Embed Size (px)
Citation preview
MULTIPLE PRIMARY CARCINOMAS 1
FRANK ROBERT HANLON, M.D.
Fellow in Surgery, The Mayo Foundation, Rochester, Minnesota
Two or more primary carcinomas rarely occur in the sameperson. I have recently reviewed the literature on the subject andplace on record forty-nine additional cases. This paper is dividedinto three sections: (1) a partial record of my survey of the literature; (2) an analysis of eighteen cases of multiple primary carcinomas occurring in 3000 consecutive post-mortem examinations atThe Mayo Clinic; (3) an analysis of thirty-one cases in which aclinical diagnosis was made at The Mayo Clinic.
REVIEW OF THE LITERATURE
Billroth (2) reported a case in 1869 of a patient with carcinomaof the stomach and also one of the external ear. He emphasizedthe importance of the criteria used as a basis for diagnosis, andestablished three postulates which he felt were necessary for thediagnosis of multiple primary tumors: (1) each tumor must havean independent histologic appearance; (2) the tumors must arisein different situations; (3) each tumor must produce its ownmetastasis. Mercanton (9) added a fourth requirement, that therebe no recurrence of tumors after their removal.
It is quite as unreasonable to demand the fulfillment of thethird and fourth postulates in the diagnosis of multiple primarycarcinomas as it would be in the diagnosis of a single carcinoma.Egli (3), Harbitz (8) and Puhr (12) objected strenuously to theadoption of Billroth's criteria.
Goetze (6) suggested the following requirements for diagnosis:(1) the macroscopic lLnd microscopic appearance of the tumorsmust be that of the usual carcinomas of the organs involved;(2) exclusion of metastasis must be certain; (3) diagnosis may beconfirmed by the character of the metastasis in each case.
1 Abstract of thesis submitted to the Faculty of the Graduate School of the University of Minnesota in partial fulfillment of the requirements for the degree of Masterof Science in Surgery, June 1929. Work done in the Section on Pathologic Anatomy,The Mayo Clinic.
2001

2002 FRANK ROBERT HANLON
The Linacre Lecture of 1927 contained a particularly noteworthy passage. Murray (10), in commenting on the excellentstudy of Puhr on multiple primary carcinomas, made the followingstatement: " A certain interest attaches to the fact that in none ofPuhr's five cases of multiple malignancies did the combinationcarcinoma mammae and carcinoma uteri occur.... As cancer ofthese two sites make up nearly half the total female cancer mortality, it is hardly possible such a combination could be consistently
FIG. 1. ADENOCARCINOMA OF THE CECUM, CASE 6, TABLE I. X 120
overlooked, and its absence from the casuistic literature is probablysignificant." I was able to review ten cases in the literature inwhich this combination occurred.
In only seven instances, so far as I have been able to determine,has a large series of post-mortem examinations been studied forthe purpose of determining the frequency of multiple primarycarcinomas. These studies have been made, respectively, byv. Hansemann (7), Redlich (13), Feilchenfeld (4), Riechelmann(14), Harbitz (8), Puhr (12), and Gade (5).
Excluding the cases of multiple primary carcinomas of the

MULTIPLE PRIMARY CARCINOMAS 2003
skin, I have found reports of sixteen cases of multiple primarycarcinoma of the same organ or of paired organs, of twenty-fourcases of multiple primary carcinoma involving three or moreorgans, and of 125 other cases of two primary carcinomas in thesame patient.2
Concerning carcinomas of the skin, Owen (11), in a review of3000 cases of malignant tumors, found 143 (4.7 per cent) of multipleprimary growths. In these 143 cases, 113 of the growths involved
FIG. 2. CARCINOMA OF THE KIDNEY, CASE 6, TABLE 1. X 120
the skin only. There were 86 cases of basal-cell carcinoma; theaverage age of the patient in the group was sixty-six years, andthe duration of the disease, eight years. In 20 of the 113 cases,a squamous-cell and a basal-cell tumor existed in the same patient.The average age of the patients in this group was sixty-five years.Seven of the 113 cases were examples of multiple squamous-cellcarcinoma. In 1915, Barber (1) reported a series of 200 casesof multiple basal-cell carcinoma.
2 References to these reports, in full, and other references on which this paper isfounded, can be found in the library of the University of Minnesota, accompanyingthe following thesis: Hanlon, F. R.: Multiple Primary Carcinomas.

2004 FRANK ROBERT HANLON
Many of the 16 cases of multiple primary carcinoma of thesame organ or of paired organs that have been referred to, mightbe subject to debate as to accuracy of diagnosis. Theilhaber andEdelberg (16) have reviewed cases of carcinoma of the same organor of paired organs, and, in addition to the 16 cases mentioned,
.FIG. 3. CARCINOMA OF THE OVARY, CASE 10, TABLE I. X 120
they have listed cases reported by Klebs, Ribbert, Handford,Rotter, and Tanberg.
Concerning the cases of multiple primary carcinoma involvingthree or more organs, the average age of the patients, in cases inwhich the age was reported, was sixty-three and six-tenths years.This age is greater than that in the cases in which two multipleprimary carcinomas existed. The majority of the tumors weresituated in the gastro-intestinal tract.
Of the 125 other cases of two primary carcinomas in the samepatient, the average age of the patients in the 81 cases in whichthe age was reported, was fifty-eight and eight-tenths years. Thisage is several years greater than the average age in the cases inwhich there was only one carcinoma.

MULTIPLE PRIMARY CARCINOMAS 2005
The distribution among the various organR corresponded closelywith the percentage distribution of carcinoma when it occurssingly. This factor alone would lead to the belief that multipleprimary malignant growths are coincidental rather than a responseto a definite law of formation of tumors.
FIG. 4. CARCINOMA OF THE THYROID GLAND, CASE 10, TABLE 1. X 120
MULTIPLE PRIMARY CARCINOMAS DISCLOSED IN 3000 CONSECUTIVE
POST-MORTEM EXAMINATIONS MADE AT THE MAYO CLINIC
In this entire group, 950 deaths were attributable to malignanttumors, of which 710 were carcinomas.
The high incidence of tumors (31.7 per cent) in this series is aconsequence of the unusually large number of patients afflicted withmalignant disease who present themselves at the clinic for examination. In a similar survey in a fairly large metropolitan center,malignant tumors were responsible for only 9 per cent of the'deaths.
In establishing the diagnosis of multiple primary carcinoma,the greatest reliance has been placed on distinct variation in the

TA
BL
EI
Dat
aC
once
rnin
gE
ight
een
Cas
esin
Whi
chN
ecro
psy
was
Per
form
ed
Sex
IF
irst
tum
or
Cas
eI
and
age.
II
year
sS
itu
atio
nH
isto
'og
icap
pea
ran
ceS
itu
ati
on
-I-1
51
MS
tom
ach
Ade
noca
rcin
oma
Par
ath
yro
idgl
and
21
57
MS
tom
ach
Ade
noca
rcin
oma,
sign
et-r
ing
cell
sC
olon
,sp
leni
cfl
exur
e
372
MS
igm
oid
Ade
noca
rcin
oma
Rig
ht
kidn
ey4
56M
Rec
tum
Ade
noca
rcin
oma
Rig
ht
kid
ney
56
0M
Mo
uth
(lip
)S
quam
ous-
cell
carc
inom
aR
ectu
m1-
:>
I6·
60
MC
ecum
Ade
noca
rcin
oma
Rig
ht
kidn
ey0
76
5M
Lef
tki
dney
Ade
noca
rcin
oma;
larg
ece
lls,
clea
rR
ight
.k
idn
ey0 0
>cy
topl
asm
877
MP
rost
ate
glan
dA
deno
carc
inom
aA
nal
mar
gin
941
MR
ectu
mA
deno
carc
inom
aR
igh
tk
idn
eylO
t6
5F
Rig
ht
ov
ary
Pap
illa
ryca
rcin
oma
Th
yro
idgl
and
11+
57
FL
eft
ov
ary
Pap
illa
rycy
stad
enoc
arci
nom
aC
ervi
xof
ute
rus
125
9F
Lef
tbr
east
Sci
rrho
usca
rcin
oma
Th
yro
idgl
and
1370
MT
hy
roid
glan
dA
deno
carc
inom
aR
igh
tk
idn
ey14
11
ML
ary
nx
Squ
amou
s-ce
llca
rcin
oma
Ileu
m15
63
MC
olon
Ade
noca
rcin
oma
Th
yro
idgl
and
166
8F
Rec
tum
Ade
noca
rcin
oma
Kid
ney
1763
MN
ose
IAde
noca
rcin
oma
Rig
ht
kid
ney
1861
MS
tom
ach
Ade
noca
rcin
oma
Rec
tum
*F
igur
es1
and
2.tF
igur
es3
and
4.:::
Rep
ort
edb
yS
usse
xan
dC
aylo
r(1
5).
Sec
ond
tum
or
His
tolo
gic
app
eara
nce
Lar
gepa
lece
lls
wit
hsh
arpl
you
tlin
edbo
rder
sA
deno
carc
inom
a,ir
regu
lar
hype
rchr
omat
iccy
lind
ric
cell
sH
ighl
yce
llul
artu
bu
lar
carc
inom
aH
emor
rhag
ican
dcy
stic
carc
inom
aA
deno
carc
inom
aC
uboi
dal-
cell
carc
inom
aA
deno
carc
inom
a;ce
llgr
owth
less
acti
veth
anth
atin
left
side
Bas
al-c
ell
carc
inom
aT
ub
ula
rca
rcin
oma
Ade
noca
rcin
oma
Squ
amou
s-ce
llca
rcin
oma
Hig
hly
cell
ular
aden
ocar
cino
mas
Pap
illa
ryad
enoc
arci
nom
aS
mal
lro
und-
cell
aden
ocar
cino
ma
Ade
noca
rcin
oma
Tu
bu
lar
carc
inom
aS
mal
l-ce
llad
enoc
arci
nom
aA
deno
carc
inom
a,de
gene
rati
onof
ap
oly
p

MULTIPLE PRIMARY CARCINOMAS 2007
microscopic appearance of the several tumors in each case. Eachtumor was considered in its possible relationship to a metastaticlesion, and an effort was made to rule out the possibility of metastasis. An extensive lapse of time between the appearance of thetumors and the absence of known metastatic lesions, associatedwith varying histologic appearances, was highly favorable towardthe diagnosis of the duality of the tumors. If one of the tumorsoccurred in an organ which was a common site of metastasis, thattumor was scrutinized most carefully with these criteria in mind, andif an element of doubt remained, it was excluded from the study.
Perhaps the most difficult cases to evaluate are the multiplecarcinomas of the gastro-intestinal tract. It is a well known factthat metastasis from intestinal tumors takes place in the liver, theregional lymph nodes, or the operative scars. The occurrence ofa second tumor at a distant point in the intestine is possibly asecond primary growth. The frequency of intestinal polyps undergoing malignant degeneration offers strong support for this theory.However, in the cases appended it has been required that thetumors possess different microscopic appearances before they beadjudged independent primary growths.
In the 710 cases of carcinoma, there were 18 cases of multipleprimary malignant growths. This represents 0.6 per cent of theentire group of cases studied and 2.5 per cent of the cases ofcarcinoma. Thirteen patients were males; the remaining 5 werefemales.
The average age of the patients in whom there were twomultiple primary carcinomas was sixty-two and six-tenths years.The average age of the group with one carcinoma was fifty-fiveand two-tenths years. The fact that these dual tumors occurredamong patients older than those who had a single tumor alreadyhas received emphasis. The organs involved were as follows:colon, 9; kidney, 9; thyroid gland, 4; stomach, 3; ovary, 2; parathyroid, 1; mouth, 1; prostate gland, 1; anal margin, 1; uterus, 1;breast, 1; larynx, 1; ileum, 1; nose, 1.
It will be noted that there is widespread distribution of theorgans involved. The high incidence of tumors of the colon is dueto the fact that operation on the colon carries with it a rather highmortality, especially because many of the cases necessitate immediate operation for intestinal obstruction. A large number thuscome to necropsy. Most of the tumors of kidneys were small,
t.::> §
TA
BL
EII
Dat
aC
once
rnin
gT
hirt
y-on
eC
ases
inw
hich
Gro
wth
sW
ere
Rec
ogni
zed
Cli
nica
lly
IA
geF
irst
tum
or
IS
econ
dtu
mo
rw
hen
Cas
eS
exre
cog-
niz
ed,
Sit
uat
ion
His
tolo
gic
app
eara
nce
Age
whe
nre
cog-
IS
itu
atio
nH
isto
logi
cap
pea
ran
ceye
ars
niz
ed.
year
s----
IM
52S
igm
oid
Ade
noca
rcin
oma
No
tre
cord
edP
enis
Squ
amou
s-ce
llca
rcin
oma
2F
Rig
ht
bre
ast
Ade
noca
rcin
oma
No
tre
cord
edC
ervi
xof
ute
rus
Squ
amou
s-ce
llca
rcin
oma
3F
Ute
rus
Ade
noca
rcin
oma
No
tre
cord
edR
igh
tb
reas
tA
deno
carc
inom
a;m
ark
edce
llul
arac
tiv
ity
and
gro
wth
4F
Rec
tum
Ade
noca
rcin
oma
No
tre
cord
edU
teru
sA
deno
carc
inom
a5
M44
Fac
eM
ixed
squa
mou
s-ce
llan
dba
sal-
No
tre
cord
edS
igm
oid
Ade
noca
rcin
oma
cell
carc
inom
a6
F6
4S
tom
ach
Ade
noca
rcin
oma
68O
var
yA
deno
carc
inom
a;no
rese
mbl
ance
toga
stri
cca
rcin
oma
7F
55U
teru
sA
deno
carc
inom
a6
6R
igh
tb
reas
tA
deno
carc
inom
a8
F49
Ute
rus
Ade
noca
rcin
oma
56R
igh
tb
reas
tA
deno
carc
inom
a9
M57
Sto
mac
hA
deno
carc
inom
a57
Ski
nbe
low
rig
ht
Squ
amou
s-ce
llca
rcin
oma
ear
IAde
noca
rcin
oma
10F
48R
ectu
mA
deno
carc
inom
a50
Lef
tb
reas
t11
M48
Cec
umA
deno
carc
inom
a56
Spl
enic
flex
ure
Ade
noca
rcin
oma;
mor
eac
tive
than
firs
ttu
mo
r12
M26
Rig
ht
kidn
eyA
deno
carc
inom
a35
Lu
ng
Ade
noca
rcin
oma
13M
61E
soph
agus
Squ
amou
s-ce
llca
rcin
oma
62L
eft
han
dS
quam
ous-
cell
carc
ino
ma
14M
43C
ecum
Ade
noca
rcin
oma
45T
ran
sver
seco
lon
Ad
en
ocarc
ino
ma,
cell
sm
uch
smal
ler
and
gro
wth
mor
era
pid
15F
47L
eft
orb
itC
om
bin
edsq
uam
ous-
cell
and
56L
eft
bre
ast
Ade
noca
rcin
oma
basa
l-ce
llca
rcin
om
a
t-:l §
TA
BL
EII
-Co
nti
nu
ed
Ag
eF
irst
tum
orS
econ
dtu
mor
wh
enC
ase
Sex
reco
g·
In
ized
,S
itu
atio
nH
isto
logi
cap
pea
ran
ceA
ge
wh
enre
cog-
Sit
uat
ion
His
tolo
gic
app
eara
nce
year
sn
ized
,ye
ars
----
16M
68U
pp
erp
art
ofle
ftS
quam
ous-
cell
carc
inom
a70
Uri
nar
yb
lad
der
Squ
amou
s-ce
llca
rcin
oma
chee
k17
M74
Ute
rus
Ade
noca
rcin
oma
75R
igh
tsh
ould
erS
quam
ous-
cell
carc
inom
a18
F56
Ute
rus
Ade
noca
rcin
oma
58L
eft
bre
ast
Ade
noca
rcin
oma
19F
56L
eft
bre
ast
Ade
noca
rcin
oma
57B
lad
der
Pap
illa
rysq
uam
ous-
cell
carc
inom
a20
M57
Sig
moi
dA
deno
carc
inom
a57
Pen
isS
quam
ous-
cell
carc
ino
ma
21:\1
48C
hee
kA
deno
carc
inom
a;hi
ghly
mal
ig-
49T
esti
sA
deno
carc
inom
a;la
rge
poly
hedr
aln
ant
hy
per
chro
mat
icce
lls
22F
64S
kin
ofri
gh
tea
rM
ixed
basa
l-ce
llan
dsq
uam
ou
s-64
Cer
vix
ofu
teru
sS
quam
ous-
cell
carc
inom
ace
llca
rcin
oma
23F
81L
eft
bre
ast
Ade
noca
rcin
oma
81U
pp
erli
pB
asal
-cel
lca
rcin
oma
24F
50L
eft
bre
ast
Ade
noca
rcin
oma
50S
kin
ofne
ckM
ixed
basa
l-ce
llan
dsq
uam
ous-
cell
carc
inom
a25
1\1
78L
ipS
quam
ous-
eell
carc
inom
a80
Sto
mac
hA
deno
carc
inom
a26
F29
Rig
ht
ov
idu
ctP
apil
lary
carc
inom
a29
Rec
tum
Ade
noca
rcin
oma
27F
64L
eft
bre
ast
Ade
noca
rcin
oma
Ute
rus
Ade
noca
rcin
oma
28F
53S
tom
ach
Ade
noca
rcin
oma
54U
teru
sA
deno
carc
inom
a29
:M48
Bla
dd
erP
apil
lary
squa
mou
s-ce
llca
rci-
50B
ron
chu
sP
apil
lary
carc
inom
an
om
a30
1\1
53T
on
gu
eS
quam
ous-
cell
carc
inom
a53
Uri
nar
yb
lad
der
Squ
amou
s-ce
llca
rcin
oma
311\
163
Bla
dd
erS
quam
ous-
cell
carc
inom
a64
Lip
~quamous-cell
carc
inom
a

2010 FRANK ROBERT HANLON
went unrecognized clinically, but possessed microscopic stigmataof malignancy. Most of them were growing slowly and representeda low degree of malignancy. However, they possessed definitepotentialities for growth, and their inclusion in this study iswarranted. The carcinomas selected do not represent the benigntumors known as adenomas. These occur either as single ormultiple neoplasms on the cortex of the kidney. They are mostfrequently found in the sclerotic type of kidney. They areclassified according to their cellular arrangement as papillary,alveolar, or tubular adenomas. They are distinguished from thecarcinomas of the kidney by the completely differentiated cells, thecircumscribed limitation of the tumor, and the definite arrangement of the cells in an orderly fashion. The carcinomas, on theother hand, represent an unrestrained growth of cells, lacking indifferentiation, and infiltrating the renal substance freely.
Of the 18 cases of multiple primary malignant growths, in 2the growths were recognized clinically as multiple, primary, andmalignant; in 2 others the diagnosis was made at necropsy only,and in the other 14 cases one tumor was recognized clinically,whereas the second was first noted at necropsy.
Twenty-one tumors gave rise to definite symptoms. Fifteenwere entirely quiescent.
The patients dated their symptoms back an average of tenmonths, with extremes varying between three years and two weeks.
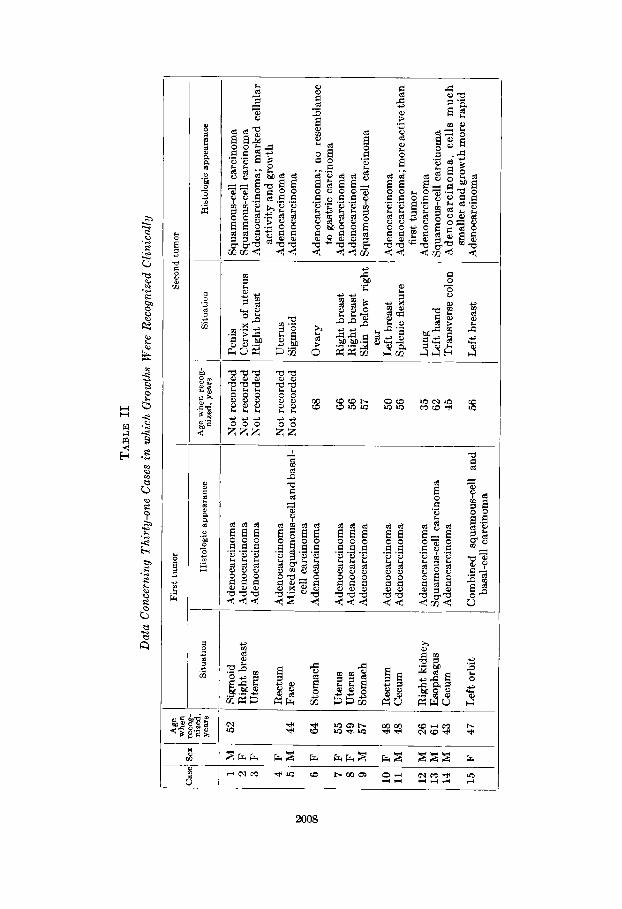
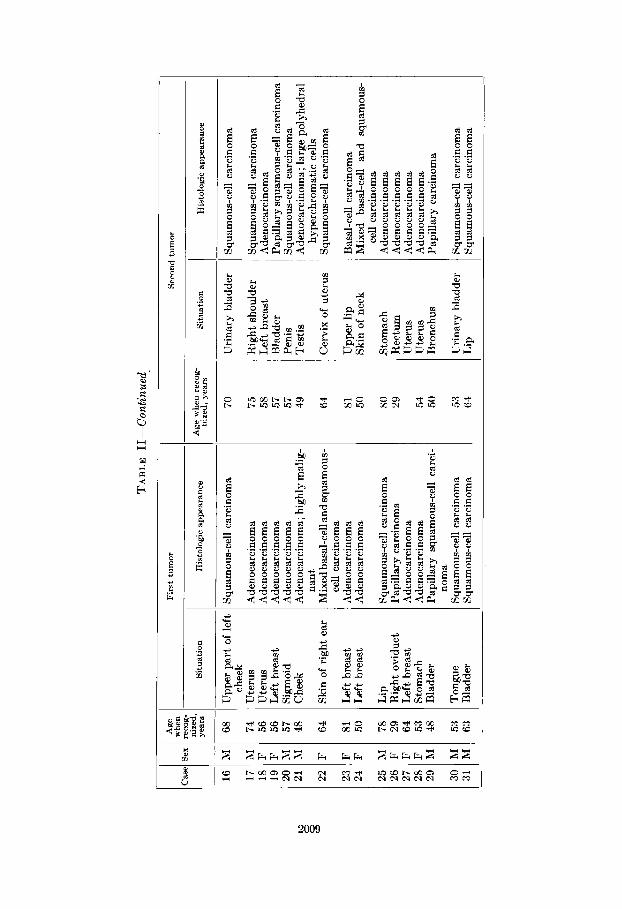
Tables I and II contain data on the 18 cases in which necropsywas performed and on the 31 cases in which the growths wererecognized clinically.
Fourteen of the patients whose cases are recorded in Table IIwere males; the remaining 17 were females. The average age atthe time when the first tumor was removed was fifty-four years,and the average age at the time when the second tumor was removed was fifty-seven and eight-tenths years. Since some of thepatients are still living, it is impossible to determine the averagespan of life of those 31 patients, but it is definitely more than sixtyyears. The distribution among the various organs of the primaryand secondary tumors, taken together, was as follows: breast, 11;colon and rectum, 10; uterus, 10; skin, 9; urinary bladder, 5;stomach, 4; lip and tongue, 4; lung and bronchus, 2; penis, 2;kidney, 1; esophagus, 1; testis, 1; fallopian tube, 1; ovary, 1.
MULTIPLE PRIMARY CARCINOMAS 2011
SUMMARY AND CONCLUSIONS
Multiple primary carcinomas probably represent incidentaloccurrences rather than a definite response to any law of neoplasticformation.
The distribution of the several tumors throughout the bodyfollows closely the frequency of occurrence of single carcinomas.
Conclusions cannot be drawn concerning the sex incidenceassociated with multiple primary tumors. There is, however, avery definite relationship between the occurrence of multipleprimary carcinomas and senescence. They occur among personswho are several years older than those who harbor but one carcinoma. This was pointed out previously by Egli, who consideredboth benign and malignant tumors. The present study confirmshis views in regard to carcinomas.
This paper adds to the literature 49 new cases of multipleprimary tumors; 18 cases were observed in a study of 3,000consecutive post-mortem examinations; the remaining 31 casesoccurred in a large group in which two tumors were removed byoperative intervention.
BIBLIOGRAPHY
1. BARBER, R. F.: Basal-celled epithelioma, Med. Rec. 87: 753-754,1915.
2. BILLROTH: Quoted by Miller, R. T., Jr.: Multiple primary malignantfoci in cancer of the colon, Ann. Surg. 80: 456-472, 1924.
3. EGLI, FRITZ: Ueber Multiplizitat von Geschwiilsten, Cor.-Bl. f.schweiz. Aerzte. 44: 449-462, 1914.
4. FEILCHENFELD: Quoted by Theilhaber and Edelberg.5. GADE: Quoted by Siebke, Harald: Uber multiple Carcinome, Ztschr.
f. Krebsforsch. 23: 66-81, 1926.6. GOETZE, OTTO: Bemerkungen iiber Multiplizitat primarer Carcinome
in Anlehnung an einen Fall von dreifachem Carcinom, Ztschr. f.Krebsforsch. 13: 281-302, 1913.
7. v. HANSEMANN: Das gleichzeitige Vorkommen verschiedenartigerGeschwiilste bei derselben Person, Ztschr. f. Krebsforsch. 1:183-198, 1904.
8. HARBITZ, FRANCIS: Uber das gleichzeitige Auftreten mehrererselbstandig wachsender (" multipler") Geschwiilste, Beitr. Z. path.Anat. U. Z. aUg. Path. 62: 503-579, 1916.
9. MERCANTON, F.: Quoted by Miller, R. T., Jr.: Multiple primarymalignant foci in cancer of the colon, Ann. Burg. 80: 456-472, 1924.
10. MURRAY, J. A.: Linacre Lecture on multiple new growths, Lancet.2: 800-803, 1927.
95

2012 FRANK ROBERT HANLON
11. OWEN, L. J.: Multiple malignant neoplasms, J. A. M. A. 76: 13291333, 1921.
12. PUHR, LUDWIG: tJber die Multiplizitat der Geschwiilste, Ztschr. f.Krebsforsch. 24: 38-62, 1926-1927.
13. REDLICH, WALTER: Die Sektions-Statistik des Carcinoms am BerlinerStadtischen Krankenhaus am Urban nebst kasuistischen Beitragen, Ztschr. f. Krebsforsch. 5: 261-325, 1907.
14. RIECHELMANN: Quoted by G6tting: Zur multiplizitiit primarerCarcinome, Ztschr. f. Krebsforsch. 7: 675-681, 1909.
15. SUSSEX, L. T., AND CAYLOR, H. D.: Epithelioma of the cervixassociated with carcinomatous cystadenoma of the ovary, Ann.Surg. 76: 949-952, 1927.
16. THEILHABER, A., AND EDELDERG, H.: Zur Lehre von der Multiplizitat der Tumoren, insbesondere der Carcinome, DeutscheZtschr. f. Chir. 117: 457-489,1912.





























