Embed Size (px)
DESCRIPTION
a partial fulfillment ... i hope this helps
Citation preview
LICEO DE CAGAYAN UNIVERSITY
COLLEGE OF NURSING
NCM104
In Partial Requirements of the course NCM104
SURGICAL WARD
Related Learning Experience
A CASE STUDY ON
Multiple physical injuries secondary to vehicular
accident
Submitted To:
Ma’am Glenda Demafeliz RN, MN
Clinical Instructor
Submitted by:
Xyrex D. Nicolas
BSN-NCM104
FEB 26, 2013
TABLE OF CONTENTS
PAGES
I. INTRODUCTION
A. OVERVIEW OF THE STUDY 2
B. SCOPE AND LIMITATIONS OF THE STUDY 3
C. OBJECTIVE OF THE STUDY 4
II. PROFILE OF THE PATIENT 5
III.DEVELOPMENTAL THEORY 6
IV. HEALTH HISTORY
a.Personal Health History 8
b.History of Present Illness 8
V. MEDICAL MANAGEMENT
a. Medical Orders with Rationale 9
b. Laboratory Results 14
c. Drug Study 16
VI. ANATOMY AND PHYSIOLOGY 22
VII. PATHOPHYSIOLOGY 27
VIII. NURSING ASSESSMENT
a. Nursing System Review Chart 28
IX. NURSING MANAGEMENT
b. Ideal Nursing Management 29
c. Actual Nursing Management 34
1
X. EVALUATION AND IMPLICATION 37
XI. REFERRALS AND RECOMMENDATION(HEALTH TEACHINGS) 38
38
XII. PROGNOSIS 40
XIII.BIBLIOGRAPHY 41
I. INTRODUCTION
a. Overview of the Study
Motorcycles are becoming more popular as a means of transportation.
However, per vehicle-mile traveled, a motorcyclist is 37 times more likely to die in a
crash and 9 times more likely to be injured (NHTSA, 2008f). As the motorcycle
itselfoffers almost no protection, the occupant is subject to severe forces similar to
those experienced by an ejected automobile or truck occupant. Head injury is
common, especially in the absence of a helmet. There may be multiple fractures and
large, painful abrasions with imbedded debris (road rash).Before looking at injury
patterns, it is helpful to review some of the physics involved. Newton’s First Law of
Motion states that an object in motion will remain in motion until acted on by another
force. Thus, a vehicle in motion will keep moving until something—a tree, another
vehicle, the brakes, or some other force—causes it to slow down, stop, or change
direction. When such a force is applied, people in the vehicle will continue to move at
the original speed and direction until a force such as the seat belt, the steering wheel,
or the windshield causes them to slow down, stop, or change direction. Even then, the
organs of the body will continue in motion until slowed or stopped by the bones and
other supporting structures within the body.
The forces on the vehicle, the body, and the organs are applied in sequence.
This sequence is rapid if the vehicle strikes a fixed object and much less so during a
controlled stop. If this sequence were to be observed in slow motion, the body and the
2
organs would seem to move toward the point of impact. This is important because it
provides clues as to where to look for injury.
Remember that it is not only the change in speed that causes the damage but how fast
the change occurs. Going from 60 mph to a full stop may do no damage if it happens
over a few seconds. But if the change occurs over a few milliseconds, a much greater
force is involved, and it can be deadly. Anything that increases the stopping time will
decrease the forces involved. This is the reason for such safety features as crush zones
in the vehicle’s front end, a collapsible steering column, and the stretch in seat belts.
b. Scope and Limitation of the Study
This study includes the collection of information specifically to the patient’s health
condition primarily to multiple physical injuries secondary to vehicular accident. The
study also includes the assessment of the physiological-emotional status, adequacy of
support systems, and care given by the family as well as other health care providers.
The scope of this study includes:
Data collected via assessment, interviews with the patient and the Wife.
Actual and Ideal problems and its appropriate nursing interventions that would be
applied throughout his stay in the hospital.
Developing a plan of care that will reduce identified predicaments and
complications
Coordinating and delegating interventions within the plan of care to assist patient
Mr. RED to reach maximum functional health.
Further evaluating the effectiveness of nursing interventions that have been
applied to patient Mr. RED entire course of therapy.
The study is limited by the following factors:
3
The nursing interventions done to patient Mr. RED are only limited to our
assessment for 2 consecutive dates: January 30, 2013 @4:00p.m (assessment – 1st
visit) and February 6,2013 (2nd visit). Information gathered was limited only to the client
himself, and to his wife. The X – ray result is also not available on the chart. There were
also limitations on the interventions we were only permitted to perform, the time and
distance allotted for our visit only. No interviews were made with the previous
physicians attending to our patient.
c. Objective of the study
At the end of 4 day-care to the patient, I will be able to do the following:
1. Assess and monitor the health status and vital signs of my patients.
2. Identify actual and potential health problems of the patient.
3. Plan for the patient’s care
4. Perform nursing interventions (medications included) effectively and
efficiently
5. Evaluate patient’s response and reaction and
6. Impart health teachings to our patient
4
II. PATIENT’S PROFILE
Name: RED
Gender: Male
Age: 37 years old
Birthdate: January 6, 1976
Place of Birth: BUKIDNON
Address: Manolo fortich,bukidnin,
Status: Married
Religion: Roman Catholic
Nationality: Filipino
Height: 5Ft. & 5inches Tall
Weight (present): 65 kg
Educational Attainment: High School Graduate
Occupation: CAA
Income: 3000/month
Chief Complaints: tenderness of face
Admitting Diagnosis: Multiple injuries secondary to vehicular accident.
Admission Date: January 29, 2013
Admission Time: 07:30p.m.
Attending Physician: DRA. Cynthia M. Woo
Hospital: CAMP EVANGELISTA STATION HOSPITAL
1
5
III.DEVELOPMENTAL THEORY
1Erik Erikson Psychosocial Theory
Later Adulthood: 20-45 years old
Ego Development Outcome: intimacy vs. isolation
Basic Strengths: LOVE
This stage takes place during young adulthood between the ages of
approximately 19 and 40. During this period of time, the major conflict centers on
forming intimate, loving relationships with other people.
While psychosocial theory is often presented as a series of neatly defined,
sequential steps, it is important to remember that each stage contributes to the next. For
example, Erikson believed that having a fully formed sense of self (established during
the identity versus confusion stage) is essential to being able to form intimate
relationships. Studies have demonstrated that those with a poor sense of self tend to
have less committed relationships and are more likely to suffer emotional isolation,
loneliness, and depression.
Erikson believed it was vital that people develop close, committed relationships with
other people. Success leads to strong relationships, while failure results in loneliness
and isolation
Robert Havighurst Theory of Developmental Task
Middle Adult (Ages 30-60)
Assisting teenage children to become responsible and happy adults. * Achieving adult
social and civic responsibility. * Reaching and maintaining satisfactory performance in
one’s occupational career. * Developing adult leisure time activities. * Relating oneself
to one’s spouse as a person. * To accept and adjust to the physiological changes of
middle age. * Adjusting to aging parent
6
IV. HEALTH HISTORY
a. History of Present Illness
Sustained injury secondary to Vehicular Accident(motorcycle passenger)
last January 13, 2013, brought to Adela Ty Memorial Hospital, where skull x-ray was
done. Brought to CESH for further evaluation and management.
b. Past Medical History
Client has no known medical history and this is the first time that he was being
hospitalized. He has previous illnesses such as fever, cough and colds but only
managed at home and no consultation was done and no medication were taken.
7
V. MEDICAL MANAGEMENT
a. Medical Orders with Rationale
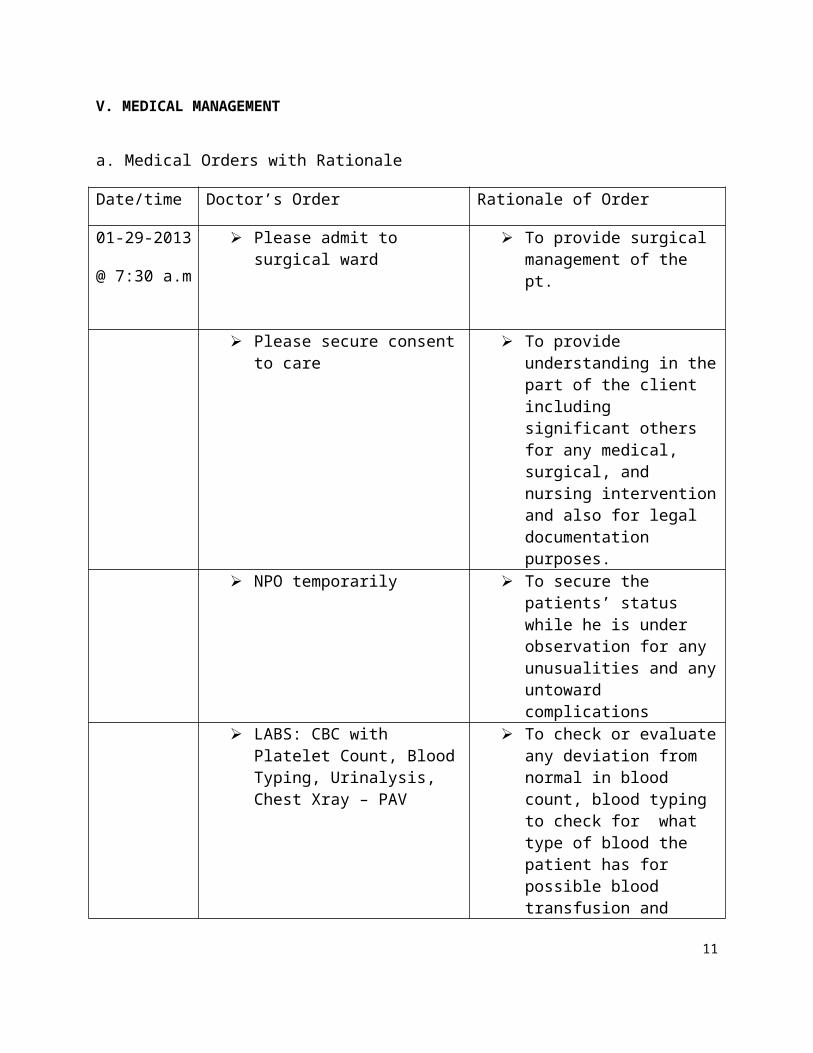
Date/time Doctor’s Order Rationale of Order
01-29-2013
@ 7:30 a.m
Please admit to surgical ward To provide surgical management of the pt.
Please secure consent to care
To provide understanding in the part of the client including significant others for any medical, surgical, and nursing intervention and also for legal documentation purposes.
NPO temporarily To secure the patients’ status while he is under observation for any unusualities and any untoward complications
LABS: CBC with Platelet Count, Blood Typing, Urinalysis, Chest Xray – PAV
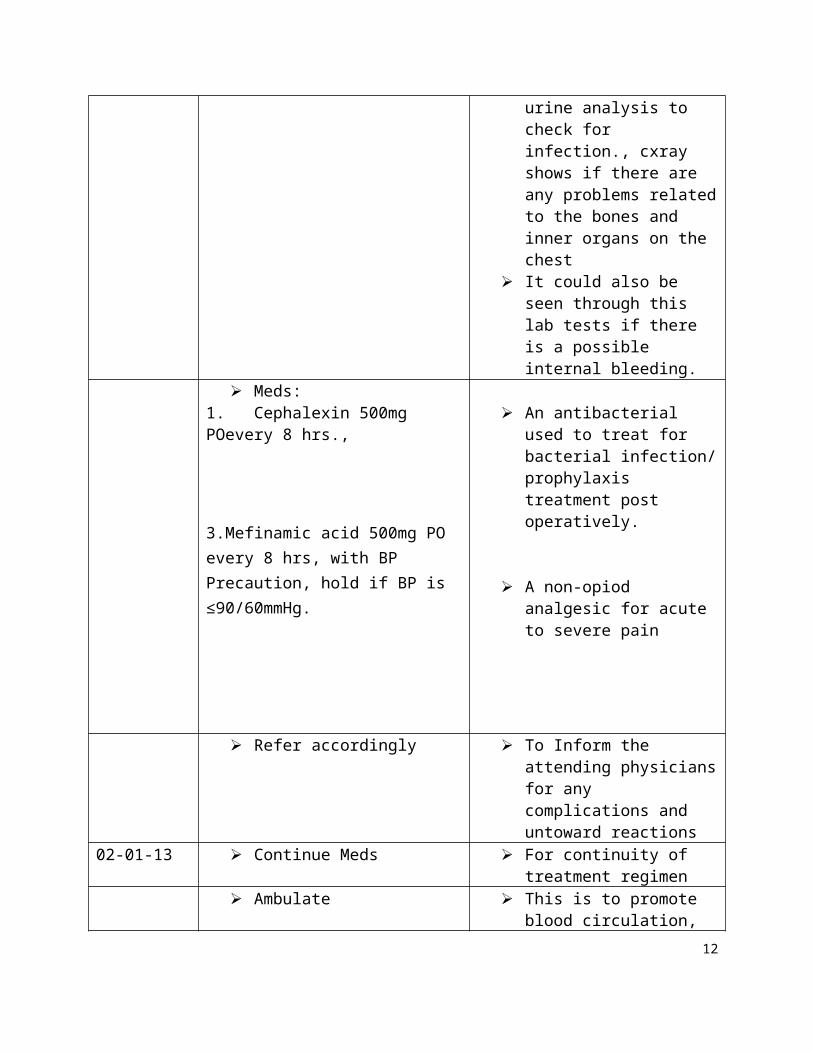
To check or evaluate any deviation from normal in blood count, blood typing to check for what type of blood the patient has for possible blood transfusion and urine analysis to check for infection., cxray shows if there are any problems related to the bones and inner organs on the chest
It could also be seen through this lab tests if there is a possible internal bleeding.
Meds:1. Cephalexin 500mg POevery 8 hrs.,
An antibacterial used to treat for bacterial infection/ prophylaxis treatment post operatively.
8
3.Mefinamic acid 500mg PO every 8 hrs, with BP Precaution, hold if BP is ≤90/60mmHg.
A non-opiod analgesic for acute to severe pain
Refer accordingly To Inform the attending physicians for any complications and untoward reactions
02-01-13 Continue Meds For continuity of treatment regimen
Ambulate This is to promote blood circulation, to prevent the risk of pressure ulcer
Refer accordingly To Inform the attending physicians for any complications and untoward reactions
9
b. Laboratory Results
COMPLETE BLOOD COUNT
Jan 30, 2013
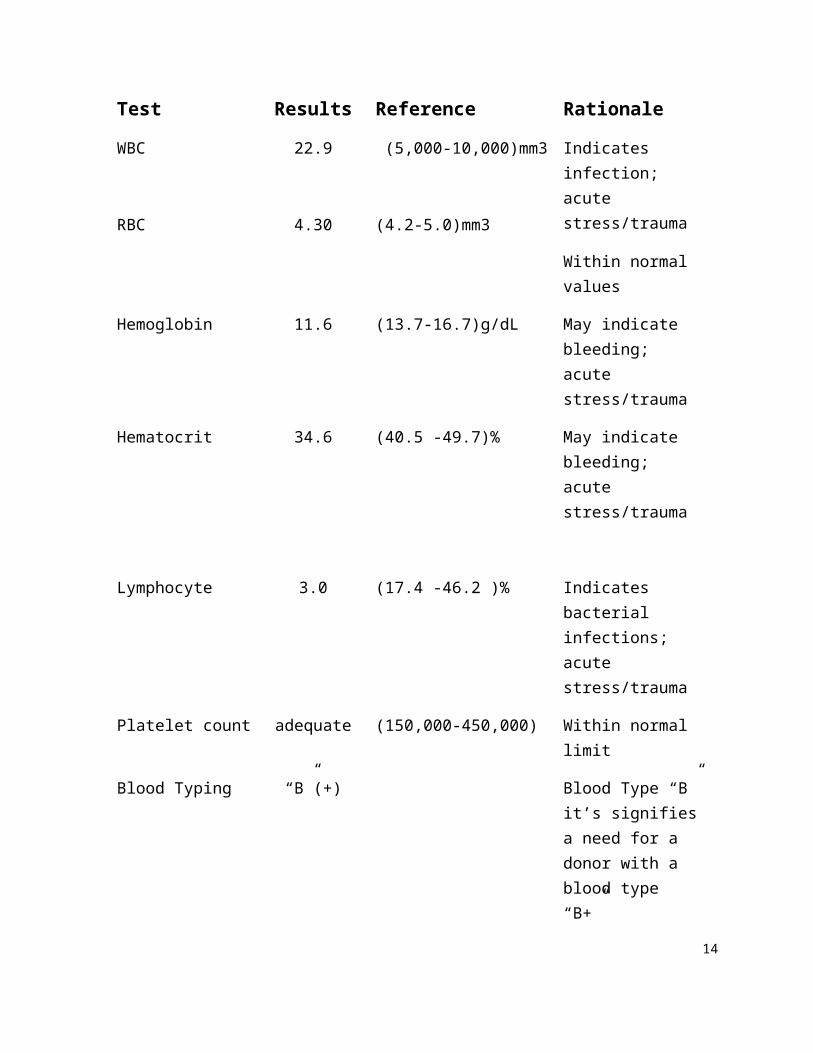
Test Results Reference Rationale
WBC
RBC
22.9
4.30
(5,000-10,000)mm3
(4.2-5.0)mm3
Indicates infection; acute stress/trauma
Within normal values
Hemoglobin 11.6 (13.7-16.7)g/dL May indicate bleeding; acute stress/trauma
Hematocrit 34.6 (40.5 -49.7)% May indicate bleeding; acute stress/trauma
Lymphocyte 3.0 (17.4 -46.2 )% Indicates bacterial infections; acute stress/trauma
Platelet count adequate (150,000-450,000) Within normal limit
Blood Typing “B”(+) Blood Type “B” it’s signifies a need for a donor with a blood type “B+”
10
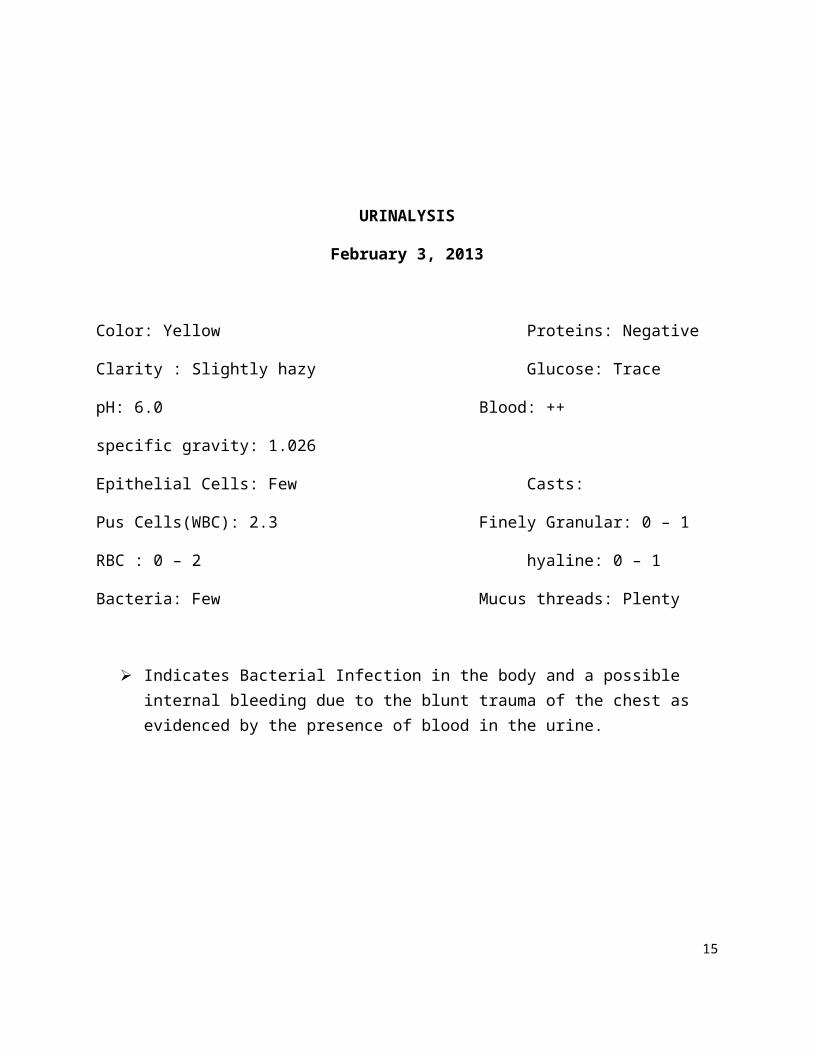
URINALYSIS
February 3, 2013
Color: Yellow Proteins: Negative
Clarity : Slightly hazy Glucose: Trace
pH: 6.0 Blood: ++
specific gravity: 1.026
Epithelial Cells: Few Casts:
Pus Cells(WBC): 2.3 Finely Granular: 0 – 1
RBC : 0 – 2 hyaline: 0 – 1
Bacteria: Few Mucus threads: Plenty
Indicates Bacterial Infection in the body and a possible internal bleeding due to the blunt trauma of the chest as evidenced by the presence of blood in the urine.
11
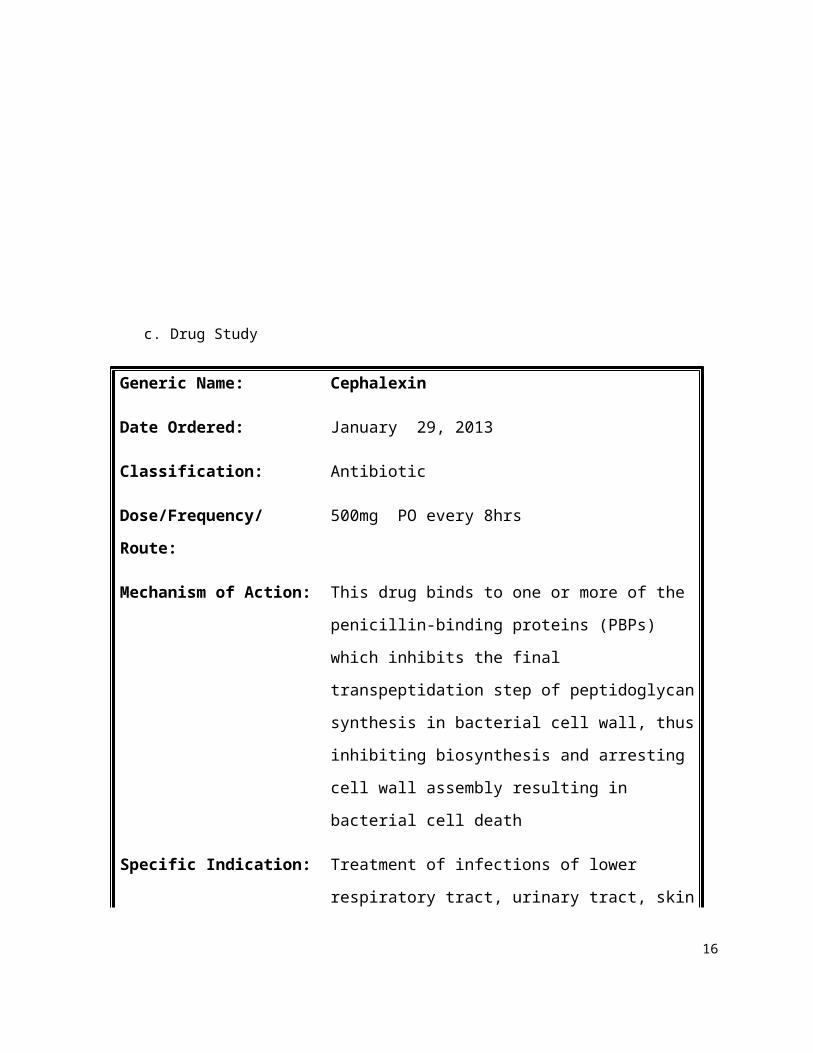
c. Drug Study
Generic Name: Cephalexin
Date Ordered: January 29, 2013
Classification: Antibiotic
Dose/Frequency/Route: 500mg PO every 8hrs
Mechanism of Action: This drug binds to one or more of the penicillin-
binding proteins (PBPs) which inhibits the final
transpeptidation step of peptidoglycan synthesis in
bacterial cell wall, thus inhibiting biosynthesis and
arresting cell wall assembly resulting in bacterial
cell death
Specific Indication: Treatment of infections of lower respiratory tract,
urinary tract, skin and skin structures.
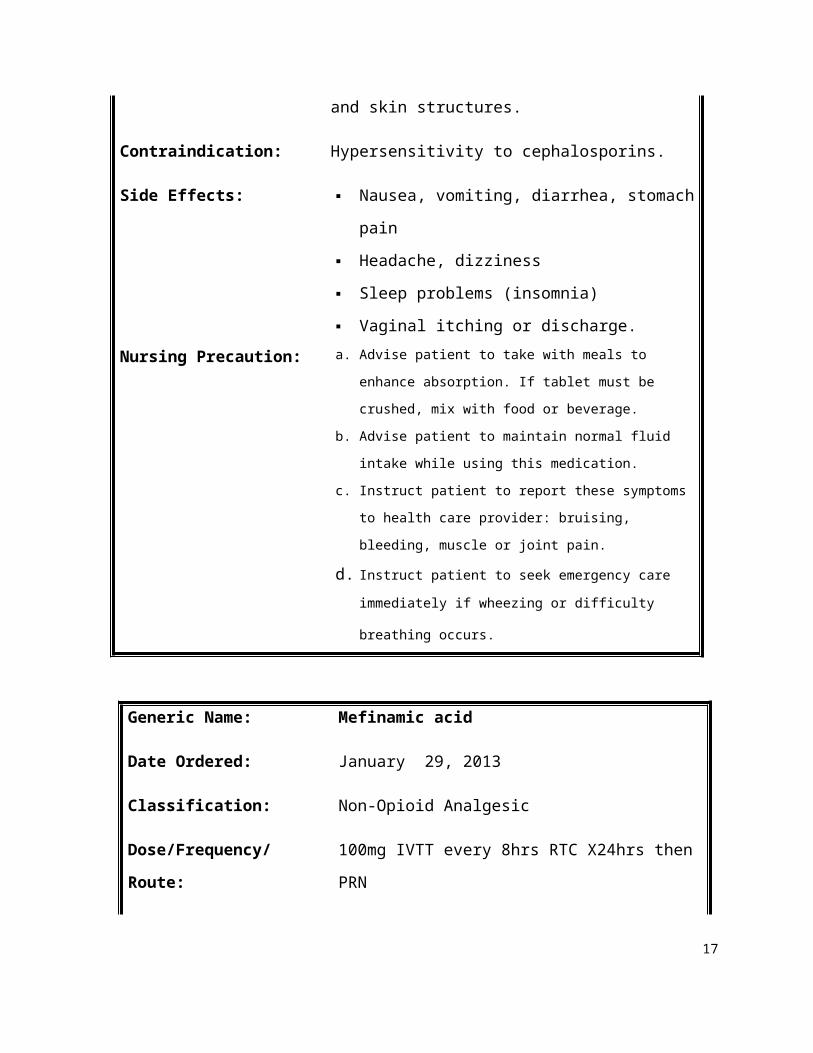
Contraindication: Hypersensitivity to cephalosporins.
Side Effects: Nausea, vomiting, diarrhea, stomach pain
Headache, dizziness
Sleep problems (insomnia)
Vaginal itching or discharge.
Nursing Precaution: a. Advise patient to take with meals to enhance absorption.
If tablet must be crushed, mix with food or beverage.
b. Advise patient to maintain normal fluid intake while using
this medication.
c. Instruct patient to report these symptoms to health care
provider: bruising, bleeding, muscle or joint pain.
d. Instruct patient to seek emergency care immediately if
wheezing or difficulty breathing occurs.
12
Generic Name: Mefinamic acid
Date Ordered: January 29, 2013
Classification: Non-Opioid Analgesic
Dose/Frequency/Route: 100mg IVTT every 8hrs RTC X24hrs then PRN
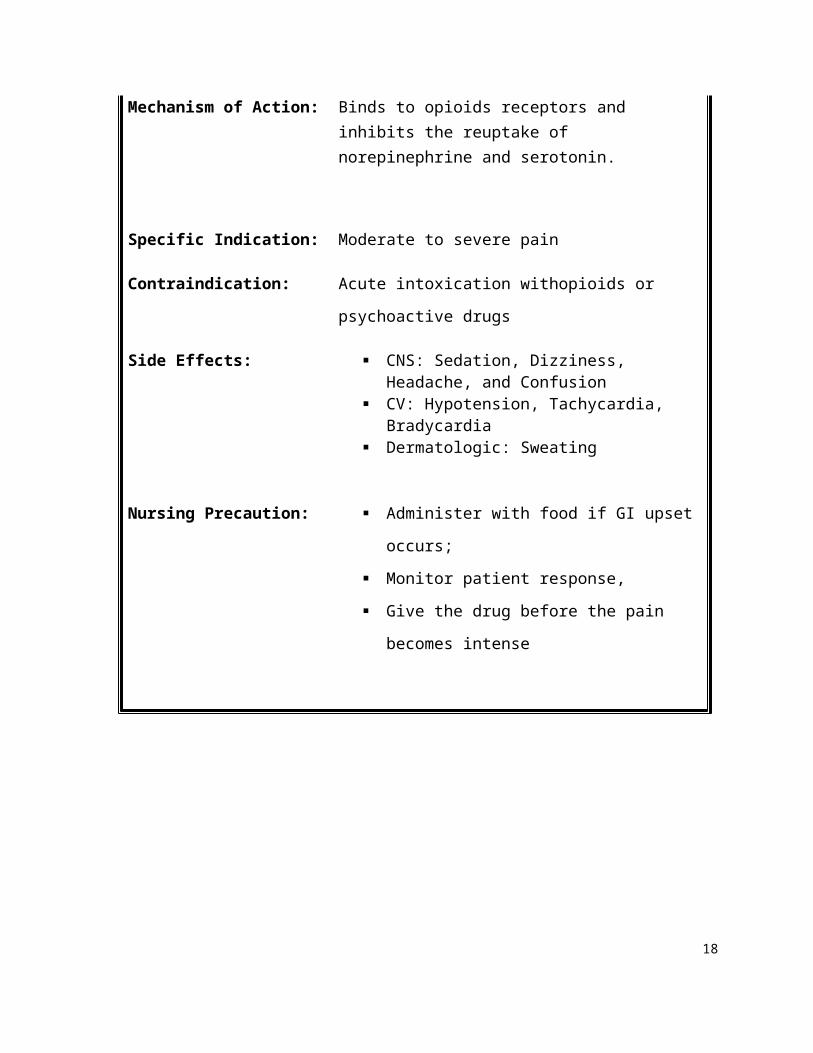
Mechanism of Action: Binds to opioids receptors and inhibits the reuptake of norepinephrine and serotonin.
Specific Indication: Moderate to severe pain
Contraindication: Acute intoxication withopioids or psychoactive
drugs
Side Effects: CNS: Sedation, Dizziness, Headache, and Confusion
CV: Hypotension, Tachycardia, Bradycardia Dermatologic: Sweating
Nursing Precaution: Administer with food if GI upset occurs;
Monitor patient response,
Give the drug before the pain becomes
intense
13
VI. ANATOMY AND PHYSIOLOGY
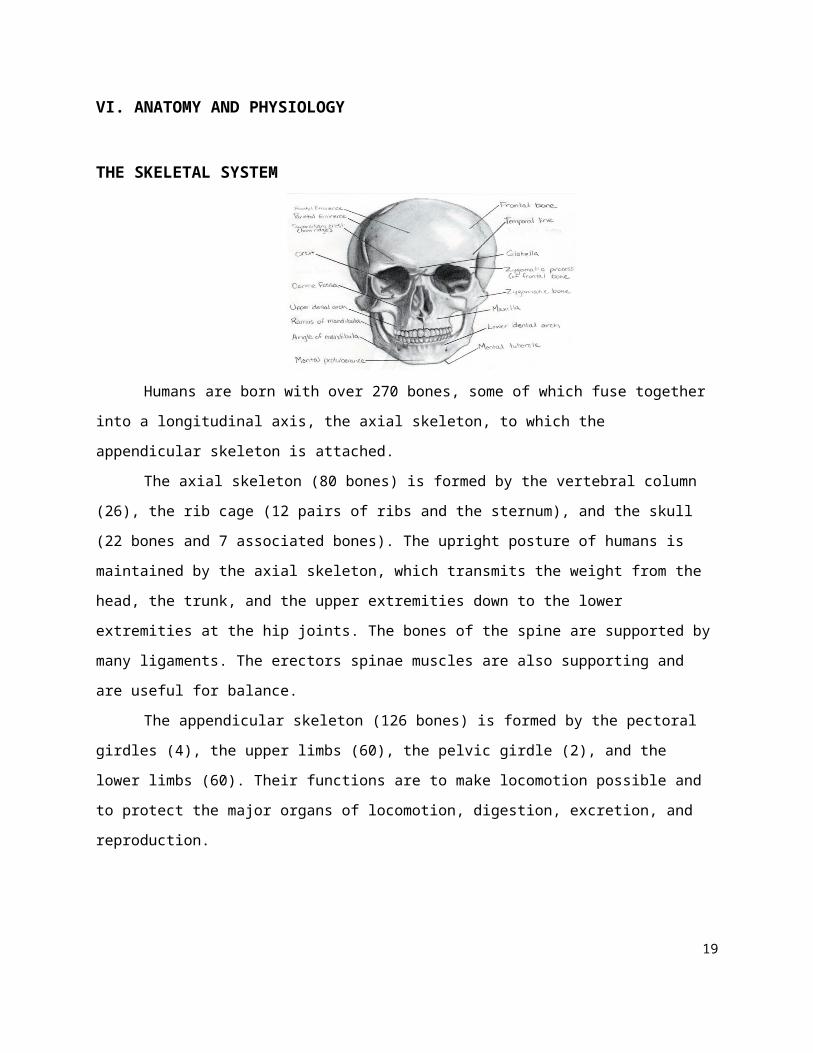
THE SKELETAL SYSTEM
Humans are born with over 270 bones, some of which fuse together into a longitudinal axis, the
axial skeleton, to which the appendicular skeleton is attached.
The axial skeleton (80 bones) is formed by the vertebral column (26), the rib cage (12 pairs of
ribs and the sternum), and the skull (22 bones and 7 associated bones). The upright posture of humans
is maintained by the axial skeleton, which transmits the weight from the head, the trunk, and the upper
extremities down to the lower extremities at the hip joints. The bones of the spine are supported by
many ligaments. The erectors spinae muscles are also supporting and are useful for balance.
The appendicular skeleton (126 bones) is formed by the pectoral girdles (4), the upper limbs
(60), the pelvic girdle (2), and the lower limbs (60). Their functions are to make locomotion possible and
to protect the major organs of locomotion, digestion, excretion, and reproduction.
Function
The skeleton serves six major functions.
Support
The skeleton provides the framework which supports the body and maintains its shape. The pelvis, associated ligaments and muscles provide a floor for the pelvic structures. Without the rib cages, costal cartilages, and intercostal muscles, the heart would collapse.
Movement
The joints between bones permit movement, some allowing a wider range of movement than others, e.g. the ball and socket joint allows a greater range of movement than the pivot joint at the neck. Movement is powered by skeletal muscles, which are attached to the skeleton at
14
various sites on bones. Muscles, bones, and joints provide the principal mechanics for movement, all coordinated by the nervous system.
Protection
The skeleton protects many vital organs:
The skull protects the brain, the eyes, and the middle and inner ears. The vertebrae protect the spinal cord. The rib cage, spine, and sternum protect the human lungs, human heart and major blood
vessels. The clavicle and scapula protect the shoulder. The ilium and spine protect the digestive and urogenital systems and the hip. The patella and the ulna protect the knee and the elbow respectively. The carpals and tarsals protect the wrist and ankle respectively.
Blood cell production
The skeleton is the site of haematopoiesis, the development of blood cells that takes place in the bone marrow.
Storage
Bone matrix can store calcium and is involved in calcium metabolism, and bone marrow can store iron in ferrotin and is involved in iron metabolism. However, bones are not entirely made of calcium, but a mixture of chondroitin sulfate and hydroxyapatite, the latter making up 70% of a bone.
15
VII. PATHOPHYSIOLOGY
DIAGNOSIS: Multiple injuries secondary to vehicular accidentl.
DEFINITION: In medical terminology, blunt trauma, blunt injury, non-penetrating trauma or blunt force trauma refers to type of physical trauma caused to a body part, either injury or physical attack; latter usually being referred as a blunt force trauma. Abdominal blunt trauma is the most common type of trauma attributed from car – to- car collisions, concussion, abrasion, laceration or bone fracturing characterized by severe abdominal pain, tenderness, rigidity, and bruising of the external abdomen. Abdominal trauma presents a
risk of severe blood loss and
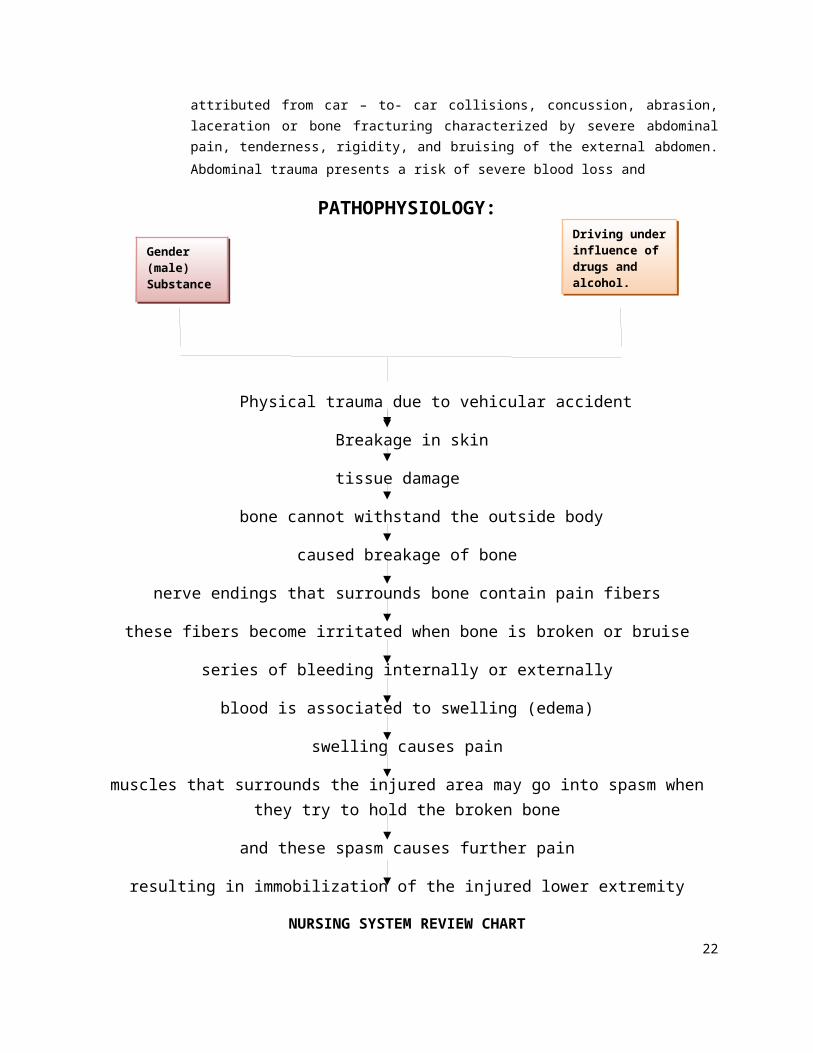
PATHOPHYSIOLOGY:
Physical trauma due to vehicular accident
Breakage in skin
tissue damage
bone cannot withstand the outside body
caused breakage of bone
nerve endings that surrounds bone contain pain fibers
these fibers become irritated when bone is broken or bruise
series of bleeding internally or externally
blood is associated to swelling (edema)
swelling causes pain
muscles that surrounds the injured area may go into spasm when they try to hold the broken bone
and these spasm causes further pain
resulting in immobilization of the injured lower extremity
Gender (male)Substance abuse
Driving under influence of drugs and alcohol.Alcohol Drinking
16
NURSING SYSTEM REVIEW CHART
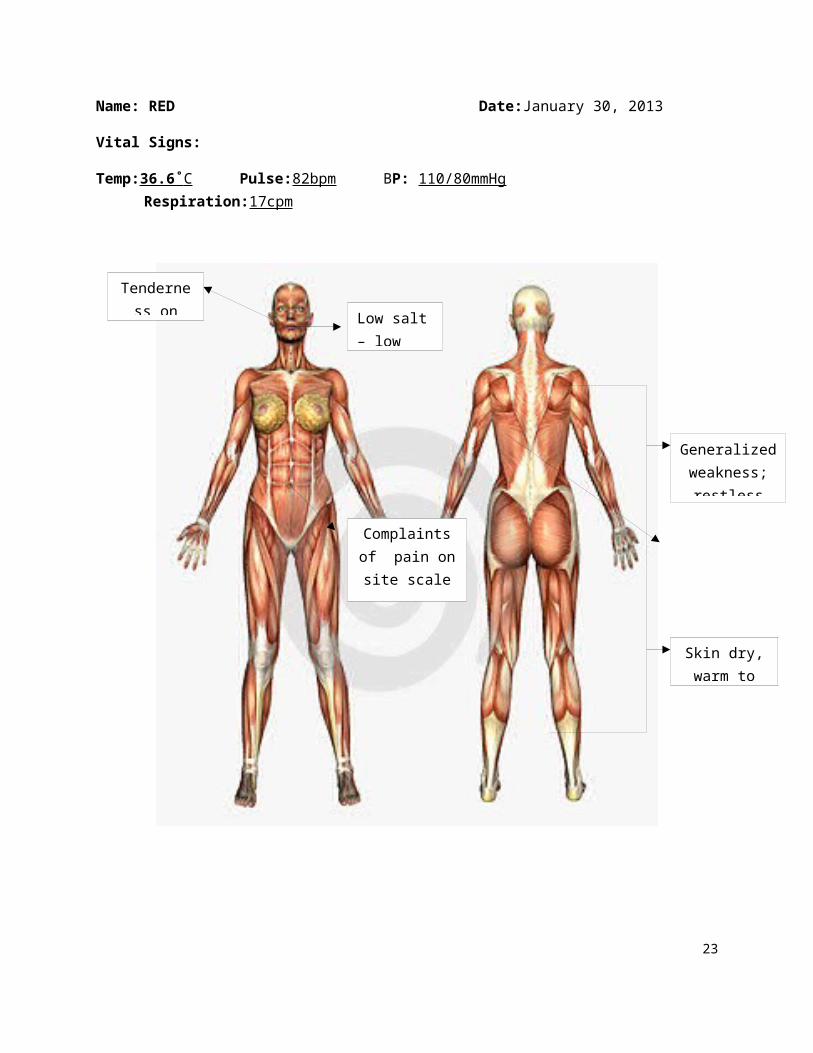
Name: RED Date:January 30, 2013
Vital Signs:
Temp:36.6˚ C Pulse:82bpm BP: 110/80mmHg Respiration:17cpm
Tenderness on face
Generalized weakness; restless
Skin dry, warm to touch
Complaints of pain on site scale
of 8/10
Low salt – low fat diet
17
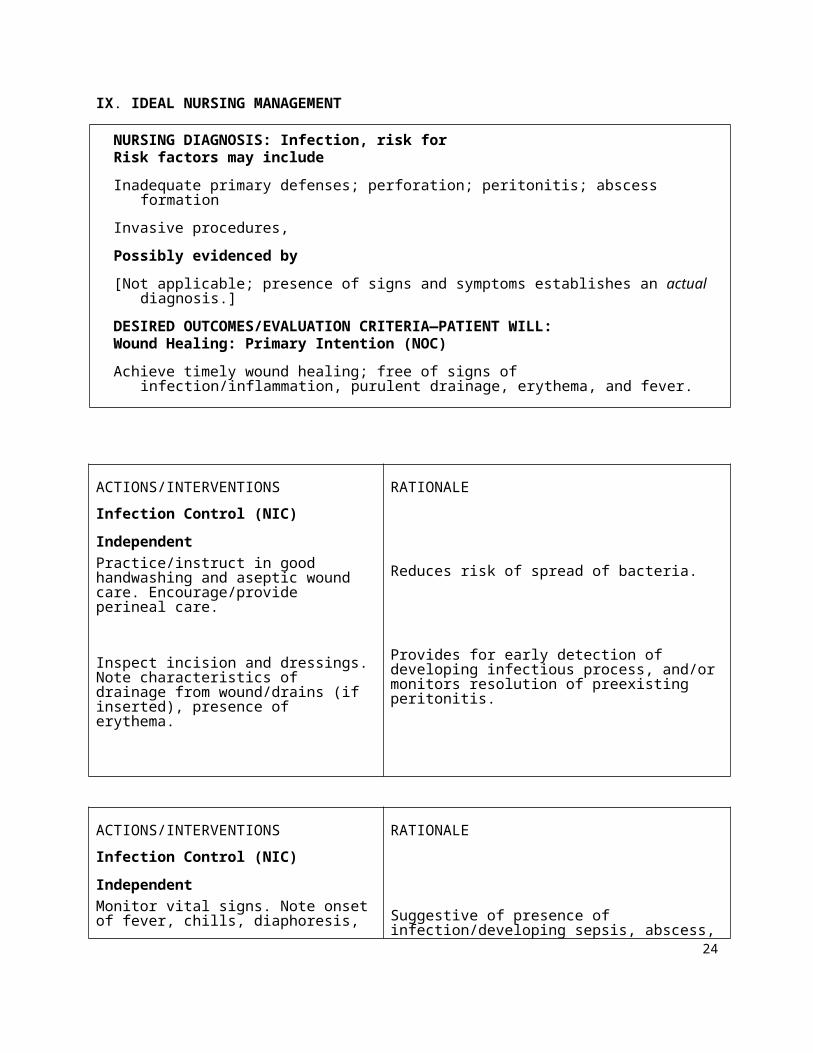
IX. IDEAL NURSING MANAGEMENT
NURSING DIAGNOSIS: Infection, risk forRisk factors may include
Inadequate primary defenses; perforation; peritonitis; abscess formation
Invasive procedures,
Possibly evidenced by
[Not applicable; presence of signs and symptoms establishes an actual diagnosis.]
DESIRED OUTCOMES/EVALUATION CRITERIA—PATIENT WILL:Wound Healing: Primary Intention (NOC)
Achieve timely wound healing; free of signs of infection/inflammation, purulent drainage, erythema, and fever.
ACTIONS/INTERVENTIONS
Infection Control (NIC)
Independent
Practice/instruct in good handwashing and aseptic wound care. Encourage/provide perineal care.
Inspect incision and dressings. Note characteristics of drainage from wound/drains (if inserted), presence of erythema.
RATIONALE
Reduces risk of spread of bacteria.
Provides for early detection of developing infectious process, and/or monitors resolution of preexisting peritonitis.
ACTIONS/INTERVENTIONS
Infection Control (NIC)
Independent
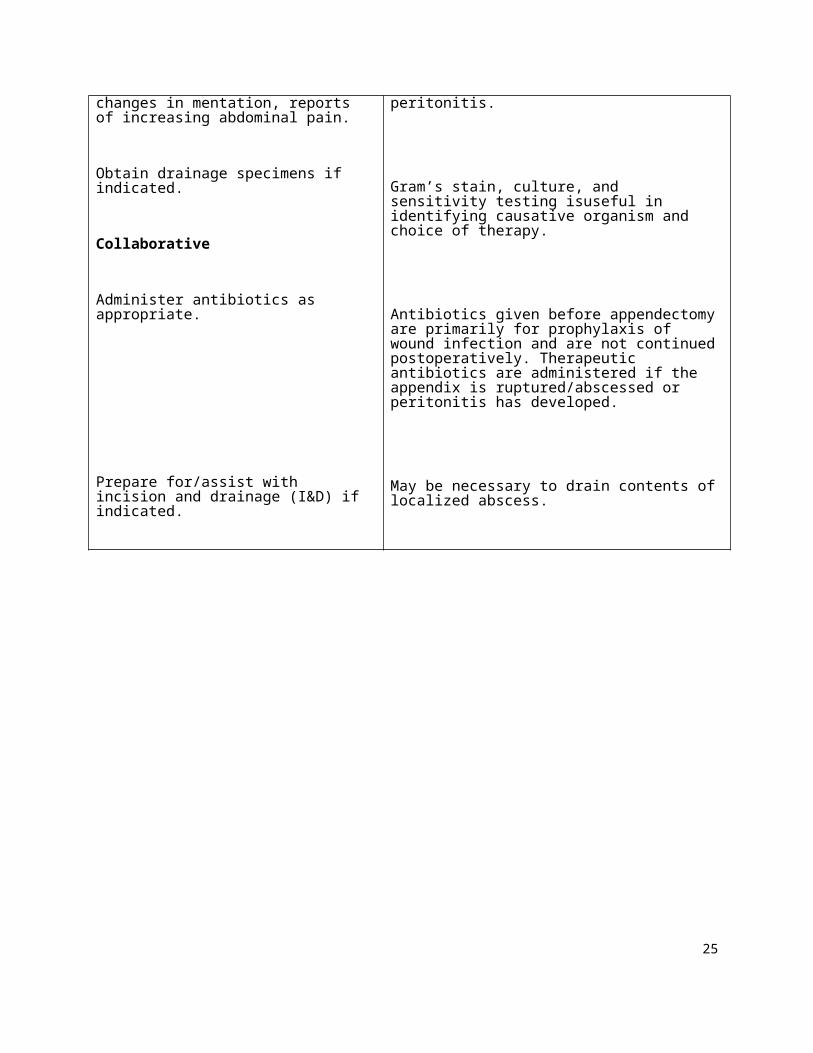
Monitor vital signs. Note onset of fever, chills, diaphoresis, changes in mentation, reports of increasing abdominal pain.
RATIONALE
Suggestive of presence of infection/developing sepsis, abscess, peritonitis.
18
Obtain drainage specimens if indicated.
Collaborative
Administer antibiotics as appropriate.
Prepare for/assist with incision and drainage (I&D) if indicated.
Gram’s stain, culture, and sensitivity testing isuseful in identifying causative organism and choice of therapy.
Antibiotics given before appendectomy are primarily for prophylaxis of wound infection and are not continued postoperatively. Therapeutic antibiotics are administered if the appendix is ruptured/abscessed or peritonitis has developed.
May be necessary to drain contents of localized abscess.
19
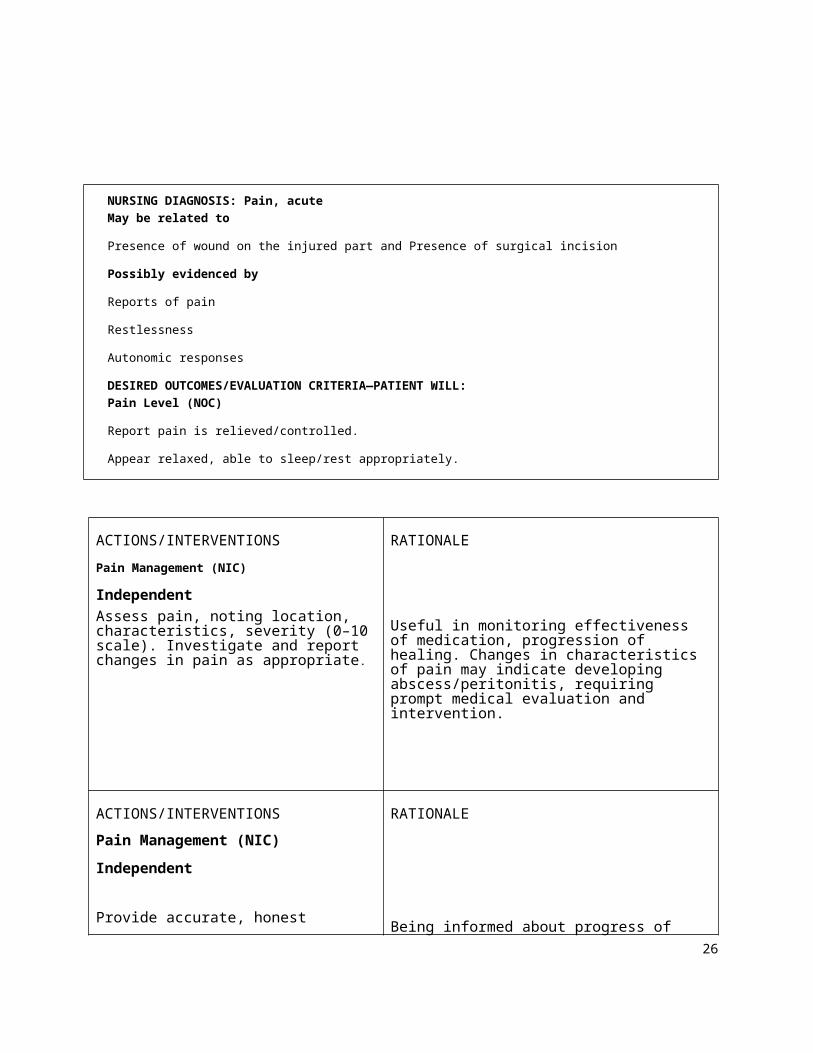
NURSING DIAGNOSIS: Pain, acute
May be related to
Presence of wound on the injured part and Presence of surgical incision
Possibly evidenced by
Reports of pain
Restlessness
Autonomic responses
DESIRED OUTCOMES/EVALUATION CRITERIA—PATIENT WILL:
Pain Level (NOC)
Report pain is relieved/controlled.
Appear relaxed, able to sleep/rest appropriately.
ACTIONS/INTERVENTIONS
Pain Management (NIC)
Independent
Assess pain, noting location, characteristics, severity (0–10 scale). Investigate and report changes in pain as appropriate.
RATIONALE
Useful in monitoring effectiveness of medication, progression of healing. Changes in characteristics of pain may indicate developing abscess/peritonitis, requiring prompt medical evaluation and intervention.
ACTIONS/INTERVENTIONS
Pain Management (NIC)
Independent
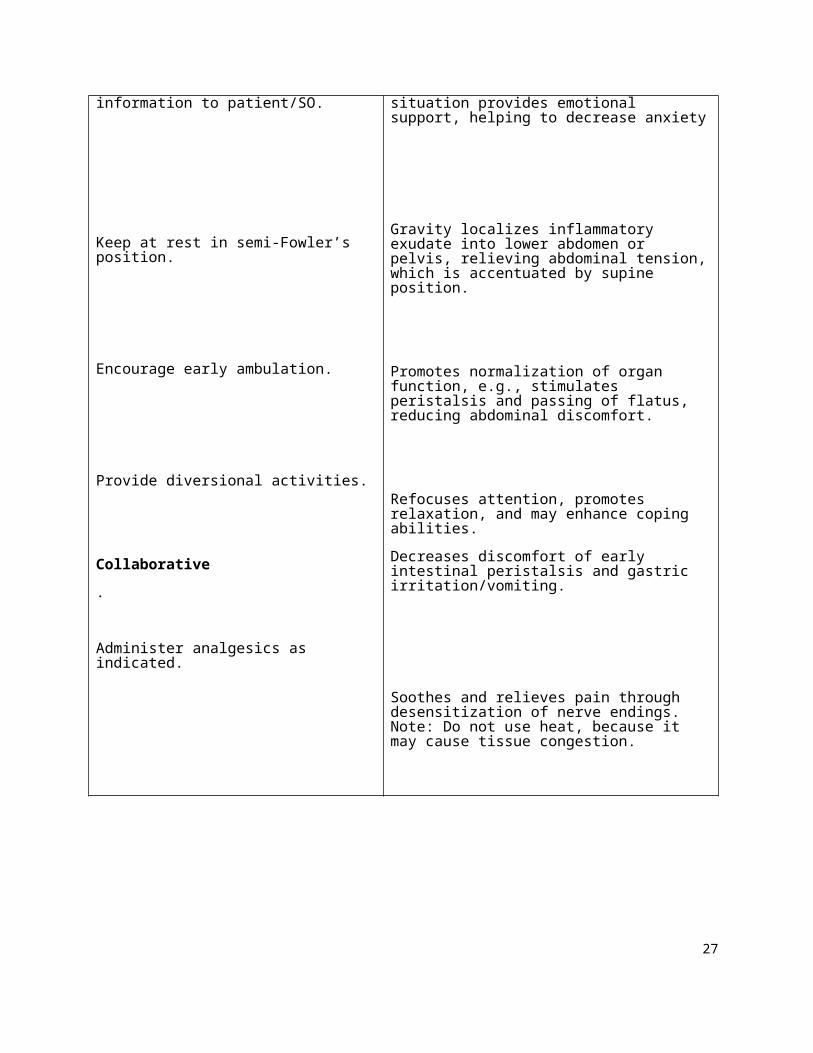
Provide accurate, honest information to patient/SO.
RATIONALE
Being informed about progress of situation provides emotional support, helping to decrease anxiety
20
Keep at rest in semi-Fowler’s position.
Encourage early ambulation.
Provide diversional activities.
Collaborative
.
Administer analgesics as indicated.
Gravity localizes inflammatory exudate into lower abdomen or pelvis, relieving abdominal tension, which is accentuated by supine position.
Promotes normalization of organ function, e.g., stimulates peristalsis and passing of flatus, reducing abdominal discomfort.
Refocuses attention, promotes relaxation, and may enhance coping abilities.
Decreases discomfort of early intestinal peristalsis and gastric irritation/vomiting.
Soothes and relieves pain through desensitization of nerve endings. Note: Do not use heat, because it may cause tissue congestion.
21
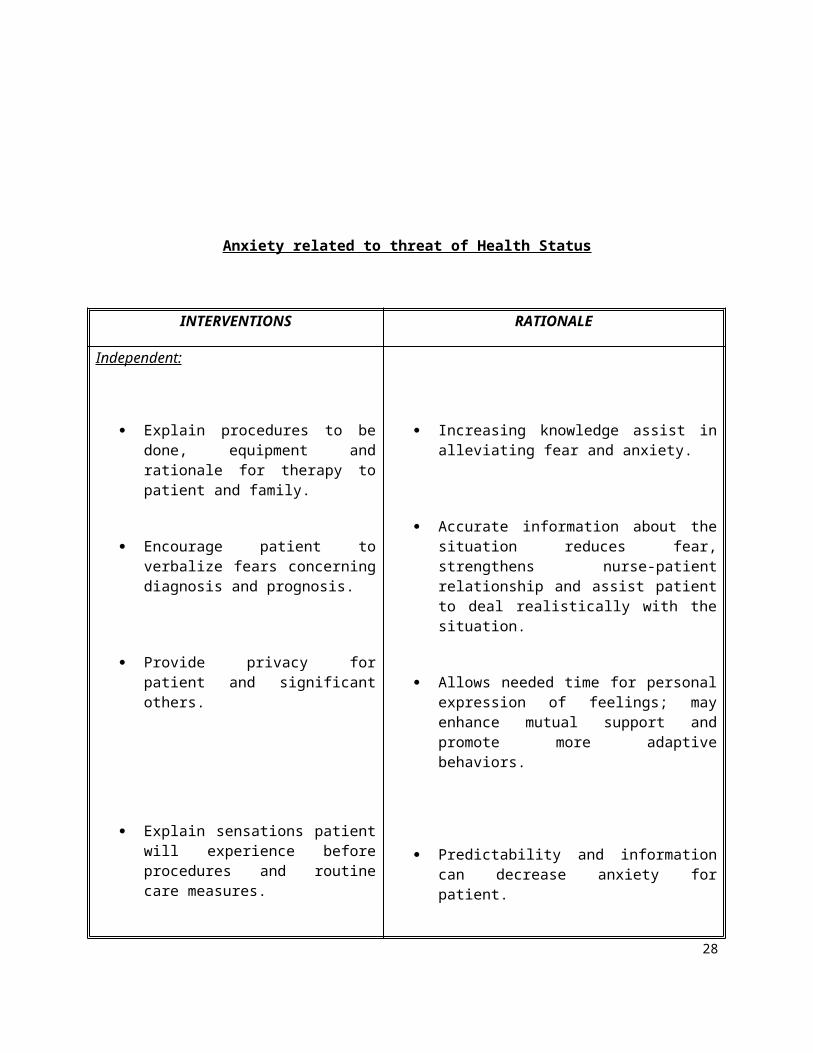
Anxiety related to threat of Health Status
INTERVENTIONS RATIONALE
Independent:
Explain procedures to be done, equipment and rationale for therapy to patient and family.
Encourage patient to verbalize fears concerning diagnosis and prognosis.
Provide privacy for patient and significant others.
Explain sensations patient will experience before procedures and routine care measures.
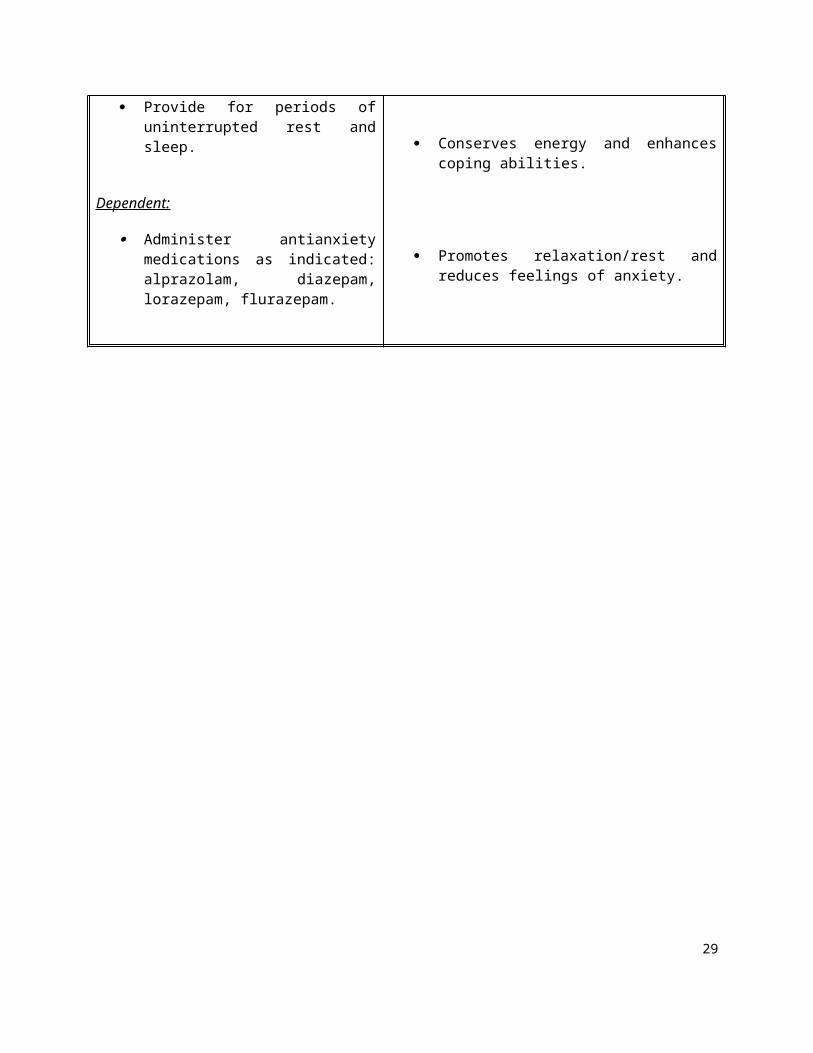
Provide for periods of uninterrupted rest and sleep.
Dependent:
Administer antianxiety medications as indicated: alprazolam, diazepam, lorazepam, flurazepam.
Increasing knowledge assist in alleviating fear and anxiety.
Accurate information about the situation reduces fear, strengthens nurse-patient relationship and assist patient to deal realistically with the situation.
Allows needed time for personal expression of feelings; may enhance mutual support and promote more adaptive behaviors.
Predictability and information can decrease anxiety for patient.
Conserves energy and enhances coping abilities.
Promotes relaxation/rest and reduces feelings of anxiety.
22
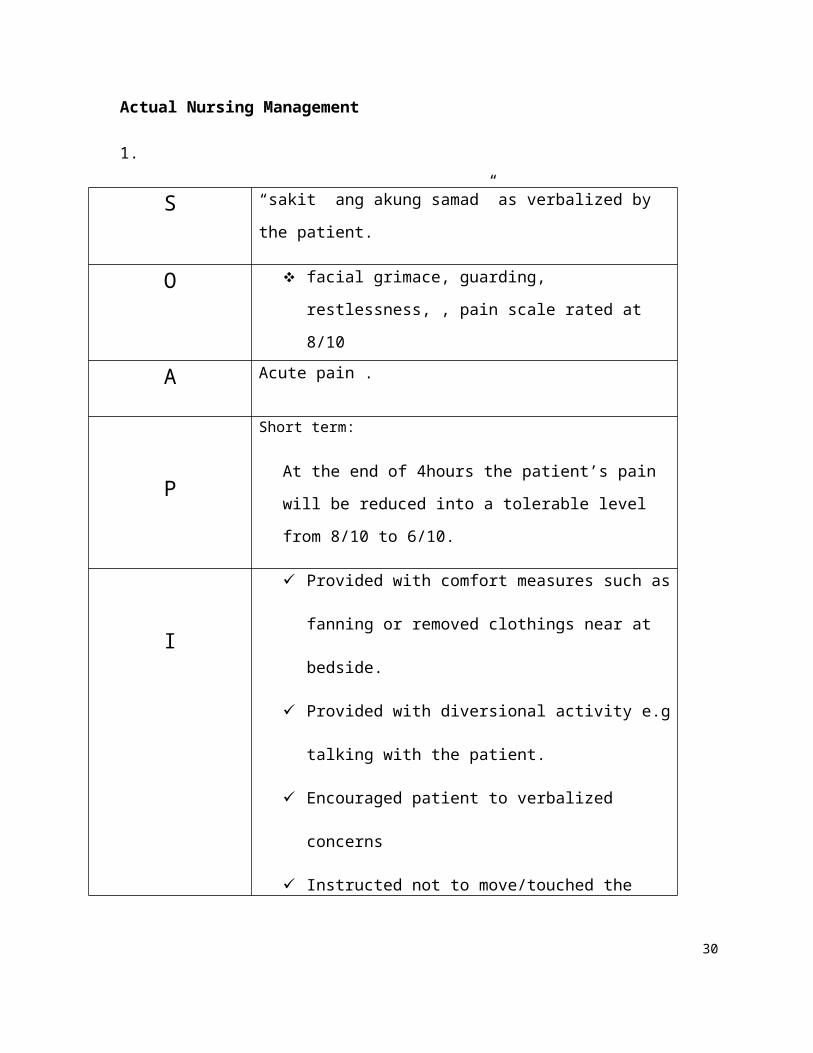
Actual Nursing Management
1.
S “sakit ang akung samad” as verbalized by the patient.
O facial grimace, guarding, restlessness, , pain scale
rated at 8/10
A Acute pain .
P
Short term:
At the end of 4hours the patient’s pain will be reduced
into a tolerable level from 8/10 to 6/10.
I
Provided with comfort measures such as fanning or
removed clothings near at bedside.
Provided with diversional activity e.g talking with
the patient.
Encouraged patient to verbalized concerns
Instructed not to move/touched the affected part.
Administered Tramadol 100mg IVTT every 8hrs
Round the clock
E At the end of 4hrs, the patient’ was able to verbalized
tolerable level of pain rated 6/10
23
2.
S -
O -
A Risk for infection related to surgical incision
PAt the end of 30 minutes the patient will verbalize
understanding on the importance of wound cleaning and
preventing infection.
I
Provided universal precaution e.g. handwashing.
Provided daily wound dressing
Encouraged to dry wound and change dressing
aseptically
Taught proper wound dressing
Encouraged proper hygiene
Instructed to take medication cephalexin 500mg I
cap TID religiously
E After 30 minutes of nursing intervention, patient was able
to verbalize understanding on the importance of a clean
and proper wound dressing.
24
3.
S “kanus-a kaha ni matangtang ning tahi sir?
O- Anxious/restlessness- Expression of fear- Preoccupied
A Anxiety related to change in health status.
P
At the end of 1 hour, the client will be able to minimize anxious behavior.
I
1. Spent times with the client.- Non- care related time spent with anxious patient
builds trust and reduces tension2. Allowed client to express feelings verbally
- This may allow patient to identify anxious behaviors and discover source of anxiety
3. Provided a comfortable stress free environment.- To relieve anxiety
4. Taught client relaxation technique- These measures can restore psychological and
physical equilibrium5. Provide privacy for patient and significant others.
- Allows needed time for personal expression of feelings; may enhance mutual support and promote more adaptive behaviors.
- 6. Provided treatment information on an ongoing basis.
E Goal met. At the end of 1 hour, the client has been able to minimize anxious behavior.
X. EVALUATION AND IMPLICATION25
During the initial assessment, patient Mr. RED was in a dire condition, sustaining
serious injuries. The incident will surely be a traumatic experience to him considering
that he feels Iikes his family no longer needs him to sustain their needs although he was
anxious, restless at first but the support of his family really gave him the courage that
they can.
In response to his condition, care was given to him. His vital signs were
monitored every 4 hours, I & 0 every hour to closely monitored his kidney functioning.
Medications due for him were given and wound dressing was done everyday. Advocacy
in nursing was definitely applied in his care, accepting his minute requests so as to
alleviate his suffering as much as possible. His temperature was also monitored
because of some changes due to his status post condition.
In caring for patient Mr. RED, I have not only contributed to the betterment of his
health, but also to the improvement of myself as student nurses. Any circumstance
during the time of caring for patient Mr. RED added to the skills, knowledge and attitude
which will surely be beneficial in the future.
26
XI. REFERRALS and RECOMMENDATION
HEALTH TEACHINGS
Name of patient:RED
Medications
Instructed client as well as the significant others about the indications and
mechanisms of actions of each drug that the doctor ordered so that without
hesitation they will really comply all the medications given with them.
Adherence to the medication promotes improvement of condition.
Exercise
Encouraged frequent changes of position according to his comfort like sitting on
bed if his body can tolerate and by turning to sides to prevent bedsores.
Avoid over strenuous activities
Encouraged passive range of motion to promote proper circulation and prevent
muscle atrophy/complication brought by immobility.
Instructed also the client at home to balance his daily activities especially when
discharged.
Encouraged patient to do deep breathing exercises/ Relaxation Technique
Treatment
Advised/Emphasized the importance to adhere to treatment regimen. That is to
facilitate faster improvement of present condition and prevent complication.
Bed rest is important to prevent over fatigability then ambulate with in tolerable
limits
Encouraged to apply lotion such as Johnson lotion and petroleum jelly to his dry
and cracked skin to prevent further skin injury.
Advised to have a regular check up at the nearest health center/health care
provider for check up monitoring.
Increased fluid intake up to 6-8 glasses a day
27
Outpatient (CHECK-UP)
Instructed the client’s family to come back one week after discharged for further
follow-up and evaluation of the client’s health condition. This is very important so
that the health condition of the client will be evaluated if there is better
improvement. The physician should see and examine the physical appearance of
the client.
Diet
Taught the importance of eating green leafy vegetables such as alugbati,
malunggay, saluyot because this will prevent constipation especially at this time
because his peristalsis decreases due to limited movement
Encouraged low salt intake. The use of salt as a flavoring agent needs to be
controlled because this is usually the cause of fluid retention.
Encouraged intake of vitamin C, such as home made lemonade and oranges
because the patient has post surgical incision that will aid in healing.
Increased intake of protein because this is important for skin integrity.
Increased intake of fruits and vegetables because this can provide vitamins and
minerals for nutrition.
The family or the significant others is advised to comeback on the scheduled
date of visit with the physician together with the referral form given during time of
discharged on the exact time/date and place specified for monitoring/rechecking of his
condition. The family is also encouraged to monitor the patient and to not allow the
patient to do strenuous activities that would be a cause of further exacerbation of the
injured area. We encouraged the patient’s family to let the patient eat more fruits and
vegetables as well to have rich in fiber to prevent constipation. And lastly encouraged
the family or the significant others to have regular visit to the health center or clinic and
avoid self-medication or taking medications out of what is being prescribed.
28
XII. PROGNOSIS
The attending physician, as well as those who gave care and studied the case of Mr. RED came up with good prognosis basing from the aforementioned indicators, and justified as follows:
A. Knowledge of the disease condition
The diagnosis for this criterion is good because he showed understanding in the importance of compliance/adhering to treatment regimen, although he has a positive attitude but lacks financial aspect was really an impact on him considering as well that he is the only person who works in the family
B. Extent of the disease
The extent of the disease was good .
C. Availability of medications and compliance
Not good, because sometimes he can take those medication needed but as much as they wanted to still there would be a times that they don’t have sufficient funds for treatment regimen compliance.
D. Attitude and willingness to take the medications and follow treatment regimen
Good prognosis because he was able to take his medications on time and followed the treatment regimen for management of his condition with a positive attitude for compliance and cooperation although there would be a time that he can’t deny that he missed some dosage due to financial aspect
E. Family support
Mr. RED’s wife was always there for him supports and helps the patient cope with stress and anxiety.
29
XIV.Bibliography
Douges, M.E. et.al., (2002).. Nurse’s pocket guide: diagnosis, interventions & rationales. (8th Edition).Philadelphia: F.A. Davis Company.
Douges, M.E. et.al., (2002).. Nursing care plan: guidelines for individualizing patient care (6th Edition) Philadelphia:
F..A. Davis Company.Gulandick, M. et.al., Nursing care plan. (3rd Edition)
Ignatavicius, D.D. & Workman, M.L. (2006). Medical-surgical nursing: critical thinking for collaborative care. (5th Edition). St. Louis, Missouri: Elsevier Saunders.
Kozier, B. et.al., (2004). Fundamentals of nursing: concepts, process & practice. (7th Edition). Philippines: Pearson Education South Asia PTE Ltd.
Smeltzer, S.C.& Bare, B.G. (2004).Textbook of medical-surgical nursing(10th
Edition, Volume 2). Philadelphia: Lippincott Williams and Wilkins. pp 553-538.
Spratto, G.R. & Woods, A.L. (1994). Nurse’s drug reference. USA: Delmar Publishers Incorporated.
Ulrich & Canale. (2005). Nursing care planning guides. (6th Edition).
Webliography:
www.mayoclinic.com/INJURIEs
www.yahoo.com/fall
www.google.com/images/lungs
30
![Motor Accident Injuries Amendment Bill 2013 Print.pdf · Insert instead “Motor Accident Injuries Act”. [18] Section 17A Insert after section 17: 17A Right to recover higher premiums](https://img.pdfslide.us/doc/110x75/5fdc4f8c0feee444ea6303e3/motor-accident-injuries-amendment-bill-2013-printpdf-insert-instead-aoemotor.jpg)