Embed Size (px)
Citation preview

Thorax (1973), 28, 782.
Multiple bilateral fibromas of the pleuraC. M. SCATTINI and A. ORSI
Hospital Rivadavia and Hospital Alvear, Buenos Aires, Argentina
Scattini, C. M. and Orsi, A. (1973). Thorax, 28, 782-787. Multiple bilateral fibromas of thepleura. A patient with multiple bilateral fibromas of the pleura which evolved over 25 yearsis presented. Tumours were resected in four successive surgical interventions during thisperiod. At the second operation 'spontaneous regression' of several small pleural fibromasnoted at the first operation four years previously was observed. The differentiation betweenpleural fibroma and pleural localized mesothelioma is discussed.
Fibromas of the pleura are rare tumours. Evenand Sors (1959) estimate that there is one primarypleural tumour for every 100 bronchial carcinomasand that in primary pleural tumours malignantlesions are four times more frequent than benignlesions. Reports of fibromas of the pleura onlyrecord the existence of single fibromas (Halperin,Bilesio, and Orlando, 1955; Decroix and Pieron,1963; Sen, Parulkar, Kinare and Gandhi, 1964),but some authors report a recurrence (Kerr andNohl, 1961) or a malignant transformation(Huguenin-Dumittan, Mach, and Press, 1968). Webelieve that our case of multiple bilateral benignfibromas of the pleura which evolved over aperiod of 25 years is unique.
CASE REPORT
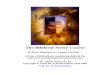
O.P. de L., a 35-year-old woman, was first seen inJanuary 1948 complaining of weakness and slightfever. Six months previously she had noticed pain inthe posterior aspect of the right chest wall madeworse by breathing. The pain was readily controlledwith analgesics, but one month later bilateral chestpain developed as well as cough made worse by dampweather. In view of these symptoms a chest radio-graph was taken which revealed an upper right para-mediastinal mass (Figs. 1 and 2).
Physical examination showed evidence of weightloss with an evening fever of about 37 5'C. Physicalexamination was otherwise normal.
Laboratory investigations showed the blood countto be normal and the sedimentation rate 11/26. Casonireaction for hydatid disease was negative. Mantouxreaction 1/1,000 was positive++++. She was treatedwith rest, calcium, and vitamins. Two months later the
Requests for reprints: Dr. C. M. Scattini, Hospital Rivadavia.Buenos Aires, Argentina
patient stated that she had no more chest pain norfever and had gained 5 kg in weight.
It was considered that the mediastinal mass observedradiographically could be due to a benign lung ormediastinal tumour. After induction of a right pneumo-thorax the tumour descended with the lung and thiswas taken as probable evidence that the mass arosefrom within the lung.
In April 1948 a right thoracotomy was performedand the tumour was felt in close relation to the rightupper lobe, well delineated and surrounded by normallung parenchyma. While exploring the rest of thelung and the parietal and visceral pleura, numerous
FIG. 1. Chest radiograph in 1948, showing right upperparamediastinal fibroma.
782
copyright. on F
ebruary 8, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.28.6.782 on 1 Novem
ber 1973. Dow
nloaded from

Miultiple bilateral fibromas of the pleurawhite hard nodules of different sizes were found overthe visceral pleura and one over the parietal pleura.The largest nodule, approximately 4 cm long and2 cm wide, was resected for histological study, andas all of these were considered to be metastases fromeither the primary pulmonary tumour or an undetectedextrapulmonary source, resection of the main tumourwas not undertaken. The histopathological diagnosisof the resected small tumour was benign fibroma ofthe pleura.The postoperative course was normal but the
patient's follow-up serial radiographs showed gradualgrowth of the main tumour. No enlargement of thesmall tumours observed during operation could bedetected.Four years later, in July 1952, in view of the pro-
gressive growth of the tumour, a second thoracotomy.l3_Ewas carried out. A few pleural adhesions were easily
divided. An unexpected finding was that from themultiple pleural seedlings observed at the previousoperation, only one, the size of a grain of corn,whitish and hard, could be seen on the visceral pleura.On the surface of the visceral pleura small granula-tions, representing spontaneous involution of thetumours observed at the first operation, could be
[G. 2. Same patient as in Fig. 1. Lateral view. palpated but not seen. The main paramediastinal
7...4
4w~~ ~ ~ ~ ~ ~
FIG. 3. Histology offibroma resectedin 1952. (Haematoxylin and eosin x 150).
FlI
783
copyright. on F
ebruary 8, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.28.6.782 on 1 Novem
ber 1973. Dow
nloaded from

C. M. Scattini and A. Orsi
tumour, which arose from the visceral pleura andwhich had vascular pedicles arising from the lungparenchyma, was resected. Histopathological studyshowed, as in the case of the small tumour resectedin the previous operation, that it was a benign fibrouspleural fibroma (Fig. 3).
Fifteen years after the second operation, in 1967,the patient, who up to that time had enjoyed goodhealth, returned complaining of weight loss, weak-ness, and cough and a complete clinical evaluationwas undertaken. A chest radiograph showed absenceof the posterior end of the fourth and part of thefifth right ribs from the previous operations. In thelungs a number of new shadows were seen. The largestwas in the right paratracheal region, and three otherswere in the left hemithorax. In addition, a markedelevation of the left hemidiaphragm was observed,which had not been noted in the previous radio-graphs. The left hemidiaphragm showed normalmotility on screening. These radiographic shadowswere interpreted as probably metastatic from anextrapulmonary tumour or as hydatid cys!ts. Anexhaustive search for an extrapulmonary tumour wasnegative. The blood count, sedimentation rate, bloodsugar and urea, serum protein electrophoresis, andurine were normal. Considering her previous opera-tions 15 and 19 years previously, which on bothoccasions demonstrated that the tumours resectedwere pleural fibromas, it was considered probable thatthe new tumours were of a similar histological natureand it was decided to observe the patient.Due to fortuitous circumstances, among them the
t ~~~.p'"_:;.
FIG. 4. Chest radiograph in 1970. A new tumour hasgrown in the right upper paramediastinal region, at the siteof the fibroma resected in 1952. In the left hemithoraxthree other round tumours can be seen, one difficult to seein the PA view.
FIG. 5. Chest radiograph in 1972. Growth of the tumoursin left hemithorax since 1970 is seen.
fact that the patient remained in perfect health, afurther chest radiograph was delayed for three years.This chest radiograph (1970) showed a large rightparatracheal mass, evidently the result of growth ofthe tumour observed three years previously. A bariumswallow showed narrowing and displacement of theoesophagus by the tumour. There was also obviousgrowth of the three tumours in the left hemithorax(Fig. 4).The growth noted during the previous three years
and the compression of important mediastinal struc-tures by the right paratracheal tumour indicated re-operation, after pulmonary function tests had beenfound to be normal. This operation (December 1970)was difficult as the right upper lobe was attachedto the thoracic wall as a result of the previous opera-tions, and, as the adhesions were vascular, haemo-stasis was difficult to achieve. After the lung hadbeen freed, a large tumour growing into the lung butarising from the pleura could be seen, from whicha small portion was resected for histological studyby frozen section. This confirmed the assumption thatit was a pleural fibroma. In the mediastinum thetumour abutted against the superior vena cava andthe trachea, although it was not invading them. Thetumour was resected; it measured 1OX 8 X 8 cm.
Exploration of the surface of the right lung revealedtwo small flat tumours 4 mm in diameter on thevisceral pleura of the middle and lower lobes. Bothwere resected and histological study showed them tobe of a fibrous nature. Histopathological examinationof the resected paratracheal tumour showed a pleuralfibroma containing areas of stroma with extensive
784
jr.,:
IbliO004........:...
copyright. on F
ebruary 8, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.28.6.782 on 1 Novem
ber 1973. Dow
nloaded from

Multiple bilateral fibromas of the pleura
six months after the last
mucoid degenerations and a fibrous capsule in whichfrequent mitoses were observed.A year and a half later obvious growth of the three
tumours in the left hemithorax was seen (Fig. 5) andsurgical resection was decided upon. The generalhealth of the patient during this period was excellentand the laboratory studies and pulmonary functiontests were completely normal. In July 1972 a leftthoracotomy was performed. The lung was free ofadhesions and on the upper lobe, in the area of thelingula, a well demarcated and superficial tumour was
found, arising from the visceral pleura but penetratinginto the lung. In order to remove it, it was necessaryto resect part of the pulmonary parenchyma. A secondtumour was found arising from the visceral pleura,well encapsulated, growing intraparenchymally, andmeasuring 2 x 1 x 1 cm. In the posterior surface ofthe superior segment of the lower lobe, the thirdtumour that had been visible in the chest film was
found, well encapsulated and measuring 3x4x4 cm.
In addition to these three main lesions another threesmall round tumours of less than 0-5 cm in diameterwere found on the visceral pleura, one on the upperlobe and the other two on the left lower lobe. Theywere locally resected. Histological examination showedthe fibrous nature of all these tumours, some of themwith areas of mucoid transformation and some withmitosis. Figure 6 shows a radiograph obtained sixmonths after the last surgical intervention.
DISCUSSION
This case presents two significant characteristics-the spontaneous regression of most of the multiple
pleural tumours observed at the first operation,and the multiplicity of fibromas over a period ofalmost 25 years. It is impossible to determine thecause of this tumour regression, although un-deniable proof of spontaneous regression ofmalignant tumours does exist (Everson and Cole,1959; Boyd, 1966). Although the determiningmechanism is uncertain, there is no doubt thatin this patient tumour regression occurred. Theright paratracheal tumour discovered in thepatient 18 years after her second operation hadthe same location as the fibroma resected then,and this raises the question whether it was a newtumour or a recurrence. The potential to recur-rence of pleural tumours is well known, and inspite of the original benign fibrous nature of thetumour in this case the recurrence may presentmalignant characteristics. Kerr and Nohl (1961)described six patients with benign intrathoracicfibromas, judged by their postoperative histo-pathological appearances. In five, the tumourrecurred with undeniably malignant character-istics; the remaining case showed a benign fibroustumour. Recurrence took place up to 12 yearsafter resection of the primary tumour.Had there not been additional pleural tumours,
the fibroma resected in 1970 might be regardedas a recurrence, but the possibility of a newtumour growing in almost the same place as theone previously resected could also be considered.It may be pointed out that the growth of fibromasseemed to be limited to the pleura, as an exhaus-tive examination of the patient did not revealother fibromas elsewhere.Numerous authors (Stout and Murray, 1942;
Stout and Himadi, 1951; Benoit and Ackerman,1953; Bilesio, Villamil, Gambarini, and Pasquini,1958) consider fibrous tumours localized to thepleura as benign localized mesotheliomas, con-ceding that they derive from the mesotheliumand that notwithstanding their benign fibrousappearance they are capable of malignant trans-formation, as shown by malignant change in some.It is possible to distinguish two types of pleuralfibroma, depending on which of the histologicalstructures of the pleura they originate from-themesothelium or the pleural connective vasculartissue (Bracco, 1964). The former would retain itspotential for malignant transformation, while thelatter would remain benign, as any fibromaoriginating in the connective tissue elsewhere inthe body. In our case, all the tumours resectedduring a 25-year period showed a benign fibro-matous nature and the tolerance of the patientto the tumour seems to confirm its overall benignnature.
FIG. 6. Chest radiographoper-ation.
785
-I.-*A;
":'L.'..
:."-, .
AVk; iw`:: .0
copyright. on F
ebruary 8, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.28.6.782 on 1 Novem
ber 1973. Dow
nloaded from

C. M. Scattini and A. Orsi
Most pleural tumours are discovered at routineradiography (Galy, 1961). If on account of theirsize or location these tumours produce symptoms,the symptomatology is in general insidious. Painis the most frequent symptom (64% in the casesrecorded by Biehl (1957)) and its location corre-sponds to where the tumour is located. Dyspnoeaoccurs in 50% and cough in 35 % of cases. Thedyspnoea is generally related to the size of thetumour and the cough is generally dry, of anirritating type, though haemoptysis may rarelyoccur. In some cases, especially when mediastinalcompression occurs from large tumours, cyanosis,collateral circulation, and oedema may appear(Temple and Jones, 1954). In this event the bariumswallow shows extrinsic compression of the oeso-phagus, though the patient may not complain ofdysphagia. At surgery, compression of the uppervena cava by the tumour can be verified. Clagett,McDonald, and Schmidt (1952) found hyper-trophic pulmonary osteoarthropathy in 16 of 24cases of localized pleural mesotheliomas. Theyconsider this to be a characteristic, and in somecases found a remarkable improvement of theosteoarthropathy following resection of thetumour.The radiological appearances of pleural fibromas
vary according to the location and size of thetumours. Generally they tend to be round, dis-crete, and of a uniform density. The differentialdiagnosis includes hydatid cysts, bronchial car-cinoma, and loculated pleural collections. In ourcase, in the presence of multiple lung shadows, themost likely diagnosis was hydaltid cysts (particu-larly in South America) or pulmonary metastasisfrom an extrapulmonary tumour. Nevertheless, thefact that the patient had been operated on manyyears before and a pleural fibroma found, andalso that in a previous operation the existence ofmultiple pleural fibromas had been verified,suggested that the new radiological shadows werepleural fibromas. Moreover, the radiographic andtomographic studies performed showed that allthe tumours were in close contact with the pleuralsurface and in no case isolated in the depth ofthe pulmonary parenchyma.
In our case, each of the tumours surgicallyresected had developed from the visceral pleuraalthough some had grown into the lung. Tumoursarising from the visceral pleura are more likelyto be benign than those arising from the parietalpleura (Friedman, 1950).Each tumour was well encapsulated, which per-
mitted easy enucleation. Histologically they showeda monoformic proliferation of connective tissueelements surrounded by fascicles of collagen-
reticular fibres with some areas of extensivemucoid degeneration. The existence of numerousmitoses explains the active growth of thesetumours and does not constitute evidence ofmalignancy in this patient, but in other cases theexistence of mitoses may constitute a sign ofmalignancy.
In the patient's last two operations both pleuraswere thoroughly explored and every small tumourthat could be seen was resected. However, onecannot say that exploration was complete becauseaccess to the mediastinal pleura was difficult andbecause small tumours not detectable macro-scopically could have been overlooked.The possibility that new tumours will appear
still exists. The prognosis of this patient, even ifnew tumours appear, is considered to be favour-able because over a period of 25 years thesetumours have invariably been histologically benignfibromas.
REFERENCESBenoit, H. W. and Ackerman, L. V. (1953). Solitary pleural
mesotheliomas. Journal of Thoracic Surgery, 25, 346.Biehl, F. (1957). Contribution A 1'etude des tumeurs primi-
tives de la plevre. Thesis, University of Nancy.Bilesio, E. A. Villamil, E. F. J., Gambarini, A., and Pasquini,
A. T. (1958). Fibromesotelioma solitario de pleuraparietal. La Prensa Medica Argentina, 45, 1343.
Boyd, W. (1966). The Spontaneous Regression of Cancer.Thomas, Springfield, Illinois.
Bracco, A. N. (1964). Mesoteliomas malignos de la pleura.Revista de la Asociacion Medica Argentina, 78, 74.
Clagett, 0. T., McDonald, J. R., and Schmidt, H. W.(1952). Localized fibrous mesothelioma of the pleura.Journal of Thoracic Surgery, 24, 213.
Decroix, G. and Pieron, R. (1963). Contribution a l'etudedes fibromes de la plevre. Bulletins et Menioires le laSociete Medicale des H6pitaux de Paris, 114, 97.
Even, R. and Sors, C. (1959). Les mesotheliomes. Essai declassification anatomo-clinique des tumeurs pleuralesprimitives. Presse Medicale, 67, 2058.
Everson, T. C. and Cole, W. H. (1959). Spontaneous regres-sion of malignant disease. Journal of the AnzericanMedical Association, 169, 1758.
Friedman L. L. (1950). Tumors of the pleura. Diseases ofthe Chest, 17, 756.
Galy, P. (1961). Le diagnostic des tumeurs pleurales primi-tives ou soit-disant telles. Journal de MeWdecine deBordeaux, 138, 1261.
Halperin, A., Bilesio, E. A., and Orlando, E. A. (1955).Fibromesotelioma solitario de pleura visceral. PrensaMe'dica Argentina, 42, 1031.
Huguenin-Dumittan, S. A., Mach, R. S., and Press, P.(1968). Fibro-mesotheliome 'benin'. Schwveizerischemedizinische Wochenschrift, 98, 1368.
Kerr. W. F. and Nohl, H. C. (1961). Recurrence of 'benign'intrathoracic fibromas. Tho,ax, 16, 180.
786
copyright. on F
ebruary 8, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.28.6.782 on 1 Novem
ber 1973. Dow
nloaded from

Multiple bilateral fibromas of the pleura
Sen, P. K., Parulkar, G. B., Kinare, S. G., and Gandhi, R. K. , and Murray, M.(1964). Giant pleural fibroma. British Journal of Surgery, thelioma. Archives51, 636.
Stout, A. P., and Himadi, G. M. (1951). Solitary (localized) Temple, L. J. and Jon(mesothelioma of pleura. Annals of Surgery, 133, 50. intrathoracic fibror
787
. R. (1942). Localized pleural meso-of Pathology, 34, 951.
Les, G. P. (1954). Two cases of giantma. Thorax, 9, 112.
copyright. on F
ebruary 8, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.28.6.782 on 1 Novem
ber 1973. Dow
nloaded from