Embed Size (px)
Citation preview
215Bulletin of the NYU Hospital for Joint Diseases 2011;69(3):215-9
Jain M, Samuels J. Musculoskeletal ultrasound as a diagnostic and prognostic tool in rheumatoid arthritis. Bull NYU Hosp Jt Dis. 2011;69(3):215-9.
Abstract
The use of musculoskeletal ultrasound (MSKUS) has increased in a variety of rheumatic conditions, particularly rheumatoid arthritis (RA). MSKUS complements the physical examination by allowing for superior visualization of synovitis and erosive changes compared to conventional radiography and provides detail comparable or supplementary to magnetic resonance imaging (MRI). This modality is also less expensive than MRI and CT scans, without claustrophobia or other contraindications, while uniquely providing dynamic, rather than static imaging. A growing body of literature for MSKUS in RA is contributing significantly to the understanding of diagnostic and prognostic utility, longitudinal assessment, and disease remission. Furthermore, scoring systems focusing on the patient level rather than individual joints have been developed, allowing for simplification of exams while still retaining accuracy and utility. The combination of these advances has led to increased use of MSKUS in RA in the realm of research as well as at the bedside and in the clinic.
The use of musculoskeletal ultrasound (MSKUS) as a diagnostic and management aid in rheumatic disease, prevalent in Europe for many years, has garnered
significant interest in the United States more recently. Musculoskeletal ultrasound provides useful information that complements the physical exam and often surpasses the diagnostic utility of plain radiography. Musculoskeletal ul-
trasound also offers advantages over other advanced imaging techniques such as magnetic resonance imaging (MRI) and computed tomography (CT), including its relative inexpense, the lack of contraindications from claustrophobia or metal implants, the ability to dynamically image the affected area, and relative ease of imaging contralateral or additional areas spontaneously when clinically indicated.1,2 Technological advances have also augmented the value of MSKUS in rheumatic diseases, including improvements in grayscale imaging (which is based on the visible contrast from struc-tures appearing as shades of black, gray, and white), and more sensitive power Doppler setting—a modality which, as discussed below, can provide improved assessment of acute inflammation.3
In this review, we focus on the key sonographic find-ings in rheumatoid arthritis (RA) and the clinical utility of MSKUS in both acute and chronic stages of this disease, before and during therapy. The benefit of MSKUS in guid-ing needle-based procedures for RA and other diseases is well-documented in the literature so in this review we will focus on MSKUS primarily as a diagnostic tool.
Synovitis and TenosynovitisSensitive and accurate assessment of joint inflammation is vital to the management of RA. Many investigators have vali-dated sonographic evaluation of synovitis in RA at multiple anatomic sites including: shoulders,4 wrists and small joints of the hands,5,6 knees,7 and feet.8 Other efforts have shown MSKUS to be reliable across anatomic sites with respect to both intra-observer and inter-observer concordance.9,10
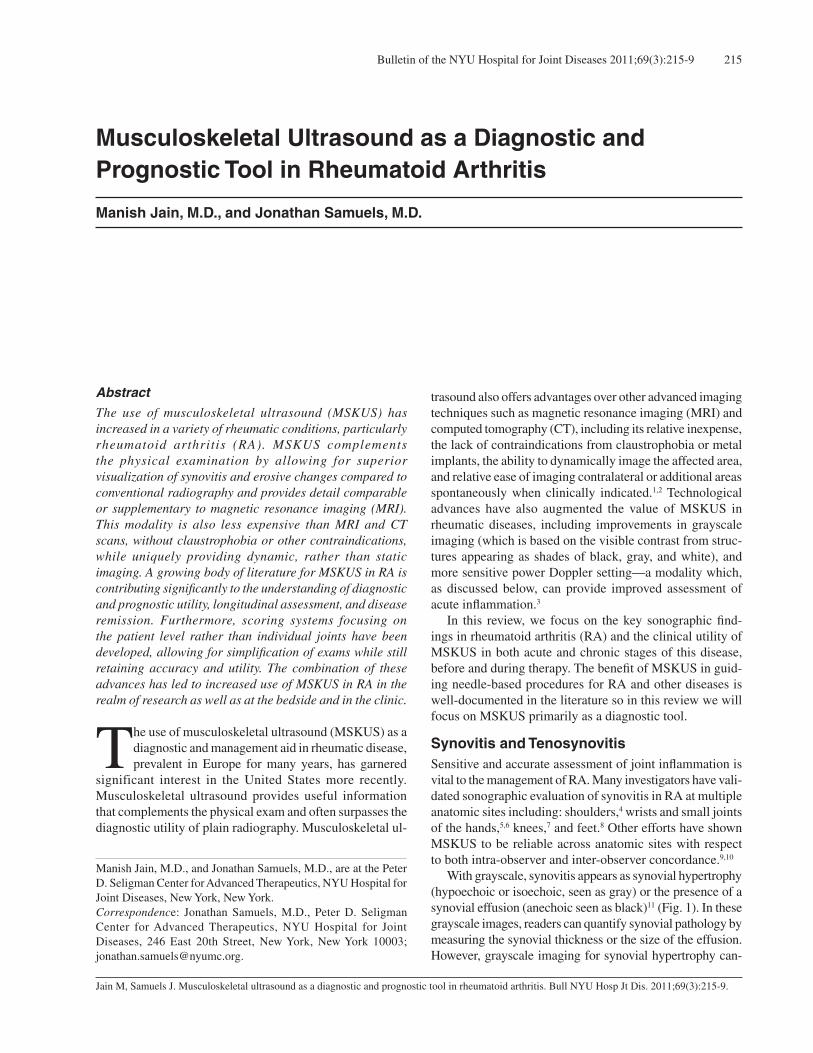
With grayscale, synovitis appears as synovial hypertrophy (hypoechoic or isoechoic, seen as gray) or the presence of a synovial effusion (anechoic seen as black)11 (Fig. 1). In these grayscale images, readers can quantify synovial pathology by measuring the synovial thickness or the size of the effusion.However, grayscale imaging for synovial hypertrophy can-
Musculoskeletal Ultrasound as a Diagnostic and Prognostic Tool in Rheumatoid Arthritis
Manish Jain, M.D., and Jonathan Samuels, M.D.
Manish Jain, M.D., and Jonathan Samuels, M.D., are at the Peter D. Seligman Center for Advanced Therapeutics, NYU Hospital for Joint Diseases, New York, New York.Correspondence: Jonathan Samuels, M.D., Peter D. Seligman Center for Advanced Therapeutics, NYU Hospital for Joint Diseases, 246 East 20th Street, New York, New York 10003; [email protected].
Bulletin of the NYU Hospital for Joint Diseases 2011;69(3):215-9216
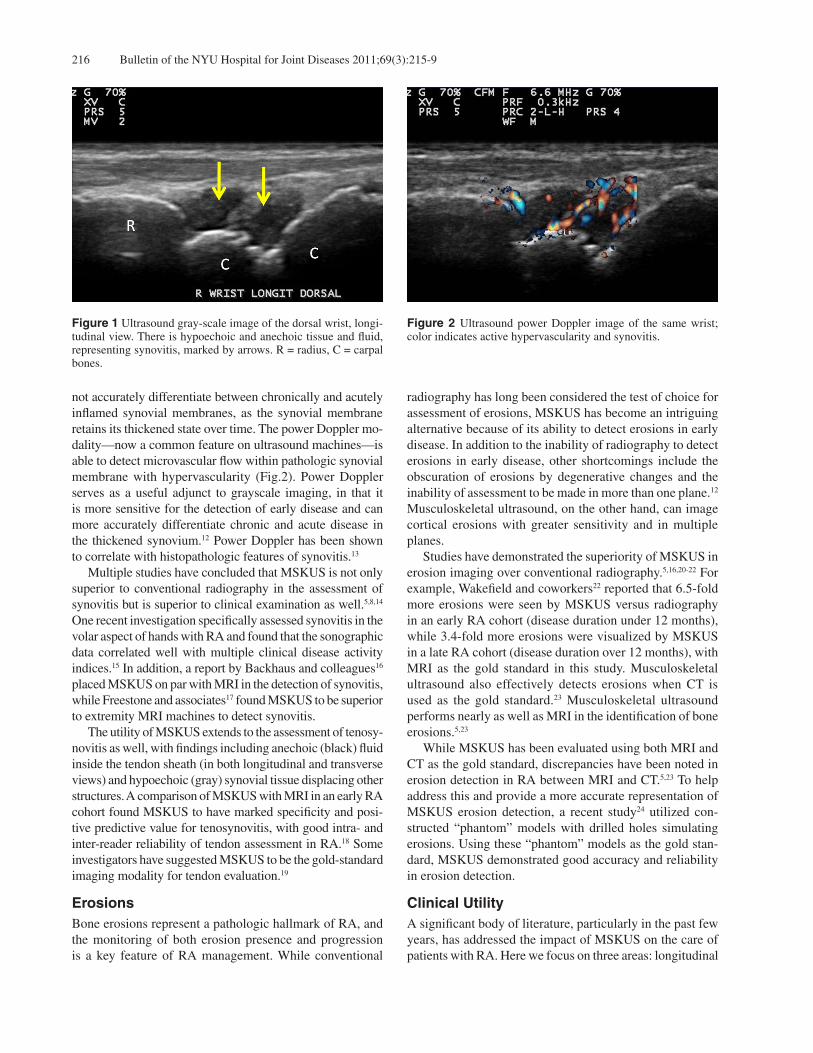
not accurately differentiate between chronically and acutely inflamed synovial membranes, as the synovial membrane retains its thickened state over time. The power Doppler mo-dality—now a common feature on ultrasound machines—is able to detect microvascular flow within pathologic synovial membrane with hypervascularity (Fig.2). Power Doppler serves as a useful adjunct to grayscale imaging, in that it is more sensitive for the detection of early disease and can more accurately differentiate chronic and acute disease in the thickened synovium.12 Power Doppler has been shown to correlate with histopathologic features of synovitis.13
Multiple studies have concluded that MSKUS is not only superior to conventional radiography in the assessment of synovitis but is superior to clinical examination as well.5,8,14 One recent investigation specifically assessed synovitis in the volar aspect of hands with RA and found that the sonographic data correlated well with multiple clinical disease activity indices.15 In addition, a report by Backhaus and colleagues16 placed MSKUS on par with MRI in the detection of synovitis, while Freestone and associates17 found MSKUS to be superior to extremity MRI machines to detect synovitis. The utility of MSKUS extends to the assessment of tenosy-novitis as well, with findings including anechoic (black) fluid inside the tendon sheath (in both longitudinal and transverse views) and hypoechoic (gray) synovial tissue displacing other structures. A comparison of MSKUS with MRI in an early RA cohort found MSKUS to have marked specificity and posi-tive predictive value for tenosynovitis, with good intra- and inter-reader reliability of tendon assessment in RA.18 Some investigators have suggested MSKUS to be the gold-standard imaging modality for tendon evaluation.19
ErosionsBone erosions represent a pathologic hallmark of RA, and the monitoring of both erosion presence and progression is a key feature of RA management. While conventional
radiography has long been considered the test of choice for assessment of erosions, MSKUS has become an intriguing alternative because of its ability to detect erosions in early disease. In addition to the inability of radiography to detect erosions in early disease, other shortcomings include the obscuration of erosions by degenerative changes and the inability of assessment to be made in more than one plane.12 Musculoskeletal ultrasound, on the other hand, can image cortical erosions with greater sensitivity and in multiple planes. Studies have demonstrated the superiority of MSKUS in erosion imaging over conventional radiography.5,16,20-22 For example, Wakefield and coworkers22 reported that 6.5-fold more erosions were seen by MSKUS versus radiography in an early RA cohort (disease duration under 12 months), while 3.4-fold more erosions were visualized by MSKUS in a late RA cohort (disease duration over 12 months), with MRI as the gold standard in this study. Musculoskeletal ultrasound also effectively detects erosions when CT is used as the gold standard.23 Musculoskeletal ultrasound performs nearly as well as MRI in the identification of bone erosions.5,23
While MSKUS has been evaluated using both MRI and CT as the gold standard, discrepancies have been noted in erosion detection in RA between MRI and CT.5,23 To help address this and provide a more accurate representation of MSKUS erosion detection, a recent study24 utilized con-structed “phantom” models with drilled holes simulating erosions. Using these “phantom” models as the gold stan-dard, MSKUS demonstrated good accuracy and reliability in erosion detection.
Clinical UtilityA significant body of literature, particularly in the past few years, has addressed the impact of MSKUS on the care of patients with RA. Here we focus on three areas: longitudinal
Figure 2 Ultrasound power Doppler image of the same wrist; color indicates active hypervascularity and synovitis.
Figure 1 Ultrasound gray-scale image of the dorsal wrist, longi-tudinal view. There is hypoechoic and anechoic tissue and fluid, representing synovitis, marked by arrows. R = radius, C = carpal bones.

217Bulletin of the NYU Hospital for Joint Diseases 2011;69(3):215-9
assessment and understanding remission, differential diag-nosis and clinical prediction, and global scoring systems.
Longitudinal Assessment and Understanding RemissionThe optimal use of MSKUS in longitudinal assessment of disease activity is still under evaluation by a number of investigators and collaborative efforts. Given the multiple categories of therapeutic options in RA, many studies have charted the sonographic versus the clinical response to these different agents before and after starting therapy. Naredo and colleagues25 provided one such evaluation by focusing on response to non-biologic disease modifying anti-rheumatic drugs (DMARDs). When studying the use of these drugs in early RA, they found that MSKUS was sensitive to change and a reliable tool for disease assessment by “minimal detectable change” based on intra-observer variability over the course of one year.25 Backhaus and colleagues reported on a 2-year follow-up of a cohort of predominantly RA patients also treated with non-biologic DMARDs, finding that MSKUS successfully detected improvement in synovitis correlating well with findings on clinical examination, MRI, and three-phase bone scintigraphy.16 Numerous cohorts of patients studied before and after biologic agents have dem-onstrated similar results with MSKUS consistently tracking disease improvement longitudinally.26,27
The study of imaging techniques has enhanced our understanding of the ever-present goal of remission in RA, and MSKUS has served this purpose on many levels.First is the observation that synovitis assessed by MSKUS is present in a significant number of RA patients deemed to be in clinical remission by multiple criteria (physician judgment, DAS28, and ACR remission criteria).28 While it is not yet clear if such subclinical synovitis eventually leads to erosions and warrants more aggressive treatment in seemingly well-controlled patients, such questions are under investigation by a number of groups. A recent study in which conventional clinical remission criteria such as DAS28 and SDAI were made even more stringent (allowing for fewer swollen or tender joints and lower CRP levels) showed that RA patients even meeting these stringent criteria continued to have synovitis on MSKUS, suggesting that clinical and biochemical assessments are less sensitive than ultrasound in detecting low disease activity.29
Additionally, there appears to be discordance between synovitis and erosive disease seen sonographically in pa-tients with RA. For example, Backhaus and colleagues16 found that while synovitis decreased on MSKUS and MRI in a cohort of predominantly RA patients on non-biologic DMARD therapy, erosions actually increased on imaging at 2-year follow-up. Another example in a more recent study by Saleem and colleagues30 showed that RA patients in clinical remission treated with combination TNF-inhibitor and non-biologic DMARD (known to have less erosive progression than patients on non-biologictherapy alone) actually had
similar synovitis burden on MSKUS as patients in clinical remission on non-biologic DMARD alone. This suggests that the mechanism by which TNF-inhibition prevents structural damage may not be associated with synovitis, thus provid-ing an important example of how MSKUS can shed light on pathogenesis of rheumatic disease. Finally, an MSKUS trial by Brown and coworkers31 has enhanced understanding of remission, by showing that a significant percentage of patients in clinical remission go on to develop erosive disease over longitudinal follow-up (making clinical remission a poor predictor of radiographic damage), in contrast to MSKUS findings which seem to be predictive of erosive damage over time, as will be discussed further below.
Differential Diagnosis and Clinical PredictionClinicians and investigators utilize MSKUS to help establish differential diagnoses for scenarios involving polyarticular joint symptoms. In an observational study of 100 rheuma-tology clinic patients referred for MSKUS, the original diagnosis (i.e., gout and rheumatoid arthritis) was changed in a number of patients based on the MSKUS findings.32 A more recent study evaluating MCP involvement in patients with RA versus psoriatic arthritis (PsA) found that a high percentage of PsA patients had an MSKUS pattern character-ized by hypoechoic swelling of the soft tissue surrounding the extensor digitorum tendon, which was not seen in any of the RA patients.33 This suggests a possible ultrasonographic method of differentiation between RA and PsA in seronega-tive patients without a clear diagnosis. As mentioned earlier, MSKUS can aid in the prediction of future radiographic (and potentially clinical) outcomes.Brown and colleagues31 showed that MCPs in RA patients displaying an increased power Doppler signal at baseline as-sessment were 12 times more likely to develop radiographic damage at one year than those without such hyperemia. Other studies have documented that MSKUS findings, particularly power Doppler signal, are predictive of erosive disease over time.25,26,34
MSKUS has also shown the potential ability to predict clinical outcomes of patients with early joint symptoms for less than 3 months. Freestone and colleagues35 showed that in patients with early hand joint symptoms, a baseline strong power Doppler signal had as much predictive value for inflammatory arthritis at 12 months as did a positive RF or anti-citrullinated protein antibody (ACPA). Furthermore, in patients with certain clinical, laboratory, and radiographic characteristics, the addition of MSKUS findings increased the probability of inflammatory arthritis at 12 months from 30% to 94%. In a more recent study, Filer and colleagues,36 using data analyzed from an extended 38 joint-count in patients with early joint symptoms, found that the use of a power Doppler index formed from bilateral wrists, second and third MCPs, and second and third MTPs (10 joints) was highly predictive of developing RA at 12 months.

Bulletin of the NYU Hospital for Joint Diseases 2011;69(3):215-9218
Global Scoring SystemsAs suggested in the above study by Filer and colleagues, efforts have been made to categorize MSKUS findings at the global level for a patient “score,” as compared to the individual joint level. Hammer and colleagues37 found that a comprehensive MSKUS assessment of 78 joints assessed longitudinally in RA patients on biologic therapy was highly sensitive to change. However, a handful of investigators have attempted to reduce the number of joints that need to be scanned while retaining sensitivity or specificity, such that MSKUS can be more feasible for clinicians in the outpa-tient setting and even future research efforts. For example, a 12-joint examination (bilateral elbow, wrist, second and third MCP, knee, and ankle), as detailed by Naredo and col-leagues,38 was found to be highly correlative (p < 0.0005) with a more comprehensive 44-joint evaluation in RA patients on biologic treatment. Backhaus and colleagues39 have proposed and validated a seven joint exam (dominant wrist, second and third MCPs and PIPs, and second and fifth MTPs), with scores correlating well with DAS28 at 3 and 6 months in patients on DMARD, biologic, and combination therapy. More recently, Hammer and coworkers40 showed high correlation with the comprehensive 78-joint evaluation and both the Naredo 12-joint system (Spearman rank .89, p < 0.001 for power Doppler baseline evaluation), as well as with the Backhaus 7-joint evaluation (Spearman rank .95, p < 0.001 for power Doppler baseline evaluation).
ConclusionThe role of MSKUS in the diagnosis and management of RA has evolved significantly in recent years. In RA as with other rheumatologic disease, MSKUS offers complementary, and often superior, assessment to the conventional methods of diagnosis such as physical exam, laboratory testing, and conventional radiography. Through the use of grayscale imaging and power Doppler technology, the evaluation of RA synovitis and erosions al-lows physicians and researchers to make better assessments of disease activity, treatment response and current damage, and potentially look forward to guide management and guide future outcomes.
Disclosure StatementNone of the authors have a financial or proprietary interest in the subject matter or materials discussed, including, but not limited to, employment, consultancies, stock ownership, honoraria, and paid expert testimony.
References1. DelleSedie A, Riente L, Bombardieri S. Limits and perspec-
tives of ultrasound in the diagnosis and management of rheumatic diseases. Mod Rheumatol. 2008;18(2):125-31.
2. Meenagh G, Filippucci E, Kane D, Taggart A, Grassi W. Ultrasonography in rheumatology: developing its potential in clinical practice and research. Rheumatology (Oxford). 2007;46(1):3-5.
3. Iagnocco A, Epis O, DelleSedie A, et al. Ultrasound imaging for the rheumatologist. XVII. Role of colour Doppler and power Doppler. Clin Exp Rheumatol. 2008;26(5):759-62.
4. Bruyn GA, Pineda C, Hernandez-Diaz C, et al. Validity of ultrasonography and measures of adult shoulder function and reliability of ultrasonography in detecting shoulder synovitis in patients with rheumatoid arthritis using magnetic resonance imaging as a gold standard. Arthritis Care Res (Hoboken). 2010;62(8):1079-86.
5. Szkudlarek M, Klarlund M, Narvestad E, et al. Ultrasonogra-phy of the metacarpophalangeal and proximal interphalangeal joints in rheumatoid arthritis: a comparison with magnetic resonance imaging, conventional radiography and clinical examination. Arthritis Res Ther. 2006;8(2):R52.
6. Terslev L, Torp-Pedersen S, Savnik A, et al. Doppler ultra-sound and magnetic resonance imaging of synovial inflamma-tion of the hand in rheumatoid arthritis: a comparative study. Arthritis Rheum. 2003;48(9):2434-41.
7. Karim Z, Wakefield RJ, Quinn M, et al. Validation and repro-ducibility of ultrasonography in the detection of synovitis in the knee: a comparison with arthroscopy and clinical examina-tion. Arthritis Rheum. 2004;50(2):387-94.
8. Wakefield RJ, Freeston JE, O’Connor P, et al. The optimal assessment of the rheumatoid arthritis hindfoot: a comparative study of clinical examination, ultrasound and high field MRI. Ann Rheum Dis. 2008;67(12):1678-82.
9. Cheung PP, Dougados M, Gossec L. Reliability of ultrasonog-raphy to detect synovitis in rheumatoid arthritis: a systematic literature review of 35 studies (1,415 patients). Arthritis Care Res (Hoboken). 2010;62(3):323-34.
10. Naredo E, Moller I, Moragues C, et al. Interobserver reli-ability in musculoskeletal ultrasonography: results from a “Teach the Teachers” rheumatologist course. Ann Rheum Dis. 2006;65(1):14-9.
11. Wakefield RJ, Balint PV, Szkudlarek M, et al. Musculoskeletal ultrasound including definitions for ultrasonographic pathol-ogy. J Rheumatol. 2005;32(12):2485-7.
12. Brown AK. Using ultrasonography to facilitate best practice in diagnosis and management of RA. Nat Rev Rheumatol. 2009;5(12):698-706.
13. Walther M, Harms H, Krenn V, et al. Correlation of power Doppler sonography with vascularity of the synovial tissue of the knee joint in patients with osteoarthritis and rheumatoid arthritis. Arthritis Rheum. 2001;44(2):331-8.
14. Naredo E, Bonilla G, Gamero F, et al. Assessment of inflam-matory activity in rheumatoid arthritis: a comparative study of clinical evaluation with grey scale and power Doppler ultrasonography. Ann Rheum Dis. 2005;64(3):375-81.
15. Vlad V, Berghea F, Libianu S, et al. Ultrasound in rheumatoid arthritis - volar versus dorsal synovitis evaluation and scoring. BMC MusculoskeletDisord. 2011 Jun 3;12:124.
16. Backhaus M, Burmester GR, Sandrock D, et al. Prospective two year follow up study comparing novel and conventional imaging procedures in patients with arthritic finger joints. Ann Rheum Dis. 2002;61(10):895-904.
17. Freeston JE, Brown AK, Hensor EM, et al. Extremity magnetic resonance imaging assessment of synovitis (without contrast) in rheumatoid arthritis may be less accurate than power Dop-pler ultrasound. Ann Rheum Dis. 2008;67(9):1351.
18. Micu MC, Serra S, Fodor D, et al. Inter-observer reliability

219Bulletin of the NYU Hospital for Joint Diseases 2011;69(3):215-9
of ultrasound detection of tendon abnormalities at the wrist and ankle in patients with rheumatoid arthritis. Rheumatology (Oxford). 2011 Jun;50(6):1120-4.
19. Grassi W, Filippucci E, Farina A, Cervini C. Sonographic imaging of tendons. Arthritis Rheum. 2000;43(5):969-76.
20. Funck-Brentano T, Etchepare F, Joulin SJ, et al. Benefits of ultrasonography in the management of early arthritis: a cross-sectional study of baseline data from the ESPOIR cohort. Rheumatology (Oxford). 2009;48(12):1515-9.
21. Scheel AK, Hermann KG, Ohrndorf S, et al. Prospective 7 year follow up imaging study comparing radiography, ultra-sonography, and magnetic resonance imaging in rheumatoid arthritis finger joints. Ann Rheum Dis. 2006;65(5):595-600.
22. Wakefield RJ, Gibbon WW, Conaghan PG, et al. The value of sonography in the detection of bone erosions in patients with rheumatoid arthritis: a comparison with conventional radiography. Arthritis Rheum. 2000;43(12):2762-70.
23. Dohn UM, Ejbjerg BJ, Court-Payen M, et al. Are bone erosions detected by magnetic resonance imaging and ultrasonography true erosions? A comparison with computed tomography in rheumatoid arthritis metacarpophalangeal joints. Arthritis Res Ther. 2006;8(4):R110.
24. Koski JM, Alasaarela E, Soini I, et al. Ability of ultrasound imaging to detect erosions in a bone phantom model. Ann Rheum Dis. 2010;69(9):1618-22.
25. Naredo E, Collado P, Cruz A, et al. Longitudinal power Doppler ultrasonographic assessment of joint inflammatory activity in early rheumatoid arthritis: predictive value in disease activity and radiologic progression. Arthritis Rheum. 2007;57(1):116-24.
26. Naredo E, Moller I, Cruz A, Carmona L, Garrido J. Power Doppler ultrasonographic monitoring of response to anti-tumor necrosis factor therapy in patients with rheumatoid arthritis. Arthritis Rheum. 2008;58(8):2248-56.
27. Wakefield RJ, Freeston JE, Hensor EM, et al. Delay in imaging versus clinical response: a rationale for prolonged treatment with anti-tumor necrosis factor medication in early rheumatoid arthritis. Arthritis Rheum. 2007;57(8):1564-7.
28. Brown AK, Quinn MA, Karim Z, et al. Presence of significant synovitis in rheumatoid arthritis patients with disease-modify-ing antirheumatic drug-induced clinical remission: evidence from an imaging study may explain structural progression. Arthritis Rheum. 2006;54(12):3761-73.
29. Saleem B, Brown AK, Keen H, et al. Should imaging be a component of rheumatoid arthritis remission criteria? A comparison between traditional and modified composite remission scores and imaging assessments. Ann Rheum Dis.
2011;70(5):792-8.30. Saleem B, Brown AK, Keen H, et al. Disease remission state
in patients treated with the combination of tumor necrosis factor blockade and methotrexate or with disease-modifying antirheumatic drugs: A clinical and imaging comparative study. Arthritis Rheum. 2009;60(7):1915-22.
31. Brown AK, Conaghan PG, Karim Z, et al. An explanation for the apparent dissociation between clinical remission and continued structural deterioration in rheumatoid arthritis. Arthritis Rheum. 2008;58(10):2958-67.
32. Karim Z, Wakefield RJ, Conaghan PG, et al. The impact of ultrasonography on diagnosis and management of pa-tients with musculoskeletal conditions. Arthritis Rheum. 2001;44(12):2932-3.
33. Gutierrez M, Filippucci E, Salaffi F, et al. Differential diag-nosis between rheumatoid arthritis and psoriatic arthritis: the value of ultrasound findings at metacarpophalangeal joints level. Ann Rheum Dis. 2011;70(6):1111-4.
34. Taylor PC, Steuer A, Gruber J, et al. Comparison of ultraso-nographic assessment of synovitis and joint vascularity with radiographic evaluation in a randomized, placebo-controlled study of infliximab therapy in early rheumatoid arthritis. Arthritis Rheum. 2004;50(4):1107-16.
35. Freeston JE, Wakefield RJ, Conaghan PG, et al. A diagnostic algorithm for persistence of very early inflammatory arthritis: the utility of power Doppler ultrasound when added to conven-tional assessment tools. Ann Rheum Dis. 2010;69(2):417-9.
36. Filer A, de Pablo P, Allen G, et al. Utility of ultrasound joint counts in the prediction of rheumatoid arthritis in patients with very early synovitis. Ann Rheum Dis. 2011;70(3):500-7.
37. Hammer HB, Sveinsson M, Kongtorp AK, Kvien TK. A 78-joints ultrasonographic assessment is associated with clini-cal assessments and is highly responsive to improvement in a longitudinal study of patients with rheumatoid arthritis starting adalimumab treatment. Ann Rheum Dis. 2010;69(7):1349-51.
38. Naredo E, Rodriguez M, Campos C, et al. Validity, reproduc-ibility, and responsiveness of a twelve-joint simplified power dopplerultrasonographic assessment of joint inflammation in rheumatoid arthritis. Arthritis Rheum. 2008;59(4):515-22.
39. Backhaus M, Ohrndorf S, Kellner H, et al. Evaluation of a novel 7-joint ultrasound score in daily rheumatologic practice: a pilot project. Arthritis Rheum. 2009;61(9):1194-201.
40. Hammer HB, Kvien TK. Comparisons of 7- to 78-joint ultra-sonography scores: all different joint combinations show equal response to adalimumab treatment in patients with rheumatoid arthritis. Arthritis Res Ther. 2011;13(3):R78.