Universitas udayana
Faculty of medicine
Myasthenia gravis
Name:Gythrie KarthikasonNim:1102005209
Myasthenia gravisDefinitionMyasthenia gravis is a chronic
autoimmune neuromuscular disease characterized by varying degrees
of weakness of the skeletal muscles of the body. The hallmark of
myasthenia gravis is muscle weakness that increases during periods
of activity and improves after periods of rest. The muscles that
control breathing and neck and limb movements may also be
affected.
EpidemiologyFrequencyUnited StatesMyasthenia gravis is uncommon.
Estimated annual incidence is 2 per
1,000,000.Mortality/MorbidityRecent advances in treatment and care
of critically ill patients have resulted in marked decrease in the
mortality rate. The rate is now 3-4%, with principal risk factors
being age older than 40 years, short history of severe disease, and
thymoma. Previously, the mortality rate was as high as 30-40%.
SexThe female-to-male ratio is said classically to be 6:4, but as
the population has aged, the incidence is now equal in males and
females. AgeMyasthenia gravis presents at any age. Female incidence
peaks in the third decade of life, whereas male incidence peaks in
the sixth or seventh decade. Mean age of onset is 28 years in
females and 42 years in males.
Causes and Risk Factors for Myasthenia Gravis MG usually is
caused by a malfunction of the immune system. The causative factor
is unknown, but the disorder may have a genetic link. Causes
include a genetic defect, which results in congenital MG, and the
circulation of maternal antibodies through the placenta, which
result in transient neonatal MG. Acetylcholine (ACh) is a
neurotransmitter that is involved in the transfer of information to
muscle tissue. In myasthenia gravis, cells that bind to other cells
to neutralize or destroy them (called antibodies) destroy
acetylcholine receptor sites (AChR) in areas of muscle tissue that
receive nerve impulses (called neuromuscular junctions), preventing
nerve impulses from reaching the muscles. This results in weakness
and rapid fatigue in affected muscles.
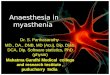
Pathophysiology of myasthenia gravis.Myasthenia gravis (MG) is
arguably the best understood autoimmune disease, and its study has
also led to fundamental appreciation of mechanisms of neuromuscular
transmission. MG is caused by antibodies against the acetylcholine
receptor (AChR), which produce a compromise in the end-plate
potential, reducing the safety factor for effective synaptic
transmission. It is clear that AChR antibody destruction of the
postsynaptic surface is dependent on complement activation. A
muscle-specific kinase has been recently found to be an antigenic
target in MG patients without antibodies against the AChR.
Autoantibody production in MG is a T-cell-dependent process, but
how a breakdown in tolerance occurs is not known. In MG there is an
interesting differential involvement of muscle groups, in
particular, the extraocular muscles. This article reviews normal
neuromuscular transmission, mechanisms of the autoimmune process of
MG, and differential susceptibility of eye muscles to MG.
Symptoms Onset of the disorder may be sudden Affect any
voluntary muscle The facial expression and swallowing are most
frequently affected Weakness of muscles that control eye and eyelid
movement causing blurred or double vision (diplopia) Difficulty in
swallowing and slurred speech may be the first signs Drooping of
one or both eyelids (ptosis), Unstable or waddling gait, weakness
in arms, hands, fingers, legs, and neck, Shortness of breath
Impaired speech (dysarthria).
DiagnosisMG can be a difficult diagnosis, as the symptoms can be
subtle and hard to distinguish from both normal variants and other
neurological disorders. A thorough physical examination can reveal
easy fatigability, with the weakness improving after rest and
worsening again on repeat of the exertion testing. Applying ice to
weak muscle groups characteristically leads to improvement in
strength of those muscles. Additional tests are often performed, as
mentioned below. Furthermore, a good response to medication can
also be considered a sign of autoimmune pathology.
TreatmentAnticholinesterase agents such as neostigmine and
pyridostigmine, which help improve neuromuscular transmission and
increase muscle strength.mmunosuppressive drugs such as prednisone,
cyclosporine, and azathioprine which help improve muscle strength
by suppressing the production of abnormal
antibodies.ThymectomyPlasmapheresis a procedure in which abnormal
antibodies are removed from the blood, and high-dose intravenous
immune globulin, which temporarily modifies the immune system and
provides the body with normal antibodies from donated blood.