Embed Size (px)
Citation preview

Myopia in Asian Subjects with Primary AngleClosureImplications for Glaucoma Trends in East Asia
Kai-Ling Yong, MBBS, MMed,1 Tianxia Gong, PhD,2 Monisha E. Nongpiur, MD,1,3 Alicia C. How, FRCS(Ed),1
Hwee Kuan Lee, PhD,2 Li Cheng, PhD,2 Shamira A. Perera, FRCOphth,1 Tin Aung, FRCS(Ed), PhD1,4
Purpose: To evaluate the occurrence of myopia in Asian subjects with angle closure and to assess the ocularbiometric parameters in these subjects.
Design: Cross-sectional study.Participants: We prospectively recruited 427 angle-closure subjects (143 primary angle-closure suspects,
75 patients with primary angle closure, 165 patients with primary angle-closure glaucoma, and 44 patients withacute primary angle closure) from a Singapore hospital.
Methods: Refractive status was derived from the spherical equivalent of autorefraction. A-scan biometry(Nidek Echoscan Ultrasound US-800; Nidek Co., Tokyo, Japan) was performed to obtain anterior chamber depth(ACD), axial length (AL), lens thickness, and vitreous cavity length (VL). Anterior segment optical coherencetomography was performed to measure lens vault.
Main Outcome Measures: Refractive status was categorized as myopia (��0.50 diopter [D]), emmetropia(�0.50 to þ0.50 D), and hyperopia (�þ0.50 D).
Results: The mean age � standard deviation of study subjects was 65.6�7.6 years, with most being Chinese(n ¼ 394; 92.3%) and women (n ¼ 275; 64.4%). Overall, myopia was present in 94 subjects (22%), hyperopia waspresent in 222 subjects (52%), and emmetropia was present in 111 subjects (26%). Of the 94 myopic angle-closure patients, 28 (29.8%) were categorized as having moderate myopia (��2.0 to �5.0D) and 11 (11.7%)were categorized as having high myopia (��5.00 D). Although myopic angle-closure subjects had longer ALs(P<0.001) and VLs (P ¼ 0.001) than their emmetropic and hyperopic counterparts, there were no significantdifferences in ACD (P ¼ 0.77), lens thickness (P ¼ 0.44), or lens vault (P ¼ 0.053).
Conclusions: Almost one quarter of angle-closure patients were myopic. Myopic angle-closure subjectshad longer VLs and ALs, but there was no difference in ACD. With the increasing rate of myopia in many EastAsian populations, there may be many subjects with axial myopia but shallow ACD and angle closure. Theimplication is that ophthalmologists should not assume that glaucoma patients who are myopic have openangles. Ophthalmology 2014;-:1e6 ª 2014 by the American Academy of Ophthalmology.
Established biometric risk factors for primary angle-closureglaucoma (PACG) include hyperopia, a short axial length(AL), shallow anterior chamber depth (ACD), and increasedlens thickness.1e5 Of these, a shallow ACD is considered acardinal risk factor for angle closure, and it is believed thathyperopic subjects have shorter ALs and shallower ACDs,which predispose them to having angle closure.6,7
Recent studies have described the presence of myopia inprimary angle-closure patients.8,9 Chakravarti and Spaeth8
reported that 6 (1.9%) of 322 angle-closure patients hadhigh myopia, whereas Barkana et al9 showed that only 9(0.05%) of 17 938 patients with high myopia (��6.0diopters [D]) had primary angle closure (PAC). However,these studies did not investigate the possible mechanism(s)for angle closure developing in such myopic patients.
With the increasing prevalence of myopia in Asia,10e12
one would expect a commensurate reduction in the preva-lence of PACG, because myopia is considered to be aprotective factor against PACG. However, in our practice,
� 2014 by the American Academy of OphthalmologyPublished by Elsevier Inc.
we have noted that there is a significant and increasingnumber of angle-closure patients with myopia. We hy-pothesize that although the mean AL and vitreous cavitylength (VL) are longer in myopic angle-closure patientscompared with those who are hyperopic, the ACD may besimilarly shallow.
The aim of this study was to evaluate the occurrence ofmyopia in Asian subjects with angle closure and to assessocular biometric parameters in these subjects. The biometricfeatures of the angle-closure patients with high myopia alsowere evaluated.
Methods
Our study recruited 427 angle-closure patients attending glaucomaclinics at the Singapore National Eye Centre. These included pa-tients categorized as primary angle-closure suspects (PACS), thosewith PAC, those with PACG, or those with previous acute primaryangle closure (APAC).13 Written informed consent was obtained
1ISSN 0161-6420/14/$ - see front matterhttp://dx.doi.org/10.1016/j.ophtha.2014.02.006

Table 1. Demographic Features of the Study Population
PrimaryAngle-Closure
Suspects(n [ 143)
PrimaryAngle-Closure(n [ 75)
PrimaryAngle-ClosureGlaucoma
Group (n [ 165)
PreviousAcute PrimaryAngle-Closure(n [ 44) P Value
Overall(n [ 427)
Subgroup proportion (%) 33.5 17.6 38.6 10.3 100Mean age (SD), yrs 63.1 (7.6) 66.0 (8.1) 68.4 (9.4) 62.2 (7.9) <0.001y 65.6 (8.8)EthnicityChinese 135 (94.4%) 66 (88.0%) 151 (91.5%) 42 (95.5%) 0.323 394 (92.3%)Non-Chinese* 8 (5.6%) 9 (12.0%) 14 (8.5%) 2 (4.5%) 33 (7.7%)
GenderMale 38 (26.6%) 28 (37.3%) 73 (44.2%) 13 (29.5%) 0.010z 152 (35.6%)Female 105 (73.4%) 47 (62.7%) 92 (55.8%) 31 (70.5%) 275 (64.4%)
APAC ¼ previous acute primary angle closure; PACG ¼ primary angle-closure glaucoma; PACS ¼ primary angle-closure suspects; SD ¼ standarddeviation.*Non-Chinese ethnicity includes Malays, Indians, Sikhs, Eurasians, Burmese, and Filipinos.ySignificant pairwise comparisons: P<0.001 for PACS vs. PACG, P<0.001 for PACG vs. APAC (1-way analysis of variance).zSignificant pairwise comparisons: P ¼ 0.002 for PACS vs. PACG (chi-square test).
Ophthalmology Volume -, Number -, Month 2014
from all subjects, and ethics approval was obtained from theinstitutional review board of the hospital. The study was carriedout in accordance with the tenets of World Medical Association’sDeclaration of Helsinki.
In brief, PACS was defined as an eye with narrow angles (inwhich the pigmented posterior trabecular meshwork was notvisible on gonioscopy for at least 180� in the primary position) andintraocular pressure (IOP) of 21 mmHg or less in the absence ofglaucomatous optic neuropathy or peripheral anterior synechiae.Primary angle closure was defined as the presence of narrow angleswith peripheral anterior synechiae, raised IOP of more than 21mmHg, or both, but without glaucomatous optic neuropathy. Pri-mary angle-closure glaucoma was defined as eyes with PACassociated with glaucomatous optic neuropathy (defined as loss ofneuroretinal rim with a vertical cup-to-disc ratio of >0.7 or anintereye asymmetry of 0.2, notching attributable to glaucoma, orboth). Previous APAC was defined if the subject had an episodewith the presence of at least 2 of the following symptoms: ocular orperiocular pain, nausea or vomiting, or both and an antecedenthistory of intermittent blurring of vision with haloes; a presentingIOP of more than 28 mmHg; and the presence of at least 3 of thefollowing signs: conjunctival injection, corneal epithelial edema,mid-dilated unreactive pupil, and shallow anterior chamber. Pa-tients with secondary glaucoma, such as neovascular and uveiticglaucoma, and patients with previous ocular surgeries or laser iri-doplasties were excluded. Laser peripheral iridotomy was per-formed previously for all subjects.
All subjects underwent a standardized eye examination thatincluded visual acuity measurement using a logarithm of minimumangle of resolution chart (Lighthouse, Inc, Long Island, New York),slit-lamp examination (Model BQ 900; Haag-Streit, Bern,Switzerland), stereoscopic optic disc examination with a 78-D lens(Volk Optical, Inc, Mentor, OH), automated refraction and kera-tometry (Canon RK 5 Auto Ref-Keratometer; Canon, Inc, Ltd,Tochigiken, Japan), and IOP measurement with Goldmann appla-nation tonometry (Haag-Streit, Koniz, Switzerland). Gonioscopywas performed in the dark using a Goldmann 2-mirror lens at highmagnification (�16). Indentation gonioscopy with a Sussman4-mirror lens (Ocular Instruments, Inc, Bellevue, WA) was used toestablish the presence or absence of peripheral anterior synechiae.
Refractive status was derived from the spherical equivalent ofthe subject’s average autorefraction. Refractive status was cate-gorized as myopia (��0.50 D), emmetropia (�0.50 to þ0.50 D),
2
and hyperopia (�þ0.50 D). Central ACD, AL, and lens thicknesswere measured by A-scan biometry (Nidek Echoscan UltrasoundUS-800; Nidek Co, Ltd, Tokyo, Japan). These results were used tocalculate vitreous cavity length (VL, calculated as: VL ¼ALeACDelens thickness) and relative lens position (calculatedas: [ACDþ0.5 lens thickness]/AL). Relative lens position wasanalyzed to rule out subclinical subluxated lens.
Anterior segment optical coherence tomography (Visante; CarlZeiss Meditec, Dublin, CA) imaging was performed under darkroom conditions (0 lux). Scans were centered on the pupil and wereobtained along the horizontal axis (nasaletemporal angles at 0� to180�) using the standard anterior segment single-scan protocol. Theimages were processed using customized software, the ZhongshanAngle Assessment Program (ZAAP, Guangzhou, China),14 by asingle observer (M.E.N.) who was masked to clinical data. Thelocations of the 2 scleral spurs were determined by the observerand the algorithm then automatically calculated the lens vault,defined as the perpendicular distance between the anterior pole ofthe crystalline lens and the horizontal line joining the 2 scleral spurs.
Statistical analysis was performed using R software (The RFoundation for Statistical Computing, Vienna, Austria). Differ-ences in mean values of parametric data among eyes of differentsubjects were examined using a 1-way analysis of variance. Thenull hypothesis was rejected at the 0.05 significance level. If thedifferences among the groups were significant, a pairwise t testwith Bonferroni adjustment was used to ascertain which pair ofgroups had a significant difference.
Results
We recruited 427 subjects, which included 143 PACS, 75 withPAC, 165 with PACG, and 44 with previous APAC. Most were ofChinese ethnicity (n ¼ 394; 92.3%), and there were more women(n ¼ 275; 64.4%). The subjects’ ages ranged from 41 to 93 years,and the mean age was 65.6 years (standard deviation [SD], 8.8years; Table 1).
The mean spherical equivalent of all subjects was þ0.65 D (SD,2.25 D). Approximately half (52%) of the subjects were hyperopic,with PACS having the highest percentage of hyperopia (70.6%;P<0.001). Overall, myopia was present in 94 (22%) of the sub-jects, with 28 (29.8%) of the myopic angle-closure patients beingcategorized as having moderate myopia (��2.0 to �5.0 D) and 11

Table 2. Refractive Status across Angle-Closure Groups
Refractive Status
PrimaryAngle-Closure
Suspects(n [ 143)
PrimaryAngle-Closure(n [ 75)
PrimaryAngle-ClosureGlaucoma(n [ 165)
PreviousAcute PrimaryAngle-Closure(n [ 44) P Value
Overall(n [ 427)
Mean spherical equivalent (SD), D þ1.65 (2.33) þ0.20 (1.88) þ0.13 (2.25) þ0.17 (1.42) <0.001* þ0.65 (2.25)Mean corneal curvature (SD), mm 7.65 (0.25) 7.64 (0.26) 7.64 (0.28) 7.56 (0.26) 0.24 7.74 (0.26)Hyperopia (�þ0.50 D)No. (%) 101 (70.6%) 29 (38.7%) 76 (46.1%) 16 (36.4%) 222 (52.0%)Mean (SD), D 2.72 (1.55) 1.89 (1.11) 1.76 (0.87) 1.57 (0.98) <0.001y 2.20 (1.34)
Emmetropia (þ0.50 to �0.50 D)No. (%) 26 (18.2%) 29 (38.7%) 43 (26.1%) 13 (29.6%) 111 (26.0%)Mean (SD), D 0.02 (0.13) 0.03 (0.19) 0.00 (0.19) 0.02 (0.16) 0.861 0.02 (0.17)
Myopia (��0.50 D)No. (%) 16 (11.2%) 17 (22.6%) 46 (27.9%) 15 (34.1%) 94 (22.0%)Mean (SD), D �2.52 (2.10) �2.38 (1.34) �2.44 (2.44) �1.20 (0.92) 0.202 �2.24 (2.06)
Low myopia (��0.5 to �2.0 D),no. (%)
8 (5.6) 7 (9.3) 29 (17.6) 11 (25.0) 55 (12.9)
Moderate myopia (��2.0 to �5.0 D),no. (%)
4 (2.8) 8 (10.7) 12 (7.3) 4 (9.1) 28 (6.5)
High myopia (��5.00 D), no. (ratio) 4 (2.8) 2 (2.7) 5 (3.0) 0 11 (2.6)
APAC ¼ previous acute primary angle closure; D ¼ diopters; PAC ¼ primary angle closure; PACG ¼ primary angle-closure glaucoma; PACS ¼ primaryangle-closure suspects; SD ¼ standard deviation.*Significance value pairwise comparison: P<0.001 for PACS vs. PAC, P<0.001 for PACS vs. PACG, and P<0.001 for PACS vs. APAC.ySignificance value pairwise comparison: P ¼ 0.012 for PACS vs. PAC, P<0.001 for PACS vs. PACG, and P ¼ 0.005 for PACS vs. APAC.
Yong et al � Myopia in Primary Angle Closure
(11.7%) categorized as having high myopia (��5.00 D). Emme-tropia was present in 111 (26%) angle-closure subjects. The meancorneal curvature was 7.74 mm (SD, 0.26 mm), and there was nosignificant difference in the corneal curvature between all the angleclosure subgroups (P ¼ 0.24; Table 2). On evaluating the cornealcurvature between the different myopic subgroups (low, moderate,and high myopia), there was no significant difference found, either(P ¼ 0.31).
Table 3 shows the biometric characteristics of the 11 highlymyopic patients with angle closure. The mean sphericalequivalent of these subjects was �6.72 D (SD, 2.29 D). Themean ACD was 2.73 mm (SD, 0.33 mm), and the mean AL was23.75 mm (SD, 2.02 mm). Eight (63.6%) of the 11 patients weremen. None of the patients had previous APAC. Patients 1, 3, 5,
Table 3. Summary of 11 Angle-Closure Patie
PatientNo. Age (yrs) Gender Diagnosis
SphericalEquivalent (D)
Anterior ChDepth (m
1 74 Male PACS �5.0 2.222 62 Male PACS �7.63 2.63 50 Female PACS �5.0 2.564 70 Female PACS �5.0 2.825 70 Female PAC �5.0 3.346 54 Male PACG �5.25 2.477 61 Female PACG �8.38 2.658 41 Male PACG �9.0 3.179 70 Male PAC �5.0 2.510 51 Male PACG �11.88 2.7211 72 Male PACG �6.8 3.0Mean 61.36 �6.72 2.73SD 10.97 2.29 0.33
D ¼ diopters; NA ¼ not available; PAC ¼ primary angle closure; PACG ¼ primstandard deviation.
6, 7, and 9 were asymptomatic patients who were referred to ourcenter by other doctors. Patients 2 and 4 had floaters, and patient5 had dry eyes. Patients 8, 10, and 11 had symptoms of blurringof vision on presentation. All these subjects were found to haveangle closure on gonioscopy. Patient 8 was a 41-year-old manwith axial myopia, a refractive error of �9.0 D, and an AL of 27.48mm. His ACD was relatively shallow at 3.17 mm, and his lensvault was 0.83 mm. Patient 10 was a 51-year-old man with myopiaof �11.88 D. He had a long AL (26.03 mm) and a shallow ACD(2.72 mm).
The differences in relative lens position among the variousdegrees of myopia were analyzed (Table 4). There were nostatistical differences in the relative lens position in the differentmyopic subgroups, nor between the angle-closure subtypes.
nts with High Myopia (��5.00 Diopters)
amberm)
Axial Length(mm)
Lens Thickness(mm)
VitreousLength (mm)
LensVault (mm)
21.33 4.94 14.17 0.7623.59 2.65 18.34 0.5322.5 2.99 16.95 0.2421.71 4.69 14.20 NA21.16 2.99 14.83 1.7924.96 4.9 17.59 0.9623.93 4.59 16.69 0.3927.48 5.09 19.22 0.8323.44 4.1 16.84 1.1826.03 4.26 19.05 0.5925.13 3.15 18.98 0.3723.75 4.03 16.99 0.762.02 0.91 1.89 0.46
ary angle-closure glaucoma; PACS ¼ primary angle-closure suspects; SD ¼
3

Table 4. Differences in Relative Lens Position between the Different Myopic Subgroups
Refractive Status
PrimaryAngle-Closure
Suspects(n [ 16)
PrimaryAngle-Closure(n [ 17)
PrimaryAngle-ClosureGlaucoma(n [ 46)
PreviousAcute PrimaryAngle-Closure(n [ 15) P Value
Overall(n [ 94)
Low myopia (��0.5 to �2.0 D)No. 8 7 29 11 55Mean RLP (SD) 0.21 (0.03) 0.21 (0.02) 0.21 (0.03) 0.21 (0.02) 0.93 0.21 (0.02)
Moderate myopia (��2.0 to �5.0 D)No. 4 8 12 4 28Mean RLP (SD) 0.20 (0.03) 0.19 (0.03) 0.21 (0.02) 0.20 (0.02) 0.38 0.20 (0.02)
High myopia (��5.00 D)No. 4 2 5 0 11Mean RLP (SD) 0.20 (0.03) 0.21 (0.02) 0.20 (0.01) d 0.75 0.20 (0.02)
P value 0.60 0.19 0.60 0.30 0.16
D ¼ diopters; RLP ¼ relative lens position; SD ¼ standard deviation.
Ophthalmology Volume -, Number -, Month 2014
Comparing the biometric parameters across different refractivestatus groups (Table 5), we found that myopic angle-closure eyeshad the highest ALs (mean � SD, 23.26�1.15 mm) and VLs(mean � SD, 16.39�1.47 mm) compared with emmetropic (P ¼0.009 for AL; P ¼ 0.019 for VL) and hyperopic (P<0.001 for AL;P ¼ 0.001 for VL) subjects. However, there was no statisticaldifference in the ACD, lens thickness, lens vault, or corneal cur-vature among myopic, emmetropic, or hyperopic angle-closurepatients.
Discussion
Our study showed that approximately one quarter of angleclosure patients have myopia. Interestingly, although the
Table 5. Refractive Status a
Myopia (n [ 94) Em
Mean spherical equivalent (SD), D �2.24 (2.06)Anterior chamber depth (mm)Mean (SD) 2.64 (0.30)Range 2.02e3.52
Lens thickness (mm)Mean (SD) 4.23 (0.95)Range 2.30e5.77
Axial length (mm)Mean (SD) 23.26 (1.15)Range 21.16e27.48
Vitreous length (mm)Mean (SD) 16.39 (1.47)Range 14.14e21.02
Lens vault (mm)Mean (SD) 0.91 (0.33)Range 0.24e1.79
Corneal curvature (mm)Mean (SD) 7.64 (0.28)Range 6.99e8.25
D ¼ diopters; SD ¼ standard deviation.*Significant pairwise comparison: P<0.001 for myopia vs. emmetropia, P<0.00ySignificant pairwise comparison: P ¼ 0.009 for myopia vs. emmetropia and P<zSignificant pairwise comparison: P ¼ 0.019 for myopia vs. emmetropia and P
4
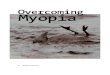
myopic subjects had longer AL and VL, the ACD was foundto be similar across groups (Fig 1). Of the 94 angle-closuresubjects who were myopic, 11 (11.7%) of them had highmyopia (��5.0 D), with the greatest proportion of highmyopes in the PAC group. Among all the angle-closuresubjects (n ¼ 427), 11 (2.6%) had high myopia, which isslightly higher than the 1.9% rate of high myopia reportedby Chakravarti et al,8 who found that of 322 PAC patients, 3subjects had high myopia (defined as ��5.0 D) and 3subjects had presumed high myopia with ALs of morethan 25 mm. Another study by Lowe et al1 also reportedthat 5.5% of patients (7 of 127 eyes) with PACG weremyopic, and only 1.6% of patients (2 eyes) had highmyopia defined as being �6.0 D or less. In a large study
nd Biometric Parameters
metropia (n [ 111) Hyperopia (n [ 222) P Value
0.02 (0.17) 2.20 (1.34) <0.001*
2.61 (0.35) 2.63 (0.29) 0.7721.98e3.41 2.02e3.50
4.35 (0.85) 4.21 (0.96) 0.4392.29e5.61 2.29e5.89
22.84 (1.05) 22.64 (0.90) <0.001y
20.77e28.61 20.95e26.81
15.88 (1.30) 15.80 (1.26) 0.001z
13.61e21.84 13.77e19.65
0.88 (0.26) 0.83 (0.27) 0.0530.24e1.54 �0.68 to 1.90
7.62 (0.27) 7.65 (0.26) 0.676.85e8.32 7.04e8.49
1 for myopia vs. hyperopia, and P<0.001 for emmetropia vs. hyperopia.0.001 for myopia vs. hyperopia.¼ 0.001 for myopia vs. hyperopia.

Figure 1. Diagram of an eye with myopic angle closure showing vitreous elongation and hence a longer axial length (AL) and vitreous length (VL) thanemmetropic and hyperopic eyes with angle closure. However, the anterior chamber depth (ACD) and lens thickness (LT) are similar.
Yong et al � Myopia in Primary Angle Closure
by Barkana et al9 conducted on a database of 17 938 personswith high myopia (��6.0 D), they found that 20 subjectshad angle closure, with only 9 of them having primarypupillary block. They attributed some of these patients’refractive statuses to lenticular myopia. However, none ofthese studies evaluated the relationship of refractive statuswith AL, ACD, or lens thickness.
Longer AL and myopia are regarded as protective factorsagainst angle closure.1,6 The prevalence of myopia (<�0.5D) in Singapore in those 40 years of age and older is estimatedto be 38.9% and that of high myopia (<�5.0 D) is estimatedto be 8.4%.15 With the increasing prevalence in myopia inAsia, one would expect Asians to have a declining risk ofangle closure. However, many epidemiologic studies haveshown that, although Chinese persons have a higherprevalence of myopia compared with Western populations,they also have a high prevalence of angle closure.2,16,17 Ofnote, we found that the angle-closure subjects with myopiahad significantly longer ALs than emmetropes or hyperopes,but there were no significant differences in corneal curvature,ACD, or lens thickness. This is in keeping with many studiesthat showed that myopia is induced by environmental factorsthat lead to elongation of the AL or VL, and hence result inaxial myopia.18,19 We thus deduce that these myopic patientswith angle closure are predominantly axial myopes with longVLs, but the characteristics of the anterior segment of theireyes are similar to those of hyperopes and emmetropes(shallow ACD). This suggests that the ACD is the importantrisk factor in the development of angle closure, regardless ofAL or refractive status.
On examining the 11 angle-closure patients with highmyopia, we noted that they were predominantly male(63.6%). Their ALs ranged from 21.16 to 27.48 mm, but alltheir ACDs were relatively shallow. Most of the patientsdid not have thick lenses. The underlying cause forangle closure to develop in these high myopes may be
multifactorial, but the configuration of the anterior segmentsomehow predisposes them to angle closure. More studiesmay be needed to evaluate other anterior segment featuressuch as ciliary body thickness, iris parameters, and anteriorchamber width and volume.
We evaluated the possibility of some of the myopic pa-tients having subclinical subluxed lenses by analyzing therelative lens position in different myopic subgroups. Nosignificant differences in the relative lens positions werenoted among both the myopic subgroups and the angle-closure subgroups. Interestingly, the lens vault, which is ameasurement of the amount of lens located anterior to theangles, also was not significantly different among themyopic, hyperopic, or emmetropic subjects.
Whereas it is generally believed that the occurrence ofmyopia in angle closure is rare, our findings suggestotherwise, with as much as 9.3% of angle-closure patientshaving moderate to high myopia. The ACD dimensions inangle closure were similar regardless of refractive status;hence, we can deduce that the mechanism of myopic angleclosure may be mediated through a crowded anteriorsegment. Therefore, it is important for clinicians to performgonioscopy in all patients suspected of having glaucoma,regardless of myopic refractive status.
The strengths of this study include the large sample sizeand that this study population encompassed the entirespectrum of PAC disease from PACS to PACG, includingprevious APAC. One of the limitations of our study was thatwe did not assess the cataract status of our patients, andhence did not take into account patients with lenticular orindex myopia. However, we did evaluate the lens thicknessof the patients, which did not show any statistical differ-ences in the different refractive subgroups. The AL wasexamined with A-scan ultrasonography, which is a contactmethod. It therefore can provide an artificially short AL ifperformed incorrectly by indenting the cornea. There is also
5

Ophthalmology Volume -, Number -, Month 2014
the possibility that in eyes with high myopia, there may be askewed AL reading brought about by the presence of aposterior staphyloma. Another limitation of our study wasthat cycloplegic refraction was not performed for our sub-jects. However, because our study population was older than40 years of age, it is likely that they do not have preservedaccommodative ability, and hence this is unlikely to affectthe results of our study.
In summary, we need to be aware that a significantproportion of angle-closure patients may have myopia witha long AL and VL, but have a relatively shallow ACD.Ophthalmologists should not assume that all glaucoma pa-tients who are myopic have open angles. Our findingsemphasize the importance of gonioscopy being performed inall glaucoma patients. Although there is an increasing rate ofmyopia in many East Asian populations, we speculate thatthe prevalence of PACG in the future may still be consid-erable, with many myopes having axial myopia but shallowACD.
References
1. Lowe RF. Aetiology of the anatomical basis for primary angle-closure glaucoma. Biometrical comparisons between normaleyes and eyes with primary angle-closure glaucoma. Br JOphthalmol 1970;54:161–9.
2. Bonomi L, Marchini G, Marraffa M, et al. Epidemiology ofangle-closure glaucoma: prevalence, clinical types, and asso-ciation with peripheral anterior chamber depth in the Egna-Neumarkt Glaucoma Study. Ophthalmology 2000;107:998–1003.
3. Lavanya R, Wong TY, Friedman DS, et al. Determinants ofangle closure in older Singaporeans. Arch Ophthalmol 2008;126:686–91.
4. Dandona L, Dandona R, Mandal P, et al. Angle-closureglaucoma in an urban population in southern India. TheAndhra Pradesh Eye Disease Study. Ophthalmology 2000;107:1710–6.
5. Thapa SS, Paudyal I, Khanal S, et al. Comparison of axiallengths in occludable angle and angle-closure glaucomadtheBhaktapur Glaucoma Study. Optom Vis Sci 2011;88:150–4.
6
6. Xu L, Cao WF, Wang YX, et al. Anterior chamber depth andchamber angle and their associations with ocular and generalparameters: the Beijing Eye Study. Am J Ophthalmol 2008;145:929–36.
7. Jonas JB, Nangia V, Gupta R, et al. Anterior chamber depthand its associations with ocular and general parameters inadults. Clin Experiment Ophthalmol 2012;40:550–6.
8. Chakravarti T, Spaeth GL. The prevalence of myopia in eyeswith angle closure. J Glaucoma 2007;16:642–3.
9. Barkana Y, Shihadeh W, Oliveira C, et al. Angle closure inhighly myopic eyes. Ophthalmology 2006;113:247–54.
10. Au Eong KG, Tay TH, Lim MK. Education and myopia in110,236 young Singaporean males. Singapore Med J 1993;34:489–92.
11. Lin LL, Shih YF, Tsai CB, et al. Epidemiologic study of ocularrefraction among schoolchildren in Taiwan in 1995. OptomVis Sci 1999;76:275–81.
12. Tan CS, Chan YH, Wong TY, et al. Prevalence and risk factorsfor refractive errors and elderly Asian population: theSingapore Longitudinal Aging Study (SLAS). Eye (Lond)2011;25:1294–301.
13. Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The defi-nition and classification of glaucoma in prevalence surveys. BrJ Ophthalmol 2002;86:238–42.
14. Console JW, Sakata LM, Aung T, et al. Quantitative analysisof anterior segment optical coherence tomography images: theZhongshan Angle Assessment Program. Br J Ophthalmol2008;92:1612–6.
15. Pan CW, Zheng YF, Anuar AR, et al. Prevalence of refractiveerrors in a multiethnic Asian population: the SingaporeEpidemiology of Eye Disease Study. Invest Ophthalmol VisSci 2013;54:2590–8.
16. Aung T, Nolan WP, Machin D, et al. Anterior chamber depthand the risk of primary angle closure in 2 East Asian pop-ulations. Arch Ophthalmol 2005;123:527–32.
17. Congdon NG, Youlin Q, Quigley H, et al. Biometry and pri-mary angle-closure glaucoma among Chinese, white, andblack populations. Ophthalmology 1997;104:1489–95.
18. Wong TY, Foster PJ, Johnson GJ, Seah SK. Education, so-cioeconomic status, and ocular dimensions in Chinese adults:the Tanjong Pagar Survey. Br J Ophthalmol 2002;86:963–8.
19. Hepsen IF, Evereklioglu C, Bayramlar H. The effect of readingand near-work on the development of myopia in emmetropicboys: a prospective, controlled, three-year follow-up study.Vision Res 2001;41:2511–20.
Footnotes and Financial Disclosures
Originally received: August 22, 2013.Final revision: February 7, 2014.Accepted: February 7, 2014.Available online: ---. Manuscript no. 2013-1418.1 Singapore National Eye Centre and Singapore Eye Research Institute,Singapore, Republic of Singapore.2 Bioinformatics Institute, A*STAR (Agency for Science, Technology andResearch), Singapore, Republic of Singapore.3 Duke-NUS Graduate Medical School, Singapore, Republic of Singapore.4 Yong Loo Lin School of Medicine, National University of Singapore,Singapore, Republic of Singapore.
Financial Disclosure(s):The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article.
Supported by the National Medical Research Council, the NationalResearch Foundation, and the Biomedical Research Council, Singapore,Republic of Singapore.
Abbreviations and Acronyms:ACD ¼ anterior chamber depth; AL ¼ axial length; APAC ¼ acute pri-mary angle closure; D ¼ diopter; IOP ¼ intraocular pressure;PAC ¼ primary angle closure; PACG ¼ primary angle-closure glaucoma;PACS ¼ primary angle-closure suspect; SD ¼ standard deviation;VL ¼ vitreous cavity length.
Correspondence:Tin Aung, FRCS(Ed), PhD, Singapore National Eye Centre, 11 ThirdHospital Avenue, Singapore 168751, Republic of Singapore. E-mail: [email protected].