Embed Size (px)
Citation preview
1
ShockShockMyoung Soo Kim M.D.Myoung Soo Kim [email protected]@wonju.yonsei.ac.kr
http://myhome.hananet.net/~kim63http://myhome.hananet.net/~kim63
Department of SurgeryYonsei University Wonju College of Medicine
http://gs.yonsei.ac.kr
Definition of Shock
“ Syndrome that results from inadequate perfusion of tissues “
insufficient to meet the metabolic demands of those tissuealterations in cellular metabolism
: cellular dysfunction / elaboration of inflammatory mediators / cellular injury
multiple organ dysfunction syndrome(MODS) or frank organ failure
WCH-GS, 1998
2
Classification of shock
Classification MechanismsAssociated
Clinical ConditionsHemorrhagic hemorrhagic loss trauma,
G-I bleeding,ruptured aneurysms
Hypovolemic
Plasma volume loss extravascular fluidsequestration
Pancreatitis, burns,bowel obstruction,excessive gastrointestinal loss
Intrinsic Infarction (MI),cardiomyopathy,valvular heart disease,
Cardiologic
Extrinsic
heart is unable togenerate an adequatecardiac output tomaintain tissue perfusion Compressive or obstructive
lesionNeurologic Failure of the sympathetic nervous system to
maintain normal vascular tone decreasedarteriolar and venous vasomotor tone
spinal cord injury,severe head injury,spinal anesthesia
Systemic inflammatoryresponse syndrome(SIRS)
(1) Infectious (septic) (2) Noninfectious
Septic shockSystemic Sepsis
Anaphylatic AnaphylaxisHypoadrenal Adrenal insufficiency
Vasogenic
Traumatic
Release ofendogenous orexogenous vasoactivemediators
Decreased arteriolarand venous vasomotortone
Trauma
Patient monitoring(1)
WCH-GS, 1998
Early treatment before irreversible tissue damageIdeal monitoring
= “monitoring of tissue and cell level perfusion”but the ideal monitoring is not possible
1. Conventional monitoring techniques ; based on physical examination or laboratory data
blood pressure, heart rate, central venous pressure, hematocrit, arterial blood gases, and urine output : more objective capillary refill, skin temperature, skin turgor
“ Poor relationship between index and clinical status”
" 그럼에도불구하고이러한 monitoring은초기 Shock치료의지표로유용하다"
3
Patient monitoring(2)
2. Adjunctive monitoring techniques. : invasive / costly / potentially hazardous
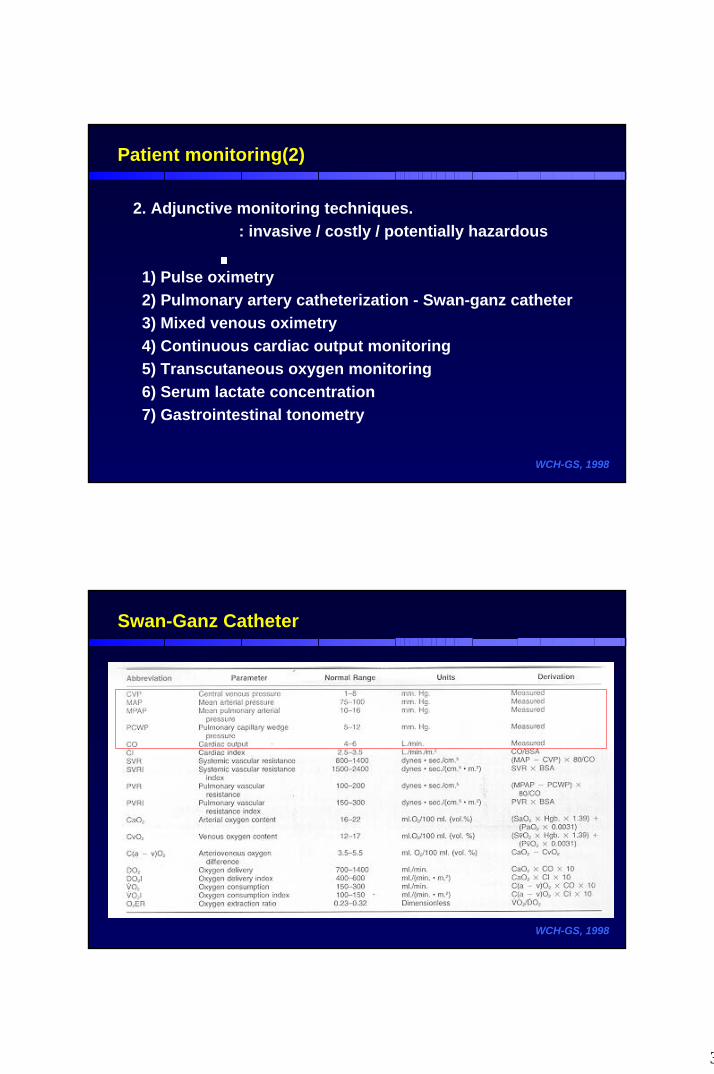
1) Pulse oximetry2) Pulmonary artery catheterization - Swan-ganz catheter3) Mixed venous oximetry4) Continuous cardiac output monitoring5) Transcutaneous oxygen monitoring6) Serum lactate concentration7) Gastrointestinal tonometry
WCH-GS, 1998
Swan-Ganz Catheter
WCH-GS, 1998
4
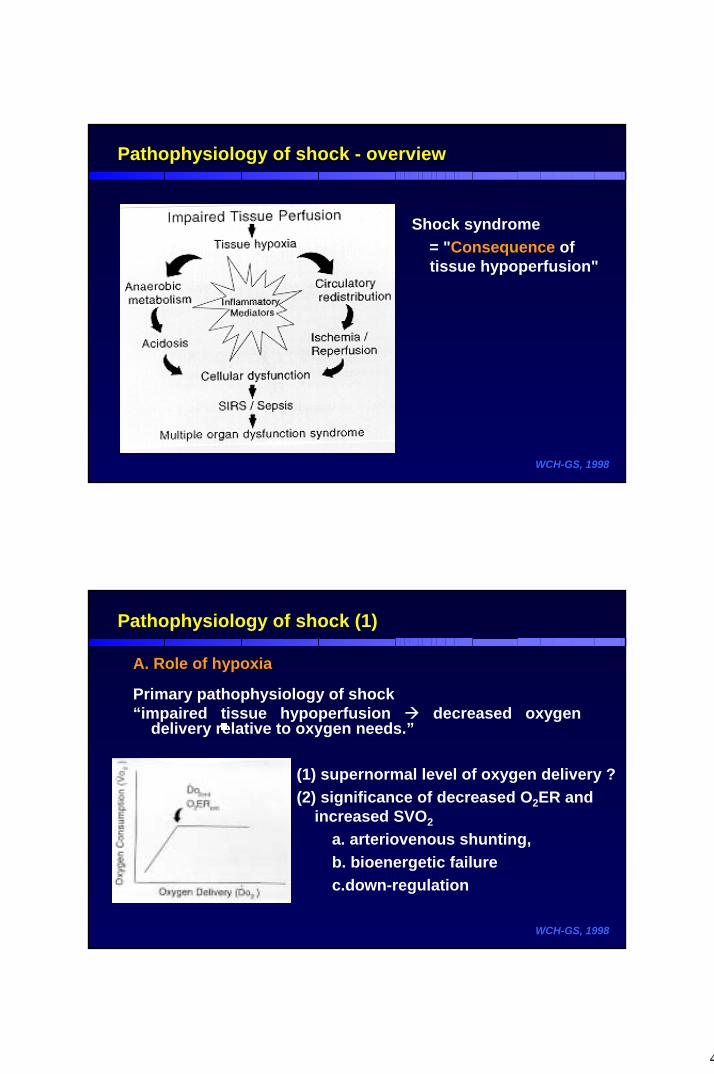
Pathophysiology of shock - overview
Shock syndrome = "Consequence of tissue hypoperfusion"
WCH-GS, 1998
Pathophysiology of shock (1)
A. Role of hypoxia
Primary pathophysiology of shock “impaired tissue hypoperfusion decreased oxygen
delivery relative to oxygen needs.”
WCH-GS, 1998
(1) supernormal level of oxygen delivery ? (2) significance of decreased O2ER and
increased SVO2
a. arteriovenous shunting, b. bioenergetic failurec.down-regulation
5
Pathophysiology of shock (2)
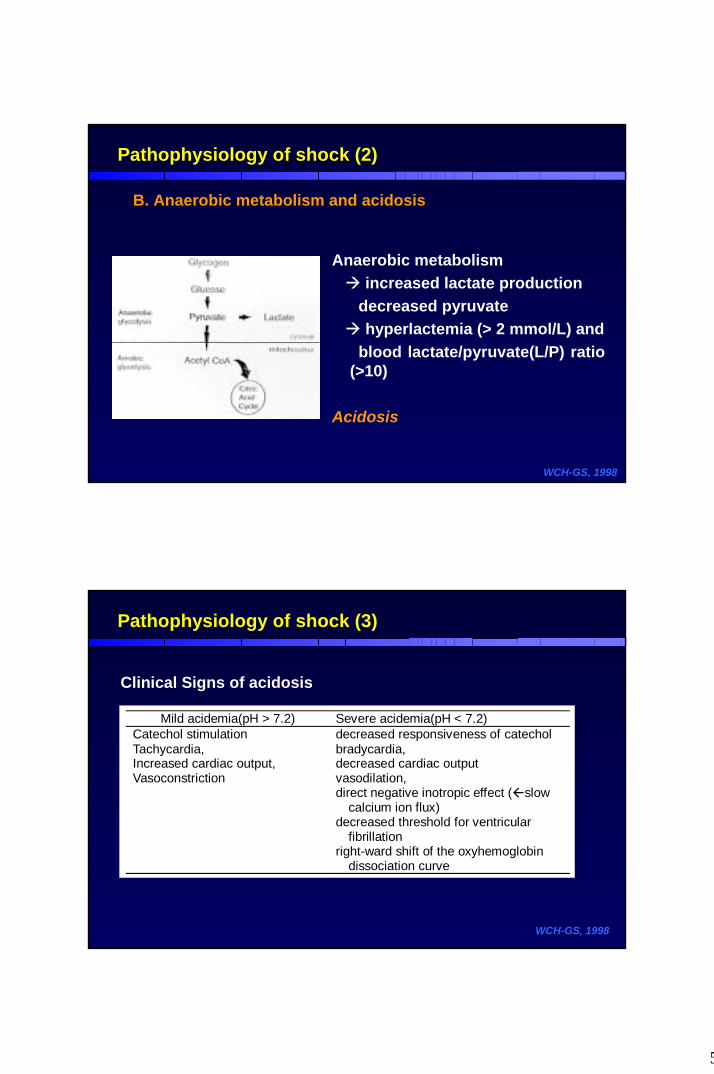
B. Anaerobic metabolism and acidosis
WCH-GS, 1998
Anaerobic metabolism increased lactate production
decreased pyruvatehyperlactemia (> 2 mmol/L) and
blood lactate/pyruvate(L/P) ratio (>10)
Acidosis
Pathophysiology of shock (3)
WCH-GS, 1998
Mild acidemia(pH > 7.2) Severe acidemia(pH < 7.2)Catechol stimulation decreased responsiveness of catecholTachycardia,Increased cardiac output,Vasoconstriction
bradycardia,decreased cardiac outputvasodilation,direct negative inotropic effect ( slow
calcium ion flux)decreased threshold for ventricular
fibrillationright-ward shift of the oxyhemoglobin
dissociation curve
Clinical Signs of acidosis
6
Pathophysiology of shock (4)
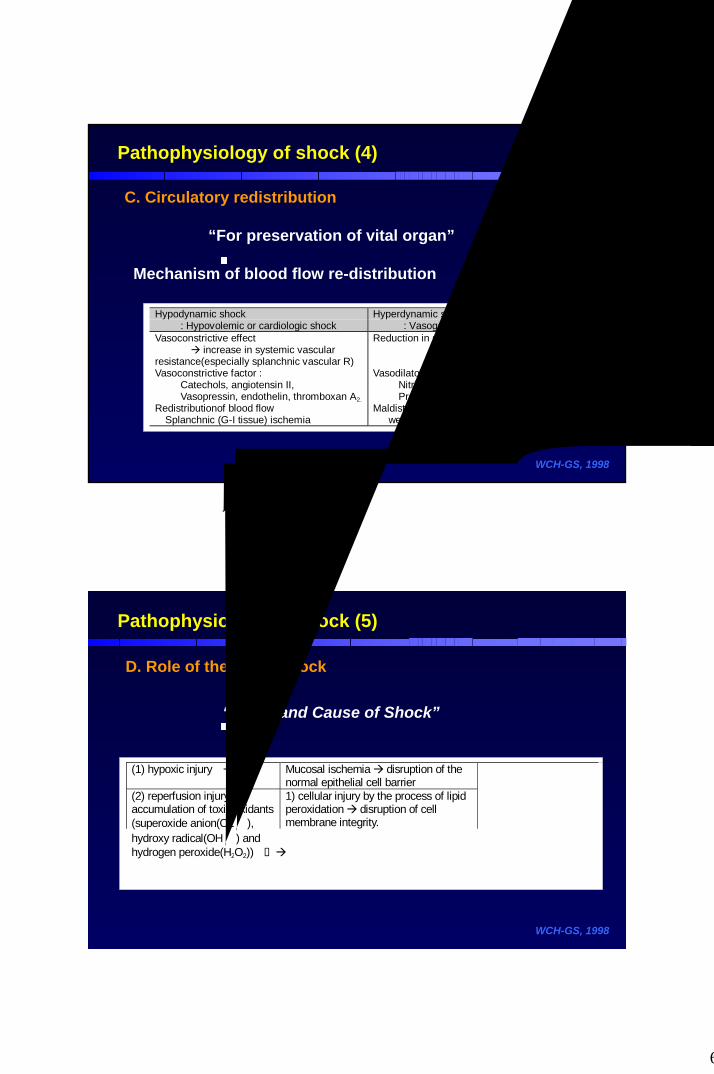
C. Circulatory redistribution
“For preservation of vital organ”
Mechanism of blood flow re-distribution
WCH-GS, 1998
Hypodynamic shock : Hypovolemic or cardiologic shock
Hyperdynamic shock : Vasogenic shock(sepsis state)
Vasoconstrictive effect increase in systemic vascularresistance(especially splanchnic vascular R)
Reduction in systemic vascular resistance
Vasoconstrictive factor : Catechols, angiotensin II, Vasopressin, endothelin, thromboxan A2.
Vasodilatory mediators: Nitric oxide, prostaglandin E2, Prostacyclin, interleukin-2, bradykinin
Redistributionof blood flow Splanchnic (G-I tissue) ischemia
Maldistribution of blood flow well-perfused regions vs. ischemic region
Pathophysiology of shock (5)
D. Role of the gut in shock
“Effect and Cause of Shock”
WCH-GS, 1998
(1) hypoxic injury Mucosal ischemia disruption of thenormal epithelial cell barrier1) cellular injury by the process of lipidperoxidation disruption of cellmembrane integrity.
(2) reperfusion injury accumulation of toxic oxidants(superoxide anion(O2ㆍ),hydroxy radical(OHㆍ) andhydrogen peroxide(H2O2))
2) chemotactic role : tumor necrosisfactor-alpha(TNF-α), platelet activatingfactor(PAF), interleukin(IL)-1 and IL-6,and others
Intestinal mucosal injuryIncreased permeabilityTranslocation of gut
bacterial and toxinmaterial
amplify SIR andMODS
7
Mediators of Shock and Sepsis -overview
1) Endotoxin 2) Complement Fragments3) Eicosanoids 4) Kinins5) Nitric oxide6) Cytokines7) Platelet activating factor8) Endogenous opioids9) Oxidants
10) Neuroendocrine mediators
WCH-GS, 1998
Mediators of Shock and Sepsis (1)
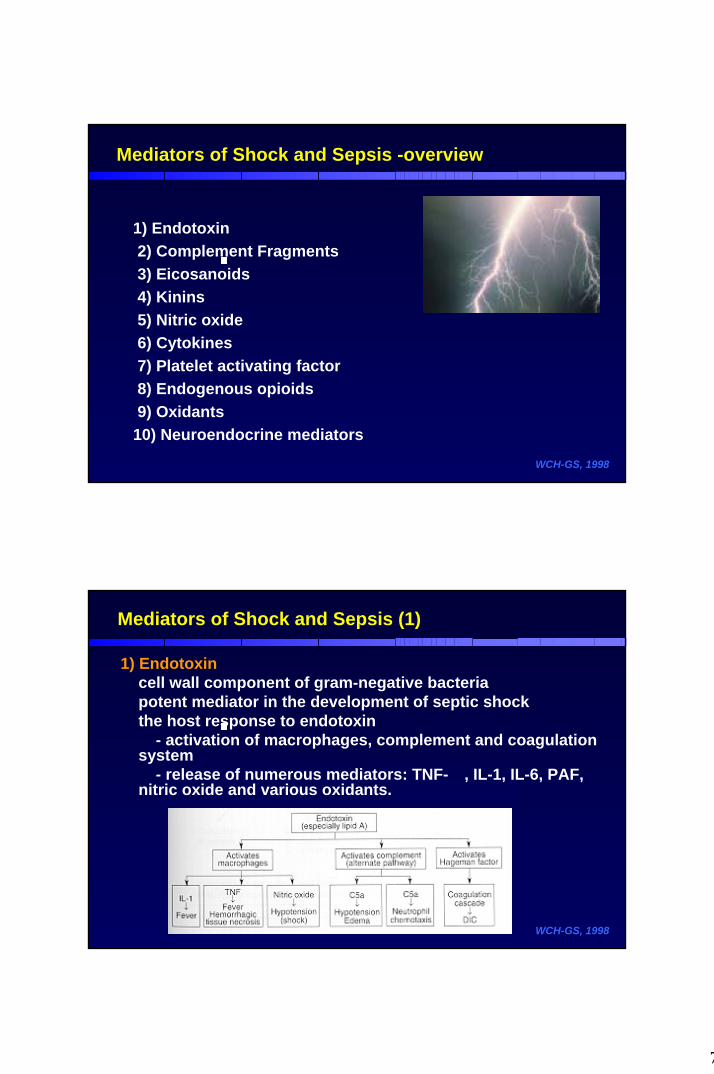
1) Endotoxincell wall component of gram-negative bacteriapotent mediator in the development of septic shockthe host response to endotoxin
- activation of macrophages, complement and coagulation system
- release of numerous mediators: TNF-α, IL-1, IL-6, PAF, nitric oxide and various oxidants.
WCH-GS, 1998
8
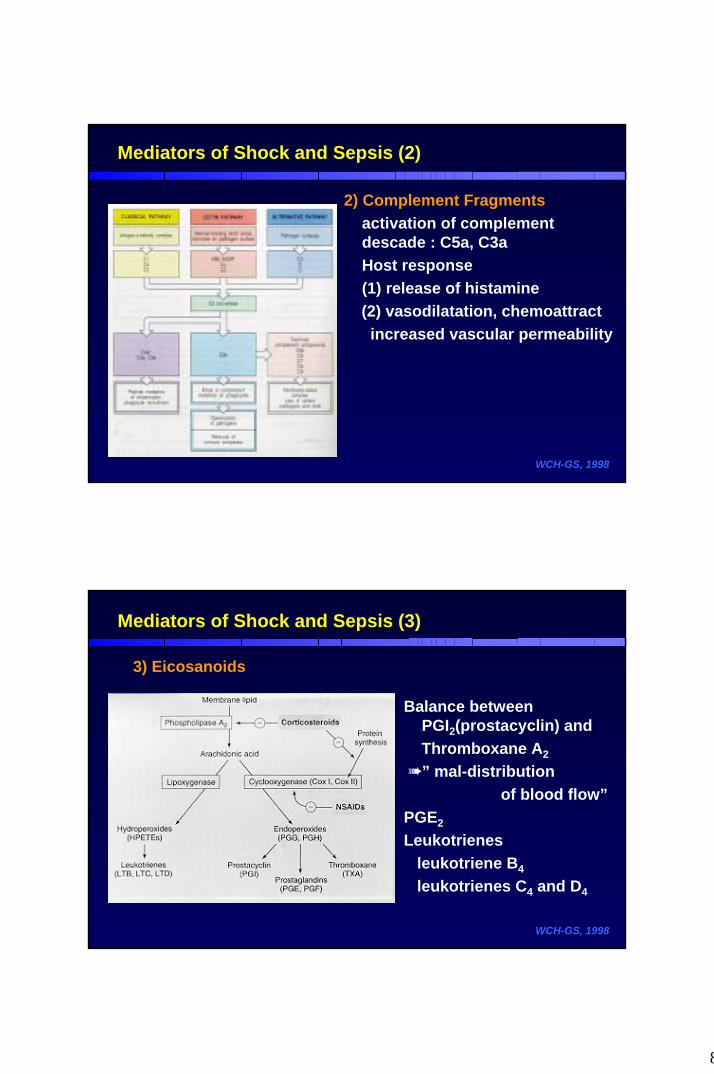
2) Complement Fragmentsactivation of complement descade : C5a, C3aHost response (1) release of histamine (2) vasodilatation, chemoattractincreased vascular permeability
WCH-GS, 1998
Mediators of Shock and Sepsis (2)
Mediators of Shock and Sepsis (3)
3) Eicosanoids
WCH-GS, 1998
Balance between PGI2(prostacyclin) and Thromboxane A2
” mal-distribution of blood flow”
PGE2
Leukotrienesleukotriene B4
leukotrienes C4 and D4
9
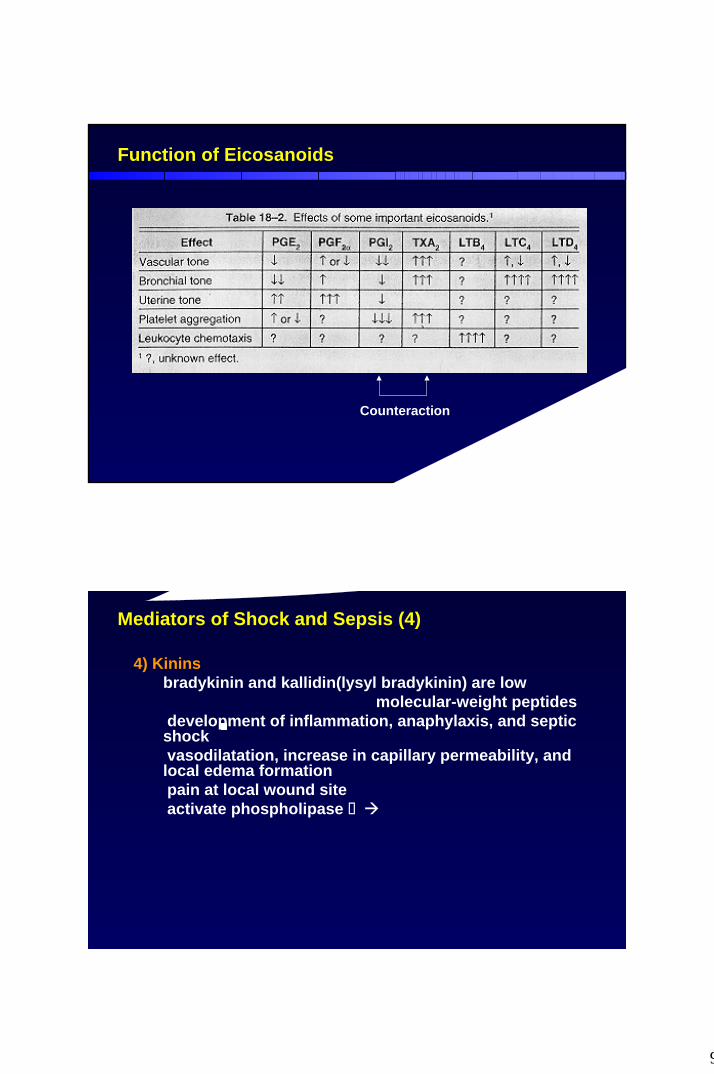
Function of Eicosanoids
WCH-GS, 1998
Counteraction
Mediators of Shock and Sepsis (4)
4) Kininsbradykinin and kallidin(lysyl bradykinin) are low
molecular-weight peptides① development of inflammation, anaphylaxis, and septic
shock② vasodilatation, increase in capillary permeability, and
local edema formation③ pain at local wound site④ activate phospholipase formation of eicosanoids
further amplification of inflammatory response.
5) Nitric oxideendothelium derived relaxing factor
WCH-GS, 1998
10
Mediators of Shock and Sepsis (5)
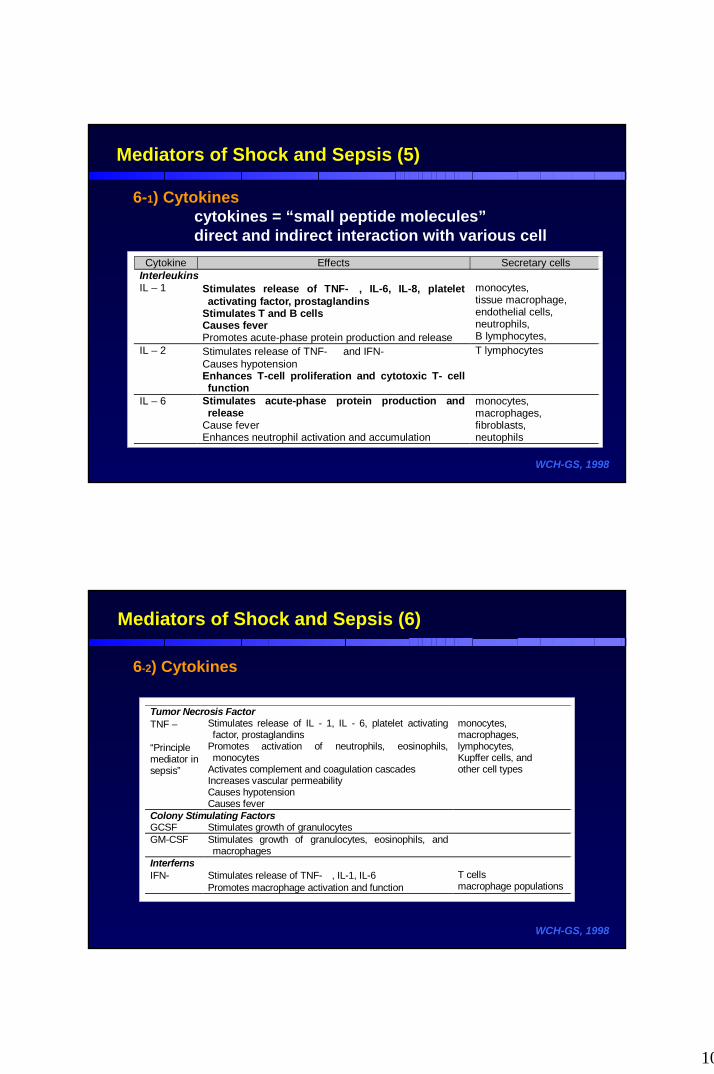
6-1) Cytokinescytokines = “small peptide molecules”direct and indirect interaction with various cell
WCH-GS, 1998
Cytokine Effects Secretary cellsInterleukinsIL – 1 Stimulates release of TNF-α, IL-6, IL-8, platelet
activating factor, prostaglandinsStimulates T and B cellsCauses feverPromotes acute-phase protein production and release
monocytes,tissue macrophage,endothelial cells,neutrophils,B lymphocytes,
IL – 2 Stimulates release of TNF-α and IFN-γCauses hypotensionEnhances T-cell proliferation and cytotoxic T- cellfunction
T lymphocytes
IL – 6 Stimulates acute-phase protein production andrelease
Cause feverEnhances neutrophil activation and accumulation
monocytes,macrophages,fibroblasts,neutophils
Mediators of Shock and Sepsis (6)
6-2) Cytokines
WCH-GS, 1998
Tumor Necrosis FactorTNF – α
“Principlemediator insepsis”
Stimulates release of IL - 1, IL - 6, platelet activatingfactor, prostaglandins
Promotes activation of neutrophils, eosinophils,monocytes
Activates complement and coagulation cascadesIncreases vascular permeabilityCauses hypotensionCauses fever
monocytes,macrophages,lymphocytes,Kupffer cells, andother cell types
Colony Stimulating FactorsGCSF Stimulates growth of granulocytesGM-CSF Stimulates growth of granulocytes, eosinophils, and
macrophagesInterfernsIFN-γ Stimulates release of TNF-α, IL-1, IL-6
Promotes macrophage activation and functionT cellsmacrophage populations
11
Mediators of Shock and Sepsis (7)
7) Platelet activating factoramplify TNF-α and IL-1.
8) Endogenous opioidsenkephalins and beta-endorphins
9) Oxidantsreactive oxygen metabolitessuperoxide anion(O2ㆍ ) , hydrogen peroxide(H2O2), hydroxyl radical(OHㆍ)Ischemia-reperfusion injury
- activated neutrophilsDeleterious effects of oxidants : multiple
WCH-GS, 1998
Mediators of Shock and Sepsis (8)
WCH-GS, 1998
10) Neuroendocrine mediators; injury, stress, infection catabolic or stress
hormones(catechols, cortisol, and glucagon).catechols(epinephrine and norepinephrine)
- tachycardia, inotropy, peripheral vasoconstriction, increased metabolic rate,increased glycogenolysis / gluconeogenesis, and inhibition of insulin secretion
cortisol - proteolysis, lipolysis and gluconeogenesisglucagon - gluconeogenesis and glucose intolerancerenin-angiotensin system
- angiotensin II further vasoconstriction ischemia/shock
- aldosterone and vasopressin : salt and water retention
12
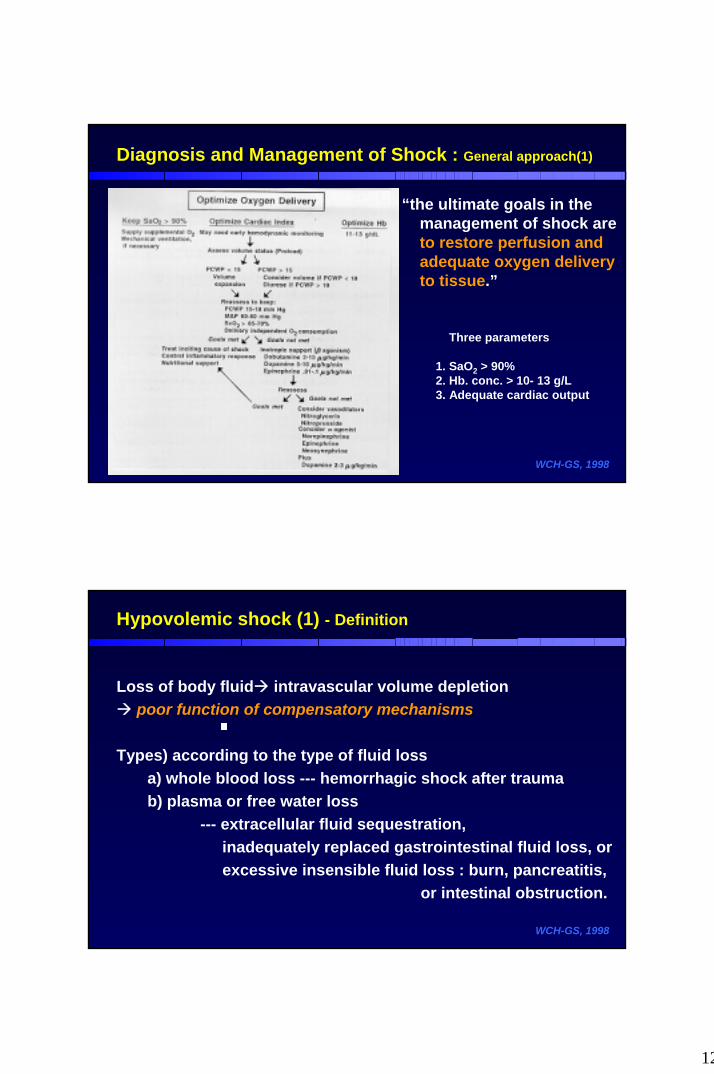
Diagnosis and Management of Shock : General approach(1)
“the ultimate goals in the management of shock are to restore perfusion and adequate oxygen delivery to tissue.”
WCH-GS, 1998
Three parameters
1. SaO2 > 90%2. Hb. conc. > 10- 13 g/L3. Adequate cardiac output
Hypovolemic shock (1) - Definition
Loss of body fluid intravascular volume depletionpoor function of compensatory mechanisms
Types) according to the type of fluid loss a) whole blood loss --- hemorrhagic shock after traumab) plasma or free water loss
--- extracellular fluid sequestration, inadequately replaced gastrointestinal fluid loss, orexcessive insensible fluid loss : burn, pancreatitis,
or intestinal obstruction.
WCH-GS, 1998
13
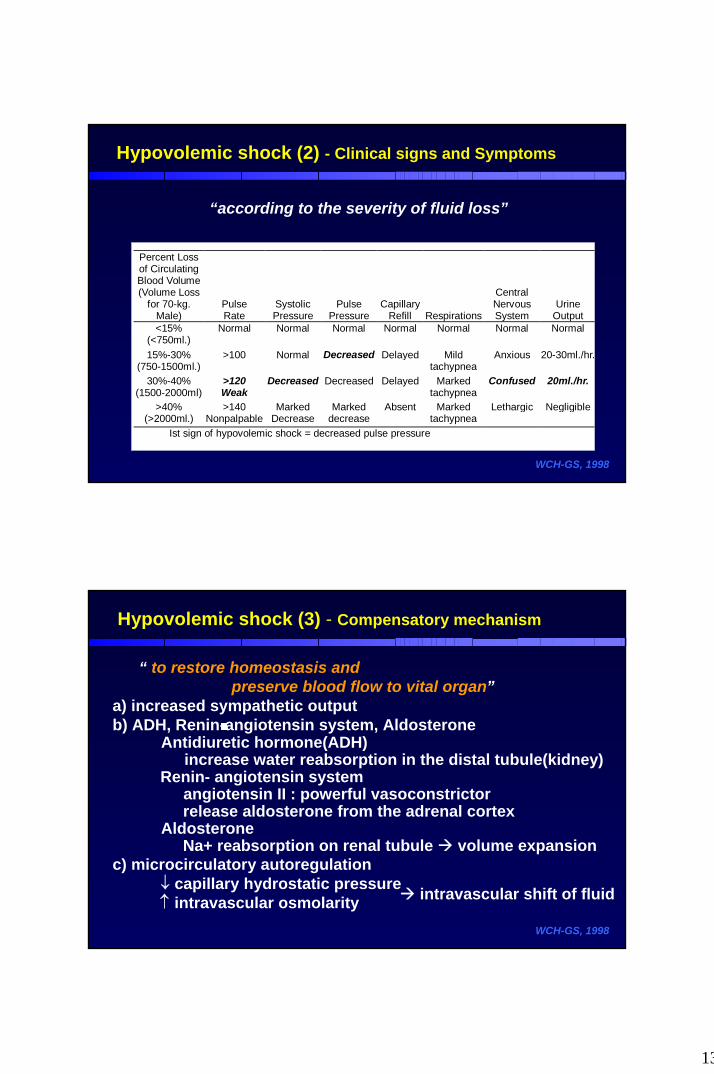
Hypovolemic shock (2) - Clinical signs and Symptoms
“according to the severity of fluid loss”
WCH-GS, 1998
Percent Lossof CirculatingBlood Volume(Volume Loss
for 70-kg.Male)
PulseRate
SystolicPressure
PulsePressure
CapillaryRefill Respirations
CentralNervousSystem
UrineOutput
<15%(<750ml.)
Normal Normal Normal Normal Normal Normal Normal
15%-30%(750-1500ml.)
>100 Normal Decreased Delayed Mildtachypnea
Anxious 20-30ml./hr.
30%-40%(1500-2000ml)
>120Weak
Decreased Decreased Delayed Markedtachypnea
Confused 20ml./hr.
>40%(>2000ml.)
>140Nonpalpable
MarkedDecrease
Markeddecrease
Absent Markedtachypnea
Lethargic Negligible
Ist sign of hypovolemic shock = decreased pulse pressure
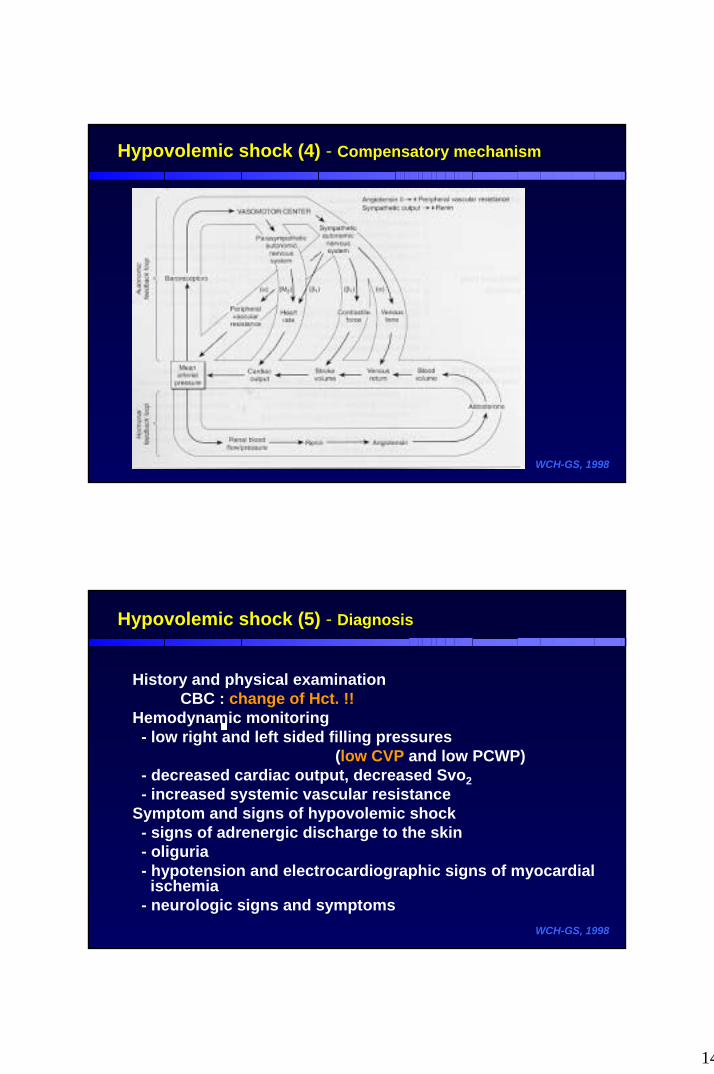
Hypovolemic shock (3) - Compensatory mechanism
WCH-GS, 1998
“ to restore homeostasis and preserve blood flow to vital organ”
a) increased sympathetic output b) ADH, Renin-angiotensin system, Aldosterone
Antidiuretic hormone(ADH)increase water reabsorption in the distal tubule(kidney)
Renin- angiotensin systemangiotensin II : powerful vasoconstrictorrelease aldosterone from the adrenal cortex
AldosteroneNa+ reabsorption on renal tubule volume expansion
c) microcirculatory autoregulation↓ capillary hydrostatic pressure↑ intravascular osmolarity intravascular shift of fluid
14
Hypovolemic shock (4) - Compensatory mechanism
WCH-GS, 1998
Hypovolemic shock (5) - Diagnosis
History and physical examinationCBC : change of Hct. !!
Hemodynamic monitoring- low right and left sided filling pressures
(low CVP and low PCWP)- decreased cardiac output, decreased Svo2- increased systemic vascular resistance
Symptom and signs of hypovolemic shock- signs of adrenergic discharge to the skin- oliguria- hypotension and electrocardiographic signs of myocardial
ischemia- neurologic signs and symptoms
WCH-GS, 1998
15
Hypovolemic shock (6) -Treatment
A. Initial Resuscitation Phase1. airway and ventilation and oxygenation2. bleeding control3. I.V. Line 4. fluid resuscitation ;
a) isotonic electrolyte solution(such as Ringer's lactate)- rapid infusion 1-2 L/hr- refractory hypotension after infusion continuous
blood lossb) blood transfusion
- fully cross-matched blood
※ Paradox of fluid resuscitation
WCH-GS, 1998
Hypovolemic shock (7) -Treatment
WCH-GS, 1998
B. Monitoring of resuscitation- central venous pressure, pulmonary artery catheter monitoring
- urinary output to a rate of 0.5 to 1.0ml/kg/hour - normal heart rate and blood pressure- adequate capillary refill - normal sensorium
C. Sequestration phase management- maintain fluid resuscitation for 1 day- until diuretic phase
D. Diuretic phase- normal body fluid compartment
16
Hypovolemic shock (8) -Treatment
WCH-GS, 1998
E. Adjunctive measure(1) pneumatic anti-shock garment(PASG)
- currently, only indication = pelvic fracture(2) colloid solutions and hypertonic saline solutions
- colloid solutions : albumin, fresh frozen plasma,dextran, hetastarch
- hypertonic solutions : 3% NaCl or 7.5% NaCl - theoretical advantage of hypertonic solution- does not use routinely
3) blood substitutes ; used in clinical study base- perfluorocarbon-based solutions- various stroma-free hemoglobin solutions
Traumatic Shock
WCH-GS, 1998
Characteristics (vs. hypovolemic shock)
(1) larger volume losses(2) greater fluid sequestration in the extravascular
compartments(3) intense activation of inflammatory mediators and
development of SIRS의차이점을가지는데
poorly response to initial fluid replacement therapyneed more intensive managementcommon Multiple Organ Dysfunction / Failure
17
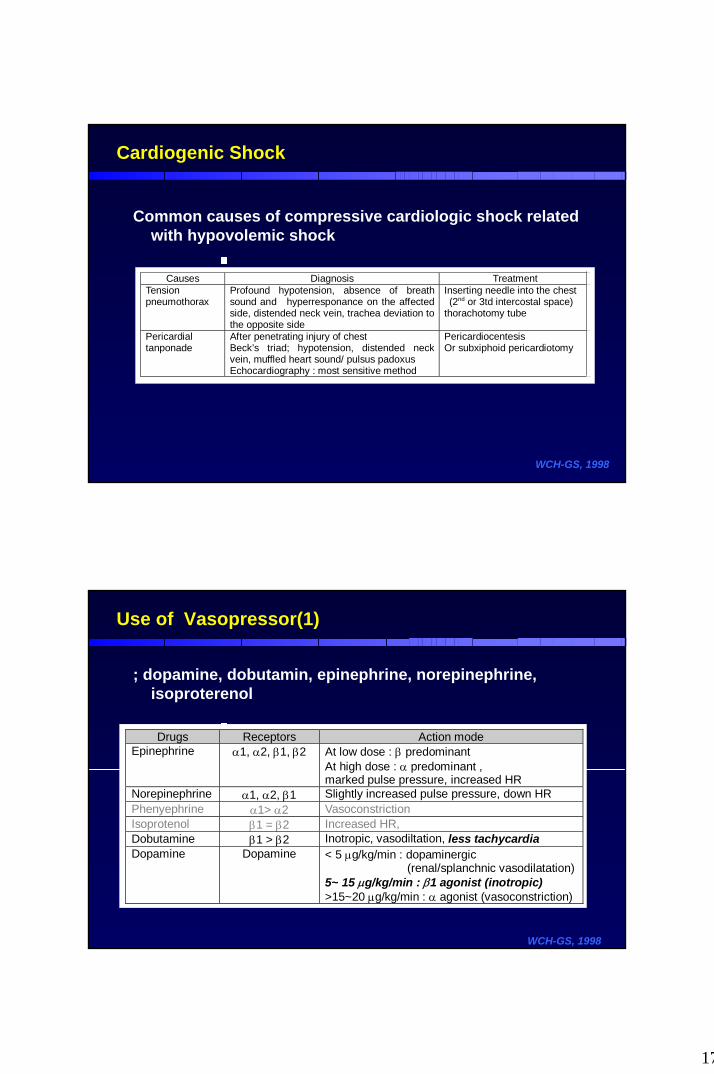
Common causes of compressive cardiologic shock related with hypovolemic shock
WCH-GS, 1998
Cardiogenic Shock
Causes Diagnosis TreatmentTensionpneumothorax
Profound hypotension, absence of breathsound and hyperresponance on the affectedside, distended neck vein, trachea deviation tothe opposite side
Inserting needle into the chest (2nd or 3td intercostal space)thorachotomy tube
Pericardialtanponade
After penetrating injury of chestBeck’s triad; hypotension, distended neckvein, muffled heart sound/ pulsus padoxusEchocardiography : most sensitive method
PericardiocentesisOr subxiphoid pericardiotomy
Use of Vasopressor(1)
; dopamine, dobutamin, epinephrine, norepinephrine, isoproterenol
WCH-GS, 1998
Drugs Receptors Action modeEpinephrine α1, α2, β1, β2 At low dose : β predominant
At high dose : α predominant ,marked pulse pressure, increased HR
Norepinephrine α1, α2, β1 Slightly increased pulse pressure, down HRPhenyephrine α1> α2 VasoconstrictionIsoprotenol β1 = β2 Increased HR,Dobutamine β1 > β2 Inotropic, vasodiltation, less tachycardiaDopamine Dopamine < 5 µg/kg/min : dopaminergic
(renal/splanchnic vasodilatation)5~ 15 µg/kg/min : β1 agonist (inotropic)>15~20 µg/kg/min : α agonist (vasoconstriction)
18
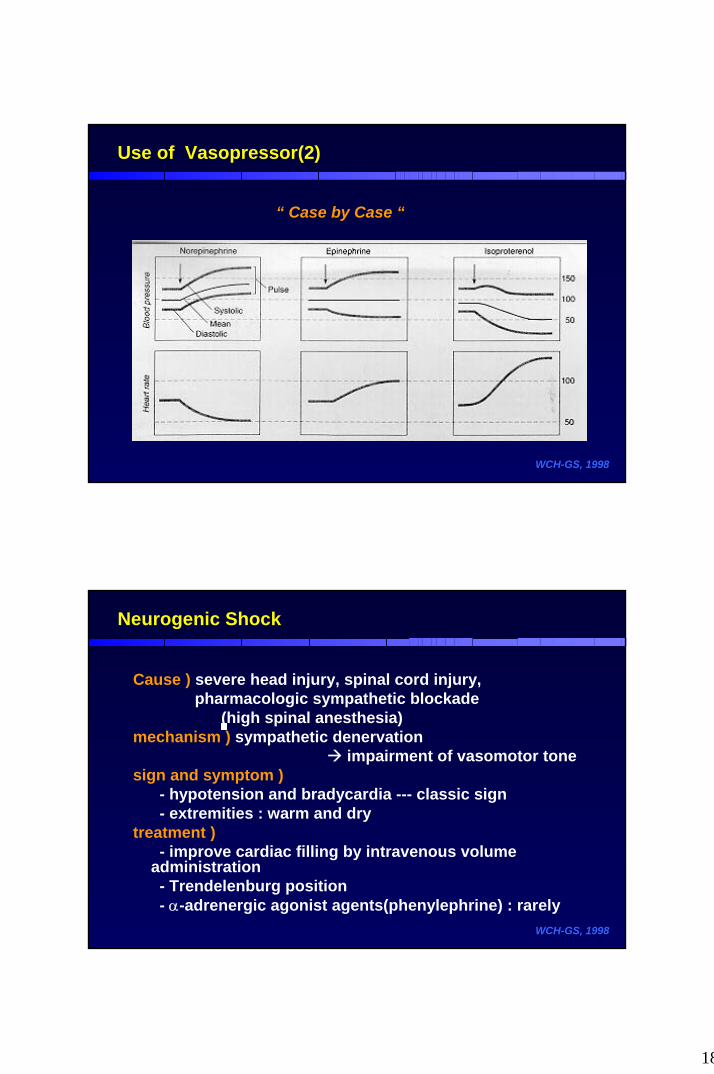
Use of Vasopressor(2)
WCH-GS, 1998
“ Case by Case “
Neurogenic Shock
Cause ) severe head injury, spinal cord injury,pharmacologic sympathetic blockade
(high spinal anesthesia)mechanism ) sympathetic denervation
impairment of vasomotor tonesign and symptom )
- hypotension and bradycardia --- classic sign- extremities : warm and dry
treatment )- improve cardiac filling by intravenous volume
administration- Trendelenburg position- α-adrenergic agonist agents(phenylephrine) : rarely
WCH-GS, 1998
19
Anaphylactic and Anaphylactoid shock(1)
Anaphylaxis : allergic response mediated by IgE antibody.antigens - insect venom, drugs, and certain foods.
Anaphylactoid reaction : not immunologically mediated.intravenous radiographic contrast dyes, narcotics in high doses,various colloids(dextrans and hydroxyethyl starch)
Mechanism )- activation and release of inflammatory mediators
(anaphylatoxins C3a and C5a, histamine, kinins, prostaglandins and others)
- vasodilatation, increased capillary permeability, bronchospasm, airway edema, circulatory collapse secondary to a sudden decrease in systemic vascular resistance and a fall in cardiac output.
WCH-GS, 1998
Anaphylactic and Anaphylactoid shock(2)
Management )- adequate airway / oxygen supply / epinephrine injection.
0.3 to 0.5 ml of epinephrine in a 1:1000 dilution/SQintravenous continuos infusion, rate of 0.5 to 5㎍/minintravenous bolus injection, 0.1 to 0.2 ml. of a 1:1000 solution.
- prevent bronchospasminhaled nebulized solutions of metaproterenol or albuterolaminophylline(5-6 mg./kg. load, followed by 0.3-0.9 mg./kg./hour)corticosteroids(250mg. hydrocortisone intravenous every 6 hours)antihistamine(25-50mg. hydroxyzine or diphenhydramine IM)
WCH-GS, 1998
20
Hypoadrenal shock
Must rule out hypoadrenal shock if (1) history of glucocorticoid therapy
(2) refractory to fluid and pressure resuscitation
Diagnosis )Addison’s disease without hyperpigmentation / weight
loss / G-I symptomsLab. : Hypoglycemia with hypotension,
hyponatremia, hyperkalemiaRapid ACTH stimulation test
(250 µg of ACTH, single dose, 30 min-60 min) Treatment ) steroid replacement and hydration
Dexamethasone 4 mg (Glucocorticoid replacement)Hydrocortisone 100 mg (mineralcorticoid replacement)
WCH-GS, 1998
Shock associated with SIRS, Sepsis and MOD
Background)
Systemic inflammatory mediator With infection versus Without infection
WCH-GS, 1998
21
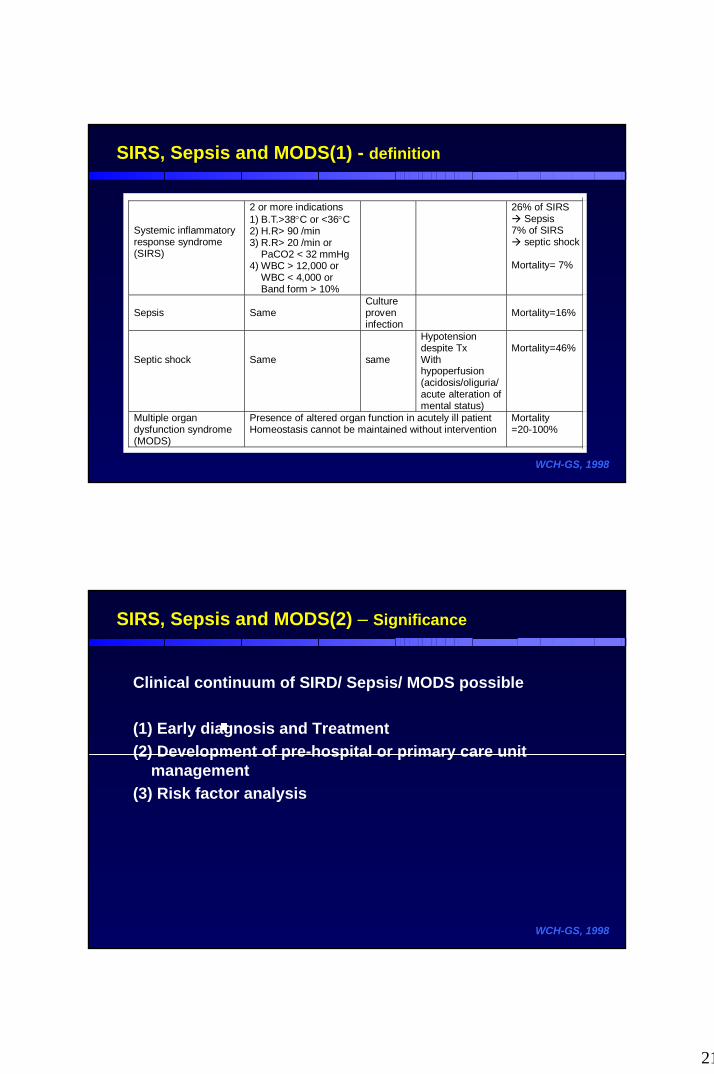
SIRS, Sepsis and MODS(1) - definition
WCH-GS, 1998
Systemic inflammatoryresponse syndrome(SIRS)
2 or more indications1) B.T.>38°C or <36°C2) H.R> 90 /min3) R.R> 20 /min or
PaCO2 < 32 mmHg4) WBC > 12,000 or
WBC < 4,000 orBand form > 10%
26% of SIRS Sepsis
7% of SIRS septic shock
Mortality= 7%
Sepsis SameCultureproveninfection
Mortality=16%
Septic shock Same same
Hypotensiondespite TxWithhypoperfusion(acidosis/oliguria/acute alteration ofmental status)
Mortality=46%
Multiple organdysfunction syndrome(MODS)
Presence of altered organ function in acutely ill patientHomeostasis cannot be maintained without intervention
Mortality=20-100%
SIRS, Sepsis and MODS(2) – Significance
Clinical continuum of SIRD/ Sepsis/ MODS possible
(1) Early diagnosis and Treatment (2) Development of pre-hospital or primary care unit
management(3) Risk factor analysis
WCH-GS, 1998
22
SIRS, Sepsis and MODS(3) - Development of MODS
“ Two hit theory of the development of MODS”
WCH-GS, 1998
PrimaryMODS
Early and direct result of insultex) thoracic trauma- pul. Contusion rhabdomyolysis – renal failureFig
SecondaryMODS
Amplified systemic inflammatoryresponse late and remote organ dysfunction“vicious cycle”
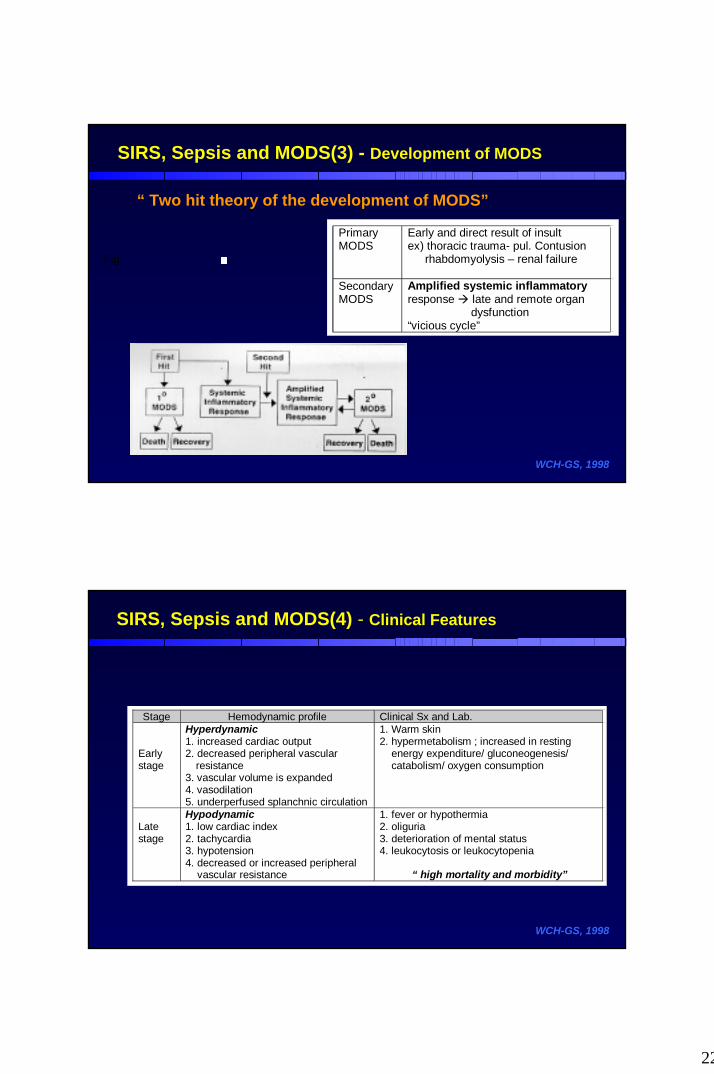
SIRS, Sepsis and MODS(4) - Clinical Features
WCH-GS, 1998
Stage Hemodynamic profile Clinical Sx and Lab.
Earlystage
Hyperdynamic1. increased cardiac output2. decreased peripheral vascular
resistance3. vascular volume is expanded4. vasodilation5. underperfused splanchnic circulation
1. Warm skin2. hypermetabolism ; increased in resting
energy expenditure/ gluconeogenesis/catabolism/ oxygen consumption
Latestage
Hypodynamic1. low cardiac index2. tachycardia3. hypotension4. decreased or increased peripheral
vascular resistance
1. fever or hypothermia2. oliguria3. deterioration of mental status4. leukocytosis or leukocytopenia
“ high mortality and morbidity”
23
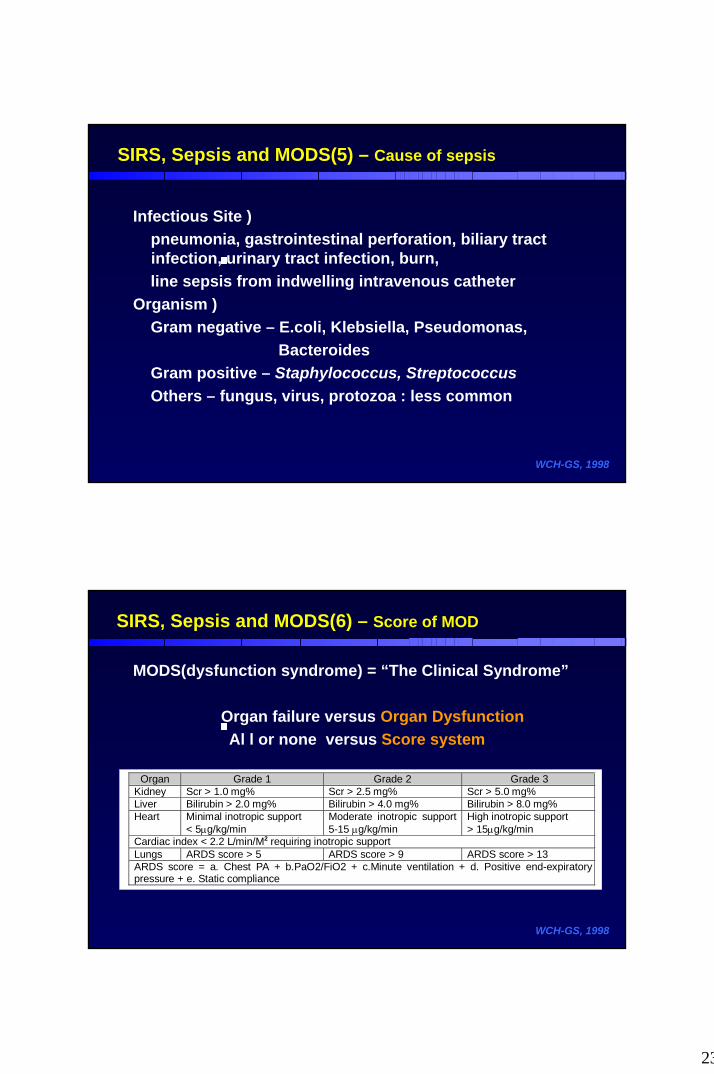
SIRS, Sepsis and MODS(5) – Cause of sepsis
Infectious Site )pneumonia, gastrointestinal perforation, biliary tract infection, urinary tract infection, burn, line sepsis from indwelling intravenous catheter
Organism ) Gram negative – E.coli, Klebsiella, Pseudomonas,
Bacteroides Gram positive – Staphylococcus, StreptococcusOthers – fungus, virus, protozoa : less common
WCH-GS, 1998
SIRS, Sepsis and MODS(6) – Score of MOD
MODS(dysfunction syndrome) = “The Clinical Syndrome”
Organ failure versus Organ DysfunctionAl l or none versus Score system
WCH-GS, 1998
Organ Grade 1 Grade 2 Grade 3Kidney Scr > 1.0 mg% Scr > 2.5 mg% Scr > 5.0 mg%Liver Bilirubin > 2.0 mg% Bilirubin > 4.0 mg% Bilirubin > 8.0 mg%Heart Minimal inotropic support
< 5µg/kg/minModerate inotropic support5-15 µg/kg/min
High inotropic support> 15µg/kg/min
Cardiac index < 2.2 L/min/M2 requiring inotropic supportLungs ARDS score > 5 ARDS score > 9 ARDS score > 13ARDS score = a. Chest PA + b.PaO2/FiO2 + c.Minute ventilation + d. Positive end-expiratorypressure + e. Static compliance
24
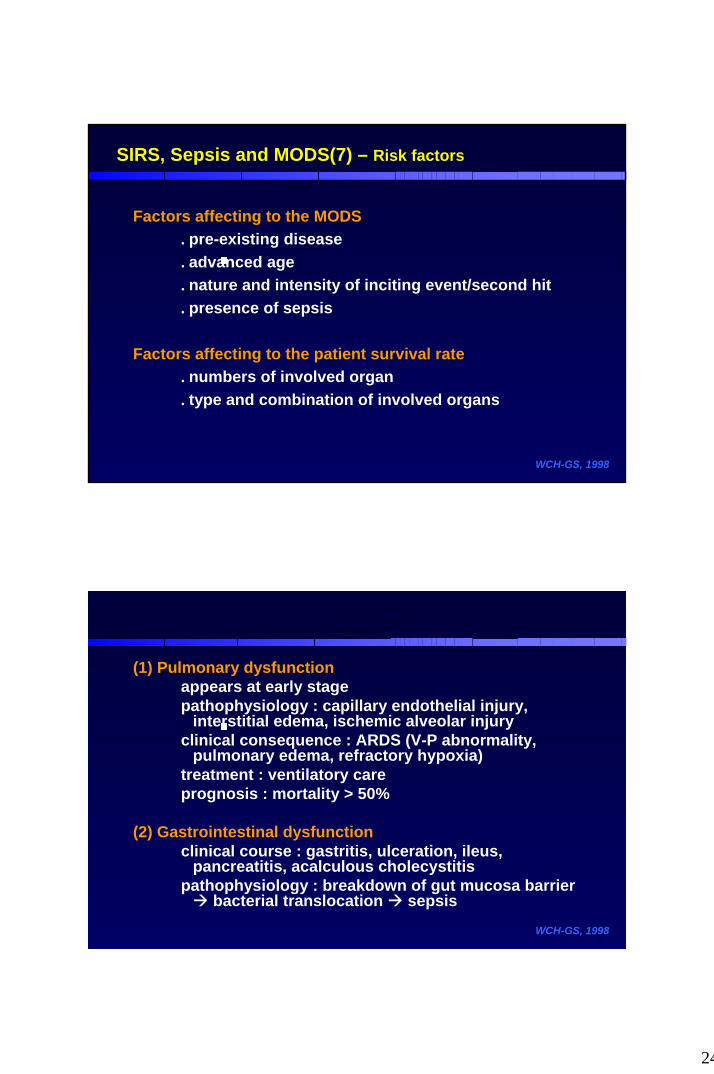
SIRS, Sepsis and MODS(7) – Risk factors
Factors affecting to the MODS. pre-existing disease . advanced age. nature and intensity of inciting event/second hit. presence of sepsis
Factors affecting to the patient survival rate. numbers of involved organ. type and combination of involved organs
WCH-GS, 1998
(1) Pulmonary dysfunctionappears at early stagepathophysiology : capillary endothelial injury,
interstitial edema, ischemic alveolar injuryclinical consequence : ARDS (V-P abnormality,
pulmonary edema, refractory hypoxia)treatment : ventilatory careprognosis : mortality > 50%
(2) Gastrointestinal dysfunctionclinical course : gastritis, ulceration, ileus,
pancreatitis, acalculous cholecystitispathophysiology : breakdown of gut mucosa barrier
bacterial translocation sepsis
WCH-GS, 1998
(1) Pulmonary dysfunction
appears at early stage
pathophysiology : capillary endothelial injury, interstitial edema, ischemic alveolar
injury
clinical consequence : ARDS (V-P abnormality, pulmonary edema, refractory hypoxia)
treatment : ventilatory care
prognosis : mortality > 50%
(2) Gastrointestinal dysfunctionclinical course : gastritis, ulceration, ileus, pancreatitis, acalculous cholecystitispathophysiology : breakdown of gut mucosa barrier bacterial translocation sepsis
SIRS, Sepsis and MODS(8) - MODS
25
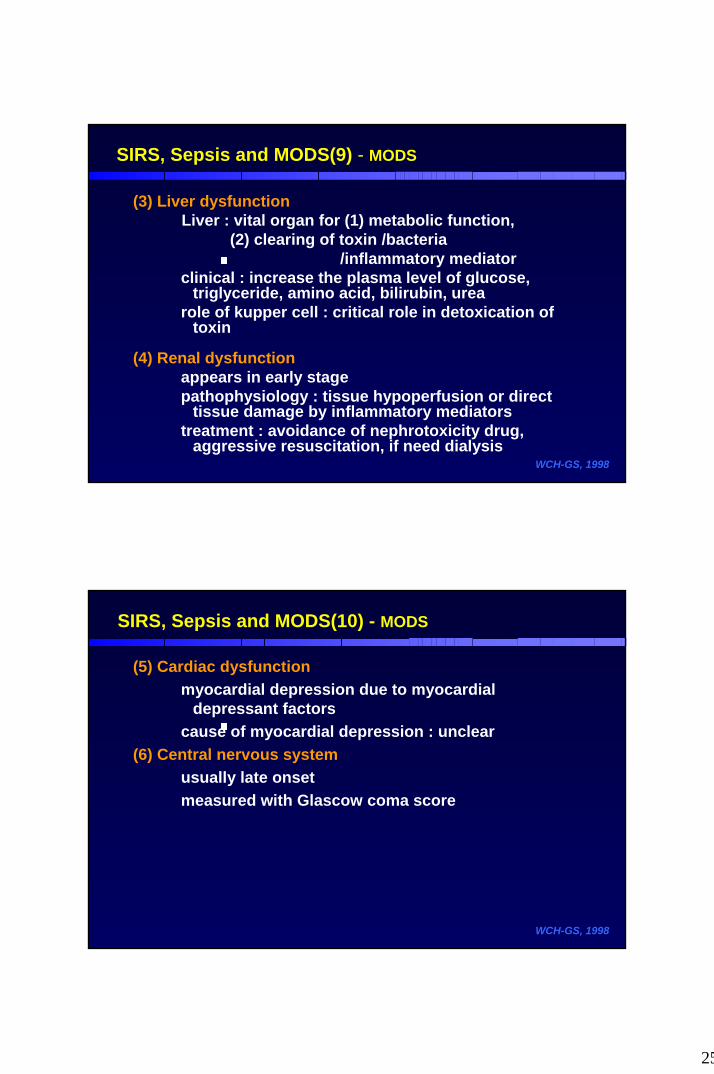
SIRS, Sepsis and MODS(9) - MODS
(3) Liver dysfunctionLiver : vital organ for (1) metabolic function,
(2) clearing of toxin /bacteria /inflammatory mediator
clinical : increase the plasma level of glucose, triglyceride, amino acid, bilirubin, urea
role of kupper cell : critical role in detoxication of toxin
(4) Renal dysfunctionappears in early stagepathophysiology : tissue hypoperfusion or direct
tissue damage by inflammatory mediatorstreatment : avoidance of nephrotoxicity drug,
aggressive resuscitation, if need dialysisWCH-GS, 1998
SIRS, Sepsis and MODS(10) - MODS
(5) Cardiac dysfunctionmyocardial depression due to myocardial
depressant factorscause of myocardial depression : unclear
(6) Central nervous systemusually late onsetmeasured with Glascow coma score
WCH-GS, 1998
26
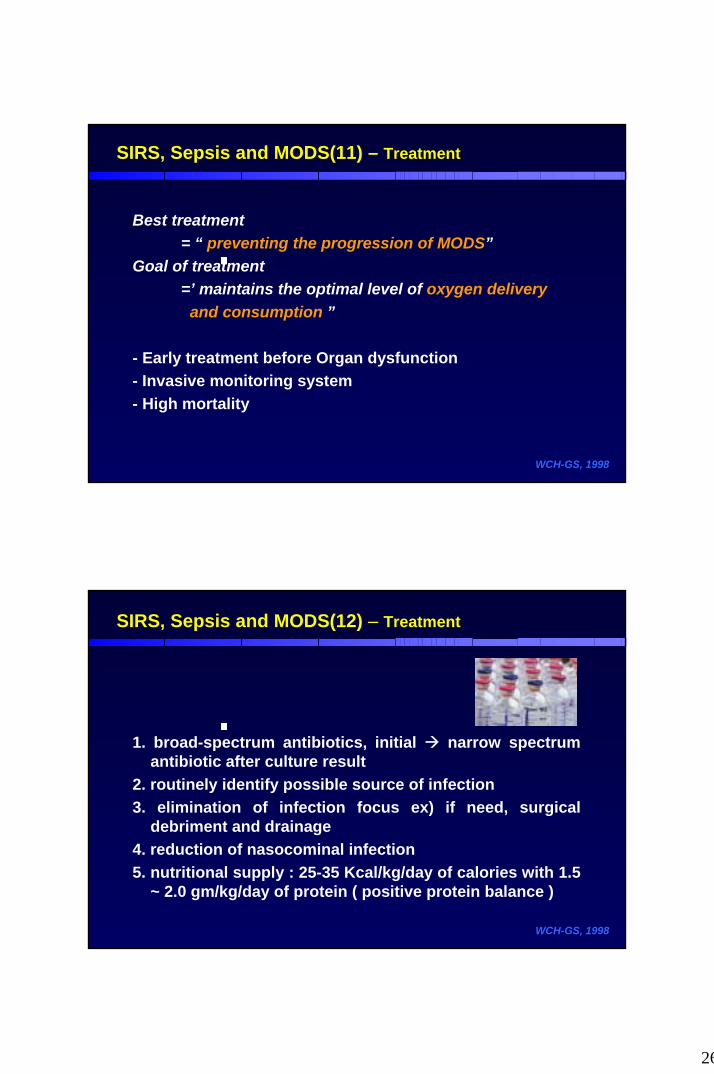
SIRS, Sepsis and MODS(11) – Treatment
Best treatment = “ preventing the progression of MODS”
Goal of treatment =’ maintains the optimal level of oxygen delivery and consumption ”
- Early treatment before Organ dysfunction - Invasive monitoring system - High mortality
WCH-GS, 1998
SIRS, Sepsis and MODS(12) – Treatment
1. broad-spectrum antibiotics, initial narrow spectrum antibiotic after culture result
2. routinely identify possible source of infection3. elimination of infection focus ex) if need, surgical
debriment and drainage4. reduction of nasocominal infection5. nutritional supply : 25-35 Kcal/kg/day of calories with 1.5
~ 2.0 gm/kg/day of protein ( positive protein balance )
WCH-GS, 1998
27
SIRS, Sepsis and MODS(13) – Treatment
Advanced pharmacologic approach : “mediator regulation”
corticosteroids NSAID(non-steroidal anti-inflammatory drug)various antioxidantsantiendotoxin antibody IL-1 receptor antagonistmonoclonal antibodies against tumor necrosis factorplatelet activating factor receptor antagonistmacrophage-specific immunomodulators
WCH-GS, 1998
Definition of shockPathophysiology of shock – hypoxia, anaerobic metabolism,
acidosis, circulation redistributionMediator of shock – Eicosanoids, cytokine, oxidantsGeneral principles of shock management – O2, Hb, COHypovolemic shock
- compensation mechanism- early management- monitoring of resuscitation
Traumatic shock, Cardiogenic shock, Neurologic shockSIRS, Sepsis, Septic shock, MODS
- definition- clinical progress and multiorgan failure- Treatment
Summary