Embed Size (px)
Citation preview

Models and Technologies
Multiplex Three-Dimensional Mapping ofMacromolecular Drug Distribution in the TumorMicroenvironmentSteve Seung-Young Lee1,2, Vytautas P. Bindokas3, and Stephen J. Kron1,2
Abstract
Macromolecular cancer drugs such as therapeutic antibo-dies and nanoparticles are well known to display slow extrav-asation and incomplete penetration into tumors, potentiallyprotecting cancer cells from therapeutic effects. Conventionalassays to track macromolecular drug delivery are poorlymatched to the heterogeneous tumor microenvironment,but recent progress on optical tissue clearing and three-dimensional (3D) tumor imaging offers a path to quantitativeassays with cellular resolution. Here, we apply transparenttissue tomography (T3) as a tool to track perfusion anddelivery in the tumor and to evaluate target binding andvascular permeability. Using T3, we mapped anti–programmed cell death protein-ligand 1 (PD-L1) antibodydistribution in whole mouse tumors. By measuring 3D pen-etration distances of the antibody drug out from the bloodvessel boundaries into the tumor parenchyma, we determined
spatial pharmacokinetics of anti–PD-L1 antibody drugs inmouse tumors. With multiplex imaging of tumor compo-nents, we determined the distinct distribution of anti–PD-L1 antibody drug in the tumor microenvironment with dif-ferent PD-L1 expression patterns. T3 imaging revealed CD31þ
capillaries are more permeable to anti–PD-L1 antibody trans-port compared with the blood vessels composed of endothe-lium supported by vascular fibroblasts and smooth musclecells. T3 analysis also confirmed that isotype IgG antibodypenetrates more deeply into tumor parenchyma than anti-Her2 or anti-EGFR antibody,whichwere restrained bybindingto their respective antigens on tumor cells. Thus, T3 offerssimple and rapid access to 3D, quantitative maps of macro-molecular drug distribution in the tumor microenvironment,offering anew tool for development ofmacromolecular cancertherapeutics.
IntroductionMacromolecular agents including antibodies, proteins, poly-
mer–drug conjugates, and drug-loaded nanoparticles for chemo-therapy, hormone therapy, targeted therapy and/or immunother-apy are critical tools in the cancer treatment armamentarium(1–4). Macromolecular drugs display distinct pharmacokineticand tumor distribution profiles from small-molecule drugs (5).The enhanced permeability and retention (EPR) effect (6), basedon the hypothesis that a disordered vasculature that favors mac-romolecule accumulation would be a common feature of tumors,has longprovided a rationale for development ofmacromolecularoncology drugs (7–9). However, real-world performance hasbeen disappointing, with many agents displaying very low tumorspecificity (10–12). Furthermore, what does reach the tumor mayonly reach perivascular cells, leaving much of the parenchyma
untreated (13). Subsequent work has revealed multiple barriersthat limit tumor delivery, leading to a range of pharmacologic andphysical approaches to enhancing extravasation and penetration(14–16). These studies have exposed a critical need for assays totrackmacromolecular drug delivery in three dimensions andwithcellular resolution.
Amajor advantage of in vivo drug trackingmethods such as PETwith CT or MRI is access to real-time monitoring of appropriatelytagged macromolecular drugs in large volumes, but theseapproaches are limited to millimeter resolution and offer limitedanatomic detail (17, 18). Although intravital fluorescencemicros-copy offers cellular resolution, imaging is often limited to aspecific tumor region and just one or two features, such as thedrug and microvasculature (19). Biopsy followed by fixation,embedding, and sectioning enables analysis by multiplexed IHCor immunofluorescence (20), allowing simultaneous detection ofthe drug along withmultiple features of themicroenvironment atmicrometer resolution (21, 22). However, the tortuous micro-vasculature makes estimating delivery from 2D thin sectionsunreliable, while 3D reconstruction from serial sections may beimpractical for multiple samples (23).
Recent advances in tissue optical clearing combined withmultiplex immunofluorescent detection and new microscopymethods have dramatically improved capabilities to map cellularmarkers in "whole mount" samples such as intact organs and/ortissue fragments that are stained and imaged without sectioning(24, 25). Several tissue clearing methods have been successfullyapplied to tumor tissue, providing high-resolution, 3D images ofthe microenvironment and demonstrating feasibility for trackingnanoparticle and macromolecular drug delivery (26, 27). At the
1Department of Molecular Genetics and Cell Biology, The University of Chicago,Chicago, Illinois. 2Ludwig Center for Metastasis Research, The University ofChicago, Chicago, Illinois. 3Integrated Light Microscopy Facility, The Universityof Chicago, Chicago, Illinois.
Note: Supplementary data for this article are available at Molecular CancerTherapeutics Online (http://mct.aacrjournals.org/).
Current address for S.S.-Y. Lee: Department of Biopharmaceutical Sciences, TheUniversity of Illinois at Chicago, Illinois.
Corresponding Author: Stephen J. Kron, 929 E. 57th Street, Chicago, IL 60637.Phone: 773-834-0250; Fax: 773-834-1815; E-mail: [email protected]
doi: 10.1158/1535-7163.MCT-18-0554
�2018 American Association for Cancer Research.
MolecularCancerTherapeutics
www.aacrjournals.org 213
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

same time, these pioneering efforts have exposed potentialdrawbacks of current approaches including slow processingspeed, antigen loss, and destructive methodologies that maylimit their application to drug distribution and pharmacokineticstudies (28).
To address these challenges, we have adapted transparent tissuetomography (T3; ref. 29), a simple and fast tissue clearing andmultiplex 3D imaging method, to track macromolecular drugdistribution in the tumor microenvironment. With T3, perfusionand extravasation of macromolecular drugs are readily measured,and the agents can be localized with respect to their moleculartarget and in the context of cell types and other features in themicroenvironment. To apply T3 to track protein drug delivery, wemodeled immune checkpoint blockade with anti–programmedcell death protein-ligand 1 (PD-L1) mAb, examining antibodydistribution and PD-L1 targeting in 3D at cellular resolution inmurine mammary tumors. T3 also enabled direct comparison ofthe tumor penetration of model therapeutic mAbs targetingtumor antigens versus an isotype control. Thereby, we examineddelivery of anti-Her2 to a Her2 transgenic murine mammarytumor and anti-EGFR antibodies to a lung cancer patient-derivedxenograft (PDX) tumor, comparing each with isotype controls.Similarly,we also validated T3withfluorescent dextran as amodelfor polymer–drug conjugates and PEGylated liposomal doxoru-bicin (Doxil) as amodel nanoparticle. This work establishes T3 asa tool for quantitative, 3D spatial analysis of macromoleculardrug distribution in the tumor microenvironment.
Materials and MethodsMouse tumor models
BALB/c female mice (6–8 weeks old) were purchased fromEnvigo. Transgenic BALB/c males carrying the mutated rat Her2/neuoncogenedrivenby theMMTVpromoter (BALB-NeuT; ref. 30)were bred with wild-type BALB/c females. Genotypes of offspringwere determined by PCR of tail snips. BALB-NeuT female micedeveloped spontaneous mammary carcinoma in each mammarygland between 5 and 33 weeks of age. TUBO cells, derived from aspontaneous mammary tumor in a BALB-NeuT female mouse,and 4T1 cells (ATCCCRL-2539TM) were cultured in 5%CO2 andmaintained in RPMI1640 and DMEM supplemented with 10%heat-inactivated FBS, 2 mmol/L L-glutamine, and 100 U/mLpenicillin, respectively. Subcutaneous tumors were formed byinjection of 5 � 105 TUBO or 4T1 cells into the right flank offemale BALB/c mice and used for the indicated studies 14 daysafter injection. A PDXmousemodel of non–small cell lung cancer(Model ID: TM00231) was purchased from The Jackson Labora-tory and engrafted into immunodeficientNSGmice. Allmiceweremaintained under specific pathogen-free conditions. The studyhas been approved by the Institutional Animal Care and UseCommittee of the University of Chicago (Chicago, IL), and allexperiments conformed to the relevant regulatory standards.
AntibodiesAnti–PD-L1, anti–ER-TR7, anti-CD8, anti-SMA, anti-CD31,
anti-EGFR, and IgG isotype antibodies were obtained from com-mercial sources (Supplementary Table S1). Anti-rat Her2 anti-body was isolated from culture supernatant from hybridoma7.16.4 (ATCC) at the Frank W. Fitch Monoclonal AntibodyFacility at the University of Chicago (Chicago, IL). Primary anti-bodies diluted in PBS pH 8.0 (Corning) were conjugated to NHS-
DyLight488, 550, 594, 633, or 680 fluorescent dyes (ThermoFisher Scientific) as shown in Supplementary Table S1. Reactionswere incubated overnight at 4�C with gentle agitation. Unreacteddye was removed by dialysis in 10K MWCO Slide-A-Lyzer cas-settes (Thermo Fisher Scientific) against PBS pH 7.4 at 4�C for 3days. Fluorescent antibody solutions were stored at 4�C.
Tumor macrosectioningTUBO tumors were harvested at time points after tail vein
injection of 0.2 mg of DyLight594-conjugated anti–PD-L1 anti-body in 0.1 mL PBS pH 7.4. At 10 minutes after injection of theantibody drug, tumors were washedwith cold PBS, fixedwith 0%,2%, or 4%paraformaldehyde in PBS for 10, 30minutes, or 1 hourat room temperature, and washed with PBS. Then, tumors werecast in 2% agarose gel (dissolved in distilled water, LE QuickDissolve Agarose, GeneMate) in 24-well plates. The gel plugscontaining tumors were marked for orientation and mounted ona vibrating microtome (VT1200S, Leica) equipped with a buffertray. Four-hundredmicron (400mm) thick sectionswere collectedin order in cold PBS.
Immunofluorescence stainingTumor macrosections (400 mm) obtained from tumors treated
with DyLight594-conjugated anti–PD-L1 were fixed in parafor-maldehyde (PFA) at 2% for 10 minutes, 2% for 1 hour or 4% for1 hour, stained with fluorescent anti-Her2 and anti-CD31 for 18hours at 4�C, clarified in D-fructose, and examined by confocalmicroscopy to evaluate staining depth (Supplementary Fig. S4A).While 1 hour of PFA preserved circulating anti–PD-L1 (Supple-mentary Fig. S4B), it preventedDyLight488-conjugated anti-Her2andDyLight633-conjugated anti-CD31penetration (Supplemen-tary Fig. S4C and S4D), making injection of DyLight633-conjugated anti-CD31 necessary to map the microvasculature(Supplementary Fig. S4E). Light fixation failed to preserve circu-lating anti–PD-L1 but allowed anti-Her2 and anti-CD31 tohomogenously stain the macrosections. To obtain complemen-tary spatial information of macromolecular drug transport anddistribution inmacrosections, tumorsweredivided and tissuewastreated with brief or long fixation in parallel.
Thus, for multiplex immunostaining, after 2% PFA fixation for10 minutes, tumor macrosections were stained with antibodycocktails in staining buffer (SB, RPMI1640 with 10 mg/mL BSAand 0.3% Triton X-100). For Supplementary Fig. S4, 50 mLDyLight488-anti-Her2 and 20 mL of DyLight633-anti-CD31were combined in 0.5 mL SB. For Figs. 3 and 4, 70 mLDyLight488-anti-Her2, 20 mL DyLight550-anti-CD8, 20 mL ofDyLight633-anti-CD31, and 80 mL DyLight680-anti-PD-L1 werecombined in 0.5 mL SB. For Fig. 5 and Supplementary Fig. S5, 50mL of DyLight488-anti-SMA, 20 mL of DyLight633-anti-CD31,and 80 mL of DyLight680-anti-ER-TR7 were combined in 0.5 mLSB. Themacrosections were incubatedwith the antibody cocktailsfor 18 hour at 4�C. After incubation, macrosections were washedthree times for 10 minutes in PBS pH 7.4 at 4�C, fixed with 2%paraformaldehyde in PBS for 10 minutes at room temperature,and washed in PBS pH 7.4.
Optical clearing of macrosectionsTo prepare D-fructose solutions for optical clearing, 20%,
50%, and 80% (w/v) solutions of D-fructose were prepared in10 mmol/L phosphate buffer pH 7.8 to a final volume of 10 mL.Thirty microliters of a-thioglycerol (Sigma Aldrich) was added to
Lee et al.
Mol Cancer Ther; 18(1) January 2019 Molecular Cancer Therapeutics214
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

each D-fructose solution. Immunostained macrosections wereincubated sequentially in 10 mL of 20%, 50%, and 80% D-fructose solutions for 1 hour each at 25�C with gentle agitationin 20 mL glass vials. The immunostained macrosections andagarose were then mounted between coverslips in 80% (w/v)D-fructose solutions.
Confocal microscopic imagingImaging was performed using a Leica TCS SP8 confocal
laser scanning microscope, white light laser, Leica HCX PL APO10�/0.4NAdry objective (2.2mmworking distance) or LeicaHCPL APO 40�/1.25 NA oil objective (0.24 mm working distance),and a SuperZ galvometric scanning stage. 3D scanning of macro-sections was performed in a defined X/Y/Z (1.82/1.82/7.5 mm)volumewith 10 frame averaging and bidirectional scanning using488 nm excitation and 496–530 nm emission filter forDyLight488, 550 nm and 563–579 nm filters for DyLight550,594 nm and 603–624 nm filter for DyLight594, 633 nm and648–662 nm filter for DyLight633, and 670 nm excitation and698–721 nm filter for DyLight680.
Comparison of 2D and 3D imagesTo obtain thin sections for conventional analysis, TUBO
tumors were excised at 12 hours after DyLight594-anti-PD-L1antibody injection, and cut in half. One of the tumor halveswas embedded in optimal cutting temperature compound(OCT, Tissue-Tek), frozen at �80�C, and sectioned at 10-mmthickness in a cryostat at �20�C. Sections were transferred tomicroscope slides, dried at room temperature, and imagedby confocal microscopy. The other half of the tumor wasanalyzed using the T3 procedure for 3D imaging of 400-mmmacrosections.
Spatial pharmacokinetics of anti–PD-L1 antibodyFor analysis of antibody transport, 0.2 mg of DyLight594-anti-
PD-L1 antibody in0.1mLPBSpH7.4was injected by tail vein intomice 14 days after TUBO cell implantation and tumors wereharvested at 10minutes, 2, 12 hours, 1, 2, and 4 days. Tenminutesbefore sacrificing the mice, 0.05 mg of DyLight633-anti-CD31antibody in 0.1 mL PBS pH 7.4 was injected by tail vein. Tumorswere fixed in 4% PFA for 1 hour, sectioned, optically cleared, andimaged as described above.
Measuring concentration of anti–PD-L1 antibody in bloodDyLight594-anti-PD-L1 antibody (0.2 mg) in 0.1 mL PBS was
intravenously injected into BALB/c mice (n ¼ 4, average weight:19 g). Blood samples (5 mL) were collected from the dorsal pedalvein at different time points. Blood samples weremixedwith 10%K3-EDTA (0.5 mL) and centrifuged (RCF 4600 � g). The plasma(2 mL)was placed in a 1,536-wellmicroplate (Corning 3891), andthe fluorescent intensity was measured using a plate reader(BioTeck, Synergy Neo2) at Ex 570 nm/Em 625 nm. Using acalibration curve (Supplementary Fig. S3), the data were profiledand fit to a two-compartment pharmacokinetic model for anti–PD-L1 profile (R2 ¼ 0.998). The two-compartment model wasy ¼ A1 e(�x/t1) þ A2 e(�x/t2), where the term y represents thefluorescent intensity of anti–PD-L1 antibody in plasma, 1/t1and 1/t2 are rate constants for the distribution phase and elim-ination phase, A1 and A2 are intercepts on the y-axis for eachexponential segment of the curve. For terminal half-time, t1/2,term¼ 2 Ln[2] / [kþ kptþ ktp� ((kþ kptþ Ktp)2� 4 k ktp)0.5].
For distribution half-time, t1/2, dist ¼ Ln[2] [k þ kpt þ ktp �((k þ kpt þ Ktp)2 � 4 k ktp)0.5]/[2 k ktp], where the terms k, kpt,and ktp represent elimination rate constant, plasma to tissue rateconstant, and tissue to plasma rate constant, respectively (20).
T3 to compare tumor perfusion of anti-Her2 or anti-EGFR andisotype IgG antibodies
DyLight594-anti-Her2 antibody (0.2 mg) and DyLight680-isotype IgG antibody (0.2 mg) in 0.2 mL PBS pH 7.4 wereinjected by tail vein into a BALB-NeuT tumor-bearing mouse.DyLight594-anti-EGFR antibody (0.2 mg) and DyLight680-isotype IgG antibody (0.2 mg) in 0.2 ml PBS pH 7.4 wereinjected by tail vein into a lung cancer PDX tumor-bearing NSGmouse. BALB-NeuT and PDX tumors were harvested at 1 hourafter injection. Ten minutes before sacrificing the mice, 0.05 mgof DyLight633-anti-CD31 antibody in 0.1 mL PBS pH7.4 was injected by tail vein. Tumors were fixed in 4%PFA for 1 hour, sectioned, optically cleared, and imaged asdescribed above.
T3 imaging of dextran and DoxilDextran amine (Invitrogen, MW 40K) was conjugated with a
fluorescent dye. In brief, 5 mg of dextran amine was dissolvedin 0.5 mL of PBS (pH 8.0), and 13 mL of DyLight594-NHS(at 10 mg/mL in dimethylformamide) was added to the dextransolution. The reaction was incubated with gentle agitation atroom temperature for 3 hours. Unreacted dye was removed bydialysis (MWCO10K) against PBSpH7.4 at room temperature for3 days, and the fluorescent dextran solution was stored at 4�C.DyLight594-dextran (1 mg in 0.1 mL PBS) or PEGylatedliposomal doxorubicin (Doxil, 0.2 mg in 0.1 mL) were injectedby tail vein in 4T1 tumor-bearingmice and tumors were harvestedafter 30minutes and 4 hours. Prior to harvesting tumors, 0.05mgDyLight633-anti-CD31 antibody in 0.1 mL PBS was injectedby tail vein and mice were sacrificed after 10 minutes. Excisedtumors were fixed, macrosectioned, cleared, and imaged asdescribed above.
Image processingWe applied the Fiji macros developed in our previous study
(29) for automated 3D reconstruction of whole-tumor images(Supplementary Table S2). In brief, macro LIFtile-restitcheraligned and stitched 3D mosaics for multi-channel "hyperstack"images (0–999 image tiles). To compensate for depth-relatedintensity losses, the mean intensity value (of Otsu-thresholdedareas; maximum gain limited to 3�) of each optical slice inthe macrosection images was normalized to the mean valueof the entire macrosection for each channel using the macroHPRstackConstantMean, facilitating thresholding and segmenta-tion as used in measurement of drug penetration distance fromblood vessel to tumor area. Macro composite big aligner enabledautomated alignment and registration of the stitched macrosec-tion images. To remove gaps between macrosections in the 3Dreconstructed tumor image, the macro closeZvoidsmerged the topand bottom of adjoining macrosections by summing signal fromtwo adjoining optical slices. Next, macro hyprBKGDfix clearedbackground outside the stained tissue to facilitate 3D volumevisualization. Finally, the 3D images were deconvolved usingHuygens Pro software v. 4.3 (Scientific Volume Imaging), tocorrect for refractive index mismatch, and to enhance spatialsignals and cell morphology discrimination. We constructed
Multiplex 3D Mapping of Macromolecular Drug Distribution
www.aacrjournals.org Mol Cancer Ther; 18(1) January 2019 215
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

3D tomographic visualizations of the tumor images using Imarissoftware v. 9.0 (Bitplane).
Data analysisFor hyperstack segmentation of anti–PD-L1 antibody, Her2þ,
and PD-L1þ cells, we visually determined the cut-off threshold forthe antibody drug, Her2, and PD-L1 channel images, and con-verted into binary (8 bit) images. Macro vessel extractor was usedfor automated segmentation of CD31þ, SMAþ, and ER-TR7þ
blood vessels from the CD31, SMA, and ER-TR7 channel images.To measure radius penetration distance of anti–PD-L1 antibodyfrom CD31þ tumor vasculature, we applied the 3D distance mapplugin to the tumor blood vessels. In brief, the ImageJ 3D-EDTplugin calculates the nearest distance of each foreground pixel tobackground in 3D space (31). The vascular space (binarized) istreated as background, so that each pixel in the nonvascular tissueis assigned a (32-bit) value corresponding to its distance to theclosest vessel in 3D space by the plugin. The antibody drug signalis then identified by thresholding and this mask is measured byredirection to the 3D-EDT volume. In this way, the 3D distance ofeach antibody drug voxel is read as the corresponding 3Ddistancefrom the vasculature. All other image analysis was conductedwithbasic analyze functions in Fiji software (http://fiji.sc/Fiji).
Statistical analysisStatistical values are expressed as mean � SD and SEM, and
statistical comparisons between groupsweremade using one-wayANOVA and Student t test. P value of <0.05 was consideredstatistically significant.
ResultsT3 for macromolecular drug distribution in the tumormicroenvironment
Using immune checkpoint blockade immunotherapy (32, 33)as a model for macromolecular drug therapy, we adapted the T3method to enable tracking drug perfusion and penetration intotumors (Fig. 1A–G; Table 1). A rat IgG2bmonoclonal anti-murinePD-L1 antibody (anti-B7/H1, clone 10F.9G2) was conjugated toan amine-reactive N-hydroxysuccinimide (NHS)-ester activatedfluorescent dye, NHS-DyLight594, dialyzed to remove freedye and injected by tail vein. Prior to harvesting tumors,the luminal endothelial surface of the tumor vasculature waslabeled by injecting anti-murine CD31 antibody conjugated toNHS-DyLight633 and, after 10 minutes, animals were sacrificedand their tumors were excised, fixed in 4%PFA for 1 hour and castin agarose. Tumors were cut into 400-mm thick macrosections byvibratome and optically cleared by sequential incubation in 20%,50%, and 80% (w/v) D-fructose, allowing the full volumes to beimaged by confocalmicroscopy. To reconstruct whole tumors, thedigital images of each macrosection were stitched, registered, andannealed using open-source Fiji image processing and analysissoftware. The resulting two-color, 3D maps enabled visualizingand quantifying anti–PD-L1 perfusion and extravasation inwhole tumors.
Thus, to evaluate antibody penetration in each tumor, wevisualized the distribution of DyLight594 fluorescence to trackanti–PD-L1 and compared it with DyLight633, marking theanti-CD31 bound to the perfused tumor vascular endothelium.T3 analysis yielded a 3D tumor model that could be examined byprojections (Fig. 1H–J) or by extracting virtual sections (Fig. 1K
and L), providing 2D representations of the data that facilitateexamination of tumor penetration of anti–PD-L1 antibody inrelation to the CD31þ microvasculature. As shown in Supple-mentary Video S1, scanning through different planes in the 3Dmodel revealed significant heterogeneity at millimeter scalesacross tumors with respect to density and distribution of perfusedvasculature and tissue levels of anti–PD-L1. Compared withimaging in cryosections (Supplementary Fig. S1A), 3D imagesobtained by T3 analysis of macrosections from the divided TUBOtumor (Supplementary Fig. S1B) allowed the correlation betweentissue distribution of injected PD-L1 and the microvascular net-work to be far better appreciated.
Spatial pharmacokinetics of anti–PD-L1 antibody delivery totumors
To probe distribution kinetics, we performed a time-courseexperiment where tumors were excised at 10minutes, 2, 12 hours,1, 2, or 4 days after intravenous injection of DyLight594-anti-PD-L1. Examining the whole macrosections, T3 analysis demon-strated an overall pattern of delivery favoring accumulation andpersistence in the tumor periphery, with antibody concentrationsappearing to peak between 12 hours and 1 day and then decreas-ing close to baseline by 4 days (Fig. 2A; Supplementary Fig. S2).Examining antibody delivery at the 10-minute time point at highmagnification captured marked heterogeneity of anti–PD-L1antibody extravasation at the level of individual microvascularelements (Fig. 2B and C; Supplementary Video S2).
Toward evaluating T3 as a tool for quantitative analysis ofdrug distribution, we first examined the kinetics of circulatinganti–PD-L1 antibody after injection using a calibration curve(Supplementary Fig. S3). Fitting the DyLight594 dye fluorescencein blood samples to a two-compartment pharmacokinetic model(Fig. 2D) yielded a distribution half-life (t1/2, dist) of 46 minutesand a terminal half-life (t1/2, term) of 1 day. Then, 3D tumorpenetrationwas examined bydelineating all CD31þblood vesselsin each macrosection and determining radial penetration of theanti–PD-L1 antibody out from the blood vessel wall and intothe tumor parenchyma via a 3D distance map (Fig. 2E). A meanpenetration of 14 mm fromblood vessel boundaries was observedat 1 day postinjection. Finally, we measured distribution volume(%) of anti–PD-L1 antibody within the macrosections (Fig. 2F),revealing a maximal coverage of 35% at 1 day after injection.A simple interpretation of the data suggests that injectedanti–PD-L1 antibody equilibrates between circulation and tumorby 1 day (34). Once PD-L1 enters the tumor, it dissipates slowlycompared with the circulating fraction, raising the questionwhether these kinetics might reflect anti–PD-L1 binding its target.
Multiplex 3D imaging of anti–PD-L1 distribution in the tumormicroenvironment
To map the delivered anti–PD-L1 with respect to other ele-ments of the tumor microenvironment, we sought to analyze thetumors by T3 and multiplex immunostaining (Fig. 3A–H;Table 2). Examining antibody penetration of macrosections cutfrom tumors subjected to different fixation conditionsindicated light fixation was optimal (Supplementary Fig. S4).Thus, at time points after injecting DyLight594-labeled anti–PD-L1, tumors were harvested and fixed for 10 minutes in 2%PFA, embedded in agar, and macrosectioned. To enable multi-plexed immunodetection, panels of primary antibodies weredirectly labeled by conjugation to different NHS fluorophores at
Lee et al.
Mol Cancer Ther; 18(1) January 2019 Molecular Cancer Therapeutics216
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

i.v. PD-L1i.v. CD31
i.v. PD-L1
i.v. CD31
100 μm
H
500 μm
I J
Z = 100 μm Z = 500 μm
Z = 900 μm Z = 1,300 μm
K L
ZX
Y Y
Z
i.v. injectionA Heavy fixation
Embedding in agarose gel MacrosectioningB C D
Confocal scanning
E F G 3D Image analysis
Tissue clearing
Before After
Y
X
Y
Z
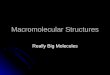
Figure 1.
T3 for tracking tumor perfusion and penetration of macromolecular drug. A–G, Workflow of T3. A, Fluorescent macromolecular drug was intravenously injectedinto tumor-bearing mice. At 10 minutes before sacrificing the mice, fluorescent anti-CD31 antibody was additionally injected for in vivo labeling of vascularendothelium. B and C, The tumors were excised and fixed with 4% PFA solution for 1 hour (B), followed by embedding in 2% agarose gel (C). D, Theembedded tumors were sectioned at 400-mm thickness using a vibratome. E, Collected tumor macrosections were optically cleared by incubating with D-fructosesolutions. F, Each macrosection was imaged by XYZ scanning using a confocal microscope. G, Whole-tumor images were reconstructed by concatenatingmacrosection images, and quantitative 3D spatial analysis of tumor perfusion and penetration of macromolecular drug was performed using Fiji software. H, 3Dvisualization of anti–PD-L1 antibody drug distribution in a whole mouse tumor. 3D rendering of a reconstructed tumor obtained by fusing images of fourmacrosections. TUBO tumors were excised at 2 days after intravenous injection of fluorescent anti–PD-L1 (red) with in vivo labeling of vascular endothelium (cyan)via intravenous injection fluorescent anti-CD31 antibody. Scale bar, 500 mm. Left top insert, tumor prior to macrosectioning. I, Lateral view of reconstructed tumor.J, 3D (left) and 2D (right) channel images for antibody drug and tumor blood vessels. Scale bar, 100 mm. K, Tomographic visualization of the reconstructedtumor imagewithmultipleorthogonal planes (X-Y,X-Z, Y-Zplanes).L,Serial tomographic sectionsofX-Yplanes at different Z-stackdepths (100, 500,900, 1,300mm).
Multiplex 3D Mapping of Macromolecular Drug Distribution
www.aacrjournals.org Mol Cancer Ther; 18(1) January 2019 217
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

Table 1. Tracking tumor perfusion and penetration
Process Average time Notes
Drug injection to mouse tumor model — –Intravenous injection of fluorescent macromolecular drug–Intravenous injection of fluorescent anti-CD31 antibody
Fixing, embedding, and macrosectioning 2 h –Fixing tumor in 4% PFA for 1 hour–Embedding tumor in 2% agarose gel–Macrosectioning at 400-mm thickness
Tissue clearing 3 h –Incubating sequentially for 1 hour each in 20%, 50%, 80% D-fructosesolutions [containing 0.3% (v/v) a-thioglycerol] at 25�C
Confocal imaging 30 min/macrolayer (6 � 5 � 0.4 mm3) –Using 10� objective (X/Y/Z grid resolutions ¼ 1.82/1.82/7.5 mm)–Using 2 different excitation and emission filters–Using 40� objective for high-resolution 3D imaging of interest area
Image processing and analysis 1 day –Using Fiji macros for 3D image reconstruction and analysis
0 10 20 30 40 50 600
5
10
15
20
25
30
35
i.v. P
D-L
1 vo
xel n
umbe
r (%
)
3D Penetration distance (μm) of i.v. PD-L1 from blood vessels into tumor
10 min 2 h 12 h 1 d 2 d
10 min 2 h 12 h 1 d 2 d 4 dA
B
0 1 2 3 4 5 6 7
020406080
100120140160180
i.v. P
D-L
1 co
ncen
tratio
n in
pla
sma
(μg/
mL)
Day
kpt
ktpTP
k
t1/2,dist=46 min
t1/2,term=1 day
i.v. CD31i.v. PD-L1 Merge C
100 μm
i.v. CD31i.v. PD-L1 Merge
30 μmX
YZ
500 μm
D
ZX
Y
Blood vessel
3D penetration distance
E F
i.v. PD-L1i.v. CD31
0 1 2 3 40
10
20
30
40
fo)%(
emulo v
ega rev oC
i.v. P
D-L
1 fo
r mac
rose
ctio
n
Day
ZX
Y
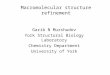
Figure 2.
3D spatial pharmacokinetics of anti–PD-L1 antibody drug in tumors.A, 3D rendering of macrosections of TUBO tumors collected at 10minutes, 2 hours, 12 hours, and1, 2, and 4 days after intravenous injection of fluorescent anti–PD-L1 antibody (red). Tumor blood vessels (cyan) in the macrosections were stained by intravenousinjection of fluorescent anti-CD31 antibody. Scale bar, 500 mm. B, Heterogeneity of anti–PD-L1 antibody drug extravasation through blood vessels in thetumor collected at 10 minutes postinjection. C, 3D vascular penetration of anti–PD-L1 antibody drug. High-resolution 3D images were obtained from the tumorcollected at 10 minutes postinjection. D, Concentration kinetics of anti–PD-L1 antibody in plasma (n ¼ 4, mean � SD). Data were fitted to a two-compartmentmodel (y ¼ A1
e(-x/t1) þA2e(-x/t2)). Insert represents two-compartment model [plasma (P), tissue (T), rate constants (kpt, ktp, k), half-time for distribution and
termination (t1/2, dist and t1/2, term)]. E, 3D tumor penetration distance profiles of anti–PD-L1 antibody away from CD31þ blood vessels at different time pointsafter injection (n ¼ 3 for each time point, merged distance data derived from total intravenous PD-L1 voxels in macrosections). Insert illustrates 3D tumorpenetration distance of antibody drug from blood vessels. F, Distribution kinetics of anti–PD-L1 antibody coverage of macrosection volume at the differenttime points (n ¼ 3 for each time point, mean � SD).
Lee et al.
Mol Cancer Ther; 18(1) January 2019 Molecular Cancer Therapeutics218
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

specific dye:antibody molar ratios (Supplementary Table S1) andcombined in a cocktail. The macrosections were immunostainedto detect cell surface antigen antibodies against PD-L1 to detectthe target, CD31 to identify endothelial cells, Her2 to identifycancer cells, and CD8 to identify cytotoxic T lymphocytes. Then,macrosections were optically cleared with D-fructose and imagedby confocal microscopy. By zooming in on specific regions, T3revealed the distribution kinetics and patterns of anti–PD-L1antibody drug in the tumor microenvironment, distinguishingPD-L1–expressing Her2þ cancer cells and CD8þ T lymphocytes atcellular resolution (Fig. 3I–L). As shown in Supplementary VideoS3, by 10 minutes after injection, a front of concentratedanti–PD-L1 antibody was observed to have reached tumor cellsin proximity to CD31þ blood vessels, apparently sufficient tosaturate binding sites on PD-L1 antigen on cancer cellmembranesand thereby prevent PD-L1 immunostaining (Fig. 3J, intravenousPD-L1/PD-L1 channel images). By 1 day postinjection, anti–PD-L1 antibody had permeated the tumor to reach essentially all PD-L1–expresssing cancer cells (Fig. 3L). We determined targetengagement of the anti–PD-L1 antibody drug by measuringspatial colocalization (%) with PD-L1–expressing Her2þ cancercells in awholemacrosection, revealing that anti–PD-L1 antibodyreached 48% of PD-L1þHer2þ expressing tumor volume at 1 daypostinjection (Fig. 4A).
T3 analysis of anti–PD-L1 distribution in the tumormicroenvironment with different PD-L1 expression patterns
We examined T3 forwhether it can provide sufficient sensitivityto distinguish drug distribution patterns among different tumormicroenvironments. Our previous report described the highexpression of PD-L1 in CD31þ blood vessels in BALB-NeuTtumors (29). However, T3 imaging of tumors formed in BALB/cmice by subcutaneous injection of TUBO cells, a Her2þ cell linederived from a BALB-NeuT tumor, failed to demonstrate a similarpattern (Fig. 3L). Using the multiplex T3 protocol, we comparedthe distributions of DyLight594-labeled anti–PD-L1 in themicro-environment of BALB-NeuT and TUBO tumors 1 day after injec-tion (Fig. 4A and B). High-resolution optical section images ofBALB-NeuT macrosections displayed both the previouslydescribed PD-L1 expression in CD31þ vascular endotheliumand a corresponding accumulation of intravenously injectedanti–PD-L1 antibody in proximity to the PD-L1þCD31þ blood
vessels (Fig. 4C). Comparing the relative distribution (%) ofintravenously injected anti–PD-L1 antibody associated with theHer2þ tumor and CD31þ blood vessels in TUBO and BALB-NeuTmacrosections (Fig. 4D) demonstrated a greater associationof anti–PD-L1 antibody with CD31þ blood vessels in theBALB-NeuT tumor versus a higher level of binding to the Her2þ
tissue in TUBO tumors. The different distributions appear toreflect distinct patterns of PD-L1 expression in the TUBO andBALB-NeuT tumor microenvironments.
T3 analysis of microvascular permeabilityDespite the known diversity of types of microvasculature in
tumors, the vascular barrier to macromolecular drug delivery isoften modeled as a single parameter. Several lines of evidencesuggest considerable heterogeneity in tumor vascular permeabil-ity (35, 36). The T3 multiplex imaging strategy enabled three-dimensional mapping of the full tumor vasculature and quanti-tative analysis of local perfusion and permeability with regards toanti–PD-L1 antibody transport. To investigate microvascular per-meability,we visualized anti–PD-L1antibody drugdistribution at10 minutes after injection by staining tumor macrosections toimage vascular fibroblasts (ER-TR7), smooth muscle cells (SMA),and endothelial cells (CD31; Fig. 5A and B; SupplementaryVideo S4). We then used a computational strategy to classify themicrovasculature based on vascular cell composition and then toexamine the dependence of anti–PD-L1 antibody distribution onvascular composites (Supplementary Fig. S5). The local radialpenetration of anti–PD-L1 antibody from the CD31 endotheliumat 10 minutes postinjection compared with the average value of10 mm(Fig. 2E) was used to evaluate local permeability. "Naked",endothelium-only microvessels that stained for CD31 but lackedER-TR7 or SMA showed greater permeability compared with themicrovessels composed of multiple cell types (Fig. 5C). High-resolution longitudinal optical section images confirmedincreased penetration along CD31-only sections of microvessels,suggesting a disproportionate role in overall anti–PD-L1 transport(Fig. 5D).
T3 to compare tumor penetration of antibody drugsImmobilization and sequestration ofmAb drugs upon binding
to their target antigens on tumor cell membranes is considered tobe a constraint on tumor penetration and, thereby, the effects of
Table 2. Mapping drug distribution in tumor microenvironment
Process Average time Notes
Drug injection to mouse tumor model — –Intravenous injection of fluorescent macromolecular drug
Fixing, embedding, and macrosectioning 1 h –Fixing tumor in 2% PFA for 10 min–Embedding tumor in 2% agarose gel–Macrosectioning at 400-mm thickness–Fixing macrosections in 2% PFA for 5 min
Immunofluorescence staining 18 h –Incubating with 4 different fluorescent primary antibodies at 4�C
Washing and fixing 40 min –Washing with PBS 3 times, and fixing in 2% PFA for 10 min
Tissue clearing 3 h –Incubating sequentially for 1 h each in 20%, 50%, 80% D-fructosesolutions [containing 0.3% (v/v) a-thioglycerol] at 25�C
Confocal imaging 1 h/macrolayer (6 � 5 � 0.4 mm3) –Using 10� objective (X/Y/Z grid resolutions ¼ 1.82/1.82/7.5 mm)–Using 5 different excitation and emission filters–Using 40� objective for high-resolution 3D imaging of interest area
Image processing and analysis 1 day –Using Fiji software and created macros for 3D image reconstructionand analysis
Multiplex 3D Mapping of Macromolecular Drug Distribution
www.aacrjournals.org Mol Cancer Ther; 18(1) January 2019 219
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

i.v. injectionA Light fixation
Embedding in agarose gel MacrosectioningB C D
Multiplex immunostaining
Confocal scanning
F G H 3D Image analysis
Tissue clearing
E
Before After
Y
X
Her2CD8i.v. PD-L1CD31PD-L1
Her2 CD8
i.v. PD-L1 CD31
PD-L1
30 μmXZ
Y
i.v. PD-L1PD-L1
50 μm
I J10 min
Her2CD8i.v. PD-L1CD31PD-L1
K L
30 μm
Her2 CD8
i.v. PD-L1 CD31
PD-L1 i.v. PD-L1PD-L1
1 day
Y
Z
ZY 50 μm
Figure 3.
T3 formappingdrugdistribution in tumormicroenvironment.A–H,Workflowof T3.A,Fluorescentmacromolecular drugwas intravenously injected into tumor-bearingmice. B–D, The tumors were excised, fixed with 2% PFA solution for 10 minutes (B), embedded in 2% agarose gel (C), and sectioned at 400-mm thicknessusing a vibratome (D).E, Themacrosectionswere stainedwith fluorescent primary antibodies. F,Afterwashing andfixing, themacrosectionswere optically cleared byincubating with D-fructose solutions. G, Complete immunostaining for each macrosection was determined by optical cross-section (Z) scanning using a confocalmicroscope, and then each macrosection was imaged by XYZ scanning with multi-excitation and emission filters. H, 3D macrosection images were reconstructed,and macromolecular drug distribution in the tumor microenvironment was quantitatively analyzed using Fiji software. I–L, Spatial mapping of anti–PD-L1antibody distribution kinetics in the tumor microenvironment. High-resolution 3D images show distribution patterns of anti–PD-L1 antibody (red) in TUBO tumorsat 10 minutes (I and J) and 1 day postinjection (K and L). The tumors were lightly fixed, sectioned, and immunostained for Her2þ cancer cells (green), CD8þ Tlymphocytes (yellow), CD31þ blood vessels (cyan), and PD-L1þ cells (magenta). I andK, 3D rendering of anti–PD-L1 distribution in the tumor microenvironment. Scalebar, 30mm.Rightbottom inserts, 2Doptical section images. Scalebar, 50mm. JandL,3D (left) and2D (right) channel images foreachcellularmarker andantibodydrug.
Lee et al.
Mol Cancer Ther; 18(1) January 2019 Molecular Cancer Therapeutics220
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

TUBOHer2CD8i.v. PD-L1CD31PD-L1
ZX
Y
Her2 CD8 i.v. PD-L1
CD31 PD-L1 i.v. PD-L1PD-L1
500 μm
Her2CD8i.v. PD-L1CD31PD-L1
Her2 CD8 i.v. PD-L1
CD31 PD-L1 i.v. PD-L1PD-L1
ZX
Y500 μm
BALB-NeuT
A
B
C DHer2 CD8 i.v. PD-L1
CD31 PD-L1 i.v. PD-L1PD-L1
50 μm
0
10
20
30
40
50
60
70
i.v. P
D-L
1 di
strib
utio
n (%
) TUBO BALB-NeuT
Her2+ tumor CD31+ blood vessels
*
*
Figure 4.
T3 analysis of anti–PD-L1 antibody distribution in tumor microenvironment with different PD-L1 expression patterns. A and B, 3D rendering of tumorperfusion of anti–PD-L1 antibody (red). At 1 day after fluorescent anti–PD-L1 antibody injection to TUBO (A) and BALB-NeuT (B) tumor mouse models,the tumors were excised, lightly fixed, sectioned, and immunostained for Her2 (green), CD8 (yellow), CD31 (cyan), and PD-L1 (magenta). Scale bar, 500 mm.C, 2D optical section images of BALB-NeuT tumor show PD-L1 expression in CD31þ vascular endothelium and colocalization of intravenous anti–PD-L1 withPD-L1þCD31þ microvessels. Scale bar, 50 mm. D, Relative quantification of microvessel anti–PD-L1 distribution (%) into Her2þ tumor and CD31þ vascularendothelium in the TUBO and BALB-NeuT tumor macrosections (n ¼ 3, mean � SEM). � , P < 0.01.
Multiplex 3D Mapping of Macromolecular Drug Distribution
www.aacrjournals.org Mol Cancer Ther; 18(1) January 2019 221
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

therapeutic agents. Toward measuring this effect by T3, we com-pared the relative tumor perfusion of fluorescently labeled anti-bodies targeting tumor cell surface antigens and their isotypecontrols labeled with a different fluorophore. Thus, we modeled
antibody therapy targeting the oncogenes Her2 and EGFR, whichare recognized by the clinical agentsHerceptin (trastuzumab) andErbitux (cetuximab). To observe impact of antibody binding ondelivery, we examined the relative penetration of the IgG2a anti-
0
20
40
60
80
+++
+–+
++–
Blo
od v
esse
l cou
nt (%
)
3D Distance of i.v. PD-L1 from CD31+ blood vessels
<10 μm >10 μm
CD31SMA
ER-TR7
+––
*
**
A B
DC
100 μm
SMA i.v. PD-L1
CD31 ER-TR7
SMA i.v. PD-L1 CD31 ER-TR7 Merge
50 μm
SMAi.v. PD-L1
CD31ER-TR7
ZX
Y
Figure 5.
Vascular permeability to anti–PD-L1 antibody drug transport. A, 3D rendering of tumor perfusion of anti–PD-L1 antibody (red) through tumor microvesselsimmunostained for SMAþ smooth muscle cells, CD31þ endothelium, and ER-TR7þ fibroblasts. Tumors were harvested at 10 minutes after fluorescent anti–PD-L1antibody injection, lightly fixed, sectioned, and immunostained. Scale bar, 100 mm. B, 3D single channel images for each vascular cell marker and antibody drug.C, Relative quantification of permeability of different types of microvessels with regards to anti–PD-L1 transport to tumor (n ¼ 6, total blood vessels inthree random 3D volume images in two macrosections, mean � SEM). Mean 3D tumor penetration distance (10 mm) of anti–PD-L1 antibody at 10 minutesafter injection was used as a guideline to determine high and low permeability of microvessels composed of different vascular cells. �, P < 0.05; �� , P < 0.001.D, 2Doptical section images show representative high and lowpermeability of CD31þ-only and SMAþCD31þER-TR7þmicrovessels, respectively,with regards to anti–PD-L1 antibody transport to tumors. Scale bar, 50 mm.
Mol Cancer Ther; 18(1) January 2019 Molecular Cancer Therapeutics222
Lee et al.
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

BALB-NeuT
Lung cancer PDX
i.v. Her2i.v. IgGi.v. CD31
i.v. EGFR/i.v. IgG/i.v. CD31
i.v. Her2 i.v. IgG i.v. CD31
i.v. EGFR
i.v. IgG
i.v. CD31
ZX
Y
ZX
Y
ZX
Y
ZX
Y
1 mm
30 μm
1 mm 30 μm
A
B
0 100 200 300 4000
2
4
6
Ant
ibod
y vo
xel n
umbe
r (%
)
3D Penetration distance (μm)from blood vessels into tumor
i.v. EGFRi.v. IgG
0 50 100 1500
2
4
6
8
10
12
Ant
ibod
y vo
xel n
umbe
r (%
)
3D Penetration distance (μm)from blood vessels into tumor
i.v. Her2i.v. IgG
C
Lung cancer PDX
BALB-NeuT
Figure 6.
T3 analysis of tumor penetration of anti-Her2 or anti-EGFR and isotype IgG antibodies. Tumors collected 1 hour after intravenous coinjection of fluorescentlylabeled specific and isotype control antibodies and 10 minutes after intravenous injection of fluorescent anti-CD31 antibody. A, 3D rendering of macrosectionof BALB-NeuT tumor indicating distribution of anti-Her2 (green), IgG isotype (red), and blood vessels (cyan). Low magnification 3D image (top, scale bar, 1 mm)demonstrates antibodies spreading through stroma with less delivery to tumor nests. High magnification 3D image (bottom, scale bar, 30 mm) of a singletumor nest suggests anti-Her2 antibody remains proximal to vasculature, while isotype control displays complete penetration. B, 3D rendering of macrosectionof lung cancer PDX tumor indicating distribution of anti-EGFR (green), IgG isotype (red), and blood vessels (cyan). High magnification view (right) similarlydisplays limited penetration of anti-EGFR antibody compared with isotype control. C, 3D tumor penetration distance profiles of anti-Her2 and IgG antibodiesin BALB-NeuT tumor (top) and anti-EGFR and IgG antibodies in lung cancer PDX tumor (bottom) determined as radial distance from CD31þ blood vessels at1 hour after injection. Merged distance data are derived from total antibody voxels detected in the 3D images of tumor nests represented inA (bottom) andB (right).
Multiplex 3D Mapping of Macromolecular Drug Distribution
www.aacrjournals.org Mol Cancer Ther; 18(1) January 2019 223
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

rat Her2 clone 7.16.4 versus IgG2a isotype control (DyLight594-anti-Her2/DyLight680-isotype IgG) into Her2þ mammarytumors formed in BALB-NeuT mice. Then, we compared pene-tration of an IgG2a anti-human EGFR clone 528 with IgG2aisotype control (DyLight594-anti-EGFR/DyLight680-isotypeIgG) into an EGFRþ non–small cell lung cancer PDX tumorformed in anNSGmouse.We injected amixture of thefluorescentantibodies intravenously and used T3 imaging to examine thedistribution of specific and control antibodies inmacrosections at1 hour (Fig. 6A and B). With CD31þ microvasculature visualiza-tion, examining antibody distribution at high magnificationcaptured deeper penetration of isotype IgG antibody into tumornests compared with the anti-Her2 or anti-EGFR antibodies(Fig. 6A bottom and B right; Supplementary Videos S5 andS6). Using 3D distance mapping, the spatial tumor penetrationof each antibody was determined by delineating all CD31þ bloodvessels in the BALB-NeuT or lung cancer PDX tumor nest (shownin Fig. 6A bottom andB right) and determining radial penetrationof the antibodies out from the blood vessel wall and into thetumor parenchyma (Fig. 6C). Themean penetrations of anti-Her2and isotype IgG antibodies in the BALB-NeuT tumor nest were 38and 63 mm from CD31þ blood vessel boundaries at 1 hour afterinjection. The mean penetrations of anti-EGFR and isotype anti-bodies in lung cancer PDX tumor nest were 45 and 114 mm at1 hour after injection. The distribution volumes (%) of anti-Her2and isotype IgG antibodies within the BALB-NeuT macrosectionwere 27% and 29%. The distribution volumes (%) of anti-EGFRand isotype IgG antibodies within the lung cancer PDX macro-section were 17% and 27%. These data support prior studies oftherapeutic antibodies showing penetration into tumor paren-chyma being limited by binding to target proteins on tumormembranes, potentially leaving watershed areas untreated.
T3 imaging of polymers and nanoparticles distribution in thetumor microenvironment
Toward establishing T3 as a general tool to visualize distribu-tion ofmacromolecular drugs in tumors, we examined delivery ofa fluorescent polymer and a model nanoparticle. Dextran hasbeen broadly used to develop polymer–drug conjugates andnanodrug formulations (37, 38), and PEGylated liposomal doxo-rubicin (Doxil) is an FDA-approved nanoformulation for treatingpatients with advanced solid tumors, including metastatic breastcancer (39, 40). With T3, we mapped 3D tumor distributions offluorescent dextran and Doxil with CD31þ blood vessels at 30minutes (dextran) and 4 hours (Doxil) after injection in 4T1tumor-bearing mice (Supplementary Fig. S6 and SupplementaryVideo S7; Doxil). T3 images revealed that dextran was efficientlydelivered from microvessels to tumor parenchyma, while thefluorescence ofDNA-bounddoxorubicinwas limited to thenucleiof perivascular cells.
DiscussionRecent advances in biology (41), immunology (42), and
chemistry (43) have enabled dramatic progress in the develop-ment of biologics and other macromolecular drugs as targetedcancer therapeutics. Similar progress has been made in nanome-dicines. However, without sufficient tools to track macromolec-ular drug distribution, it remains a challenge to overcome trans-port barriers, sequestration mechanisms and other interactionswith the tumor microenvironment that may limit efficacy (44).
For example, nanoscale drug formulations have been designedand developed on the basis of their potential to leverage the EPReffect (9, 45). However, translation has lagged as it has becomeapparent that the EPR effect is negligible in many human tumors.Even in mice, the EPR effect is typically only sufficient to deliver atiny fraction of circulating nanoparticles to tumors (10, 46). Inturn, although mAbs may extravasate more efficiently, theirbinding to target antigens and resulting sequestration makecharacterization of spatial distribution challenging (47).Methodssuch as spectroscopic imaging in tissue or microscopy in thinsections (48–50) are well-established as tools to track drugdelivery, but a technology gap has remained, which has criticallylimited analysis of drug distribution in the heterogeneous tumormicroenvironment.
Recent progress in tissue optical clearing and light microscopyhave led to significant advances in 3D immunofluorescenceimaging of tissues. In particular, CLARITY (51) and related meth-ods (52) have provided powerful tools to establish connectivity inthe central nervous system. Applications for cancer are emerging(53–55), but initial studies have revealed challenges, includingrendering the tumor tissue sufficiently transparent while main-taining structural integrity and protein immunogenicity, obtain-ing satisfactory penetration of antibodies and conjugates, andperforming multiplexed detection with high sensitivity and spec-ificity at cellular resolution (56).
To overcome these challenges and advance technologies avail-able for pharmacokinetic/pharmacodynamic studies, we haveadapted the T3 platform (29) to enable multiplex 3D imaging ofmacromolecular drugs in mouse tumor tissues and performcomputational analysis of spatial distribution, interaction withtarget cells, andvascularpenetrationusingopen-source Fijimacros(57). Using in vivo CD31 vasculature labeling and heavy fixationafter excising tumors soon after intravenous injection, it waspossible to capture the macromolecular drugs still circulating inthe blood stream and track their initial extravasation from bloodvessels into tumor parenchyma. Lighter fixation facilitated tissuestaining with fluorescent primary antibodies, allowing detectionofmultiple antigens alongwith tracking drug binding to its target.
Thereby, we used T3 to map the distribution of anti–PD-L1antibody in whole mouse tumors and analyze the spatial phar-macokinetics of anti–PD-L1 antibody bydetermining 3Dvascularpenetration distance at different time points postinjection. Poten-tial limitations of applying the T3 method for spatial pharmaco-kinetics are that it depends on harvesting tumor tissues at a seriesof time points and concentration is measured by relative fluores-cent intensity. However, T3 data can be readily linked to plasmadrug concentration profiling and in vivo imaging to enhance boththe quantitative and temporal resolution, which along with cell-level spatial distribution mapping, would provide a route to trulycomprehensive analysis of drug delivery.
Because T3 is a multiplex method, it enables not only drugtracking but also analysis of features in the tumor and microen-vironment that may influence delivery. Thus, T3 allowed cell-resolution analysis of the efficiencyof targetingmembrane-boundPD-L1 by anti–PD-L1 antibody. In turn, T3 also enabled analysisof the distribution pattern of anti–PD-L1 antibody with respect totumor-scale heterogeneity of PD-L1 expression. Studying micro-vascular permeability, we found that CD31þ capillaries wereleakier with regards to anti–PD-L1 antibody transport thanmicro-vessels surrounded by SMAþ smooth muscle cells and ER-TR7þ
fibroblasts. Furthermore, T3 made it straightforward to track the
Lee et al.
Mol Cancer Ther; 18(1) January 2019 Molecular Cancer Therapeutics224
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

relative perfusion of two antibodies in a tumor, with T3 analysisconfirming that coinjected nonspecific IgG extravasates deeperinto tumor parenchyma than targeted antibodies. T3 revealed theextent to which anti-Her2 and anti-EGFR antibodies were seques-tered by binding to their target antigens at the periphery of tumornests. The T3 strategy was also validated by tracking dextran todemonstrate transport through the interstitial space and to dem-onstrate intracellular delivery of doxorubicin to tumor cells byDoxil, demonstrating potential for broad applications for mac-romolecular drugs.
We report T3 as a new tool for 3D spatial imaging and quan-titative analysis of macromolecular drug transport to tumors. Byassessingmultiple spatial parameters simultaneously, T3 providesa unique 3D window into macromolecular drug distribution inthe tumor microenvironment. Although demonstrated here as atool to examine delivery of macromolecular drugs, T3 might alsobe adapted to tracking small-molecule agents in the tumormicro-environment using covalent immobilization and detection withantidrug antibodies (58). Toward determining the absolute localconcentration of a drug in the tumor microenvironment, we arepursuing further development of methods to improve fluores-cence detection and calibration that will enable direct measure-ment of drug levels by fluorescence intensity. Combinedwith T3'smultiplexing capabilities, this would enable determination ofdrug concentration–therapeutic effect relationships in pharma-cokinetic/pharmacodynamic analysis at cellular resolution. Toaddress another limitation of T3, we intend to automate samplestaining, image acquisition and image processing, and implementmachine learning strategies to enhance pattern recognition duringdata analysis, thus decreasing hands-on effort and speeding upsample-to-answer time while increasing the information gainedfrom each sample. Thereby, we anticipate that T3 can be applied
broadly to facilitate the development of new cancer drugs andstrategies for targeted drug delivery to tumors.
Disclosure of Potential Conflicts of InterestThe authors are founders of Transnostics LLC to commercialize T3.
Authors' ContributionsConception and design: S.S.-Y. Lee, S.J. KronDevelopment of methodology: S.S.-Y. Lee, V.P. BindokasAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): S.S.-Y. Lee, V.P. BindokasAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): S.S.-Y. Lee, V.P. BindokasWriting, review, and/or revision of the manuscript: S.S.-Y. Lee, V.P. Bindokas,S.J. KronStudy supervision: S.J. Kron
AcknowledgmentsThis study was supported by NCI R01s CA164492 and CA199663 and a
Cancer Research Institute CLIP Grant to S.J. Kron and by National Institute ofBiomedical Imaging and Bioengineering (NIBIB) K99 EB022636 and Susan G.Komen Postdoctoral Fellowship PDF15333618 (made possible through fund-ing from American Airlines) to S.S.-Y. Lee. Imaging, image processing, and dataanalysis were performed at the University of Chicago Integrated Light Micros-copy Facility directed by V.P. Bindokas, supported by the NCI P30 CA014599.TUBO cells were generously provided by the Emerling Lab at Sanford BurnhamPrebys Medical Discovery Institute.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received May 23, 2018; revised August 30, 2018; accepted October 10, 2018;published first October 15, 2018.
References1. Chen H, Zhang W, Zhu G, Xie J, Chen X. Rethinking cancer nanother-
anostics. Nat Rev Mater 2017;2:17024.2. Carter PJ, Lazar GA. Next generation antibody drugs: pursuit of the
'high-hanging fruit'. Nat Rev Drug Discov 2017;17:197–223.3. SernaN, S�anchez-García L, Unzueta U,Díaz R, V�azquez E,Mangues R, et al.
Protein-based therapeutic killing for cancer therapies. Trends Biotechnol2017;36:318–35.
4. Jiang W, von Roemeling CA, Chen Y, Qie Y, Liu X, Chen J, et al. Designingnanomedicine for immuno-oncology. Nat Biomed Eng 2017;1:0029.
5. Thurber GM, Weissleder R. A systems approach for tumor pharmacoki-netics. PLoS One 2011;6:e24696.
6. Matsumura Y,MaedaH. Anew concept formacromolecular therapeutics incancer chemotherapy: mechanism of tumoritropic accumulation of pro-teins and the antitumor agent smancs. Cancer Res 1986;46:6387–92.
7. Maeda H, Nakamura H, Fang J. The EPR effect for macromolecular drugdelivery to solid tumors: improvement of tumor uptake, lowering ofsystemic toxicity, and distinct tumor imaging in vivo. Adv Drug Deliv Rev2013;65:71–9.
8. Nakamura H, Jun F, Maeda H. Development of next-generation macro-molecular drugs based on the EPR effect: challenges and pitfalls. ExpertOpin Drug Deliv 2015;12:53–64.
9. Shi J, Kantoff PW, Wooster R, Farokhzad OC. Cancer nanomedicine:progress, challenges and opportunities. Nat Rev Cancer 2016;17:20–37.
10. Wilhelm S, Tavares AJ, Dai Q, Ohta S, Audet J, Dvorak HF, et al. Analysis ofnanoparticle delivery to tumours. Nat Rev Mater 2016;1:16014.
11. Nakamura Y, Mochida A, Choyke PL, Kobayashi H. Nanodrug delivery: isthe enhanced permeability and retention effect sufficient for curing cancer?Bioconjugate Chem 2016;27:2225–38.
12. Park K. Facing the truth about nanotechnology in drug delivery. ACS Nano2013;7:7442–7.
13. Dewhirst MW, Secomb TW. Transport of drugs from blood vessels totumour tissue. Nat Rev Cancer 2017;17:738–50.
14. SunQ,Ojha T, Kiessling F, Lammers T, Shi Y. Enhancing tumor penetrationof nanomedicines. Biomacromolecules 2017;18:1449–59.
15. Zhang B, Hu Y, Pang Z. Modulating the tumor microenvironment toenhance tumor nanomedicine delivery. Front Pharmacol 2017;8:952.
16. Wang Y, Kohane DS. External triggering and triggered targeting strategiesfor drug delivery. Nat Rev Mater 2017;2:17020.
17. Weissleder R, Schwaiger MC, Gambhir SS, Hricak H. Imagingapproaches to optimize molecular therapies. Sci Transl Med 2016;8:355ps16–ps16.
18. Beckmann N, Kaltashov IA, Windhorst AD. Editorial: in vivo imaging inpharmacological research. Front Pharmacol 2017;7:511.
19. Miller MA, Weissleder R. Imaging the pharmacology of nanomaterials byintravital microscopy: toward understanding their biological behavior.Adv Drug Deliv Rev 2017;113:61–86.
20. Lee SS, Li J, Tai JN, Ratliff TL, Park K, Cheng JX. Avasimibe encapsulated inhuman serum albumin blocks cholesterol esterification for selective cancertreatment. ACS Nano 2015;9:2420–32.
21. BlomS, Paavolainen L, BychkovD, Turkki R,M€aki-Teeri P,HemmesA, et al.Systems pathology by multiplexed immunohistochemistry and whole-slide digital image analysis. Sci Rep 2017;7:15580.
22. Remark R, Merghoub T, Grabe N, Litjens G, Damotte D, Wolchok JD, et al.In-depth tissue profiling using multiplexed immunohistochemical conse-cutive staining on single slide. Sci Immunol 2016;1:aaf6925.
23. Wang CW, Budiman Gosno E, Li YS. Fully automatic and robust 3Dregistration of serial-section microscopic images. Sci Rep 2015;5:15051.
24. Feuchtinger A, Walch A, Dobosz M. Deep tissue imaging: a review from apreclinical cancer research perspective. Histochem Cell Biol 2016;146:781–806.
Multiplex 3D Mapping of Macromolecular Drug Distribution
www.aacrjournals.org Mol Cancer Ther; 18(1) January 2019 225
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

25. Lagerweij T, Dusoswa SA, Negrean A, Hendrikx EML, de Vries HE, Kole J,et al. Optical clearing and fluorescence deep-tissue imaging for 3D quan-titative analysis of the brain tumor microenvironment. Angiogenesis2017;20:533–46.
26. Dobosz M, Ntziachristos V, Scheuer W, Strobel S. Multispectral fluores-cence ultramicroscopy: three-dimensional visualization and automaticquantification of tumor morphology, drug penetration, and antiangio-genic treatment response. Neoplasia 2014;16:1–13.
27. Sindhwani S, Syed AM, Wilhelm S, Glancy DR, Chen YY, Dobosz M, et al.Three-dimensional optical mapping of nanoparticle distribution in intacttissues. ACS Nano 2016;10:5468–78.
28. Sindhwani S, Syed AM,Wilhelm S, ChanWCW. Exploring passive clearingfor 3D optical imaging of nanoparticles in intact tissues. Bioconjug Chem2017;28:253–9.
29. Lee SS, Bindokas VP, Kron SJ. Multiplex three-dimensional optical map-ping of tumor immune microenvironment. Sci Rep 2017;7:17031.
30. Boggio K, Nicoletti G, Di Carlo E, Cavallo F, Landuzzi L, Melani C, et al.Interleukin 12–mediated prevention of spontaneousmammary adenocar-cinomas in two lines of Her-2/neu transgenic mice. J Exp Med 1998;188:589–96.
31. Borgefors G. On digital distance transforms in three dimensions. ComputVis Image Underst 1996;64:368–76.
32. Pardoll DM. The blockade of immune checkpoints in cancer immuno-therapy. Nat Rev Cancer 2012;12:252–64.
33. Ribas A, Wolchok JD. Cancer immunotherapy using checkpoint blockade.Science 2018;359:1350–5.
34. Shargel L, Yu ABC. Applied biopharmaceutics and pharmacokinetics. NewYork: McGraw-Hill; 1999.
35. Ekdawi SN, Stewart JMP, Dunne M, Stapleton S, Mitsakakis N, Dou YN,et al. Spatial and temporal mapping of heterogeneity in liposome uptakeand microvascular distribution in an orthotopic tumor xenograft model.J Control Release 2015;207:101–11.
36. Mittapalli RK,AdkinsCE, BohnKA,MohammadAS, Lockman JA, LockmanPR. Quantitative fluorescence microscopy measures vascular pore size inprimary and metastatic brain tumors. Cancer Res 2017;77:238–46.
37. Varshosaz J. Dextran conjugates in drug delivery. Expert Opin Drug Deliv2012;9:509–23.
38. Foerster F, Bamberger D, Schupp J, Weilb€acher M, Kaps L, Strobl S, et al.Dextran-based therapeutic nanoparticles for hepatic drug delivery. Nano-medicine 2016;11:2663–77.
39. Szebeni J, F€ul€op T, D�ezsi L, Metselaar B, Storm G. Liposomal doxorubicin:the good, the bad and the not-so-ugly. J Drug Target 2016;24:765–7.
40. Rivankar S. An overview of doxorubicin formulations in cancer therapy.J Cancer Res Ther 2014;10:853–8.
41. WangM, Zuris JA, Meng F, Rees H, Sun S, Deng P, et al. Efficient delivery ofgenome-editing proteins using bioreducible lipid nanoparticles. Proc NatlAcad Sci U S A 2016;113:2868–73.
42. Cuesta-Mateos C, Alcaraz-Serna A, Somovilla-Crespo B, Mu~noz-Calleja C.Monoclonal antibody therapies for hematological malignancies: not justlineage-specific targets. Front Immunol 2018;8:1936.
43. Kobayashi H, Turkbey B, Watanabe R, Choyke PL. Cancer drug delivery:considerations in the rational design of nanosized bioconjugates. Biocon-jugate Chem 2014;25:2093–100.
44. Rosenblum D, Joshi N, Tao W, Karp JM, Dan P. Progress and challengestowards targeted delivery of cancer therapeutics. Nat Commun 2018;9:1410.
45. Aftab S, Shah A, Nadhman A, Kurbanoglu S, Aysl Ozkan S, Dionysiou DD,et al. Nanomedicine: an effective tool in cancer therapy. Int J Pharm2018;540:132–49.
46. Hansen AE, Petersen AL, Henriksen JR, Boerresen B, Rasmussen P, ElemaDR, et al. Positron emission tomography based elucidation of theenhanced permeability and retention effect in dogs with cancer usingcopper-64 liposomes. ACS Nano 2015;9:6985–95.
47. Thurber GM, Schmidt MM, Wittrup KD. Factors determining antibodydistribution in tumors. Trends Pharmacol Sci 2008;29:57–61.
48. Schluep T, Hwang J, Hildebrandt IJ, Czernin J, Choi CHJ, Alabi CA, et al.Pharmacokinetics and tumor dynamics of the nanoparticle IT-101 fromPET imaging and tumor histologicalmeasurements. ProcNatl Acad Sci U S A2009;106:11394–9.
49. Hoppin J, Orcutt KD, Hesterman JY, Silva MD, Cheng D, Lackas C, et al.Assessing antibody pharmacokinetics in mice with in vivo imaging.J Pharmacol Exp Ther 2011;337:350–8.
50. Lee CM, Tannock IF. The distribution of the therapeutic monoclonalantibodies cetuximab and trastuzumab within solid tumors. BMC Cancer2010;10:255.
51. Chung K, Wallace J, Kim SY, Kalyanasundaram S, Andalman AS, DavidsonTJ, et al. Structural andmolecular interrogationof intact biological systems.Nature 2013;497:332–7.
52. Tainaka K, Kuno A, Kubota SI, Murakami T, Ueda HR. Chemical principlesin tissue clearing and staining protocols for whole-body cell profiling.Annu Rev Cell Dev Biol 2016;32:713–41.
53. Tanaka N, Kanatani S, Tomer R, Sahlgren C, Kronqvist P, KaczynskaD, et al. Whole-tissue biopsy phenotyping of three-dimensionaltumours reveals patterns of cancer heterogeneity. Nat Biomed Eng2017;1:796–806.
54. Cuccarese MF, Dubach JM, Pfirschke C, Engblom C, Garris C, Miller MA,et al. Heterogeneity ofmacrophage infiltration and therapeutic response inlung carcinoma revealed by 3D organ imaging. Nat Commun 2017;8:14293.
55. Lloyd-Lewis B, Davis FM,Harris OB, Hitchcock JR, Lourenco FC, PascheM,et al. Imaging the mammary gland and mammary tumours in 3D: opticaltissue clearing and immunofluorescence methods. Breast Cancer Res2016;18:127.
56. Richardson DS, Lichtman JW. Clarifying tissue clearing. Cell 2015;162:246–57.
57. Schindelin J, Arganda-Carreras I, Frise E, Kaynig V, Longair M, Pietzsch T,et al. Fiji: an open-source platform for biological-image analysis. NatMethods 2012;9:676–82.
58. Lawson ADG. Antibody-enabled small-molecule drug discovery. Nat RevDrug Discov 2012;11:519–25.
Mol Cancer Ther; 18(1) January 2019 Molecular Cancer Therapeutics226
Lee et al.
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554

2019;18:213-226. Published OnlineFirst October 15, 2018.Mol Cancer Ther Steve Seung-Young Lee, Vytautas P. Bindokas and Stephen J. Kron Distribution in the Tumor MicroenvironmentMultiplex Three-Dimensional Mapping of Macromolecular Drug
Updated version
10.1158/1535-7163.MCT-18-0554doi:
Access the most recent version of this article at:
Material
Supplementary
http://mct.aacrjournals.org/content/suppl/2018/10/13/1535-7163.MCT-18-0554.DC1
Access the most recent supplemental material at:
Cited articles
http://mct.aacrjournals.org/content/18/1/213.full#ref-list-1
This article cites 57 articles, 9 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/18/1/213To request permission to re-use all or part of this article, use this link
on August 9, 2021. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst October 15, 2018; DOI: 10.1158/1535-7163.MCT-18-0554