Embed Size (px)
Citation preview

Myelodysplastic Syndromes“What is on the horizon?”
Rami Komrokji, MDSenior Member & Professor of Oncologic Sciences
Section Head – Leukemia & MDSVice Chair - Malignant Hematology Department
H Lee Moffitt Cancer Center & Research InstituteTampa, Florida

Myelodysplastic Syndromes (MDS)
• A group of malignant hematopoietic neoplasms characterized by1
– Bone marrow failure with resultant cytopenia and related complications
– Evidence of clonality by cytogenetic abnormalities or somatic gene mutations.
– Dysplastic cytologic morphology is the hallmark of the disease
– Tendency to progress to AML
• Overall incidence 3.7-4.8/100,0002
– In US (true estimates ≈37,000-48,000)
• Median age: 70 yrs; incidence: 34-47/100,000 >75 yrs3
AML = acute myeloid leukemia.1. Bennett J, et al. The myelodysplastic syndromes. In: Abeloff MD, et al, eds. Clinical Oncology. New York, NY: Churchill Livingstone; 2004:2849-2881. 2. SEER data. 2000-2009. 3. SEER 18 data. 2000-2009.

Non-clonal ICUS
CHIP CCUS LR-MDS HR-MDS
Traditional ICUS MDS by WHO 2016
Clonality
Dysplasia
Cytopenias
Overall Risk
+ – ++ ++ ++
–/+ – – + ++
– + + + ++
Very Low Very Low Low (?) Low High
BM Blast %< 5% < 5% < 5% < 5% 5-19%
Are these two the same?Does morphologic dysplasia matter?
CCUS = clonal cytopenias of undetermined significance; ICUS = idiopathic cytopenias of undetermined significance; CHIP = clonal hematopoiesis of indeterminate potential; LR = lower risk, HR = higher risk
MDS the spectrum?

Risk Groups for the IPSS-RRisk group Points % of Patients Median survival, years
Time until 25% of patients develop AML,
years
Very low ≤ 1.5 19 % 8.8 Not reached
Low > 1.5 – 3 38 % 5.3 10.8
Intermediate > 3 – 4.5 20 % 3.0 3.2
High > 4.5 – 6 13 % 1.6 1.4
Very High > 6 10 % 0.8 0.73
100
Overall Survival, years
Pa
tie
nts
, %
00 2 4 6 8 10 12
20
40
60
80
Pa
tie
nts
, %
Time to AML Evolution, years
0 2 4 6 8 10 12
100
0
20
40
60
80
Very low Low Int High Very high
Adapted from Greenberg PL, et al. Blood. 1997;89:2079-2088.

Somatic Gene Mutations Improve Precisionof the IPSS-R
Bejar R. Haematologica 2014; 99: 956.

Summary of Risk Stratification
• very low risk R-IPSS +/- 1 HR somatic mutation (SM).
• Low risk R-IPSS no HR SM• Very low/low/intermediate R-IPSS with SF3B1 SM.
• Low risk R-IPSS + 1 HR SM.• Intermediate risk R-IPSS no HR SM.
• Intermediate risk R-IPSS + HR SM• Very high and high risk R-IPSS.• Complex monosomy karyotype.• > 3 HR SM.• P53 mutation.

Anemia Management Algorithm in LR-MDS 2019
Fenaux P, et al. Lancet Oncol. 2009;10:223-232..
Epo<200mU/mL
<2U RBC/mo
ESA
Non-del5q
AZA 5 dayLEN+/- Epo
Del (5q)
Iso- or +1
LenalidomideDel5q
Epo>200mU/mL
>2U RBC/mo
Age
>60 <60
SF3B1 Mu+ No SGM or SF3B1 Mu-
MDS > 24 mos HLA-DR15+,+8
ISTNon-del5qpathway
*SGM, somatic gene mutation.

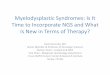
Excess Smad2/3 Signaling Suppresses Late-Stage RBC Maturation in MDS
TGF-β ligands (e.g. GDF15,
GDF11, BMP6, activin A)
negatively regulate late
erythropoiesis
Bone marrow microenvironment
Luspatercept releases maturation block
Baso E Poly E Ortho E Reticulocyte RBC
SCFIL-3EPO
BFU-E CFU-E Pro-E
EPO-responsive
EPO-dependent
EPO
8–64 cells500 cells
Sustained Hb increase Rapid Hb increase
• Mobilizes cells from precursor pools into blood• Effect relies on continuous formation of
late-stage precursors from earlier progenitors
Zhou L, et al. Blood. 2008;112:3434-3443.

The MEDALIST Trial: Results of a Phase 3, Randomized, Double-Blind,
Placebo-Controlled Study of Luspatercept to Treat Patients With Very Low-,
Low-, or Intermediate-Risk Myelodysplastic Syndromes (MDS) Associated
Anemia With Ring Sideroblasts (RS) Who Require Red Blood Cell (RBC)
Transfusions
Pierre Fenaux, Uwe Platzbecker, Ghulam J. Mufti, Guillermo Garcia-Manero, Rena Buckstein, Valeria Santini, María Díez-Campelo, Carlo Finelli, Mario Cazzola, Osman Ilhan, Mikkael A. Sekeres, José F. Falantes, Beatriz Arrizabalaga, Flavia Salvi, Valentina Giai, Paresh Vyas, David Bowen, Dominik Selleslag, Amy E. DeZern, Joseph G. Jurcic, Ulrich Germing, Katharina S. Götze, Bruno Quesnel, Odile Beyne-Rauzy, Thomas Cluzeau, Maria Teresa Voso, Dominiek Mazure, Edo Vellenga, Peter L. Greenberg, Eva Hellström-Lindberg, Amer M. Zeidan, Abderrahmane Laadem,
Aziz Benzohra, Jennie Zhang, Anita Rampersad, Peter G. Linde, Matthew L. Sherman, Rami S. Komrokji, Alan F. List

MEDALIST Trial
Luspatercept
• Luspatercept is an investigational first-in-class erythroid maturation agent that neutralizes select TGF-β superfamily ligands to inhibit aberrant Smad2/3 signaling and enhance late-stage erythropoiesis in MDS models1
• In a phase 2 study in LR, non-del(5q) MDS, luspatercept yielded a high frequency of transfusion reduction or RBC-TI in patients with MDS-RS vs other subtypes2
ActRIIB, human activin receptor type IIB; IgG1 Fc, immunoglobulin G1 fragment crystallizable; RBC-TI, red blood cell transfusion independence; RS, ring sideroblasts; TGF-β, transforming growth factor beta.
1. Suragani RN, et al. Nat Med. 2014;20:408-414;
2. Platzbecker U, et. A. Lancet Oncol. 2017; 18:1338.
Modified extracellular domain ofActRIIB
HumanIgG1 Fcdomain
LuspaterceptActRIIB / IgG1 Fc recombinant
fusion protein
Cytoplasm
Nucleus
Erythroid maturation
Smad2/3
Complex
P
TGF-βsuperfamily
ligandActRIIB

MEDALIST TrialStudy Design – A Randomized, Double-Blind, Placebo-Controlled, Phase 3 Study
Data cutoff: May 8, 2018 Includes last subject randomized + 48 weeks.EPO, erythropoietin; HMA, hypomethylating agent; iMID, immunomodulatory drug; IWG, International Working Group; s.c., subcutaneously; SF3B1, splicing factor 3b subunit 1; WHO, World Health Organization.
Patient Population
• MDS-RS (WHO): ≥ 15% RS or ≥ 5% with SF3B1mutation
• < 5% blasts in bone marrow
• No del(5q) MDS
• IPSS-R Very Low-, Low-, or Intermediate-risk
• Prior ESA response
– Refractory, intolerant
– ESA naive: EPO > 200 U/L
• Average RBC transfusion burden ≥ 2 units/8 weeks
• No prior treatment with disease-modifying agents (e.g. iMIDs, HMAs)
Randomize 2:1
Luspatercept 1.0 mg/kg (s.c.) every 21 daysn = 153
Placebo (s.c.) every 21 daysn = 76
Dose titrated up to a maximum of 1.75 mg/kg
Disease & Response Assessment week 24 & every 6 months Treatment discontinued for lack of clinical benefit or disease
progression per IWG criteria; no crossover allowed
Subjects followed ≥ 3 years post final dose for AML progression, subsequent MDS treatment and overall survival

MEDALIST TrialPrimary Endpoint: Red Blood Cell Transfusion Independence ≥ 8 Weeks
RBC-TI ≥ 8 weeks Luspatercept
(n = 153)Placebo(n = 76)
Weeks 1–24, n (%) 58 (37.9) 10 (13.2)
95% CI 30.2–46.1 6.5–22.9
P valuea < 0.0001a Cochran–Mantel–Haenszel test stratified for average baseline RBC transfusion requirement (≥ 6 units vs < 6 units of RBCs/8 weeks) and baseline IPSS-R score (Very Low or Low vs Intermediate).CI, confidence interval.

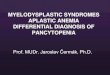
MEDALIST TrialDuration of RBC-TI Response in Primary Endpoint Responders
a During indicated treatment period. Patients who maintained RBC-TI at the time of analysis are censored.
Duration of RBC-TIa (week)
Pro
ba
bilit
y o
f M
ain
tain
ing
RB
C-T
I
Number of patients
Luspatercept 58 49 37 29 22 18 10 6 3 2 1 1 0
Placebo 10 9 3 2 2 2 0
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 10 20 30 40 50 60 70 80 90 100 110 120
Luspatercept
Placebo
Censored
Median duration (weeks) (95% CI): 30.6 (20.6–40.6) vs 13.6 (9.1–54.9)

MEDALIST TrialSecondary Endpoint: Erythroid Response (HI-E)
Luspatercept(n = 153)
Placebo(n = 76)
Achieved HI-Ea (weeks 1–24), n (%) 81 (52.9) 9 (11.8)
Reduction of ≥ 4 RBC units/8 weeks(baseline transfusion burden ≥ 4 units/8 weeks) 52/107 (48.6) 8/56 (14.3)
Hb increase of ≥ 1.5 g/dL(baseline transfusion burden < 4 units/8 weeks) 29/46 (63.0) 1/20 (5.0)
95% CI 44.72–61.05 5.56–21.29
P valueb < 0.0001
Achieved HI-Ea (weeks 1–48), n (%) 90 (58.8) 13 (17.1)
Reduction of ≥ 4 RBC units/8 weeks(baseline RBC transfusion burden ≥ 4 units/8 weeks) 58/107 (54.2) 12/56 (21.4)
Hb increase of ≥ 1.5 g/dL(baseline RBC transfusion burden < 4 units/8 weeks) 32/46 (69.6) 1/20 (5.0)
95% CI 50.59–66.71 9.43–27.47
P valueb < 0.0001a Defined as the proportion of patients meeting the HI-E criteria per IWG 2006 criteria (Cheson et al. 2006) sustained over a consecutive 56-day period during the indicated treatment period. b Luspatercept compared with placebo, Cochran–Mantel–Haenszel test.

Imetelstat Treatment Leads to Durable Transfusion Independence in RBC Transfusion-Dependent,
Non-Del(5q) Lower Risk MDS Relapsed/Refractory to Erythropoiesis-Stimulating Agent Who Are
Lenalidomide and HMA Naive
David P. Steensma, MD1, Uwe Platzbecker, MD2, Koen Van Eygen, MD3, Azra Raza, MD4, Valeria Santini, MD5, Ulrich Germing, MD, PhD6, Patricia Font, MD7, Irina Samarina, MD8, Maria Díez-Campelo, MD, PhD9, Sylvain Thepot, MD10, Edo Vellenga, MD11, Mrinal M. Patnaik, MD, MBBS12, Jun Ho Jang, MD, PhD13,
Jacqueline Bussolari, PhD14, Laurie Sherman, BSN14, Libo Sun, PhD14, Helen Varsos, MS, RPh14, Esther Rose, MD14 and Pierre Fenaux, MD, PhD15
1Dana-Farber Cancer Institute (US), 2University Hospital Carl Gustav Carus, Dresden (DE), 3Algemeen Ziekenhuis Groeninge, Kortrijk (BE),
4Columbia University Medical Center (US), 5MDS Unit, AOU Careggi-University of Florence (IT), 6Heinrich-Heine-Universität, Düsseldorf (DE),
7Hospital General Universitario Gregorio Marañon, Madrid (ES), 8Emergency Hospital of Dzerzhinsk, Nizhny Novgorod (RU),
9The University Hospital of Salamanca (ES), 10CHU Angers (FR), 11University Medical Center Groningen (NE), 12Mayo Clinic, Rochester (US),
13Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul (KO), 14Janssen Research & Development, LLC (US),
15Hôpital Saint-Louis, Université Paris (FR)
ASH 2018 Abstract #463

single arm
open label
Background: IMerge/NCT02598661 (Part 1) Study Design1
1o Endpoint: 8-Week RBC TI2o Endpoints: 24-Week RBC TI / Time to TI / TI duration / TR (HI-E: Transfusion Reduction by ≥ 4 RBC units over 8 weeks) / MDS response per IWG / Overall survival / Incidence of AML / SafetyExploratory: telomerase activity / hTERT / telomere length / genetic mutations
Pre-medication:diphenhydramine, hydrocortisone 100-200 mg (or equivalent)
Supportive care: RBC transfusions, myeloid growth factors per local guidelines
1. Fenaux P, et al. HemaSphere 2018;2(S1):S1557 [oral presentation]
Patients with MDS
• IPSS Low or Int-1• Relapsed / refractory to ESA or
ineligible for ESA• Transfusion dependent (≥4u RBC/8
weeks)• ANC ≥ 1.5 x 109/L • Platelets ≥ 75 x 109/L
ImetelstatTreatment
7.5 mg/kg IV q4w (2-hr infusion)
AML, acute myeloid leukemia; ANC, absolute neutrophil count; HI-E, hematologic improvement-erythroid; IWG, International Working Group; TI, transfusion independence; TR, transfusion reduction.

IMerge: Longest Transfusion-Free Interval
Parameters N=38
Rate of 8-week TI, n (%) 14 (37)
Rate of 24-week TI, n (%) 10 (26)
Median time to onset of TI (range), weeks 8.1 (0.1-33.1)
Median duration of TI (range), weeks NE (17.0-NE)
Among the patients achieving durable TI, all showed a Hbrise of ≥ 3.0 g/dL compared to baseline during the transfusion-free interval
Hb, hemoglobin; HI-E, hematologic improvement-erythroid; TI, transfusion independence; TR, transfusion reduction.
150
125
75
50
25
0Patients
24-week TI 8-week TI HI-E (TR) No response
24
8
Treatment Group: Imetelstat (N=38)
100
Lo
ng
es
t T
ran
sfu
sio
n F
ree
In
terv
al (W
ee
ks
)

AHSCT candidate
? AHSCT at time of HMA failure
HMA
Clinical trial
NO
Proposal for HR-MDS Treatment Algorithm
TET-2 MT VAF > 10%/ASXL-1 WT
P53 VAF > 40% P53 VAF < 20%
YES
YES NO
HMACytopenia/ Myeloblasts > 10%
HMA prior to AHSCT
YESNO
Observe prior to AHSCT
Decitabine
AHSCT
P53 clearance

Phase 1b/2 Combination Study of APR-246 and Azacitidine(AZA) in Patients with TP53 Mutant Myelodysplastic
Syndromes (MDS) and Acute Myeloid Leukemia (AML)
David A Sallman1, Amy DeZern2, David P Steensma3, Kendra Sweet1, Thomas Cluzeau4, Mikkael Sekkeres5, Guillermo
Garcia-Manero6, Gail Roboz7, Amy McLemore1, Kathy McGraw1, John Puskas1, Ling Zhang1, Chirag Bhagat8, Jiqiang
Yao9, Najla H Al Ali1, Eric Padron1, Roger Tell10, Jeffrey E. Lancet1, Pierre Fenaux11, Alan F List1 and Rami S Komrokji1
1Malignant Hematology Department, H. Lee Moffitt Cancer Center and Research
Institute, Tampa, FL, USA.; 2Sidney Kimmel Comprehensive Cancer Center, Johns
Hopkins University, Baltimore, MD, USA; 3Department of Medical Oncology, Dana
Farber Cancer Institute, Harvard Medical School, Boston, MA, USA; 4Cote D’azur
University, Nice Sophia Antipolis University, Hematology Department, CHU Nice, Nice,
France; 5Department of Hematology and Medical Oncology, Cleveland Clinic,
Cleveland, OH, USA; 6Department of Leukemia, MD Anderson Cancer Center,
Houston, TX, USA; 7Weill Cornell Medical College, New York, NY, USA; 9Cancer
Informatics Core, H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL, USA; 10Aprea Therapeutics, Stockholm, Sweden; 11Hospital St Louis, Paris 7 University,
Paris, France.
2018 ASH Abstract # 3091

APR-246 (PRIMAMET) Restores Wild-type p53 Function
• Most TP53 gene mutations are single AA missense mutations in the DNA-binding domain
• APR-246 covalently binds to cysteines in mutant p53 or p63
• Reconstitutes WT conformation & function in mutant proteins by stabilizing protein folding
• Intrinsic & additive in vitro schedule-dependent cytotoxicity with azacitidine
Khoo et al., Nature Reviews Drug Discovery; 2014, 13, 217-36 .

Study Design
• TP53 mutant (mTP53) HMA naïve MDS and AML (≤ 30% blasts)

Treatment Duration and Response

The First-in-Class Anti-CD47 Antibody Hu5F9-G4 is Well Tolerated and Active Alone or with
Azacitidine in AML and MDS Patients: Initial Phase 1b Results
David A Sallman1, William Donnellan2, Adam Asch3, Daniel Lee4, Monzr Al Malki5, Guido Marcucci5, Daniel Pollyea6, Suman Kambhampati7, Rami Komrokji1, Joanna Van Elk8, Ming Lin8, James Y Chen8, Jens-Peter Volkmer8, Chris Takimoto8, Mark
Chao8, Paresh Vyas9
1Moffitt Cancer Center, Tampa, FL; 2Sarah Cannon Research Institute, Nashville, TN; 3University of Oklahoma, Oklahoma City, OK, City of Hope, Duarte, CA;
4Columbia University, New York, NY; 5City of Hope, Duarte, CA; 6University of Colorado, Denver, CO; 7Healthcare Midwest, Kansas City, MO;
8Forty Seven, Inc., Menlo Park, CA; 9University of Oxford, Oxford, UK

CONFIDENTIAL
Targeting Macrophages Leverages the Innate Immune System in the Fight Against Cancer
o CD47 is a “do not eat me” signal on cancers that enables macrophage immune evasion
o CD47 is the dominant macrophage checkpoint overexpressed on most cancers
o Increased CD47 expression predicts worse prognosis in AML patients
o 5F9 is a First-in-class Macrophage Immune Checkpoint Inhibitor Targeting CD47
o 5F9 Synergizes with Azacitidine to Induce Remissions in AML Xenograft Models
Majeti, Chao et al., Cell 2009
AML Patients
Macrophages are a key part of the innate immune
system serving as first responder cells:
o Phagocytose cells displaying abnormal “eat me” signals,
including cancer cells
o Recruit, activate, and present cancer cell antigens to T cells

CONFIDENTIAL
5F9005 Study Design: 5F9 Alone or in Combination with Azacitidine in AML
and MDS
o A 5F9 priming dose (1 mg/kg) and dose ramp up was utilized to mitigate on target
anemia
o 5F9 monotherapy safety was confirmed in r/r AML/MDS patients prior to
5F9+AZA combination
Relapsed/
refractory (r/r)
AML or MDS
5F9: 1, 30
mg/kg* twice
weekly
5F9: 1, 30
mg/kg* weekly
AZA: 75 mg/m2
D1-7
5F9 Monotherapy
Safety Run-in Cohort (N=10) 1) Safety of 5F9 alone or with AZA
2) Efficacy of 5F9 in r/r AML/MDS
and 5F9+AZA in untreated
AML/MDS
1) PK, PD and immunogenicity of 5F9
2) Additional measures of efficacy
(DOR, PFS, OS)
Primary objectives
Secondary objectives
1) To assess CD47 receptor
occupancy, markers of immune
cell activity, and molecular
profiling in AML/MDS
Exploratory objectives
Untreated AML
ineligible for
induction
chemotherapy
or untreated
MDS
intermediate to
very high risk
by IPSS-R
5F9 + AZA Combo
Safety Evaluation (N=6) Expansion (N=30)
5F9: 1, 30
mg/kg* weekly
AZA: 75 mg/m2
D1-7
*Dose ramp up from 1 to 30 mg/kg by week 2,then 30 mg/kg maintenance dosing

CONFIDENTIAL 26
Anti-Leukemic Activity is Observed with 5F9 Monotherapy and in Combination with AZA in AML and MDS
Response assessments per 2017 AML ELN criteria and 2006 IWG MDS criteria; Patients with at least one
post-treatment response assessment are shown
“-” not applicable
2 patients not shown due to missing
values
<5% blasts imputed as 2.5%
Best Overall
Response
R/R
AML/MD
5F9
mono
N=10
1L
AML
5F9+AZA
N=14
1L
MDS
5F9+AZA
N=11
ORR 1 (10%) 9 (64%) 11 (100%)
CR 0 5 (36%) 6 (55%)
CRi 0 2 (14%) -
PR 0 0 0
MLFS/
marrow CR1 (10%) 2 (14%)
4 (36%)
2 with
marrow
CR+HI
Hematologic
improvement
(HI)
- - 1 (9%)
SD 7 (70%) 5 (36%) 0
PD 2 (20%) 0 0
o 5F9 monotherapy has an ORR of 10% in r/r AML/MDS
o 5F9+AZA has an ORR of 100% in MDS, 64% in AML which compares favorably to AZA monotherapy
o ORR Median time to response is more rapid (1.9 months) than AZA alone
Patient
Be
st R
ela
tive
Ch
ange
fro
m B
ase
line
in
Bo
ne
Mar
row
Bla
st (
%)
5F9+AZA
+ AML patient

CONFIDENTIAL 27CONFIDENTIAL
Parameter 1L AML
N=14
1L MDS
N=11
RBC transfusion
independence9/14 (64%) -
Complete
cytogenetic
response in
responders*
2/7 (29%) 3/7 (43%)
MRD negativity in
responders3/9 (33%) 2/10 (20%)
Median duration of
response (months)
NR
(0.03+ –
8.3+)
NR
(0.5+ –
4.3+)
Median follow-up
[range] (months)
3.8 (1.9 –
10.3)
3.7 (2.5 –
6.8)
Minimal residual disease (MRD) was evaluated by multiparameter flow cytometry
Hematologic improvement (HI-E, HI-P, HI-N) defined per 2006 IWG MDS criteria
Cytogenetic response defined per 2003 and 2006 IWG criteria; NE: not reached
*Cytogenetic responses shown for all responding patients with abnormal
cytogenetics at baseline
“-” not applicable
Deep and Potential Durable Responses Seen in 5F9 + AZA Treated Patients
Time on therapy (months)
Pat
ien
t
5F9+AZA treated patients
*underwent transplant
**
**
*HI
HI
Hematologic
improvement HI
o No responding patient has relapsed or progressed on 5F9 + AZA
o Multiple patients have improved responses over time
o MRD negativity has been observed (time to MRD negativity ranged from 1.7 to 6.1 months)
o 5/20 (25%) of responding patients have successfully received an allogeneic stem cell transplant
o The longest patient in response is in CR 9+ months on therapy and ongoing
HI

CONFIDENTIAL 28
On Target Anemia is a Pharmacodynamic Effect and is Mitigated with a 5F9
Priming and Maintenance Dosing Regimen
Hemoglobin changes on 5F9+AZA therapy in AML/MDS
Ch
ange
in H
em
ogl
ob
in (
g/d
L) f
rom
Bas
elin
e-1
01
23
Baseline
o Aging RBCs can be cleared by CD47
blockade leading to an on target anemia
o A priming dose mitigates on target anemia
through a temporary/mild decline in
hemoglobin by clearing aged RBCs with
reticulocytosis
o Anemia returns to baseline with treatment
with 5F9 even at higher maintenance
doses (30mg/kg)
o A mild hemoglobin drop (mean of 0.5 g/dL)
with the priming dose was observed with
5F9+AZA
o Many patients have had hemoglobin
improvement and decrease in
transfusion frequency while on
5F9+AZA therapy

Primary failure (lack of primary response) 25%
• Clear evidence of disease progression on therapy or death on
treatment
• Median OS 4.7 mo (Rigosertib study), 5.5 mo (MCC database)
Secondary failure ≈ 75%
• Loss of initial response or probably only stable disease after 9 cycles.
• Median OS 6.9 mo (MCC database)
• 25% AML progression at time of failure
Defining HMA failure

Prognostic models after HMA failure
Nazha et al , Hematologica 2016

New HMAAgent mechanism Preliminary resultsCC-486 Oral azacitidine • In phase I study, 41 patients received SC and oral azacitidine. Dose-
limiting toxicity (grade 3/4 diarrhea) occurred at the 600-mg dose and
MTD was 480 mg. Overall response rate was 35% in previously treated
patients and 73% in previously untreated patients.
• In Phase 2, Patients with LR-MDS received 300 mg CC-486 once daily
for 14 days (n=28) or 21 days (n=27) of repeated 28-day cycles. Overall
response was attained by 36% of patients receiving 14-day dosing and
41% receiving 21-day dosing. RBC TI rates were similar with both dosing
schedules (31% and 38%, respectively).
SGI-110 dinucleotide of
decitabine and
deoxyguanosine that
protects it from
deamination
• In a phase I study that included 14 patients with MDSs after HMA failure,
SGI-110 had a 4.5-fold longer half-life than decitabine. An equivalent or
higher area under the curve was reached with lower Cmax compared
with reference levels from intravenous decitabine.
• A dose-dependent increase in demethylation was observed up to 60
mg/m2 daily for 5 days.
• In the phase II part of the study for treatment-naive elderly patients with
AML or refractory/relapsed AML, 43% and 16% remission rates were
reported.
ASTX727 Fixed dose oral cytidine
deaminase inhibitor
E7727 with oral
decitabine
• AEs are consistent with IV decitabine with no GI toxicity.
• ASTX727 is clinically active 33% response rate in phase I, 50% had prior
HMA.
• The fixed oral dose of 30 mg decitabine and 100 mg E7727 results in
decitabine AUC equivalent to 20 mg/m2 IV and will be further studied in a
Phase 2 trial in HMA naïve MDS
Savona et al, ASH 2015, abstract # 1683
Kantarjian HM, et al. ASH 2013. Abstract 497.Garcia Manero et al, J Clin Oncol. 2011 Jun 20; 29(18): 2521–2527
Garcia Manero et al , Leukemia 2016 Apr;30(4):889-96

Response, n/N (%) MDS Pts
(N = 17)
ORR* 10/17 (59)
CR† 1/11 (9)
PR† 1/11 (9)
mCR† 3/11 (27)
Any HI
Erythrocytes
Platelets
Neutrophils
Trilineage
improvement
Bilineage
improvement
5/17 (29)
3/15 (20)
4/12 (33)
4/10 (40)
2/5 (40)
2/5 (40)
Enasidenib in mIDH2 MDS: Response
• 7 of 13 pts (54%)
with prior HMA
responded to
enasidenib
• Median time to
response: 21 days
(range: 10-87)
Stein EM, et al. ASH 2016. Abstract 343.
*CR + PR + mCR + HI.†Investigator-assessed; pts had ≥ 5% BM blasts at BL.

Ivosidenib for mIDH-MDS
• 12 MDS patients demonstrated a 91.7% ORR and a CR rate of 41.7%.
• Among 13 patients progressed to AML after HMA failure CR/CRh (4/13) 33%

Out of the box
• Shifting HMA+Venetoclax or add on Venetoclax (n=19, ORR 47%, 56% proceeded to Allo-SCT) (unpublished data)
• RAS mutations- Trametinib?
• CBL mutations- Dasatinib?

Induction after HMA failure
Talati, et al. ASH 2018.

MDS: Lower risk
Upfront: first line
MCC 19872
“Commands Study”
Luspatercept (ACE-536) vs. ESA for
low risk MDS.
CRC: William Prada
PI: Komrokji
Light Blue: Actively Accruing
Gray: Closed to Accrual
Yellow: Long-Term Follow-Up
Purple: Pending
Green: Final Closed
Future considered
2nd line after ESA failure
MCC 18634
IIT: Ph. Ib/II LB-100 for
Low to Int.-1 MDS
Preferred for del 5 q len
failure
CRC: Lisa Nardelli
PI: Komrokji
ESA NaiveMCC 19939
Oral Decitabine
CRC: Willliam Prada
PI: Sallman
MCC 19430
Sponsor: TEW
Phase I/II TEW TGFB inhibitor
for lower risk MDS
CRC: Lisa Nardelli
PI: Dr. Komrokji
HMA candidate
MCC XXXX
Canakinumab/darbepoetin
CRC: TBD
PI: Sallman
MCC XXXX
Luspatercept
CRC: TBD
PI: komrokji
ESA failure
HMA failure
MCC 19658
SX682 for HMA failure
MDS
CRC: William Prada
PI: Sallman

A Phase 1b/2 Study Evaluating the Safety and Efficacy of Canakinumab with Darbepoetin alfa in Patients with Lower-Risk MDS who have Failed ESA
Dose Level Canakinumab (mg) Darbepoetin alpha (µg)
S.C q 4 weeks S.C q 2weeks
-1 75 300
1 (Starting dose) 150 300
2 300 300
Study population• Very low/low/intermediate R-IPSS risk MDS. • Transfusion dependent anemia.• ESA failure or low chance of response in non-del5q.• ESA and lenalidomide failure in del5q.
RP2DStage 1: 10 patients & Stage2: 19 patients
Phase 1b
(n=9-18)
Phase II
(n=29)
Primary end point • MTD & RP2D
Primary end point • HI-IWG 2016 criteria• safety
Correlative studies:• Determine recurrent gene mutations utilizing a targeted next generation sequencing (NGS) myeloid panel at study entry and serially throughout treatment to assess
changes in somatic mutation landscape. Comparison between responding and non-responding patients will be performed using qualitative analyses.
• To characterize in vivo IL-1 inhibition, as determined by inflammatory pathway analysis via serial high sensitivity CRP, un-neutralized IL-1, peripheral blood ASC specks, circulating oxidized mitochondrial DNA, S100A9 and comprehensive cytokine profiling.
• Evaluation of innate immune and pyroptosis biomarker indices including ASC specks by flow cytometry and Il-1, S100A9 and oxidized mitochondrial DNA by ELISA in PB plasma; ASC speck immunofluorescence on mononuclear cells by flow cytometry. In BM will evaluate changes in MDSC number by flow cytometry, colony forming capacity (CFC) and pyroptosis biomarkers.
PI: David Sallman

LB100: PP2A inhibitor

MDS: Higher risk
Upfront: first line
Light Blue: Actively Accruing
Gray: Closed to Accrual
Yellow: Long-Term Follow-Up
Purple: Pending
Green: Final Closed
Future considered
2nd line after standard therapy
MCC 19322
Ph. II Azacitidine and anti-CD47
monoclonal antibody
CRC: Yainet Sanchez
PI: Sallman
MCC xxxx
Phase III Azacitidine/Tim- MCC 19862
PRGN-3006 CD33 CART
CRC: ICEPI: Sallman
MCC 20039
NKG2D CAR-T
CRC: ICE
PI: Sallman
Immune Therapy
MCC 19825
IIT: MDS consortium
Phase III: Azactidine +/- APR
246 for p53 mutated MDS/AML
CRC: lisa Nardelli
PI Sallman
MCC 20061
Phase II: CPX-351 for HR-MDS
CRC: William Prada
PI Sallman
MCC 19658
SX682 for HMA failure MDS
CRC: William Prada
PI: Sallman