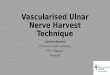
Figure 1: a,b – Pre- and postoperative view of patient – the use
of RFFF with tendon lip suspension.
(a)
(b)
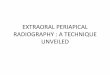
Figure 2: a,b – The steps of total lip reconstruction with
RFFF.
successful outcome. In one case (after flap salvage surgery)
partial flap loss (smaller than 30%) occurred. There were no donor
site complications except two cases were skin graft partial loss
was noted (requiring second regrafting).
According to quality of life assessment the material was
subdivided into two groups, based on postressective defect volume
(Gr. A- 30-60 cm2, Gr. B- > 60 cm2). Both aesthetic and
functional outcome were better in Group A than in Group B (70 vs 50
points). Quality of life analysis did not show any differences
between different modalities of lip suspension (palmaris longus
tendon – zygomatic arch vs palmaris longus tendon – orbicularis
oris muscle). Moreover better results were noticed in patients were
no lip suspension was performed.
Complete oral competence was achieved in all but one patient
(the largest defect with marginal mandibulectomy). The type of lip
suspension except one case did not affect the speech and
articulation function. None of patients presented microstomia.
Detailed QOL results are presented in Table 3.
Although the results of reinnervation were not analyzed, no
subjective differences were noticed between 4 cases were
antebrachial was anastomosed with menthal nerve and cases were no
sensate recreation was performed.
-
Citation: Szymczyk C, Maciejewski A, Wierzgoń J, Krakowczyk Ł,
Grajek M, et al. (2011) The Use of Radial Forearm Free Flap for
Total Lower Lip Reconstruction: The Analysis of 10 Consequentive
Cases and Quality of Life Evaluation. Otolaryngol 1:104.
doi:10.4172/2161-119X.1000104
Page 4 of 5
Volume 1 • Issue 2 • 1000104OtolaryngolISSN:2161-119X
Otolaryngology an open access journal
DiscussionThe lips play an important role in facial expression,
speech
and eating. To achieve optimal functional and aesthetic outcome
a significant attention must be put to make a right plan of both
resection and reconstruction. Although for total lip defects many
different methods have been suggested, the introduction of
microvascular techniques allowed for single stage reconstruction of
a complex and extended tissue loss. Among many techniques the
radial forearm free flap is the most commonly used for soft tissue
defect only. It provides a decent support especially when it is
transferred with palmaris longus tendon. In different authors
opinion the tendon can be sutured to either nasolabial area, the
malar periostium, or to the bilateral modiolus. Those variations
allow reconstruct a static suspension only. Recently, Sawhney [2]
proposed the technique of dynamic suspension, where the tendon is
connected to transferred masseter muscle. Jeng et al. [3] reported
the principles of looping the palmaris longus tendon to orbicularis
oris muscle. Our experiences show that this technique of tendon
fixation is able to restore complete circumference of oral
sphincter. Moreover, this variant of dynamic reconstruction is an
easy, one stage procedure providing similar functional outcome
comparing to cases where the tendon was sutured to zygomatic arches
[4-6]. In our limited data the results show only the idea of
different radial flap modalities influencing the quality of life
outcome and
therefore it is presented as preliminary report. The QOL
analysis presents no differences between static and dynamic lip
suspension. It can be explained by careful choice of suturing the
palmaris longus tendon to zygomatic arch or orbicularis oris muscle
due to the size of postressective defect volume and extension. In
cases were the defect was relatively small and limited to lower lip
only, no suspension was performed with good functional and
aesthetic results. In very thin patient the flap is sometimes to
thin and does not provide bulk. This can be overcome with a
brachiradialis muscle being harvested with the skin flap to add
bulk. For bulky flaps secondary thinning in the appropriate zones
with liposuction will improve the aesthetics and the use of fat
injection is also of value secondary bulking of the neo-lip [7,8].
From aesthetic point of view the use of distant flaps i.e. radial
forearm gives the color mismatch and according to forearm anatomy,
bulk can decrease the aesthetic outcome. Therefore the flap
thinning or second procedures are often required. In our series
after harvesting and detaching the flap was individually thinned
when necessary, with no second procedures. In 8 of 10 cases the
proper lip symmetry was achieved, and in more than half of the
patients size of the lip and its contour, with good status of scars
were noticed [9,10].
In our series there were no differences in sensation whether the
menthal nerve was anastomosed with antebrachial nerve or not. It
can be explained by short period of observation and small group of
analyzed patients and on the other hand by difficulties of
comparing the sensate recreation coming from anastomosing the
menthal and antebrachial nerve and spontaneous reinnervation itself
[11].
ConclusionsOur experience with free radial forearm free flap for
total lip
reconstruction suggests that the careful and detailed planning
of the size, shape and type of lip suspension influence both
functional and aesthetic results. Static lip suspension for defects
limited to lower lip only is comparable to dynamic suspension in
cases where the defect is complex and extended. Results of quality
of life analysis may be a predictive factor influencing the choice
of individual flap modification including the type of lip
suspension.
References
1. Song R, Gao Y, Song Y, Yu Y (1982) The forearm flap. Clin
Plast Surg 9: 21-26.
2. Sawhney CP (1986) Reanimation of lower lip reconstructed by
flaps. Br J Plast Surg 39: 114-117.
3. Jeng SF, Kuo YR, Wei FC, Su CY, Chien CY (2004) Total lower
lip reconstruction with a composite radial forearm – palmaris
longus tenton flap: a clinical series. Plast Reconstr Surg; 113:
19-23.
4. Furuta S, Sakaguchi Y, Iwasawa M, Kurita H, Minemura T (1994)
Reconstruction of the lips, oral commissure, and full thickness
cheek with a composite radial forearm palmaris longus free flap.
Ann Plast Surg 33: 544-547.
5. Ozdemir R, Ortak T, Kocer U, Celebioğlu S, Sensöz O, et al.
(2003) Total lower lip reconstruction using sensate composite
radial forearm flap. J Craniofac Surg 14: 393-405.
6. Jeng Sf, Kuo YR, Wei FC, Su CY, Chien CY (2003)
Reconstruction of concomitant lip and cheek through-and-through
defects with combined free flap and advancement flap from the
remaining lip. Plast Reconstr Surg 113: 491-498.
7. Carroll CM, Pathak I, Irish J, Neligan PC, Gullane PJ (2000)
Reconstruction of total lower lip and chin defects using the
composite radial forearm--palmaris longus tendon free flap. Arch
Facial Plast Surg 2: 53-56.
8. Baumann D, Robb G (2008) Lip reconstruction. Semin Plast Surg
22: 269-280.
9. Coppit GL, Lin DT, Burkey BB (2004) Current concepts in lip
reconstruction. Curr Opin Otolaryngol Head Neck Surg 12:
281-287.
(a)
(b)
Figure 3: a,b – The use of double independent free flaps –
radial forearm for lip and fibula for mandible reconstruction.
http://www.ncbi.nlm.nih.gov/pubmed/7094519http://www.ncbi.nlm.nih.gov/pubmed/3947792http://www.ncbi.nlm.nih.gov/pubmed/3947792http://journals.lww.com/plasreconsurg/Abstract/2004/01000/Total_Lower_Lip_Reconstruction_with_a_Composite.2.aspxhttp://journals.lww.com/plasreconsurg/Abstract/2004/01000/Total_Lower_Lip_Reconstruction_with_a_Composite.2.aspxhttp://journals.lww.com/plasreconsurg/Abstract/2004/01000/Total_Lower_Lip_Reconstruction_with_a_Composite.2.aspxhttp://journals.lww.com/annalsplasticsurgery/Abstract/1994/11000/Reconstruction_of_the_Lips,_Oral_Commissure,_and.13.aspxhttp://journals.lww.com/annalsplasticsurgery/Abstract/1994/11000/Reconstruction_of_the_Lips,_Oral_Commissure,_and.13.aspxhttp://journals.lww.com/annalsplasticsurgery/Abstract/1994/11000/Reconstruction_of_the_Lips,_Oral_Commissure,_and.13.aspxhttp://journals.lww.com/jcraniofacialsurgery/Abstract/2003/05000/Total_Lower_Lip_Reconstruction_Using_Sensate.20.aspxhttp://journals.lww.com/jcraniofacialsurgery/Abstract/2003/05000/Total_Lower_Lip_Reconstruction_Using_Sensate.20.aspxhttp://journals.lww.com/jcraniofacialsurgery/Abstract/2003/05000/Total_Lower_Lip_Reconstruction_Using_Sensate.20.aspxhttp://journals.lww.com/plasreconsurg/Abstract/2004/02000/Reconstruction_of_Concomitant_Lip_and_Cheek.4.aspxhttp://journals.lww.com/plasreconsurg/Abstract/2004/02000/Reconstruction_of_Concomitant_Lip_and_Cheek.4.aspxhttp://journals.lww.com/plasreconsurg/Abstract/2004/02000/Reconstruction_of_Concomitant_Lip_and_Cheek.4.aspxhttp://journals.lww.com/plasreconsurg/Abstract/2004/02000/Reconstruction_of_Concomitant_Lip_and_Cheek.4.aspxhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Carroll
CM%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Pathak
I%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Irish
J%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Neligan
PC%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Gullane
PJ%22%5BAuthor%5Dhttp://archfaci.ama-assn.org/content/2/1/53.shorthttp://archfaci.ama-assn.org/content/2/1/53.shorthttp://archfaci.ama-assn.org/content/2/1/53.shorthttp://www.ncbi.nlm.nih.gov/pubmed/10925425##http://www.ncbi.nlm.nih.gov/pubmed?term=%22Baumann
D%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Robb
G%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed/20567703http://www.ncbi.nlm.nih.gov/pubmed/20567703##http://journals.lww.com/co-otolaryngology/Abstract/2004/08000/Current_concepts_in_lip_reconstruction.3.aspxhttp://journals.lww.com/co-otolaryngology/Abstract/2004/08000/Current_concepts_in_lip_reconstruction.3.aspx
-
Citation: Szymczyk C, Maciejewski A, Wierzgoń J, Krakowczyk Ł,
Grajek M, et al. (2011) The Use of Radial Forearm Free Flap for
Total Lower Lip Reconstruction: The Analysis of 10 Consequentive
Cases and Quality of Life Evaluation. Otolaryngol 1:104.
doi:10.4172/2161-119X.1000104
Page 5 of 5
Volume 1 • Issue 2 • 1000104OtolaryngolISSN:2161-119X
Otolaryngology an open access journal
10. Zilinsky I, Winkler E, Weiss G, Haik J, Tamir J, et al.
(2001) Total lower lip reconstruction with innervated
muscle-bearing flaps: a modification of the Webster flap. Dermatol
Surg 27: 687-691.
11. Roldan JC, Teschke M, Fritzer E, Dunsche A, Harle F, et al.
(2007) Reconstruction of the lower lip: Rationale to preserve the
aesthetic units of the face. Plast Reconstr Surg 120:
1231-1239.
http://onlinelibrary.wiley.com/doi/10.1046/j.1524-4725.2001.00214.x/fullhttp://onlinelibrary.wiley.com/doi/10.1046/j.1524-4725.2001.00214.x/fullhttp://onlinelibrary.wiley.com/doi/10.1046/j.1524-4725.2001.00214.x/fullhttp://journals.lww.com/plasreconsurg/Abstract/2007/10000/Reconstruction_of_the_Lower_Lip__Rationale_to.15.aspxhttp://journals.lww.com/plasreconsurg/Abstract/2007/10000/Reconstruction_of_the_Lower_Lip__Rationale_to.15.aspxhttp://journals.lww.com/plasreconsurg/Abstract/2007/10000/Reconstruction_of_the_Lower_Lip__Rationale_to.15.aspx
TitleCorresponding authorAbstractIntroductionAim of the Study
Material and Methods ResultsDiscussionConclusionsTable 1Table
2Table 3Figure 1Figure 2Figure 3References