Embed Size (px)
Citation preview
1
next speaker:
Lawrence Ginsberg
Houston/US
My Most Unforgettable Mistakes
Lawrence E. Ginsberg, M.D.Department of Diagnostic Imaging
University of Texas M.D. Anderson Cancer CenterHouston, Texas
Why Do We Miss?� Distracted/Disinterested� Hurried/Harried/Hassled� Satisfaction of search� Didn’t look
�didn’t know where to look�didn’t cover it� just didn’t look
� Looked but didn’t see it� Bias
� referrer issues�scan issues-too soon, wrong modality, etc.�bad attitude
Why Do We Miss?
� Knowledge gap� Ignore bone or brain windows � Saw it but didn’t piece together the puzzle� Inaccurate or incomplete hx
�clinic note not yet generated/transcribed, or patie nt not yet seen
�nothing worse than misleading history. It’s like starting a journey pointed in the wrong direction
�patient hadn’t yet developed or reported the symptom or sign that would direct your attention to the lesion you missed
My Most Unforgettable Mistakes
� Some are so horrible or embarrassing I don’t have the courage to show, but fortunately only have 20 minutes!
� If I simply missed something obvious, what’s the teaching value? Must be more interesting.
� I place great importance on the teaching value of mistakes, and I show mine every Monday morning
Only have 18 minutes.
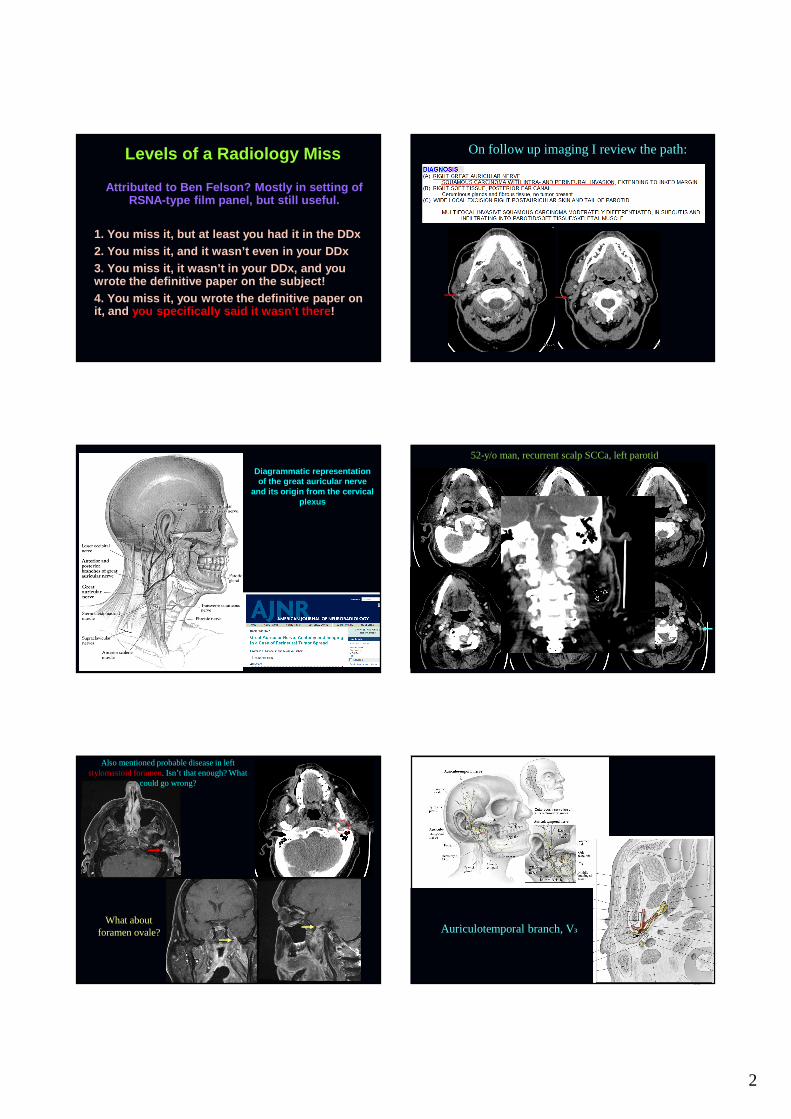
75-y/o man with recurrent skin Ca to right parotid
2
Levels of a Radiology Miss
Attributed to Ben Felson? Mostly in setting of RSNA-type film panel, but still useful.
1. You miss it, but at least you had it in the DDx2. You miss it, and it wasn’t even in your DDx3. You miss it, it wasn’t in your DDx, and you wrote the definitive paper on the subject!4. You miss it, you wrote the definitive paper on it, and you specifically said it wasn’t there !
On follow up imaging I review the path:
Diagrammatic representation of the great auricular nerve
and its origin from the cervical plexus
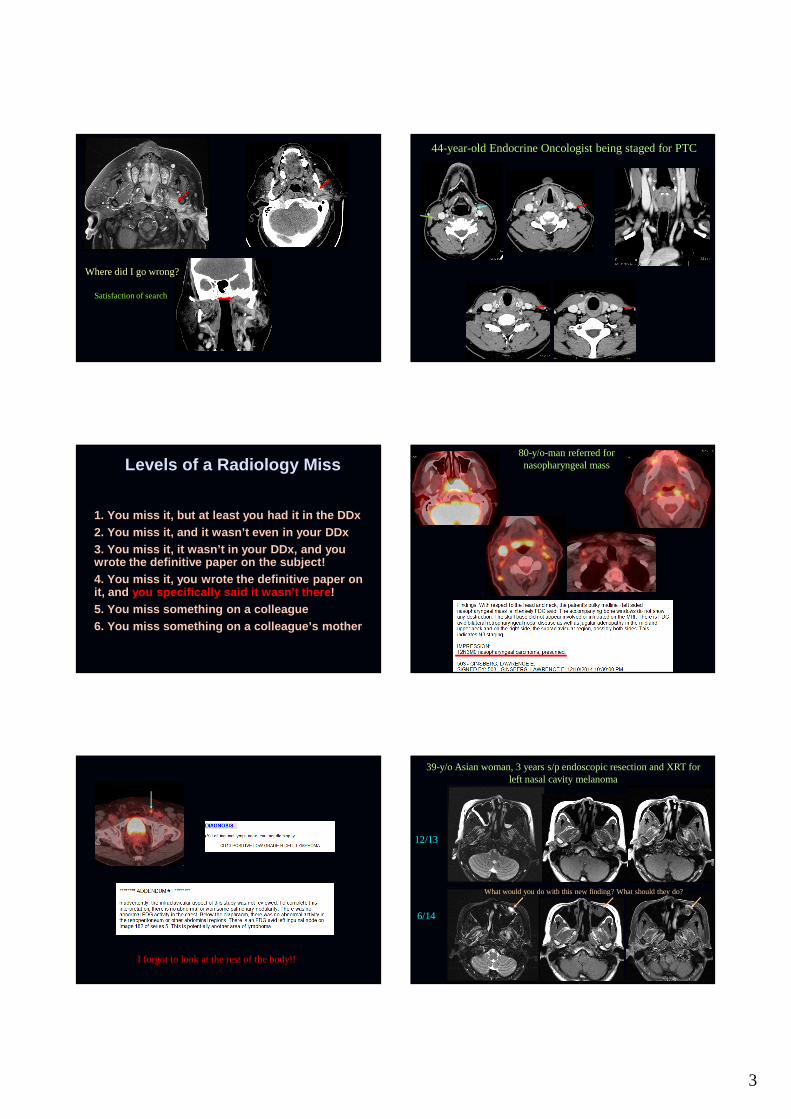
52-y/o man, recurrent scalp SCCa, left parotid
Also mentioned probable disease in left stylomastoid foramen. Isn’t that enough? What
could go wrong?
What aboutforamen ovale? Auriculotemporal branch, V3
3
Where did I go wrong?
Satisfaction of search
44-year-old Endocrine Oncologist being staged for PTC
Levels of a Radiology Miss
1. You miss it, but at least you had it in the DDx2. You miss it, and it wasn’t even in your DDx3. You miss it, it wasn’t in your DDx, and you wrote the definitive paper on the subject!4. You miss it, you wrote the definitive paper on it, and you specifically said it wasn’t there !5. You miss something on a colleague6. You miss something on a colleague’s mother
80-y/o-man referred for nasopharyngeal mass
I forgot to look at the rest of the body!!
39-y/o Asian woman, 3 years s/p endoscopic resection and XRT for left nasal cavity melanoma
12/13
6/14
What would you do with this new finding? What should they do?
4
What would you do with this new finding? What should they do?
“Material in the left maxillary sinus is lobulated, but essentially of mucosal or secretion-type signal, and
the enhancement is that of a mucosal pattern. Obviously careful imaging surveillance is necessary.”
Should I have come down harder?Would a PET/CT have helped?Surgery/Bx?Would survival be better with earlier detection of recurrence?
8/14
Where Did I Go Wrong?
� Well I didn’t do too bad, right?� Did I rush through the case because we’re
under-staffed and the list in +ive flux?
I Know What You’re Thinking
� These aren’t really misses� They’re puff-pieces, designed to show off while
pretending to demonstrate a “miss”� Where’s the real unforgettable misses?
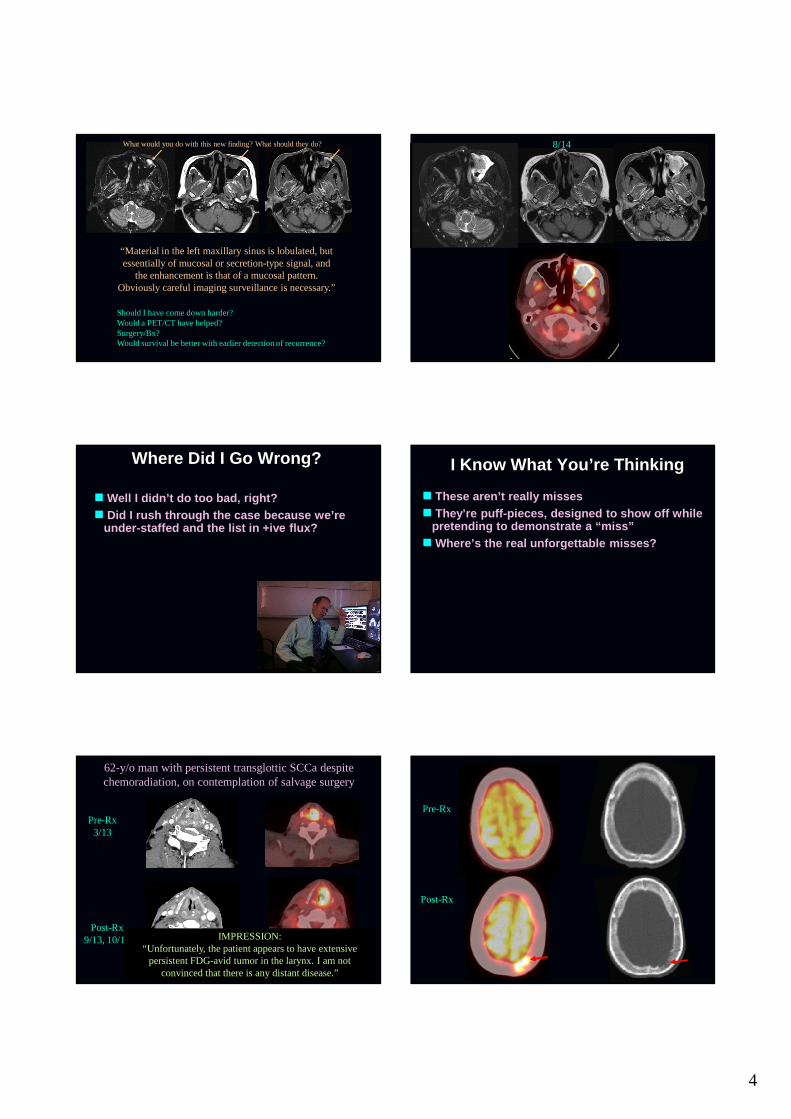
62-y/o man with persistent transglottic SCCa despite chemoradiation, on contemplation of salvage surgery
Pre-Rx3/13
Post-Rx9/13, 10/13
Read as equivocal Certainly easier
IMPRESSION: “Unfortunately, the patient appears to have extensive
persistent FDG-avid tumor in the larynx. I am not convinced that there is any distant disease.”
Pre-Rx
Post-Rx
5
Where Did I Go Wrong?� Pretty clearly I didn’t look at the entire H&N
fused sequence� Post-Rx CT, 9/13 didn’t go to vertex-why should
it? Who expected this?
12/13
Seeing the distant metastasis would have prevented the total laryngopharyngectomy
and free flap, which had rapid distant failure
Another Blunder? 64-y/o woman being staged for PTC.
My impression: “solitary focus of disease in the right mid neck.”
“Elsewhere in the body, there is no abnormal pulmonary nodularity, and no metabolically active distant disease in
the chest, abdomen, or pelvis.”
2010
2010
Incidental pick up 2013 on Chest CT
Bx: met adeno Ca
Where Did I Go Wrong?� It’s not like I don’t look for synchronous
malignancies. Not showing the ones I have picked up.
� Bowel activity variable, often diffuse or little/no activity
� Focal intense activity with little or no other bowel avidity should raise concern of lesion, Ca, adenoma, etc. Not specific for cancer.
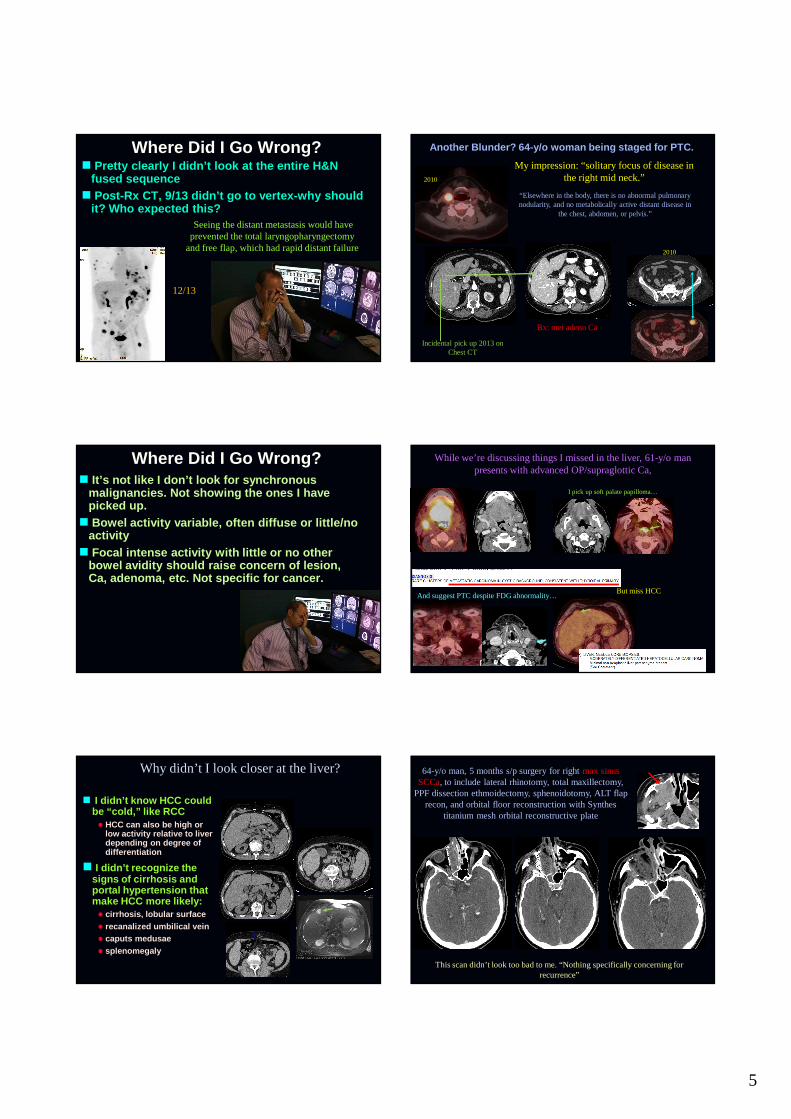
While we’re discussing things I missed in the liver, 61-y/o man presents with advanced OP/supraglottic Ca,
I pick up soft palate papilloma…
And suggest PTC despite FDG abnormality…But miss HCC
Why didn’t I look closer at the liver?
� I didn’t know HCC could be “cold,” like RCC� HCC can also be high or
low activity relative to liver depending on degree of differentiation
� I didn’t recognize the signs of cirrhosis and portal hypertension that make HCC more likely:� cirrhosis, lobular surface� recanalized umbilical vein� caputs medusae� splenomegaly
64-y/o man, 5 months s/p surgery for right max sinus SCCa, to include lateral rhinotomy, total maxillectomy,
PPF dissection ethmoidectomy, sphenoidotomy, ALT flap recon, and orbital floor reconstruction with Synthes
titanium mesh orbital reconstructive plate
This scan didn’t look too bad to me. “Nothing specifically concerning for recurrence”
6
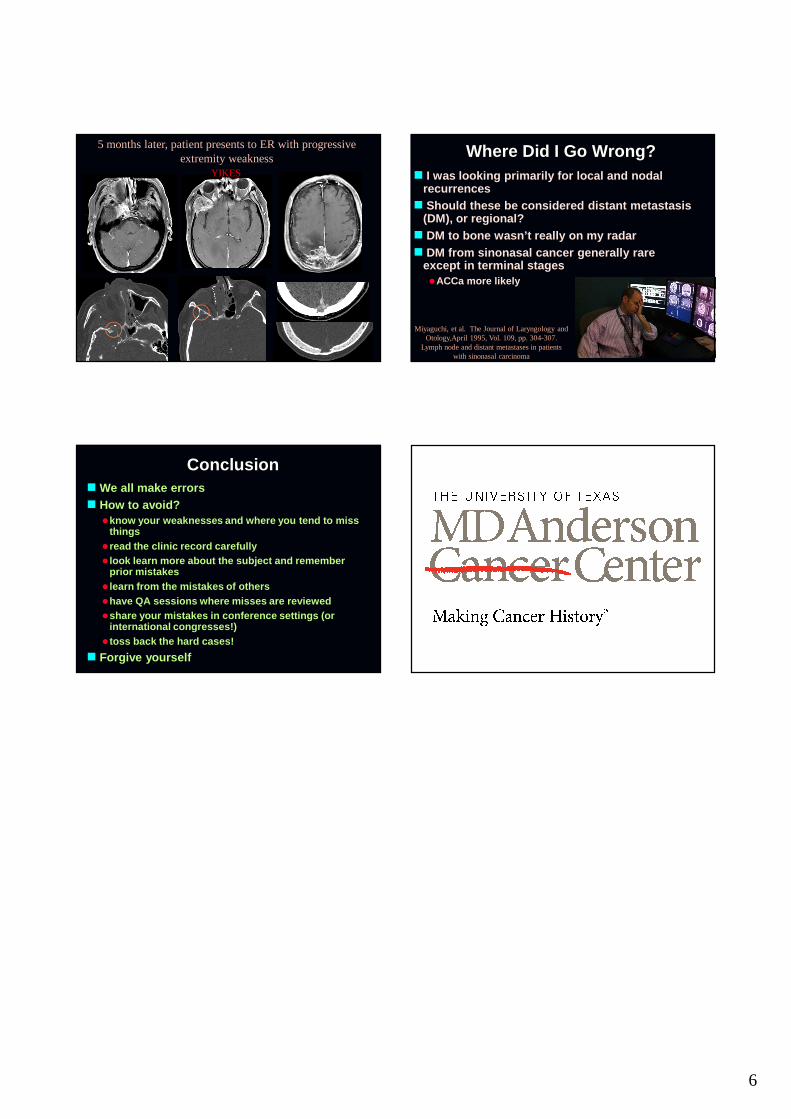
5 months later, patient presents to ER with progressive extremity weakness
YIKES
Where Did I Go Wrong?� I was looking primarily for local and nodal
recurrences� Should these be considered distant metastasis
(DM), or regional?� DM to bone wasn’t really on my radar� DM from sinonasal cancer generally rare
except in terminal stages�ACCa more likely
Miyaguchi, et al. The Journal of Laryngology and Otology,April 1995, Vol. 109, pp. 304-307.
Lymph node and distant metastases in patients with sinonasal carcinoma
Conclusion� We all make errors� How to avoid?
�know your weaknesses and where you tend to miss things
� read the clinic record carefully� look learn more about the subject and remember
prior mistakes� learn from the mistakes of others�have QA sessions where misses are reviewed�share your mistakes in conference settings (or
international congresses!)� toss back the hard cases!
� Forgive yourself



![Salivary gland nodules [Schreibgeschützt] - ESHNR · salivary gland nodules C. Czerny ... • Tumor benign – malignant • Posttherapie Introduction ... Normale Parotis Perfusion](https://img.pdfslide.us/doc/110x75/5ca9d62488c993c9218d4289/salivary-gland-nodules-schreibgeschuetzt-salivary-gland-nodules-c-czerny.jpg)