Embed Size (px)
Citation preview

NORTHWEST AIDS EDUCATION AND TRAINING CENTER
Primary Care of the HIV Infected Patient: 2014 Robert D. Harrington, M.D.

Primary Care of the HIV Infected Patient: 2014
• Primary Care Guidelines for the Management of Persons
Infected with HIV: 2013 Update by the HIV Medicine Association of the Infectious Diseases Society of America (Clinical Infectious Diseases, November, 2013)

Primary Care of the HIV Infected Patient: 2013
• The Initial Evaluation • Opportunistic Infection Prophylaxis • Starting Antiretroviral Therapy • Follow-up Care
• Laboratory • Cancer screening • Vaccinations • STD screening • Metabolic disorders

The Initial Evaluation

Case 1
• A 23 year old gay man presents after testing positive for HIV by “rapid test” at a night club.
• This is his first ever HIV test. He is sexually active with men exclusively, has ~ 10 partners per year and does not regularly use protection.
• He is well and without symptoms • His PMH is notable for depression, a history of
methamphetamine use, gonorrhea and syphilis • He is a college graduate, works in retail, drinks 6 beers on
weekend nights, smokes ½ ppd and no longer uses illicit drugs
• His physical exam is normal

Case 1
• Dates of HIV testing (negative and first positive) • ARV history (including adherence, drug resistance and drug
intolerances), CD4 nadir and HIV RNA zenith • HIV related illnesses • Cardiac, renal and hepatic disease history • TB exposure and risk • Travel and residence history (exposure to dimorphic fungi) • Mental health and substance abuse history • Sexual and STD history • Partner’s HIV status • Medications (watch for significant drug interactions) • Physical exam – particular attention to skin, mouth, lymphnodes,
neurological and cognitive exam, anogenital exam, fat distribution and evidence for liver disease
Elements of a comprehensive HIV history and exam !

Case 1
• HIV serology • CD4 count (absolute and percent) • HIV RNA level • HIV genotypic resistance testing • CBC, chemistries and urinalysis • Fasting lipids • G6PD level • TST or IGRA • Toxoplasma serology • Syphilis serologies (IgG if no h/o disease, otherwise RPR or VDRL) • Hepatitis B sAG, sAB, cAB – if isolated cAB, check HBV DNA • Hepatitis C AB (repeat annually if at risk), if AB+, check HCV RNA • Hepatitis A AB • CMV AB (if at low risk for infection, not MSM or IDU)
What laboratory testing is indicated at the initial visit? !

Occult HBV infection with isolated HBcAb
• Swiss cohort study: 57 patients with isolated HBcAb: Over time HBV DNA + in 51/57 (89.5%) (Eur J Clin Microbiol Infect Dis, 1998)
• Range in other studies from 0.6 to 83.3% - Khamduang, Clin Infect Dis, 2013 – 24% - Karaosmanoglu, HIV Clin Triala, 2013 – 7.5% - DiLello, Enferm Infecc Microbiol Clin, 2012 – 0.7% - N’Dri-Yoman, Antivir Ther, 2010 – 10% - Ramia, Int J STD AIDS, 2008 – 83.3% - Azadmanesh, Intervirology, 2008 – 13.6% - Neau, Clin Infect Dis, 2005 – 0.6%

Case 1
• What about an STD evaluation? - All women should be screen for Trichomoniasis - Men and women should be screened for GC and Chlamydia - Anyone testing + for GC or Chlamydia or Trichomoniasis should be
retested in 3 months due to high rates of re-infection • Cervical cancer screening?
- Pap smear on presentation and a second one 6 months later – then annually (if normal). If abnormal (any abnormality), refer for colposcopy
• Anal cancer screening? - Anyone practicing RAI or with a h/o genital warts and women with
abnormal pap smears should have an anal pap smear (weak recommendation, moderate quality evidence)
• Testosterone testing? - In men with decreased libido, ED, reduced bone mass, hot flashes: test
morning testosterone levels

Follow-up Care
Cancer screening • Women: pap smears annually • Women: mammograms annually > age 50 and individualized
for those 40-49 • Colon cancer screening: > 50; colonoscopy every 5-10 years or
annual FOBT • Anal cancer screening?

Anal Pap Smears?
High anal cancer rates (up to 137/100,000 py in MSM)!High rates of anal HPV + SIL in HIV+ women with cervical SIL!High grade SIL can progress to invasive cancer!Anal Pap smears can detect anal dysplasia (sensitivity ~69-93%)!IRC provides a safe and effective means to treat lesions (AIN2-3)!Survival from anal cancer is much improved if detected early! !
Calore, Diagnostic Cytol 2010!Hessol AIDS 2013!Tandon Am J OBGYN 2010!Berry Int J Cancer 2014!Sirera AIDS 2013!
Anal dysplasia rates 41-97% (M) and 14-28% (W)!Anal dysplasia can regress spontaneously!Anal Pap smear specificity 32-59%!Variable correlation between cytology and Bx results!No evidence that anal Paps improve outcomes!Low availability of HRA and IRC !
Nathan AIDS 2010!Chiao, CID, 2006!

Anal cancer screening: Madison Clinic
• Routine anal Pap smears are not done. • Individuals with a h/o anal warts need annual DRE and anoscopy
• Individuals with ongoing anal symptoms needs semi-annual DRE and anoscopy
• Individuals with a h/o anal cancer or anal dysplasia on previous studies should be referred for HRA

Case 1
• Vaccinations? - Influenza (inactivated) annually - S. pneumonia: PCV-13 once and Pnvax 23 twice, 5 years apart - HPV: women 9-26, men 9-21 and consider 22-26 - HAV: if HAV AB negative – test for seroconversion and re-vaccinate if
NR - HBV: (40ug Recombivax x 3 OR 2-20ug doses of Energix B x 4) if
sAG negative and sAB < 10. Consider, if isolated cAB+ and HBV DNA negative
- MMR: if not immune and CD4 > 200 - TDAP: once as an adult - Varicella: if not immune and CD4 > 200 - Zoster vaccine: consider in those > 60 and with CD4 > 200

Vaccinations
• Hepatitis A vaccine - Sero-reversion to negative happens in ~ 10% of patients.
• Hepatitis B vaccine - IDSA vaccination guidelines say “consideration of the higher (40 ug)
dosing” - Better response rates are reported with
• 40 ug dose • When patients are on ART with a suppressed viral load • At higher CD4 count
- Isolated HBcAb: check for HBV DNA: if negative then vaccinate with 3 dose series
• Zoster vaccine - Listed as contraindicated in HIV+ persons in the IDSA vaccination
guidelines - Preliminary results of zoster vaccination of 286 HIV+ persons on stable
ART showed safety and immunogenicity

Opportunistic Infection Prophylaxis

Primary Prophylaxis
Infection Criteria Treatment PCP CD4 < 200 or
CD4% < 14 or Thrush or ADI
TMP/SMX or dapsone or atovaquone or aerolsolized pentamidine
Tuberculosis PPD > 5 mm INH Toxoplasmosis IgG+ and CD4 <
100 TMP/SMX or dapsone + pyrimethamine + leukovorin
MAC CD4 < 50 Azithromycin VZV CD4 > 200 Vaccine HAV Vaccine HBV Vaccine Streptococcus pneumoniae
Vaccine
Influenza Vaccine

Follow-up Care

Follow-up Care
• Laboratory • HIV RNA: every 3-4 months, may be extended to every 6 months if suppressed for 2-3
years • CD4: every 3-4 months, may be extended to every 6-12 months in those with good CD4
reconstitution • HCV AB testing annually for those at risk • Repeat TST or IGRA for those who tested negative initially and had low CD4 counts and
who now have CD4 > 200 • Special tests: CCR5 testing of virus (if considering maraviroc) and HLA-B5701 testing (if
considering abacavir) • Repeat genotype resistance if there has been a delay since initial visit (superinfection)
• Vaccinations • Influenza (inactivated) annually • S. pneumonia: PCV-13 (once lifetime) and Pnvax23 (once and repeat in 5 years)
• STD screening • Annual testing for those at risk • Re-testing 3 months after any positive test for GC, CT or Trichomonas
• Metabolic disorders • FBS, A1C and fasting lipids before and 1-3 months after starting ART • Bone densitometry: in post menopausal women and men > 50

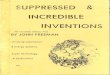
IGRA Results and CD4 Count Prospective longitudinal study of 830 HIV+ patients at a single center
• Distribution of QuantiFERON-TB Gold In Tube assay results according to the actual CD4>+ T cell count and the CD4>+ T cell nadir. *P<.001 and **P<.05, • Indeterminate test results at lower CD4 counts
Aichelburg M C et al. Clin Infect Dis. 2009;48:954-962

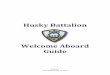
Tuberculosis Immune Responses and CD4 Count
Leidl Eur Respir J 2010: ;35:619-26!
Frequencies of positive immune responses in HIV-infected persons from Kampala Uganda, with <100, 100–250 and >250 CD4+ T-cells and HIV-uninfected controls T-Spot.TB test (□), QuantiFERON-TB (▓;), TST ≥5 mm (▒), ≥10 mm (░) ≥ 15mm (▪).!

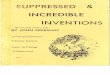
HIV Superinfection?
Redd AD, Lancet Infectious Diseases, Volume 13, Issue 7, 2013, 622 - 628 !
Worldwide cases of HIV-1 superinfection!
Rates of superinfection 0 to 7.7 % per yr!More common early after infection but has been !reported up to 2 years post-infection!

Questions!