Embed Size (px)
Citation preview

Multiprofessional Critical Care Review Course - 2005
1
DISTURBANCES OF CARDIAC RHYTHM: TACHYARRHYTHMIAS
Sarah A. Stahmer, MD, FACEP
OBJECTIVES
• Understand the basic mechanisms of arrhythmias• Understand the basic types of supraventricular arrhyth mias
and their treatments• Understand the basic assessment of wide complex tachy-
cardias• Understand the basic management of atrial fi brillation • Understand the basic treatment of ventricular tachycardia
and fi brillation
Key Words: atrial fi brillation, atrial fl utter, atrioventricu-lar nodal reentrant tachycardia, orthodromic reciprocating tachycardia, ventricular fi brillation, ventricular tachycardia, Wolff-Parkinson-White syndrome
MECHANISMS OF TACHARRHYTHMIAS
The mechanisms of tachyarrhythmias are as follows:• Abnormal automaticity: This mechanism involves impulse
generation from cells that are not normally arrythmo-genic.
• Triggered automaticity: This mechanism is attributable to secondary depolarizations that arise during or after repolarization.
• Reentry: Reentry is the most commonly encountered mechanism. The genesis and propagation of an arrhyth-mia requires the presence of an area of slowed or delayed conduction, an anatomical or functional separate path of conduction and unidirectional block. Sites of reentry include the atria, perinodal tissues, and ventricles.
REGULAR SUPRAVENTRICULAR TACHYARRHYTHMIAS
Sinus Tachycardia
Electrocardiogram (ECG) criteria: With sinus tachycardia, the P wave morphology is upright in leads I, II, and aVF. There is a P wave before every QRS complex and constant P-R intervals. The rate is not fi xed; it varies with sympa-thetic/parasympathetic stimulus.
Clinical setting: The clinical setting includes catecholamines (cocaine, amphetamines), fever, hypotension, hypoperfusion, anxiety/fear, and tricyclic antidepressants (TCA, phenothi-azines, antihistamines).
Treatment: The preferred treatment is to treat the underly-ing disorder.
Atrial Tachycardia
The second type of regular supraventricular tachycardia is atrial tachycardia, which is shown in Figure 1.
ECG criteria: Atrial tachycardia is characterized by an atrial rate of 150 to 250 beats per minute (bpm). The P wave morphology is distinctly different from that of sinus rhythm, and the PR interval is usually greater than 0.12 milliseconds (msec). Atrioventricular node (AVN) is not necessary for rhythm maintenance. Administration of adenosine may cause AVN blockade, and the atrial tachycardia may be sustained or may abruptly terminate.
Clinical Setting: The mechanism of atrial tachycardia is frequently related to associated comorbidities. • Incisional reentrant atrial tachycardia is seen in patients
with a history of cardiac surgery. It is characterized by abrupt onset and termination.
• Focal atrial tachycardia is initiated and sustained by a nonsinus atrial focus. Episodes are usually prolonged, and the rhythm will typically “warm up” at onset. It is usually associated with digoxin toxicity, particularly when also associated with atrioventricular block (AVB). It is also seen in cardiomyopathy.
Treatment: Treatment depends on the underlying etiology and frequently requires antiarrhythmic therapy or ablation. Rate control may be diffi cult, and response to β-blockers or calcium channel blockers is unpredictable.
Atrial Flutter
The third type of regular supraventricular tachyarrhythmia is atrial fl utter (Figure 2).
Recognition: Atrial fl utter generally has an atrial rate be-tween 250 and 350 bpm and ventricular rates one half to one third the fl utter rate. Occasionally, atrial fl utter presents with a variable ventricular response. Atrial fl utter is a circuit that typically rotates in a counterclockwise fashion around the right atrium and has a negative saw-tooth pattern in inferior leads II and aVF and positive fl utter waves in lead VI. It is usually regular in untreated patients. Clinical pearl: An unchanging ventricular rate of 148-150 is atrial fl utter with 2:1 block until proven otherwise.
Clinical setting: This includes acute myocardial infarction (MI)/ischemic heart disease, congestive cardiomyopathy, pulmonary embolism (PE), and myocarditis.

Multiprofessional Critical Care Review Course - 2005
2
Figure 1. Atrial tachycardia

Multiprofessional Critical Care Review Course - 2005
3
Figure 2. Atrial Flutter

Multiprofessional Critical Care Review Course - 2005
4
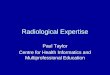
Figure 3. Paroxysmal supraventricular tachycardia: AV nodal reentrant tachycardia
Treatment: With atrial fl utter, the rhythm is inherently unstable and will convert to normal sinus rhythm (NSR) or atrial fi brillation (Afi b). For unstable patients, synchro-nized cardioversion is 25-50 J. For stable patients, control the ventricular rate with diltiazem, β-blockers, or digoxin. Never use Type Ia anti arrhythmics before ventricular rate is controlled. (They will enhance AV conduction and may result in 1:1 conduction.)
Paroxysmal Supraventricular Tachycardia: AV Nodal Reentrant Tachycardia
The fi nal type of regular supraventricular tachyarrhythmia (SVT) is paroxysmal supraventricular tachycardia. AV nodal reentrant tachycardia (AVNRT, Figure 3) is one of the sub-categories of this type of tachycardia.
Recognition: This type of tachycardia is characterized by regular, rapid rhythm with ventricular rates ranging from 140-280 beats/minute (bpm). The QRS is narrow, unless there is a preexisting bundle branch block (BBB) or rate-related bundle. Most reentrant arrhythmias are triggered by
a premature atrial contraction (PAC) that blocks down the fast pathway (which has a long refractory period) and con-ducts down the slow pathway ( which has a short refractory period). The atrium is depolarized retrograde, and the P wave is usually buried. When the P-wave is seen, it suggests that the reentry pathway is conducting retrograde via the slow pathway, or via a bypass tract. Clinical setting: The precipitating event in reentrant tachy-cardias is usually a premature atrial beat, so any process that causes PACs will put the patient at risk. These include processes that result in atrial stretch (acute coronary syn-drome [ACS], congestive heart failure [CHF]), irritability (exogenous catecholamines), and irritation (pericarditis).
Treatment: Typical treatment includes vagal maneuvers, adenosine (this is the drug of choice), diltiazem, or β-block-ers. Unstable patients should be synchronously cardioverted at 25-50 J.

Multiprofessional Critical Care Review Course - 2005
5
Figure 4. Orthodromic reciprocating tachycardia
Paroxysmal Supraventricular Tachycardia: Orthodromic Reciprocating Tachycardia
The other subcategory of paroxysmal supraventricular tachy-cardia is known as orthodromic reciprocating tachycardia (ORT) (Figure 4).
Recognition: ORT is a narrow complex tachycardia. An-terograde (forward) conduction occurs via the normal AV nodal conduction system with retrograde conduction via a concealed accessory pathway. The PR interval is forcibly longer than with AVNRT because of slow retrograde conduc-tion up the accessory pathway.
Clinical setting: The clinical setting is similar to that of AVNRT. Treatment: The treatment is similar to that for AVNRT. Be-cause this dysrhythmia it is obligated to use the AV node for anterograde conduction, it is amenable to AV nodal blocking agents for acute and chronic therapy. However, pharmaco-logic therapy is frequently less than adequately effective, and
recurrences on medical therapy are common. This arrhythmia is also very amenable to catheter ablation, which has a 95% success rate and a low complication rate.
IRREGULAR SUPRAVENTRICULAR TACHYARRHYTHMIAS
Multifocal Atrial Tachycardia
The fi rst type of irregular supraventricular tachyarrhythmia discussed in this chapter is the multifocal atrial tachycardia (Figure 5).
Recognition: Multifocal atrial tachycardia is a narrow com-plex, irregular tachycardia that is attributable to abnormal automaticity of multiple atrial foci. The P waves will dem-onstrate at least three different morphologies, with variable PR intervals. The atrial rate varies from 100-180 bpm.
Clinical Setting: Multifocal atrial tachycardia is typically seen in patients with acute exacerbations of chronic obstruc-

Multiprofessional Critical Care Review Course - 2005
6
Figure 5. Multifocal atrial tachycardia
tive pulmonary disease. It is occasionally associated with CHF, sepsis, and theophylline toxicity.
Treatment: Treat the underlying disorder! Antidysrhythmics are usually not helpful in treating multifocal atrial tachy-cardia. Intravenous (IV) magnesium (which may reduce atrial ectopy) and IV verapamil/diltiazem may decrease the ventricular response rate, and amiodarone may restore sinus rhythm. The rhythm will usually abate once the underlying (usually respiratory) disorder is treated.
Atrial Fibrillation
Atrial fi brillation is one of the most common atrial arrhyth-mias (Figure 6).
Recognition: Atrial fi brillation is characterized by a lack of organized atrial activity. On the ECG it manifests as a lack of clear P waves between QRS complexes and an irregular ventricular response. Atrial fi brillation has now been shown to be attributable to multiple reentrant wavelets conducting between the right and left atrium.
• Baseline wavers without P waves (the atria never uniformly depolarize)
• Ventricular rate determined by degree of AV conduction (untreated usually > 170 bpm)
• QRS usually narrow unless there is a preexisting BBB or, after a long R-R interval, a beat is conducted with a short R-R interval and is aberrant (Ashman’s phenomenon).
Clinical Setting: Ischemic heart disease (with or without infarction), hypertension, thyrotoxicosis, “holiday heart,” pericarditis
Treatment: Acute management of atrial fi brillation initially focuses on rate control and anticoagulation. Rate control is usually achieved through the use of calcium channel blockers, β-blockers, amiodarone, and digoxin to slow the ventricular response. Digoxin and amiodarone may be particularly effec-tive in light of their lack of negative inotropic effect.
Emergent cardioversion: Emergent cardioversion is indicat-ed in the setting of severe refractory congestive heart failure, intractable angina, or refractory hypotension when ventricular

Multiprofessional Critical Care Review Course - 2005
7
Figure 6. Atrial fi brillation
response cannot be controlled. Unstable patients may be cardioverted (synchronized) beginning at 100-200 J.
Elective cardioversion: Patients with duration of atrial fibrillation less than 48 hours may generally undergo cardio version to normal sinus rhythm with minimal risk of thromboembolism. The rate of embolism with cardio ver sion within 48 hours without prior anticoagulation is estimated to be approximately 0.8%. Pharmacologic therapy for acute conversion to sinus rhythm may also be performed within 48 hours.
Chemical conversion (after slowing VR): Procainamide, disopyramide, propafenone, sotalol, fl e cainide, amiodarone, and ibutilide. A newer agent is dofetilide, a recently approved class III antiarrhythmic.
Anticoagulation: Atrial fi brillation is known to be associated with increased risk of stroke and death. The risk of thrombo-embolism in nonanticoagulated patients is between 5% and 6% per year but may be as high as 20% in certain populations, including the elderly and those with certain valvular lesions (i.e., mitral stenosis).
WIDE COMPLEX TACHYCARDIAS
Polymorphic VT
Defi ned as a QRS complex greater than 120 msec with rate greater than 100 beats per minute. The differential diagnosis includes SVT with aberrancy, accessory pathway conduc-tion, pre-excitation syndrome (e.g., Wolff-Parkinson-White syndrome [WPW]) or ventricular tachycardia (VT). The majority of patients presenting with a wide complex tachy-cardia will be diagnosed with VT; if the patient has a history of coronary artery disease the incidence increases to 95%. Careful inspection of the 12-lead ECG will allow correct determination of the diagnosis in approximately 90% of patients. Despite this fact, VT is frequently misinterpreted as being supraventricular tachycardia with aberrancy. Common errors include the assumption that VT cannot be “narrow,”and that it cannot occur in an awake patient. In addition, there is a lack of familiarity with ECG criteria for VT. See Table 1 for an algorithm demonstrating steps in diagnosing wide QRS-complex tachycardia.

Multiprofessional Critical Care Review Course - 2005
8
ECG criteria: A number of decision rules have been pro-posed in an attempt to identify features on the 12-lead ECG that will aid in the diagnosis of VT. The criteria vary in their reliability when applied individually and must be interpreted in conjunction with the other criteria —and with the patient’s clinical presentation, medical history, and previous ECG when available. A frequently used diagnostic algorithm by Brugada et al incorporates many previously published morphology criteria in a stepwise algorithm (see Table 2); it has been demonstrated to be very sensitive and specifi c in the absence of preexisting intraventricular conduction abnormalities. Wide complex tachycardias are divided into right and left bundle branch type. If the complex is upright in lead V1 of a standard 12-lead ECG then it is defi ned as a right bundle branch type. If the complex is negative in lead V1 then it is defi ned as a left bundle branch type.
Clinical setting: Sustained VT is defi ned as VT lasting greater than 30 seconds. The rhythm can originate from any part of the myocardium and/or conduction system below the atrioventricular node. VT is frequently seen as a complication of coronary artery disease (CAD) due to active ischemia or presence of scar tissue, both of which can create substrates for ventricular arrhythmias. Patients with cardio myopathies, particularly the idiopathic dilated type, are the second largest group of patients at risk for developing VT. However, VT can also occur (although rarely) in healthy people, or it may be the fi rst indication of organic heart disease, for example, right ventricular dysplasia. Medications, particularly some antiarrhythmic therapies can be proar rhyth mic under certain clinical conditions, and give rise to ventric ular arrhythmias.
Table 1. Diagnosis of wide QRS complex tachycardia with a regular rhythm
They include digoxin, Type I anti ar rhythmics, phenothi-azines, tricyclic antiarrhythmics, and sympathomimetics. Medications that cause prolongation of the QT interval can generate a specifi c polymorphic form of VT known as torsades de pointes. Finally, severe or acute electrolyte imbalances, particularly hypokalemia and hyperkalemia, can give rise to VT.
Treatment: The new Advanced Cardiac Life Support (ACLS) guidelines differentiate the treatment of VT in patients with normal left ventricular function from those with diminished function. For patients with depressed left ventricular func-tion, the pharmacologic treatment of choice is IV amiodarone administered as a 150-mg bolus over 10 minutes. It has been successfully used for out-of-hospital cardiac arrests with a 300-mg IV bolus. In patients with preserved left ventricular function and wide complex arrhythmia of unknown etiology or VT, acceptable choices of therapy include DC cardio ver sion, amiodarone, or procainamide. For every tachy ar rhyth mia, amiodarone may be used as a primary or secondary choice. Lidocaine is now considered secondary in therapy as a result of its limited effectiveness in ventricular tachycardia in nonisch-emic tissue. It should be noted that the use of combination antiarrhythmic therapy is strongly discouraged because of a proarrhythmic potential and limited effi cacy.
DC cardioversion is a universally acceptable treatment option, and it should be considered whenever a patient is hemodynamically unstable, fails to respond to antiarrhythmic therapy, or is experiencing chest pain or its equivalent. Proper sedation should always be provided before cardioversion.
Polymorphic VT: Torsades de Pointes: Prolonged QT Interval
Recognition: Torsades de pointes (see Figure 7) is a rapid polymorphic VT that is characterized by beat-to-beat vari-ability in the QRS complexes, which vary in both amplitude and polarity. The resultant QRS complexes appear to “twist” around the isoelectric line. A prerequisite for the rhythm is baseline prolongation of the QT interval, which may be congenital or acquired. Torsades is initiated by a series of ectopic beats that begin with a premature ventricular beat or salvo of ventricular beats, followed by a pause, and then a supraventricular beat. Another premature ventricular beat arrives at a relatively short coupling interval and falls on the preceding T wave, precipitating the rhythm.
Torsades is usually paroxysmal in nature, and the underlying rhythm and intervals can be identifi ed during “breaks” in the rhythm. Typically, there are 5 to 20 complexes in each cycle, and the rhythm self-terminates or degenerates into ventricular fi brillation. The ventricular rate is usually between 200 and 250 bpm, and the amplitude of the QRS complexes will vary in a sinusoidal pattern.The baseline ECG will usually provide important clues to the nature of the arrhythmia. Because the QT interval lengthens with decreasing heart rate, measure-

Multiprofessional Critical Care Review Course - 2005
9
ment of a rate-independent QT interval may be calculated. The standard correction for rate is the QT interval divided by the square root of the R-R interval measured in milliseconds. The presence of a corrected QT interval of greater than 440-450 milliseconds should be considered abnormal. Patients with QT intervals corrected for rate greater than 500 mil-liseconds, and certainly 600 milliseconds, have been shown to be at increased risk for torsades de pointes. In addition to prolongations of the corrected QT interval (QTc), there may be changes in the ST segment and T wave that would provide clues to an underlying metabolic abnormality.
Clinical Setting: Acquired causes of QT prolongation are by far the most common, with medications (type Ia anti-arrhythmics) and electrolyte imbalances (hypokalemia, hypomagnesemia) the most frequent culprits.
Some patients present with syncope or sudden death and are found to have polymorphic VT, torsades de pointes, and a prolonged QT interval without any clear predisposing medication or condition. These patients have congenital long QT syndrome. Treatment: Treatment of torsades in the setting of acquired long QT syndrome leading to torsades de pointes consists of removing offending agents or conditions. Further therapy includes treatment with IV magnesium, which prevents the onset of torsades de pointes. Temporary pacing or admin-istering isoproterenol increases the underlying heart rate and shortens the QT interval. Therapy for symptomatic congenital long QT syndrome is considered to consist of β-blocker therapy and pacing. Some advocate a left stellate ganglionectomy.
Right ventricular outfl ow tract ventricular tachycardia (RVOT-VT): This form of VT (see Figure 8) is seen in patients without underlying heart disease. It originates from or near the right ventricular outfl ow tract and, typically, has a left bundle branch block (LBBB) morphology and right inferior axis.
Patients will present with palpitations or syncope, and trig-gers are thought to be exercise and other causes of increased adrenergic tone. It typically responds to β-blockers or cal-cium-channel blockade. It has been reported to respond to adenosine, and it can be misinterpreted as supraventricular tachycardia with aberrancy.
Polymorphic VT: Normal QT Interval
This form of VT will often appear as torsade, the difference is the absence of QT prolongation. Patients with this rhythm are often found to have unstable coronary artery disease, and acute myocardial ischemia is felt to be an important prerequisite for this arrhythmia. These patients are usually unstable, and DC cardioversion is the treatment of choice.
Table 2. Morphology criteria for ventricular tachycar-dia*
Ventricular Fibrillation
Recognition: For ventricular fi brillation (VF) the ECG shows complexes that are grossly irregular without P waves or clear QRS morphology (see Figure 9). Clinical Setting: This rhythm does not generate meaningful cardiac contractions, and the patient is always unconscious. VF is seen in patients with severe ischemic heart disease, acute MI, hypothermia, blunt chest trauma.
Treatment: VF is treated by immediate defi brillation. This process should be repeated if the fi rst attempt is unsuccess-ful. Amiodarone 300 mg IVP if the patient fails to respond to defi brillation 3 times and fails to cardiovert. Rewarming should be initiated if the patient becomes hypothermic. PRE-EXCITATION SYNDROMES
WPW Syndrome
Recognition: With WPW syndrome, the baseline ECG when the patient is in sinus rhythm is a short PR interval and “delta” wave —a slurring of the upstroke of the R wave. There are associated ST-T changes secondary to altered depolariza-tion/repolarization. A predisposition to tachy dys rhythmias is associated with WPW syndrome; atrial fl utter (5%), atrial

Multiprofessional Critical Care Review Course - 2005
10
Figure 7. Polymorphic ventricular tachycardia: Torsades de pointes
Figure 8. Right ventricular outfl ow tract ventricular tachycardia

Multiprofessional Critical Care Review Course - 2005
11
Figure 9. Ventricular fi brillation
Figure 10. Wolff-Parkinson-White syndrome, a pre-excitation syndrome

Multiprofessional Critical Care Review Course - 2005
12
fi brillation (10% to 20%), and paroxysmal SVT (40% to 80%) are the most common (see Figure 10).
Clinical Setting: WPW is the most common form of pre-ex-citation. The cause of this abnormal ventricular depolarization is the presence of one or more accessory pathways. These ac-cessory pathways are small bands of tissue, called the Kent’s bundle, that failed to separate during development, thereby al-lowing continued electrical conduction between the atria and ventricles at sites other than at the AV node. The accessory pathway conduction circumvents the usual conduction delay between the atria and ventricles that occurs within the AV node. This leads to early eccentric activation of the ventricles with subsequent fusion with the usual AV nodal conduction. These pathways may allow rapid conduction from the atria to the ventricle, which may predispose patients to a risk of sudden death from ventricular fi brillation.
Treatment: Treatment of the dysrhythmia requires one to identify the underlying rhythm, and then understand the implications of “usual treatment” in the presence of a bypass tract. The key difference lies in rhythms that do not depend on the AVN for perpetuation, such as atrial fi brillation and fl utter. Usual treatment in these rhythms consists of control-ling the ventricular rate with agents that block the AVN. In
the setting of a bypass tract, blocking the AVN will result in impulse conduction down the accessory pathway, which does not have the inherent refractoriness that the AVN has. The pathway can conduct atrial rates in excess of 300 bpm, which can precipitate degeneration into ventriculoar fi brillation.
Atrial fi brillation and fl utter in the setting of WPW
Atrial fi brillation and fl utter are less commonly seen in as-sociation with WPW, and yet are the most feared (Figure 11). In both atrial fi brillation and fl utter, atrial depolarization rates are equal to or greater than 300 bpm. Atrial impulses are blocked at the AV node because of its relatively long refractory period, and concealed conduction and ventricular response rates are much slower. Accessory pathways have signifi cantly shorter refractory periods and faster conduction time compared to the AV node, and in these rhythms, nearly all atrial depolarizations are conducted down the accessory pathway. The pattern of ventricular activation will vary dependent on the relative proportion of electrical activation conducted via the AV node and accessory pathway, resulting in widened and bizarre-appearing QRS complexes that vary in width on a beat-to-beat basis.
Figure 11. Atrial fi brillation and fl utter in the setting of Wolff-Parkinson-White syndrome

Multiprofessional Critical Care Review Course - 2005
13
The appearance of atrial fi brillation in the setting of a bypass tract can easily be confused with polymorphic VT or atrial fi brillation with rate-related aberrancy. The ventricular re-sponse in polymorphic VT is never as grossly irregular as atrial fi brillation. Inspection of the ECG in atrial fi brillation in WPW will also show that the QRS is usually relatively narrow at the shortest R-R intervals (fastest heart rates) due to sole conduction down the bypass tract. This is because the AV node cannot conduct at ventricular response rate approaching 300 bpm, whereas the bypass tract can. This is also in direct contrast to rate-related aberrancy, where the QRS complexshould be most aberrant at the shortest R-R intervals.
Usual treatment of atrial fi brillation (without an accessory pathway) consists of cardioversion for unstable patients. For stable patients the ventricular response is controlled with agents that block the AVN. Cardioversion of the atrial fi brillation is still the intervention of choice for unstable patients, and the presence of an accessory pathway does not alter this. For the stable patient with an accessory pathway, blocking the AVN will result in impulse conduction entirely down the accessory pathway. The pathway has the potential to conduct at rates in excess of 300 bpm, which can precipitate degeneration into ventricular fi brillation. The treatment is to
slow conduction through the bypass tract, which is usually accomplished with procainamide and amiodarone.
Orthodromic, Reentrant SVT
Orthodromic, reentrant SVT will appear as a narrow com-plex, regular tachycardia. Drugs or maneuvers that slow AV conduction can be used, where even in the presence of a bypass tract the AVN is an integral component of the reentrant pathway. Blocking the AVN will abruptly “break” the rhythm.
Antidromic wide complex SVT
Because of antegrade conduction down the bypass tract, the rhythm will be regular and will have wide QRS complexes. Agents that block the AVN will be effective in breaking the reentrant circuit, but the clinician must be sure of the rhythm interpretation. When in doubt, a trial of adenosine is often helpful. If the rhythm fails to “break,” then procainamide or amiodarone are reasonable choices.
Figure 12. Orthodromic, reentrant supraventricular tachycardia

Multiprofessional Critical Care Review Course - 2005
14
Pacemaker-Mediated Tachycardia
Recognition: Regular, rapid, wide complex rhythm in a patient with a DDD (dual pacing, sensing, and inhibition)pacemaker.
Clinical setting: This is a reentrant tachycardia that occurs when sensing of a retrograde atrial depolarization triggers ventricular pacing and is sustained by the pacemaker. It is usually initiated by a premature ventricular contraction, which is conducted retrograde to the atria and is subsequently sensed by the pacemaker.
Treatment: Application of a magnet converts the pacer to the DOO (pacing function only) mode, which disrupts the sensing function of the pacemaker and terminates the rhythm. The rhythm will not recur once the magnet is removed. If the rhythm does reoccur, then the rhythm is likely to be atrial fl ut-ter where the ventricular response rate is at the programmed upper limit of the pacemaker.
BIBLIOGRAPHY
Akhtar M. Clinical spectrum of ventricular tachycardia. Circulation. l990;82:l561-1573.
Cardall TY, Brady WJ, Chan TC, Perry JC, Vilke GM, Rosen P. Per-manent cardiac pacemakers: issues relevant to the emergency physician, part II. J Emerg Med. 1999;17:697-709.Excellent review of problems due to pacemaker malfunction or complications arising from having a pacemaker. Includes topics such as recognition of AMI in paced rhythms, pace-maker mediated tachycardia, and pacemaker Twiddler’s syndrome.
Brady WJ, Skiles J. Wide QRS complex tachycardia: ECG differ-ential diagnosis. Am J Emerg Med. 1999;17:376-381. Comprehensive review of causes of wide complex tachycar-dia.
Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new ap-proach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991;83:1649-1659. A classic article illustrating an algorithmic and reproduc-ible approach to differentiating wide complex tachycardia.
Buxton AE, Duc J, Berger EE, Torres V. Nonsustained ventricular tachycardia. Cardiol Clin. 2000;18:327-336, viii.
Delle Karth G, Geppert A, Neunteufl T, et al. Amiodarone versus diltiazem for rate control in critically ill patients with atrial tachyarrhythmias. Crit Care Med. 2001;29:1149-1153.Crit Care Med. 2001;29:1149-1153.Crit Care MedA prospective randomized study comparing the effects of diltiazem and 2 amiodarone regimens in their ability to
Figure 13. Pacemaker-mediated tachycardia

Multiprofessional Critical Care Review Course - 2005
15
control the rate of acute atrial tachyarrhythmias in criti-cally ill patients. The drugs were comparable with respect to rate control, but diltiazem was associated with a higher incidence of hypotension.
Ferguson JD, DiMarco JP. Contemporary management of parox-ysmal supraventricular tachycardia. Circulation. 2003;107: 1096-1099.Excellent review of new approaches to management of paroxysmal SVT.
Fogel RI, Prystowsky EN. Management of malignant ventricular arrhythmias and cardiac arrest. Crit Care Med. 2000;28(10 Crit Care Med. 2000;28(10 Crit Care MedSuppl):N165-N169.Reviews the current management of patients with sudden cardiac arrest, including identifi ers of patients at risk, treat-ment of acute cardiac arrest, and management of survivors.
Kindwall KE, Brown J, Josephson ME. Electrocardiographic criteria for ventricular tachycardia in wide complex left bundle branch block morphology tachycardias. Am J Cardiol. 1988;61:1279-1283.Identifi es criteria for distinguishing SVT with preexisting left bundle branch block from patients with VT.
Fuster V, Ryden LE, Asinger RW, et al. ACC/AHA/ESC Guide-lines for the Management of Patients With Atrial Fibrilla-tion: Executive Summary A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation) Developed in Collaboration With the North American Society of Pacing and Electrophysi-ology. Circulation. 2001;104:2118-2150. Current updated recommendations for management of atrial fi brillation.
Gregoratos G, Cheitlin MD, Conill A. ACC/AHA guidelines for im-plantation of cardiac pacemakers and antiarrhythmia devices: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Com-
mittee on Pacemaker Implantation). J Am Coll Cardiol. 1998; 31:1175-1209. Review of indications for implantation of pacemakers and implantable cardiac defi brillators.
Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2000;102(Suppl). The entire supplement features updated guidelines for resus-citation and an explanation of supportive data.
Passman R, Kadish A. Polymorphic ventricular tachycardia, long Q-T syndrome, and torsades de pointes. Med Clin North Am.2001;85:321-341.Comprehensive review of “atypical” ventricular tachy ar-rhyth mias—recognition and clinical and pharmacologic management.
Pollack ML, Chan TC, Brady WJ. Electrocardiographic manifesta-tions: aberrant ventricular conduction. J Emerg Med. 2000; 19:363-367.Reviews ECG criteria to identify patients with aberrant conduction resulting in wide QRS.
Stewart RB, Bardy GH, Greene HL. Wide complex tachycardia: misdiagnosis and outcome after emergent therapy. Ann Intern Med. 1986;104:766-771.Description of common misdiagnoses of wide complex tachy-cardias and cliical outcomes.
Trohman RG. Supraventricular tachycardia: implications for the intensivist. Crit Care Med. 2000;28(10 Suppl):N129-N135An excellent review of SVT, including recognition, mecha-nisms, precipitants, and treatment of commonly encountered rhythms.
Wellens HJ, Brugada P. Diagnosis of ventricular tachycardia from the 12-lead Eeectrocardiogram. Cardiol Clin. 1987;5: 511-525.Classic article describing fi ndings on the 12-lead ECG that will identify patients with VT as the cause of their wide complex tachycardia.