Embed Size (px)
Citation preview
MVA and (mainly) Malaria
Adrian Hill
The Jenner Institute, Oxford University

MVA: A Growing Safety Database
• 120,000 MVA vaccines during 1970s
• Poxvirus boosting for T cell response amplification
discovered in malaria
– Vaccinia then MVA (1996)
• First clinical trial of MVA boosting in 1999
• Since then over 100 clinical trials
– 46 in malaria (six inserts), 35 in TB, HIV, influenza, HCV
– >1000 vaccinees in malaria, > 2000 in TB, > 1000 others
– Therapy: melanoma, renal cancer, prostate cancer, HIV,
HCV, HPV (over 500 cancer patients for Trovax alone)
– No myocarditis issue

MVA: some updates
• BAC recombineering technology has accelerated vector
construction (Cottingham et al PLoS One, 2008)
– as have flow sorting methods
– Attempts to enhance immunogenicity further: limited success
– Immunogenicity dependent on cross-presentation
– Vector genetic and thermo-stability generally excellent
• Some differences from NYVAC reported
– But appear minor
• Orthopox vectors being developed for diverse species
– e.g. cattle (TB) and chickens (influenza)
– Multiple avipox vectors widely used as veterinary vaccines

Malaria A Complex Parasite Life-Cycle

The MeTRAP Vaccine Insert
Targets the Liver-Stage of Plasmodium falciparum
ME: Multiple malaria epitopes
TRAP: Thrombospondin-
Related Adhesion Protein
TRAP strain is T9/96
in this vaccine
A Polyepitope-Protein Vaccine Construct

Why Use Viral Vectors
in Prime-Boost Regimes?
• Best means of safely inducing T cells in humans
• 7 vaccines have induced >1500 SFU/ml – in malaria (x 3), HCV, HIV, tuberculosis and influenza
– all used MVA viral vector boosting
• Adenovirus – MVA is the most potent approach – better than DNA – Adenovirus
– better than Adenovirus - Heterologous Ad
Adenovirus Prime MVA Boost
8 weeks
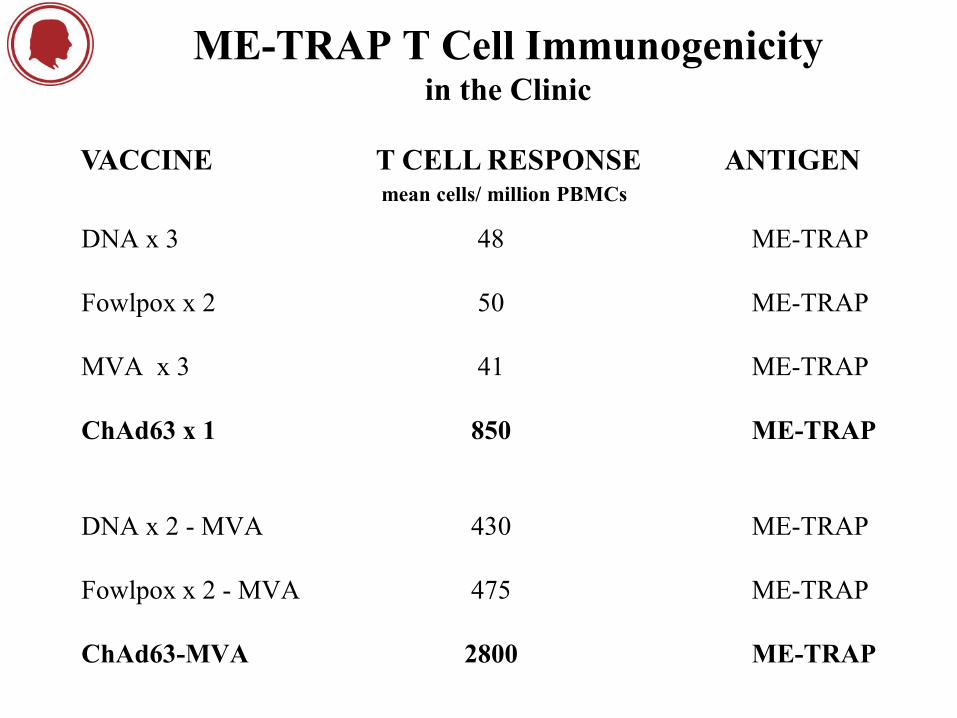
ME-TRAP T Cell Immunogenicity in the Clinic
DNA x 3 48 ME-TRAP
Fowlpox x 2 50 ME-TRAP
MVA x 3 41 ME-TRAP
ChAd63 x 1 850 ME-TRAP
DNA x 2 - MVA 430 ME-TRAP
Fowlpox x 2 - MVA 475 ME-TRAP
ChAd63-MVA 2800 ME-TRAP
VACCINE T CELL RESPONSE mean cells/ million PBMCs
ANTIGEN
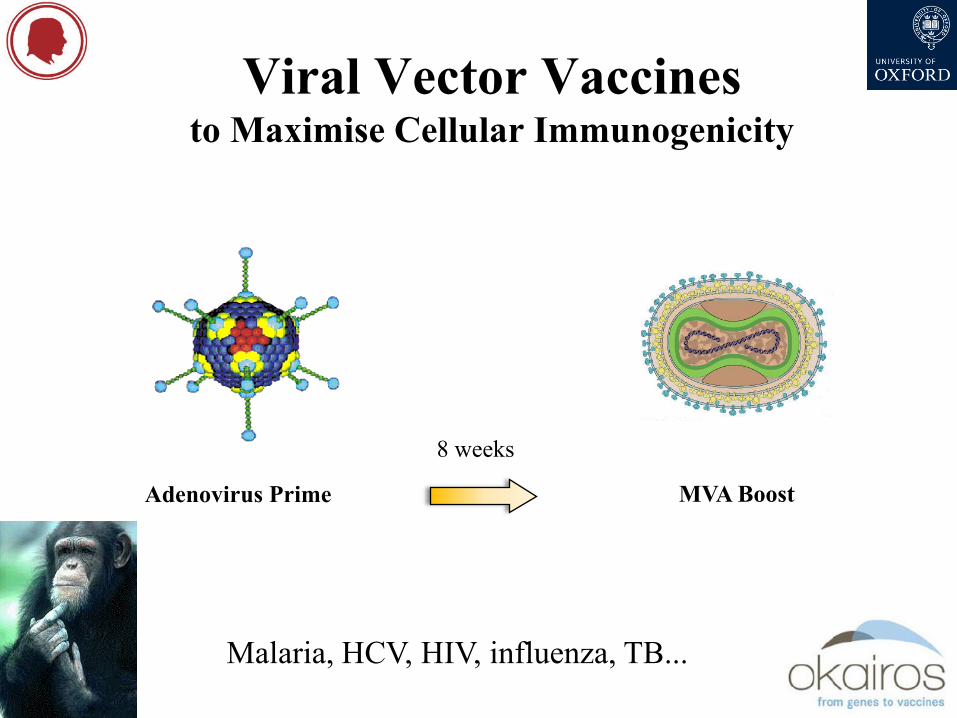
Viral Vector Vaccines to Maximise Cellular Immunogenicity
Adenovirus Prime MVA Boost
8 weeks
-
Malaria, HCV, HIV, influenza, TB...
0
100
200
300
400
500
600
700
800
1 2 3 4 5 6 7
SF
Cs / M
ILL
ION
PB
MC
s
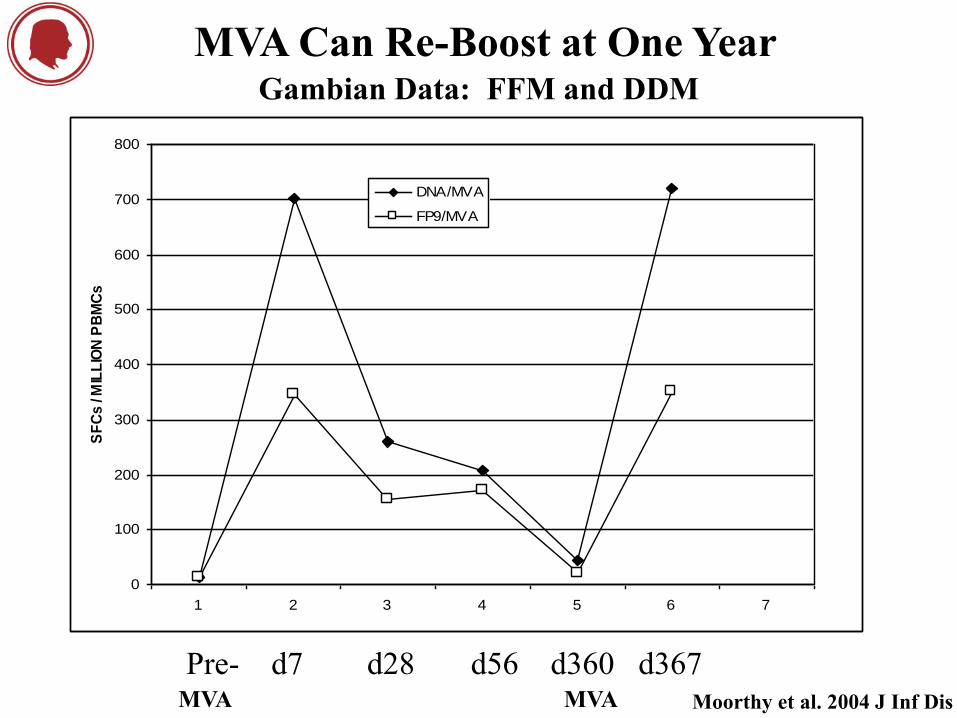
DNA/MVA
FP9/MVA
MVA Can Re-Boost at One Year Gambian Data: FFM and DDM
Pre- d7 d28 d56 d360 d367 Moorthy et al. 2004 J Inf Dis MVA MVA

ChAd-MVA Responses
are Durable and Can Be Re-Boosted at 6-30 Months Post-MVA
O’Hara et al. 2012 J Inf Dis

ChAd63-MVA MeTRAP Efficacy correlates with CD8+ T cells
CD8+ T cells correlate with efficacy specifically g -interferon +ve cells
Ewer et al. submitted
57% (8/14) of volunteers show vaccine efficacy 21% (3/14) show sterile protection
3/3 showed efficacy at 8 months

0 20 40 60 80 100 120 1401
10
100
1000
10000
Time (d)
An
ti-A
MA
1 (
3D
7)
EL
ISA
un
its
0 20 40 60 80 100 120 1401
10
100
1000
10000
Time (d)
An
ti-M
SP
11
9 E
LIS
A u
nit
s
0 20 40 60 80 100 120 1400
1000
2000
3000
4000
5000
6000
AdCh63-MVA MSP1
AdCh63 MSP1
Time (d)
IFN
- g S
FU
/ M
illi
on
PB
MC
s
0 20 40 60 80 100 120 140
0
1000
2000
3000
AdCh63 AMA1
AdCh63-MVA AMA1
Time (d)
IFN
- g S
FU
/ M
illi
on
PB
MC
s
MVA Boosts MSP1 & AMA1 Antibodies ChAd63-MVA Phase Ia clinical trials
Sheehy SH et al. (2011) Mol Ther 19:2269-76
Sheehy SH et al. (2012) PLoS ONE 7:e31208
ChAd63 prime = 5 x 1010 vp (i.m.)
MVA boost = 1.25 - 5 x 108 pfu (i.m.)
MSP1
0 20 40 60 80 100 120 140 1601
10
100
1000
10000
Group 2A
Group 1A
Time (d)
An
ti-M
SP
11
9 E
LIS
A u
nit
s0 20 40 60 80 100 120 140 160
1
10
100
1000
10000
Group 2B+C
Group 1B
Time (d)
An
ti-M
SP
11
9 E
LIS
A u
nit
s
A B
C
Figure 5
3D7 FVO 3D7 FVO
0
20
40
60
80
100
An
ti-M
SP
14
2 I
gG
(
g/m
L)
D
Group 1 Group 2
rs = 0.87P < 0.0001
rs = 0.90P < 0.0001
d28 d84 / dC-1d28 MSP1 ETSR vs QKNG
1 10 100 10001
10
100
1000
MSP119 ELISA units (ETSR)
MS
P1
19 E
LIS
A u
nit
s (
QK
NG
)
d84 MSP1 ETSR vs QKNG
100 1000 10000 100000100
1000
10000
100000
MSP119 ELISA units (ETSR)
MS
P1
19 E
LIS
A u
nit
s (
QK
NG
)
0 20 40 60 80 100 120 140 1601
10
100
1000
10000
Group 2A
Group 1A
Time (d)
An
ti-M
SP
11
9 E
LIS
A u
nit
s
0 20 40 60 80 100 120 140 1601
10
100
1000
10000
Group 2B+C
Group 1B
Time (d)
An
ti-M
SP
11
9 E
LIS
A u
nit
s
A B
C
Figure 5
3D7 FVO 3D7 FVO
0
20
40
60
80
100
An
ti-M
SP
14
2 I
gG
(
g/m
L)
D
Group 1 Group 2
rs = 0.87P < 0.0001
rs = 0.90P < 0.0001
d28 d84 / dC-1d28 MSP1 ETSR vs QKNG
1 10 100 10001
10
100
1000
MSP119 ELISA units (ETSR)
MS
P1
19 E
LIS
A u
nit
s (
QK
NG
)
d84 MSP1 ETSR vs QKNG
100 1000 10000 100000100
1000
10000
100000
MSP119 ELISA units (ETSR)
MS
P1
19 E
LIS
A u
nit
s (
QK
NG
)
1B 2B 1B 2B
0
20
40
60
80
100
120
Group
An
ti-A
MA
1 Ig
G (
g/m
l)
1B 2B 1B 2B
0
20
40
60
80
100
120
Group
An
ti-A
MA
1 Ig
G (
g/m
l)
AMA1
1B 2B 1B 2B
0
20
40
60
80
100
120
Group
An
ti-A
MA
1 Ig
G (
g/m
l)
1B 2B 1B 2B
0
20
40
60
80
100
120
Group
An
ti-A
MA
1 Ig
G (
g/m
l)

Sukuta Vaccine Clinic The Gambia

MVA: Immunogenicity Summary
• MVA is a poor priming vector
– but it remains the best boosting vector
• Generally MVA boosts what is primed
– responses appear to broaden
• Mixtures of different vectors (Ad mixed with MVA)
– are more potent than the individual vectors
– both pre-clinically and clinically (Reyes-Sandoval et al. Mol Therapy 2012)
• Many adjuvants reduce MVA immunogenicity
– IMX313 increases it as a carrier protein (Spencer et al. PLoS One 2012)
• Late re-boosting should be explored further

Why Might You Not Use MVA?
Three potential concerns
1. Cost of scale-up
2. Instability
3. IP
Use cell lines (EB66, AGE1.CR)
Use the right promoter
No longer an issue

3 Take Home Messages
• In nearly all cases MVA boosts pre-existing T cell
responses by about 5 to 10 fold
– to 1,000 - 10,000 SFU / million
– significant efficacy in 6 phase II malaria trials required MVA
boosting
– also good antibody boosting, by about a 10 fold
• Safety has been very good in thousands of vaccinees
– Malaria, TB, HIV, cancer, flu, HCV:- > 4000 subjects
– Europe, Africa, US
• Re-boosting with MVA vector after 6 months works
– in mice and in humans

Malaria Acknowledgements
Malaria Pre-Clinical BioManufacturing Clinical Trials
Simon Draper Sarah Moyle Geraldine O’Hara
Arturo Reyes-Sandoval Eleanor Berrie Susanne Sheehy
Alex Spencer Chris Duncan
Migena Bregu Nick Anagnostou
Matt Cottingham Katharine Collins
Sarah Gilbert Alfredo Nicosia Katherine Gantlett
Stefano Colloca Ian Poulton
The Gambia Riccardo Cortese Sean Elias
Kalifa Bojang Nick Edwards
Katie Flanagan Kilifi, Kenya Alison Lawrie
Muhammed Afolabi Roma Chilengi Katie Ewer
Jenny Mueller Caroline Ogwang Bob Sinden
Britta Urban
European Vaccine Initiative WRAIR
Egeruan Imoukhuede Jitta Murphy





























