Embed Size (px)
Citation preview
respectively. For those aped 65 or older. the corresponding estimated relative risks were 0.73.0.54. and 0.29. respectively. These two studies suggest that the risk of lung cancer may decline less steeply with increasing abstinence for older ex-smokers.
Multistage Modeling
Multistage models provide a conceptual framework for facilitating understanding of the relationship of lung cancer incidence with amount smoked, duration of smoking. and time since cessation. These models. proposing theoretical constructs of fundamen- tal biologic mechanisms. have been useful for evaluating epidemiologic data in a biologic framework and thereby furthering the understanding of tobacco carcino- genesis. However, fitting these models to epidemiologic data cannot establish the veracity ofthe underlying biologic theory. Multistage modeling approaches have been used to describe respiratory carcinogenesis and to assess smoking cessation and lung cancer risk. Although a number of different mathematic models of carcinogenesis have been proposed (e.g.. two-stage. multicell, multistage). this discussion primarily ad- dresses the Armitage and Doll (1954. 1957) multistage model, which has been used most extensively in studies of lung cancer.
Based on a series of studies examining age-specific mortality rates for various cancers. Armitage and Doll (1954. lYS7) proposed a multistage theory of carcino- genesis. Their model assumes that a single cell can generate a malignant tumor only after undergoing a certain number of genetic changes. Animal studies also support the multistage model. Multistage theories also predict the age pattern of occurrence of many tumors induced in experimental animals by continuous exposure to chemical carcinogens. Experimental regimens involving initiation and promotion provide direct evidence of the effect of early- and late-stage events in the carcinogenic process (Stenback. Peto. Shubik 198la.b.c).
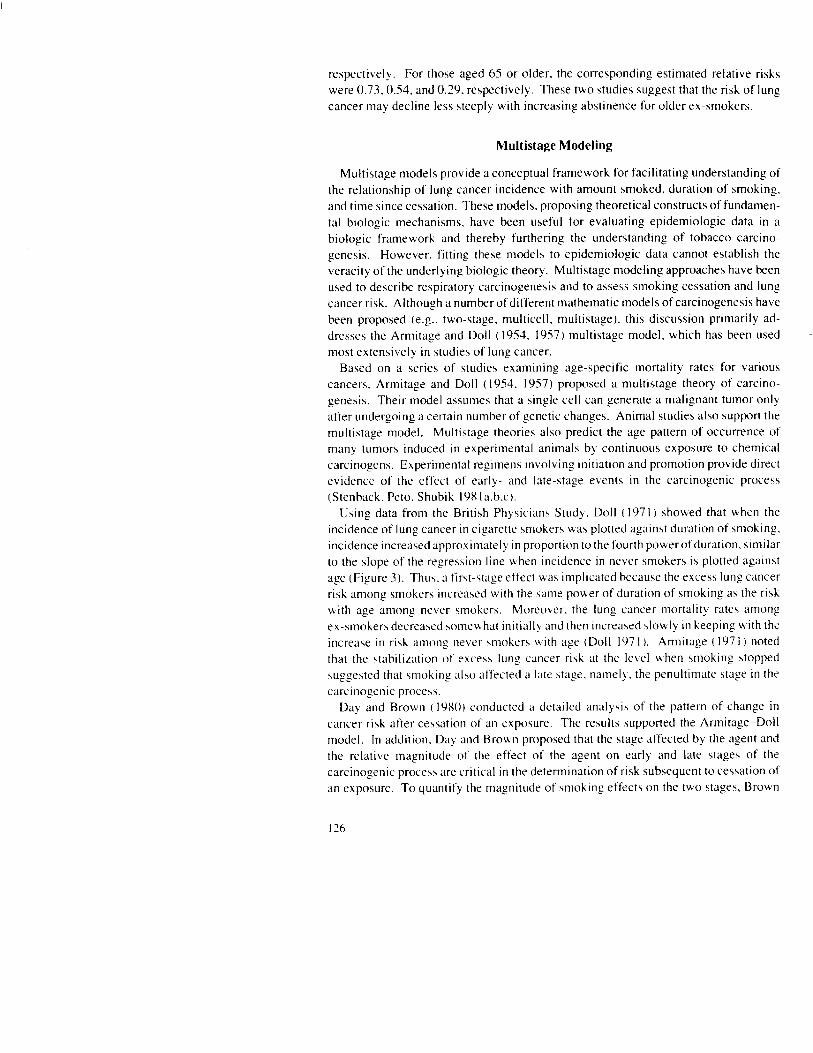
Using data from the British Physicians Study,. Doll (197 I ) showed that when the incidence of lung cancer in cigarette smokers was plotted against duration of smoking. incidence increased approximately in proportion to the fourth powerofduration. similar to the slope of the regression line when incidence in never smokers is plotted against age (Figure 3). Thu\. a first-stage effect uas implicated because the excess lung cancer risk among smokers increased with the same power of duration of smoking as the risk with ape among never smokers. Moreover. the lung cancer mortality rates among ex-smoker:, decreased someu hat initially and then increased ,Iowly in beeping with the increase in rish among never smohers vv ith age (Doll I97 I ). Armitage ( 197 I) noted that the stabilir.ation of excess lung cancer risk at the level when smoking stopped suggested that smoking also affected a late stage. namely. the penultimate stage in the carcinogenic process.
Day and Brown (IYXO) conducted a detailed analysis of the pattern of change in cancer risk after cessation of an exposure. The results supported the Arnmitage-Doll model. In addition. Day and Brown proposed that the stage affected by the agent and the relative magnitude of the effect of the agent on early and late stages of the carcinogenic process are critical in the determination of risk subsequent to cessation of an exposure. To quantify the magnitude of smoking et’fectj on the two stages. Brown
1,000
100
10
1
X-X Cigarette smokers by duration of smoking x ---a# Cigaretie smokers by age .-. Never smokers by age
I I I I I I I 20 30 40 50 60 70 80
YEARS
FIGURE 3.4ncidence of bronchial carcinoma among continuing cigarette smokers in relation to age and duration of smoking and among
never smokers in relation to age, double logarithmic scale SOCRCE Doll c I’)7 I), xlth LO~XC~K~ (11 prIntin; ~‘rrw m the w~yn,d figure
and Chu ( 1987) reexamined data on ex-smokers from the European case+zontrol stud) of lung cancer (Lubin et al. lOX4a) and concluded that smoking had an almost double relative effect on late-stage events compared with first-stage events. Using data from a case<ontrol study in New Mexico, Whittemore ( 198X) developed a predictive model for lung cancer that showed a twofold stronger effect on late-stage than on early-stage events; the model overpredicted cases among ex-smokers and under-predicted cases among current smokers. Therefore. Whittemore suggested that smoking may have an even stronger effect on late-stage events than was assumed in the model.
.4lternative models and interpretation of data on former smohers and lung cancer ha\,e also been suggested in several recent studA. Freedman and i%a\ idi ( 19X9) tested the

fit of the multistage model to data from ACS CPS-I and the U.S. Veterans Study. These researchers observed that crude rates of lung cancer decreased u ith increasing years of smoking abstinence although the trend w’as less steep when average amount of smoking and ages when smoking started and stopped were considered in the analysis. Moreover. the observed lung cancer rates among ex-smokers were compared with the expected rates. which w)ere computed in three ways-risk at the time of quitting. risk at current age with excess risk frozen at the time of quitting. and never smokers of the same age. For each comparison approach. the ratio of observed to expected rates decreased u ith increasing years of smoking abstinence. Freedman and Navidi ( 1989) concluded that this pattern was incompatible with the multistage model. which predicts \tabiliration of excess risk when an individual stops smoking.
Gaffney and Altshuler ( 1988) reexamined data from the British Physicians Study and found that the best-fitting model among current smohers predicted an increase in the excess incidence amon ex-smohers. which &as inconsistent with the obsened decreased rates. These researchers found that a two-stage model fit the incidence of lung cancer in both current smohers and ex-smohers. Gaffney and .i\ttshuter ( 1988) then proposed a two-stage model with clonal growth in R hich cigarette smoke induced the initial transition and promoted clonal grouth in these cells initiated by cigarette smoke. Moolgavkar. Dewanji. and Luebeck ( 1989) questioned the biologic plausibilit\, of the proposal by Gaffney and Altshuler ( 198X) and noted that their model oni) fit part of the British physicians data set. did not consider each age-smoking le\,el. and discounted the possibility that making affected two transition rates in the carcinogenic process.
Moolgavhar. Dewanji. and Luebech ( IYXY) reanalyzed the British Physician\ Stud> within the framework ofthe two-mutation. recessive oncogenesis model. Ba\ed on this model. the second-mutation rate would be affected by \mohing. and a sudden decline in risk after cessation of smohing v.ould be predicted. HoNever. this model implies that smoking affect\ the last stage in a multi$tape process. contrary to current con\ider:t- tions.
In summary. multistage models have been used to describe the interrelationships among number of cigarettes smoked dail>. duration. time \inctz e\posurr ended. and lung cancer incidence. Several In\,c\tigators hale interpreted the data on rish among former smokers in different ~a> \. The epidemiologic data clearI> indicate that the rish among former smohers i\ between that of continuin, (1 smoher\ and nekrr smohers. Various models can be fit to the different data ~1s. The expected pattern ofrith among former sniohers is sensitive lo the model \clectrd and dependent on the relati\ e magnitude of the effect of smohing on earl> \ er\u\ late stage\ of the proces\ ot carcinogenesis. Lsing multistage models. the data on t.ormer smohcr\ are insufficient to allow precise quantification of the relati\ c cffcct\ of \mohin, 0 on the earl\ and late stages of the carcinogenic proce\\. H hich smokin, (7 i4 assumed to affect. Ne~ertticle\\. data indicate that \mohing ha\ an dt’cct on the late \tagt’\ of the carcinogenic proce\c and that cessation reduce\ lung cancer occurrcncc.

Cessation After Developing Disease
Individuals who stopped smoking are not a randomly selected group in most studies (Chapter 2). Often. smohers quit as a result of developing symptoms of a life- threatening disease or immediately after diagnosis of cancer. This phenomenon is ev id,enced by the increase in risk of lung cancer in the immediate period after cessation. Sotne studies have grouped these former smokers with the continuing smohcrs or have excluded them from the analysis.
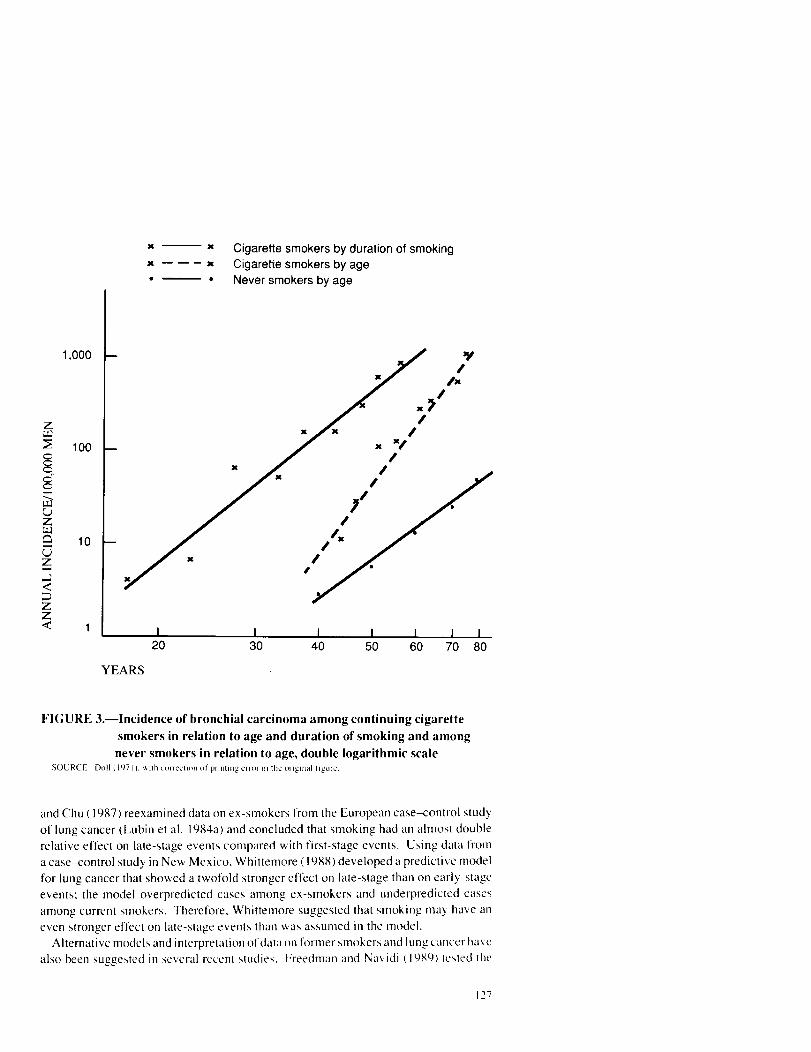
A few epidemiologic studies have assessed the risk of lung cancer among those who quit for health reasons and for non-health-related reasons. In the U.S. Veterans Study. about 10 percent of the smokers quit because of a doctor’s orders: these smokers here presumably ill. The lung cancer mortality ratio relative to never smohers for es- smokers who stopped because of non-health-related reasons MLIS 3.43 compared with 5.83 among ex-smohers who stopped on a doctor’s orders and X.98 among continuing smohers (Kahn 1966). In the European case-control study. Brown and Chu ( I YX7) reported that the relative risk of lung cancer for those who stopped smoking because of health reasons compared with those who stopped for reasons other than health uas 1.3 (p<O.OOl ). Moreover, the percentage who stopped for health reasons decreased uith increasing years of abstinence. Among those who had stopped for I year or less. 95.X percent stopped because of health reasons compared with 65.7 percent of longer term ex-smokers. In ACS CPS-II, men and women who did not have a history of heart disease. stroke, or cancer at the time of interview showed a decreased risk of lung cancer in the first 2 years after smoking cessation when compared v+ ith continuing smokers. In contrast, the risks for all subjects combined (i.e.. those with and without a history of previous chronic disease) were increased during the first 2 years after smoking cessation when compared with continuing smokers. The lower risks among the group with no history of previous disease compared with the total group persisted for subsequent periods of smoking abstinence (Table 7).
Cessation After Diagnosis of Lung Cancer
Two studies examined the relationship between smoking status and treatment out- come of patients with small cell lung cancer. In the study by Johnston-Early and associates ( 1980). survival was prolonged in patients who were ex-smokers or who had stopped smoking at diagnosis, whereas no difference in survival by smoking status was detected in the study by Bergman and Sorenson ( 1988).
The study by Johnston-Early and colleagues (1980) involved I 12 patients with small cell lung cancer: 20 had stopped smoking before diagnosis; 35 had stopped at diagnosis; and 57 continued smoking. Therapies included chemotherapy with radiation therapy. with or without thymosin fraction V. The three patient groups were similar in disease extent, pretreatment performance status, pack-years smoked, and age and sex distribu- tion. The patients who had stopped smoking prior to diagnosis had the best survival, followed by those who had stopped at diagnosis, and finally by those who continued smoking; the median survival for the three groups was 70. 52. and 47 weeks. respec- tively. Overall survival differences remained after individually adjusting for disease
TABLE 7.--Standard mortality ratios of lung cancer among former smokers in AC!+CPS II (relative to never smokers) by years of smoking abstinence, daily cigarette consumption at time of cessation, and history of chronic disease
I-20 >?I erg/da\ q/da\
7.4 i-l.3 Y I 19.5 7 Y 11.6 I .(I Y. I I .5 SY 1-l 26
extent. performance status. and type of protocol treatment. Similarly. statistical sig- nificance was maintained after simultaneous adjustment for both thbmosin and radia- tion therapy.
The study b> Bergman and Sorenson ( IYXX) involved 153 small cell lung cancer patients who received combination chemotherap>. Thirty-two had stopped smohing at least 6 months before the initiation of treatment or had ne\‘er smoked. 51 patients stopped smoking less than 6 months prior to the start of treatment. and 71 patients continued to smoke during the treatment period: the median survival was 39. 42. and 30 weeks. respectively. Reasons for differences in results betbeen the two studies are not clear. Overall. patients in the study hy Bergman and Sorenson ( 1988) had smoked fewer pack-years. but the median survi\,al and performance status of each of the three
130

smoking status groups were poorer than for the comparable smoking status groups in the study by Johnston-Early and associates ( 1980).
LARYNGEALCANCER
Pathophysiologic Framework
Smoking has been firmly established as a cause of laryngeal cancer (US DHHS 1982. 1989) based on numerous epidemiologic studies. These studie, have employed diverse methodologies and have been performed in different countries and covered various time periods. Tobacco smoke exposure has been measured by number of cigarettes smoked per day. number of years of smoking, age when started to smoke, type of cigarettes smoked. and depth of inhalation (US DHHS 1982).
In the larynx, as in the bronchus. a sequence of histologic changes occurs with continued smoking. These changes progress from cells with atypical nuclei. to car- cinoma in situ. to invasive carcinoma. Autopsy studies show that recovery of the laryngeal epithelium can follow smoking cessation. Auerbach, Hammond. and Gar- finkel (1970) studied postmortem specimens of laryngeal epithelium from 942 men (644 current cigarette smokers, 94 cigar and/or pipe smokers, I I6 ex-cigarette smokers. and 88 never smokers). Ex-smokers in this study had stopped smoking for at least 5 years. Compared with current smokers, ex-smokers showed fewer histologic changes: 75 percent of ex-smokers and never smokers showed no cells with atypical nuclei. whereas almost all current smokers showed some cells with atypical nuclei.
Similar findings were reported by Muller and Krohn ( 1980). who obtained laryngeal epithelial specimens from autopsy. Of the 148 cases in the study. 24 were never smokers and 24 were ex-smokers who had stopped smoking for at least 5 years. Table 8 shows the relative distribution of selected histologic features by smoking status. Occurrence of all histologic changes was lowest among never smokers, intermediate among ex-smokers, and highest among current smokers. However. the histologic findings of ex-smokers in this study were more similar to those of light current smokers (<lOcig/day) than to those of never smokers.
Smoking Cessation and Laryngeal Cancer Risk
A few studies provide data on the relationship between smoking cessation and risk of laryngeal cancer (Table 8). Former smokers are at less risk than current smokers. but have about six times the risk of never smokers. The relative risk of laryngeal cancer is higher immediately after smoking cessation (i.e., l-3 years after quitting) compared with continuing smokers. However. after approximately 3 to 3 years of smoking abstinence, former smokers show lower relative risks with increasing years of smoking abstinence (Table 8). Based on a case-control study of laryngeal and hypopharyngeal cancer conducted in Europe, Tuyns and colleagues ( 1988) suggested that the benefit of smoking cessation seemed to appear sooner after cessation for cancer of the hypopharynx/epilarynx than for the larynx.
131
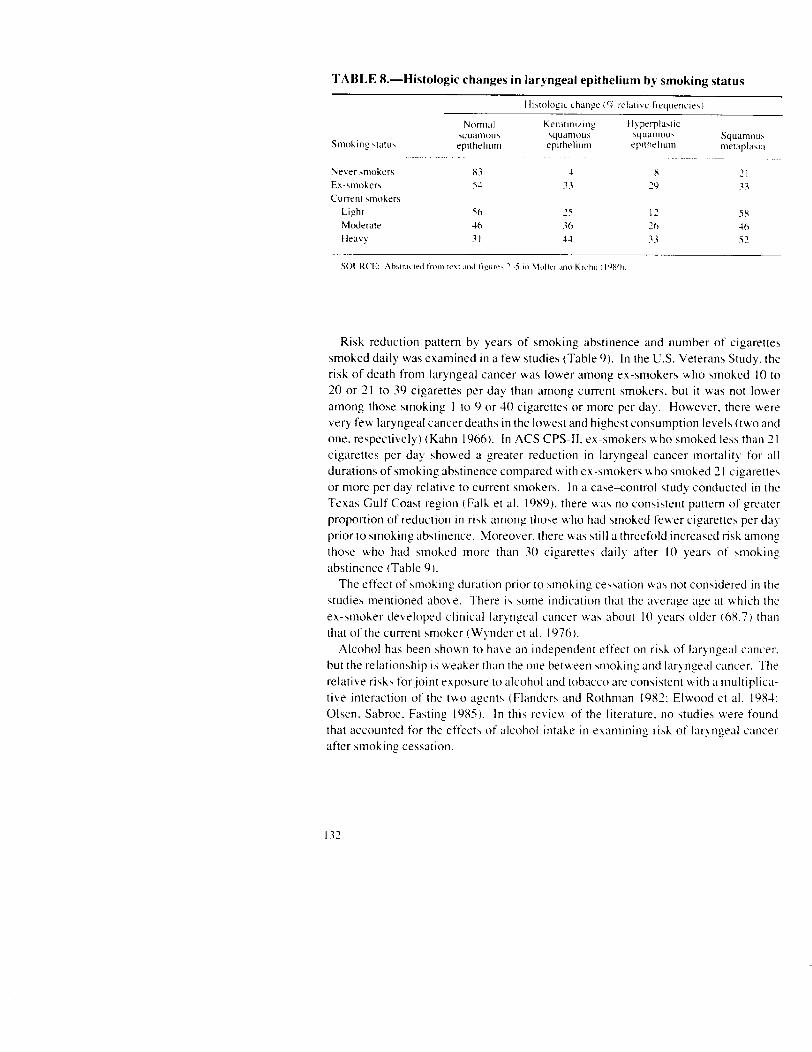
Risk reduction pattern by years of smoking abstinence and number of cigarettes smoked daily was examined in a few studies (Table 9). In the U.S. Veterans Study. the risk of death from laryngeal cancer was lower among ex-smokers upho smoked 10 to 20 or 71 to 39 cigarettes per dav than among current smokers. but it was not lower among those smoking 1 to 9 or 30 cigarettes or more per day. However. there were very few laryngeal cancer deaths in the lowest and highest consumption levels (two and one. respectively) (Kahn 1966). In ACS CPS-II. es-smokers u ho smoked less than 2 I cigarettes per day showed a greater reduction in laryngeal cancer mortalit) for all durations of smoking abstinence compared with ex-smokers uho smoked 31 cigarettes or more per day relative to current smokers. In a case<ontrol study conducted in the Texas Gulf Coast region (Fall\ et al. 1989). there uas no consistent pattern of greater proportion of reduction in risk among those who had smoked fe\s#er cigarettes per dab prior to smoking abstinence. Moreover. there was still a threefold increaKed risk among those who had smoked more than 30 cigarettes daily after IO years of smoking abstinence (Table 9).
The effect of smohing duration prior to smohing cessation M as not considered in the studies mentioned above. There is some indication that the average age at which the ex-smoher developed clinical laryngeal cancer was about IO years older (6X.7) than that of the current smoker (Wnder et al. 1976).
Alcohol has been shown to have an independent effect on risk of iqngeal cancer, but the relationship is weaher than the one betu,een smohing and laryngeal cancer. The relative risks forjoint exposure to alcohol and tobacco are consistent with a multiplica- tive interaction of the two agents (Flanders and Rothman 1982: Elwood et al. 19X-l: Olsen. Sabroe. Fasting 19X5). In this revie\* of the literature. no studies were found that accounted for the effects of alcohol intahe in examining rish of laryngeal cancer after smoking cessation.
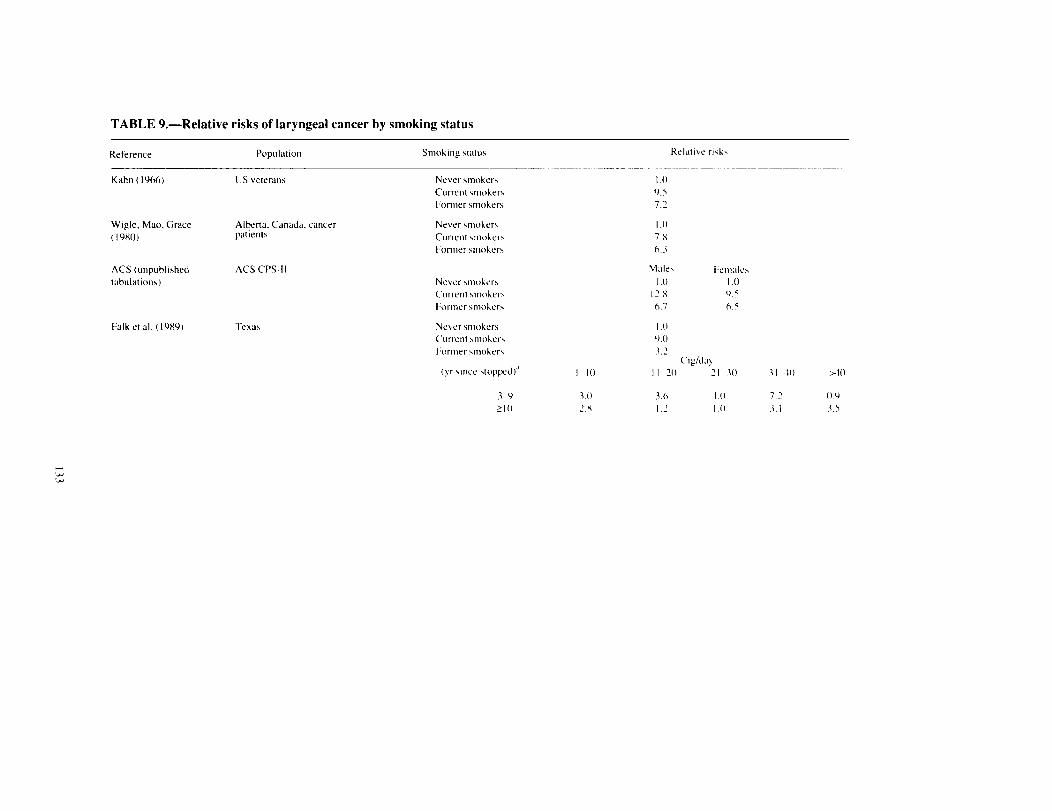
TABLE 9.-Relative risks of laryngeal cancer by smoking status
Reference Population
Kahn ( 1966) US veterans Never smoker\ Current \mohrrs Former wloher\
WI+, Mao. Grace (19X0)
Alberta. Canada. cancer patlent\
Never rmoher\ Current vnoherr Former \moher\
ACS (unpublished tabulations)
AC-S CPS-II Never \mohrr\ Cut rent winher\ Former \mohcr\
Fall\ et al. (1089) TCXl\ Never winher\ (‘urrent smoher\ Former \moher\
(y \mce stopped)”
3-Y >I0
I IO
3.11 2.x
I .o Y.5 7.2 I .o 7.x (1.3
Malt\ I~cnl;tle\ I .o I .o
17.x Y.5 (7.7 6.5
I .o 0.0 3.2
(‘lg/d;l) II 70 ‘I 30 31 40 >40
3.0 J.(I 72 0.Y I.2 I .I) .3 I 3.5

TABLE 9.--Continued
‘l‘U> II\ ct XI (IYXX)
Former vnoher\ (yr \incc 4loppetl)
I-3 44 7-10
II-15 >Ih
Cutrent wider\ Never w~oher\
Relative risk\
Malea
17.9 8.5 3.0 3.4 1.5
I4 3 I .I)
Female
h.Y 2.6 -
X.X
I1.h I .o
Entlolnry nx I .5 I

CONCLUSIONS
I. Smohing cessation reduces the risk of lung cancer compared M ith continued \moh- ins. For example. after 10 years of abstinence. the ri\h of lung cancer is about 30 to 50 percent of the rish for continuing smokers: with further abstinence. the ri\h continue\ to decline.
2. The reduced risk of lung cancer among former w~ohers i\ oh3erved in male\ and females. in smokers of filter and nonfilter cigarette>. and for all histologic types of luns cancer.
3. Smohing cessation lower\ the risk of larynyxl cancer compared with continued smoking.
1. Smohing ce\\ation reduce\ the severity and extent of premalignant histologic changes in the epithelium of the larynx and lung.
References
ALDERSON, M.R.. LEE. P.N.. WANG. R. Risks of lung cancer. chronic bronchitis. ischaemic heart disease. and stroke in relation to type of cigarette smoked. .lou/.rwl of E/?/d’nriolo,~~ trrrtl Con7/777//7i7~ Hcr~ltlr 3Y(4):2Xh-293. December 1 YXS.
AMERICAN CANCER SOCIETY. Unpublished tabulations. ARMITAGE. P. Discussion on paper hy R. Doll. .lorrr-/rt/l of 7hc R(JJU/ S~c17i.s//c~c/I Soc.ret?.
A134:155-156. 1971. ARMITAGE. P.. DOLL. R. The age distribution of cancer and a multi-stage theory of
carcinogenesis. British ./07//77~1/ c$Cu/7wr 8: l-l I . 195-t. ARMITAGE. P.. DOLL. R. A two-stage theory of carcinogenew in relation to the age
distribution of human cancer. B/-iris/7 .lor/r/7ct/ ofC~w7wr I I : I6 I-164,. 19.57. AUERBACH. 0.. GARFINKEL. L.. HAMMOND. E.C. Relation of smoking and age to
findings in lung parenchyma: A microscopic study. Cl7cw 6% I t:2Y-35. January 1974. AUERBACH. 0.. GERE. J.B.. FORMAN. J.B.. PETRICK. T.G.. SMOLIN. H.J.. MLIEHSAM.
G.E.. KASSOUNY. D.Y.. STOUT. A.P. Changes in the bronchial rptthelium in relation to smoking and cancer of the lung. .4 report of progress. i%‘crc, h~ltrr7rl .lortr~7t/l of Merlic~i/rr’
256(3):97-104. January 17, 1957. AUERBACH. 0.. HAMMOND. E.C.. GARFINKEL. L. Histologtc changes m the larynx in
relation to smoking habits. c‘crww 2S( I ):92-10-l. January 1970.
AUERBACH. 0.. HAMMOND. EC.. GARFINKEL. L.. BENANTE. C. Relation of smoking and age to emphysema. Whole-lung section stud!,. Nc,i\, E/7,g/tr/7cl .lor/r/7trl c!f Medic 717~
2X6( 16):853-X57. April 70. 1972. AUERBACH. 0.. STOUT. A.P.. HAMMOND. EC.. GARFINKEL. L. Changes in bronchial
epithelium in relation to sex. age. residence. smoking and pneumonia. R;rzic, E/7,~/o/7cl./o7//./7ol
of‘Mcdic~i/7r 267(j): I I l-l 25. July 19. I Yh’a. AUERBACH. 0.. STOUT. A.P.. HAMMOND. E.C.. GARFINKEL. L. Bronchial epithelium
in former smokers. Nw E/7q/c//7d ./oI//~/~LI/ ~!f’MedicY/~e 267t3 ): I I Y- 125. July I Y. 1962h. AUERBACH. 0.. STOUT. A.P.. HAMMOND. E.C.. GARFINKEL. L. Smoking habits and
age in relation to pulmonary changes. Rupture of alveolar septums. fibrosis and thickening of walls of small arteries and arterioles. hicu E/7,~/o/d Jorr7~/7c// of’M~dki/7c 269(X)): 103% 1054. November 14. 1963.
AUERBACH. 0.. STOUT. A.P.. HAMMOND, E.C.. GARFINKEL. L. Interrelationships among various histologic changes in bronchial tubes and in lung parenchyma. An7er~ic~tu7 Ke\~ie~. r!fRes/)i~u/or.~ Discuw 90(6):867-X76. December 1964.
BENHAMOU. S.. BENHAMOU, E., TIRMARCHE, M.. FLAMANT. R. Lung cancer and use of cigarettes: A French case-control study. Jorrr-/7u/ of the NuI~o/~u/ Cufrt CI lux7i717t~
74(6):1169-l 17.5. June 19x5. BERGMAN. S.. SORENSON. S. Smoking andeffect ofchemotherapy in small cell lung cancer.
Eu/w/mui Re.\/mm~~ ./ort/~7u/ I :932-937. 19x8. BIRRER. M.J.. MINNA. J.D. Molecular genetics of lung cancer. SPnri/7tri~.\ i/7 O/,r n/o,g~
lS(3):22623.5. June 198X. BROWN. C.C., CHU. K.C. Use of multistage models to infer stage affected by carcinogenic
exposure: Example of lung cancer and cigarette smoking. .lorrr/7o/ ofC‘l7wr7ic~ D/.wo.w.v 40 (Supplement 2):17lS-17%. 1987.
CANADIAN DEPARTMENT OF NATIONAL HEALTH AND WELFARE. A Cur7udim7 Strtdy cfSnwki~,g md Hculrh. Department of National Health and Welfare. Epidemiolog) Division. Health Services Branch. Bioatatistics Division. Research and Statistics Directorate. 1966. 137 pp.
137
CEDERLOF. R.. FRIBERG. L.. HRI’BEC. Z.. LORICH. L;. 1/w Kc/~rr/r~/r\/r//, of S,,~oX/,,;; c//r</ .sot/lr’ sot ill/ c-01 ol-lo/~lc~.\ IIJ iCfiwr‘//ll~ LIIIIl C‘l/llC “I’ .M/Jlhrr/ll~. .A 7-c/1 YCl//. F-/,tl,J\,+l /’ 111 (/ f i.r~hohr///,~ .S‘r,~~/>lc, ofT?,liOi) Srwcli.\/r Srt/?/cI I.\ .-\ pc’ /S%f’)Y. Part 112. Stochholm. S\*cden: The Karolink Iwtitute. Department ofEn\ironmentaI H>sirne. 1975.
CORREA. P.. PICKLE. L.W.. FONTHAM. E.. DXLAGER. N.. LIN. ‘t.. HAENSZEL. M‘.. JOHNSON. W.D. The c;~u\es of lung cancer in Louisiana. In: Il~/ell. M.. Correa. P. (ed\.) Ll//+! ctnrc~c~r’ C~/rc.\l~.\ ~111d Pi-c,1 l’/rfi/vr. P,-rlc~cc~/l~r~~.c ~lf‘llrr~ Ilrrc~r~lrtrri~ltl~,/ LWI’ C‘rllrc-c,r L’/,clt/rc~ C~/tfi’w~~c.c, Ncu Orleans: Verlq Chcmic International. Inc.. 19X-l. p. 73.
DAUBER. L.A.. LARSSON. L.G. Smohing and lung cancer utth special refxd to t!Je of smoking and type ofcancer. A c;tv--controI study in north Sv.eden. B,-iri\/,./or,r-,tcl/ofCo,rc (‘I 535 ,:673-6X I. May 10X6.
DAY. N.E. Epidemiological data and multistage carcinopenc\i\. In: Btirrsonyi. M.. Lapi\. K.. Day. N.E.. Yama\ahi. H. (edz.) Mc~t/c/.\. Mc,c~/rc/~~i.\/r/v t/lx/ Erio/o,p\. of’ 7ltnlcw Proruo/io/r. Lyon: IARC. lYX5. pp. MY-357.
DAY. N.E.. BROWN. C.C. Multt\tage model\ and primary pro cntton of cancer. ./ow~rtr/ ot t/w R;tr/io/rtr/ Ctrrtc w //t\/iro/c f&1):977-YXY. April I YXO.
DEVESA. S.S.. BLOT. W.J., FRAUMENI. J.F. JR. Decltning lunp cancer totes among )outy men and \%omen tn the United State\: .4 cohort analysk ./c~rrrw/ off/w ,Vr///orw/ Cr/,rc.c,v /usrirt/fc~ X I : 156X- I 5 7 1 . I YXY.
DOLL. R. The age distribution of cancer: Implication\ for model\ ofcarctnogenest~. ./rjr,r/~r// of’rtw Roy// .Srtr/r.\rrc~r// .Soc~icv,v A 131: 133-l 66. I97 I
DOLL. R.. GRAk’. R., HAFNER. B.. PETO. R. Mortalit> in relatton to \mohtnf: 22 bear\‘ obwvation\ on kmale Britt\h doctor\. HI-I/;\/I .Wc,c//c c//./c~r//./rc// 2X0(62 lY):Y67-Y7l. April 5. IYXO.
DOLL. R.. HILL. A.B. Mortality tn rclatwn to wtohing: Ten years’ ohvrvation\ of British doctor\. Bvrrrsl~ Mcv//w/ .torowl I : I iYY-I-I IO. Ma) 30. I YhJ.
DOLL, R.. PETO. R. blortality in relation to wiohin2: 20 yearh‘ oknations on male Britirh doctor\. &rri.sh Mrclic,ol .I~~rrm// 2: 1525% 1536. Dwemtw 25. I Y76.
DOLL. R.. PETO. R. Cigarette \tnoking and bronchial carcinom;t: Do\e and time rrlattonhhlp\ atnonp regular wloher\ and lifelong non-moherz. ./owrttr/ c,f’E/,iclc,t,rr~j/,~~~, oml C~~w~~~~~~r\ Hctrlflr 31(1):303~3 13. December lY7X.
ELWOOD. J.M.. PEARSON. J.C.G.. SKIPPEN. D.H.. JACKSON. S.M. Alcohol. smoking. wcial and occupational factor\ in the ac‘tiology ot‘cancerofthe oral ca\ It!. phar! nx and lar> nx. /,ttc~,.trt/tio/f[// .toromr/ ~~t’(‘rr/lc~cv~ 31:6034 12. I YX1.
FALK. R.T.. PICKLE. L.W.. BROWN. L.M.. !vlASON. T.J.. BUFFLER. P.A.. FRAUMENI. J.F. JR. Eftrct ofmohtn? and alcohol conwmption on lar). nseal cancer rt\h m co;t\tal Tc‘u\.
Ccr,rc,c>/. Rcsc,trr.c /I -!Y( I-l 1:-10211O’Y. Jtil! 15. I YXY. FARBER. E. The multtxtep nature of caner de\elopmwt. Cw( (‘I’ Kcccwj-c II 11:12 171223.
October 19X-1. FLAbDERS. W.D.. ROTHMAN. K.J. Interaction of ;Ilcohol and tobacco in larl,n~~al c;Lnct’r.
Anwit UII ./mmtr/ ,!l’E/~iclc,,trro/c,~?. I I& 3 ):37 I-i7Y. March I YX2. FREEDMAN. D.A.. NAVIDI. W.C. ‘vlulti\tuge model\ for carcinogencsi\. E/lr,f,-o,crlrc,rlro/
Hcwlrlr Prr-.\/w/i\ c\ XI : 169-l XX. May IYXY. GAFFNEY. M.. ALTSHULER. B. Exammatton of the role of cigarette mohc tn lung
carcinogenesk u\tng multi\tage model\. .tltro-llc/t lff r/w rVr/rioll1/l COIli ('I' /ll.\rl/lrrc~
X0( 12):Y25-Y3 I, Augu\t 17. I YXX. GAO. Y.T.. BLOT. W.J.. ZHENG. W.. FRALMENI. J.F.. HSI’. C.W. Lung cancer and
smohtnp tn Shanghai. //~rc~~~tftrr/o~rc//./or~~~~~o/ of E/Gc/c’r)lro/oq\. 17(21:277-2X0. June I YXX.
13X
GARFINKEL. L.. STELLMAN. S.D. Smoking and lung cancer in women: Findings in a prospective study. Cuticer Rescc~rc~/t 48(23):695 I-6955. December I. 1988.
GRAHAM, S.. LEVIN, M.L. Smoking withdrawal in the reduction of rish of lung cancer. Cancer 27(4):865-87 1. April I97 1.
HAENSZEL. W.. LOVELAND. D.B.. SIRKEN. M.G. Lung-cancer mortality as related to residence and smoking historic\. I. White males. ./orrrxu/ of’rhc, Nutir~tinl Ca,rc~o- //rsrrf(((c~ 28:947-1001. April 1962.
HAMMOND, E.C. Smoking in relation to the death rates of one million men and women. In: Haenszel. W. (ed.) El’idf,nlio/o~~;t,u/ Approtrc~tre.r I,J r/w Strtr!\ c!f’Cur~t~er (I/U/ Other Chrrvrrc~ Diseuws. NC1 Monograph 19. U.S. Department of Health. Education. and Welfare. Public Health Service. National Cancer Institute. January 1966. pp. 127-203.
HIGGINS, 1.T.. WYNDER. E.L. Reduction in risk of lung cancer among ex-smokers with particular reference to histologic type. C’ar~c~rr 62( I I ):2397-2401. December I. 19x8.
HIGGINS, I.T.T.. MAHAN. C.M.. WYNDER. E.L. Lung cancer among cigar and pipe smokers. P wI.eufi\,e Meclrr i/w 17( I ): 1 I61 28. January 198X.
JOHNSTON-EARLY. A.. COHEN, M.H.. MINNA. J.D., PAXTON. L.M.. FOSSIECK. B.E. JR.. IHDE. D.C.. BUNN. P.A. JR.. MATTHEWS, M.J.. MAKUCH. R. Smoking abstinence and small cell lung cancer survival. ./or(/./rol c!t r/tc ilntc~r-rc~tr~~ M~~tl/c~u/ 4.\.xo( i&w 244( I9):2 175-2 179. November 14. 19X0.
JOLY. O.G., LUBIN. J.H., CARABALLOSO. M. Dark tobacco and lung cancer in Cuba. ./arc/xc// c
PETO. J. Early- and late-stage carcmogene\is in mouse \kin and In man. In: BGrzs(inyi. M.. Lapis, K.. Day. N.E.. Yamasaki. H. (rds.) .Mr&/.\. Mc~c./l~/~~/\nl.c t/)1(/ &tirj/o,yx of’ 7rrn,olr,. Pwnrorio~~. Lyon: IARC. 1 YXI. pp. 33%370.
PHILLIPS. D.H.. HEWER, A., MARTIN. C.N.. GARNER. R.C.. KING. M..M. Correlation of DNA adduct levels in human lung with cigarette smoking. !%‘c/ntr.e 336(6101 ):790-792. December 2?-2Y. IYXX.
RANDERATH. E.. MILLER. R.H.. MITTAL. D.. AVITTS. T.A.. DUNSFORD. H.A..
RANDERATH. K. Covalent DNA damqe in tissues of cigarette smohers as determined hq “‘P-postlabeling assay. ./o/r,-,ro/ c!f rhc, ,v”lc!tioflcl/ CUII(.LJI. //~.srj!ll/c 8 I (5):3-l I-337. March l
19X9. ROGOT. E., MURRAY. J.L. Smoking and causes of death among U.S. veterans: I6 years of
observation. P~rhlic, Hculth /?q~~~/‘~.s Y5(3):2 13-227. May-June 1980. SACCOMANNO. G.. ARCHER. V.E.. AUERBACH. 0.. SAUNDERS. R.P.. BRENNAN.
L.M. Development of carcinoma of the lun, 17 as reflected tn exfoliated cells. Ctr,rcc/. 3 I ( I ):256-270. January 1971.
STENBACK. F.. PETO. R.. SHUBIK. P. Initiation and promotion at different ages and doses in 7200 mice. I. Methods. and the apparent persistence of initiated cells. &.itr.slr Jolrj./lu/ of Co/1~~c/~44(1):1-13.July 198la.
STENBACK. F.. PETO. R.. SHUBIK. P. Initiation and promotion at different ages and doses in 2100 mice. Il. Decrease in promotion bv TPA with age&g. B/.irich ./o~rr!,o/ (!/‘Co!rc,~r. 44(l):]%‘3.July IYXlb.
STENBACK, F.. PETO. R.. SHUBIK. P. Initiation and promotion at different ages and doses in 2200 mice. III. Linear extrapolation from high doses may underestimate low-dose tumour risks. R/?risll Jorrr./itil of’Cojlc,cj,- W( I ):21-31. July I9X Ic.
TUYNS, A.J.. ESTEVE. J.. RAYMOND. L.. BERRINO, F.. BENHAMOU. E.. BLANCHET. F.. BOFFETTA. P.. CROSIGNANI. P.. DEL MORAL. A.. LEHMAKK. W.. ET AL. Cancer of the larynx/hypopharynx. tobacco and alcohol: IARC International Case-Control Stud) in Turin and Varese (Italy). Zaragoza and Navarra (Spain). Geneva (Swnzerland) and Calvados (France). /,~rc’i.,~atio,lrr/ Jr)ro.,ltr/ of Ctr,,c,cl~- 4 I1J):4X3--20 I . April 15. 10x8.
U.S. DEPARTMENT OF HEALTH AND HUM?rN SERVICES. Tllr Hcwlth Co,t.~eyrre/l(.r.s oj Snlokiq: CU~~C~O~. ,4 Kcy~,.t ,~t rlrc, .SII~C~O/~ &,~c/-~r/. L1.S. Department of Health and Human Services. Public Heath Service.Officeon Smohlng and Health. DHHS Publication No. (PHS, x2-50179. 19x2.
U.S. DEPARTMENT OF HEALTH .4ND HCM.4N SERVICES. 7-/r<, Heulth C~,rr.\cc/ltolc,c,s of
SnloXlrl,~.~ cIiwflic~ oh.\rrlct Ill‘l’ LlfU~ ni.\tYrw .A Rq”“/ 1!/’ /AC Sfrrywi Gcvlcv~tr/. U.S. Department of Health and Human Sen ice\. Public Health Serb ice. Office on Smokmg and Health. DHHS Publication No. (PHS) XJ-50205. IYXI.
U.S. DEPARTMENT OF HEALTH r\ND HL’M.4N SERVICES. 7-11~~ Hctrlrl7 Co/l.\c,c/lrc,/lc,c,.\ of ImYdrorrrri~~ .stm~Aiu~. .4 Rt~/‘fw/ cq r/w Sfri-,~l~~Jll GcrIc~rtrl. 1’3. Department of Health and
Human Services. Public Health Sen ice. Centers for Disease Control. DHHS Publication No. ,CDC j X733YX. 19X6.
U.S. DEPARTMENT OF HEALTH AND HC‘XIAN SERVICES. Reclrrt ir,y //,c H~lrh Come- ~pm C.S 0f‘ .Snd~t~~ 2.5 ~~cw-.s of’ PuJ:‘I-CV. .4 Rrp/-t of //fly Sfrrqcwrl Grw,u/. U.S.
Department of Health and Human Senlces. Public Health Senice. Centers for Disease Control, Center for Chronic Di\es\e Prevention and Health Promotion. Office on Smohins and Health. DHHS Publication No. (CD0 X9-X-II I. 19x9.
U.S. DEPARTMENT OF HEALTH. EDUCATION. AND WELFARE. Sn,oX~rq (11r~/ Hrc~lrh il Report c!frlrp S~lqco/l &,r~c?rz~/. U.S. Department of Health, Education. and Welfare. Public Health Service. Office of the Assistant Secretary for Health. Office on Smoking and Health. DHEW Publication No. (PHS) 79-50066. 1979.
140

U.S. PUBLIC HEALTH SERVICE. S,voX/,i,q tr/rt/ H~wlrh. Rc/~~wI of I/W AC/I isor:\. Cor~rnrirrc~c~ lo /Iw S~rr.qvcw <;c,wrx/ cd r/w P~rh//c, Hctrlrlr .Sc/-r~/c~c. U.S. Department of Health. Education. and Welfare. Public Health Scn~ce. Center for Disease Control. PHS Publication No. I 103. 196-I.
WHITTEMORE. X.S. Effect of cigarette smohing in epidemiolofical \tudle\ of lung cancer. Sttrfrstic .< 111 Mcvlic~//rt~ 7( I-2 ):223-23X, January-February I OXX.
WIGLE. D.T.. M.40. Y.. GRACE. M. Relative importance of \mohing ;I\ a ri\k factor for selected cancers. C‘o,rtr<l/tr!! ./o~rr./rc// ofP/rh/it Hcwlth 7 I (-!):264-275. Jul!/August I YXO.
WI-I. A.H.. HENDERSON. B.E.. PIKE, M.C.. YL’. M.C. Smoking and other ri& factors for lung cancer In v.onien. .Io~o./ro/ o/‘//w NLI/I’OIINI Cwrc,er- I~l.ctr/~r/c 73(-I 1:7-17-75 I April I YX5.
WYNDER. E.L.. COVEY. L.S.. MABUCHI. K.. M1ISHINSKl. M. En\ lronmental factors in cancer of the lar) nx. A second look. C~/IIC (‘1. 3X(-I):15Y 1~1601. October 1976.
WYNDER. E.L.. KABAT. G.C. The effect of lowyIeld cigarette smoking on lung cancer risk. Cr/~,c PI’ 62(6):1223-l 230. September 15. 19Xx.
WYNDER. E.L.. STELLMAN. S.D. Comparative epldemlolog of tobacco-related cancers. C~/~~c.cr~ Rc~rtwrc.h 37( 12 ):360X3622. December I Y77.
WYNDER. E.L.. STELLMAN. S.D. Impact of long-tcm filter cigarette usage on lung and larynx cancer rish: A ca\e--controI stud). ./orrwtr/ ~!t’rlrc,.~trri~~/~o/ (‘t/!~( cj/-/,rsrirrtrc, 63 3 ):37 l- 377. March lY7Y.
I11
CHAPTER 5 SMOKING CESSATION AND
NONRESPIRATORY CANCERS

CONTENTS Introduction . .
Review of Specific Site\ Oral Cancer. . Esophageal Cancer . Pancreatic Cancer Bladder Cancer . Cervical Cancer . Breast Cancer Endometrial Cancer Other Cancer Sites
Multiple Primary Cancer<
Summary . .
Conclusion5 . .
References . .
.....................
.....................
.
......
......
. . . 117
147 l-17 IS2
. IS5 IS9 I65
. 16Y I69
. I72
. 176
177
. 17X
. . . l7Y
INTRODUCTION
Lung cancer. the first neoplasm causally linked to cigarette smoking, has been the cancer most thoroughly studied with respect to exposure-response relationships and benefits of cessation (US DHHS 1982). Subsequently, cigarette smoking has been established as a cause of cancer at diverse other sites. For some sites (e.g.. oral cavity ). the target cells are exposed directly to the various constituents of tobacco smoke. For other sites (e.g.. urinary bladder). absorption. transport. and metabolic activation of carcinogens in tobacco smoke result in exposure of target tissues. This Chapter reviews the evidence on smoking cessation and cancer risk at various nonrespiratory sites. The sites selected for review are those for which cigarette smoking has been determined to be a cause of cancer. or contributing cause. or those for which evidence indicates a possible association.
Methodologic issues encountered in inferring causality on the effects of smoking cessation have been discussed in Chapter 2 and will not be reviewed in detail in thts Chapter. Potential confounding by differences in prior tobacco exposure at the time of quitting. and by differences between former smokers and continuing smokers in other cancer-related risk factors may pose a greater obstacle to causal inference for the nonrespiratory cancers than for cancers of the lung or larynx: the smoking effects are generally smaller for nonrespiratory cancers. and the potential confounding factors are more numerous.
REVIEW OF SPECIFIC SITES
Oral Cancer
Tobacco use is a major cause of oral cancer (US PHS 1964: US DHHS 1982. 1989). An exposure-response relationship has been identified between the amount of tobacco consumed and the risk of cancer of the oral cavity after considering the effects of alcohol consumption. The proportion of 1985 oral cancer deaths attributable to cigarette smoking in the United States has been estimated to be 92 percent for men and 6 I percent for women (US DHHS 1989). The oral cavity, like the lung. receives direct exposure tocigarette smoke. Presumably, the causal association of cigarette smoking with cancer of the oral cavity reflects this contact and the same initiating and promoting agents that are considered to determine the development of lung cancer.
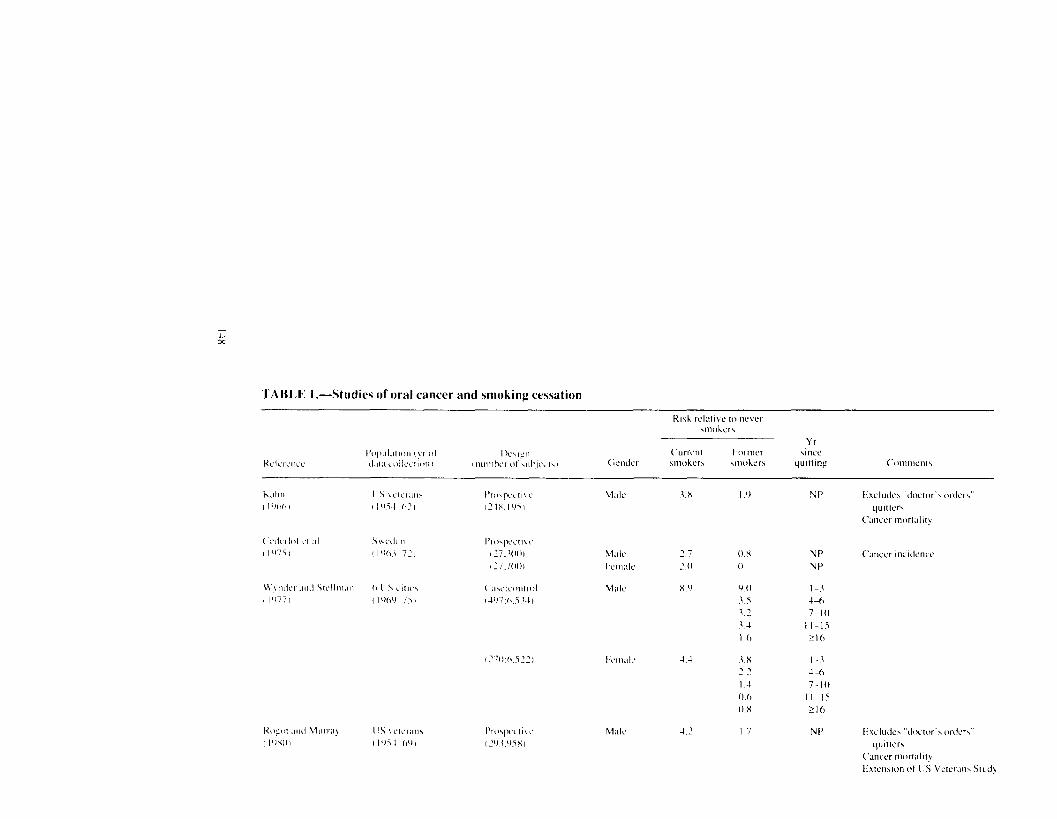
Table I summarizes studies that have examined the relationship between smoking cessation and oral cancer risk. In these studies, the risk of oral cancer among current smokers ranges from 2.0 to 18.1 times (median of approximately 4) the risk among never smokers. Oral cancer risks for women who are currently smoking seem lower than those for men in studies conducted prior to the mid- 1970s. but little difference by gender has been noted in more recent research. This gender pattern may be because of the initiation of smoking at an older age among earlier birth cohorts of women (US DHHS 1989) born during this century and the resultant low cumulative lifetime exposure of such women.
I17
4.4
12
3’ 3-t I 0
3.X 7.2 I.-l 0.6 0.x
I 7
NP Exclude\ “doctw .\ ordw” qutttee
<‘anccr mortalit)
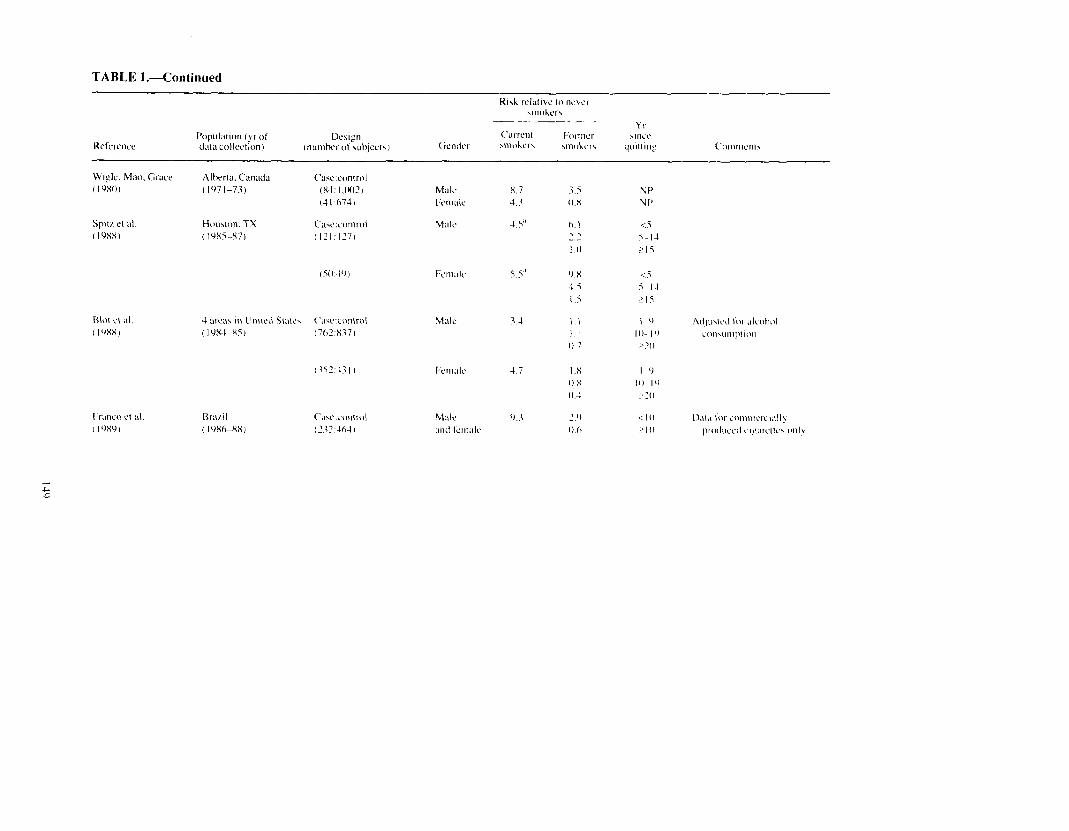
TABLE I.--Continued
Wifle. M:w, Grsce Alherra. Canada ( IYXOI (lY71-73)
(‘t~wxontrol (x3:l,lwJ (4 I .h74)
Houwm. TX (IYX5-X7)
Blot c, al (I’JXX)
Frsnco Cl d. ( I YXY )
Rrwil ( I ‘)X&XX,
X.7 2.5 3.3 0.X
4.5” h I 2.2 I 0
Nf’ N t’
<5 5-l 1
?I5

TAHIX I.--Continued








![Application of Multistage Stochastic Programming in ... · Mathematical modeling and optimization is a powerful tool for network plan-ning [36]. Stochastic programming provides modeling](https://img.pdfslide.us/doc/110x75/5e1ab9334eb1125af667c4ff/application-of-multistage-stochastic-programming-in-mathematical-modeling-and.jpg)