Embed Size (px)
Citation preview

M
Ja
b
a
KMTSIF
isvwt
T
pttcovfr
hawcma
j
0d
The Arts in Psychotherapy 36 (2009) 75–83
Contents lists available at ScienceDirect
The Arts in Psychotherapy
usic, trauma and silence: The state of the art
ulie Sutton, PhDa,∗, Jos De Backer, PhDb
Centre for Psychotherapy, Belfast HSC Trust, Belfast, N. Ireland BT8 8BH, UKU.P.C. - K.U. Leuven, Campus Kortenberg, Belgium
r t i c l e i n f o
eywords:
a b s t r a c t
usicraumailencemprovisationorm
This joint-authored article explores the ways in which music can speak directly to the traumatic, and howmusic therapy offers a unique means of coming to an understanding of the traumatised patient. We takea musical and psychoanalytical theoretical stance. Drawing on case material from work with a young boyand an adult attending a psychiatric outpatient department, we show how a form of musical listeningand thinking about what is emerging in the clinical room can help us to understand something about thepatient, about the treatment of those traumatised, and also about the art of music itself. Our aim is to
herap
place the music and the t“Where I am, I don’t know, I’ll never know, in the silence you don’tknow, you must go on, I can’t go on, I’ll go on.” Samuel Becket
Consider the qualities of traumatic material: compacted, repeat-ng, shapeless narrative; collapsed time. Consider the qualities ofilence: in presence, an open, receptive, reflective space; in absence,oid. Through case material with a child and an adult patient, weill explore the ways in which music therapy can speak directly to
he traumatic, and the impact of silence within such work.
he state of the art
Within music therapy we find a kind of poetry, and a musicalrocess we describe as a form-giving exchange between patient andherapist. We note that this is true even when the patient is not ableo participate in improvisation; in this case, it is the therapist’s per-eption (both personally and musically) of the affective resonancef the patient that provides the starting point for musical impro-isation. It is the music’s very qualities that enable the potentialor such a direct, affective resonance to be sounded in the therapyoom, via musical sounds and silences.
Like speech (language), music is a symbolic system specific touman beings, but which both underlies and contains more thanshared language meaning system. Music cannot “mean” in the
ay that language might “mean”; music goes beyond the kinds ofonceptual meaning that could be captured in words, but whichay underlie words. Music has a unique quality that enables direct
ccess to an affective and corporal aspect of the human psyche.
∗ Corresponding author.E-mail addresses: [email protected] (J. Sutton),
[email protected] (J. De Backer).
197-4556/$ – see front matter © 2009 Elsevier Inc. All rights reserved.oi:10.1016/j.aip.2009.01.009
eutic relationship as the central focus in the work.© 2009 Elsevier Inc. All rights reserved.
This is music’s intimate dimension and it plays a central role in thefundamental process of symbolisation. Music has something dis-tinctive to offer through its capacity to develop a space betweentherapist and patient, within which it is possible for the one to res-onate with the other. Music can also speak to the inner world andpersonality of very disturbed patients, imparting a unique qual-ity not only in the space between, but also within therapist andpatient.
Music therapy is particularly effective with patients who,because of their specific pathologies (e.g., strong defence mecha-nisms, aphasia, dementia, regressed states, or psychic disturbance),lack the resources or motivations necessary for most forms of ver-bal psychotherapy. In music therapy, we bear in mind and give formto psychic problems on a musical-symbolic level via a process ofmusical improvisation, which is present and held within a thera-peutic relationship in music in conjunction with verbal reflection.Our art of music offers the possibility of coming into resonancewith the psychic level itself, a level that is found mostly in a roughor almost uncultivated form, but which is necessary for the devel-opment of the therapy. Therefore, we define music therapy as aform of pre-verbal psychotherapy, conveyed via a therapist and apatient in musical improvisation. This is a therapeutic relationshipbetween one or more patients and one or more therapists with theaim of reducing or solving psychic difficulties, conflicts, or distur-bances.
In this article, we explore and develop further these ideas andinclude two clinical examples of work with patients’ traumaticmaterial. Within the clinical material, we reflect on the thera-
pist’s maintenance of a particular type of human presence that ispersonally and musically receptive to what might come from thepatient. It is in the spaces in which these kinds of presences livethat the patient and therapist can come closest to the particularsense of poetry available in music, in which, there is “a sense of
7 s in Ps
at1
T
t1citieeu
teta(a1btol“i1
spbrlthwseadsa
M
ooaanoaneo
6 J. Sutton, J. De Backer / The Art
n essence” that as Ogden noted, “is not already there. . .waitingo be illuminated; it is newly created each time” (Ogden, 2001, p.77).
rauma and repetition
Etymologically the word “trauma” refers to a wound, createdhrough damage from an event or from different events (Garland,998). As Caruth noted, “trauma is always the story of a wound thatries out, that addresses us in the attempt to tell us of a reality thats not otherwise available” (Caruth, 1996, p. 4). Something compelshe person to tell his or her story and to repeat it, creating a tensionn the repetition that is in itself a compulsion to heal. Traumaticvents always repeat in order to try to form a story and a coher-nt narrative with which to shape what cannot be assimilated ornderstood.
Trauma is not a single entity, but involves an inner processhat can be compared to the concept of Fremdkörper,1 somethingmbedded in the psyche that is connected with other, undigestedraumatic events. The trauma is not only an external event. It is
linking of an external danger with a perceived internal threatincluding its real link with the past), creating connections betweennxiety about physical death and psychic death (Bertrand & Dory,989). With internalisation of an external trauma there is a gapetween the event and the response to it, within which exists theraumatic experience. This is an experience that is new, sudden andverwhelming, and which from this point is then repeated end-essly. The repetition is described by Caruth as the original eventnot assimilated or experienced fully at the time, but only belatedly,n its repeated possession of the one who experiences it” (Caruth,995, p. 4).
External trauma can come into someone’s inner world in ahocking and alarming way, where it remains unknown until theoint at which psychic pain is experienced, even when there maye no conscious experience of this pain (as with dissociation). As aesult of the inner impact of an external trauma, a normal way ofiving is disrupted. As one patient described, “When the externalrauma happened, it felt like my jigsaw (a metaphor for her life ander being) was hit very hard from underneath, and all the piecesent into the air. Therapy was like watching the pieces falling, and
eeing where they landed. You [the therapist] helped to make thedges of the new jigsaw, and helped me to see the shapes, oldnd new, that were made when the pieces landed.” These wordsescribed the therapeutic process, which continued until a new jig-aw was created by the patient, who simultaneously experiencednd noticed this process unfolding.
usic, repetition, time and trauma
“Time becomes real to us primarily through movement” Roger Ses-sions
Music can be described as an embodied flow in time of our sensef being. When listening to music, we have available the possibilityf experiencing ourselves as both familiar and changed. We losemomentary sense of time, space, and personal identity, while
lso retaining an overall sense of being and feeling. When we con-ect with a process of receiving internally a music from outsideurselves, the past and the present sit together in relationship, in
nd through time, as the music moves along with its and our past,ewly experienced in the present, in motion towards a future that isxperienced as it is being shaped (Sabbadini, 1996). The therapist’spenness to staying with the unexpected in the ongoing movement1 “foreign body.”
ychotherapy 36 (2009) 75–83
of thoughts and feelings becomes an act of staying with the primaryprocess that is unfolding in the patient in the room. This process isone that is fundamentally musical.
With traumatic material, the content reverts to a form of pri-mary process thinking (Sutton & McDougall, in press; Williams,2007). However, instead of the experience of musical listening,time and space appear to collapse, leaving fragments of experiencewhere past, present, and future appear simultaneously, alongsidethe unbearable trauma that these connect with. Such fragments popup, repeating endlessly in any one moment, where the one cannotbe differentiated from the other. There is no bodily (embodied, orbody-mind) connection with the movement of time as narrativeunfolding into the future.
Traumatic repetition results from the patient’s unsuccessfulattempts to annul the impact of traumatic events. Traumata havetwo aspects that Freud (1920) notes in the process of Nachträg-ligkeit, in which initial experiences, impressions, and memories areafterwards experienced again. This re-experiencing takes place ina further, developing phase wherein these experiences, impres-sions, and memories are reactivated, and out of which emergesnew meaning. Stroeken (2000) explains it as a re-interpretationof earlier experiences on the basis of new knowledge. This conceptinvolves a form of repetition that can also be linked technically tothe analytic third space, which is in itself a creative act betweenpatient and therapist, but which must reside first in the therapist(Ogden, 1997/1999). We hypothesise that in music we have manypossibilities for this creative process to open up, through the veryact of improvisation, at the fundamental (primary) level accessiblethrough the art of music. Music therapy follows a process in whichpassive victim moves towards active player, as the traumatic eventis repeated in a play (improvisation).
In a music therapeutic context, we often experience the samekind of music in post-traumatic play, which we define as a sensorialplay (De Backer, 2006). Sensorial play describes the character-istic playing of patients who, while producing sounds, are notable to connect with or experience these sounds as coming fromthemselves. The patient’s music is characterised by repetitivenessand/or fragmentation. The improvisation cannot really be begunnor ended, and there is no clear melodic, rhythmic, or harmonicdevelopment, no variation, and no recapitulation. The patient isperceptually and emotionally detached from his own musical pro-duction. Improvising, therefore, is not a real “experience” for thepatient, who is neither inspired nor affected by the music and isinstead disconnected from his or her sounds and the playing ofthese sounds. There is an absence of shared playing and intersub-jectivity with the therapist, in the sense that patients do not engagein the joint music, and their sounds remain outside of and discon-nected from them. “The music therapist experiences the patient asisolated, becomes completely caught up in the patient’s music (i.e.the musical behaviour) and is not free to introduce his or her ownmusical images; because of this, no interaction is possible, and it isimpossible to engage in a shared timbre in the ‘co-play”’ (De Backer,2006, p. 268).
We suggest that in clinical work the repetitiveness of traumaticplay can be described as coming from a psyche that exists as apacked, compacted mass. Through the traumatic event, the psycheis so compressed and filled up that thinking becomes impossible.It could be said that this compact and compressed psychic spacecan only spin around its own axis, where time has collapsed. Themusic therapeutic process we have observed in patients, who movetowards an inner image or a musical form, suggests that in this
compact mass, a small opening can emerge. This becomes possi-ble when the therapist can be at the same level as the affect ofthe patient, waiting for a moment to arise in which his or hermusical play can come into resonance with the different layersof the trauma. A part of the patient’s compact psychic space can
s in Ps
tacoiici
ieiibltobcfepcoah2
vpdaowbnttep
Fpwtlc
iaabBuoaeoioTstTacB
J. Sutton, J. De Backer / The Art
herefore be appropriated because of such a moment opening up,fter which mentalisation2 can occur, a process possible specifi-ally through the appearance of a musical theme or of rhythmsr a melody from patient and therapist working together. Thisndicates the first presence of a small space that could allow annitial step towards symbolisation. In this first opening in theompact mass one can see brief moments of attunement happen-ng.
Music can be called an art in which material can repeat adnfinitum, but always with the possibility of endless variety, as forxample the music of Bach attests. This is repetition that takes placen and through time, and offers patients the potential for an embod-ed experience of themselves, as their music (and they themselves)ecome newly created from moment to moment, at the same
evel at which trauma is experienced. We can see from work withraumatised patients that there is a clear musical psychopathol-gy (sensorial play), but with a recurring theme of moments ofeing something other than this (moments of synchronicity3) thatoalesce towards more of a new musical embodied self (musicalorm). Moving through this process (both backwards and forwards)nables the patient to re-experience him- or herself as an activearticipant, rather than a passive victim trapped in an endlessycle. When the patient can find release from the confines of hisr her traumatic prison, and discover a means of giving the traumaform of expression through musical improvisation, it can only
appen through a creative process in potential space (Leibovici,007).
We explore further the ideas outlined above in two clinicalignettes: the first depicting part of an early session with an adultatient at the limit of what can be treated dynamically; the secondescribing an unexpected moment in further developed work withtraumatised child. Both examples can be understood in relation tone another, showing subsequent aspects of the process of workingith sensorial play. The first vignette demonstrates how silence can
e not only a defence, but also a protective shield through whichothing should penetrate. The therapist’s attitude towards, and lis-ening to, this silence is critical for the further development of the
herapy. The second vignette describes how such a listening laternables a new space to emerge, within which intersubjectivity isossible.2 Not to be confused with the term “mentalisation” described by Bateman andonagy (2004), we use it here to indicate a phenomenon of a process in which theatient can digest mentally or musically his traumatic affect. In the musical space,hich is developed in the musical improvisation, the patient can play and think. “In
he appearance of the musical form the traumatic affect and verbalisation will noonger be disconnected from one another and from now on, the traumatized patientan speak for himself” (De Backer, 2006, p. 296).
3 Synchronicity is a term that describes a point in time in which there is a sharednner experience of the patient and the therapist, in which they feel free andutonomous in their play during a musical improvisation. This shared experienceppears unexpectedly and unintentionally, and is characterised phenomenologicallyy attunement between the musical parameters of the patient and the therapist.oth patient and therapist have the feeling that they are able to come into a gen-ine shared play for the first time with an intertwining of two musical lines intone entity, or one whole; for example, where both share the same pulse with sharedccents in the meter. Underpinning this moment is the paradoxical experience ofach individual’s freedom and autonomy. The mutual dependency in the creationf a shared musical object leads to a liberating feeling of being able to make musicn a completely independent way. The patient and therapist are free in relation tone another and can play, think, exist, and develop his or her own musical thoughts.his paradox involves emerging autonomy in the patient and therapist while, at theame time, there exists acceptance and recognition of mutual dependency. Amidhis paradox, brief moments occur in which the timbre of both players intertwines.hese moments of synchronicity can be brief, unexpected and infrequent, actings possible precursors for the development of the musical form. Moments of syn-hronicity usually appear at a specific or “right moment” in a shared experience (Deacker, 2006, p. 276).
ychotherapy 36 (2009) 75–83 77
Example 1: A deathly sleep—work with a traumatised adult
“Absolute silence leads to sadness. It is the image of death.” JeanJacques Rousseau
Vicky was born three decades ago, and arrived at her third fosterfamily at the age of 6 months. She was then adopted by this family,who recall that she had significant problems feeding and that hershort life up to this point had been full of disruption and confusion.Vicky developed through childhood as impulsive and emotional.Her medical notes reveal a dramatic adolescence, full of conflictand suffering, marked by an eating disorder, risk-taking behaviour,cutting, and overdoses. In her twenties, she was raped during a tripto another country. The impact of this event and its aftermath, alongwith what she had experienced from her early years onward, led toa serious overdose and further psychiatric treatment. Vicky latermothered two children but the relationship with the father brokedown.
After a series of stressful events within the past year, she hadanother major overdose and attempted to hang herself. She wasresuscitated but, due to hypoxia, she now uses a wheelchair andhas laboured and sometimes unclear speech, as well as confusedmemory and thought processes. Her neuropsychiatrist referredher for psychotherapy in order to ascertain how much of her dis-ability was a result of traumatic brain injury and how much wascaused by the traumatic nature of her early life experiences. Amusic psychotherapy assessment was undertaken in order to meetVicky’s traumatised inner world via the primary processing avail-able through clinical musical improvisation. Vicky attended aninitial meeting and agreed to come to music therapy for 6 months,after which a further decision might be made about open-ended,long-term therapy. She is currently halfway through this 6-monthprocess.
On first meeting, Vicky entered the therapy room with anambivalent, distant, vague interest in the instruments and the ther-apist. She was compliant, with a tendency to mirror nuances of thetherapist’s facial expression and speech. She seemed to be merelya reflection of a person, psychically absent and responding in a waythat suggested she was mechanically producing what she felt wasneeded by the therapist. Yet, for brief periods something appearedin the room that had a stronger and clearer affect, which felt tothe therapist as though Vicky was more present and alive. She waswary of playing, but managed to explore the bongo drums and thepiano for a few minutes at a time, choosing to share the instru-ments with the therapist but abruptly closing off the music bysaying, “That’s enough.” She had no reflections about the music.While quiet and slow-moving, the music had been tense, with small,fragmented silences during which Vicky disappeared. During andafter the session, the therapist experienced a deep, projected sad-ness and anxious confusion about recalling what had happened.The image of sitting with a two-dimensional reflection of a per-son remained throughout the week. At her next session, Vickyarrived appearing more emotionally mixed-up than she did theprevious visit. She stated she had no memory of being in the roombefore, but recognised the piano and the drums. This made sense,because she had been barely present in the first session, yet didengage with more affect during musical play and on other briefoccasions.
The following example is of a short piano duet from this secondsession, with Vicky seated at the treble register of the piano and thetherapist at the bass register. She and her therapist exchange sin-
gle notes. There is no sense of forward movement in Vicky’s musicand she appropriates the post-resonance of the therapist’s first sin-gle note. Brief silences appear and fall into a void, with an almosttangible shock. Vicky’s notes do not resonate; they die away. Duringthe play, the therapist is caught in an intense concentration focused
78 J. Sutton, J. De Backer / The Arts in Psychotherapy 36 (2009) 75–83
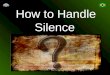
Fig. 1. Example 1 Vicky.

s in Ps
oooif“aanameV
iibtiospVswa
ofmieatsbc
ardVssthy
bopnoftomtancttbrt
J. Sutton, J. De Backer / The Art
n staying present. At times, Vicky joins the therapist’s note’s res-nance as if it breathes her alive for a fleeting moment. The impactf this connectedness followed by a falling into a deathly silences terrifying for Vicky. She dissociates from this terror, but returnsor her next session in a distressed state. She begins emphatically,I want to tell you something important,” and tumbles out a storybout a music teacher from her past who had a terrible accident,nd who she wants to know that she is thinking of her but haso way of contacting her. A feeling of intense pain and tragedyccompanies this story, which is relayed with the urgency of a trau-atic narrative, with past and present intermingled. The therapist
xperiences Vicky in a disturbed psychotic state Fig. 1 Example 1:icky.
The score shows how Vicky joins the musical play by attach-ng her own notes to the post-resonance of the therapist’s notes,n the same way that she mimicked the facial expression and ver-al utterances of the therapist earlier in the session. One can notehat there is no possible forward movement, as the sense of time isnterrupted, and Vicky plays as if sucked into the therapist’s previ-us note (as at: ‘52). She does this in an attempt not to exist but tourvive, remaining in her encapsulated state. At other points in thelay, two types of traumatic silence can be observed: first, whereicky loses a sense of continuity in the music and herself, with herounds falling into nothingness (i.e. ‘27–‘28 and ‘31–‘33); second,here she breaks the potential for connection (as at: ‘49), by letting
ny hint of musical momentum subside.Between ‘56 and ‘59, there is a single example of the beginnings
f a live connection between Vicky and her therapist in which,or the first time, a fragile pulse almost emerges. A melodic frag-
ent (c#-d#-a#) develops out of Vicky’s placing of the note d#,n relation to the therapist’s preceding c# and following a#. How-ver, rather than complete the melody, which would result in Vickyppropriating the therapist’s first note of the group and maintaininghe momentum and forward direction (in full: c#-d#-a#-c#-g#),he loses connection with the music, preventing the melody fromreathing further. At this point, the image of suffocating the musicame to the therapist in somatic transference.
The music continues much as before, with Vicky’s soundsttaching to or avoiding the therapist’s resonant notes. A final post-esonance of the therapist’s last note is accompanied by anothereadly silence, but this time with a quality of affect that is painful.icky looks at the piano notes, desolate and alone. A further intenseilence then follows, similar to those experienced in the first ses-ion. Vicky says, “I find it hard to play, can’t play like I used to andhat’s hard, do you know what I mean?” The therapist answers, “Iturts to play because you remember.” Vicky replies, “Yes, I could,ou understand.”
One can sense how this work with Vicky exists in the silencesefore a note could be imagined, which is far away from the ideaf a note being sounded. Rosenfeld (1987) has observed how someatient’s earliest difficult experiences colour emotional connected-ess at a fundamental level. These experiences leave them in a statef terror during which they must guard against external intrusionrom the mother, blocking her out to avoid the pain of such con-act. The confusion of different families in Vicky’s first 6 monthsf life and her reported early refusal to take food from her fosterother fits Rosenfeld’s picture of a baby turning away from con-
act. Work with such patients should proceed extremely carefullynd gradually, focused on containment and the patient’s primaryeed to feel safely held and accepted. Rosenfeld notes that thesehildren’s experiences “are also much more related to the inside of
he mother than to the breast; and analysts who tend to interprethe positive and negative feelings only towards the nipple and thereast rather than to the inside of the mother may find difficulty ineaching children of this kind” (Rosenfeld, 1987, p. 278). In musicalerms, we can note how the silent, embodied presence of the ther-ychotherapy 36 (2009) 75–83 79
apist will be of utmost significance. A primary musical listeningto the material that cannot and must not be sounded is essential,for it is only in experiencing the therapist’s commitment to beingpresent at this level that the patient may first feel seen, heard andacknowledged.
The strength of Vicky’s survival instinct is paradoxically in itsdissociated quality (autistic and/or autistic-contiguous position;Ogden, 1989). While it registers strongly in the transference, itfeels passive in another way. For Vicky, it is a desire for a death-like existence and not a fight against it. She makes herself dead(not alive) so that the fear and the unbearable pain cannot touchher. With this patient, it is the silence itself that is silenced;rather than destroy the silence with sound (as in the second caseexample), silence is not allowed to exist externally because of thepresence of a different, dissociated, cut-off internal silence. Thisexample reveals how unbearable silence is for the traumatisedpatient. No open, alive, relational silence is possible, because thepatient must keep at bay the terrible pain of separation followinga connection with the therapist, a connection that is wanted butdreaded.
Mentalisation after the session
Holding and working through the traumatic play of a patient issometimes unbearable for the therapist. However, the music ther-apist has, unlike the patient, the possibility of making it tolerableand digestible by improvising in a reverie style after the session (DeBacker, 2008). Following session with this patient, the therapistimprovised warm, gentle, holding music that was full of tender-ness. A picture of Vicky as a small baby came immediately to mind:a completely vulnerable infant who needed to be held with careand gentleness. Through this (mentalisation) play, the therapistcould create in musical form everything that had affected her dur-ing the session. Mentalising via these musical improvisations madeit possible for the therapist to back out of the mire of a traumaticplay. The therapist could then integrate the emptiness or compact-ness of the affect within an inner imagination (impression) andlet a hope and desire exist in order to continue the therapeuticprocess.
We could describe Vicky’s music as an attempt to maintain a sta-tus in which nothing can intrude nor touch because nothing existsto receive it. It is a position in which one remains impenetrableto what is outside, safe within a lonely fortress. Through the ther-apist’s willingness to sit beside this compact, deadly silence, andthrough musical reverie after sessions, another silence could existwithin the therapist’s mind. Only when this internal silence canalso exist in the room can a traumatised patient like Vicky sense thepresence of something alive in a less terrifying way. This emergedin a later session when Vicky asked the therapist to share a gazewith her. Vicky repeatedly sought out, maintained, and then brokea shared gaze. This occurred in lengthy, intense silences, the quali-ties of which changed. This was a new kind of silence, and one fromwhich movement emerged, as Vicky experienced herself as con-nected to a reliable, stable other. During one prolonged silence thetherapist noticed, with surprise, that an auditory image appeared,in a silent, gentle lullaby. The space for this to be sounded was notyet available, but the anticipation of it was present.
Another illustration of this process can be seen in the secondcase, of Tony, who left an intense, full emptiness behind in thefirst sessions. However, unlike the patient, the therapist had thepossibility of making the vibrating affect in his body bearable and
digestible through a musical improvisation. By improvising, a ther-apeutic silence was allowed, something that was essential for thementalisation of the compact sessions, as via the play the therapistgave form to the trauma that had to this point remained exter-nal.
8 s in Ps
Ea
cyhcTth(hsw
iomAitiM“sadwa
tTottdhcetom
tspltpdwv
aiip“mdiss
rial play brings into dynamic motion. This can only be set in motionby penetrating this compact sensorial substance (the traumaticmaterial). By taking something away from the traumatic material,
0 J. Sutton, J. De Backer / The Art
xample 2: From deathly silence to open silence—work withtraumatised boy
“The silence sank like music on my heart.” Samuel Taylor Coleridge
Tony is a 9-year-old boy who is very short and small. He has ahronic metabolism disorder, a disease that caused the death of hisounger brother a few years ago. Because his parents felt that Tonyad difficulties in getting over the death of his younger brother, theyontacted a music therapist to explore the possibility of treatment.he parents are both musicians and believed strongly in the poten-ial of music to help their son. It soon became apparent that Tonyad an existential fear of death, shown through anxiety of silenceswhich we can describe as an experience of “deathly” silence). Inis experiences in therapy, Tony discovered the creation of an innerilence through music, from which he could come back into contactith the traumatic—namely, his experience of loss and death.
Tony always presented himself as a very active, excited boy who,n the musical play, directly or defensively showed his fear of silencer of standing still. We often observe this phenomenon with trau-atised patients. It is reminiscent of the personality of Frits in “De
vonden” (The Nights), a novel by the Dutch writer Reve (2007). Fritss a young man who tries to master a psychic crisis by talking con-inuously in order to not be confronted with silence, because hes afraid that out of this silence his constant fear would surface.
usically, this can be related to, for example, repetitive, hypnotichouse” music, or systemic music—that is, music that enables a dis-ociated, altered state. It could be that Frits’ talking serves not onlys a defensive act of negating the possibility of silence, but also as aistraction (dissociation) and the manufacture of an altered state,hereby contact with the terror of deathly silence is kept at bay
nd he can become lost in the sounds.In a similar way, Tony does not allow a pause or a silence during
he first 12 sessions; rest and silence cannot and may not be present.he sessions are full of energy and sound, and Tony fluctuates fromne play situation or improvisation to the other. Sometimes, out ofhe transference he beats the gong very hard and unexpectedly,o assure himself that whatever silence could originate is beingestroyed. Even though there is a certain rhythm in the sessions,e cannot allow a pause or a phrasing in his music. The therapistan feel the projected fear in Tony’s music. Tony has to continuouslyscape his inner conflicts, rejecting or destroying each overture theherapist makes that attempts to offer the possibility of a phraser a silence that would enable an access to his inner world via ausical form.The therapist became fascinated by these musical improvisa-
ions because of their dynamic movements and volume, noting withurprise the strength and determination that this slight boy dis-layed. Play involving music and puppetry is central to the sessions,
eading to the session focused on in this vignette, and during whichhe therapist musically accompanies the events played out by theuppets. In a continuous, tyrannical way, on the musical level, Tonyestroys these dolls. The control of his fear and of the confrontationith death happens through the power he gets over life and death
ia the dolls.The next session begins differently, when Tony enters the ther-
py room showing an unusual restraint and he chooses a new musicnstrument: the small finger cymbals. The beginning of the musics surprising: Tony sits down quietly beside the therapist at theiano and a silence appears. The therapist’s session notes state:Immediately, I come into resonance with Tony’s inner psyche and
yself. During this resonance, I ‘get caught’ by something that Iid not expect at all—an atmosphere of space that comes over andnspires me. Not knowing what inspires me, I slow down my pacepontaneously and discover that I enter into a kind of melancholytate. I notice, again with surprise, how time is being stretched and
ychotherapy 36 (2009) 75–83
how the tone ‘b-flat’ musically attracts Tony. It is not the soundthat follows me, but it is I who follows the sound, and I am sur-prised by something that pops up in the relation with Tony andreact immediately.”
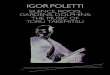
In a peculiar way, Tony experiences the sounds and the rhythmthat appear unintentionally with the therapist as something thatis not foreign to him and joins the musical play instantly. In thepost-resonation of the therapist’s falling second tone “a′,” a spaceoriginates which is not only the psychic space of the therapist, butalso that of Tony. In other words, this is a shared psychic and musi-cal space that is inhabited by both individuals. This space originatesfrom a kind of “pulsing,” in that it is not one but two notes. The sec-ond note (a′) refers to the first (b-flat), connects with it and, throughthis connection, then creates a pace. The second note creates aspace, which is the space between the first and the second note, andbetween these alternated sounds the therapist and Tony could hearan inaudible inner sound. Sensing something from Tony and fromthe resonance between them, the therapist intuitively makes themusic sing a melancholic “sigh,” at which point the appoggiatura4
figure appears. The therapist’s session notes record a poetic imageof “a sound of somnolent water, from an awakening wind, the soundof an extinct season sounds of phenomena which are pregnant ofan unprecedented meaning.” The second note colours the space notonly melodically but also harmonically.
Tony then creates a silence by taking over the therapist’s pacethat had emerged directly out of the resonance with his patient.Tony plays with the pulse, and it can be observed that once thereis the (musical) space, Tony can create his own perception of whatoccurs. Through this perception, he can seek out a specific rhythmor form for himself. This melodic movement is a falling minor sec-ond (from b′-flat to a′), during which the dissonance is apparent ina stretched form. This dissonance can be interpreted as the appear-ance of the traumatic material, which is now being carried by thetherapist Fig. 2 Example 2: Tony.
The specific feature of this improvisation is the appearance ofpace—of forward movement and direction in the music. The ther-apist offered the pace and, in a slowing down and stretching outof time, an inner silence originated. This extended silence (a sup-ported resonance of sounds and melody) was the silence of thetrauma, of the loss and the pain of this loss. For the first time, thetherapist experienced a seriousness in Tony, something that hadnot previously been present. The post-resonance of the dissonance(b′-flat to a′) made it possible for the traumatic to be present andcontained. During this improvisation, Tony was finally able to makea first step towards experiencing his sadness and began a process ofmourning. What first sounded outside, in the music, could suddenly(thanks to the form of this music) be experienced as somethingcoming from within himself. After a long and intense silence, theboy said in the reflection that he thought of his little brother andhow he said goodbye to him. As we know, the traumatic experienceis always outside, with a challenge for the music therapist to be inresonance with the patient, to listen to the silence of this traumaand allow the possibility of being surprised by a musical form thatmakes it possible that the outside at the same time becomes aninside.
This example illustrates the significance of silence in the cre-ation of a musical form. We define musical form as everything thatthe compact, repetitive, endless heaviness of the traumatic senso-
a new space can be created that contains the silence that is taken
4 An appoggiatura is a decorative addition to the primary theme of a piece ofmusic.

J. Sutton, J. De Backer / The Arts in Psychotherapy 36 (2009) 75–83 81
ampl
fetTa
o2ctgiToacbtio(abtaIhtawp
F
ttomow
Fig. 2. Ex
rom the sound. This silence enables us to move from the full pres-nce of the sound, and transforms it, so that it becomes possiblehat all sounds might be given meaning in relation to one another.he introduction of this silence is in this sense a symbolisingct.
Silence phenomenologically can appear in various forms. Onef them is what we term the anticipating inner sound (De Backer,006). One can describe the anticipating inner sound as the musi-al presence of an inaudible sound, in the silence that the musicherapist experiences and listens within, at the moment they areoing to play music with their patient. In the silence before themprovisation, the player anticipates the unknown that will come.his “preparation silence” allows one to come into resonance withneself and, in a music therapeutic context, with the other, wheren inner space must be created from which each authentic musi-al play derives. This anticipating inner sound is not only inaudible,ut also completely unknown and unpredictable. It is the soundhrough which the player lets himself be surprised while listen-ng, and which guides the musical improvisation; it is not thoughtut, it does not belong to anyone, but is heard by the “third ear”Reik, 1998) of the music therapist when he displays a receptivettitude towards the presence of his patient. The player lets himselfe guided by the power that originates from this empty sound. Afterhe silence that precedes the improvisation, the first tone soundsnd from this point one knows how the improvisation will elapse.n music therapy, it is of major importance to have awareness ofow patients enter into improvisation; for example, whether or nothey are able to allow this necessary anticipating inner silence, tollow themselves to be guided by something that they do not know,ith the alternative being that they might immediately fill up everyossible silence with sound or noise.
inal thoughts about silence
The two previous cases illustrate how traumatic patients havehe tendency to fill up every emptiness and silence in order to avoid
he possibility of creating a psychic space in which perceptions canriginate, and in which there might be fantasy or thought. Trau-atic material makes it impossible to anticipate an inner sound notnly before a first improvisation, but also often stretched across ahole play or throughout an entire session. It is also not possible to
e 2 Tony.
have ownership of the musical material, and the music producedremains completely external, foreign, and unfocused.
As we have shown, the phenomenon of silence is an impor-tant aspect of music therapy and trauma. Sutton’s work (2001,2002, 2006, 2007) has introduced new thinking about silence inmusic and music therapy; for example, illustrating how silence issignificant as an organising principle during musical improvisa-tion. Within a clinical research focus, De Backer (2007) identifiedconcepts of silence that related to psychopathology and furtherdeveloped these ideas in a process model of work with psychoticpatients. Silence is the driving force of intersubjective play inimprovisations during which there are moments of attunementto musical form. Paradoxically, it is only thanks to moments ofsilence (which act as a kind of punctuation) that phrasing becomespossible, that sounds become structured and that musical formoriginates with traumatic patients. In musical form, we noted thatsilences added an important dynamic in the structure of the soundsand rhythms that were being played.
We have shown that in sensorial play one can hear a compactsilence, in which no movement or dynamics are possible. In con-trast, we noted the concept of an open silence, which is a silence thatallows a psychic space and can be seen in parallel with Winnicott’s“potential space” (1971). In the first case example, we see silenceas a defence against a connectedness with another, a state intowhich no one can be allowed to enter, because of a terrible terrorof being intruded into. Here silence itself is negated, destroyed, ornot allowed to breathe, and what remains is a deadly, empty spacewhere nothing can live. The therapist’s task was to take in and hearthis silence and to find meaning in a nothingness. This was pos-sible through musical listening, maintaining a space described asthe intersubjective analytic third, and making use of mentalisationpost-session in order to open a space within which something asyet unknown might appear at a later point in the therapy.
If the therapist had instead filled the deadly silent space withsound, she would have intruded upon and negated the patient’sreality. Not to have remained present would have been to destroy
in turn the potential for two people to exist, with the therapist join-ing the deadly silence. This process was one of staying with a lackof anticipating inner sound, without a sign that anything differentmight be possible. It formed a therapeutic sense of hope for the pos-sibility of something else to grow. As such, the therapist’s silences
8 s in Ps
dwtpe
tttaiTtiTrha
fwlctiItai
emariaemttiwocwsddiw
pc(cdiitptmpiaf
2 J. Sutton, J. De Backer / The Art
uring and after session punctuated the patient’s silent void thatas present in the sessions. This void was a form of un-felt silence
hat the therapist recognised and aimed to feel and understand. Therocess of mentalisation gave meaning to the therapy and wouldventually enable the patient to feel accepted.
In the second case example, an open silence was introducedhrough phrasing, holding sounds, or delaying and slowing downhe tempo. Through this introduction, the pure repetitiveness ofraumatic play could be broken, allowing the first moments ofttunement to appear. In this vignette, silence created a spacen the compact mass of the psyche of the traumatised patient.hrough this silence, the full presence of the traumatic sound (inerms of repetitiveness in sensorial play) could be transformednto other sounds, which, in turn, gained a certain mutual value.his space made it possible for the endless heaviness of senso-ial play to be brought into motion. The musical form originatedere. The introduction of silence into it was a kind of symbolisingct.
As the case material has demonstrated, silence can only be trulyelt if there is a connection with what previously happened, wherehat has sounded before continues to sound in what we term a
inking tension. Such a tension becomes a “time-bridge” that canarry a continuation of the music into a lived future. Without thisime-bridge, the connection between time and space loses its link-ng character and becomes empty, without meaning or significance.n considering the space between patient and therapist in terms ofhis potential for the significance of silence within musical play, were in contact with an affective primary process, within which theres a possibility for inner and outer worlds to connect.
As Winnicott (1971) noted, the creation of such a space is at thedges of both the internal and external, at the very place that weark our being in the world. Potential space also occurs in time,
s it bridges past, present, and future, while traumatic experienceobs us of our sense of this relationship of space and time. Musicalmprovisation enables the therapist to remain at the affect level,nd creates a space in which traumatic events once more can bexperienced, but this time in a safe context. During the patient’susical improvisation with the therapist, while the uncontrolled,
errible, dreadful traumatic core remains, there can be created athe same time a manageable, aesthetic distance—a new space. Thiss a necessary process in order to mentalise the trauma, without
hich the patient would remain trapped inside his or her repetitionf the raw, unprocessed traumatic material. Without a therapeuticonsideration of silence in work with the traumatised, the therapistill be missing the fundamental core of the treatment; for without
ilence no space can be created. The state of the art of music speaksirectly to this process, coming out of and returning into silence. Aelicate and depth-embodied understanding of traumatic silence
n the therapist introduces a human presence with which to bearitness to the traumatic.
In our work, the idea of mentalisation-in-music results in theatient potentially coming to a musical form through the pro-ess of his improvisation. Musical form in a therapeutic contextDe Backer, 2006) is a term describing a musical structure that isreated within a symbolising process that develops from the foun-ations laid down during moments of synchronicity (e.g., as noted
n the second case vignette). Through such moments, which orig-nate out of traumatic sensorial play, clear rhythmic and melodichemes may appear that can be further explored or varied by theatient, and by patient and therapist together. Musical figures canhen be characterised by phrasing and pauses, with features of the
usical improvisation typically having a clear beginning and end,repared for mentally by patient and therapist. This phenomenon
s always an intersubjective dialogue between patient(s) and ther-pist, in which both experience themselves as equal to the other,eeling free and autonomous to play, think, exist, and develop their
ychotherapy 36 (2009) 75–83
own images and thoughts, with an intertwining of the timbre ofboth players.
During this process, the sounds that are generated in a musicalimprovisation are guided by something unknown to the subject.The music resonates with an inner awareness of something that isno longer experienced as external or unrelated. As we have shown,it is a form of poetry, and it can be discovered in the fundamentallymusical processes generated in which “potential potential space”can be found (Williams, 2007), and through which the patient isable to experience him or herself moving out of the traumatic mate-rial into the shared connection of intersubjectivity. When musicallyexperiencing, listening, digesting and thinking, one is able to under-stand traumatic material at the level at which it occurs. In musicalthinking, primary processing is revealed in depth and detail. Itcomes closest to what musicians know, that “Music can bring abouta ‘different state’. . .it can take one out of time or enfold itself end-lessly, as it were, within time. It can therefore be a process, andsimultaneously freeze time” (Brendel, 2001, p. 253).
As therapists we must find ways in which to come to terms withthe unbearable nature of the life experiences of our patients, inorder to remain present when traumatic material fills the therapyroom. In the gap between the traumatic event and the response to itexists the actual traumatic experience; but it is within this same gapthat another kind of space can be found to exist: the potential space.We have argued that in musically perceiving, experiencing, feelingand thinking about such spaces, we can be alongside our patients atthe same level at which traumatic material is experienced. Throughmusical listening and improvising, we can discover potential poten-tial space within traumatic experience. In being alongside theun-sounded silences that contain the patient’s unbearable mate-rial, and by finding our own musically resonant silent presence,we can offer some meaning to patients who have experienced andare caught inside the ever-repeating unthinkable. We believe thatthis potential can be carried specifically in the state of the art ofmusic.
References
Bateman, A. W., & Fonagy, P. (2004). Psychotherapy for borderline personality disorders:Mentalization based treatment. Oxford: Oxford University Press.
Bertrand, M., & Dory, B. (1989). Psychanalyse et sciences sociales. Paris: La Découverte.Brendel, A. (2001). The veil of order: Conversations with Matrin Meyer (R. Stokes,
Trans.). London: Faber & Faber.Caruth, C. (1995). Trauma: Explorations in memory. Baltimore: Johns Hopkins Univer-
sity Press.Caruth, C. (1996). Unclaimed experience – Trauma, narrative and history. Baltimore:
The Johns Hopkings University Press.De Backer, J. (2006). Music and psychosis. Unpublished doctoral dissertation, Uni-
versity of Aalborg, Denmark. http://www.musikterapi.aau.dk/forskerskolen2006/phd-backer.htm.
De Backer, J. (2007). Die Entwicklung eines psychischen und musikalischen Raumes.Adrian– eine Einzelfallstudie. In S. Metzner (Hrsg.), Nachhall. Musiktherapeutis-che fallstudien (pp. 45–89). Giessen: Psychosozial Verlag.
De Backer, J. (2008). Music and Psychosis: A research report detailing the transitionfrom sensorial play to musical form by psychotic patients. Nordic Journal of MusicTherapy, 17(2), 89–104.
Freud, S. (1920). Herrineren, herhalen en doorwerken. Werken 6. Amsterdam: Boom.,pp. 165–218
Garland, C. (Ed.). (1998). Understanding trauma: A psychological approach. London:Tavistock.
Leibovici, S. (2007). Trauma and creativiteit. Tijdschrift voor Psychoanalyse, 13(2),108–120 [jaargang].
Ogden, T. (1989). On the concept of an autistic-contiguous position. The InternationalJournal of Psychoanalysis, 70, 127–140.
Ogden, T. (1997). Reverie and interpretation: Sensing something human. London:Karnac Books.
Ogden, T. (2001). Conversations at the frontier of dreaming. London: Karnac Books.Reik, T. H. (1998). Listening with the third ear: The inner experience of a psychoanalyst.
New York: Farrar, Straus and Giroux.
Reve, G. (2007). De Avonden. Amsterdam: Uitgeverij De Bezige Bij.Rosenfeld, H. (1987). Impasse and interpretation: Therapeutic and anti-therapeutic fac-tors in the psychoanalytic treatment of psychotic, borderline, and neurotic patients.London: Tavistock.
Sabbadini, A. (1996, March 16). On sounds, children, identity and a ‘quite unmusicalman.’ Paper presented at a Study Day on Psychoanalysis and Music at the Centre

s in Ps
SS
S
S
Ashgate Publishing Ltd.Sutton, J., & McDougall, I. (in press). The roar on the other side of silence: Some
J. Sutton, J. De Backer / The Art
for Psychoanalytic Studies, University of Kent, Canterbury. Retrieved April 24,2008, from http://www.ukc.ac.uk/sdfva/sound-journal/sabbadini981.html.
troeken, H. (2000). Nieuw psychoanalytisch woordenboek. Amsterdam: Boom.utton, J. P. (2001). The pause that follows. . .Silence, improvised music & music
therapy. Nordic Journal of Music Therapy, 11(1), 27–38.utton, J. (2002). Music, music therapy and trauma: International perspectives. London:
Jessica Kingsley.utton, J. P. (2006). Hidden music: An exploration of silence in music and music
therapy. In I. Deliège & G. A. Wiggins (Eds.), Musical creativity: Multidisciplinaryresearch in theory and practice (pp. 252–271). East Sussex: Psychology Press.
ychotherapy 36 (2009) 75–83 83
Sutton, J. P. (2007). The air between two hands: Silence, music and communication. InN. Losseff & J. Doctor (Eds.), Silence, music, silent music (pp. 169–186). Hampshire:
thoughts about silence and the traumatic in music therapy. US: Satchnote Press.Williams, P. (2007). The worm that flies in the night. British Journal of Psychotherapy,
23(3), 343–364.Winnicott, D. W. (1971). Playing and reality. London: Routledge.