Embed Size (px)
Citation preview

The Arts in Psychotherapy, Vol. 22. No. 3, pp. 249-263, 1995 Copyright 0 1995 Else&r Science Ltd Printed in the USA. All rights reserved
0197-4556/95 $9.50 + .OO
Pergamon
0197-4556(95)00026-7
MUSIC THERAPY WITH A CLIENT SUFFERING FROM MUSICOGENIC
EPILEPSY: A NATURALISTIC QUALITATIVE SINGLE-CASE RESEARCH
HENK SMEIJSTERS, PhD and PIETER VAN DEN BERK, RMTh*
Abstract in Dutch
Met behulp van een aan kwalitatief onderzoek gekop- pelde vorm van actieve muziektherapie werd een clien- te behandeld die in haar leven als gevolg van psy- chotraumatische ervaringen musicogene epilepsie had ontwikkeld. Met name melodie leidde tot epileptische aanvallen. Zowel het koppelen van melodie aan ritme, het werken met voorgestructureerde melodi- sche motieven, als het gebruik van aleatorische mel- odische lijnen verminderde de kans op een aanval. De epileptische aanvallen waren rechtshemisferisch gelo- caliseerd. Het gegeven dat de cerebrale verwerking van ritme, het analytisch en aleatorisch verwerken van melodie niet rechtshemisferisch, de gestaltmatige verwerking van bekende of welgevormde melodieen daarentegen we1 rechtshemisferisch geschiedt, vormt een mogelijke verklaring hiervoor. Zowel structure- ring als aleatoriek waren succesvol, maar met name de laatste werd door de cliente ook emotioneel als zeer positief ervaren. Omdat de cliente zowel epilep- tische aanvallen bij ontspanning als activering on- derging, wordt de veronderstelling dat ontspanning en activering voorkomen dat prikkels het kritieke fre- quentiebereik van de epilepsie verspreidende neu- ronen bereiken niet bevestigd.
Musicogenic epilepsy, unlike spontaneous epi- lepsy, is a form of epilepsy that is evoked by a mu- sical stimulus. Critchley (1937) hypothesized that the epileptic seizure might be a conditioned response to a conditioned musical stimulus when there is a low threshold for epilepsy and a connection has been made between a stressful situation (that resulted in epileptic seizures) and music that was linked to this situation. Pascher and Rollin (1970), in reference to Teglbjaerg and Domnick, suggested this might be called “emotional epilepsy.” Shaw and Hill (1947) described the case of a client who used to turn on the radio during World War II in order not to have to hear the sirens. Musicogenic epilepsy developed after ep- ileptic seizure had begun to occur independently of any musical stimulus. The types of music that evoked the seizures were extremely varied. Pascher and Rollin (1970) concluded that the musical stimulus can be extremely varied. Bash and Bash-Liechti (1959) reported a client who, as a result of a stressful situa- tion, suffered from musicogenic seizures some years after epilepsy had begun to occur. The music that caused the seizure was a song the client was very fond of and that she heard during the event. Daly and Barry (1957) described the case of a client who used to hallucinate when listening to music as a child.
*Henk Smeijsters is Co-Director and Researcher at the Music Therapy Laboratory Nijmegen, Coordinator and Lecturer of the Music Therapy
Training Program Enschede, and Lecturer of the Music Therapy Training Program Nijmegen, The Netherlands.
Pieter van den Berk is Co-Director and Music Therapist at the Music Therapy Laboratory Nijmegen, Director of DICS and Lecturer of the
Music Therapy Training Program Nijmegen.
The authors thank the neurologists, the verbal psychotherapist, and the musician who participated in the peer debriefing group.
This research was funded by the Dutch Music Therapy Fund (Fends Muziektherapie) of the BUMA Association and the Hogeschool
Nijmegen.
249

SMEIJSTERS AND VAN DEN BERK
In the case described by Fujinawa and Kawai (1978), there was no connection between the song that induced the epileptic seizures and the client’s life history. These authors hypothesized that the meaning a person attributes to the music is of greater impor- tance than the actual presence of the music during a stressful event. Thus far it seems there are several possibilities. First, a specific piece of music can be linked to a stressful event. Second, not one specific piece, but music as such can be connected to a stress- ful event. Third, music is not connected to a life event by actual appearance, but by symbolic and/or emo- tional connotations. When thinking in terms of con- ditioning, the occurrence of a seizure to various and even unfamiliar pieces of music might be explained by stimulus generalization. However, this explanation does not hold when there seems to be no actual con- nection of any piece of music with a traumatic event in the client’s life history. If it is thought that the emotional meaning of music retrospectively was linked to a traumatic event, then this explanation only makes sense when indeed such an event has occurred. Eventually one might consider the possibility of re- pression of the traumatic event as a fourth possibility.
A fifth possibility comes from a very different per- spective when looking to cognitive information pro- cessing rather than emotional connotations. Accord- ing to Van den Bosch (1988), when automatic infor- mation processing is disturbed, hallucinations disappear when they are confronted with a well- constructed stimulus because this takes over from the disturbed information processing automatism. Based on this and assuming that seizures resemble halluci- nations, it might be hypothesized that structuring mu- sical stimuli could have a positive effect. Musical structure and musical instruments seem to be impor- tant. Forster, Hallgrim, Peterson and Bengzon (1965), in contrast to Fujinawa and Kawai, discov- ered that a piano version of a particular piece of music did not induce a seizure, whereas an orchestrated ver- sion of the same piece did. By an overview provided by Pascher and Rollin (1970), however, it can be concluded that more negative reactions are evoked by piano music compared to organ music, vocal music and symphonic music. According to Forster, Booker and Gascon (1967), seizures can be evoked by unfa- miliar music, but not by single tones. The fact that single tones do not induce seizures can be attributed to the occurrence of music-and not single notes- during the stressful situation, but it also can be ex- plained by the fact that the complexity of the infor-
mation that has to be cognitively processed or the emotional content differs with regard to music and single notes.
A final perspective that can be of help is the neu- rological difference between rhythm and melody. First, there is the fact that rhythm by the brain stem is linked to the autonomous nervous system (Scartelli, 1991). Second, rhythm is controlled by the left and pitch/tonality by the right hemisphere (Borchgrevink, 1983). Also the fact that the left hemisphere acts an- alytically and the right hemisphere holistically can be of importance (Marin, 1982). Brown and Fenwick (1989) and Fenwick and Brown (1989) suggested that there are “group two” neurons that enhance the spread of seizure activity by damaged “group one” neurons. These group two neurons are strongly de- pendent on the psychic condition of the person, which in turn depends on stimuli outside the person. Emo- tions and strong concentration activate group two neu- rons and thus can enhance seizure activity. It is sug- gested by these authors that the client can prevent epileptic seizures by using stimuli, cues like “relax” or “stop,” and making a fist during aura. They sug- gested further that relaxation and activation both can help group two neurons out of the “critical band of excitation,” the region of activity in which neurons are recruited into the epileptic discharge. In the opin- ion of Keyser (1994) and Sonnen (1994), only a small number of people are capable of suppressing a seizure by themselves. This can only be done if the individual feels the seizure coming on, which happens when a seizure is partial, focal and gradually spreading. Con- trol is only possible during the onset of the seizure (the aura).
In the literature, non-medical treatment is divided into behavioral therapy and insight-oriented psycho- therapy (Scott, 1977). After treatment by Bash and Bash-Liechti (1959) using extinction techniques, one of their clients was able to listen to any kind of music for 40 to 50 minutes. Forster, Hallgrim, Peterson and Bengzon (1965) desensitized the musical stimulus by gradually introducing the orchestrated version. For- ster, Booker and Gascon (1967), when playing the music during a seizure and during the subsequent pe- riod of confusion, used a flooding technique. Repe- tition of this procedure led to a normalization of the EEG and made the music innocuous. In the opinion of Sonnen (1994), desensitization by means of gradually increasing the duration of a piece is only possible in cases where the reaction is linked to a specific piece and where the reaction occurs rapidly. Daly and Barry

MUSIC THERAPY AND MUSICOGENIC EPILEPSY 251
(1957) found that after the termination of insight- oriented psychotherapy the seizures occurred 15 min- utes after the music began, whereas before treatment it had been 2 minutes. Joynt, Green and Green (1962) reported one case where psychotherapy was effective. Physical movement combined with decreased brain activity also can prevent seizures (Pascher & Rollin, 1970).
Research Method
The qualitative naturalistic single-case research method developed at the Music Therapy Laboratory is guided by criteria such as reliability, construct valid- ity, internal validity and external validity (Smeijsters, 1995). Because these criteria strongly differ in the way they are used in quantitative research, alternative definitions and techniques are used:
member check inside the team of participants by independent self-reports and observations from dif- ferent participants, a process of iterative feedback given by the music therapist and client to the sum- marized and analyzed data by the researcher, and dialectical interviews between researcher and mu- sic therapist; peer debriefing interviews with experts from other disciplines (neurologists, verbal psychotherapist, musician); repeated analysis by disciplined subjectivity (re- peated analysis of the interpretations by the re- searcher during the research process) and writing a detailed research report so that replication of the chain of evidence by another independent resear- cher will be possible. It includes: (a) summaries of all observations and self-reports; (b) the “focus points” (conceptualizations of the essential aspects of the disturbance that were developed); (c) memos (comments and hypotheses about diagnosis and treatment); (d) the action plan (indications, aims and objectives, techniques of music therapy de- duced from the focus points, suggested phases of treatment); (e) argumentations about effectiveness (connections and analogies between treatment, ef- fects, side-effects, disturbances, catalysts and sug- gested guidelines). Side-effects are unintended positive or negative effects of treatment. Distur- bances are factors from outside treatment that are counterproductive. Catalysts are factors from out- side that stimulate treatment. Guidelines are rules of thumb that may be used in similar cases.
Special qualitative aspects of the research method are:
open coding and hypothesis generating: develop- ing theory from practice in an ongoing process of refinement; weighting different theoreticallmethodical models for the “goodness of fit”; qualitative content analysis: searching for patterns, themes, recurrences in the data; triangulation: using different sources (client, mu- sic therapist, researcher, experts), using different data collecting techniques (self-reports, observa- tion reports, interviews) and using several theoret- ical models; negative case analysis: searching for data that do not fit the already existing interpretations; dialectical roles: splitting the roles of researcher and music therapist; musical analysis: searching for analogies between musical syntax, musical semantics and personal aspects.
Although the research is qualitative, the results will be registered quantitatively as to the number of sei- zures and the number of minutes of musical playing.
The Client
The client was a 40-year-old woman who since childhood had suffered from allergies and asthma. After her father died, the client experienced a psy- chotrauma and reacted by becoming asthmatic. She played the clarinet to express her feelings of grief. She left home. Soon thereafter she began to immerse herself in new experiences in order to “learn some- thing from my life,” as she put it. She joined medi- tation and therapy groups for three years and experi- enced a happy time. She later lived for seven years with her Japanese husband in Japan. Before her stay in Japan she had never suffered epileptic seizures. During her stay there she was physically assaulted by her husband. She used music to protect herself from an intolerable situation. Her non-musicogenic epilep- tic seizures began three years after she moved to Ja- pan. After her divorce and departure from Japan she learned that an acquaintance in Japan had attempted suicide as a result of her leaving. The musicogenic epilepsy began three months after her return to Hol- land, during a concert performance of the Matthew

252 SMEIJSTERS AND VAN DEN BERK
Passion. Before she started music therapy she moved from Amsterdam to a small rural village.
Previous neurological tests had shown that she had non-hereditary, localized epilepsy, beginning in the right mesio-temporal area. The EEG showed devia- tions in the delta waves (OS-4 Hz) and the theta waves (4-8 Hz). The seizure could be repeatedly in- duced by all kinds of music except compositions called “The Chinaconcert” and music from Kitaro (percussion and synthesizer music). The client could listen to one tape of Kitaro, not to other synthesizer music. External symptoms during the seizures were: increasing restlessness, hyperventilation, vocalizing, frequent swallowing, rubbing movements over sev- eral places of the body. The client was not completely unconscious. Non-musicogenic and musicogenic sei- zures took place both at night and during the day. They occurred suddenly; she did not feel them com- mencing. Frisium (10 mg twice daily) and Tegretol (200 mg four times a day) reduced the non- musicogenic seizures from 10 to an average of 4 a month. However, the medication had no effect on the musicogenic epilepsy. Movements like swimming, cycling and dancing evoked seizures too. The client was not able to influence seizures.
Musical Intake (sessions 1-5)
During the intake it became clear that the client had a good sense of rhythm, dynamics and tempo, and that she varied her playing. The client was able to associate to music. In session 5, a seizure occurred when arpeggio intervals, fragments of melodies and scales were introduced for six minutes on the piano and on the vibraphone in a fast tempo with no breaks. It was concluded from the intake sessions that rhythm functioned as a basis and that the client lost her bal- ance when melody was involved. She called it “being earthed” as opposed to “being directed upwards.”
Indication for Music Therapy
Avoidance of stimuli was not a feasible option due to the fact that the client’s seizures were caused by almost every kind of music. This would force the client to live an extremely isolated life. A neurochi- rurgical treatment, perhaps, would have been worth- while were it not for the client’s rejection, the diffi- culty of a specified location of the brain region and the presence of psychosocial indications justifying
psychotherapy. In considering the indication for a psychotherapeutic approach, especially music ther- apy, the following factors were significant:
0 the symbolic significance of musical instruments and musical elements;
l the possibility of rhythm functioning as the basis for desensitization.
Treatment
First Phase of Treatment: Imagery and Counterconditioning (Sessions 6-33)
1. Focus Points. The following focus points were formulated on the basis of the verbal and musical intake:
(a) The symbolic meaning of musical instruments and musical elements;
(b) The existence of unsafe and safe musical in- struments and musical elements.
2. Aims. The following aims were formulated on the basis of the focus points and the provisional literature study:
(a) Increasing insight into the symbolic meaning of music by means of imagery;
(b) The reduction of threatening musical stimuli by means of reciprocal inhibition with non- threatening musical stimuli.
Both approaches-the associative and the countercon- ditioning-were often used within one session. De- pending on the phase of therapy, a session centered around either association or training. 3. Process of Treatment: Imagery. An imagination that was used in the first sessions was “water and rock.” It reminded the client of a place in Japan where water came shooting out of a crack in a rock. This rock, she said, anchored her and satisfied her need to be near the ground. During the sessions she explored grounding images and instruments like gong and conga. When playing “the fear of a seizure,” she used high, dry sounding notes on the vibraphone, while the music therapist accompanied her softly on a cymbal and a rattle. The client repeatedly interrupted her own playing and reported being anxious, desper- ate and tearful and wanting to kick. By playing louder and faster on the gong and by playing low vibrating notes on the vibraphone, she drowned out the music therapist’s playing. In addition to her need to be grounded, she also described her wish to “open all my pores wide, being a hollow tube, letting in as

MUSIC THERAPY AND MUSICOGENIC EPILEPSY 253
much as possible as deeply as possible.” She also longed for the unexpected and surprising. She ex- plored this wish to be open using the gong, the vibra- phone and the drum. She described long sounding notes as, “a totality, something complete, perfect, an all-encompassing thing in which everything is possi- ble.” While exploring musical elements and associ- ations, gradually the following pattern began to emerge:
melody = boundary = closed = negative rhythm = grounding
long sounding notes = open = the cosmos= positive
When the client had seen a photograph of a Viet- namese soldier holding his dead baby wrapped in a rush-mat, this was used as a theme during session 14. She played on the cymbal, the solid bar chimes and drums at varying levels of intensity, with fortissimo beats on the cymbal, sometimes playing rolls and sometimes playing with both hands at once. The mu- sic therapist accompanied her on split drums. The music as a whole had a march-like character and the tension increased gradually. After a middle passage involving a crescendo on the cymbal and a restless passage on the solid bar chimes, there was a break during which the client cried. During the verbal re- flection of the session she told the music therapist that the music had been about “. . . the awful, the terri- ble, the insanity and aggression in life . . .” and the trouble she had accepting this. Although she denied any connection with her past in Japan, she neverthe- less talked about an abortion she had and she hypoth- esized that her epilepsy had started as a result of the batterings she had been subjected to. Some months later she added that fighting soldiers reminded her of how she was physically beaten. However, she stressed that her remembering the past was not an emotional effect only an intellectual one.
In session 2 1, the imagery “an elephant in a shop- ping center at night” was introduced. The client played on the kettle drum, conga, gong and vibra- phone; the music therapist on the vibraphone, solid bar chimes and temple blocks. The music contained fast passages with crescendi on the drum and gong, reminiscent of a dark jungle. When, in a second trial, the music therapist asked her if melody would be possible too, in a subsequent disco improvisation this indeed was possible. Now there was no dark jungle and the music sounded happy. The client commented, “Music is hate and love.”
Some conclusions that could be drawn from imag- ery were:
the client wanted to be grounded but also open; because of the musicogenic epilepsy she felt im- prisoned in present-day life; she abominated aggression she knew from history; melody was associated with the negative feeling of being imprisoned, whereas long-sounding tones and rhythm made her feel good.
4. Process of Treatment: Counterconditioning. Dur- ing the initial period, musical play centered on pure rhythm and melody grounded in rhythm (the client on congas and the music therapist on the metallophone playing single tones, intervals and short melodic mo- tives). Special techniques were:
attaching rhythms to snippets of melodies: here the client was able to direct the music therapist’s pre- arranged melodic motives by changing from one prearranged rhythm to another; expanding melodic material: while the client played the congas the music therapist played a rapid variation of melodic fragments, expanded melodic fragments with a few extra notes and took melodic fragments from familiar songs.
In sessions 15-33, training was the main focus. Duration of melodic playing increased and no seizures occurred except in session 17. Being able to change the melody by means of the rhythm gave the client confidence; this felt pleasurable and dissipated her anxiety. In session 15, it was possible to work with three connected rhythmical and melodic motives. By integrating these elements in the following form: 4 X A - 4 x B - 2 x C, a large musical whole was created including long melodic motives. In session 17, the scope of the training was broadened. While the client played a 6/8 rhythm or a march with a dotted rhythm, the music therapist played various me- lodic fragments in which one or more nuclei were constantly repeated, elaborated and/or varied:
f-d, f-d-b, f-d-c-d, f-d-e-c-d, d-f-e-c-d, d-f-e-g-f, a-g- e-f-d, d-g-e-f, d-a-f-g-e-f.
Variations of this were: the client playing the rhythm on the metallophone and the music therapist playing variations of scale fragments on the vibra- phone, and the client herself playing a melodic frag- ment on the metallophone. Even though the melodic

SMEIJSTERS AND VAN DEN BERK
events were unpredictable, there were no seizures for a long time. At the end of the improvisation, how- ever, when playing a change of key (e-e-d-d-c, f-f-e- e-d) a seizure occurred. Because of this seizure it was decided to limit the melodic material and to again increase the control and the rhythmical basis. This step backward in the conditioning procedure was ef- fective and, after some time, it became possible to introduce a key change in the first line of “What shall we do with the drunken sailor?” But it remained im- portant that the client be able to direct the behavior and that not too many successive or simultaneous changes were introduced. This, for instance, was done by a YES/NO game in which the client could decide when the music therapist was allowed to in- troduce a motive.
In session 22, the music therapist started with the production of tape recordings for at home use. The rationale was to make a transfer from music therapy to daily life. The client’s reactions showed that, when listening, she initially found the music chaotic, but through repeated listening and counting the melodic motives the music became more clearly structured for her.
In session 23, the music therapist for the first time introduced a cadence (I-IV-V-I). It made her nervous. However, when in session 24 one player played a rhythmic ground, the client herself introduced parts of a cadence on the vibraphone. When, in session 25, the music therapist played three different chords, ev- ery chord split up in two intervals, the client was unable to connect a different conga to a different chord. After one minute she started crying. She also felt the pitch of the congas did not go together well with the pitch of the vibraphone chords.
The alternation of playing solo or accompaniment in session 26 differed from conditioning because now the outline and not the details of the musical structure were pre-established. Every time the music therapist played a solo he used a different chord; when the client played solo she did it rhythmically. Listening to this tape caused a seizure. There were differences between playing at the session and listening at home. Passages where materials were expanded could lead to seizures at home. Seizures at home were caused also because she could not stop listening. Other causes were stress factors occurring at the same time, such as visits, her birthday and a trip to a big city. In her self-report the client wrote that she had problems with quick changes. There seemed to be an analogy between changes in the music and changes in her life
situation. From session 26 on, spontaneous seizures and seizures while cycling again happened.
Problems with chords occurred when there were too many intervals from too many different chords on different pitches, too quick changes between those intervals and between the solo and accompaniment sections. When, as in session 27, the music therapist decided to play only three intervals from three chords, quick changes were no problem. In session 28 and 29, two congas and up to three drums were linked to five intervals from different chords on the vibraphone. The client played the percussion instruments, the mu- sic therapist the vibraphone. Leading and following were alternated. Alternations between intervals were very quick.
In sessions 30 and 3 1, the client introduced tones of different chords (f-a-des, f-as-des, e-a-cis) on the split drum. The music therapist used the same chords and rhythmically played accents or supplemented her rhythms on the vibraphone. They both experimented with sound effects and changes in tempo and dynam- ics. The client described the play as hodge-podge, and “ . . . very funny and playful.” She no longer liked the structured conditioning procedure where rhythmic fragments grounded and were attached to melodic fragments, and one player had to follow the other. What became especially important now was that the music could give her the feeling of playfulness and freedom she longed for. In session 32, the music ther- apist introduced the piano while the client on the split drum was playing ostinati and variations of the chords e-a-cis and e-g-cis. The music therapist played long- standing or broken intervals of these chords as a back- ground. They also used instruments like congas, cow- bell, triangle, cymbal, hand drum and others. It sounded like a modem art musical composition. Now the piano gave the client a feeling of waves that could take her away.
At this time she read a book about psychotrauma and felt fully understood and accepted by the author. At the start of music therapy, she had said that she thought that musicogenic epilepsy was a result of her past experiences. Now she found affirmation and ex- perienced better insight.
Some conclusions that were drawn from condition- ing were:
l rhythm satisfied her need for grounding and she was able to ground melody;
l using melody was possible when melodic motives were pre-established, linked to pre-established

MUSIC THERAPY AND MUSICOGENIC EPILEPSY
rhythms and the client could direct the melodic change or the melodic change was predictable; expanding melody by elaboration or variation, when grounded in rhythm, was possible; changing of key was possible; cadence was possible when there were not too many chords, not too many intervals in each chord and not too quick changes; tapes with elaborated musical material and stress factors at home caused seizures; there seemed to be feelings about her traumatic experience that needed expression; at the end of the first phase, experiencing freedom in musical improvisation became important.
Second Phase of Treatment: Musical Freedom, Freedom in Interaction and Grieving (Sessions 34-5 1)
1. Focus Points. (a) feeling restricted by conventional musical
structures; (b) grief about her handicap, the sense of life, a
lot of feelings; (c) being the victim of power in relationships, ex-
periencing no freedom in interaction, subordi- nating herself to others.
2. Aims. (a) experiencing freedom of melodic unintended
play; (b) expressing grief; (c) experiencing freedom in relationships.
3. Process of Treatment: Freedom of Melodic Unin- tended Play, Expressing Grief and Freedom in Rela- tionships.
During summer holidays most of the seizures were caused by activities such as: singing, cycling, reading the psychotrauma book, reading a journal, thoughts about dying. After summer holidays the client criti- cized some of the hypotheses by the researcher and felt confronted by them. This moment of tension, however, led to the new insight that when she felt forced into an idea it made her unhappy.
In cooperation with the client two decisions were made:
(a)
(b)
because of her deep emotional reactions to the psychotrauma book she was referred to a special- ist in the psychotherapy of grieving. From then on she had one session of verbal psychotherapy ev- ery second week; in music therapy a new phase was started where instead of structure, freedom was the main focus.
In session 35, she played on a tree of bells. She played from a musical perspective (a deep sound as a basis), from imagery (“rain,” “storm” and “sun”) and from interaction (imitation, complementary rhythm, question and answer). For the the first time she reported that she disliked the synchronizing play by the music therapist. She wanted openness, no boundaries. In her self-report she wrote, “I do not like boundaries, but perhaps I need them; I love open- ness, but this can cause a seizure.” Later on she had doubts about this sentence.
In session 36, the music therapist used the con- cepts “figure and background.” He explained to her that when a melody becomes a figure it becomes a problem. She agreed by saying, “As long as there is no structure and I can go everywhere it is okay.” In the first phase of treatment, when a melodic figure came up, it was possible to counteract it by an ana- lytic handling of melody and connecting it with a rhythmic background. In the seond phase of treat- ment, however, this changed completely because she disliked the organized play. She no longer wanted to play a rhythmic background nor a melody being forced into a structured figure.
The idea of “figure and background” had struck her. She went home thinking a lot about it and wrote in her self-report, “Figure is power; I hate power. I am afraid that somebody has power over me. I think about death, I am anxious. ” It emerged that melody as figure was associated with power. This association could be understood because of the fact that melody caused seizures, and seizures are very powerful. But she also hated the abuse of power by human beings. There seemed to be a pattern where melody, seizure, power and interaction were connected. Melody was associated with power because of seizures, and inter- action was felt as aggressive power that caused epi- lepsy and musicogenic epilepsy. Melody played by another person especially was a situation where she suffered from power.
While listening to melodic fragments from session 36 (she on bell tree and the music therapist on vibra- phone) on tape, she suffered seizures. It made her sad because she thought she never could pass these mu- sical boundaries. But, as in the first phase, some of these seizures probably happened because she forced herself to listen several times. Also now, there emerged the association of power when the music therapist played melody. She wrote in her session report, “Can it be that I am struck by something, try to hide it and then have a seizure?”

256 SMEIJSTERS AND VAN DEN BERK
In session 38, the music therapist repeated the bell tree and vibraphone play where he himself played less melodic intervals and made interruptions with the conga and rests. Now the client felt very easy, and listening at home (45 minutes without repetitions) was okay. She experienced that her own variable melodic play acted as a background.
In session 39, several new aspects developed. First there was a very dynamic interaction play on one cymbal with quick taking turns. Although she liked this, during the entire session she felt like crying. A circle play was introduced where instruments were placed in a circle and music therapist and client were free to choose. Suddenly she looked at the vibraphone and said, “I am angry with this.” Immediately she started to play rubbing the sticks on different places of the vibraphone. After that she played a lot of very long-sounding tones that were mixed. The music ther- apist contained her play with loud sounds on the same instrument and the play developed into a cathartic expression of anger. At the end of the play she started talking about the sense of being alive. Because of her handicap, she no longer found life significant and started to cry. In this session, she expressed feelings of anger and sadness; she grieved about her handicap. In her session report she wrote that the expression of anger felt very good, but that she did not expect this could be of any help.
In the following session, the powerful and free play on the vibraphone was transformed by using dif- ferent feelings, fixing the duration of the play and using a rondo form. The music therapist felt tension because of the ever-changing melodic play of the cli- ent. He was unable to give it a musical structure and described her melodic play as almost unrecognizable, without melodic development. The client, however, loved this kind of music with no fixed rhythm and melody. She did not want to stay in one feeling and said, “I do not want to be in borders; I am full of emotions; I want to express all impressions together. I am afraid to continue in the same melody. ”
The tape from session 40 had a very positive effect on her. She played very free on the vibraphone, split drum and conga while the music therapist indepen- dently played the cymbal, woodblock and gong. When in other sessions she felt forced into conven- tional musical structure or forced herself into musical structure because she wanted to please the music ther- apist, these tapes could cause seizures. For instance, in session 42, she played diatonic and chromatic me- lodic and harmonic lines on the piano (transposition,
reversals, symmetries, extensions, sequences). It sounded as a well-formed piece of modem music. At home she experienced a seizure when listening to this session, and in her self-report she wrote that she forced herself to play melodic lines. At the same time she had a hard time because she was confronted with cancer and death among her acquaintances. These stress factors also were responsible for seizures. Other aspects that contributed to seizures at that time were fatigue, experiencing too many impressions at one time, listening to the tapes too often and reading or thinking about death.
Concerning grieving, several aspects now were combined-there was the grief about her handicap (see the feeling of anger in session 39)) the grief about her psychotrauma (see her reaction when reading the book), and the grief about the death of acquaintances (the feeling of dismay she had at the beginning of session 42). Because death played an important role in her life, in session 44 it was taken as the theme of an improvisation. The music therapist in a threatening and frightening way played at the piano, ending with powerful and screaming low sounds symbolizing the end. The client played “The Heaven” on the vibra- phone and alternated this with a march. Together it sounded like a Mahler symphony where the treadmill of life and the inexorable end of life are confronted with the wish for a careless life in heaven. While listening at home the client suffered several seizures from this death play, but again music alone was not responsible because it was at the same time that two of her acquaintances had died.
In one of her self-reports, the client told about her painting group where she wanted to cross borders too. Her music also symbolized her need to lead an un- conventional life, not living in the center, but at the extremes, not wanting to remain in only one state of feeling, but experiencing many feelings. When a mel- ody became a figure on a ground, she did not like it and even feared it. At that time the client did not tell why she told this story. After some time, when it became clear that the therapy process again was changing, she said she had told the story about the painting group because she felt her music was not understood in music therapy.
When, in session 45 the music therapist imitated the rhythm of a clock, the client introduced herself; because of the repetition, the music became struc- tured and she felt like crying. She asked for more variation in the music therapist’s playing. Again there were several seizures because of an interaction of

MUSIC THERAPY AND MUSICOGENIC EPILEPSY 251
sickness, bad news, her feelings of despair and lis- tening too long to unsafe fragments of music.
In session 46, the music therapist played on a split drum and conga as the client played on the vibra- phone. They both played without structure. Playing together occurred spontaneously, was not intended, and the client liked it, but felt misunderstood. Be- cause, in session 47, these moments of alternately playing together and not playing together also devel- oped spontaneously, and because there were a lot of tones and a loose structure where the client experi- enced feelings of freedom and the music therapist was unable to lock her up musically, this session, like session 40, became a very safe tape, without seizures at home. The client-playing on the vibraphone me- lodic motives up to six tones and leaps in a very free manner-sometimes synchronized her play with the rhythmic foreground play of the music therapist who played South American rhythms on the conga, but also freed herself from this play again.
While listening to the tape of session 48, the client experienced several seizures. Session 48 had been a session with parts where music therapist and client were musically independent and parts where they were very close. For instance, the client played a melodic ostinato and the music therapist played a me- lodic motive or the client played a melodic contour and the music therapist played its inversion. There also was imitation with a lot of tones. During session 49, the client started crying and talked about all the bad things in her daily life. She again experienced feelings of grief. In session 50, she suffered a seizure during a “safe” play. This play, however, followed a musical interaction that had been very intensive and powerful. The client played melodic motives with ac- centuations at the end on the vibraphone; the music therapist played powerful melodic statements on the piano and there was tuning and reciprocity. The title of the play was “The Music Therapist in the Client’s Meadow.” During the seizure in session 50, the client used the cue “Stop,” but was not able to stop the seizure. Saying “Stop” decreased the pain in her chest. At home she suffered a seizure while listening to this musical play.
After this session, it was concluded that there should be two different “meadows.” Playing in an- other person’s meadow by the client or letting another person in the client’s meadow reduced her freedom. It now became clear that the safe music (like sessions 40 and 47) was characterized by unstructured melodic play, and the unsafe music (like session 48 and 50) by
synchronized or interactive musical play. The video- tapes were analyzed by a musician specialized in 20th century music (Saladin, 1995). He described the cli- ent’s play as:
0 very soft dynamics; 0 little (like short piano pieces); 0 no clear tonality like Hindemith or Webem 0 strong tension curves; 0 transparent; l without passion.
He described the musical play of the music thera- pist as disturbing the play of the client. The client felt that session 40 had been very important for her and that she wanted to explore this musical play. Al- though the music therapist tried to continue it, except in session 47, he did not succeed. He described how terribly difficult it was to go into her free musical play and, at the same time, grounding it and thus prevent- ing seizures. He experienced a double bind.
The possibility to go deeper into her feelings and to work through her psychotrauma also was considered. Because the client was submissive and always trying to please others, and feeling down when being over- powered by events in her environment, setting bounds to overwhelming impressions seemed to be more im- portant. After peer debriefing with her verbal psycho- therapist and several talks among the music therapist, the client and the researcher, it was decided to make a break in music therapy. There was one final session to say goodbye. Music therapy for the time being was counter-indicated because giving space to herself and strengthening her boundaries in music therapy would be difficult due to the risk of seizures. Also, reading the research report sometimes made her feel overpow- ered. Experiencing a seizure always had a negative influence on her ego-strength. Also, reading the re- search report acted upon her ego. After an interlude of verbal psychotherapy, music therapy was continued.
Some conclusions drawn from interaction and grieving were:
0
0
when she felt forced into another person’s musical play she felt unhappy; there was an analogy between being forced into a musical structure and being forced into feelings, conclusions and music. She disliked the synchro- nizing play by the music therapist and she disliked a melody being forced into a structured figure;

258 SMEIJSTERS AND VANDENBERK
l melodic figures were associated with power be- cause of seizures;
0 interaction was connected with aggression and power because of her psychotrauma;
0 melody played by another person was connected with seizures and power in relationships;
l seizures were evoked by a combination of stressful events in daily life, listening too long and the as- sociation of power;
0 the client was able to express anger, sadness and despair about her handicap;
0 playing in an unstructured interaction, where play- ing together occurred unintentionally, was safe.
Effects, Side Effects, Disturbances and Catalysts
Effects
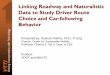
By linking melody to rhythm it was possible to extend the duration of the rhythmic or combined me- lodic and rhythmic playing without causing seizures (sessions 611). When melody was extended too much or melody was played alone, seizures occurred
Fits 17 per 16 week 15
14 13 12 11 10 9 8 7 6 5 4 3 2 1 0
musical intake I
12 3 4* 5 7 8 9 10 11* 12
Legenda:
n u seizures
I rhythm alone
I extension of
start treatment
I
on the day of the music therapy session, at home before or after the session (sessions 14-20). One sei- zure happened during session 17.
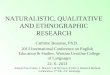
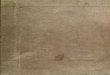
When melody or harmonics again were combined with rhythm, seizures diminished (sessions 21-35). Most of the seizures during this period occurred be- cause of events outside music therapy (singing at home, inviting persons at home, visiting the city, cy- cling, imagination, reading about psychotrauma, thinking about death or power). Several seizures hap- pened when listening to the melodic tapes without the stimulus of special events (for instance, tapes 36, 37, 39). Session 40 was a turning point. It was experi- enced as a very valuable tape, but, because the music therapist was not able to combine freedom and grounding, sessions 40-50 increased seizures. There also were seizures linked to events outside music ther- apy (death of acquaintances, reading about death, be- ing tired or sick, cycling), but now sessions and tapes became divided into “bad” and “good” tapes. The tapes of sessions 42, 44 and 48 were bad. The tapes of sessions 40 and 47 were good. As in session 17, the bad sessions culminated in a seizure during session 50 (See Figures l-3).
or rhythm combined with melody
melody or melody alone
17 Minutes 16 of improv. 15 14 13 12 11 10 9 8 7 6 5 4 3 2 1 0
15 16 Sessions
* holidays / illness (after 11 one week, after 12 two weeks) A musical play with an association or associations outside music
therapy S shopping Si singing outside music therapy
Figure 1. Duration of improvisations and number of seizures (1-16).

Fits 25 per 24 week 23
22 21 20 19 18 17 16 15 14 13 12 11 10 9 8 7 6 5 4 3 2 1 0 *17 18 19 20
Legenda:
# A
Si V I
General Effects
the extension of the duration of rhythmic playing; the extension of the duration of melodic playing combined with rhythm;
MUSIC THERAPY AND MUSICOGENIC EPILEPSY 259
.
I . . 25 Minutes of . . 24 improv.
. . 23
. . 22
. . 21
. . 20
. . 19
. . 18
. . 17
. . 16
. . 15
. . 14 1.113 . . .rl2 __
22*23 24* 25 26*27 28 29 30 31 32 * Sessions
seizures rhythm alone or rhythm combined with melody
extension of melody or melody alone
harmonics (with rhythm)
holidays / illness (before 17 one week, after 22 three weeks, after 24 two weeks, after 26 one week, after 32 summer holidays) verbal session musical play with an association or associations outside music therapy singing outside music therapy visits threatening instrumentation (e.g. piano)
Figure 2. Duration of improvisations and number of seizures (17-32).
drive to subordinate in relationships dominate her life-script.
Side Effects
the elaboration of melodic playing combined with Unintentional negative effects of the music therapy rhythm; were: the extension of the duration of music listening outside music therapy; 0 making free hidden feelings as a result of trauma; 0 making free feelings of grief about her handicap; experiencing a need to be unconventional and mu- sically free;
three seizures during music therapy sessions; seizures outside therapy, while listening to the tapes, caused by a combination of melodic or in- teractional elaboration during the session and other psycho-social variables;
experiencing that power in relationships and her 0 the client, sometimes in the musical improvisation

260 SMEIJSTERS AND VAN DEN BERK
Fits 25 per 24 week 23
22 21 20 19 18 17 16 15 14 13 12 11 10 9 8 7 6 5 4 3 2 1 0 33 34 35 36 37 38 3
CF
Legenda:
0 !I#
I ::: :::
ii A
I F T E C
seizures rhythm alone or rhythm combined with melody
extension of melody or melody alone
melodic aleatory
holidays / illness (after 40 one week, after 48 three weeks) verbal session (after session 50 there were three verbal sessions) musical play with an association or associations outside music
therapy threatening instrumentation (e.g. piano) musical form playing together (figure-ground, question-answer, imitation, echoing) sound effects playing clusters
Figure 3. Duration of improvisations and number of seizures (K&51).
with the music therapist and during member check with the researcher, felt overpowered. This trans- ference, however, contributed to therapy because it became clear that there was a problem of power and subordination in relationships. The client, be- cause of her psychotrauma, projected power in re- lationships and subordinated herself when she feared being “hit.” The transferences were coun- terproductive when the “grounding” of the music therapist felt like being misunderstood or being hit; the client felt disturbed when, because of deadlines for a congress and funding, there was no time to review a video and a paper made by the music therapist and researcher.
Disturbances
Among events outside the therapy that may be con- sidered to have had a negative influence on the pro- cess are:
0 her negative relationship with her neighbors be- cause of her musicogenic epilepsy;
0 her inability to participate in activities outside her home. Her domestic situation exerted a negative influence on her resistance and on her expectations with regard to therapy;
0 the negotiations with insurance companies, which meant that possible positive effects from music therapy were unwelcome;

MUSIC THERAPY AND MUSICOGENIC EPILEPSY
0
0
her repeated singing, and listening too long to the tapes at home, which caused her to violate her own boundaries and produced seizures; seizures at home before sessions. Then she felt bad when coming to music therapy.
Catalysts
0 reading a book about psychotrauma.
Guidelines
0
0
0
0
0
0
0
0
0
0
Music therapy techniques that can be used:
*Musical grounding techniques:
the use of secure images while improvising; the counterconditioning or shading of melody by using rhythm; predictability: deciding beforehand which motives would be played and in what order; the synchro- nous connecting of short melodic and rhythmic mo- tives that were arranged beforehand; the repetition of intervals and chords; not simultaneously using too many chords that are split up in intervals with too wide pitches. Although predictability caused no seizures, the client disagreed with the hypothesis that this happened because she knew what hap- pened. She said, “I don’t know what is happening in music, and if you split up melodies in parts I don’t like it.” fragmentation: dividing existing melodies into small, well-structured gestalts; melodic chain formation: the gradual expansion of three tone motives while repeating musical cells in improvisation; conservation and variation: certain elements are kept constant while others are varied. This can be arranged synchronously (one parameter remains constant while the other changes), sequentially (variations are inserted between parts which remain constant) or synchronously and sequentially (e.g., a steady rhythm linked to a melodic rondo); using an overall rondo structure: alternating play- ing on melodic and percussive instruments, alter- nating solo and accompaniment (in a combination of melodic and percussive instruments), alternating leading and following; tuning rhythmic and melodic instruments; the use of breaks and slow tempo; no quick changes between different musical parts;
0 the possibility of the client to direct musical struc-
ture: the client determines when and which melodic fragment has to be played;
0 preparing home listening tapes in music therapy; 0 an analytical listening attitude: while listening at
home the client has to count the different types of musical motives;
0 preventing or limiting spontaneous singing at home.
*Techniques of symbolizing:
0 the exploration of the symbolic meaning of mu- sical instruments, musical elements and musical interaction;
0 using metaphors like “playing in your own meadow.”
*Techniques of aleatory:
0 playing without conventional musical structures and without conventional musical interaction, play- ing at random, without rules.
Discussion
When reviewing the literature it can be concluded that this case affirms the concept of conditional or emotional epilepsy (Critchley, 1937; Keyser, 1994; Pascher & Rollin, 1970; Shaw & Hill, 1947). There were several indications that the musicogenic epilepsy was caused by the client’s psychotraumatic experi- ence. The reasons for this are: (a) the client as a child already had a low threshold for psychosomatic reac- tions to stress; (b) epilepsy and musicogenic epilepsy started after the occurrence of maltreatment; (c) mu- sicogenic seizures followed non-musicogenic sei- zures; (d) music had been used as consolation during maltreatment; (e) melody as a figure before a back- ground was symbolized with power; (f) the client was emotionally moved by music; (g) a fixed stimulus necessary for reflex epilepsy was absent; (h) the client herself felt that musicogenic epilepsy was caused by her maltreatment; and (i) seizures that happened at home many times were caused by a combination of variables (listening to tapes, having associations, ex- periencing stress at home and so on).
The client always longed to live an unconventional life, crossing borders. When she was maltreated she was locked up in a very narrow emotional space. Her body reacted to this by developing epilepsy and mu- sicogenic epilepsy. Seizures itself also exerted power

262 SMEIJSTERS AND VAN DEN BERK
and thus well-structured melody became associated with power and evoked feelings of being imprisoned.
When playing music she avoided melody and structure to avoid being imprisoned. The feeling of being in prison was transferred to her musical inter- action with the music therapist. In this interaction she longed for musical play where everybody plays from their own self, not trying to influence the other’s play musically and not being influenced by the other. Be- cause being forced into a musical structure was felt as if being imprisoned in daily life, this case supports the theoretical concept that in music therapy there is an analogy between musical processes and personal pro- cesses; that mental disorders are expressed in musical play and can be treated through musical processes (Smeijsters, 1993).
There were some indications that the client had not worked through her psychotrauma. She reacted very intellectually when talking about her past and she felt no emotions, but she cried when she read a book about psychotrauma, and often was thinking about death. Thinking about death was also a result of her frustrating daily life, and negative associations with melody were caused by seizures. Because seizures were likely when there were more than three melodic tones, too many harmonies and intervals, when there was quick tempo and quick changes, when music lasted too long, there seemed to be also a difficulty with cognitive processing on the part of the client. This, however, seemed to hold true only when con- ventional musical structure was aimed at and she felt forced into a developing conventional melodic struc- ture or forced herself into it. She reacted to this by saying that maybe, because of the emotional stress, more cognitive effort was required. When there were pre-composed short musical motives without devel- opment or aleatoric play, and when she did not follow the music therapist’s structure, there was less negative emotion, less cognitive tension and no cerebral reac- tion that caused stimulation of the vulnerable area.
Musicogenic epilepsy can be treated by extinction techniques and by cognitive techniques, which dose, structure and make predictable the flow of informa- tion. A structured flow of stimuli keeps the flow of information under control (Van den Bosch, 1988). Desensitization was possible also when seizures were not linked to fixed musical motives. But these tech- niques need to be supported by symbolizing tech- niques and techniques of aleatory. At termination of treatment the client felt that using musical structure emotionally was not satisfying. She wanted freedom
of musical play and not curtailment. She also felt extinction techniques were directed at symptoms only.
The client experienced no aura and was not able to influence the seizures by using keywords. With the help of keywords it, however, was possible to lessen some effects of seizures. Because seizures happened during states of relaxation and states of activity they do not corroborate Brown and Fenwick’s (1989) hy- pothesis that relaxation and activation both can keep group two neurons out of the “critical band of exci- tation.” However, when musical play was very well- structured and predictable (in the first phase) or com- pletely at random and unintended (in the second phase), the client experienced a cognitive and emo- tional state that was able to reduce the activity of group two neurons and thus to inhibit seizure activity.
Because the client’s epilepsy was located in the right hemisphere, the explanation for the effect of rhythm is that rhythm affects the brain stem and the left hemisphere, whereas pitch, tonality and melody affect the right hemisphere. Unstructured melodies are different from “gestalt-like” melodies, which are processed by the holistic right hemisphere.
A final comment-because in this type of research the researchers interact with the clients, but not as therapists, this interaction can cause positive or neg- ative side effects. When the researchers act as thera- pists they disturb the division of roles between music therapist and researcher, but when researchers act as scientists, clients can feel misunderstood or con- fronted when checking the interpretations of the re- searchers. This can lead to transference between cli- ents and researchers. Especially when clients need self support and emotional boundaries to the environ- ment, being confronted by the research report can be counterproductive.
References
Bash, K. W., & Bash-Liechti, J. (1959). Die Psychotherapie eines Falles von musikogener Epilepsie [The psychotherapy of a case of musicogenic epilepsy]. Schweizerisches Archiv fiir Neuro- logic und Psychiatric, 83, 196221.
Borchgrevink, H. M. (1983). Prosody and musical rhythm are con- trolled by the speech hemisphere. In M. Clynes (Ed.), Music, mind and brain. The neuropsychology of music (pp. 151-157). New York: Plenum Press.
Bosch, R. J. van den (1988). De smalle marges van de schizofrene patient. Over symptoomcontrole en zelfbescherming. [The nar- row margins of the schizophrenic patient. Controlling symp- toms and self protection]. Maandblad Geestelijke Volksgezond- heid, 10, 1067-1078.

MUSIC THERAPY AND MUSICOGENIC EPILEPSY 263
Brown, S. W., & Fenwick, P. B. C. (1989). Evoked and psy- chogenic seizures: II. Inhibition. Acra Neurologica Scandina- via. 80. 541-547.
Critchley, M. (1937). Musicogenic epilepsy. Brain, 60, 13-27. Daly, D. D., & Barry, M. J. (1957). Musicogenic epilepsy: Report
of three cases. Psychosomatic Medicine, 19, 399. Fenwick, P. B. C., & Brown, S. W. (1989). Evoked and psy-
chogenic seizures. I. Precipitation. Acra Neurologica Scandi- navia, 80. 535-540.
Forster, F. M., Booker, H. E., & Gascon, G. (1967). Condition- ing in musicogenic epilepsy. Transactions of the American Neurological Association, 92, 236237.
Forster, F. M., Hallgrim, K., Peterson, W. G., & Bengzon, A. R. A. (1965). Modification of musicogenic epilepsy by ex- tinction technique. Transcriprs of the American Neurological Association, 90, 179.
Fujinawa, A., & Kawai, I. (1978). Ueber musikogene Epilepsie. [On musicogenic epilepsy]. Psychiarria clin., I I, 47-59.
Joynt, R. J., Green, D., & Green, R. (1962). Musicogenic epi- lepsy. Journal of the American Medical Association, 179(7), 125-128.
Keyser, A. (1994). Personal communication. Nijmegen: University of Nijmegen.
Marin, 0. S. M. (1982). Neurological aspects of music perception and performance. In D. Deutsch (Ed.), The psychology of mu- sic (pp. 453477). Orlando: Academic Press.
Pascher, W., & Rollin, H. (1970). Akustische Reflexepilepsien. [Acoustic reflex epilepsies]. Der Nervenartz, 41(2), 68-72.
Saladin, A. (1995). Musical analysis of session 47 and 50. Nij- megen: Hogeschool Nijmegen.
Scartelli, J. P. (1991). A rationale for sub-cortical involvement in rhythmic response. In C. D. Maranto (Ed.), Applicarions of music in medicine (pp. 29-40). Washington: The National As- sociation for Music Therapy.
Scott, D. (1977). Musicogenic epilepsy. (2) The later story: Its relation to auditory hallucinatory phenomena. In M. Critchley & R. A. Henson (Eds.), Music and rhe brain (pp. 354-364). London: William Heinemann Medical Books.
Shaw, D., & Hill, D. (1947). A case of musicogenic epilepsy. Journal of Neurology, Neurosurgery and Psychiatry, 10. 107- 117.
Smeijsters, H. (1993). Music therapy and psychotherapy. The Arts in Psychotherapy. 20, 223-229.
Smeijsters, H. (1995). Qualitative single-case research in practice: A necessary, reliable and valid alternative for music therapy research. In M. Langenberg, J. Frommer, & K. Aigen (Eds.), Qualitative approaches to music therapy research: Under- standing processes and dialogues from the first infernational symposium. Phoenixville: Barcelona Publishers.
Sonnen, A. E. H. (1994). Literature investigation of musicogenic epilepsy. Breda: Hans Berger Kliniek.