Embed Size (px)
Citation preview

Companion animal praCtiCe
444 In Practice October 2010 | Volume 32 | 444–452
Mycobacterial infections in cats and dogs
Danièlle Gunn-moore, rachel Dean and Susan Shaw
doi:10.1136/inp.c5313
Mycobacterial infections are not commonly recognised in cats and dogs in the UK. However, with improved recognition they are now being diagnosed more frequently, at least in cats. This article discusses the causes of infection, possible clinical signs and methods of diagnosis, and considers the complexities of treatment and potential therapeutic options. It also outlines the prospects for prognosis.
Q. Which mycobacteria can cause disease in cats and dogs?
TuberculosisTuberculosis is caused by members of the tuberculosis complex: Mycobacterium tuberculosis, Mycobacterium bovis and Mycobacterium microti (this was previously, erroneously, termed M microti-like and is also known as ‘vole bacillus’). Although Mycobacterium avium is a member of the Mycobacterium avium-intracellulare complex (MAC) and a slow-growing saprophyte, it is sometimes considered with these bacteria as it can result in disease indistinguishable from that caused by members of this group.
Tuberculosis is now recognised infrequently in cats and dogs in the UK. When seen, it is usually caused by M microti or M bovis. Of the 159 cases of mycobac-terial infection in cats that have been confirmed on culture by the Veterinary Laboratories Agency (VLA) over a four-year period to December 2008 in the UK, 40 per cent were caused by M microti, 33 per cent by M bovis and 15 per cent by MAC. Dogs are less resist-ant to M tuberculosis than cats but infection with this species of mycobacteria is rare – only five cases of tuberculosis have been confirmed by the VLA in dogs in the past 20 years, all of which were due to M bovis.
Feline leprosyFeline leprosy syndrome classically describes mycobac-terial infections in cats with single or multiple cutane-ous or subcutaneous granulomas, where the bacteria cannot be cultured using traditional techniques. In these cases, infection with Mycobacterium lepraemurium was largely assumed. However, in Australia, feline leprosy takes two forms:
One that is caused by ■■ M lepraemurium in younger cats; Another form that is caused by a novel undefined ■■
mycobacterium in older cats.As molecular techniques have become more avail-
able, a number of other mycobacteria have also been found to cause feline leprosy: Mycobacterium szulgai, Mycobacterium kansasii, Mycobacterium malmoense, Mycobacterium visibilis and Mycobacterium species strain Tarwin. This makes the differentiation between feline leprosy and cutaneous non-tuberculous mycobac-teria (NTM) difficult. It would be better to classify all cases of single or multiple cutaneous or subcutaneous granulomas as feline leprosy, regardless of whether the species of mycobacteria can be identified.
Non-tuberculous mycobacteriaAn increasing number of usually saprophytic bacteria are being found in cats and dogs, particularly in cases of feline skin disease. This is partly due to an improved understanding of ‘fight and bite site’ lesions (ie, those on the face and legs – areas that are most likely to be bitten by small mammals) and access to molecular diagnostics.
NTM found in cats include fast-growing Mycobacterium fortuitum, Mycobacterium smegmatis, the
Danièlle Gunn-Moore graduated from Edinburgh in 1991. She is currently professor of feline medicine and head of companion animal sciences at Edinburgh. She holds a PhD for studies on the molecular epidemiology of feline coronavirus infection.
Rachel Dean graduated from Glasgow in 1996. She is currently a clinical associate professor in feline medicine at Nottingham where she is director of the Centre of Evidence-Based Veterinary Medicine. She holds a PhD for studies on the epidemiology of feline injection site sarcomas in the UK, and is a recognised RCVS specialist in feline medicine.
Susan Shaw graduated from the University of Sydney, Australia, in 1974. She is currently a senior lecturer at Bristol and is head of the university’s Acarus Unit, which investigates arthropod-borne infections in companion animals.
Classification of mycobacteria
Mycobacteria of veterinary importance may be divided into:
Obligate pathogens (eg, the tuberculosis complex)■■
Mycobacteria that are difficult to culture so their ■■
environmental niche cannot be determined (eg, feline leprosy and canine leproid granuloma syndrome – the latter has not been recognised in the UK and so is not discussed in this article);Facultatively pathogenic saprophytes that can ■■
be divided into fast-growing and slow-growing opportunistic non-tuberculous mycobacteria (NTM). As molecular techniques develop, the number of
mycobacterial species found to infect cats and dogs will increase, and classification of the diseases they cause may need to be altered.
444-452 Mycobacteria.indd 444 30/9/10 12:41:15
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from
Companion animal praCtiCe
445In Practice October 2010 | Volume 32 | 444–452
Myco bacterium peregrinum group, Mycobacterium chelonaeabscessus, Mycobacterium goodii, Myco bacterium phlei, Mycobacterium thermoresistible, Mycobacterium flavescens, Mycobacterium alvei, Mycobacterium septicum and Mycobacterium mucogenicum, and slow-growing Mycobacterium genavense, Myco bacterium simiae, Mycobacterium xenopi, M malmoense, M visibilis, M szulgai, Mycobacterium ulcerans and Mycobacterium terrae. Infections have been seen in many countries, including the UK and mainland Europe, the USA, Canada, Australia and New Zealand. NTM infections are rarely seen in dogs, but cases with M fortuitum, Mycobacterium chelonae, M smegmatis and M genavense have been reported.
Q. How do dogs and cats become infected?
TuberculosisTuberculosis in cats and dogs may be transmitted via the inhalation or ingestion of infectious particles, or by direct penetration of the skin. The epidemiology in cats is not fully understood, but is thought to occur by:
Direct spread from wild rodents. Most cases of ■■
tuberculosis in cats present as cutaneous lesions, typically affecting fight and bite sites. Studies in the UK have shown that wild field and bank voles and wood mice may be infected with M microti and an even wider range of wild mammals can be infected with M bovis, including species that cats predate (eg, field and bank voles, common shrews and wood mice). The M bovis strains identified in these ani-mals are typically the same as those found in cattle and badgers from the same area. Since a risk factor for feline tuberculosis is hunting rodents, it is likely that this is how most cats become infected;Direct infection from cattle or badgers. Infection ■■
could possibly follow heavy environmental con-tamination (eg, by badgers visiting the garden).
Feline leprosy and non-tuberculous mycobacteriaFeline leprosy is believed to arise from contaminated rodent bites, and may possibly occur secondarily to soil or plant contamination of cutaneous wounds. NTM are typically found in soil, water and decaying vegeta-tion, so infection is thought to be secondary to wound contamination, particularly involving adipose tissue.
Q. How common are mycobacteria infections?
The overall prevalence of mycobacterial infections within the UK is unknown. However, they are reported only rarely. They are seen more frequently in cats than dogs, with most cases presenting with skin lesions. Data from the VLA shows that, of the 339 feline samples with histopathological changes indicative of mycobacterial infection received in the four years up to December 2008, 19 per cent were M microti, 15 per cent M bovis, 7 per cent M avium, 1 per cent M malmoense, 1 per cent M fortuitum and 4 per cent were unclassified. The samples failed to grow in 53 per cent of patients, partly
because the culture system is optimised for M bovis, but also because these organisms are difficult to grow.
Q. What predisposes animals to infection?
TuberculosisTuberculosis is seen mainly in adults, although MAC can also cause disease in younger animals. No gender predisposition is seen in dogs, but male cats are over-represented. There is little evidence of immunosuppres-sion except with MAC infections, which also appear to be more common in certain breeds such as Siamese and Abyssinian cats, and, possibly, bassett hounds and miniature schnauzers. M bovis in cats tends to be seen in areas where infection is endemic in cattle and the local wild mammal population, while M microti has been seen more in south-east England.
Feline leprosyThere are no breed or gender predispositions for feline leprosy, but adult cats are more frequently affected. Disease is more common in temperate maritime cli-mates (eg, Australia, New Zealand, Europe, western Canada and the USA), and usually presents in win-ter. Concurrent infection with feline leukaemia virus (FeLV) or feline immunodeficiency virus (FIV) is not a consistent feature.
Non-tuberculous mycobacteriaCats appear to be at a greater risk than dogs of becom-ing infected with NTM. Adult animals with hunting or fighting lifestyles are most commonly affected. Immunosuppression has only been found in a small number of cases. Pyogranulomatous panniculitis typi-cally occurs in overweight cases, and is seen more fre-quently in coastal temperate to subtropical climates.
Q. What are the zoonotic risks?
All members of the tuberculosis complex and some NTM pose potential zoonotic risks. However, there have been no recently documented cases of cats or dogs infecting humans. Humans with M bovis (and M tuberculosis) can infect cats and dogs. While there is no zoonotic potential known for feline leprosy and most of the mycobacteria involved in NTM, ongoing advances in molecular diagnostics may demonstrate this for some organisms.
Q. What are the clinical signs of infection?
Currently, most cases of mycobacterial infection in pets in the UK involve skin lesions in cats, which are typically cutaneous nodules, sometimes with draining tracts and/or ulceration. Some of these may spread to show more generalised signs, but only occasional cases present with primary systemic disease. If seen, systemic disease is likely to be due to infection with MAC or a member of the tuberculosis group; patients with NTM have been seen to progress to systemic disease but this is rare.
444-452 Mycobacteria.indd 445 30/9/10 12:41:15
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from
Companion animal praCtiCe
446 In Practice October 2010 | Volume 32 | 444–452
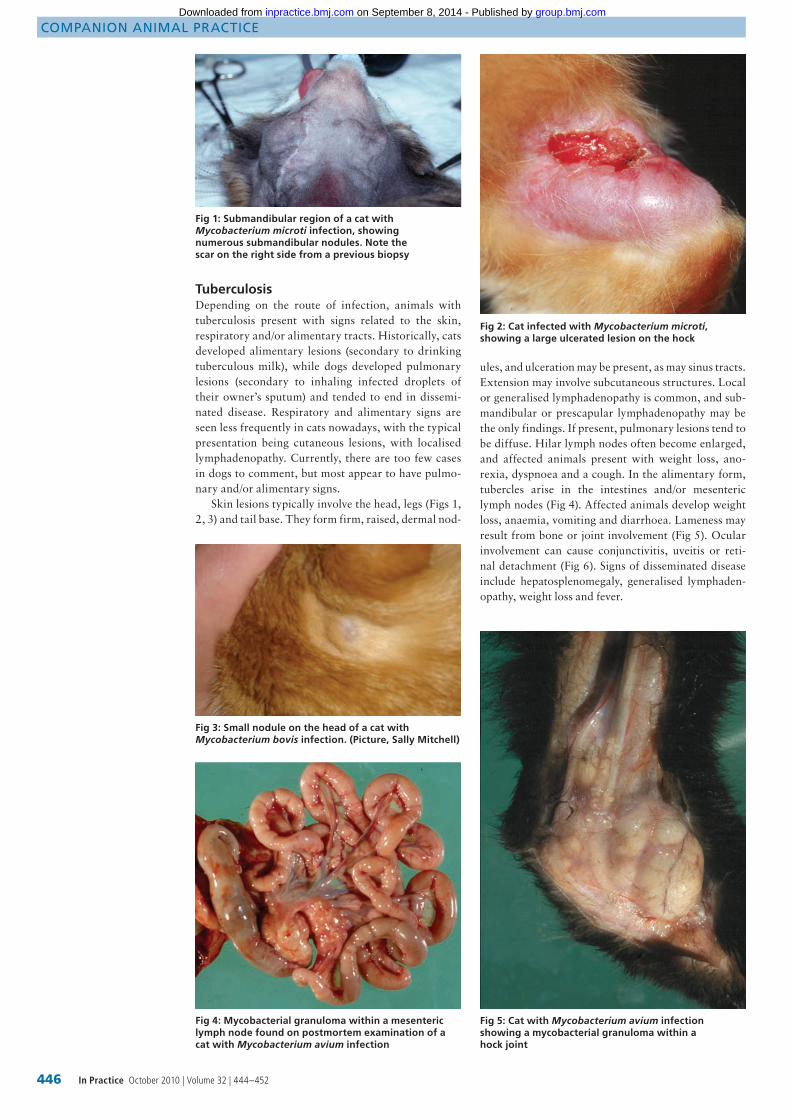
TuberculosisDepending on the route of infection, animals with tuberculosis present with signs related to the skin, respiratory and/or alimentary tracts. Historically, cats developed alimentary lesions (secondary to drinking tuberculous milk), while dogs developed pulmonary lesions (secondary to inhaling infected droplets of their owner’s sputum) and tended to end in dissemi-nated disease. Respiratory and alimentary signs are seen less frequently in cats nowadays, with the typical presentation being cutaneous lesions, with localised lymphadenopathy. Currently, there are too few cases in dogs to comment, but most appear to have pulmo-nary and/or alimentary signs.
Skin lesions typically involve the head, legs (Figs 1, 2, 3) and tail base. They form firm, raised, dermal nod-
ules, and ulceration may be present, as may sinus tracts. Extension may involve subcutaneous structures. Local or generalised lymphadenopathy is common, and sub-mandibular or prescapular lymphadenopathy may be the only findings. If present, pulmonary lesions tend to be diffuse. Hilar lymph nodes often become enlarged, and affected animals present with weight loss, ano-rexia, dyspnoea and a cough. In the alimentary form, tubercles arise in the intestines and/or mesenteric lymph nodes (Fig 4). Affected animals develop weight loss, anaemia, vomiting and diarrhoea. Lameness may result from bone or joint involvement (Fig 5). Ocular involvement can cause conjunctivitis, uveitis or reti-nal detachment (Fig 6). Signs of disseminated disease include hepatosplenomegaly, generalised lymphaden-opathy, weight loss and fever.
Fig 1: Submandibular region of a cat with Mycobacterium microti infection, showing numerous submandibular nodules. Note the scar on the right side from a previous biopsy
Fig 2: Cat infected with Mycobacterium microti, showing a large ulcerated lesion on the hock
Fig 3: Small nodule on the head of a cat with Mycobacterium bovis infection. (Picture, Sally Mitchell)
Fig 4: Mycobacterial granuloma within a mesenteric lymph node found on postmortem examination of a cat with Mycobacterium avium infection
Fig 5: Cat with Mycobacterium avium infection showing a mycobacterial granuloma within a hock joint
444-452 Mycobacteria.indd 446 30/9/10 12:41:19
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from
Companion animal praCtiCe
447In Practice October 2010 | Volume 32 | 444–452
MAC infections in cats have been associated with cutaneous lesions, peripheral vestibular disease, general-ised lymph node and pulmonary involvement, gastroin-testinal disease, intracranial infection and disseminated tuberculosis. In dogs, they most commonly cause dis-seminated tuberculosis, which presents as chronic leth-argy, vomiting, diarrhoea, lameness and collapse.
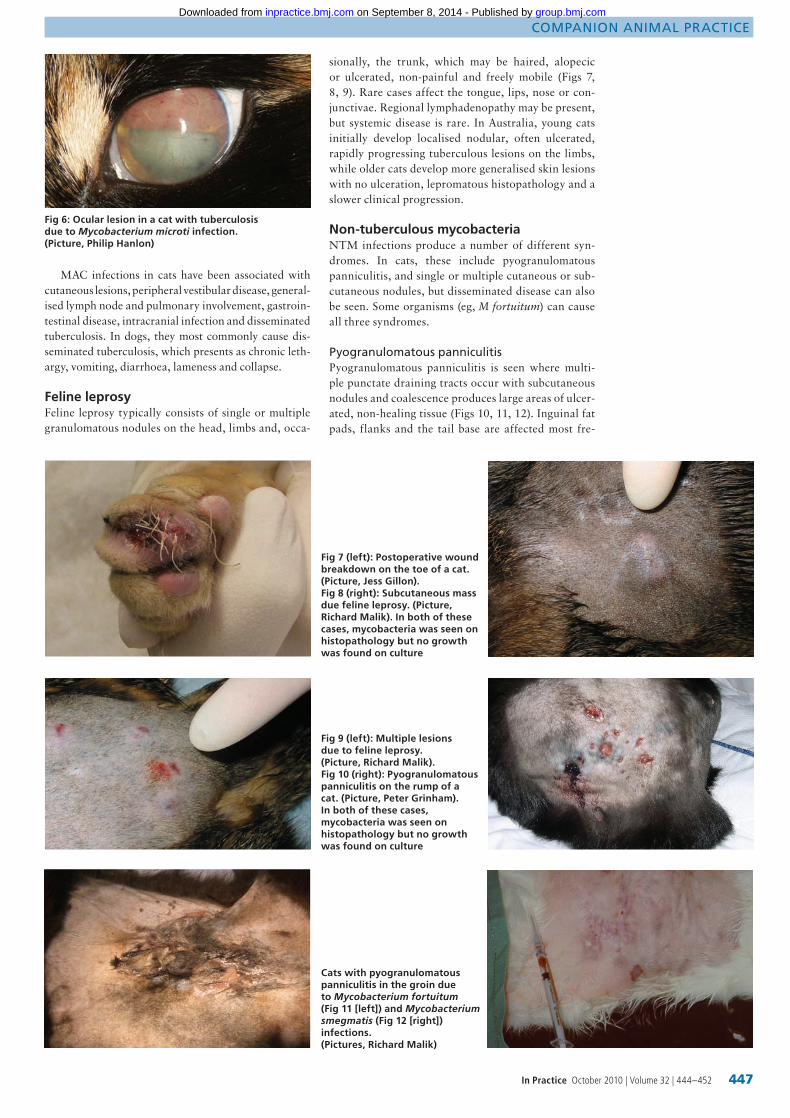
Feline leprosyFeline leprosy typically consists of single or multiple granulomatous nodules on the head, limbs and, occa-
sionally, the trunk, which may be haired, alopecic or ulcerated, non-painful and freely mobile (Figs 7, 8, 9). Rare cases affect the tongue, lips, nose or con-junctivae. Regional lymphadenopathy may be present, but systemic disease is rare. In Australia, young cats initially develop localised nodular, often ulcerated, rapidly progressing tuberculous lesions on the limbs, while older cats develop more generalised skin lesions with no ulceration, lepromatous histopathology and a slower clinical progression.
Non-tuberculous mycobacteriaNTM infections produce a number of different syn-dromes. In cats, these include pyogranulomatous panniculitis, and single or multiple cutaneous or sub-cutaneous nodules, but disseminated disease can also be seen. Some organisms (eg, M fortuitum) can cause all three syndromes.
pyogranulomatous panniculitisPyogranulomatous panniculitis is seen where multi-ple punctate draining tracts occur with subcutaneous nodules and coalescence produces large areas of ulcer-ated, non-healing tissue (Figs 10, 11, 12). Inguinal fat pads, flanks and the tail base are affected most fre-
Fig 6: Ocular lesion in a cat with tuberculosis due to Mycobacterium microti infection. (Picture, Philip Hanlon)
Fig 7 (left): Postoperative wound breakdown on the toe of a cat. (Picture, Jess Gillon). Fig 8 (right): Subcutaneous mass due feline leprosy. (Picture, Richard Malik). In both of these cases, mycobacteria was seen on histopathology but no growth was found on culture
Fig 9 (left): Multiple lesions due to feline leprosy. (Picture, Richard Malik). Fig 10 (right): Pyogranulomatous panniculitis on the rump of a cat. (Picture, Peter Grinham). In both of these cases, mycobacteria was seen on histopathology but no growth was found on culture
Cats with pyogranulomatous panniculitis in the groin due to Mycobacterium fortuitum (Fig 11 [left]) and Mycobacterium smegmatis (Fig 12 [right]) infections. (Pictures, Richard Malik)
444-452 Mycobacteria.indd 447 30/9/10 12:41:29
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from
Companion animal praCtiCe
448 In Practice October 2010 | Volume 32 | 444–452
quently. Although systemic spread is rare, affected cats may show fever, anorexia and a reluctance to move, and affected areas can be painful. Organisms asso-ciated with pyogranulomatous panniculitis include fast-growing M fortuitum, M smegmatis, M chelonae, M phlei, M alvei and M thermoresistible and, occasion-ally, slow-growing M xenopi and M ulcerans.
Cutaneous or subcutaneous nodulesSingle or multiple cutaneous or subcutaneous nod-ules with or without ulceration may look like feline leprosy. Organisms involved in this syndrome include fast-growing M fortuitum, M chelonae, M smegmatis and M phlei, and slow-growing M xenopi, M ulcerans, M simiae and M visibilis. While the definition of feline leprosy was previously reserved for similar cutaneous infections (but where the bacteria could not be grown), it is now starting to be used to describe this clinical presentation in general, regardless of whether or not a causal organism can be identified; this presentation can therefore be considered as a form of feline leprosy.
Disseminated diseaseRarer clinical presentations include cases of primary pulmonary infection with M fortuitum or M thermoresistible, tracheal granuloma with an organism similar to M xenopi, cutaneous, ocular, lymph node and pul-monary involvement with M visibilis and M simiae, and lymphadenitis and peritonitis with M xenopi. M avium should really be discussed here, rather than with tuberculous, as it is a slow-growing saprophyte not an obligate pathogen.
Similar clinical entities have also been seen in dogs, but are rare. These include panniculitis, multiple subcu-taneous abscesses and non-painful, non-pruritic cuta-
neous masses, with or without ulceration and drainage (due to M fortuitum, M smegmatis and M chelonae- abscessus), M fortuitum-contaminated surgical wounds, hindlimb weakness and ataxia (due to M genavense infection), pneumonia (as a result of M fortuitum and M chelonaeabscessus infection) and disseminated disease (due to M smegmatis infection).
Q. How are mycobacterial infections diagnosed?
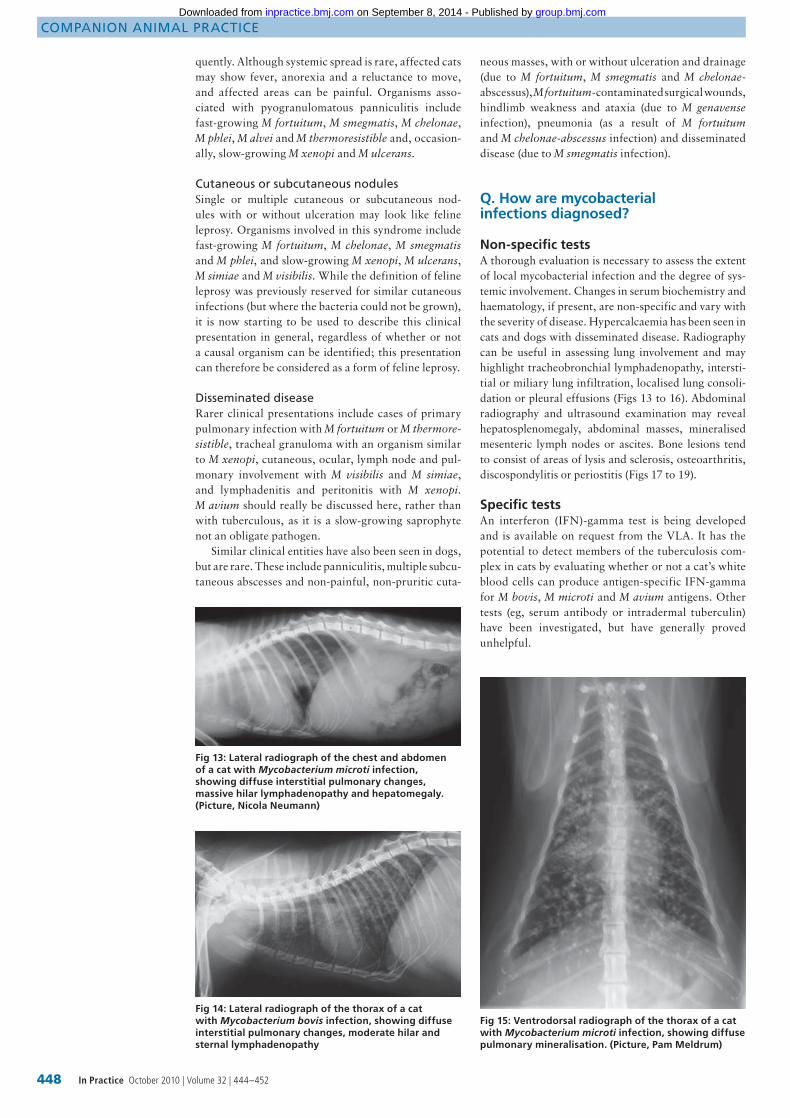
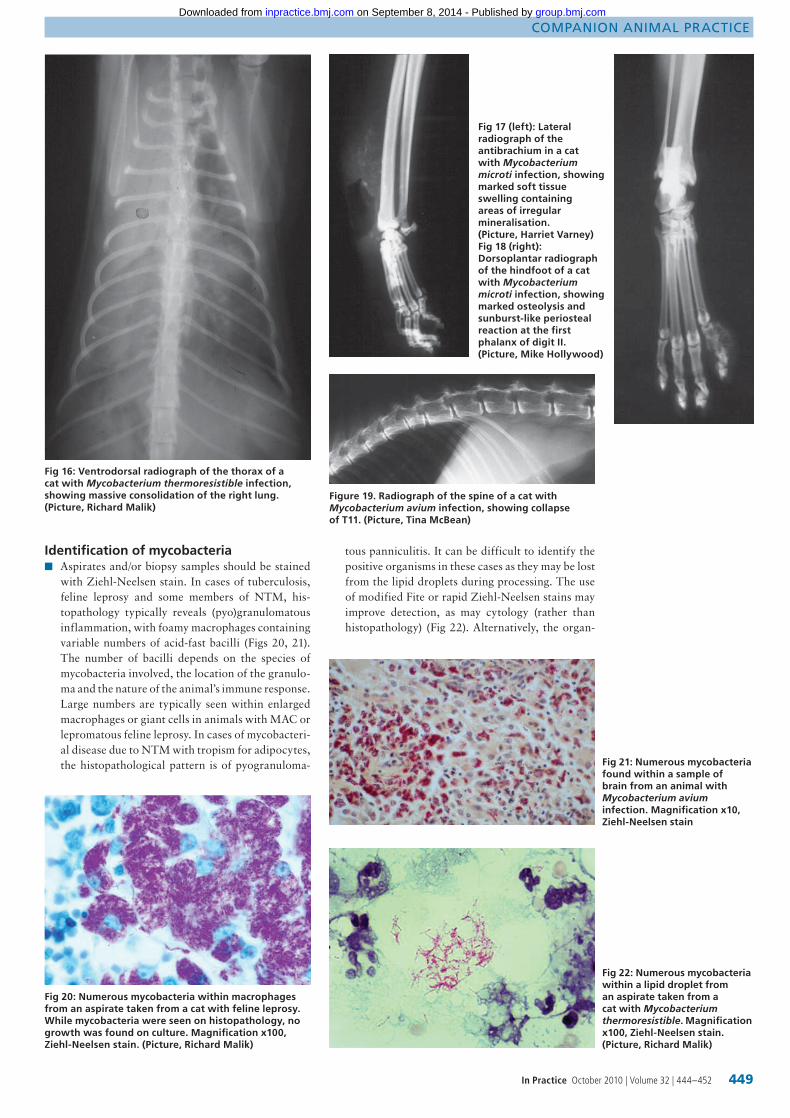
Non-specific testsA thorough evaluation is necessary to assess the extent of local mycobacterial infection and the degree of sys-temic involvement. Changes in serum biochemistry and haematology, if present, are non-specific and vary with the severity of disease. Hypercalcaemia has been seen in cats and dogs with disseminated disease. Radiography can be useful in assessing lung involvement and may highlight tracheobronchial lymphadenopathy, intersti-tial or miliary lung infiltration, localised lung consoli-dation or pleural effusions (Figs 13 to 16). Abdominal radiography and ultrasound examination may reveal hepatosplenomegaly, abdominal masses, mineralised mesenteric lymph nodes or ascites. Bone lesions tend to consist of areas of lysis and sclerosis, osteoarthritis, discospondylitis or periostitis (Figs 17 to 19).
Specific testsAn interferon (IFN)-gamma test is being developed and is available on request from the VLA. It has the potential to detect members of the tuberculosis com-plex in cats by evaluating whether or not a cat’s white blood cells can produce antigen-specific IFN-gamma for M bovis, M microti and M avium antigens. Other tests (eg, serum antibody or intradermal tuberculin) have been investigated, but have generally proved unhelpful.
Fig 13: Lateral radiograph of the chest and abdomen of a cat with Mycobacterium microti infection, showing diffuse interstitial pulmonary changes, massive hilar lymphadenopathy and hepatomegaly. (Picture, Nicola Neumann)
Fig 14: Lateral radiograph of the thorax of a cat with Mycobacterium bovis infection, showing diffuse interstitial pulmonary changes, moderate hilar and sternal lymphadenopathy
Fig 15: Ventrodorsal radiograph of the thorax of a cat with Mycobacterium microti infection, showing diffuse pulmonary mineralisation. (Picture, Pam Meldrum)
444-452 Mycobacteria.indd 448 30/9/10 12:41:30
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from
Companion animal praCtiCe
449In Practice October 2010 | Volume 32 | 444–452
Identification of mycobacteriaAspirates and/or biopsy samples should be stained ■■
with Ziehl-Neelsen stain. In cases of tuberculosis, feline leprosy and some members of NTM, his-topathology typically reveals (pyo)granulomatous inflammation, with foamy macrophages containing variable numbers of acid-fast bacilli (Figs 20, 21). The number of bacilli depends on the species of mycobacteria involved, the location of the granulo-ma and the nature of the animal’s immune response. Large numbers are typically seen within enlarged macrophages or giant cells in animals with MAC or lepromatous feline leprosy. In cases of mycobacteri-al disease due to NTM with tropism for adipocytes, the histopathological pattern is of pyogranuloma-
Fig 16: Ventrodorsal radiograph of the thorax of a cat with Mycobacterium thermoresistible infection, showing massive consolidation of the right lung. (Picture, Richard Malik)
Figure 19. Radiograph of the spine of a cat with Mycobacterium avium infection, showing collapse of T11. (Picture, Tina McBean)
Fig 17 (left): Lateral radiograph of the antibrachium in a cat with Mycobacterium microti infection, showing marked soft tissue swelling containing areas of irregular mineralisation. (Picture, Harriet Varney)Fig 18 (right): Dorsoplantar radiograph of the hindfoot of a cat with Mycobacterium microti infection, showing marked osteolysis and sunburst-like periosteal reaction at the first phalanx of digit II. (Picture, Mike Hollywood)
Fig 21: Numerous mycobacteria found within a sample of brain from an animal with Mycobacterium avium infection. Magnification x10, Ziehl-Neelsen stain
Fig 20: Numerous mycobacteria within macrophages from an aspirate taken from a cat with feline leprosy. While mycobacteria were seen on histopathology, no growth was found on culture. Magnification x100, Ziehl-Neelsen stain. (Picture, Richard Malik)
Fig 22: Numerous mycobacteria within a lipid droplet from an aspirate taken from a cat with Mycobacterium thermoresistible. Magnification x100, Ziehl-Neelsen stain. (Picture, Richard Malik)
tous panniculitis. It can be difficult to identify the positive organisms in these cases as they may be lost from the lipid droplets during processing. The use of modified Fite or rapid Ziehl-Neelsen stains may improve detection, as may cytology (rather than histopathology) (Fig 22). Alternatively, the organ-
444-452 Mycobacteria.indd 449 30/9/10 12:41:33
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

Companion animal praCtiCe
450 In Practice October 2010 | Volume 32 | 444–452
isms can be seen more readily using Romanowsky-stained cytology samples, which typically reveal large numbers of negatively-stained bundles of mycobacteria (Fig 23). The same stains can be used to reveal similar negatively-stained bundles of mycobacteria within macrophages and giant cells with MAC or lepromatous feline leprosy.Specialist culture is needed to determine which ■■
mycobacterial species are involved. Once identi-fied, it is possible to evaluate zoonotic risk, poten-tial sources of infection and feasible treatment options. However, many samples that contain acid-fast bacilli are negative even after extended culture (eg, M leprimurium) and some species require two (M bovis) or three months (M microti) to grow. Molecular techniques, such as PCR, can be used ■■
to identify mycobacteria, but are expensive, can currently only detect a small number of different mycobacteria and have limited availability. These tests can sometimes detect mycobacteria in fixed tissue and/or where there are few Ziehl-Neelsen-positive bacteria in the sample; however, positive identification is most likely when using fresh tis-sue and where there are numerous Ziehl-Neelsen-positive bacteria within the sample.
Correct handling of biopsy materialIn practice, when diagnostic material is taken, mycobac-terial disease is only one of the possible differential diag-noses. However, in suspect cases, particular attention should be paid to appropriate biosecurity procedures. Whenever handling potentially tuberculous material it is necessary to take precautions – wear gloves and use routine aseptic practices when handling the biopsy
sample and the biopsy site. Until the organism is defin-itively identified, it should be considered a potential human pathogen.
Multiple punch biopsies or an excisional biopsy can be used as long as there is adequate biopsy mate-rial and special stains (formalin-fixed) for histopa-thology and microbial culture. After collecting the biopsy sample(s), cut them into three or four pieces, fix one in formalin for histopathological examina-tion and Ziehl-Neelsen staining and, pending results, place two in a sterile container and freeze them (Fig 24). Where other infections are suspected, the fourth sample should be placed on saline soaked gauze and sent unfixed for routine bacterial/fungal culture (and Ziehl-Neelsen staining). If the sample is found to have Ziehl-Neelsen-positive organisms, one of the frozen pieces can be sent for specialist culture (at the VLA and/or a mycobacterial reference laboratory). The last sample should be kept in case further investigation is needed. This is advisable for all enlarged lymph nodes and cutaneous/subcutaneous nodules in cats.
Under the Tuberculosis Orders in force in England, Wales and Scotland, the identification of M bovis in clinical or pathological samples taken from any mam-mal (except humans) is notifiable. The Orders impose a duty on any veterinary surgeon who suspects tuber-culosis in a domestic pet to immediately notify the Divisional Veterinary Manager at the local office of Animal Health. Even if a definitive diagnosis of M bovis is not yet available, cases that are Ziehl-Neelsen-positive on biopsy are suspect and must be reported.
Q. Can mycobacterial infections be treated and, if so, how?
Initial considerationsTreating mycobacterial disease in cats or dogs is con-tentious (see Box 1). Before embarking on treatment, a number of points should be considered:
The potential zoonotic risk. The authors do not ■■
advise treatment in animals that live with poten-tially immunosuppressed people, or if animals have generalised disease, significant respiratory involve-ment or extensive draining lesions;M bovis■■ is notifiable. DEFRA must be notified and it can recommend that the pet is euthanased, although it rarely does so;Treatment is long-term and difficult to maintain ■■
given patient non-compliance, drug toxicity and financial costs. Some cases require indefinite treat-
Fig 24: Part of a biopsy sample should always be frozen, so that it is available for culture if histopathology results are suggestive of mycobacterial infection
Box 1: To treat or not to treat?
The treatment regimens discussed in this article are based on published literature and the authors’ personal experience, but there have been no controlled treatment studies for any of these infections in cats or dogs. In addition, there is currently debate within the UK veterinary community about whether:
Infected animals should be treated at all (rather ■■
that they should all be euthanased);Drugs that are needed for treating humans with ■■
mycobacterial infections should be used to treat animals.
Fig 23: Numerous non-stained mycobacteria within
macrophages from an aspirate taken from a cat with feline
leprosy. Mycobacteria was seen on histopathology but no growth was found on culture. Magnification x100, Diff-Quik
stain (Picture, Richard Malik)
444-452 Mycobacteria.indd 450 30/9/10 12:41:36
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

Companion animal praCtiCe
451In Practice October 2010 | Volume 32 | 444–452
ment. Uncomplicated cutaneous disease has the most favourable prognosis;There are no drugs licensed for treating mycobacte-■■
rial infections in cats and dogs;Tailoring treatment is difficult as sensitivity testing ■■
does not always correlate with in vivo results;Surgical excision of small cutaneous lesions may ■■
be considered, but debulking larger lesions risks wound dehiscence and local recurrence.Pending a definitive diagnosis, interim therapy with
a fluoroquinolone has previously been recommended. However, it is better to give double or triple therapy (see later and Table 1), which carries a better chance of clinical resolution and decreases the potential for fluo-roquinolone resistance. Mycobacteria readily develop resistant clones, particularly those of the tubercle group and MAC, which would be detrimental to the animal and could endanger humans.
Specific therapyDeciding on continued treatment may depend on culture results. It is inadvisable to continue treatment when M tuberculosis or disseminated M bovis is con-firmed. Unfortunately, it is often two to three months before results are known and, in many cases, the organ-isms do not grow even though mycobacteria were seen on cytology/histopathology. Counsel owners carefully to make sure they are aware of all the potential risks and complications.
tuberculosisAnti-tuberculosis treatment should consist of initial and continuation phases. The initial phase usually requires
Table 1: Potentially useful drugs for the treatment of feline and canine mycobacterial disease
Uses Drug SpeciesDose (mg/kg)
interval (hours) toxicity
1st line treatment for TB and NTM
Marbofloxacina
Enrofloxacina
Moxifloxacinb
Cats and dogsDogsCats
2 po5 po10 po
242424
Retinal degeneration
1st line treatment for TB, MAC and NTM
Rifampicinb Cats and dogs 10-15 po(maximum 600 mg/day)
24 Hepatotoxicity, induction of liver enzymes, discoloration of body fluids, generalised erythema and pruritus, teratogenic, poor palatability
1st line treatment for TB, leprosy and NTM
Clarithromycinbc
Azithromycinb
Cats and dogs
Cats and dogs
5-15 po
5-15 po
12
24
Pinnal or generalised erythema, possible hepatotoxicityPossible gastrointestinal signs
2nd line treatment for TB
Prophylaxis for TB
Isoniazidb Cats and dogs
Cats and dogs
10-20 po(maximum 300 mg/day)10 po
24
24
Hepatotoxicity, peripheral neuritis, seizures, acute renal failureAs above
2nd line treatment for TB Dihydrostreptomycinb Cats and dogs 15 im 24 Ototoxicity
2nd line treatment for TB Pyrazinamidebd Cats and dogs 15-40 po 24 Hepatotoxicity, gastrointestinal signs
2nd line treatment for TB Ethambutolb Cats and dogs 10-25 po 24 Optic neuritis
Treatment for leprosy, NTM and MAC
Clofazaminebe Cats
Dogs
4-8 (occasionally ~10) po (maximum 25 total)
4-12 po
24
24
Hepatotoxicity, gastrointestinal signs, discoloration of body fluids, photosensitisation, pitting corneal lesions in catsAs above
2nd line treatment for NTM and MAC
DoxycyclineAmikacinb
Cefoxitinb
Cats and dogsCats and dogsCats and dogs
5-10 po10-15 iv, im, sc20-30 iv, im, sc, po
12-24246-8
Gastrointestinal signs, oesophagitisf
Nephrotoxic, ototoxicPain on injection im or sc
See text for information on potential drug combinations and treatment duration. Second line treatments for tuberculosis should be reserved for resistant infections. Drugs licensed for human use can be obtained by veterinary prescription from larger chemists as long as all aspects of the prescribing cascade have been consideredTB Tuberculosis, NTM Non-tuberculous mycobacteria, MAC Mycobacterium avium-intracellulare complex, po Orally, sc Subcutaneously, iv Intravenously, im IntramuscularlyaThe authors recommend using a fluoroquinolone that is not enrofloxacin when treating cats as the latter has been associated with retinal degeneration. Most fluoroquinolones are not effective against MAC infections. bThese drugs are not licensed for use in pets. cParticularly useful when treating MAC infections. dNot effective against M bovis infection. eCan be difficult to obtain. fGive with food or give water after medication to avoid oesophageal injury
two to three drugs and lasts for two months, while the continuation phase requires two drugs and lasts for a further four to six months, depending on the extent of disease. If triple therapy is not feasible, two drugs should be given for a minimum of six to nine months. Fluoroquinolones are useful when treating tuberculo-sis and some NTM, but are usually ineffective against MAC, except possibly some newer drugs such as moxifloxacin. Clarithromycin is useful, especially when given in combination with rifampicin and/or another antibiotic. A once daily alternative to clarithromycin is azithromycin, although it is perhaps not as effec-tive against MAC. Experience over 15 years supports treatment with an initial phase of rifampicin-fluoro-quinolone-clarithromycin/azithromycin, followed by a continuation phase of rifampicin and either a fluo-roquinolone or clarithromycin/azithromycin (Table 1). Rifampicin is often poorly tolerated and may need to be withdrawn early. If the lesions have resolved by this time, treatment should be continued using the two other drugs; if not, add another drug, perhaps doxycycline. For ease of administration, all three once-daily medica-tions can be given as liquids (syringe-mixed before oral administration) or as tablets given in a single gelatine capsule. Alternatively, an oesophagostomy tube can be left in place for the duration of treatment.
MAC responds poorly to treatment. Local cuta-neous lesions may be amenable to surgery and better results are seen with clarithromycin plus either clofaz-imine or rifampicin as first line treatment, with doxy-cycline as second line therapy.
If tuberculosis resistance develops, rifampicin-isoniazid-ethambutol may be considered. If necessary,
444-452 Mycobacteria.indd 451 30/9/10 12:41:36
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

Companion animal praCtiCe
452 In Practice October 2010 | Volume 32 | 444–452
ethambutol can be substituted with dihydrostrepto-mycin or pyrazinamide. However, M bovis is resistant to pyrazinamide. Rifampicin and isoniazid are more effective and less toxic than ethambutol and dihydro-streptomycin.
Feline leprosySurgical removal of small nodules is the treatment of choice and spontaneous regression has been reported. If surgery is not possible, clarithromycin, clofazimine, rifampicin, fluoroquinolones, aminoglycosides and even doxycycline have all been used with variable responses (Table 1). The use of two or three drugs has been recommended (eg, clarithromycin and rifampicin), which are best given for two months beyond apparent clinical resolution. However, the use of antibiotics for the treatment of feline leprosy has been poorly stud-ied and post-treatment outcome information is scarce. Dapsone is toxic in cats.
non-tuberculous mycobacteriaTreatment of NTM is difficult and needs to be tai-lored, ideally following culture and sensitivity testing. Different species have differing sensitivity patterns, which can vary between individual isolates (Table 2). Consider using double or triple therapy as for tuber-culosis (Table 1). Most cases make a significant clini-cal improvement within a month. Antibiotic therapy should be continued for at least one to two months beyond apparent clinical resolution; systemic infec-tions typically need six to 12 months of treatment.
Pyogranulomatous panniculitis requires long-term antibiotics and radical well-planned surgery. This may involve the administration of doxycycline for several weeks, followed by radical surgical excision and local reconstruction plus parenteral gentamicin periopera-tively for three to five days, and a prolonged (three to six months) course of a fluoroquinolone.
Q. What is the prognosis?
Prognosis depends on the type of mycobacteria involved, and the extent and severity of disease. Many cutaneous M microti and M bovis infections have
Table 2: Potentially useful drugs for the treatment of feline and canine non-tuberculous mycobacterial disease
mycobacterial species Generally sensitive to Generally resistant to
Mycobacterium fortuitum
Amikacin (100%), cefoxitin (94%), fluoroquinolones (75%), clarithromycin (75%), clofazimine, gentamicin, doxycycline (29%)
Trimethoprim
Mycobacterium smegmatis
Fluoroquinolones, tetracyclines, gentamicin, trimethoprim
Clarithromycin
Mycobacterium chelonae-abscessus
Amikacin (100%), cefoxitin (94%), ciprofloxacin (75% ), clarithromycin (71%)
Doxycycline
Mycobacterium xenopi Fluoroquinolones, clarithromycin, rifampicin, clofazimine
Mycobacterium simiae Rifampicin, clarithromycin, fluoroquinolones
Mycobacterium thermoresistible
Rifampicin, doxycycline, clarithromycin
Mycobacterium terrae Macrolides, ethambutol
Mycobacterium genavense
Clarithromycin, fluoroquinolones, ethambutol
achieved clinical resolution (even those with pulmo-nary involvement). However, the prognosis for tuber-culosis should always be stated as guarded. While some cases of feline leprosy respond favourably to treatment and some resolve spontaneously, some may be more complicated. The prognosis for NTM is variable, from good in some cutaneous and even disseminated cases, through to poor to guarded for cases with panniculitis if it is not treated aggressively. The prognosis deterio-rates if there have been previous unsuccessful attempts at surgery.
AcknowledgementsThe authors would like to thank everyone who has helped with the cases discussed in this article, par-ticularly for sending in blood samples, photographs, radiographs and case histories.
Further readingBARAL, R. M., METCALFE, S. S., KROCKENBERGER, M. B., CATT, M. J., BARRS, V. R., MCWHIRTER, C., HUTSON, C. A., WIGNEY, D. I., MARTIN, P., CHEN, S. C., MITCHELL, D. H. & MALIK, R. (2006) Disseminated Mycobacterium avium infection in young cats: overrepresentation of Abyssinian cats. Journal of Feline Medicine and Surgery 8, 23-44 BURTHE, S., BENNETT, M., KIPAR, A., LAMBIN, X., SMITH, A., TELFER, S. & BEGON, M. (2008) Tuberculosis (Mycobacterium microti) in wild field vole populations. Parasitology 135, 309-317DELAHAY, R. J., SMITH, G. C., BARLOW, A. M., WALKER, N., HARRIS, A., CLIFTON-HADLEY, R. S. & CHEESEMAN, C. L. (2007) Bovine tuberculosis infection in wild mammals in the south-west region of England: a survey of prevalence and a semi-quantitative assessment of the relative risks to cattle. Veterinary Journal 173, 287-301GREENE, C. E. & GUNN-MOORE, D. A. (2006) Infections with slow-growing mycobacteria. In Infectious Diseases of the Dog and Cat, 3rd edn. Ed C. E. Greene. St Louis, Missouri, Saunders Elsevier. pp 462-477GUNN-MOORE, D. A. (2010) Mycobacterial infections in cats and dogs. In Textbook of Veterinary Internal Medicine, 7th edn. Eds. S. Ettinger and E. Feldman. Philadelphia, W. B. Saunders. pp 875-881HORNE, K. S. & KUNKLE, G. A. (2009) Clinical outcome of cutaneous rapidly growing mycobacterial infections in cats in the south-eastern United States: a review of 10 cases (1996-2006). Journal of Feline Medicine and Surgery 11, 627-632MALIK, R. (2005) Mycobacterial disease of cats and dogs. In Advances in Veterinary Dermatology: Vol 5. Eds A. Hillier, A. Foster and K. Kwocha. Oxford Blackwell Publishing. pp 219-237MALIK, R., SHAW, S. E., GRIFFIN, C., STANLEY, B., BURROWS, A. K., BRYDEN, S. L., TITMARSH, J., STUTSEL, M. J., CARTER, S. A., WARNER, A., MARTIN, P., WIGNEY, D. I. & GILPIN, C. (2004) Infections of the subcutis and skin of dogs caused by rapidly growing mycobacteria. Journal of Small Animal Practice 45, 485-494MALIK, R., HUGHES, M. S., MARTIN, P. & WIGNEY, D. (2006) Feline leprosy syndromes. In Infectious Diseases of the Dog and Cat. Ed C. E. Greene, 3rd edn. St Louis, Missouri, Saunders Elsevier. pp 477-480RHODES, S. G., GRUFFYDD-JONES, T., GUNN-MOORE, D. & JAHANS, K. (2008) Adaptation of IFN-gamma ELISA and ELISPOT tests for feline tuberculosis. Veterinary Immunology Immunopathology 124, 379-384
444-452 Mycobacteria.indd 452 30/9/10 12:41:37
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from
doi: 10.1136/inp.c5313 2010 32: 444-452In Practice
Danièlle Gunn-Moore, Rachel Dean and Susan Shaw Mycobacterial infections in cats and dogs
http://inpractice.bmj.com/content/32/9/444.full.htmlUpdated information and services can be found at:
These include:
References
http://inpractice.bmj.com/content/32/9/444.full.html#related-urlsArticle cited in:
http://inpractice.bmj.com/content/32/9/444.full.html#ref-list-1This article cites 7 articles, 1 of which can be accessed free at:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from