Embed Size (px)
Citation preview

REVIEW
Imaging
Myocardial ischaemia and viability: the pivotalrole of echocardiographyPetros Nihoyannopoulos1,2* and Jean Louis Vanoverschelde 3,4
1National Heart and Lung Institute, Imperial College School of Medicine, London, UK; 2Cardiology Department, Hammersmith Hospital, Du Cane Road, London W12 0NN, UK;3Pole de Recherche Cardiovasculaire, Institut de Recherche Experimentale et Clinique, Universite Catholique de Louvain, Belgium; and 4Division of Cardiology, CliniquesUniversitaires Saint-Luc, Brussels, Belgium
Received 13 July 2010; revised 20 December 2010; accepted 6 January 2011; online publish-ahead-of-print 4 February 2011
Echocardiography has a central role for the diagnosis and management of patients with known or suspected coronary artery disease. Besidesthe fact that it provides an essential role in the differential diagnosis of patients presenting with chest pain in the emergency department,echocardiography provides a comprehensive non-invasive haemodynamic and functional assessment of those patients. Stress echocardio-graphy in many institutions is now the preferred stress modality associated with imaging as it is cost-effective and does not use ionizingradiation. It is used for assessing patients with known or suspected coronary artery disease, risk stratification and for assessing myocardialviability. The recent introductions of ultrasound contrast agents as well as deformation imaging techniques have eliminated the last limitationsof stress echocardiography such as image quality and quantification, respectively.- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Myocardial ischaemia † Echocardiography
IntroductionA lot has changed over the past 10 years in the world of echocar-diography. The developments of other cardiac imaging modalitiesand in particular cardiac magnetic resonance imaging (cMR) andCT angiography provided a stimulus for the development of newsequences and modalities in echocardiography such as deformationimaging and three-dimensional echocardiography (3D-Echo). As aconsequence, echocardiography has become a multimodality tech-nique on its own rights. The widespread use of echocardiographyhas allowed for the collection of a large amount of outcome dataso that today it is inconceivable for any patient with known or sus-pected coronary artery disease (CAD) not to have at least oneechocardiographic examination. Finally, established training and awell-structured accreditation programmes provide the platformfor regulating the practice of echocardiography.1 – 3
Acute chest pain syndroms
Differential diagnosisPatients with acute chest pain often pose a diagnostic dilemma, asthey can present with either acute myocardial infarction (AMI)with or without ST-segment elevation, or myocardial ischaemia.
The distinction is made by rise in troponin levels in AMI butremain normal in ischaemia. Subarachnoid haemorrhage, acutepericarditis or myocarditis, hypertrophic cardiomyopathy, aorticdissection may all mimic acute coronary syndromes, with potentialdire consequences as treatment for each of these conditions is fun-damentally different. A potentially catastrophic scenario would beto give thrombolysis for suspected evolving AMI in a patient withaortic dissection or acute pericarditis. Conversely, not givingthrombolysis quickly enough in a patient with evolving AMI maycondemn the patient to sustain extensive myocardial damage.While troponin levels are essential to diagnose AMI, those takeseveral hours to become diagnostic. Echocardiography in theother hand can immediately differentiate the above conditionsand provide the precise diagnosis, allowing for the appropriateand speedy intervention.
Assessing resting left ventriclefunction in coronary artery disease
Global functionAlthough historically M-mode has been used to estimate left ven-tricle (LV) function, it has inherent flaws. It indeed only evaluates
* Corresponding author. Tel: +44 20 8383 8156, Fax: + 44 20 8383 4392, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2011. For permissions please email: [email protected]
European Heart Journal (2011) 32, 810–819doi:10.1093/eurheartj/ehr002
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

the most proximal portion of the LV and ignores the most prog-nostically important LV regions, such as the anterior wall andapex. Consequently, in the setting of CAD, M-mode echocardio-graphy should not be performed.
Two-dimensional echo is the reference technique to assessglobal LV function using the apical biplane method (Simpson’s).4,5
Its main advantage is that it uses series of cross-sectional sectionsof the LV from base to apex, independent of shape and size. Asecond advantage is that all coronary vascular beds are evaluatedso that the derived volumes provide accurate measurement ofthe global LV function.6 Finally, the large amount of outcomedata from many clinical studies have established two-dimensionalechocardiography (2D-Echo) as the mainstay technique for asses-sing LV function. One disadvantage, however, is that often the truecardiac apex is not fully visualized due to tangential cuts.
A prerequisite for accurate measurement of LV function is theability to adequately visualize the endocardium. This is not alwayspossible, particularly in the settings of coronary care or emergencyunits where the equipment used is not the most state-of-the-art.Suboptimal visualization and consequently measurement of LVvolumes may lead to erroneous assessment of LV function, particu-larly when it is most needed, such as after an AMI. Although newtransducer technologies and post-processing methods haveimproved image quality, there are still a number of patients inwhom LV volumes cannot be evaluated. In these patients, it is rec-ommended to use intravenous ultrasound contrast agents in orderto improve endocardial border definition and consequently theaccuracy of LV volumes measurements (Figure 1).7,8
The emergence of 3D-Echo adds to the accuracy of assessing LVvolumes in a fast, semi-automatic fashion, and is not hampered byforeshortened views.9 Its accuracy was shown to be similar to thatof cMR,10,11 even in a multicentre setting with variable levels ofexperience.12 The addition of contrast can further optimize image
acquisition and analysis.13 The recent introduction of single beat3D-Echo makes this technique the current method of choice forthe assessment of LV volumes. Progress is such that frame ratesand image quality improve at galloping pace so that LV volumeassessment by 3D-Echo will probably become the standard.
Regional left ventricle functionThis requires the evaluation of all 16 segments of the LV accordingto the American and European guidelines.5 Those take intoaccount all coronary vascular beds from at least one projection.The role of echocardiography in the detection of regional myocar-dial dysfunction is based on its ability to delineate myocardial thick-ness. During systole, a normally functioning myocardium thickensand moves towards the centre of the cavity. A typical segmentcan be 8–10 mm in diastole increasing by �50% during systole.Reduced systolic thickening in one or more myocardial regionswill indicate reduced blood supply in this territory. The degreeof hypokinesia may vary from minimal (hypokinesia) throughsevere (akinesia), up to paradoxical systolic expansion (dyskinesia).While assessing regional LV function is largely qualitative, it is poss-ible to semi-quantify this using a 4-point scale from normal (grade1) to dyskinetic (grade 4). The sum of the individual segmentscores gives the wall motion score (WMS), which is used toassess severity of LV dysfunction. Dividing the WMS by thenumber of segments assessed gives the WMS index, which hasbeen shown to be an important prognostic indicator.14 New quan-titative methods for evaluating myocardial performance haveemerged taking in consideration the direction of myocardial fibrearchitecture. Strain or strain rate (the rate of deformation overtime) is derived from a high frame rate Tissue Doppler Imagingand measure myocardial deformation and contractility.15,16 Thesemodalities were introduced in order to overcome tethering ofabnormal myocardial segment by adjacent normal segments and
Figure 1 Apical four-chamber two-chamber and three-chamber projections from a patient with sub-optimal endocardial visualization (top)improving dramatically after 0.3 mg of sonovue contrast injection (bottom).
Echocardiography in myocardial ischaemia and viability 811D
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

thus distinguishing between active thickening and passive myocar-dial motion. Tissue Doppler-based measurements provide hightemporal resolution (usually by 200 s21) but is limited by thesignal noise ratio and thus limited reproducibility. More recently,non-Doppler strain quantification has been made possible in allthree myocardial deformation directions: longitudinal, radial, andcircumferential.17 Two-dimensional strain is based on grey-scaleimaging by tracking myocardial speckles at frame rates of 40–80 s21 and can be traced throughout the cardiac cycle in two aswell as in three dimensions. It is therefore likely that this methodwill be the preferred way of quantifying regional myocardial defor-mation, both at rest and during stress (Figure 2).
Detecting myocardial ischaemia
PathophysiologyThere is a well-established parallel relationship between regionalcoronary blood flow and contractile function in the correspondingterritory.18,19 In patients with normal coronary arteries, myocardialblood flow (MBF) can increase .3-fold when oxygen demandincreases, such as during exercise or inotropic stimulation usingdobutamine stress, to allow for the increased heart rate and wallmotion thickening (contractile reserve).
In patients with a significant coronary artery stenosis (.70%),resting MBF usually remains normal, as coronary resistances automa-ticaly decrease to compensate for the presence of the epicardial ste-nosis. Since part of the vasodilatory reserve is used for this purpose,the ability of MBF to increase when oxygen demand increases is lessin the area subtended by a stenotic artery than in non-stenoticvascular beds. The concommittant decrease in distal coronary per-fusion pressure leads to an absolute reduction in MBF in subendo-cardial layers, which in turn results in the hallmark of regionalischaemia, i.e. reduced in wall thickening (hypokinesia). Whenoxygen demand returns to normal (with exercise cessation), thereis resolution of ischaemia with restoration of wall thickening.19
Acute coronary artery occlusion leads to a rapid reduction inresting MBF and hence cessation of muscular contraction in thearea supplied. Relief of the occlusion, either spontaneously or bytreatment (such as thrombolysis or PCI) allows regional wall func-tion to recover back to normal. The duration and severity ofmyocardial ischaemia determines the severity of wall motionabnormalities (WMA) and the rate at which it recovers after theacute episode (‘stunned myocardium’).20
Stress echo for ischaemiaMyocardial ischaemia is accompanied by characteristic mechanical,electrical, and perfusion abnormalities. Although coronary angiogra-phy is the unequivocal reference method for the diagnosis of CAD,the anatomical description alone does not indicate the physiologicalsignificance of stenosis, stressing the need for a functional test. Exer-cise ECG, perfusion defects on single photon emission computedtomography (SPECT) or positron emission tomography (PET), andregional WMA on stress echocardiography or cMR, all permitassessment of the functional significance of coronary stenoses.The detection of regional LV dysfunction occurs early in the ‘ischae-mic cascade’ preceding ECG changes and symptoms.
Echocardiography has by far the best spatial resolution (2 mm)over SPECT (12–15 mm) or PET (4 mm), only parallels that ofCMR so that all myocardial regions can be visualized at rest andduring stress. As a result, stress echocardiography has gained anunquestionable clinical role as an accurate and inexpensive stresstest.21 With the most recent use of ultrasound contrast agentsduring stress, there is additional information provided by assessingmyocardial perfusion.22,23
Specific markers of ischaemiaThe presence of CAD does not automatically imply ischaemia,which is a dynamic phenomenon. For this, a functional test is pre-ferred instead of just the anatomic detection of a stenotic lesion byeither computed tomography or coronary angiography. RestingWMA alone may be indicative of a previous AMI, the age ofwhich may be difficult to determine by echocardiography. Never-theless, the detection of a substantial WMA (at least two contigu-ous segments) in a symptomatic patient may well point thediagnosis to the right direction.
Myocardial ischaemia can be detected in the following waysusing echocardiography:
(1) If normal resting wall motion, reduction in wall thickening of atleast two contiguous segments during stress.
(2) If resting akinesia (or hypokinesia) deteriorating during stress,both in extent (more segments) or in severity (from hypokine-sia to akinesia).
(3) If resting akinesia or hypokinesia that temporarily improvesduring low dose of dobutamine followed by subsequent deterio-ration at a higher dose. This implies that the myocardial segmentis viable but subtented by a stenotic vessel and thus jeopardized.
(4) A clear fall in overall LV function compared with baselinesuggests extensive ischaemia. This may be evaluated by a fallin ejection fraction.
(5) Using contrast ultrasound, the appearance of a perfusiondefects during vasodilator stress or dobutamine. The perfusion
Figure 2 Two-dimensional speckle tracking echocardiographyfrom an apical three-chamber projection showing reduced con-traction in the anterior wall expressed by the most faint color-ation as opposed to the normal contraction of the posteriorwall expressed by the most vivid red coloration. The bar codeon the right shows the scale of regional contraction.
P. Nihoyannopoulos and J.L. Vanoverschelde809cD
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

defect will appear as an absence of contrast opacification inone of the three coronary vascular beds compared with theresting images (Figure 3)
Methods of stress echocardiographyExercise echocardiographyThe fundamental advantage of exercise is that it provides physio-logical cardiovascular stress and that physicians are used to recog-nize associated ECG changes and symptoms. It is also wellestablished with long experience and good outcome data.24 Exer-cise can be performed in either upright or supine positions, thelatter being preferred when combined with echocardiography asit allows for the concomitant assessment of mitral or aorticvalve function.
Dobutamine stress echocardiographyDobutamine stress, which is easier to combine with echocardio-graphy, has become the preferred method of stressing the heartin Europe,21 with similar diagnostic accuracy to exercise. Dobuta-mine is a synthetic catecholamine that stimulates primarilyb1-adrenergic receptors with minimal b2 and a1 effects. It isgiven intravenously starting from 5 to 40 mg kg21 min21 in incre-ments of 5 or 10 mg kg21 min21 for 3 min each. At low doses(,10 mg kg21 min21), it demonstrates a relatively more potentinotropic than the chronotropic effect, allowing stimulation ofmyocardial contractility before significant increases in the heartrate, and presumably ischaemia, occur. At higher doses, both ino-tropic and chronotropic stimulation occur, resulting in increasedcardiac output, myocardial oxygen consumption, and ischaemiain myocardial regions subtended by significantly stenosed coronaryarteries. Given intravenously, its half life is �2 min.
Dipyridamole stress echocardiographyVasodilator stress with adenosine or dipyridamole induces MBFheterogeneity and ischaemia. Dipyridamole (which provokes theaccumulation of adenosine) stimulates adenosine receptors. Inthe presence of coronary stenosis, its administration causes adrop in post-stenotic pressure and therefore, a critical drop in
subendocardial perfusion pressure, which in turn provokes adecrease in absolute subendocardial flow.
FeasibilityThe perceived disadvantage of stress echocardiography is itsinability to obtain optimal imaging in all patients. However, withthe availability of ultrasound contrast agents, image quality is nolonger an issue. The use of ultrasound contrast agents duringstress echocardiography is now recommended by the EuropeanAssociation of Echocardiography when more than two contiguoussegments are not well visualized.7
Stress echocardiography, like all imaging techniques, is operatordependent, both in respect of data acquisition and interpretation.Familiarity with all forms of stresses is an index of the quality of anecho laboratory. Indications for the individual patient can thereforebe optimized, thereby avoiding the relative and absolute contraindi-cations of each test. Proper training and experience is pivotal, as is forall imaging.25 The use of ultrasound contrast agents during stressechocardiography may also give additional information of myocardialperfusion. Following the ischaemic cascade, hypoperfusion precedesWMA. Consequently, the addition of perfusion should be more sen-sitive than contraction alone. Myocardial contrast echocardiography(MCE) has been used to assess myocardial perfusion at rest andduring stress.26,27 Low power imaging is the optimal mode fordetecting myocardial perfusion and wall motion simultaneously.Two large prospective clinical studies showed the added value indiagnosing myocardial ischaemia when MCE was used to assess per-fusion.28,29 They indicated that MCE significantly improves overalland regional sensitivity as well as negative predictive value for thediagnosis of CAD, when compared with wall motion assessment.Myocardial contrast echocardiography indeed allows perfusionabnormalities to be identified before WMA occur, thus improvingsensitivity and accuracy in patients who fail to achieve the targetheart rate, as well as in those in whom the test needs to be termi-nated prematurely.
The increasing availability of 3D-Echo may also allow for a betterand easier assessment of LV function during stress. It has beenshown to be equally accurate to 2D-Echo, but with muchshorter acquisition times and greater reproducibility, owing tothe use of the same transducer position throughout the examin-ation. Although current 3D-systems provide relatively low frame-rates, the new equipment generation only requires a single heart-beat with higher frame rates, thus making stress 3D-Echo a clinicalreality.30
The combination of 3D-Echo with contrast is an attractive evol-ution of two of the most important recent developments in echo-cardiography. With contrast-enhanced 3D-Echo, LV volumemeasurements can be made fast, accurately and reproducibly,regional wall motion assessment is feasible for most LV segments,and perfusion defects can be assessed both at rest and duringstress.31
Comparison with other imagingmodalitiesThere are four imaging modalities that can be used to assess myo-cardial ischaemia, each presenting with a number of advantages and
Figure 3 Apical four-chamber view using myocardial contrastechocardiography at rest and during stress (dobutamine). Whilethe resting images show an homogeneous myocardial opacifica-tion, during stress there is a clear absence of opacification atthe apex.
Echocardiography in myocardial ischaemia and viability 813D
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

limitations. All those are set to assess the functional significance ofa coronary lesion. Those modalities include stress echocardiogra-phy, MCE, SPECT, and cMR.
Table 1 compares the sensitivities and specificities for thesevarious modalities derived in studies that have coronary angiogra-phy as a reference method.32– 38 In general, these studies haveshown that perfusion imaging had a somewhat better sensitivitybut a somewhat lower specificity than techniques assessingregional wall motion. Interestingly, cMR has not shown to besuperior to dobutamine stress echocardiography (DSE), despiteclaims of better image quality and reproducibility. These data indi-cate that whichever modality is perferred should not only be amatter of individual choice and local expertise but should alsotake into account any possible harmful effects for the patient, par-ticularly irradiation. Most patients with chronic CAD will indeedneed repeated coronary testing during the course of theirdisease and many will also require exposure to ionizing radiationas part of the workup of other intercurrent diseases. Accordingly,stress echocardiography and/of cMR should be preferred imagingmodalities to assess CAD in these patients, the former havingthe advantage of being far more available.
Risk assessment and outcomesStress echocardiography can be used for screening high-riskpatients before major peripheral vascular surgery or orthopaedicsurgery, or in patients with chronic renal failure.
Assessment of patients’ prognosis is important for cost-effectiveclinical decision making. A number of studies have demonstratedthat the yearly event rate following a normal exercise or DSE isonly 0.4–0.9%, a value not different from that seen following anormal SPECT.39,40 In a randomized controlled study in patientswith suspected acute coronary syndrome and negative troponins,DSE resulted in less diagnostic uncertainty, fewer referrals forfurther investigations and a significant cost-benefit comparedwith exercise ECG.41
In a landmark study, Poldermans et al.42 showed that the rate ofcardiac death or myocardial infarction in patients with new WMAduring DSE or extensive resting WMA increased 3.6- and 2.5-fold,respectively. In patients with extensive resting WMA or a leftbundle branch block (LBBB), induction of new WMA increasedthe frequency of cardiac death or (re)infarction during a 5-year
period from 12 to 31% and from 16 to 44%, respectively. Theyconcluded that the risk of future cardiac events can be assessedby DSE, distinguishing subgroups of patient with high (.30% in5 years), median (12% in 5 years), and low (8% in 5 years) risk.Importantly, patients with normal DSE have a good prognosis.
In the particular group of patients presenting with troponinnegative acute chest pain syndrome, stress echocardiography wassuperior to exercise ECG in identifying patients with myocardialischaemia.43 Similarly, in patients with new onset of chest painand not previously known CAD, stress echocardiography providedan independent and incremental prediction of hard cardiac eventsbeyond that provided by ECG and clinical data alone.44
Finally, Rinkevich et al.45 convincingly demonstrated the advan-tages of early use of MCE in the emergency room. In a 2-yearfollow-up study in .1000 patients they showed that myocardialperfusion provides incremental prognostic value than regionalfunction alone and that this is essentially confined to those withabnormal resting regional function. Those patients with abnormalregional function and normal myocardial perfusion fare betterthan those with both, abnormal function, and perfusion. Theauthors provide compelling evidence that contrast improvesassessment of regional function.
Assessment of myocardial viabilityAssessment of myocardial viability is another area in which echo-cardiography plays an important diagnostic role. It indeed allowsfor the assessment of two of the main features of myocardial via-bility, i.e. maintained resting perfusion and residual inotropicreserve.
PathophysiologyResting myocardial perfusionAssessment of perfusion-contraction matching is crucial to theunderstanding of chronic LV ischaemic dysfunction. It requiresthe ability to measure regional MBF and to correlate these findingswith data on regional myocardial function, acquired simul-taneously.46 In clinical practice, this can only be achieved usingPET47,48 and MCE.49 Resting flow measurements obtained inviable myocardium have been remarkably variable, about half ofthe segments showing reduced perfusion, the other half displaying
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Comparable sensitivities and specificities using different stress test modalities that used coronary angiographyas the reference test
Modality No. of studies No. of patients Sensitivity Specificity
Dipyridamole stress 26 2302 61–87 (78) 70–94 (92)
Dobutamine stress echo 16 2594 61–94 (80) 72–96 (86)
MCE 21 2998 78–96 (83) 51–87 (80)
MPS SPECT 25 4698 76–96 (87) 43–92 (72)
CMR—perfusion 17 1140 82–91 (87) 58–94 (77)
CMR WM (dobutamine) 11 1006 78–91 (86) 75–100 (86)
DSE strain rate echocardiography 1 44 86 89
Modified from references20,32– 38.
P. Nihoyannopoulos and J.L. Vanoverschelde814D
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

only minor or no reductions in MBF.50 Viable myocardium encom-passes a wide range of perfusion-contraction matching patterns,from perfusion-contraction mismatch, a characteristic feature ofmyocardial stunning, to moderate parallel reductions in perfusionand contraction (so-called myocardial hibernation).
Myocardial flow reserveIrrespective of resting flow, perfusion reserve is always reduced inviable myocardium,51 albeit more severely in segments with lowrest perfusion.52 The severity of flow reserve reduction directlyimpacts on contractile reserve, as this requires increases in MBFand oxygen consumption.53
Inotropic reserveViable myocardium often displays contractile reserve when chal-lenged by an inotropic stimulus, such as dobutamine or low levelexercise.54,55 However, its response to these stimuli varies fromsegment to segment as well as with the intensity and the durationof stimulation.
Most viable segments exhibit a biphasic response when chal-lenged by increasing levels of inotropic stimulation.56 At lowlevels, and provided that sufficient residual flow reserve ispresent,53 systolic wall thickening usually increases earlier insystole. At higher levels, when the increased in demand cannotbe matched anymore by a further increase in MBF because ofthe underlying CAD, systolic function deteriorates and can evenbecome worse than at baseline. The observation of such a biphasicpattern is extremely important to rule out other causes of regionaldysfunction, like the presence of a subendocardial scar or theoverall process of remodeling,57 in which a sustained contractileresponse at both low and high levels of inotropic stimulation isobserved.
Not every viable segment improves during inotropic stimulation.About 25% of ‘metabolically’ viable segments, i.e. those with pre-served energy metabolism, exhibit no contractile reserve.54 Com-pared with viable segments with recruitable contractile reserve,those lacking contractile reserve usually have a lower restingMBF and take up more glucose under fasting conditions thannormal segments or viable segments with recruitable inotropicreserve,53 a finding consistent severely blunted myocardial flowreserve. Other factors also likely contribute to the lack of contrac-tile reserve in otherwise viable segments, such as severity of thestructural changes affecting the cardiomyocytes (vide infra) andthe density and affinity of b-adrenoreceptors.58
Structural modificationsSeveral structural alterations that affect the microcirculation, thecardiomyocytes and the extracellular matrix have been describedin biopsy specimens harvested from viable segments in patientsundergoing bypass surgery.51
MicrocirculationThe microvasculature is usually better preserved in viable than innon-viable segments. This is particularly true for the capillarieswhose density is usually normal in viable segments but reduced,albeit to a variable extent, in non-viable segments.59 As would
be expected, the major determinant of capillary density is theseverity of interstitial fibrosis.
Myocyte alterationsThe primary alteration seen in cardiomyocytes is the depletion ofcontractile elements.51 In some cells, this is limited to the vicinity ofthe nucleus, whereas in others it is very extended, leaving only fewor no sarcomeres at the cell periphery. The space previously occu-pied by the myofilaments is filled with glycogen. Alterations inmitocondria, sarcoplasmic reticulum, T-tubules, and endoplasmicreticulum are also frequently noted. Many of the sarcomeric com-ponents are significantly reduced, whereas cytoskeletal proteinsare usually disorganized. Gap junctions and the expression ofconnexin-43, a major gap junction protein, are also reduced.
Extracellular matrixThe interstitial alterations consist in increased amounts of type Icollagen, type III collagen, and fibronectin.60 Within the widenedinterstitium are variable numbers of fibroblasts and macrophages,and scant increased amounts of elastic fibres. Importantly, acuteischaemic changes such as endothelial swelling of the microvascu-lature are absent.
Animal models of myocardial hibernationAnimal models of chronic coronary stenosis or progressiveameroid occlusion have shed a new light on both the mechanismsand the temporal progression of reversible ischaemic dysfunc-tion.61 During the first weeks after the onset of dysfunction, endo-cardial MBF has been found to be either normal or only marginallydecreased, implying that chronic myocardial stunning is the mostlikely mechanism of dysfunction. With time and probably alsoincreases in the physiological significance of the underlying coron-ary narrowings, some of the dysfunctional segments which were‘chronically stunned’ on early examination, eventually becomeunderperfused. The transition from chronic stunning to chronichibernation only occurs for threshold reductions in myocardialflow reserve. The experimental data thus suggest that chronicreversible myocardial ischaemic dysfunction is a complex, pro-gressive, and dynamic phenomenon, that is initiated by repeatedepisodes of ischaemia, and in which resting perfusion, althoughinitially preserved, may subsequently become reduced, probablyin response to the decrease in myocyte energy demand.
The pathophysiological spectrum of myocardial viabilityAltogether, the currently available data suggest that a spectrum ofmyocardial dysfunction exists in patients with coronary disease(Table 2). The initial stages of dysfunction most likely correspondto chronic stunning and are characterized by normal resting per-fusion but reduced flow reserve, mild myocyte alterations, main-tained membrane integrity (allowing the transport of cations andmetabolic fuels), preserved capacity to respond to an inotropicstimulus and no or little tissue fibrosis. Following revascularization,functional recovery is likely to be rapid and complete. At the oppo-site, more advanced stages of dysfunction are probably associatedwith reduced rest perfusion, increased tissue fibrosis, more severemyocyte remodelilng and a decreased ability to respond to inotropicstimuli.62 Nonetheless, membrane function and energy metabolism
Echocardiography in myocardial ischaemia and viability 815D
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

long remain preserved. Following revascularization, functionalrecovery, if any, is usually delayed and in the end mostlyincomplete (Figures 3–6).
Role of echocardiographyEchocardiography is probably the most versatile imaging modalityfor assessing myocardial viability. First, it readily identifies thecore of the problem, i.e. the presence of regional WMA. It alsoallows one to assess their severity. Second, it allows for theinitial characterization of the dysfunctional segments, both interms of residual wall thickness and tissue reflectivity. Third,when combined with the use of ultrasonic contrast agents, itpermits the assessment of MBF, both at rest and during hyperhe-mia. Forth, when performed during an inotropic challenge, suchas the infusion of increasing doses of dobutamine, it allows forthe evaluation of the presence of recruitable inotropic reserve.And last but not least, it is the most frequently used techniqueto assess functional recovery after revascularization.
Rest echocardiographyDiastolic wall thickness measured during resting echocardiographyprovides some information on the relative amounts of myocardialtissue vs. fibrotic scar tissue within a particular myocardialsegment. A diastolic wall thickness .6 mm has a sensitivity of94% but a specificity of only 48% for predicting recovery of con-tractility after revascularization.63 The appeal of this method isobvious, as rest echocardiography is readily available and relativelyinexpensive when compared with alternative modalities. However,it is limited by its poor specificity and the variability in the imagequality which affects the accuracy and reproducibility of wall thick-ness measurements, as well as by the relatively small number ofsegments exhibiting reduced thickness.
Rest echocardiography and particularly contrast-enhanced3D-Echo offers the opportunity to directly assess the amountand distribution of scar tissue. Indeed, myocardial scar tissueusually appears brighter than normal myocardium on diagnosticechocardiographic images, the intensity of the backscatteredecho signals being proportionate to the amount, orientation, andcompactness of the underlying collagen fibres. Although theseareas of increased brightness can be readily seen on M-modeand 2D-Echo, a recent study has demonstrated that they couldbe more accurately localized and sized using 3D-Echo.64 Thesefindings suggest that 3D-Echo could become an alternative toassess the amount of myocardial scar to cMR when cMR iseither unavailable or contra-indicated.
Myocardial contrast echocardiographyThe basic premise behind the use of MCE to assess myocardial via-bility is that only viable myocardium has an intact microcirculation.Earlier investigators used the intracoronary route for contrastadministration. In both the immediate post-AMI setting or inpatients with chronic dysfunction, MCE predicted recovery of LVfunction after revascularization with a high sensitivity (85–94%)and a lower specificity (43–65%). From these initial studies,MCE appeared to have similar test properties as thallium SPECT.65
With the development of new contrast ultrasound agents thatcan cross capillaries, and the introduction of newer contrastimaging modalities that reduce the microbubble destruction,MCE now allows essential parameters of the microcirculatoryfunction, such as MBF and myocardial blood volume (MBV), tobe measured. Measures of MBV by MCE correlate well with micro-vascular density and capillary area and inversely with collagencontent.58 Myocardial blood flows have also been shown to beinversely correlated with collagen content. Yet, their relationshipwith microvascular density appears to be somewhat morecomplex. When microvascular density is reduced, MBF hasusually been found to be reduced in proportion. Converesly,when the microvascular density is preserved, MBF can either benormal or reduced. Thus, whenever MBV is normal, assessmentof MBF may help differentiate chronically stunned from truly hiber-nating myocardium. Accordingly, MCE predicts functional recoverywith both a high sensitivity and a high negative predictive value(.90%). Specificity is somewhat lower (+65%), but better thanwith SPECT imaging.66
Dobutamine stress echocardiographyThe demonstration of contractile reserve using various provocativestimuli, such as nitroglycerin, dipyridamole, post-extrasystolicpotentiation, catecholamines (e.g. isoprenaline, adrenaline, dopa-mine, or dobutamine), and exercise, can be studied with echocar-diography. Dobutamine stress echocardiography is the mostaccepted and widely available of these techniques.
The protocol in most laboratories uses dobutamine infusion attwo low-dose stages (5 and 10 mg kg21 min21), with each stagelasting 3 min. Some advocate utilizing an even lower startingdose of 2.5 mg kg21 min21 because in patients with critical coron-ary stenosis, myocardial ischaemia may be precipitated even withdoses as low as 5 mg kg21 min21. Thereafter, the dose is increasedin 10 mg kg21 min21 increments to a maximum dose of50 mg kg21 min21. Atropine may be given if the target heart rateis not achieved with standard dobutamine doses. The test is
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 The patterns of chronic ischaemic dysfunction
Rest flow Flow reserve Contractile reserve Fasting FDG uptake Structural changes Reversibility
Chronic stunning ↔ � Yes ↔ No Yes
Transition phase ↔ �� Yes ↔ or � Mild Yes
Chronic hibernation � ��� May be absent � More severe/fibrosis Delayed/incomplete
Infarction � �� No � Fibrosis No
Remodelling ↔ ↔ May be absent ↔ Fibrosis No
P. Nihoyannopoulos and J.L. Vanoverschelde816D
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

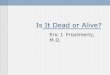
Figure 4 Inotropic response to dobutamine in dysfunctional segments (white arrows) with normal rest flow (13NH3) and F-18-fluorodeoxy-glucose (18FDG) uptake. The upper row shows images obtained from the apical four-chamber view in end-diastole at baseline and during theinfusion of 5, 10, and 20 mg kg21 min21 of dobutamine. The lower row shows the corresponding end-systolic images. The yellow arrows indi-cate segments improving function, whereas red arrows indicate deteriorating segments. The sequence illustrates a typical biphasic response inthe distal septum and the apex. Since blood flow and FDG uptake are normal in these segments, this is an example of chronically stunnedmyocardium.
Figure 5 Inotropic response to dobutamine in dysfunctional segments (white arrows) with mildly reduced rest flow (13NH3) and a normalFDG uptake (18FDG). The upper row shows images obtained from the apical two-chamber view in end-diastole at baseline and during theinfusion of 5, 10, and 20 mg kg21 min21 of dobutamine. The lower row shows the corresponding end-systolic images. The yellow arrows indi-cate segments improving function, whereas red arrows indicate deteriorating segments. The sequence illustrates a very transient biphasicresponse in the mid-anterior segment, followed by immediate deterioration at the low heart rate. Since blood flow was slightly reducedand FDG uptake was normal in that segment, this is an example of mildly hibernating myocardium.
Echocardiography in myocardial ischaemia and viability 817D
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

Figure 7 Inotropic response to dobutamine in dysfunctional segments (white arrows) with severely reduced rest flow (13NH3) and FDG uptake(18FDG). The upper row shows images obtained from the apical four-chamber view in end-diastole at baseline and during the infusion of 5, 10, and40 mg kg21 min21 of dobutamine. The lower row shows the corresponding end-systolic images. The sequence shows the absence of inotropicreserve in the distal septum. Since blood flow and FDG uptake were both reduced in that segment, this is an example of irreversibly infarctedmyocardium.
Figure 6 Inotropic response to dobutamine in dysfunctional segments (white arrows) with moderately reduced rest flow (13NH3) and anormal FDG uptake (18FDG). The upper row shows images obtained from the parasternal long-axis view in end-diastole at baseline andduring the infusion of 5 and 10 mg kg21 min21 of dobutamine. The lower row shows the corresponding end-systolic images. The sequenceillustrates the absence of inotropic reserve in the anteroseptal segment. Since blood flow was definitively reduced and FDG uptake wasnormal in that segment, this is an example of severely hibernating myocardium.
P. Nihoyannopoulos and J.L. Vanoverschelde818D
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

terminated when the patient achieves 85% of the age-predictedmaximum heart rate or clinical or echocardiographic evidence ofischaemia occurs (Figure 7).
Most viable segments will demonstrate improvement of contracti-lity at doses of 10 mg kg21 min21 or less.56 The benefit of proceedingto higher doses of dobutamine, even if contractile reserve is demon-strated at lower doses, is to observe the ‘biphasic response’. In thepresence of significant coronary stenosis, an initial improvement in sys-tolic wall thickening mayoccur at low dosesof dobutamine, represent-ing the region’s contractile reserve as previously stated. However, asoxygen consumption increases when contractility and the heart raterise, the flow-limiting stenotic vessel is unable to keep up with theoxygen demand, and the ensuing ischaemia leads to hypokinesis ofthe affected wall segment. This biphasic response demonstrates twocritical components to the definition of myocardial viability, namelyviability itself and flow limitation. It is therefore not surprising if thebiphasic response has the best predictive value of all the possibleresponses to dobutamine in determining improvement in LV functionfollowing revascularization. Accordingly, it is recommended to use thecombined low- and high-dose approach in all patients who do not havecontraindications.
The cumulative sensitivity, specificity, positive, and negative predic-tive values of DSE based on a recent meta-analysis were 81, 78, 75, and83%, respectively.67 Although generally good, these figures imply thatthere are a significant number of false positive and false negative find-ings. False positive results can be partially explained by tethering ofnon-viable segments by adjacent normally contracting segments,leading to the illusion of improved function, by the presence of non-transmural infarction, by incomplete revascularization of otherwiseviable segments and by the fact that functional recovery sometimesoccur more slowly than allowed for by the follow-up periods. Falsenegative findings are most often related to the fact that the myocardialflow reserve is reduced to such an extent that any increase in oxygendemand, even in viable segments, leads to ischaemia. Additionally, theultrastructural changes occurring in viablemyocardium may be sopro-found that contraction is not possible until sustained restoration ofMBF has taken place. As with all stress echocardiographic techniques,wall motion scoring is limited by subjectivity and technical challenges.More objective assessment of regional wall function using myocardialdeformation imaging should thus theoretically provide a better accu-racy. However, a recent study using both tissue Doppler and Speckletracking echocardiography did not show a significant advantage ofthese new methods when compared with the visual assessment ofregional wall motion.68
Dobutamine stress echocardiography also predicts prognosis inpatients with chronic LV dysfunction. Several studies have demon-strated that long-term survival is better among patients with echo-cardiographic evidence of myocardial viability who had beenrevascularized than in those with either viable myocardiumtreated medically, non-viable myocardium undergoing revasculari-zation, or non-viable myocardium treated medically.69,70 Thesedata lend further support to the use of dobutamine echocardiogra-phy for the assessment of myocardial viability, as this technique notonly allows accurate identification of which patient will improve itsregional and global left ventricular function after coronary revascu-larization, but also may indicate those most likely to benefit withrespect to prognosis.
Immediate post-infarction vs. chronic leftventricular dysfunction settingsThe echocardiographic methods used to assess myocardial viabilityin the immediate post-infarction settings are similar to those inchronic LV dysfunction, i.e. assessment of residual myocardial per-fusion, residual contractile reserve, and detection of inducibleischaemia. Several studies have demonstrated that the extent ofregional perfusion and contractile reserve abnormalities correlatedwith the likelyhood of spontaneous or post-revascularizationrecovery.71 After thrombolysis, observation of a biphasic responsenot only suggests the presence of viable myocardium but also indi-cates the persistence of significant residual stenosis on theinfarct-related artery. One should nonetheless recognize that inthe era of primary PCI, the interest in post-MI viability assessmenthas progressively been mollified, particularly whenever theinfarct-related artery has been succesfully treated.
Summary and conclusionsEchocardiography with its multiple modalities plays a central role inthe evaluation of patients with known or suspected CAD, startingfrom the differential diagnosis of the patient presenting with acutechest pain. In the patient presenting with AMI, with or withoutST-segment elevation, echocardiography is the first imagingmodality to be used in order to ascertain the presence andextent of LV dysfunction and the presence of complications. Inthe absence of AMI, echocardiography will play an important diag-nostic role to identify the presence of reversible myocardial ischae-mia. Stress echocardiography in many institutions is now thepreferred stress modality associated with imaging as it is cost-effective and does not use ionizing radiation. Finally, echocardio-graphy plays a pivotal role in the assessment of myocardial viabilitysince the presence and extent of viable myocardium may guidetherapeutic strategies. It has been stressed that laboratories andindividuals need to have experience and be accredited by the auth-orities so that the results of the range of echocardiographic inves-tigations will be credible. Current and future developments, suchas 3D-Echo and deformation imaging either with tissue Dopplerof speckle tracking, hold the promise of making echocardiographyeven more quantitative, less operator-dependent and more repro-ducible than it is today. However, clinical studies are necessary todemonstrate their real clinical value.37
Conflict of interest: none declared.
References1. Popescu BA, Andrade MJ, Badano LP, Fox KF, Flachskampf FA, Lancellotti P,
Varga A, Sicari R, Evangelista A, Nihoyannopoulos P, Zamorano JL. EuropeanAssociation of Echocardiography recommendations for training, competence,and quality improvement in echocardiography. European J Echocardiogr 2009;10:893–905.
2. British Society of Echocardiography Guidelines. Training in echocardiography. BrHeart J 1994;71:2–5.
3. Nihoyannopoulos P, Fox K, Fraser A, Pinto F. EAE laboratory standards andaccreditation. Eur J Echocardiogr 2007;8:80–87.
4. Lang RM, Bierig M, Devereux RB, Flachskamf FA, Foster E, Pellikka PA, Picard MH,Roman MJ, Seward J, Shanewise J, Solomon S, Spencer KT, St John Sutton M,Stewart W. Recommendations for chamber quantification. Eur J Echocardiogr2006;7:79–108.
Echocardiography in myocardial ischaemia and viability 819D
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

5. Evangelista A, Flachskampf F, Lancellotti P, Badano L, Aguilar R, Monaghan M,Zamorano J, Nihoyannopoulos P. European Association of Echocardiography rec-ommendations for standardization of performance, digital storage and reportingof echocardiographic studies. Eur J Echocardiogr 2008;9:438–448.
6. Gordon EP, Schnittger I, Fitzgerald PJ, Williams P, Popp RL. Reproducibility of leftventricular volumes by two-dimensional echocardiography. J Am Coll Cardiol 1983;2:506–513.
7. Senior R, Becher H, Monaghan M, Agati L, Zamorano J, Vanoverschelde JL,Nihoyannopoulos P. Contrast echocardiography: evidence-based recommen-dations by European Association of Echocardiography. Eur J Echocardiogr 2009;10:194–212.
8. Hoffmann R, von Bardeleben S, Kasprzak JD, Borges AC, ten Cate F, Firschke C,Lafitte S, Al-Saadi N, Kuntz-Hehner S, Horstick G, Greis C, Engelhardt M,Vanoverschelde JL, Becher H. Analysis of regional left ventricular function by cine-ventriculography, cardiac magnetic resonance imaging, and unenhanced andcontrast-enhanced echocardiography. J Am Coll Cardiol 2006;47:121–128.
9. Hare JL, Jenkins C, Nakatani S, Ogawa A, Yu CM, Marwick TH. Feasibility andclinical decision-making with 3D echocardiography in routine practice. Heart2008;94:440–445.
10. Jenkins C, Bricknell K, Hanekom L, Marwick TH. Reproducibility and accuracy ofechocardiographic measurements of left ventricular parameters using real-timethree-dimensional echocardiography. J Am Coll Cardiol 2004;44:878–886.
11. Kuhl HP, Schreckenberg M, Rulands D, Katoh M, Schfer W, Schummers G,Bucker A, Hanrath P, Franke A. High-resolution transthoracic real-time three-dimensional echocardiography: quantitation of cardiac volumes and functionusing semi-automatic border detection and comparison with cardiac magneticresonance imaging. J Am Coll Cardiol 2004;43:2083–2090.
12. Mor-Avi V, Jenkins C, Kuhl HP, Nesser H-J, Marwick T, Franke A, Ebner C,Freed BH, Steringer-Mascherbauer R, Pollard H, Weinert L, Niel J, Sugeng L,Lang RM. Real-time 3-dimensional echocardiographic quantification of left ventri-cular volumes: multicenter study for validation with magnetic resonance imagingand investigation of sources of error. J Am Coll Cardiol Img 2008;1:413–423.
13. Krenning BJ, Kirschbaum SW, Soliman OI, Nemes A, van Geuns RJ, Vletter WB,Veltman CE, Ten Cate FJ, Roelandt JR, Geleijnse ML. Comparison of contrastagent-enhanced versus non-contrast agent-enhanced real-time three-dimensionalechocardiography for analysis of left ventricular systolic function. Am J Cardiol2007;100:1485–1489.
14. Sabia P, Afrookteh A, Touchstone DA, Keller MW, Esquivel L, Kaul S. Value ofregional wall motion abnormality in the emergency room diagnosis of acute myo-cardial infarction. A prospective study using two-dimensional echocardiography.Circulation 1991;84(3 Suppl.):185–192.
15. D’Hooge J, Heimdal A, Jamal F, Kukulski T, Bijnens B, Rademakers F, Hatle L,Suetens P, Sutherland GR. Regional strain and strain rate measurements bycardiac ultrasound: principles, implementation and limitations. Eur J Echocardiogr2000;1:154–170.
16. Greenberg NL, Firstenberg MS, Castro PL, Main M, Travaglini A, Odabashian JA,Drinko JK, Rodriguez LL, Thomas JD, Garcia MJ. Doppler-derived myocardial sys-tolic strain rate is a strong index of left ventricular contractility. Circulation 2002;105:99–105.
17. Helle-Valle T, Crosby J, Edvardsen T, Lyseggen E, Amundsen BH, Smith H-J,Rosen BD, Lima JAC, Torp H, Ihlen H, Smiseth OA. New non-invasive methodfor assessment of left ventricular rotation: speckle tracking echocardiography.Circulation 2005;112:3149–3156.
18. Tennant R, Wiggers CJ. The effect of coronary artery occlusion on myocardialcontraction. Am J Physiol 1935;12:351.
19. Gallagher KP, Matsuzaki M, Osakada G, Kemper S, Ross J Jr. Effect of exercise onthe relationship between myocardial blood flow and systolic wall thickening indogs with acute coronary stenosis. Circ Res 1983;52:716–729.
20. Tsoukas A, Ikonomidis I, Cokkinos P, Nihoyannopoulos P. Significance of persist-ent left ventricular dysfunction during recovery after dobutamine stress echocar-diography. J Am Coll Cardiol 1997;30:621–626.
21. Sicari R, Nihoyannopoulos P, Evangelista A, Kasprzak J, Lancellotti P,Poldermans D, Voigt J-U, Zamorano JL. Stress echocardiography expert consen-sus statement European Association of Echocardiography (EAE). Eur J Echocar-diogr 2008;9:415–437.
22. Kaul S, Jayaweera AR. Coronary and myocardial blood volumes: non-invasivetools to assess the coronary microcirculation? Circulation 1997;96:719–724.
23. Swinburn JM, Senior R. Real time contrast echocardiography—a new bedsidetechnique to predict contractile reserve early after acute myocardial infarction.Eur J Echocardiogr 2002;3:95–99.
24. Marwick TH, Nemec JJ, Pashkow FJ, Stewart WJ, Salcedo EE. Accuracy and limit-ations of exercise echocardiography in a routine clinical setting. J Am Coll Cardiol1992;19:74–81.
25. Pamela SD. ACCF/ASE/ACEP/AHA/ASNC/SCAI/SCCT/SCMR 2008 Appropri-ateness Criteria for Stress Echocardiography: A Report of the American
College of Cardiology Foundation Appropriateness Criteria Task Force, Ameri-can Society of Echocardiography, American College of Emergency Physicians,American Heart Association, American Society of Nuclear Cardiology, Societyfor Cardiovascular Angiography and Interventions, Society of CardiovascularComputed Tomography, and Society for Cardiovascular Magnetic Resonance.J Am Coll Cardiol 2008;51:1127–1147.
26. Wei K, Jayaweera AR, Firoozan S, Linka A, Skyba DM, Kaul S. Basis for detectionof stenosis using venous administration of microbubbles during myocardial con-trast echocardiography: bolus or continuous infusion? J Am Coll Cardiol 1998;32:252–260.
27. Linka AZ, Sklenar J, Wei K, Jayaweera AR, Skyba DM, Kaul S. Assessment oftransmural distribution of myocardial perfusion with contrast echocardiography.Circulation 1998;98:1912–1920.
28. Elhendy A, O’Leary EL, Xie F, MvGrain AC, Anderson JR, Porter TR. Comparativeaccuracy of real-time myocardial contrast perfusion imaging and all motion analy-sis during dobutamine stress echocardiography for the diagnosis of coronaryartery disease. J Am Coll Cardiol 2004;44:2185–2191.
29. Tsutsui JM, Elhendy A, Anderson JR, Xie F, McGrain AC, Porter TR. Prognosticvalue of dobutamine stress myocardial contrast perfusion echocardiography.Circulation 2005;112:1444–1450.
30. Matsumura Y, Hozumi T, Arai K, Sugioka K, Ujino K, Takemoto Y, Yamagishi H,Yoshiyama M, Yoshikawa J. Non-invasive assessment of myocardial ischaemiausing new real-time three-dimensional dobutamine stress echocardiography:comparison with conventional two-dimensional methods. Eur Heart J 2005;26:1625–1632.
31. Bhan A, Kapetanakis S, Rana BS, Ho E, Wilson K, Pearson P, Mushemi S,Deguzman J, Reiken J, Harden MD, Walker N, Rafter PG, Monaghan MJ. Real-timethree-dimensional myocardial contrast echocardiography: is it clinically feasible?Eur J Echocardiogr 2008;9:761–765.
32. Senior R, Monaghan M, Becher H, Mayet J, Nihoyannopoulos P. Stress echocar-diography for the diagnosis and risk stratification of patients with suspected orknown coronary artery disease: a critical appraisal. Heart 2005;91:427–436.
33. Geleijnse ML, Elhendy A. Can stress echocardiography compete with perfusionscintigraphy in the detection of coronary artery disease and cardiac risk assess-ment? Eur J Echocardiogr 2000;1:12–21.
34. Tsutsui JM, Elhendy A, Xie F, O’Leeary E, McGrain AC, Porter TR. Safety of dobu-tamine stress real time myocardial contrast echocardiography. J Am Coll Cardiol2005;45:1235–1242.
35. Beleslin BD, Ostojic M, Djordjevic-Dikie A, Babic R, Nedeljkovic M, Stankovic G,Stojkovic S, Marinkovic J, Nedeljkovic I, Stepanovic J, Saponjski J, Petrasinovic Z,Nedeljkovic SKanjuh V. Integrated evaluation of relation between coronarylesion features and stress echocardiography results: the importance of coronarylesion morphology. J Am Coll Cardiol 1999;33:717–726.
36. Smart SC, Bhatia A, Hellman R, Stoiber T, Krasnow A, Collier BD, Sagar KB.Dobutamine-atropine stress echocardiography and dipyridamole sestamibi scinti-graphy for the detection of coronary artery disease: limitations and concordance.J Am Coll Cardiol 2000;36:1265–1273.
37. Voigt J-U, Exner B, Schmiedehausen K, Huchzermeyer C, Reulbach U, Nixdorff U,Platsch G, Kuwert T, Daniel WG, Flachskampf FA. Strain-rate imaging duringdobutamine stress echocardiography provides objective evidence of inducibleischemia. Circulation 2003;107:2120–2126.
38. Gibbons RJ, Chatterjee K, Daley J, Douglas JS, Fihn SD, Gardin JM, Grunwald MA,Levy D, Lytle BW, O’Rourke RA, Schafer WP, Williams SV, Ritchie JL,Cheitlin MD, Eagle KA, Gardner TJ, Garson A Jr, Russell RO, Ryan TJ,Smith SC Jr. ACC/AHA/ACP-ASIM guidelines for the management of patientswith chronic stable angina: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee onManagement of Patients With Chronic Stable Angina). J Am Coll Cardiol 1999;33:2092–2197.
39. Sawada SG, Ryan T, Conley MJ, Corya BC, Feigenbaum H, Armstrong WF. Prog-nostic value of a normal exercise echocardiogram. Am Heart J 1990;120:49–55.
40. Metz LD, Beattie M, Hom R, Redberg RF, Grady D, Fleischmann KE. The prognos-tic value of normal exercise myocardial perfusion imaging and exercise echocar-diography: a meta-analysis. J Am Coll Cardiol 2007;49:227–237.
41. Jeetley P, Burden L, Stoykova B, Senior R. Clinical and economic impact of stressechocardiography compared with exercise electrocardiography in patients withsuspected acute coronary syndrome but negative troponin: a prospective ran-domized controlled study. Eur Heart J 2007;28:204–211.
42. Poldermans D, Fioretti PM, Boersma E, Bax JJ, Thomson IR, Roelandt JR,Simoons ML. Long-term prognostic value of dobutamine-atropine stress echocar-diography in 1737 patients with known or suspected coronary artery disease: asingle-center experience. Circulation 1999;99:757–762.
43. Jeetley P, Burden L, Senior R. Superior risk stratification by stress echocardiogra-phy compared to exercise electrocardiography in troponin negative acute chestpain—a prospective randomised trial. Eur J Echocardiogr 2006;7:155–164.
P. Nihoyannopoulos and J.L. Vanoverschelde819aD
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022

44. Chelliah R, Anantharam B, Burden L, Alhajiri A, Senior R. Independent and incre-mental value of stress echocardiography over clinical and stress electrocardio-graphic parameters for the prediction of hard cardiac events in new-onsetsuspected angina with no history of coronary artery disease. Eur J Echocardiogr2010;11:875–882.
45. Rinkevich D, Kaul S, Wang X-Q, Tong KL, Belcik T, Kalvaitis S, Lepper W,Dent JM, Wei K. Regional left ventricular perfusion and function in patients pre-senting to the emergency department with chest pain and no ST-segmentelevation. Eur Heart J 2005;26:1606–1611.
46. Ross J Jr. Myocardial perfusion-contraction matching. Circulation 1991;83:1076–1083.
47. Bergmann SR, Herrero P, Markham J, Walsh MN. Noninvasive quantitation ofmyocardial blood flow in human subjects with oxygen-15-labeled water and posi-tron emission tomography. J Am Coll Cardiol 1989;14:639–652.
48. Bol A, Melin JA, Vanoverschelde JL, Baudhuin T, Vogelaers D, De Pauw M,Michel C, Luxen A, Labar D, Cogneau M, Robert A, Heyndrickx GR, Wijns W.Direct comparison of N-13 ammonia and O-15 water estimates of perfusionfor quantitation of regional myocardial blood flow by microspheres. Circulation1993;87:512–525.
49. Van Camp G, Ay T, Pasquet A, London V, Bol A, Gisellu G, Hendrickx GR,Rafter P, Melin JA, Vanoverschelde J-L. Quantification of myocardial blood flowwith real-time power modulation myocardial contrast echocardiography. J AmSoc Echo 2003;16:263–270.
50. Vanoverschelde J-L, Melin JA. The pathophysiology of myocardial hibernation.Current controversies and future directions. Prog Cardiovsc Dis 2001;43:387–398.
51. Vanoverschelde J-LJ, Wijns W, Depre C, Essamri B, Heyndrickx G, Borgers M,Bol A, Melin JA. Mechanisms of chronic regional postischemic dysfunction inhumans: New insights from the study of non-infarcted collateral dependent myo-cardium. Circulation 1993;87:1513–1523.
52. Marzullo P, Parodi O, Sambuceti G, Giogetti A, Picano E, Gimelli A, Salvadori P,Abbate A. Residual coronary reserve identifies segmental viability in patients withwall motion abnormalities. J Am Coll Cardiol 1995;26:342–350.
53. Lee HH, Davila-Roman VG, Ludbrook PA, Courtois M, Walsh JF, Delano DA,Rubin PJ, Gropler RJ. Dependency of contractile reserve on myocardial bloodflow. Implications for the assessment of myocardial viability with dobutaminestress echocardiography. Circulation 1997;96:2884–2891.
54. Gerber BL, Vanoverschelde J-L, Bol A, Michel C, Labar D, Wijns W, Melin JA.Myocardial blood flow, glucose uptake and recruitment of inotropic reserve inchronic left ventricular ischemic dysfunction. Implications for the pathophysiologyof chronic myocardial hibernation. Circulation 1996;94:651–659.
55. Hoffer EP, Dewe W, Celentano C, Pierard LA. Low-level exercise echocardiogra-phy detects contractile reserve and predicts reversible dysfunction after acutemyocardial infarction: comparison with low-dose Dobutamine echocardiography.J Am Coll Cardiol 1999;34:989–997.
56. Afridi I, Kleiman NS, Raizner AE, Zoghbi WA. Dobutamine echocardiography inmyocardial hibernation. Optimal dose and accuracy in predicting recovery of ven-tricular function after coronary angioplasty. Circulation 1995;91:663–670.
57. Schinkel AF, Poldermans D, Rizzello V, Vanoverschelde JL, Elhendy A, Boersma E,Roelandt JR, Bax JJ. Why do patients with ischemic cardiomyopathy and a substan-tial amount of viable myocardium not always recover in function after revascular-ization? J Thorac Cardiovasc Surg 2004;127:385–390.
58. Shan K, Bick RJ, Poindexter BJ, Nagueh SF, Shimoni S, Verani MS, Keng F,Reardon MJ, Letsou GV, Howell JF, Zoghbi WA. Altered adrenergic receptordensity in myocardial hibernation in humans: a possible mechanism of depressedmyocardial function. Circulation 2000;102:2599–2606.
59. Shimoni S, Frangogiannis NG, Aggeli CJ, Shan K, Quinones MA, Espada R,Letsou GV, Lawrie GM, Winters WL, Reardon MJ, Zoghbi WA. Microvascularstructural correlates of myocardial contrast echocardiography in patients withcoronary artery disease and left ventricular dysfunction: implications for theassessment of myocardial hibernation. Circulation 2002;106:950–956.
60. Depre C, Vanoverschelde J-LJ, Melin JA, Borgers M, Bol A, Ausma J, Dion R,Wijns W. Structural and metabolic correlates of the reversibility of chronic leftventricular ischemic dysfunction in humans. Am J Physiol 1995;268:H1265–H1275.
61. Canty JM Jr, Fallavollita JA. Resting myocardial flow in hibernating myocardium:validating animal models of human pathophysiology. Am J Physiol 1999;277:H417–H422.
62. Vanoverschelde J-L, Depre C, Gerber BL, Borgers M, Wijns W, Melin JA,Dion R. Time-course of functional recovery after coronary bypass surgery inpatients with chronic left ventricular ischemic dysfunction. Am J Cardiol 2000;85:1432–1439.
63. Cwajg JM, Cwajg E, Nagueh SF, He ZX, Qureshi U, Olmos LI, Quinones MA,Verani MS, Winters WL, Zoghbi WA. End-diastolic wall thickness as a predictorof recovery of function in myocardial hibernation: relation to rest-redistributionTl-201 tomography and dobutamine stress echocardiography. J Am Coll Cardiol2000;35:1152–1161.
64. Montant P, Chenot F, Goffinet C, Poncelet A, Vancraeynest A, Pasquet A,Gerber BL, Vanoverschelde J.-L. Detection and quantification of myocardialscars using contrast-enhanced 3D-echocardiography. Circulation Cardiovasc Imag2010;3:415–423.
65. Nagueh SF, Vaduganathan P, Ali N, Blaustein A, Verani MS, Winters WL Jr,Zoghbi WA. Identification of hibernating myocardium: comparative accuracyof myocardial contrast echocardiography, rest-redistribution thallium-201tomography and dobutamine echocardiography. J Am Coll Cardiol 1997;29:985–993.
66. Janardhanan R, Swinburn JM, Greaves K, Senior R. Usefulness of myocardial con-trast echocardiography using low-power continuous imaging early after acutemyocardial infarction to predict late functional left ventricular recovery. Am JCardiol 2003;92:493–497.
67. Schinkel AF, Bax JJ, Poldermans D, Elhendy A, Ferrari R, Rahimtoola SH. Hibernat-ing myocardium: diagnosis and patient outcomes. Curr Probl Cardiol 2007;32:375–410.
68. Bansal M, Jeffriess L, Leano R, Mundy J, Marwick TH. Assessment of myocardialviability at dobutamine echocardiography by deformation analysis using tissue vel-ocity and speckle-tracking. JACC Cardiovasc Imaging 2010;3:121–131.
69. Pasquet A, Robert A, D’Hondt A-M, Melin JA, Vanoverschelde J-L. Prognosticvalue of myocardial ischemia and viability in patients with chronic left ventricularischemic dysfunction. Circulation 1999;100:141–148.
70. Allman KC, Shaw LJ, Hachamovitch R, Udelson JE. Myocardial viability testing andimpact of revascularization on prognosis in patients with coronary artery diseaseand left ventricular dysfunction. J Am Coll Cardiol 2002;39:1151–1158.
71. Mollema SA, Nucifora G, Bax JJ. Prognostic value of echocardiography after acutemyocardial infarction. Heart 2009;95:1732–1745.
Echocardiography in myocardial ischaemia and viability 819bD
ownloaded from
https://academic.oup.com
/eurheartj/article/32/7/810/2398474 by guest on 31 January 2022