Embed Size (px)
Citation preview

Myocardial Perfusion Grade After Late Infarct ArteryRecanalization Is Associated With Global and Regional Left
Ventricular Function at One YearAnalysis From the Total Occlusion Study of Canada-2
Terje K. Steigen, MD, PhD; Christopher E. Buller, MD; G.B. John Mancini, MD; Vinod Jorapur, MD;Warren J. Cantor, MD; James M. Rankin, MD; Boban Thomas, MD; John G. Webb, MD;
Shari S. Kronsberg, MS; Deborah J. Atchison, RN, PhD; Gervasio A. Lamas, MD;Judith S. Hochman, MD; Vladimír Dzavík, MD
Background—Whether myocardial perfusion grade (MPG) following late recanalization of infarct-related arteries (IRAs)predicts left ventricular (LV) function recovery beyond the acute phase of myocardial infarction (MI) is unknown.
Methods and Results—The Total Occlusion Study of Canada-2 enrolled stable patients with a persistently occluded IRAbeyond 24 hours and up to 28 days post-MI. We studied the relationship between the initial MPG and changes in LVfunction and volume as well as the change in MPG from immediate post-percutaneous coronary intervention (PCI) to1 year in 139 PCI patients with thrombolysis in myocardial infarction grade 3 epicardial flow post-PCI and with pairedvalues grouped into impaired or good MPG groups (MPG 0/1 or MPG 2/3). MPG 0/1 patients were more likely to havereceived thrombolytic therapy and to have a left anterior descending IRA. They had lower blood pressure and LV ejectionfraction (LVEF) and a higher heart rate and systolic sphericity index at baseline. Changes in the MPG 0/1 and MPG 2/3 groupsfrom baseline to 1 year were LVEF, 3.3�9.0% and 4.8�8.9% (P�0.42); LV end-systolic volume index (LVESVI),�1.1�9.2 and �4.7�12.3 mL/m2 (P�0.25); LV end-diastolic volume index (LVEDVI), 0.08�19.1 and �2.4�22.2 mL/m2
(P�0.67); and SDs/chord for infarct zone wall motion index (WMI), 0.38�0.70 and 0.84�1.11 (P�0.01). By covariate-adjusted analysis, post-PCI MPG 0/1 predicted lower WMI (P�0.001), lower LVEF (P�0.001), and higher LVESVI(P�0.01) but not LVEDVI at 1 year. Of the MPG 0/1 patients, 60% were MPG 2 or 3 at 1 year.
Conclusions—Preserved MPG is present in a high proportion of patients following late PCI of occluded IRAs post-MI. PoorMPG post-PCI frequently improves MPG over 1 year. MPG graded after IRA recanalization undertaken days to weeks postMI is associated with LV recovery, indicating that MPG determined in the subacute post-MI period remains a marker ofviability.
Clinical Trial Registration—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00025766.(Circ Cardiovasc Interv. 2010;3:00-00.)
Key Words: acute coronary syndrome � myocardial infarction � myocardial reperfusion � angioplasty� coronary artery disease
Timely recanalization and sustained patency of the infarct-related artery (IRA) are major determinants of left
ventricular (LV) function and survival after acute myocardialinfarction (MI). Patients with normal epicardial flow in theIRA (thrombolysis in myocardial infarction [TIMI] grade 3)but reduced tissue-level perfusion as quantified by TIMImyocardial perfusion grade (MPG) immediately following
acute reperfusion with fibrinolysis or primary or rescuepercutaneous coronary intervention (PCI)1 have longerischemic times, larger infarcts, worse global and regionalLV systolic function, and increased mortality.2,3 Theseobservations suggest that MPG marks microvascular integ-rity and is thereby a surrogate for myocardial viability inthe acute phase of MI.4 –7
Received October 28, 2009; accepted August 23, 2010.From the University of Tromsoe (T.K.S.), Tromsoe, Norway; Division of Cardiology (C.E.B., G.B.J.M.), Vancouver General Hospital, Vancouver,
British Columbia, Canada; Columbia University Division of Cardiology (V.J., G.A.L.), Mount Sinai Medical Center, Miami Beach, Fla; Division ofCardiology (W.J.C.), Southlake Regional Health Center, Newmarket, Ontario, Canada; Department of Cardiovascular Medicine (J.M.R.), Royal PerthHospital, Perth, Australia; Hospital Fernando Fonseca (B.T.), Lisbon, Portugal; St Paul’s Hospital (J.G.W.), Vancouver, British Columbia, Canada;Maryland Medical Research Institute (S.S.K.), Baltimore, Md; Peter Munk Cardiac Centre (D.J.A., V.D.), University Health Network, Toronto, Ontario,Canada; and Division of Cardiology (J.S.H.), New York University School of Medicine, New York, NY.
The online-only Data Supplement is available at http://circinterventions.ahajournals.org/cgi/content/full/CIRCINTERVENTIONS.109.918722/DC1.Correspondence to Vladimír Dzavík, MD, Interventional Cardiology Program, Peter Munk Cardiac Centre, University Health Network, Toronto,
Ontario, Canada. E-mail [email protected]© 2010 American Heart Association, Inc.
Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.109.918722
1
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

Clinical Perspective on p ●●●
In contrast to the extensively documented benefit of earlyrecanalization, routine late recanalization (beyond 24 hours)after symptom onset is not well supported by evidence8,9 and isnot guideline recommended. Until recently, late PCI for persis-tent occlusion generally has been performed on the basis of thelate open artery hypothesis.10 The extent to which effectivemicrovascular reperfusion can be achieved by PCI performedafter the acute phase and whether it is followed by regional orglobal functional recovery of the LV are unknown. The Oc-cluded Artery Trial (OAT)9 was a multicenter randomizedcontrolled trial that evaluated the benefit of PCI in addition tooptimal medical therapy compared with optimal medical therapyalone in patients beyond the first 24 hours and up to 28 days afterMI onset. The Total Occlusion Study of Canada-2 (TOSCA-2)was a National Heart, Lung, and Blood Institute-funded angio-graphic ancillary study of OAT with coprimary end points ofIRA patency at 1 year and change in LV ejection fraction (EF)from baseline to 1 year.8 Paired coronary and LV angiogramswere obtained at baseline and 1 year post-PCI (n�332), provid-ing a unique opportunity to evaluate the association betweenMPG at baseline (following successful PCI) and global andregional functional recovery at 1 year follow-up and to examinethe stability of perfusion grade over time.
MethodsStudy PopulationThe primary results of TOSCA-28 as well as the study design11 andresults9 of the parent OAT have been published. Inclusion criteria forTOSCA-2 and OAT included a documented index MI and anoccluded IRA (TIMI flow grade 0 or 1) in addition to 1 of 2 high-riskcriteria: (1) proximal occlusion or (2) LVEF �50%. Importantexclusion criteria included a clinical indication for revascularization(significant angina, severe inducible ischemia, left main or triple-vessel disease), serum creatinine �2.5 mg/dL, severe valvulardisease, New York Heart Association (NYHA) class III or IV heartfailure, or cardiogenic shock at the time of screening. Inclusioncriteria for the MPG analysis included OAT treatment assignment tothe PCI group with subsequent successful PCI of IRA with post-PCIantegrade TIMI 3 flow. Finally, baseline, post-PCI, and 1-yearfollow-up coronary angiograms suitable for MPG analysis andanalyzable LV angiograms were required.
Data CollectionBaseline characteristics were recorded from the time of index MI tothe time of randomization. Qualifying coronary and LV angiogramsperformed after the first 24 hours and up to 28 days post-MI as wellas post-PCI and follow-up angiograms performed after 1 year weresubmitted for quantitative analysis performed in a dedicated coreangiographic laboratory. LV volumes, LVEF, regional wall motion,and sphericity index were calculated as described previously.12–14
PCIProtocol PCI of the IRA with routine stenting was performed within24 hours of randomization. All patients received aspirin and eitherticlopidine or clopidogrel beginning the day of the procedure orearlier. Anticoagulation with heparin during PCI to a target activatedclotting time of �250 seconds was recommended. Use of glycopro-tein IIb/IIIa inhibitors was encouraged.
MPGThe MPG substudy was prospectively planned, and participatingcenters were instructed with respect to technique for obtaining
immediate post-PCI and 1-year follow-up angiograms optimized forMPG analysis, generally requiring a longer cine-angiographic re-cording focusing on the myocardial segment likely to demonstrateblush. MPG was graded semiquantitatively by 2 independent corelaboratory readers (V.J., T.S.) trained to use standard TIMI MPGcriteria1 and blinded to clinical data and timing and sequence ofangiography. In case of discrepancies, angiograms were re-readindependently by both readers, and any remaining discrepancieswere resolved by a third reader (G.B.J.M.). Post-PCI and follow-upangiograms also were evaluated for residual thrombus and evidenceof distal embolization. The present analysis was limited to patientswith post-PCI TIMI flow grade 3 because it is technically difficult tograde myocardial blush when the epicardial vessel is poorly opaci-fied and, moreover, abnormalities of MPG might no longer reflectmicrovascular function if flow were restricted proximally. We haverecently published a reproducibility study that included the TIMIMPG method in an angiographic core laboratory where we found ahigh degree of interobserver reproducibility when MPG was dichot-omized to 0 or 1 versus 2 or 3.15 Because of the relatively smallnumber of patients in the present study and the inherent difficultiesin MPG grading, we prospectively defined grouping of MPG to 0 or1 (MPG 0/1) versus 2 or 3 (MPG 2/3).
Statistical AnalysisCategorical variables are expressed as frequencies and percentages andcontinuous variables as mean�SDs. Categorical variables were com-pared using �2 test or, alternatively, Fisher exact test if expectedfrequency for any cell in a 2�2 table was �5. The Wilcoxon 2-sampletest was used to compare time intervals from index MI to baselineangiography, randomization, and PCI. Independent-sample t test wasused to compare other continuous variables that were normally distrib-uted. Within-group changes over time were compared using a paired ttest of the difference, and between-group differences were comparedwith 2-sample t tests. The prespecified level of significance for allsecondary analyses of OAT was P�0.01, whereas P�0.01 and �0.05were considered to indicate a trend toward statistical significance.
Effects of impaired post-PCI MPG (MPG 0/1) on 1-year LVEF, wallmotion index (WMI), LV end-systolic volume index (LVESVI), andLV end-diastolic volume index (LVEDVI) were examined in anunadjusted as well as a covariate-adjusted linear regression model. Allbaseline covariates that were tested for are listed in Table 1 of the mainOAT publication.9 Adjustments were made for other baseline covari-ates, with P�0.05 on multiple linear regression using backward elimi-nation. WMI was adjusted for baseline WMI, days to randomization,body mass index (BMI), and new Q waves. LVEF was adjusted forbaseline LVEF, heart rate, BMI, and new Q waves. LVESVI wasadjusted for baseline LVESVI, no family history, NYHA class �I atpresentation, and left anterior descending artery (LAD) as the IRA.
ResultsDistribution of MPGOf the 381 patients enrolled in TOSCA-2, 195 were assigned toPCI, and of these, 186 had angiograms potentially suitable forbaseline MPG analysis. The 9 angiograms that were excludedhad cine-angiographic recordings that were too short for analy-sis. The distribution of post-PCI TIMI flow grade in these 186patients was grade 0 in 12 (6.5%), grade 1 in 6 (3.2%), grade 2in 11 (5.9%), and grade 3 in 157 (84.4%). The distribution ofMPG, evaluated in all 157 patients with TIMI flow grade 3, wasMPG 0 in 25 (15.9%), MPG 1 in 8 (5.1%), MPG 2 in 77(49.0%), and MPG 3 in 47 (29.9%). Baseline clinical character-istics of the MPG 0/1 and MPG 2/3 groups are provided in Table1,and angiographic and procedural characteristics are providedin Table 2. Of these 157 evaluable patients, 142 also had MPGand global and regional LV functional parameters suitable foranalysis at 1-year follow-up. Paired analyses were available for139 patients (post-PCI and 1 year).
2 Circ Cardiovasc Interv December 2010
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

Univariate Correlates of Impaired MPG Post-PCIAt baseline, patients with MPG 0/1 had evidence of largerinfarcts, lower systolic blood pressure and LVEF, and a trend toa larger LVESVI and higher peak creatine kinase compared withpatients with MPG 2/3. They also were more likely to have anoccluded LAD and to have been treated with fibrinolytic therapyfor the index MI and less likely to have angiographically visiblecollaterals. Glycoprotein IIb/IIIa inhibitors were used in a
majority of cases, with no difference between groups (Tables 1and 2). These baseline findings are similar to those reported forthe larger cohort of 261 OAT ancillary study patients in whombaseline MPG was measured.16
Optimal Medical TreatmentBoth MPG groups had high rates of optimal medical therapyduring hospital stay, at discharge, and at 1-year follow-up,with no differences observed between the groups (Table 3).
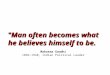
Changes in LV Size and Function Over 1 YearAs a group, patients with MPG 2/3 showed significant improve-ment at follow-up in measures of global contractility, includingLVEF and LVESVI. In contrast, those with MPG 0/1 showed noimprovement. The more demanding between-group comparisontesting for differential effects of post-PCI MPG on these LVparameters, however, was not significant (Figure A and B).Regional contractility of the infarct zone as expressed by thewall motion score improved in both MPG groups at follow-up,but the degree of wall motion improvement observed in theMPG 2/3 group was significantly greater than that observed inthe MPG 0/1 group (Figure D). No significant change or
Table 1. Baseline Clinical Characteristics by Post-PCI MPG
Characteristic
Post-PCIMPG 0/1(n�33)
Post-PCIMPG 2/3(n�124) P
Male sex, % 78.8 85.5 0.350
Age, y 54.6�9.2 57.4�10.5 0.174
BMI, kg/m2 28.6�4.5 27.6�4.1 0.21
Diabetes 24.2 16.9 0.336
Hypertension 48.5 50.8 0.813
Hyperlipidemia 48.5 58.9 0.285
Family history of CAD 42.4 48.4 0.542
Current-smoker 42.4 31.5 0.236
Prior angina 12.1 21.8 0.216
Prior MI 6.1 13.7 0.368
Interval from MI to baselineangiogram, d
5 (4, 8) 5 (3, 9) 0.566
Interval from MI torandomization, d
9 (5, 17) 10 (6, 20) 0.512
Interval from MI to PCI, d 10 (5, 18) 10 (7, 20) 0.507
Interval from baselineangiogram to PCI, d
3 (0, 9) 2 (0, 12) 0.939
Heart rate, beats/min 74.9�12.1 67.4�10.9 0.001
Systolic blood pressure,mm Hg
108.4�16.5 119.3�15.1 0.0004
Diastolic blood pressure,mm Hg
66.9�9.7 72.1�10.8 0.014
Fibrinolytic therapy duringfirst 24 h of index MI
45.4 16.9 �0.001
ST elevation �0.1 mV 72.7 59.8 0.175
ST depression �0.1 mV 36.4 30.3 0.508
New Q waves 63.4 65.3 0.860
Maximum pre-PCI total CKdivided by ULN
10.1�6.2* 7.1�7.3† 0.048
Maximum pre-PCI CK MBdivided by ULN
23.4�26.6 11.8�14.3 0.123
Maximum pre-PCI TNIdivided by ULN
172.4�152.0 271.4�713.6 0.253
Maximum pre-PCI TNTdivided by ULN
229.5�215.9 50.6�50.3 0.138
Killip class �1 duringindex MI
9.1 10.5 0.999
NYHA class �I atrandomization
9.1 6.4 0.700
Data are presented as mean�SD, median (interquartile range), or percent-age. CAD indicates coronary artery disease; CK, creatine kinase; TNI, troponinI; TNT, troponin T; ULN, upper limit of the local laboratory normal.
*n�27.†n�104.
Table 2. Angiographic and Procedural Characteristics byPost-PCI MPG
CharacteristicPost-PCI
MPG 0/1 (n�33)
Post-PCIMPG 2/3(n�124) P
Pre-PCI coronary angiography
LAD IRA 54.6 21.8 �0.001
Circumflex IRA 21.2 9.7
RCA IRA 24.2 68.5
IRA TIMI flow grade 0 to 1 100.0 98.4 1.000
Collaterals present 72.3 95.1 �0.001
Single-vessel disease 87.9 81.4 0.385
Pre-PCI LV angiography
Infarct segment regionalWMI SD/chord
�3.2�0.7 �2.9�1.0 0.177
LVEF 42.6�11.6 50.6�8.7 �0.001
LVESVI 39.8�20.1 31.3�14.3 0.08
LVEDVI 69.7�27.3 63.6�24.7 0.34
Diastolic sphericity index 31.0�5.3 30.8�6.4 0.862
Systolic sphericity index 25.3�6.1 22.9�5.5 0.035
Mitral regurgitation present 28.1 35.8 0.414
Procedural characteristics andpost-PCI angiography
Residual thrombus 9.1 2.4 0.108
Distal embolization 3.0 8.9 0.462
Post-PCI residual %diameter stenosis
29.8�17.6 27.8�14.3 0.507
Post-PCI minimalluminal diameter, mm
2.2�0.6 2.3�0.5 0.097
Glycoprotein IIb/IIIainhibitors used
90.9 83.1 0.27
Stent implanted 100.0 99.2 1.000
Data are presented as mean�SD or percentage. RCA indicates rightcoronary artery.
Steigen et al MPG and LV Function After Recanalization Over Time 3
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

difference was noted within or between MPG groups forLVEDVI (Figure C). We also observed a significantly lowersystolic sphericity index at 1 year in the MPG 2/3 (0.206) versusthe MPG 0/1 (0.240) group (P�0.008).
Changes in MPG Over 1 YearOf the 109 MPG 2/3 group patients, 18 (17%) had MPG 0 or 1at 1 year (Table 4). Binary restenosis in the IRA was observedin 16 (88.9%) of these patients and in 27 (29.7%) of 91 patientsin whom MPG remained 2 or 3 (P�0.0001). Mean diameterstenosis was 82.5�22.8% versus 43.9�20.4% (P�0.0001) in
these 2 groups. Of the post-PCI MPG 0/1 group, 60% had MPG2 or 3 at 1 year. Among the 30 MPG 0/1 group patients withangiographic follow-up, restenosis was observed in 9 (50%) ofthe 18 with MPG 2 or 3 at 1 year and 3 (25%) of 12 withpersistent MPG 0 or 1 (P�0.17).
Independent Correlates of LV Size and Functionat 1 Year (by Post-PCI MPG)On multivariable analysis (Table 5) post-PCI MPG 0/1predicted lower WMI (P�0.0002) and LVEF (P�0.0008)and a higher LVESVI (P�0.0056) at 1 year.
Figure. Comparison of baseline (post-PCI) and follow-up at 1 year of LVEF (A).LVESVI (B), LVEDVI (C), and targetregion wall motion (SD/chord) (D)between groups (MPG 0/1 versus MPG2/3) (paired data). Values are given forchange within group and P values forwithin-group and between-group com-parisons. ED indicates end diastolic; ES,end systolic.
Table 3. Use of Medical Therapies at Discharge and at 1 Year (by MPG)
Discharge 1-Year Follow-Up
MPG 0/1(n�30)
MPG 2/3(n�109) P
MPG 0/1(n�29)
MPG 2/3(n�106) P
Discharge
Aspirin 29 (96.7) 108 (99.1) 0.39 28 (96.6) 100 (94.3) 1.00
Thienopyridines (clopidogrel orticlopidine)*
30 (100.0) 108 (99.1) 1.00 9 (31.0) 29 (27.4) 0.70
Aspirin or thienopyridine 30 (100.0) 109 (100.0) NA 28 (96.6) 103 (97.2) 1.00
Aspirin plus thienopyridine 29 (96.7) 107 (98.2) 0.52 9 (31.0) 26 (24.5) 0.48
Warfarin 5 (16.7) 4 (3.7) 0.02 … … …
One or more of aspirin,warfarin, thienopyridine
30 (100.0) 109 (100.0) NA … … …
Two or more of aspirin,warfarin, thienopyridine
30 (100.0) 107 (98.2) 1.00 … … …
�-blocker 28 (93.3) 97 (89.0) 0.73 28 (96.6) 89 (84.0) 0.12
ACE inhibitor or ARB 29 (96.7) 94 (86.2) 0.19 28 (96.6) 92 (86.8) 0.19
Spironolactone 4 (13.3) 2 (1.8) 0.02 4 (13.8) 6 (5.7) 0.22
Lipid-lowering agent 28 (93.3) 92 (84.4) 0.37 28 (96.6) 93 (87.7) 0.30
Data are presented as no. (%). ACE indicates angiotensin-converting enzyme; ARB, angiotensin receptor blocking agent.*Only clopidogrel for 1-year follow-up.
4 Circ Cardiovasc Interv December 2010
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

DiscussionThis study addresses the ability of MPG to discriminate amongpatients with successful PCI of occluded infarct arteries andthose who will have favorable changes in LV function fromthose who will not. To our knowledge, this study is the first toaddress the association between MPG and global and regionalrecovery of LV function following late recanalization of the IRAafter MI and to describe MPG at 1-year follow-up.
The study population was uniformly selected and uniquelysuited to test MPG as a predictor of LV recovery post-MI.OAT-enrolled, stable patients with occluded IRAs underwentrecanalization with PCI/stent. We selected only patients withnormal epicardial flow immediately post-PCI after a medianocclusion time of 10 days. Notably, 79% of our cohortdemonstrated MPG 2 or 3. Extending the results of studiesexamining acute reperfusion cohorts, preserved MPG wassignificantly associated with better indices of LV systolicfunction at 1 year (Figure). We also observed that MPGimproved significantly from post-PCI to follow-up at 1 year.
Distribution of MPGOur results are consistent with a large study of early recan-alization by primary PCI with good epicardial and microvas-cular flow in 1190 (76.9%) of 1548 patients.17 In a recentpublication on thrombus aspiration in the setting of acute MI,75% to 82% of patients had myocardial blush grade 2 or 3.18
Both of these studies used myocardial blush grade,17 which,
although it uses somewhat different criteria, is angiographi-cally and conceptually similar to the MPG system used in thepresent study. The results are comparable to the 79% preva-lence following successful late recanalization after the first 24hours and up to 28 days post-MI in the present study.
Several factors may be responsible for the high rates ofpreserved MPG following late PCI in the present study. Weselected only patients with TIMI 3 flow post-PCI, as ex-plained in the Methods section. Stents were implanted innearly all (99.4%) patients, and angiographic evidence ofresidual thrombus and distal embolization was seen only in avery small number of patients. Finally, the myocardial edemaand microvascular plugging by aggregates of leukocytes andplatelets, typical of acute MI, may have begun to resolve inmany of our patients. Rochitte and colleagues19 showed thatthe extent of microvascular obstruction increases over thefirst 48 hours after experimental acute MI and reperfusion incanines. The same group reported that the peak extent ofmicrovascular obstruction occurs 2 days after reperfusion andis unchanged at 9 days.20 Using coronary Doppler ultrasound,Hozumi and coworkers,21 reported a short deceleration timeof diastolic flow velocity (DDT), a measure of microvascularresistance, 1 day after IRA recanalization, indicating poorrunoff in the microcirculation. Interestingly, they foundsignificantly longer DDT, indicating lower microvascularresistance, 1 and 2 weeks after acute IRA recanalization in agroup with viable myocardium and a group with nonviablemyocardium in the region of interest. In both groups, theDDT normalized by 2 weeks after recanalization. The authorspostulated that after the first 2 days following reperfusion,there is a gradual recanalization of the occluded microvessels,causing a progressive decrease in coronary resistance, even inareas without viable myocardium. In support of this hypoth-esis, we observed an increase in the number of patientsshowing MPG 2 or 3 at 1 year compared with post-PCI. Inlight of these data, it seems clear that poor blush can improve,indicating that it does not always imply irreversible necrosisof the microvasculature even if the subtended myocardium issubstantially infarcted. The change in MPG from good toworse is associated with severe restenosis in the IRA,suggesting that parts of the microcirculation in areas with scartissue may occlude spontaneously over time in the presenceof severe restenosis, even if the epicardial artery remainspatent with TIMI 3 flow. Alternatively, assessment of MPGin the presence of a severe upstream stenosis, particularly ina previously infarcted region, may be unreliable.
Functional Recovery in the Context ofTOSCA-2 ResultsIn TOSCA-2, significant improvement in LVEF was observed at1 year in both medically treated and PCI patients of about thesame magnitude as in the MPG 2/3 group in the present substudy(4.8�8.9%).8 The MPG 0/1 subgroup likely had more denselyinfarcted myocardium and microvascular derangement as evi-denced by the significantly lower LVEF and larger volumes justa few days post-MI. As already stated, however, it does notappear that, if poor myocardial perfusion represents a largerinfarct and microvascular derangement, this derangement isentirely irreversible. In addition, improvement in LVEF ap-
Table 4. Changes in MPG Over 1 Year
Post-PCI MPG
1-Year MPG
TotalMPG 0/1 MPG 2/3
MPG 0/1 12 (40) 18 (60) 30 (22)
MPG 2/3 18 (17) 91 (83) 109 (78)
Total 30 (22) 109 (78) 139 (100)
Data are presented as no. (%). P�0.006 for changes.
Table 5. Effects of Post-PCI MPG 0/1 Versus Post-PCI MPG2/3 on LV Outcome Measures at 1 Year
VariableParameterEstimate SEM T P
Unadjusted
Infarct segment regionalWMI (n�118)
�0.67 0.23 �2.90 0.0045
LVEF (n�126) �8.86 1.92 �4.60 �0.0001
LVESVI (n�76) 7.23 3.14 2.30 0.023
LVEDVI (n�76) 4.66 5.34 0.87 0.39
Covariate adjusted
Infarct segment regionalWMI
�0.71 0.18 �3.89 0.0002
LVEF �5.75 1.67 �3.43 0.0008
LVESVI 7.16 2.50 2.86 0.0056
LVEDVI 4.49 4.81 0.93 0.35
WMI adjusted for baseline WMI, days to randomization, BMI, and new Qwaves. LVEF adjusted for baseline EF %, heart rate, BMI, and new Q waves.LVESVI adjusted for baseline LVESVI, no family history, NYHA class �I, and LADculprit. LVEDVI adjusted for baseline LVEDVI, baseline LVEF, and LAD culprit.
Steigen et al MPG and LV Function After Recanalization Over Time 5
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

peared to be attenuated in the MPG 0/1 subgroup but was notsignificantly different from the MPG 2/3 subgroup, and thetarget regional wall motion score significantly increased in theMPG 0/1 subgroup, which means that there is some viabilityretained, even with poor blush immediately post-PCI.
Rather, early poor perfusion may represent a larger extentof injury causing microvascular dysfunction and early ven-tricular dilation that has potential for recovery over time. Thisnotion is further supported by the OAT nuclear ancillarystudy22 in which improvement in LVEF over 1 year waspredicted by baseline infarct zone viability.
Infarct Size and MPGPatients with baseline clinical and angiographic features oflarger infarct size subsequently exhibited impaired MPG follow-ing PCI in agreement with previous studies, suggesting thatinfarct size is closely related to microvascular obstructiondespite restoration of epicardial patency.23,24 Infarct size wasshown to be a major determinant of reflow following release ofcoronary occlusion in an experimental model of coronary occlu-sion and recanalization.24 We found fewer collaterals, signifi-cantly more LAD occlusions, and a greater likelihood of unsuc-cessful fibrinolytic therapy in the MPG 0/1 group. Thesefindings are similar to those reported for the larger cohort of 261OAT ancillary study patients in whom baseline MPG wasmeasured16 and in correspondence with data published byKandzari et al25 from a study of primary percutaneous revascu-larization in acute MI, showing that anterior infarction isassociated with greater impairment of LVEF, less frequentcollateral flow, and diminished reperfusion success as measuredby MPG.
We reported in our previous publication16 that failed fibrino-lytic therapy was significantly associated with impaired MPGfollowing late recanalization of occluded IRAs by PCI. Theassociation was no longer significant when adjusted for multiplevariables that correlate with infarct size, suggesting that impairedpost-PCI MPG in patients with failed fibrinolytic therapy ismainly related to larger infarct size, and we may speculate thatfibrinolytic therapy is preferentially administered to more criti-cally ill patients. Thus, the higher frequency of impaired MPG inpatients with LAD occlusion may be related to larger infarcts inthese patients. Absence of collaterals, noted more often withLAD occlusion, may have further contributed to higher fre-quency of impaired MPG in this subset.
LimitationsMyocardial perfusion as assessed by contrast angiography issemiquantitative and might be considered a difficult parameterto adjudicate. However, we have recently published a reproduc-ibility study that included the TIMI MPG method in an angio-graphic core laboratory.15 We found a high degree of interob-server reproducibility when MPG was dichotomized to 0 or 1versus 2 or 3; thus, we prospectively defined the grouping asMPG 0/1 versus MPG 2/3. The study population in TOSCA-2was relevant to examining the benefit of routine late PCIcompared with medical therapy alone in patients with occludedIRAs post-MI, and the results cannot be extrapolated to allpatients undergoing late PCI after MI. We analyzed MPG onlyin the subset of this population with antegrade TIMI 3 flow after
late IRA recanalization. Follow-up coronary angiography mayreflect ascertainment bias, with sicker patients not returning.Therefore, it is unknown whether the reported findings in asubset of patients extend to the entire cohort.
ConclusionsPreserved MPG is present in the majority of patients with MIwith normal epicardial flow following late PCI recanalization oftheir occluded IRA. Impaired baseline MPG is associated withunfavorable LV indices, whereas preserved baseline MPG in ourcohort is associated with segmental and global LV recovery.This observation extends prior analyses undertaken in acute MIsettings and is consistent with favorable MPG marking retainedviability within the infarct zone. Finally, patients with poorbaseline MPG frequently show MPG improvement and signifi-cantly, but modestly improved wall motion over 1 year and,thus, a relative lack of LV functional improvement. These datasuggest that microvascular integrity and myocardial viability canbe disengaged from each other in the chronic post-MI phase andwarrant further study.
AcknowledgmentsWe thank the investigators and the staff at the study sites for theirimportant contributions and Eunice Yeoh for her excellent work in theangiography core laboratory. We also thank Dr Harmony R. Reynoldsfor her editorial input on the manuscript and Zubin Dastur and EmilyLevy for their assistance in the preparation of the manuscript.
Sources of FundingThe project described was supported by award numbersU01HL062509, U01HL062511, R01 HL72906, and R01 HL75456from the National Heart, Lung, and Blood Institute. The content issolely the responsibility of the authors and does not necessarilyrepresent the official views of the National Heart, Lung, and BloodInstitute or the National Institutes of Health.
DisclosuresDr Buller received consultation/advisory board honoraria fromAbbott Vascular. Dr Hochman received grant support to her institu-tion from Eli Lilly and Bristol Myers Squibb Medical Imaging;product donations from Millennium Pharmaceuticals, Schering-Plough, Guidant, and Merck for OAT; consultation fees from BristolMyers Squibb; honoraria for steering committee service from EliLilly and GlaxoSmithKline; and honoraria for serving on the datasafety monitoring board of a trial supported by Schering-Plough. DrDzavík received research, honorarium, and advisory board memberfunds from Cordis and Johnson & Johnson; advisory board memberfunds from Abbott Vascular; and honoraria from Boston Scientific.
References1. Buller CE, Welsh RC, Westerhout CM, Webb JG, O’Neill B, Gallo R,
Armstrong PW. Guideline adjudicated fibrinolytic failure: incidence,findings, and management in a contemporary clinical trial. Am Heart J.2008;155:121–127.
2. Gibson CM, Cannon CP, Murphy SA, Ryan KA, Mesley R, Marble SJ,McCabe CH, Van De Werf F, Braunwald E. Relationship of TIMImyocardial perfusion grade to mortality after administration ofthrombolytic drugs. Circulation. 2000;101:125–130.
3. van ’t Hof AW, Liem A, Suryapranata H, Hoorntje JC, de Boer MJ,Zijlstra F; Zwolle Myocardial Infarction Study Group. Angiographicassessment of myocardial reperfusion in patients treated with primaryangioplasty for acute myocardial infarction: myocardial blush grade.Circulation. 1998;97:2302–2306.
4. De Luca G, van ’t Hof AW, de Boer MJ, Ottervanger JP, Hoorntje JC,Gosselink AT, Dambrink JH, Zijlstra F, Suryapranata H. Time-to-treatment significantly affects the extent of ST-segment resolution and
6 Circ Cardiovasc Interv December 2010
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

myocardial blush in patients with acute myocardial infarction treated byprimary angioplasty. Eur Heart J. 2004;25:1009–1013.
5. Gibson CM, Murphy SA, Kirtane AJ, Giugliano RP, Cannon CP, AntmanEM, Braunwald E. Association of duration of symptoms at presentationwith angiographic and clinical outcomes after fibrinolytic therapy inpatients with ST-segment elevation myocardial infarction. J Am CollCardiol. 2004;44:980–987.
6. Henriques JP, Zijlstra F, Ottervanger JP, de Boer MJ, van ’t Hof AW,Hoorntje JC, Suryapranata H. Incidence and clinical significance of distalembolization during primary angioplasty for acute myocardial infarction.Eur Heart J. 2002;23:1112–1117.
7. Kotani J, Mintz GS, Pregowski J, Kalinczuk L, Pichard AD, Satler LF,Suddath WO, Waksman R, Weissman NJ. Volumetric intravascularultrasound evidence that distal embolization during acute infarct inter-vention contributes to inadequate myocardial perfusion grade. Am JCardiol. 2003;92:728–732.
8. Dzavik V, Buller CE, Lamas GA, Rankin JM, Mancini GB, Cantor WJ,Carere RJ, Ross JR, Atchison D, Forman S, Thomas B, Buszman P, VozziC, Glanz A, Cohen EA, Meciar P, Devlin G, Mascette A, Sopko G,Knatterud GL, Hochman JS. Randomized trial of percutaneous coronaryintervention for subacute infarct-related coronary artery occlusion toachieve long-term patency and improve ventricular function: the TotalOcclusion Study of Canada (TOSCA)-2 trial. Circulation. 2006;114:2449–2457.
9. Hochman JS, Lamas GA, Buller CE, Dzavik V, Reynolds HR, AbramskySJ, Forman S, Ruzyllo W, Maggioni AP, White H, Sadowski Z, CarvalhoAC, Rankin JM, Renkin JP, Steg PG, Mascette AM, Sopko G, PfistererME, Leor J, Fridrich V, Mark DB, Knatterud GL. Coronary interventionfor persistent occlusion after myocardial infarction. N Engl J Med. 2006;355:2395–2407.
10. Hochman JS, Choo H. Limitation of myocardial infarct expansion byreperfusion independent of myocardial salvage. Circulation. 1987;75:299–306.
11. Hochman JS, Lamas GA, Knatterud GL, Buller CE, Dzavik V, Mark DB,Reynolds HR, White HD. Design and methodology of the OccludedArtery Trial (OAT). Am Heart J. 2005;150:627–642.
12. Lamas GA, Vaughan DE, Parisi AF, Pfeffer MA. Effects of left ventric-ular shape and captopril therapy on exercise capacity after anterior wallacute myocardial infarction. Am J Cardiol. 1989;63:1167–1173.
13. Sandler H, Dodge HT. The use of single plane angiocardiograms for thecalculation of left ventricular volume in man. Am Heart J. 1968;75:325–334.
14. Sheehan FH, Bolson EL, Dodge HT, Mathey DG, Schofer J, Woo HW.Advantages and applications of the centerline method for characterizingregional ventricular function. Circulation. 1986;74:293–305.
15. Steigen TK, Claudio C, Abbott D, Schulzer M, Burton J, Tymchak W,Buller CE, John Mancini GB. Angiographic core laboratory reproduc-ibility analyses: implications for planning clinical trials using coronaryangiography and left ventriculography end-points. Int J CardiovascImaging. 2008;24:453–462.
16. Jorapur V, Steigen TK, Buller CE, Dzavik V, Webb JG, Strauss BH,Yeoh EE, Kurray P, Sokalski L, Machado MC, Kronsberg SS, Lamas
GA, Hochman JS, Mancini GB. Distribution and determinants of myo-cardial perfusion grade following late mechanical recanalization ofoccluded infarct-related arteries postmyocardial infarction: A report fromthe occluded artery trial. Catheter Cardiovasc Interv. 2008;72:783–789.
17. De Luca G, van ’t Hof AW, Ottervanger JP, Hoorntje JC, Gosselink AT,Dambrink JH, Zijlstra F, de Boer MJ, Suryapranata H. Unsuccessfulreperfusion in patients with ST-segment elevation myocardial infarctiontreated by primary angioplasty. Am Heart J. 2005;150:557–562.
18. Svilaas T, Vlaar PJ, van der Horst IC, Diercks GF, de Smet BJ, van denHeuvel AF, Anthonio RL, Jessurun GA, Tan ES, Suurmeijer AJ, ZijlstraF. Thrombus aspiration during primary percutaneous coronary inter-vention. N Engl J Med. 2008;358:557–567.
19. Rochitte CE, Lima JA, Bluemke DA, Reeder SB, McVeigh ER, Furuta T,Becker LC, Melin JA. Magnitude and time course of microvascularobstruction and tissue injury after acute myocardial infarction. Circulation.1998;98:1006–1014.
20. Wu KC, Kim RJ, Bluemke DA, Rochitte CE, Zerhouni EA, Becker LC,Lima JA. Quantification and time course of microvascular obstruction bycontrast-enhanced echocardiography and magnetic resonance imagingfollowing acute myocardial infarction and reperfusion. J Am CollCardiol. 1998;32:1756–1764.
21. Hozumi T, Kanzaki Y, Ueda Y, Yamamuro A, Takagi T, Akasaka T,Homma S, Yoshida K, Yoshikawa J. Coronary flow velocity analysisduring short term follow up after coronary reperfusion: use of transtho-racic Doppler echocardiography to predict regional wall motion recoveryin patients with acute myocardial infarction. Heart. 2003;89:1163–1168.
22. Kloner RA, Rude RE, Carlson N, Maroko PR, DeBoer LW, Braunwald E.Ultrastructural evidence of microvascular damage and myocardial cellinjury after coronary artery occlusion: which comes first? Circulation.1980;62:945–952.
23. Udelson JE, Pearte CA, Kimmelstiel CD, Kruk M, Teresinska A,Bychowiec B, Marin-Neto JA, Hochtl T, Cohen EA, Caramori P, Busz-Papiez B, Adlbrecht C, Sadowski ZP, Ruzyllo W, Forman SA, Kinan DJ,Lamas GA, Hochman JS. The Occluded Artery Trial (OAT) ViabilityAncillary Study (OAT-NUC): influence of infarct zone viability on leftventricular remodeling after PCI vs medical therapy alone. Circulation.2007;116:II624–II625.
24. Reffelmann T, Hale SL, Li G, Kloner RA. Relationship between noreflow and infarct size as influenced by the duration of ischemia andreperfusion. Am J Physiol Heart Circ Physiol. 2002;282:H766–H772.
25. Tarantini G, Cacciavillani L, Corbetti F, Ramondo A, Marra MP, Bac-chiega E, Napodano M, Bilato C, Razzolini R, Iliceto S. Duration ofischemia is a major determinant of transmurality and severe micro-vascular obstruction after primary angioplasty: a study performed withcontrast-enhanced magnetic resonance. J Am Coll Cardiol. 2005;46:1229–1235.
26. Kandzari DE, Tcheng JE, Gersh BJ, Cox DA, Stuckey T, Turco M,Mehran R, Garcia E, Zimetbaum P, McGlaughlin MG, Lansky AJ, Con-stantini C, Grines CL, Stone GW; CADILLAC Investigators. Rela-tionship between infarct artery location, epicardial flow, and myocardialperfusion after primary percutaneous revascularization in acute myo-cardial infarction. Am Heart J. 2006;151:1288–1295.
CLINICAL PERSPECTIVEThe extent to which effective microvascular perfusion can be achieved by percutaneous coronary intervention (PCI)performed after the acute phase of a myocardial infarction (MI) and whether the magnitude of microvascular perfusionaffects left ventricular (LV) recovery is unknown. The Total Occlusion Study of Canada-2, an ancillary study of the2166-patient Occluded Artery Trial, enrolled 381 stable patients with a persistently occluded infarct-related artery (IRA)days to weeks post-MI to PCI or medical therapy alone. Change in myocardial perfusion grade (MPG) was determinedfrom immediate post-PCI to 1 year follow-up (157 patients), and the relationship between initial MPG and LV functionand volume was assessed in 139 patients. Preserved MPG was present in the majority of patients with normal epicardialflow following late PCI recanalization of the IRA. Impaired baseline MPG was associated with unfavorable LV indices,whereas preserved baseline MPG was associated with segmental and global LV recovery. Patients with poor baseline MPGfrequently showed MPG improvement and significantly, but only modestly improved wall motion over 1 year. Thus,microvascular integrity and myocardial viability can be disengaged from each other in the chronic post-MI phase, butsubgroups of stable patients with areas of viable myocardium might benefit from late recanalization. Preserved MPGimmediately post-PCI may be associated with LV recovery.
Steigen et al MPG and LV Function After Recanalization Over Time 7
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

Gervasio A. Lamas, Judith S. Hochman and Vladimír DzavíkJames M. Rankin, Boban Thomas, John G. Webb, Shari S. Kronsberg, Deborah J. Atchison,
Terje K. Steigen, Christopher E. Buller, G.B. John Mancini, Vinod Jorapur, Warren J. Cantor,Occlusion Study of Canada-2
Global and Regional Left Ventricular Function at One Year: Analysis From the Total Myocardial Perfusion Grade After Late Infarct Artery Recanalization Is Associated With
Print ISSN: 1941-7640. Online ISSN: 1941-7632 Copyright © 2010 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleCirculation: Cardiovascular Interventions
published online November 9, 2010;Circ Cardiovasc Interv.
http://circinterventions.ahajournals.org/content/early/2010/11/09/CIRCINTERVENTIONS.109.918722World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circinterventions.ahajournals.org/content/suppl/2010/12/15/CIRCINTERVENTIONS.109.918722.DC1Data Supplement (unedited) at:
http://circinterventions.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Interventions Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Answer
Permissions and Rights Question andunder Services. Further information about this process is available in thepermission is being requested is located, click Request Permissions in the middle column of the Web pageClearance Center, not the Editorial Office. Once the online version of the published article for which
can be obtained via RightsLink, a service of the CopyrightCirculation: Cardiovascular Interventionsin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 15, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

Supplemental Material
OAT Follow up BLUSH – Results of Multiple Regression Model Outcome = 1 Year Ejection Fraction
Table 1 – compares ejection fraction with 32 baseline covariates that were analyzed in the main OAT publication. Those with p-values <= 0.20 are in bold. Covariates listed in the main OAT publication that are linear combinations of other covariates were excluded.
Table 2 – linear regression model showing the effect of post PCI MPG on the ejection fraction outcome adjusting for the significant covariates in Table 1. Table 3 – compares the ejection fraction outcome with the baseline covariates which were significant univariately (p <= 0.20). Those that are significant in this multiple regression model are in bold.. Table 4 – linear regression model showing the effect of post PCI MPG on the ejection fraction outcome adjusting for the significant covariates in Table 3. The differences between tables 1 and 3 are that age, bmi, cerebrovascular, and pvd are significant in table 1 and new q and rloss are significant in table 3. In all models, post PCI MPG is significantly related to 1 year ejection fraction adjusting for significant covariates.

Table 1. 1 Year EF Outcome – Relationship with 37 Covariates
Number of Observations Read 126
Number of Observations Used 126
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 34 6982.84365 205.37775 3.72 <.0001
Error 91 5025.95794 55.23031
Corrected Total 125 12009
Root MSE 7.43171 R-Square 0.5815
Dependent Mean 53.81746 Adj R-Sq 0.4251
Coeff Var 13.80910
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 46.79850 12.82082 3.65 0.0004
EFall ef(Core or Site) 1 0.37869 0.09769 3.88 0.0002
mpg2cat MPG 0/1 1 -5.07763 1.97080 -2.58 0.0116
age10 age/10(years) 1 -1.71634 0.89532 -1.92 0.0584
hr10 heart rate/10(bpm) 1 -1.30292 0.73422 -1.77 0.0793
lowsbp10 -sbp10 1 -0.83012 0.72381 -1.15 0.2544
lowdbp10 -dbp10 1 0.97502 1.09048 0.89 0.3736
fgluc10 fasting glucose/10(mg/dl) 1 0.12813 0.21050 0.61 0.5443
lowckd10 -ckd10 1 0.24592 0.40825 0.60 0.5484
bmi10 bmi/10 1 3.81791 1.80938 2.11 0.0376
lowqmidays -qmidays 1 0.11522 0.09187 1.25 0.2130
female 0=male,1=female 1 -0.05717 2.21364 -0.03 0.9795
minority 0=white,1=minority 1 -2.61932 1.99062 -1.32 0.1915
anginahx 1=angina,0=no 1 1.22216 3.21005 0.38 0.7043

Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
mihx 1=mi,0=no 1 1.61557 3.78349 0.43 0.6704
cerevashx 1=cerebrovascular,0=no 1 4.92028 3.02524 1.63 0.1073
pvdhx 1=pvd,0=no 1 -11.07846 6.11663 -1.81 0.0734
chfhx 1=chf,0=no 1 0.90520 6.19715 0.15 0.8842
pcihx 1=pci,0=no 1 2.95459 4.83930 0.61 0.5430
diabhx 1=diabetes,0=no 1 0.93682 2.22718 0.42 0.6750
hychhx 1=hypercholesterolemia,0=no 1 0.93334 1.53839 0.61 0.5456
htenhx 1=hypertension,0=no 1 -1.12812 1.55037 -0.73 0.4687
nofamhxhx 0=family history,1=no 1 -0.08691 1.51302 -0.06 0.9543
killip24 1=Killip2-4 0=Killip1 1 0.70426 2.85548 0.25 0.8057
nyhahi24 1=Class2-4 0=Class1 1 -4.35144 2.81931 -1.54 0.1262
s3any 1=s3 present 0=none 1 4.99304 6.39461 0.78 0.4369
ralesany 1=rales present 0=none 1 -6.00707 5.94111 -1.01 0.3146
cursmoke 1=current 0=else 1 0.09268 1.70768 0.05 0.9568
newq 1=newQ 0=no 1 -1.95091 1.80730 -1.08 0.2832
stelev 1=STelev 0=no 1 -0.85922 1.80920 -0.47 0.6360
Rloss 1=Rloss 0=no 1 -1.67855 1.60150 -1.05 0.2974
multi 1=multi(>70), 0=single 1 1.16005 2.09774 0.55 0.5816
nocollany 1=none, 0=any collateral 1 0.50611 2.45045 0.21 0.8368
ladall ira=LAD(Core or Site) 1 1.66504 1.84056 0.90 0.3680
thromb 1=yes in first24hrs, 0=no 1 -4.16936 2.07669 -2.01 0.0476

Table 2. Relationship with 1 YR EF Among those with p <= 0.20 in Table 1
Number of Observations Read 126
Number of Observations Used 126
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 10 5907.18216 590.71822 11.13 <.0001
Error 115 6101.61943 53.05756
Corrected Total 125 12009
Root MSE 7.28406 R-Square 0.4919
Dependent Mean 53.81746 Adj R-Sq 0.4477
Coeff Var 13.53476
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 48.38891 9.18332 5.27 <.0001
EFall ef(Core or Site) 1 0.33545 0.08206 4.09 <.0001
mpg2cat MPG 0/1 1 -5.21058 1.67114 -3.12 0.0023
age10 age/10(years) 1 -1.20497 0.71146 -1.69 0.0930
hr10 heart rate/10(bpm) 1 -1.45987 0.67405 -2.17 0.0324
bmi10 bmi/10 1 3.45378 1.55390 2.22 0.0282
minority 0=white,1=minority 1 -4.10469 1.64281 -2.50 0.0139
cerevashx 1=cerebrovascular,0=no 1 3.72418 2.72966 1.36 0.1751
pvdhx 1=pvd,0=no 1 -6.96919 4.40420 -1.58 0.1163
nyhahi24 1=Class2-4 0=Class1 1 -5.48042 2.23125 -2.46 0.0155
thromb 1=yes in first24hrs, 0=no 1 -4.79788 1.78586 -2.69 0.0083

Table 3. Relationship with 1 Year EF Outcome: Combining those covariates significant Univariately
Number of Observations Read 126
Number of Observations Used 126
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 15 5964.20769 397.61385 7.24 <.0001
Error 110 6044.59390 54.95085
Corrected Total 125 12009
Root MSE 7.41288 R-Square 0.4967
Dependent Mean 53.81746 Adj R-Sq 0.4280
Coeff Var 13.77413
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 47.20219 8.87087 5.32 <.0001
EFall ef(Core or Site) 1 0.34948 0.09160 3.82 0.0002
mpg2cat MPG 0/1 1 -5.25868 1.76234 -2.98 0.0035
hr10 heart rate/10(bpm) 1 -1.06379 0.69351 -1.53 0.1279
lowsbp10 -sbp10 1 -0.21739 0.46196 -0.47 0.6389
minority 0=white,1=minority 1 -2.59438 1.66668 -1.56 0.1224
mihx 1=mi,0=no 1 -0.38858 2.15365 -0.18 0.8571
hychhx 1=hypercholesterolemia,0=no 1 1.01027 1.37194 0.74 0.4631
nofamhxhx 0=family history,1=no 1 -1.44115 1.37123 -1.05 0.2956
nyhahi24 1=Class2-4 0=Class1 1 -4.37431 2.32686 -1.88 0.0628
s3any 1=s3 present 0=none 1 -0.06802 5.58164 -0.01 0.9903
newq 1=newQ 0=no 1 -2.76924 1.65466 -1.67 0.0971
stelev 1=STelev 0=no 1 -0.67513 1.66137 -0.41 0.6853
Rloss 1=Rloss 0=no 1 -1.98186 1.53339 -1.29 0.1989

Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
ladall ira=LAD(Core or Site) 1 1.94590 1.73911 1.12 0.2656
thromb 1=yes in first24hrs, 0=no 1 -3.28034 1.93001 -1.70 0.0920

Table 4. Relationship with 1 Year EF Outcome Among those with p <= 0.20 in Table 3
Number of Observations Read 126
Number of Observations Used 126
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 8 5780.00911 722.50114 13.57 <.0001
Error 117 6228.79247 53.23754
Corrected Total 125 12009
Root MSE 7.29641 R-Square 0.4813
Dependent Mean 53.81746 Adj R-Sq 0.4458
Coeff Var 13.55769
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 51.37730 6.86485 7.48 <.0001
EFall ef(Core or Site) 1 0.33569 0.08213 4.09 <.0001
mpg2cat MPG 0/1 1 -5.17942 1.67702 -3.09 0.0025
hr10 heart rate/10(bpm) 1 -1.18143 0.67490 -1.75 0.0826
minority 0=white,1=minority 1 -3.07153 1.60508 -1.91 0.0581
nyhahi24 1=Class2-4 0=Class1 1 -3.99308 2.26259 -1.76 0.0802
newq 1=newQ 0=no 1 -3.49434 1.45882 -2.40 0.0182
Rloss 1=Rloss 0=no 1 -1.58752 1.40165 -1.13 0.2597
thromb 1=yes in first24hrs, 0=no 1 -2.97986 1.83517 -1.62 0.1071

OAT Follow up BLUSH – Results of Multiple Regression Model Outcome = 1 Year End Systolic Volume Index
Table 1 – compares end systolic volume index with 32 baseline covariates that were analyzed in the main OAT publication. Those with p-values <= 0.20 are in bold. Covariates listed in the main OAT publication that are linear combinations of other covariates were excluded.
Table 2 – linear regression model showing the effect of post PCI MPG on the end systolic volume index outcome adjusting for the significant covariates in Table 1. Table 3 – compares the end systolic volume index outcome with the baseline covariates which were significant univariately (p <= 0.20). Those that are significant in this multiple regression model are in bold.. Table 4 – linear regression model showing the effect of post PCI MPG on the end systolic volume index outcome adjusting for the significant covariates in Table 3. The difference between tables 1 and 3 are that only LAD is significant in table 1 and LAD as well as no family history are significant in table 3. In all models, post PCI MPG is significantly related to 1 year end systolic volume index adjusting for significant covariates.

Table 1. 1 Year ESVI Outcome – Relationship with 37 Covariates
Number of Observations Read 76
Number of Observations Used 76
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 34 11543 339.49829 2.85 0.0008
Error 41 4875.90223 118.92444
Corrected Total 75 16419
Root MSE 10.90525 R-Square 0.7030
Dependent Mean 29.83523 Adj R-Sq 0.4568
Coeff Var 36.55159
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 23.49087 28.22898 0.83 0.4101
ESIndex 1 0.61101 0.11348 5.38 <.0001
mpg2cat MPG 0/1 1 8.48392 4.09186 2.07 0.0445
age10 age/10(years) 1 0.23332 1.91224 0.12 0.9035
hr10 heart rate/10(bpm) 1 -1.01516 1.64282 -0.62 0.5400
lowsbp10 -sbp10 1 -0.55193 1.45638 -0.38 0.7067
lowdbp10 -dbp10 1 0.25526 2.41175 0.11 0.9162
fgluc10 fasting glucose/10(mg/dl) 1 0.00387 0.39022 0.01 0.9921
lowckd10 -ckd10 1 0.26753 0.73632 0.36 0.7182
bmi10 bmi/10 1 -1.47537 4.20556 -0.35 0.7275
lowef10 -ef10 1 2.34501 2.39544 0.98 0.3333
lowqmidays -qmidays 1 0.09748 0.20843 0.47 0.6425
female 0=male,1=female 1 2.22390 4.40095 0.51 0.6160

Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
minority 0=white,1=minority 1 3.00353 3.93724 0.76 0.4499
anginahx 1=angina,0=no 1 3.38984 10.25250 0.33 0.7426
mihx 1=mi,0=no 1 1.15543 11.16018 0.10 0.9180
cerevashx 1=cerebrovascular,0=no 1 -0.94406 6.10872 -0.15 0.8779
chfhx 1=chf,0=no 1 -11.44472 13.97111 -0.82 0.4174
pcihx 1=pci,0=no 1 0.73489 9.83210 0.07 0.9408
diabhx 1=diabetes,0=no 1 -0.72799 4.77339 -0.15 0.8795
hychhx 1=hypercholesterolemia,0=no 1 0.49009 3.09530 0.16 0.8750
htenhx 1=hypertension,0=no 1 0.43403 3.62742 0.12 0.9053
nofamhxhx 0=family history,1=no 1 4.45464 3.56287 1.25 0.2183
killip24 1=Killip2-4 0=Killip1 1 -0.82064 6.81198 -0.12 0.9047
nyhahi24 1=Class2-4 0=Class1 1 5.78104 5.75430 1.00 0.3210
s3any 1=s3 present 0=none 1 -2.27237 13.96859 -0.16 0.8716
ralesany 1=rales present 0=none 1 11.26300 14.90142 0.76 0.4541
cursmoke 1=current 0=else 1 0.00702 3.63699 0.00 0.9985
newq 1=newQ 0=no 1 1.33336 3.93223 0.34 0.7363
stelev 1=STelev 0=no 1 0.33003 4.38188 0.08 0.9403
Rloss 1=Rloss 0=no 1 1.22230 3.73234 0.33 0.7450
multi 1=multi(>70), 0=single 1 -0.36502 4.20354 -0.09 0.9312
nocollany 1=none, 0=any collateral 1 2.02259 5.16200 0.39 0.6972
ladall ira=LAD(Core or Site) 1 -9.33595 4.12091 -2.27 0.0288
thromb 1=yes in first24hrs, 0=no 1 -1.21254 5.41712 -0.22 0.8240

Table 2. Relationship with 1 YR ESVI Among those with p <= 0.20 in Table 1
Number of Observations Read 76
Number of Observations Used 76
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 3 10024 3341.40447 37.62 <.0001
Error 72 6394.63082 88.81432
Corrected Total 75 16419
Root MSE 9.42413 R-Square 0.6105
Dependent Mean 29.83523 Adj R-Sq 0.5943
Coeff Var 31.58728
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 7.13376 2.43764 2.93 0.0046
ESIndex 1 0.68048 0.06943 9.80 <.0001
mpg2cat MPG 0/1 1 7.08821 2.60404 2.72 0.0081
ladall ira=LAD(Core or Site)
1 -6.59627 2.58786 -2.55 0.0129

Table 3. Relationship with 1 Year ESVI Outcome: Combining those covariates significant Univariately
Number of Observations Read 76
Number of Observations Used 76
Analysis of Variance
Source DF Sum of
SquaresMean
Square F Value Pr > F
Model 15 11157 743.78047 8.48 <.0001
Error 60 5262.13722 87.70229
Corrected Total 75 16419
Root MSE 9.36495 R-Square 0.6795
Dependent Mean 29.83523 Adj R-Sq 0.5994
Coeff Var 31.38890
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 10.06966 12.61000 0.80 0.4277
ESIndex 1 0.61640 0.08527 7.23 <.0001
mpg2cat MPG 0/1 1 7.68294 2.89140 2.66 0.0101
lowsbp10 -sbp10 1 -0.61082 1.03242 -0.59 0.5563
lowdbp10 -dbp10 1 0.09286 1.63994 0.06 0.9550
lowef10 -ef10 1 1.99969 1.72013 1.16 0.2496
lowqmidays -qmidays 1 0.18652 0.15167 1.23 0.2236
anginahx 1=angina,0=no 1 3.26826 7.54659 0.43 0.6665
mihx 1=mi,0=no 1 -0.01512 8.27513 -0.00 0.9985
nofamhxhx 0=family history,1=no 1 5.23123 2.38472 2.19 0.0321
nyhahi24 1=Class2-4 0=Class1 1 5.03650 4.45750 1.13 0.2630

Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
ralesany 1=rales present 0=none 1 12.66874 11.12604 1.14 0.2594
newq 1=newQ 0=no 1 0.74587 2.82836 0.26 0.7929
stelev 1=STelev 0=no 1 0.40130 2.80021 0.14 0.8865
Rloss 1=Rloss 0=no 1 1.42226 2.58830 0.55 0.5847
ladall ira=LAD(Core or Site) 1 -9.23571 3.03950 -3.04 0.0035

Table 4. Relationship with 1 Year ESVI Outcome Among those with p <= 0.20 in Table 3
Number of Observations Read 76
Number of Observations Used 76
Analysis of Variance
Source DF Sum of
SquaresMean
Square F Value Pr > F
Model 4 10306 2576.52662 29.93 <.0001
Error 71 6112.73774 86.09490
Corrected Total 75 16419
Root MSE 9.27873 R-Square 0.6277
Dependent Mean 29.83523 Adj R-Sq 0.6067
Coeff Var 31.09993
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 5.59380 2.54645 2.20 0.0313
ESIndex 1 0.66008 0.06928 9.53 <.0001
mpg2cat MPG 0/1 1 7.11457 2.56390 2.77 0.0071
nofamhxhx 0=family history,1=no 1 3.98913 2.20457 1.81 0.0746
ladall ira=LAD(Core or Site) 1 -6.90132 2.55351 -2.70 0.0086

OAT Follow up BLUSH – Results of Multiple Regression Model Outcome = 1 Year End Diastolic Volume Index
Table 1 – compares end diastolic volume index with 32 baseline covariates that were analyzed in the main OAT publication. Those with p-values <= 0.20 are in bold. Covariates listed in the main OAT publication that are linear combinations of other covariates were excluded.
Table 2 – linear regression model showing the effect of post PCI MPG on the end diastolic volume index outcome adjusting for the significant covariates in Table 1. Table 3 – compares the end diastolic volume index outcome with the baseline covariates which were significant univariately (p <= 0.20). Those that are significant in this multiple regression model are in bold.. Table 4 – linear regression model showing the effect of post PCI MPG on the end diastolic volume index outcome adjusting for the significant covariates in Table 3. In all models, post PCI MPG is not significantly related to 1 year end diastolic volume index adjusting for significant covariates.

Table 1. 1 Year EDVI Outcome – Relationship with 37 Covariates
Number of Observations Read 76
Number of Observations Used 76
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 34 23829 700.84894 1.72 0.0496
Error 41 16747 408.45976
Corrected Total 75 40576
Root MSE 20.21039 R-Square 0.5873
Dependent Mean 64.54388 Adj R-Sq 0.2450
Coeff Var 31.31263
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 68.20039 51.63985 1.32 0.1939
edIndex 1 0.61178 0.11307 5.41 <.0001
mpg2cat MPG 0/1 1 5.12086 7.56101 0.68 0.5020
age10 age/10(years) 1 -1.91593 3.54280 -0.54 0.5916
hr10 heart rate/10(bpm) 1 -1.18103 3.04378 -0.39 0.7000
lowsbp10 -sbp10 1 -0.49151 2.68945 -0.18 0.8559
lowdbp10 -dbp10 1 -0.50395 4.46733 -0.11 0.9107
fgluc10 fasting glucose/10(mg/dl) 1 0.43258 0.72250 0.60 0.5527
lowckd10 -ckd10 1 0.80136 1.36470 0.59 0.5603
bmi10 bmi/10 1 2.60214 7.79325 0.33 0.7402
lowef10 -ef10 1 7.61679 4.19576 1.82 0.0768

Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
lowqmidays -qmidays 1 0.17996 0.38851 0.46 0.6457
female 0=male,1=female 1 -0.91020 8.13447 -0.11 0.9115
minority 0=white,1=minority 1 3.96754 7.29392 0.54 0.5894
anginahx 1=angina,0=no 1 -0.19044 19.00489 -0.01 0.9921
mihx 1=mi,0=no 1 10.00147 20.72728 0.48 0.6320
cerevashx 1=cerebrovascular,0=no 1 5.06501 11.27063 0.45 0.6555
chfhx 1=chf,0=no 1 -26.31920 25.97339 -1.01 0.3169
pcihx 1=pci,0=no 1 2.24095 18.26706 0.12 0.9030
diabhx 1=diabetes,0=no 1 -2.82090 8.84604 -0.32 0.7514
hychhx 1=hypercholesterolemia,0=no 1 4.43646 5.73673 0.77 0.4438
htenhx 1=hypertension,0=no 1 -2.82782 6.72914 -0.42 0.6765
nofamhxhx 0=family history,1=no 1 5.83752 6.58132 0.89 0.3803
killip24 1=Killip2-4 0=Killip1 1 -2.31918 12.61757 -0.18 0.8551
nyhahi24 1=Class2-4 0=Class1 1 0.76180 10.65288 0.07 0.9433
s3any 1=s3 present 0=none 1 3.12483 26.06670 0.12 0.9052
ralesany 1=rales present 0=none 1 25.14429 27.61630 0.91 0.3679
cursmoke 1=current 0=else 1 0.40676 6.74293 0.06 0.9522
newq 1=newQ 0=no 1 -4.63290 7.23669 -0.64 0.5256
stelev 1=STelev 0=no 1 -0.32802 8.13101 -0.04 0.9680
Rloss 1=Rloss 0=no 1 2.29896 6.89299 0.33 0.7404
multi 1=multi(>70), 0=single 1 -3.52595 7.77929 -0.45 0.6528
nocollany 1=none, 0=any collateral 1 6.37643 9.52462 0.67 0.5069
ladall ira=LAD(Core or Site) 1 -17.91050 7.67345 -2.33 0.0246
thromb 1=yes in first24hrs, 0=no 1 -2.73725 10.01245 -0.27 0.7859

Table 2. Relationship with 1 YR EDVI Among those with p <= 0.20 in Table 1
Number of Observations Read 76
Number of Observations Used 76
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 4 19625 4906.18099 16.63 <.0001
Error 71 20951 295.08437
Corrected Total 75 40576
Root MSE 17.17802 R-Square 0.4837
Dependent Mean 64.54388 Adj R-Sq 0.4546
Coeff Var 26.61448
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 55.01273 14.51704 3.79 0.0003
edIndex 1 0.57913 0.07608 7.61 <.0001
mpg2cat MPG 0/1 1 4.48779 4.81121 0.93 0.3541
lowef10 -ef10 1 5.28996 2.53876 2.08 0.0408
ladall ira=LAD(Core or Site) 1 -13.94464 5.01594 -2.78 0.0070

Table 3. Relationship with 1 Year EDVI Outcome: Combining those covariates significant Univariately
Number of Observations Read 76
Number of Observations Used 76
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 12 22161 1846.74387 6.32 <.0001
Error 63 18415 292.29822
Corrected Total 75 40576
Root MSE 17.09673 R-Square 0.5462
Dependent Mean 64.54388 Adj R-Sq 0.4597
Coeff Var 26.48854
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 55.16720 22.11564 2.49 0.0152
edIndex 1 0.58695 0.08321 7.05 <.0001
mpg2cat MPG 0/1 1 4.15654 4.98713 0.83 0.4077
lowdbp10 -dbp10 1 -1.71752 2.05175 -0.84 0.4057
lowckd10 -ckd10 1 0.00822 0.87855 0.01 0.9926
lowef10 -ef10 1 6.81888 2.82083 2.42 0.0185
lowqmidays -qmidays 1 0.32496 0.26917 1.21 0.2318
chfhx 1=chf,0=no 1 -18.39414 18.79616 -0.98 0.3315
diabhx 1=diabetes,0=no 1 -5.23374 5.42287 -0.97 0.3382
nofamhxhx 0=family history,1=no 1 6.00476 4.40391 1.36 0.1776
ralesany 1=rales present 0=none 1 20.10301 18.55640 1.08 0.2828

Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
newq 1=newQ 0=no 1 -4.98282 4.47714 -1.11 0.2700
ladall ira=LAD(Core or Site) 1 -17.73215 5.41008 -3.28 0.0017

Table 4. Relationship with 1 Year EDVI Outcome Among those with p <= 0.20 in Table 3
Number of Observations Read 76
Number of Observations Used 76
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 4 19625 4906.18099 16.63 <.0001
Error 71 20951 295.08437
Corrected Total 75 40576
Root MSE 17.17802 R-Square 0.4837
Dependent Mean 64.54388 Adj R-Sq 0.4546
Coeff Var 26.61448
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 55.01273 14.51704 3.79 0.0003
edIndex 1 0.57913 0.07608 7.61 <.0001
mpg2cat MPG 0/1 1 4.48779 4.81121 0.93 0.3541
lowef10 -ef10 1 5.28996 2.53876 2.08 0.0408
ladall ira=LAD(Core or Site) 1 -13.94464 5.01594 -2.78 0.0070

OAT Follow up BLUSH – Results of Multiple Regression Model
Outcome = 1 Year Wall Motion Table 1 – compares wall motion with 33 baseline covariates that were analyzed in the main OAT publication. Those with p-values <= 0.20 are in bold. Covariates listed in the main OAT publication that are linear combinations of other covariates were excluded.
Table 2 – linear regression model showing the effect of post PCI MPG on the wall motion outcome adjusting for the significant covariates in Table 1. Table 3 – compares the wall motion outcome with the baseline covariates which were significant univariately (p <= 0.20). Those that are significant in this multiple regression model are in bold.. Table 4 – linear regression model showing the effect of post PCI MPG on the wall motion outcome adjusting for the significant covariates in Table 3. The only difference between tables 1 and 3 is that body mass index is significant in table 1 and systolic blood pressure is significant in table 3. In all models, post PCI MPG is significantly related to 1 year wall motion adjusting for significant covariates.

Table 1. 1 Year WM Outcome – Relationship with 37 Covariates
Number of Observations Read 118
Number of Observations Used 118
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 35 77.56234 2.21607 2.98 <.0001
Error 82 60.88952 0.74256
Corrected Total 117 138.45185
Root MSE 0.86172 R-Square 0.5602
Dependent Mean -2.26805 Adj R-Sq 0.3725
Coeff Var -37.99370
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 -3.74791 1.77811 -2.11 0.0381
WM Wall motion 1 0.31037 0.13857 2.24 0.0278
Mpg2cat MPG 0/1 1 -0.81996 0.23663 -3.47 0.0008
age10 age/10(years) 1 -0.04277 0.11192 -0.38 0.7033
hr10 Heart rate/10(bpm) 1 -0.01509 0.08878 -0.17 0.8655
lowsbp10 -sbp10 1 -0.07869 0.08560 -0.92 0.3607
lowdbp10 -dbp10 1 -0.01262 0.13021 -0.10 0.9230
Fgluc10 fasting glucose/10(mg/dl) 1 0.00327 0.02483 0.13 0.8957
lowckd10 -ckd10 1 -0.05660 0.04800 -1.18 0.2417
bmi10 bmi/10 1 0.44846 0.22021 2.04 0.0449
lowef10 -ef10 1 -0.15293 0.14907 -1.03 0.3079
lowqmidays -qmidays 1 0.02610 0.01121 2.33 0.0224
Female 0=male,1=female 1 0.05453 0.27481 0.20 0.8432
Minority 0=white,1=minority 1 -0.13261 0.23676 -0.56 0.5769

Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Anginahx 1=angina,0=no 1 -0.12138 0.40516 -0.30 0.7653
Mihx 1=mi,0=no 1 0.36384 0.50229 0.72 0.4709
cerevashx 1=cerebrovascular,0=no 1 0.09881 0.37813 0.26 0.7945
Pvdhx 1=pvd,0=no 1 0.59585 0.75440 0.79 0.4319
Chfhx 1=chf,0=no 1 0.59828 0.73314 0.82 0.4168
Pcihx 1=pci,0=no 1 -0.67621 0.57081 -1.18 0.2396
Diabhx 1=diabetes,0=no 1 -0.07127 0.26619 -0.27 0.7896
Hychhx 1=hypercholesterolemia,0=no 1 0.07111 0.18526 0.38 0.7021
Htenhx 1=hypertension,0=no 1 0.10687 0.18382 0.58 0.5626
nofamhxhx 0=family history,1=no 1 -0.03513 0.18085 -0.19 0.8465
killip24 1=Killip2-4 0=Killip1 1 -0.30455 0.36442 -0.84 0.4057
nyhahi24 1=Class2-4 0=Class1 1 -0.25109 0.34326 -0.73 0.4666
s3any 1=s3 present 0=none 1 -0.78331 0.77549 -1.01 0.3154
Ralesany 1=rales present 0=none 1 -0.01840 0.70568 -0.03 0.9793
cursmoke 1=current 0=else 1 0.02961 0.20533 0.14 0.8857
Newq 1=newQ 0=no 1 -0.54991 0.22418 -2.45 0.0163
Stelev 1=STelev 0=no 1 -0.18414 0.22038 -0.84 0.4058
Rloss 1=Rloss 0=no 1 0.04193 0.19785 0.21 0.8327
Multi 1=multi(>70), 0=single 1 0.05372 0.25188 0.21 0.8316
nocollany 1=none, 0=any collateral 1 0.11861 0.28648 0.41 0.6799
Ladall ira=LAD(Core or Site) 1 0.59746 0.26003 2.30 0.0241
Thromb 1=yes in first24hrs, 0=no 1 0.15174 0.26368 0.58 0.5666

Table 2. Relationship with 1 YR WM Among those with p <= 0.20 in Table 1
Number of Observations Read 118
Number of Observations Used 118
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 6 63.07751 10.51292 15.48 <.0001
Error 111 75.37434 0.67905
Corrected Total 117 138.45185
Root MSE 0.82404 R-Square 0.4556
Dependent Mean -2.26805 Adj R-Sq 0.4262
Coeff Var -36.33268
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 -1.46441 0.56608 -2.59 0.0110
WM Wall motion 1 0.46015 0.09017 5.10 <.0001
mpg2cat MPG 0/1 1 -0.81065 0.18707 -4.33 <.0001
lowqmidays -qmidays 1 0.02112 0.00917 2.30 0.0232
bmi10 bmi/10 1 0.49642 0.18219 2.72 0.0075
newq 1=newQ 0=no 1 -0.65307 0.16266 -4.01 0.0001
ladall ira=LAD(Core or Site) 1 0.33943 0.17435 1.95 0.0541

Table 3. Relationship with 1 Year WM Outcome: Combining those covariates
significant Univariately
Number of Observations Read 118
Number of Observations Used 118
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 16 66.86472 4.17905 5.90 <.0001
Error 101 71.58713 0.70878
Corrected Total 117 138.45185
Root MSE 0.84189 R-Square 0.4829
Dependent Mean -2.26805 Adj R-Sq 0.4010
Coeff Var -37.11966
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 -2.22631 1.37668 -1.62 0.1090
WM Wall motion 1 0.27120 0.11881 2.28 0.0245
mpg2cat MPG 0/1 1 -0.64350 0.20694 -3.11 0.0024
hr10 heart rate/10(bpm) 1 -0.03756 0.08213 -0.46 0.6484
lowsbp10 -sbp10 1 -0.08297 0.05333 -1.56 0.1229
lowef10 -ef10 1 -0.17733 0.13870 -1.28 0.2040
lowqmidays -qmidays 1 0.02726 0.01003 2.72 0.0077
minority 0=white,1=minority 1 -0.17288 0.19741 -0.88 0.3832
mihx 1=mi,0=no 1 0.25392 0.30180 0.84 0.4021
pvdhx 1=pvd,0=no 1 0.28319 0.57704 0.49 0.6247
nofamhxhx 0=family history,1=no 1 -0.06841 0.16626 -0.41 0.6816
killip24 1=Killip2-4 0=Killip1 1 -0.12165 0.32973 -0.37 0.7129
nyhahi24 1=Class2-4 0=Class1 1 -0.30055 0.29470 -1.02 0.3102
newq 1=newQ 0=no 1 -0.50455 0.19512 -2.59 0.0111
stelev 1=STelev 0=no 1 -0.15231 0.19422 -0.78 0.4347

Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
ladall ira=LAD(Core or Site) 1 0.60092 0.23941 2.51 0.0137
thromb 1=yes in first24hrs, 0=no 1 0.15848 0.23436 0.68 0.5004

Table 4. Relationship with 1 Year WM Outcome Among those with p <= 0.20 in
Table 3
Number of Observations Read 118
Number of Observations Used 118
Analysis of Variance
Source DFSum of
SquaresMean
Square F Value Pr > F
Model 6 60.60711 10.10118 14.40 <.0001
Error 111 77.84475 0.70130
Corrected Total 117 138.45185
Root MSE 0.83744 R-Square 0.4377
Dependent Mean -2.26805 Adj R-Sq 0.4074
Coeff Var -36.92329
Parameter Estimates
Variable Label DFParameter
EstimateStandard
Error t Value Pr > |t|
Intercept Intercept 1 -1.35606 0.69831 -1.94 0.0547
WM Wall motion 1 0.41541 0.09188 4.52 <.0001
mpg2cat MPG 0/1 1 -0.67963 0.19191 -3.54 0.0006
lowsbp10 -sbp10 1 -0.09723 0.05078 -1.91 0.0581
lowqmidays -qmidays 1 0.02437 0.00934 2.61 0.0103
newq 1=newQ 0=no 1 -0.65975 0.16527 -3.99 0.0001
ladall ira=LAD(Core or Site) 1 0.35705 0.17820 2.00 0.0475