Embed Size (px)
Citation preview

Volume 16 - N
umber 1-2 - A
pril 2021M
ultid
isciplin
ary Resp
iratory M
edicin
e
Abstracted/Indexed in: PubMed, PubMed Central, Embase, ESCI, Academic Search, DOAJ, EBSCO, Google Scholar, OCLC, SCImago, Summon and SCOPUS
Volume 16 - Number 1-2 - April 2021
Editor-in-ChiefC.M. Sanguinetti
In PubMed
Central
Cite score 2018 2.21
SJR value 2018 0.7
SNIP 2018 1.139
M. Heim, T. Lahmer, S. Rasch, S. Kriescher, W. Berg-Johnson, K. Fuest, B. Kapfer, G. Schneider, C.D. Spinner, F. Geisler, J.R. Wießner, K. Rothe, S. Feihl, A. RanftRapid clinical evolution for COVID-19 translates into early hospital admission and unfavourable outcome: a preliminary report
J. Hunt, K.M. Chapple, A. Nasar, L. Cherrier, R. WaliaEfficacy of low-dose valganciclovir in CMV R+ lung transplant recipients: a retrospective comparative analysis
M. Povero, P. Turco, L. Bonadiman, R.W. Dal NegroThe Global Usability Score Short-Form for the simplified assessment of dry powder inhalers (DPIs) usability
N. Tani, N. Kataoka, Y. Kunimatsu, Y. Tachibana, T. Sugimoto, I. Sato, Y. Ogura, K. Hirose, T. TakedaEarly responders within seven days of dupilumab treatment for severe asthma evaluated by patient-reported outcome: a pilot study
R. Jaques, A. Shakeel, C. HoyleNovel therapeutic approaches for the management of cystic fibrosis
A. KantarWhat makes flunisolide different among inhaled corticosteroids used for nebulization: a close look at the role of aqueous solubility
A. Mohr, L. Dannerbeck, T.J. Lange, M. Pfeifer, S. Blaas, B. Salzberger, F.Hitzenbichler, M. KochCardiopulmonary exercise pattern in patients with persistent dyspnoea after recovery from COVID-19
Multidisciplinary Respiratory Medicine
Official Journal of IRS Research CenterRivista ufficiale di Centro Studi SIP

AIMS AND SCOPEMultidisciplinary Respiratory Medicine is a peer-reviewed, open access journal encompassing all aspects of respiratory medicine. It has a particular focus on interdisciplinary and translational research. Multidisciplinary Respiratory Medicine is published online at http://www.mrmjournal.org. The journal aims to provide a forum for the publication and free access of high quality original scientific articles, reviews and position papers documenting clinical and experimental advances in respiratory medicine, and related fields.Given the journals interdisciplinary character, the target readership is wider than respiratory medicine, embracing numerous related disciplines (allergology, immunology, internal medicine, geriatrics, infectious diseases, intensive care, etc) and health professionals.
COPYRIGHT AND LICENSE AGREEMENTAll articles published on the online version by Multidisciplinary Respiratory Medicine are made freely and permanently accessible online immediately upon publication, without subscription charges or registration barriers at http://www.mrmjournal.org. Further information about open access can be found at https://pagepress.org/index.php/pagepress/openaccess.Authors of articles published on the online version of the Journal are the copyright holders of their articles and have granted to any third party, in advance and in perpetuity, the right to use, reproduce or disseminate the article, according to the journal’s copyright and license agreement (see https://www.mrmjournal.org/mrm/copy for more information).
PRODUCTION ONLINE VERSIONPAGEPress PublicationsVia A. Cavagna Sangiuliani 527100 Pavia, ItalyTel.: +39-0382-464340Fax: +39-0382-34872www.pagepress.orge-mail: [email protected] or [email protected]
PRODUCTION PRINT VERSION AND ADVERTISINGNovamedia SrlVia M. della Libertà 528041 Arona (NO), ItalyTel.: +39-345-5099724e-mail: [email protected]
EDITORIAL OFFICELilia GianniniVia Martiri della Libertà 5, 28041 Arona (NO), ItalyTel.: +39-345-5099724 - Fax: +39-0322-072069e-mail: [email protected]
MANAGING DIRECTOR – DIRETTORE RESPONSABILEClaudio M. Sanguinetti, Rome, Italy
SUBSCRIPTION INFORMATIONAnnual subscription rate for the print version (3 issues plus eventual supplements) € 90.00.For further information, contact Novamedia srl,tel. +39-345 5099724, [email protected] 1828-695X
INFORMATION TO THE READERNotification in accordance to the General Data Protection Regulation (EU) 2016/679 (GDPR). Subscribers’ information is utilized, also in electronic mode, for the purpose of journal delivery as required and for related activities. Data treatment is owned by Novamedia Srl, M. della Libertà 5, 28041 Arona (NO), Italy. The categories of persons responsible for data treatment for the above purpose are those involved in the registration, modification, elaboration and printing of data, in the production and delivery of the journal, in the call centers, and in the administration and economic management. As at the General Data Protection Regulation (EU) 2016/679 (GDPR), it is possible to exercise one’s right to consult, modify, update or cancel one’s information by applying to Novamedia srl, at the above address, who, on request, will provide a list of the responsible persons.
TYPESETTERMadison, Milan, Italy
PRINTERLa Terra Promessa Scs, Novara, Italy
Registered at the Court of Novara n. 120/05 on 11/11/05.Distribution in Italy occurs according to the General Data Protection Regulation (EU) 2016/679 (GDPR).
OWNERSHIPNovamedia Srl, Via M. della Libertà 5, 28041 Arona (NO), Italy
Multidisciplinary Respiratory Medicine
Official Journal of IRS Research CenterRivista ufficiale di Centro Studi SIP

Editor-in-Chief Claudio M Sanguinetti Quisisana Clinical Center, Rome, Italy
Associate Editors Coordinator:Stefano Nardini Vittorio Veneto General Hospital, Vittorio Veneto, Italy
• Nicolino Ambrosino ICS Maugeri, Montescano, Italy • Isabella Annesi-Maesano Institut National de la Santé et
de la Recherche Médicale, Paris, France• Heinrich Becker University of Heidelberg, Heidelberg, Germany• Roberto W. Dal Negro National Centre for Respiratory
Pharmacoeconomics & Pharmacoepidemiology, Verona, Italy• Günseli Kilinc University of Istanbul, Istanbul, Turkey • Stefano Marinari SS. Annunziata Hospital, Chieti, Italy • Carlo Mereu Santa Corona Hospital, Pietra Ligure, Savona, Italy • Antonio Sanna San Jacopo Hospital, Pistoia, Italy
Editorial Board Coordinator:Mario Polverino High Specialty Regional Centre, Salerno, Italy
• Marco Alifano Paris Descartes University, Paris, France• Alvar Augusti University of Barcelona, Barcelona, Spain• Giorgio Bertolotti Scientific Institute of Tradate, Tradate, Italy• Surinder S Birring King’s College Hospital, London, UK• Pierre-Régis Burgel Cochin Hospital, Paris, France• Walter G. Canonica University of Genoa, Genoa, Italy • Stefano Carlone San Giovanni-Addolorata General Hospital,
Rome, Italy• Richard Casaburi UCLA Medical Center, Los Angeles, USA• Lucio Casali University of Perugia, Perugia, Italy • Ciro Casanova University “La Laguna”, Santa Cruz de Tenerife, Spain• Bartolome Celli Brigham and Women’s Hospital, Boston, USA • Alexander A Chuchalin Russian Medical State University, Moscow,
Russian Federation • Peter A. Cistulli University of Sidney, Sidney, Australia• Bruno Crestani Université de Paris, Inserm U1152, Paris, France• Claudia Crimi AOU Vittorio Emanuele Hospital, Catania, Italy• Giacomo Cusumano Vittorio Emanuele Hospital, Catania, Italy • Gennaro D’Amato A. Cardarelli Hospital, Naples, Italy • Fernando De Benedetto University of Chieti, Chieti, Italy• Juan Pablo de Torres Tajes Clinica Universidad de Navarra,
Pamplona, Spain• Mario Del Donno University “Federico II”, Naples, Italy• Peter Dicpinigaitis Albert Einstein College of Medicine,
New York, USA• Miguel Divo Brigham and Women’s Hospital, Boston, USA
• Claudio F. Donner Mondo Medico Clinic, Borgomanero, Italy• Emmi Lorenzo University of Florence, AOU Careggi, Florence, Italy• Andrew Farmer University of Oxford, Oxford, UK• Alessandro Fois University of Sassari, Sassari, Italy• Roger Goldstein University of Toronto, Toronto, Canada • Stefano Guerra University of Arizona, Tucson, USA• Peter Howard University of Sheffield, Sheffield, UK • Arturo H. Huerta Garcia Hospital Clinic de Barcelona,
Barcelona, Spain• Marc Humbert Université Paris-Sud, Paris, France• Ahmad Kantar Pediatric Asthma and Cough Center,
Ponte San Pietro, Italy• José Ma Marin University of Zaragoza, Zaragoza, Spain• Fernando J Martinez Weill Cornell Medical College, New York, USA• Alyn H. Morice University of Hull, Cottingham, UK• Margherita Neri Renato Piatti Onlus, Varese, Italy • Luis VF Oliveira University Center of Anápolis, Anápolis, Brazil• Fabio Pace Bolognini Hospital, Seriate, Italy• Paolo Palange Sapienza University, Rome, Italy• Martyn R Partridge Imperial College London, UK• Riccardo Pela C. e G. Mazzoni Hospital, Ascoli Piceno, Italy • Massimo Pistolesi AOU Careggi, Florence, Italy• Eva Polverino Hospital Universitari Vall d’Hebron, Barcelona, Spain• Francesca Polverino University of Arizona, Tucson, USA• Stephen I Rennard University of Nebraska, Omaha, USA• Josep Roca Institut d’Investigacions Biomèdiques August Pi i Sunyer,
Barcelona, Spain • Yogesh Saini University of North Carolina, Chapel Hill, USA • Sundeep Salvi Chest Research Foundation, Pune, India• Gianfranco Sevieri Viareggio, Lucca, Italy • Joan B. Soriano Universidad Autónoma de Madrid, Madrid, Spain • Samy Suissa McGill University, Montreal, Canada • Martin Tobin University of Chicago, Maywood, USA• Philip Tǿnnesen Gentofte University Hospital, Copenhagen, Denmark• Domenico M. Toraldo “V Fazzi” Hospital, Lecce, Italy• Hoi Nam Tse Hong Kong Baptist Hospital, Hong Khong, China• Giovanni Viegi National Research Council, Institute of Biomedicine
and Molecolar Immunology A. Monroy, Palermo, Italy • Jadwicha Wedzicha University College London, London, UK• Robert West University College, London, UK• Emiel FM Wouters University Hospital Maastricht, Mastricht,
Netherlands • Alessandro Zanasi Italian Association for Cough Study (AIST),
Bologna, Italy• Salah Zeineldine American University of Beirut, Beirut, Lebanon• Richard Zuwallack University of Connecticut, Hartford, USA
Managing Editor Lilia Giannini Editorial Office. Arona, Italy
Multidisciplinary Respiratory Medicine

70MRM
Campagna 5x1000 anno 2021

3MRM
Congress report
Original research articlesRapid clinical evolution for COVID-19 translates into early hospital admission and unfavourable outcome: a preliminary report 5Markus Heim, Tobias Lahmer, Sebastian Rasch, Silja Kriescher, Wiebke Berg-Johnson, Kristina Fuest, Barbara Kapfer, Gerhard Schneider, Christoph D. Spinner, Fabian Geisler, Johannes R. Wießner, Kathrin Rothe, Susanne Feihl,Andreas Ranft
Early responders within seven days of dupilumab treatment for severe asthma evaluated by patient-reported outcome: a pilot study 12Nozomi Tani, Nobutaka Kataoka, Yusuke Kunimatsu, Yusuke Tachibana, Takumi Sugimoto, Izumi Sato, Yuri Ogura, Kazuki Hirose, Takayuki Takeda
Efficacy of low-dose valganciclovir in CMV R+ lung transplant recipients: a retrospective comparative analysis 20Jessica Hunt, Kristina M. Chapple, Aasya Nasar, Lauren Cherrier, Rajat Walia
The Global Usability Score Short-Form for the simplified assessment of dry powder inhalers (DPIs) usability 26Massimiliano Povero, Paola Turco, Luca Bonadiman, Roberto W. Dal Negro
Respiratory symptoms and associated risk factors among under-five children in Northwest, Ethiopia: community based cross-sectional study 33Zewudu Andualem, Asefa Adimasu Taddese, Zelalem Nigussie Azene, Jember Azanaw, Henok Dagne
Primary care management of allergic rhinitis: a cross-sectional study in four ASEAN countries 41Baharudin Abdullah, Kornkiat Snidvongs, Marysia Recto, Niken Lestari Poerbonegoro, De Yun Wang
Value of modified Burns Wean Assessment Program scores in the respiratory intensive care unit: an Egyptian study 49Nermeen A. Abdelaleem,Sherif A.A. Mohamed, Azza S. Abd ElHafeez, Hassan A. Bayoumi
ReviewsNovel therapeutic approaches for the management of cystic fibrosis 56Ryan Jaques, Arslan Shakeel, Cameron Hoyle
What makes flunisolide different among inhaled corticosteroids used for nebulization: a close look at the role of aqueous solubility 71Ahmad Kantar
INDEX

4MRM
Index
Short reportCardiopulmonary exercise pattern in patients with persistent dyspnoea after recovery from COVID-19 79Arno Mohr, Laura Dannerbeck, Tobias J. Lange, Michael Pfeifer, Stefan Blaas, Bernd Salzberger, Florian Hitzenbichler, Myriam Koch
RubricheL’angolo della Cultura (non solo Medicina…) L’eterna giovinezza del Circolo Pickwick IFrancesco Iodice
Meeting calendar IV

5MRM
Rapid clinical evolution for COVID-19 translates into early hospital admission and unfavourable outcome: a preliminary reportMarkus Heim,1 Tobias Lahmer,2 Sebastian Rasch,2 Silja Kriescher,1 Wiebke Berg-Johnson,1 Kristina Fuest,1 BarbaraKapfer,1 Gerhard Schneider,1 Christoph D. Spinner,2,3 Fabian Geisler,2 Johannes R. Wießner,2Kathrin Rothe,4 Susanne Feihl,4 Andreas Ranft1
1Department of Anaesthesiology and Intensive Care Medicine, University hospital rechts der Isar, Technical University of Munich,School of Medicine, Munich2Department of Internal Medicine II, University hospital rechts der Isar, Technical University of Munich, School of Medicine, Munich3German Centre for Infection Research (DZIF), Partner Site Munich, Munich 4Institute for Medical Microbiology, Immunology and Hygiene, Technical University of Munich, School of Medicine, Munich,Germany
Background: A wide range of mortality rates has been reported in COVID-19 patients on the intensive care unit. Wewanted to describe the clinical course and determine the mortality rate in our institution’s intensive care units. Methods: To this end, we performed a retrospective cohort study of 50 COVID-19 patients admitted to the ICU at alarge German tertiary university hospital. Clinical features are reported with a focus on ICU interventions, such asmechanical ventilation, prone positioning and extracorporeal organ support. Outcome is presented using a 7-pointordinal scale on day 28 and 60 following ICU admission. Results: The median age was 64 years, 78% were male. LDH and D-Dimers were elevated, and patients were low onVitamin D. ARDS incidence was 75%, and 43/50 patients needed invasive ventilation. 22/50 patients intermittentlyneeded prone positioning, and 7/50 required ECMO. The interval from onset of the first symptoms to admission to thehospital and to the ICU was shorter in non-survivors than in survivors. By day 60 after ICU admission, 52% of thepatients had been discharged. 60-day mortality rate was 32%; 37% for ventilated patients, and 42% for those requiringboth: ventilation and renal replacement therapy. Conclusions: Early deterioration might be seen as a warning signal for unfavourable outcome. Lung-protective ven-tilation including prone positioning remain the mainstay of the treatment.
Key words: COVID-19; SARS-CoV-2; critical care; mortality; acute respiratory distress syndrome; prone position;invasive ventilation; retrospective cohort study.
AB
STR
ACT
Correspondence: Dr. med. Markus Heim, Technical University of Munich, School of Medicine, University Hospital rechts der Isar,Department of Anaesthesiology and Intensive Care Medicine, Ismaninger Str. 22, 81675 Munich, Germany. Tel. +49.89.41405990 - Fax: +49.89.41404804. E-mail: [email protected]
Contributions: MH, AR, conception and design, analysis and interpretation of data, drafting the article, final approval of the versionto be published, agreement to be accountable for all aspects of the work; TL, SR, SK, WBJ, KF, BK, GS, CDS, FG, JRW, KR, SF,analysis and interpretation of data, revising the article for important intellectual content, final approval of the version to be published,agreement to be accountable for all aspects of the work.
Conflict of interest: Susanne Feihl reports personal fees and non-financial support from Smith and Nephew, personal fees and non-financial support from Curetis, personal fees and non-financial support from Zimmer Biomet, personal fees and non-financial supportfrom Limbach, personal fees and non-financial support from MSD, outside the submitted work; Sebastian Rasch reports travel-grantsfrom Gilead, outside the submitted work. Christoph D. Spinner reports grants from Aperion, grants and personal fees from GileadSciences, grants and personal fees from MSD, grants and personal fees from GSK/ViiV Healthcare, grants and personal fees fromJanssen-Cilag, personal fees from Molecular Partners, personal fees from Formycon, from null, outside the submitted work. All otherauthors (Wiebke Berg-Johnson; Kristina Fuest; Fabian Geisler; Markus Heim; Barbara Kapfer; Silja Kriescher; Tobias Lahmer; KathrinRothe; Gerhard Schneider; Johannes R. Wießner) have no conflict of interest to disclose.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Availability of data and materials: The complete anonymised set of individual patient data is available from the authors upon request.
Ethics approval and consent to participate: The Ethics Committee of the Technical University of Munich approved this retrospectivestudy (approval no. 723/20 S-SR).
ORIGINAL RESEARCH ARTICLE
®Multidisciplinary Respiratory Medicine 2021; volume 16:744
MRM_02 original.qxp_Hrev_master 02/04/21 11:10 Pagina 33

6MRM
Multidisciplinary Respiratory Medicine 2021; 16:744 - M. Heim et al.
IntroductionThe coronavirus disease 2019 (COVID-19) outbreak, with its
beginning in Wuhan in December 2019, led into a pandemic.While most patients develop mild or uncomplicated illness, otherrequire hospitalisation, and of these about 15% need treatment onan intensive care unit (ICU) [1]. Complications such as acute res-piratory distress syndrome (ARDS), sepsis, and multiorgan failurecan occur [1-3]. With continuously growing knowledge about thepathogen, its transmission and the manifestations of this new dis-ease, widely varying mortality rates have been reported. Reportedclinical data are heterogeneous with respect to the number ofpatients treated and also the censoring day to determine outcome.For instance, in a cohort of 52 patients on a single ICU in Wuhan,the 28-day mortality rate was 62%, and up to 74% if ARDS waspresent [4]. Early reports from smaller cohorts in Seattle (WA,USA) showed ICU mortality rates between 50% (12 of 24 patients)and 67% (14 of 21 patients) rising up to 75% in patients on inva-sive ventilation [5,6]. These mortality rates for severe acute respi-ratory syndrome coronavirus 2 (SARS-CoV-2) induced ARDS aresignificantly higher than those in the ‘LUNG SAFE’ study fromthe pre COVID-19 era, which presented hospital mortality ratesbetween 35% and 46% depending on the severity of ARDS [7]. Incontrast, an in-hospital mortality of 36% (59 of 165 patients) wasreported from Atlanta (GA, USA) [8]. It is widely acknowledgedthat mortality in critically ill patients is associated with the severityof illness on arrival to the ICU and the need for interventions suchas mechanical ventilation, renal replacement therapy and vasopres-sor support [9,10]. Likewise, older age and the presence of comor-bidities worsen outcome [4,11,12]. In COVID-19 patients, thepresence of chronic lung diseases like asthma or chronic obstruc-tive pulmonary disease (COPD), as well as obesity and persistingelevation of infection parameters are associated with an increasedlikelihood to develop ARDS [3].
The aim of our study was to characterise the COVID-19 ICUpatients treated in our university hospital, to describe the interven-tions and the outcomes, and to identify differences betweenpatients that had survived and those who had died until day 60 afterICU admission.
MethodsWe performed a retrospective single-centre cohort study of 50
adult patients with confirmed COVID-19 during the first pandemicwave, admitted to the ICU between 11 March and 24 April 2020.Patients were treated on two different intensive care units in a uni-versity hospital with 1,163 beds, one affiliated to the department ofinternal medicine II and one to the department of anaesthesiologyand intensive care medicine.
The Ethics Committee of the Technical University of Munichapproved this retrospective study (approval no. 723/20 S-SR).
Medical records including clinical charts and nursing recordswere reviewed. Data collection included patient biometrics,comorbidities, clinical parameters, laboratory findings, informa-tion on inpatient management, ICU interventions, as well as ICUand hospital stay. On day 28 and day 60 from ICU admission, out-come was measured with a 7-point ordinal scale from category 1(not hospitalized with no limitations on activities) to category 7(dead) as used before [13].
Laboratory confirmation of SARS-CoV-2 was achieved bypolymerase chain reaction (PCR) of respiratory swabs or combina-tion of IgG/IgM-seropositivity and COVID-19 symptoms. Details
to the PCR and serological testing methods are published else-where [14]. Additionally, a chest computed tomography (CT) scanwas performed for nearly all patients (48/50) to identify typical CTfindings for COVID-19 [15,16]. Patients with positive PCR or pos-itive IgM/IgG serology results were defined as definite COVID-19cases. Patients with suspected disease in whom diagnosis could notbe confirmed were excluded from the analysis.
Continuous data are described by median (interquartile rangefrom quartile 25% to quartile 75%), and categorical data by abso-lute and relative frequencies. Data were analysed using a chi-square or Wilcoxon rank-sum test for categorical and continuousvariables, respectively, with a two-sided p-value of less than 0.05considered statistically significant. Due to the exploratory natureof the study, uncorrected p-values are reported. Statistical analyseswere performed using Microsoft Excel 2013 and IBM SPSSStatistics ver. 25.0 (IBM Corp, Armonk, NY). The completeanonymised set of individual patient data is available from theauthors upon request.
Medical recordsIn March and April 2020, 50 adult patients with a confirmed
diagnosis of COVID-19 were admitted to ICU in our universityhospital. Comprehensive datasets containing clinical and laborato-ry parameters were compiled from these cases. Thirty-threepatients (66%) had initially been treated on the normal ward beforetransfer to the ICU, 17 patients (34%) were assigned directly to theICU via the emergency department. At the time of symptom onset,6 patients (12%) were in hospital for a diagnosis other thanCOVID-19. Oxygen therapy was started when SpO2 droppedbelow 94%. All COVID-19 patients received respiratory therapyby a physiotherapist at least once daily. According to our standardoperating procedure for COVID-19 patients, the need for intensivecare was discussed when the respiratory rate rose above 30 per minand SpO2 fell below 90% at an oxygen flow rate of 8 L/min by facemask. An overview of the variables not presented in Tables 1 and2 can be found the Tables S1 to S4 in the Supplementary Material.Presence of SARS CoV-2 was proven by PCR in 47 cases. In 42out of 44 cases, serologic testing (IgG and IgM) indicated SARS-CoV-2 infection, including all three cases with negative PCR.Imaging findings were consistent with COVID-19 in all patientsreceiving a chest-CT scan (n=48).
Patient characteristicsThe median age in the whole cohort was 64 (range, 26-96)
years. Seventy-eight percent (39/50) of patients were male. In tenpatients (20%), no prior comorbidity was documented. At least oneunderlying comorbidity was present in 38/50 patients (76%), witharterial hypertension being the most frequent (in 56%). Three ormore comorbidities were present in 36% of all patients (supple-mentary Table S1). The distribution of blood groups in the ABOsystem was similar between survivors and non-survivors, withcomparable proportions of group O.
After a median of four days (1-7) after onset of symptoms,patients were admitted to hospital, and one day (0-3) later, trans-ferred to ICU. On admission to the ICU, sepsis-related organ fail-ure assessment score (SOFA) score was six (3-10) and acute phys-iology and chronic health evaluation score (APACHE) was 18 (14-26). The majority of patients (92%) was lymphopenic, and allshowed elevated LDH and D-dimers. Median concentration ofvitamin D (25-OH-vitamin D3) was 14 ng/mL; more than threequarters of our patients were low on vitamin D (£30 ng/mL), and42% presented a manifest deficiency (threshold, 12 ng/mL).Hypalbuminaemia (£3.5 g/dL) was found in 70%, with a median of3.0 g/dL. Leukocytes, PCT and interleukin-6 did not show a
MRM_02 original.qxp_Hrev_master 02/04/21 11:10 Pagina 34

7MRM
Multidisciplinary Respiratory Medicine 2021; 16:744 - M. Heim et al.
notable elevation. For four selected timepoints during the ICU stay(on day of admission, intubation, first proning and extracorporealmembrane oxygenation (ECMO) initiation), no significantchanges in the laboratory parameters (leukocytes, CRP, Il6, PCT,LDH and D-dimer) could be detected. Median time to first nega-tive PCR was 16 days (10-22). Patient characteristics and initiallaboratory data are shown in Table 1 and supplementary Table S1,course of laboratory data are shown in Supplementary Table S2.
Treatment and course of diseaseNon-invasive ventilation (NIV) or high flow nasal oxygen
therapy (high flow nasal oxygen, HFNO) was used in four casesbut could not obviate the need for subsequent endotracheal intuba-tion. 43 (86%) of the patients received invasive ventilation. Inmore than 90%, the Berlin criteria for diagnosis of ARDS were meton day of intubation, with 65% (n=28) categorized as moderate orsevere with a median Horovitz index (HI) of 160 mmHg (113-216)[17]. On the day after intubation, there was no relevant change inseverity of ARDS. After intubation, the median peak airway pres-sure was 25 mbar, with a median positive endexpiratory pressure(PEEP) of 10 mbar which was largely maintained on this leveluntil the next day. Half of the ventilated patients (n=22) neededprone positioning at a median HI of 87 mmHg (72-107). Duringthe first proning period (approximately 16 hours) the achievedaverage HI was 135 mmHg (115-155), a clinically relevant and sta-tistically significant increase (p£0.01) (Figure 1). After a median ofnine days (6-11) on invasive ventilation, seven patients underwentveno-venous ECMO. On day of ECMO initiation, the medianSOFA score was 10 (10-11).
During hospital stay, nine patients of our ICU cohort receivedremdesivir within clinical studies or early access programs, and sixpatients received convalescent plasma. Dexamethasone (or anyother glucocorticoid) were not administered routinely, as no gener-al recommendation was available at the time of the study period.In our hospital, lopinavir/ritonavir, chloroquine or hydroxychloro-
Table 1. Demographic characteristics and laboratory findings on ICU admission.
Characteristics, median (IQR) All (n=50) Survivors* (n=34) Non–survivors* (n=16) p°
Age 64 (53–77) 59.5 (53–75) 71 (54–81) 0.174Male sex, n (%) 39 (78) 26 (76) 13 (81) 1.0SOFA 6 (3–10) 6 (3–10) 7 (4.5–10.5) 0.5552Apache II 18 (14–25.5) 17 (14–23) 21 (14.5–34.5) 0.215Comorbidities
None, n (%) 10 (20) 8 (23.5) 2 (12.5) 0.4684Any, n (%) 38 (76) 25 (73.5) 13 (81.3) 0.7278≥3, n (%) 18 (36) 13 (38.2) 5 (31.3) 0.7568Laboratory findings on ICU admission
Leucocytes (G/L) 7.93 (5.9–10.9) 7.92 (6.02–10.77) 8.79 (4.97–11.61) 0.6527Lymphocytes (% of Leucs) 9 (5–13) 9 (7–12) 8 (4–14.5) 0.984CRP (mg/dL) 13.65 (8.6–20.6) 15.1 (10.4–21) 10.3 (7.3–17.8) 0.7114Il6 (pg/mL) 135 (89–195) 135 (85–193) 133 (118–193) 0.3125PCT (ng/mL) 0.3 (0.1–0.9) 0.3 (0.2–1.4) 0.3 (0.1–0.8) 0.5093D-Dimer (µg/L FEU) 1983 (982–6614) 2023.5 (983–6578) 1983 (1093–6640) 0.9442LDH (U/L) 468 (340–592) 468 (355–573) 471 (319–713.75) 0.8026Albumin (g/dL) 3 (2.6–3.5) 3 (2.7–3.5) 3.1 (2.6–3.8) 0.502925-OH-Vitamin D3 (ng/mL) 14 (8.5–26.5) 14 (8–27) 13 (10.25–19.5) 0.7642
*Until outcome day 60 from ICU admission; °Chi Square or Wilcoxon rank-sum test comparing those who survived vs died up to day 60 from ICU admission.
Table 2. Outcome on day 28 and 60 after ICU admission.
Scale Description Day 28 Day 60value n (%) n (%)
1 Not hospitalized, no limitation on activities 6 (12) 10 (20)2 Not hospitalized, limitation on activities 11 (22) 16 (32)3 Hospitalized, not requiring supplemental oxygen 3 (6) 1 (2)4 Hospitalized, requiring supplemental oxygen 3 (6) 3 (6)5 Hospitalized, on non-invasive ventilation or high flow 2 (4) 0 (0)6 Hospitalized, on invasive ventilation or ECMO 14 (28) 4 (8)7 Dead 11 (22) 16 (32)
Figure 1. Oxygenation (expressed as Horovitz Index) on day ofintubation (‘ITN’, n=43), one day later (‘ITN +1’, n=39), beforeproning (prone -1, n=20), and in prone position (prone, n=20,average of repeated measurements). In prone position, oxygena-tion improved significantly (prone -1 vs prone, p<0.0001,Wilcoxon matched-pairs signed rank test). Box and whiskers aremedian, lower/upper quartile, and 1.5 times interquartile range.
MRM_02 original.qxp_Hrev_master 02/04/21 11:10 Pagina 35

8MRM
Multidisciplinary Respiratory Medicine 2021; 16:744 - M. Heim et al.
quine were used for potential treatment of COVID-19. 84% of allpatients needed vasopressor support. 20 patients (40%) underwentrenal replacement therapy (Supplementary Table S4). As describedrecently, severe bacterial and fungal co-infections were rare in ourcohort [14]. During their hospital stay, 48 patients (96%) weretreated with antibiotics. Bloodstream infections on the day ofadmission were rare and could be detected in a total of 14 patients(28%) during the course of intensive care therapy. For preventionof thromboembolism, all patients received low-molecular-weightheparins in double prophylactic dosage, with the exception ofpatients for whom therapeutic anticoagulation was indicated (e.g.,due to ECMO therapy).
ResultsMedian length of stay on the ICU was 17 days (9-38).
Ventilated patients spent 19 days (11-42) on the ICU with an aver-age time on the ventilator of 18 days (6-11). Among the 31 patientsthat could be discharged from the ICU, 22 were transferred to aregular ward, 4 were transferred to another ICU or a weaning facil-ity, 4 to rehabilitation centre, and 1 patient could return home. Onday 60, 52% of our patients (n=26) had been discharged home, and38% of them (n=10, a fifth of the whole cohort) reported no limi-tations on activities. Four (8%) patients were still on ICU on day60, one of them still being on ECMO. Sixty-day mortality rate was
32% for all patients, 37% for the patients on ventilator and 42% forpatients requiring both mechanical ventilation and renal replace-ment therapy. Four of seven patients treated with ECMO died,three of them due to fatal intracerebral haemorrhage. One patientwas still on ECMO on day 60 (Table 2).
Factors associated with adverse outcome in COVID-19 haverepeatedly been described, among them, age, obesity and comor-bidities [18,19]. For further exploratory analysis, we divided ourcohort into two subgroups: Patients who survived (n=34) or died(n=16) up to day 60 after ICU admission. Between these groups,age, body mass index and number of comorbidities did not differsignificantly. A large proportion of survivors (76%) and all (100%)non-survivors needed vasopressor support (p=0.04). Patients notsurviving to day 60 after ICU admission received dialysis morefrequently (50% vs 35%), although this was not statistically signif-icant. Counted from the first onset of symptoms, non-survivorswere admitted earlier than survivors – both to hospital and to ICU(Figure 2 A,B and Supplementary Table S3), and this differencewas statistically significant (hospital admission: 1.5 vs 4.5 days,p£0.01, ICU admission: 4 vs 8 days, p£0.01). The in-house interval‘from door to ICU’ however, did not differ. None of the laboratoryresults on day of admission to the ICU was associated with sur-vival (Table 1) and also disease severity scores (APACHE andSOFA, Figure 2 C,D) were similar between groups. Taken togeth-er, early disease progression (expressed as time interval fromsymptom onset to hospital admission) was found to be more rapidin patients who did not survive 60 days. Vice versa, a lower prob-
Figure 2. Delay of admission (days after onset of symptoms) and severity of illness on first day in ICU. Patients who died until day 60were admitted earlier (A) to Hospital (p=0.0018), and (B) to ICU (p=0.0037, both Mann Whitney U test) compared to those who sur-vived day 60. Days are counted from ICU admission. (C) APACHE and (D) SOFA scores did not differ significantly (Mann WhitneyU test). Box and whiskers as explained in Figure 1.
MRM_02 original.qxp_Hrev_master 02/04/21 11:10 Pagina 36

9MRM
Multidisciplinary Respiratory Medicine 2021; 16:744 - M. Heim et al.
ability of survival was also shown when the total cohort was divid-ed into patients admitted to hospital within 2 days of symptomonset or later (Figure 3).
DiscussionIn our first 50 COVID-19 patients treated on the ICU, we ini-
tially focused on the extent of lung damage in comparison withother cohorts. In a retrospective study on 10,021 hospitalizedCOVID-19 patients in 920 German hospitals, 17% receivedmechanical ventilation [20]. Although this proportion of 17% notnecessarily equals the prevalence of ARDS (which was not report-ed), it is far below ARDS prevalence of about 33% in 2,486 hospi-talized COVID-19 patients in five countries. In this cohort, 63% ofpatients needed mechanical ventilation, and ARDS prevalence was75% [21]. In our ICU patients, a proportion of 78% fulfilled thediagnostic criteria for ARDS. Among those who were mechanical-ly ventilated, ARDS prevalence exceeded 90% and remained onthis level in a second assessment the subsequent day. Althoughbeing profoundly hypoxaemic, our patients showed comparativelywell-preserved lung mechanics, which is rarely seen in patientswith ‘typical’ ARDS. The combination of a large shunt fraction anda rather good lung compliance suggests a novel pathophysiology,thus leading to the hypothesis of gasless tissue being hyperper-fused. Accordingly, an increase in oxygenation achieved by PEEPor prone positioning might not primarily result from recruitmentbut rather from gravity and/or pressure forces [22]. Proningpatients with relatively high compliance therefore might not holdmuch promise. Nevertheless, half of our ventilated patients (n=22)were put in the prone position, and during the first proning period,pO2 rose considerably (Figure 1). Survivors underwent three peri-ods in prone position in median. It has been put forward that autop-sy findings of deceased patients with COVID-19 pneumoniamatched the original description of ARDS, as diffuse alveolardamage was seen in most cases, notably also in patients who hadnever been invasively ventilated [23]. Clinically, patients whounderwent ECMO therapy presented the ‘typical’ ARDS findingsat this stage of disease: the initially well-preserved lung compli-ance had finally been lost. This might not only be due to the naturalcourse of the viral pneumonia, but also due to mechanical chal-
lenge caused by the great and sustained respiratory efforts ofCOVID-19 patients before receiving ventilator support. Last butnot least, the worsening of lung compliance might also result frompositive pressure ventilation itself [24]. In our cohort, NIV orHFNO was rarely used due to the concern of spreading viralaerosols. Furthermore, the distressed patients arriving at our ICUsneeded immediate relief from their pronounced shortness of breath– and this included sedation to an extent that precluded an initialnon-invasive support. All our patients requiring invasive ventila-tion were intubated at the latest one day after ICU admission. Sinceour hospital (like the German health-care system in general) wasnot overrun by the pandemic at any time during the last months, allpatients in need for intensified therapy and mechanical ventilationcould be admitted to ICU. In our hospital, all physicians on thewards could call an intensivist 24/7 to discuss the treatment includ-ing the possible need to transfer the patient to the ICU. Also,ECMO indication was discussed in an interdisciplinary approachbetween anaesthesiological and medical ICU specialists. Thisinvasive strategy could be put into action in every case the boardhad agreed on the indication. Although their number is low, thehigh in-hospital mortality of our ECMO patients (86%) compareswith the one in the large German retrospective study (71%) [20].This exceeds by far the numbers from the ELSO registry, with anin-hospital mortality of 39% in COVID-19 patients [25]. Althougha possible bias cannot be ruled out for these numbers from centreswhich voluntarily decided to report to the registry, the differenceremains remarkable. We did not administer dexamethasone (or anyother corticosteroid routinely) to our COVID-19 patients, but,regarding the data available until present, this could be a helpfuljigsaw piece in the treatment – although it might be desirable toadminister this medication before ICU admission [26].Remdesivir, as an antiviral agent, does not seem promising forpatients needing invasive ventilation [27-29]. As long as a specificantiviral or disease modifying drug is not at hand, the establishedtreatment options against non-COVID-19 ARDS remain our cor-nerstones taking care of our critical ill COVID-19 patients. Abouthalf of our patients could return home until day 60, and less thanhalf of them reported no limitation on activities on this day (20%of the whole cohort). This underlines the medium- and long-termconsequences of the disease for patients who needed critical care.The worst outcome ensued for the intubated patients with a parallelneed for renal replacement therapy (60-day mortality, 42.1%).
Figure 3. Kaplan Meier estimates of survival (A) in the whole cohort and (B) in the subgroups of patients admitted to hospital within2 days or later after onset of symptoms. The two survival curves differ significantly (Log-rank test, p=0.0003).
MRM_02 original.qxp_Hrev_master 02/04/21 11:10 Pagina 37

10MRM
Multidisciplinary Respiratory Medicine 2021; 16:744 - M. Heim et al.
Against the backdrop of the German retrospective mega studywhich offered data on the course of the disease [20], our group ofpatients showed a comparatively good outcome. Clearly, the timefrom onset of symptoms to admission to the hospital or to the ICUwas significantly lower in the group of non-survivors. It mighttherefore be concluded that early deterioration of symptoms pre-dicts an unfavourable course of the disease.
Vitamin D values were generally low in our patient cohort. Itis still not known whether this is a relevant prognostic factor. It isalso unknown whether a substitution (of calcifediol or cholecalcif-erol) can play a role in treatment of COVID-19 or whether a pro-phylactic substitution might be warranted. Inverse correlationsbetween vitamin D status and COVID-19 incidence and mortalityhave been reported in Europe [30,31]. Higher levels of circulatingvitamin D have been associated with lower SARS-CoV-2 positivi-ty rates [32]. As vitamin D has pleiotropic actions on the immunesystem, the supplementation might help to protect against an infec-tion with SARS-CoV-2. In a pilot study, administration of a high-dose calcifediol reduced the need for ICU treatment in patientswith COVID-19 [33].
The limitations of our study are the retrospective design, thesingle centre character and the small sample size. The lack of stan-dardised pharmacological treatment also may be an importantparameter influencing the outcome. Ordinal scoring of outcome ona 7-point scale might be seen as an improperly simplistic assess-ment of patients with COVID-19. However, we captured data fromall of our first 50 patients, including the outcome score for each ofthem on day 60 after ICU admission. We feel our data can illustratethe potential harm for COVID-19 patients at any age group, as wellas the potential for recovery even for the most severely affectedpatient group with the need for ventilator and renal replacementtherapy.
ConclusionsRapid deterioration after onset of symptoms can be seen as an
early warning signal for a further unfavourable course of diseaseand, ultimately, a poor outcome in COVID-19. The consistentlylow vitamin D concentration gives reason to take a closer look atthe role of vitamin D in COVID-19 patients. As long as there is nospecific drug that mitigates the course of COVID-19, lung-protec-tive ventilator therapy including prone positioning remain main-stay of the treatment.
Abbreviations COVID-19, coronavirus disease 2019; ICU, intensive care unit; ARDS, acute respiratory distress syndrome; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; COPD, chronic obstructive pulmonary disease; PCR, polymerase chain reaction; CT, chest computed tomography; SOFA, sepsis-related organ failure assessment score; APACHE, acute physiology and chronic health evaluation score; ECMO, extracorporeal membrane oxygenation; NIV, non-invasive ventilation; HFNO, high flow nasal oxygen; HI, Horovitz index; PEEP, positive endexpiratory pressure.
References1. Richardson S, Hirsch JS, Narasimhan M, Crawford JM,
McGinn T, Davidson KW, et al. Presenting characteristics,comorbidities, and outcomes among 5700 patients hospitalizedwith COVID-19 in the New York City area. JAMA2020;323:2052-9.
2. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al.Clinical characteristics of Coronavirus disease 2019 in China.N Engl J Med 2020;382:1708-20.
3. Dreher M, Kersten A, Bickenbach J, Balfanz P, Hartmann B,Cornelissen C, et al. The characteristics of 50 hospitalizedCOVID-19 patients with and without ARDS. Dtsch Arztebl Int2020;117:271-8.
4. Yang X, Yu Y, Xu J, Shu H, Xia Ja, Liu H, et al. Clinical courseand outcomes of critically ill patients with SARS-CoV-2 pneu-monia in Wuhan, China: a single-centered, retrospective,observational study. Lancet Respir Med 2020;8:475-81.
5. Bhatraju PK, Ghassemieh BJ, Nichols M, Kim R, Jerome KR,Nalla AK, et al. Covid-19 in critically ill patients in the SeattleRegion — Case series. N Engl J Med 2020;382:2012-22.
6. Arentz M, Yim E, Klaff L, Lokhandwala S, Riedo FX, ChongM, et al. Characteristics and outcomes of 21 critically illpatients with COVID-19 in Washington State. JAMA2020;323:1612-4.
7. Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A,et al. Epidemiology, patterns of care, and mortality for patientswith acute respiratory distress syndrome in intensive care unitsin 50 countries. JAMA 2016;315:788-800.
8. Auld SC, Caridi-Scheible M, Blum JM, Robichaux C, Kraft C,Jacob JT, et al. ICU and ventilator mortality among criticallyill adults with Coronavirus Disease 2019. Crit Care Med2020;48:e799-809.
9. Bouch DC, Thompson JP. Severity scoring systems in the crit-ically ill. Continuing Education in Anaesthesia Critical Care &Pain 2008;8:181-5.
10. Vincent JL, Moreno R. Clinical review: Scoring systems in thecritically ill. Crit Care 2010;14:207.
11. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinicalfeatures of patients infected with 2019 novel coronavirus inWuhan, China. Lancet 2020;395:497-506.
12. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinicalcharacteristics of 138 hospitalized patients with 2019 novelCoronavirus–infected pneumonia in Wuhan, China. JAMA2020;323:1061-9.
13. Spinner CD, Gottlieb RL, Criner GJ, Arribas López JR,Cattelan AM, Soriano Viladomiu A, et al. Effect of remdesivirvs standard care on clinical status at 11 days in patients withmoderate COVID-19: A randomized clinical trial. JAMA2020;324:1048-57.
14. Rothe K, Feihl S, Schneider J, Wallnöfer F, Wurst M, Lukas M,et al. Rates of bacterial co-infections and antimicrobial use inCOVID-19 patients: a retrospective cohort study in light ofantibiotic stewardship. Eur J Clin Microbiol Infect Dis 2020.
15. Wang Y, Dong C, Hu Y, Li C, Ren Q, Zhang X, et al. Temporalchanges of CT findings in 90 patients with COVID-19 pneu-monia: A longitudinal study. Radiology 2020;296:e55-64.
16. Ai T, Yang Z, Hou H, Zhan C, Chen C, Lv W, et al. Correlationof chest CT and RT-PCR testing in Coronavirus Disease 2019(COVID-19) in China: A report of 1014 cases. Radiology2020;296:e32-40.
17. ARDS Definition Task Force, Ranieri MR, Rubenfeld GD,Thompson BT, Ferguson ND, Caldwell E, et al. Acute respira-
MRM_02 original.qxp_Hrev_master 02/04/21 11:10 Pagina 38

11MRM
Multidisciplinary Respiratory Medicine 2021; 16:744 - M. Heim et al.
tory distress syndrome: The Berlin definition. JAMA2012;307:2526-33.
18. Zádori N, Váncsa S, Farkas N, Hegyi P, Erőss B, Szakó L, etal. The negative impact of comorbidities on the disease courseof COVID-19. Intensive Care Med 2020;46:1784-6.
19. Chen L, Yu J, He W, Chen L, Yuan G, Dong F, et al. Risk fac-tors for death in 1859 subjects with COVID-19. Leukemia2020;34:2173-83.
20. Karagiannidis C, Mostert C, Hentschker C, Voshaar T,Malzahn J, Schillinger G, et al. Case characteristics, resourceuse, and outcomes of 10 021 patients with COVID-19 admittedto 920 German hospitals: an observational study. LancetRespir Med 2020;8:853-62.
21. Tzotzos SJ, Fischer B, Fischer H, Zeitlinger M. Incidence ofARDS and outcomes in hospitalized patients with COVID-19:a global literature survey. Crit Care 2020;24:516.
22. Gattinoni L, Coppola S, Cressoni M, Busana M, Rossi S,Chiumello D. COVID-19 does not lead to a "typical" acute res-piratory distress syndrome. Am J Respir Crit Care Med2020;201:1299-300.
23. Bos LDJ. COVID-19–related acute respiratory distress syn-drome: Not so atypical. Am J Respir Crit Care Med2020;202:622-4.
24. Gattinoni L, Chiumello D, Rossi S. COVID-19 pneumonia:ARDS or not? Crit Care 2020;24:154.
25. Barbaro RP, MacLaren G, Boonstra PS, Iwashyna TJ, SlutskyAS, Fan E, et al. Extracorporeal membrane oxygenation sup-port in COVID-19: an international cohort study of theExtracorporeal Life Support Organization registry. Lancet2020;396:1071-8.
26. RECOVERY Collaborative Group, Horby P, Lim WS,
Emberson JR, Mafham M, Bell JL. Dexamethasone in hospi-talized patients with Covid-19 — Preliminary report. N Engl JMed 2021;384:693-704.
27. Pan H, Peto R, Karim QA, Alejandria M, Henao-Restrepo AM,García CH, et al. Repurposed antiviral drugs for COVID-19 –interim WHO SOLIDARITY trial results. medRxiv2020:2020.10.15.20209817.
28. Wang Y, Zhang D, Du G, Du R, Zhao J, Jin Y, et al. Remdesivirin adults with severe COVID-19: a randomised, double-blind,placebo-controlled, multicentre trial. Lance. 2020;395:1569-78.
29. Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS,Kalil AC, et al. Remdesivir for the treatment of Covid-19 —Final report. N Engl J Med 2020;383:1813-26.
30. Laird E, Rhodes J, Kenny RA. Vitamin D and inflammation:Potential implications for severity of Covid-19. Ir Med J2020;113:81.
31. Ilie PC, Stefanescu S, Smith L. The role of vitamin D in theprevention of coronavirus disease 2019 infection and mortali-ty. Aging Clin Exp Res 2020;32:1195-8.
32. Kaufman HW, Niles JK, Kroll MH, Bi C, Holick MF. SARS-CoV-2 positivity rates associated with circulating 25-hydrox-yvitamin D levels. PLoS One 2020;15:e0239252.
33. Entrenas Castillo M, Entrenas Costa LM, Vaquero Barrios JM,Alcalá Díaz JF, López Miranda J, Bouillon R, et al. Effect ofcalcifediol treatment and best available therapy versus bestavailable therapy on intensive care unit admission and mortal-ity among patients hospitalized for COVID-19: A pilot ran-domized clinical study. J Steroid Biochem Mol Biol2020;203:105751.
Received for publication: 25 December 2020. Accepted for publication: 23 February 2021.This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0).©Copyright: the Author(s), 2021Licensee PAGEPress, ItalyMultidisciplinary Respiratory Medicine 2021; 16:744doi:10.4081/mrm.2021.744
MRM_02 original.qxp_Hrev_master 02/04/21 11:10 Pagina 39

12MRM
Early responders within seven days of dupilumab treatment for severe asthma evaluated by patient-reported outcome: a pilot studyNozomi Tani, Nobutaka Kataoka, Yusuke Kunimatsu, Yusuke Tachibana, Takumi Sugimoto, Izumi Sato, Yuri Ogura, Kazuki Hirose, Takayuki TakedaDepartment of Respiratory Medicine, Japanese Red Cross Kyoto Daini Hospital, Kyoto, Japan
Background: The management of severe asthma-associated symptoms is essential since they are distressing to theaffected patients, and also greatly impair their quality of life. Dupilumab, a monoclonal antibody, blocks interleukin(IL)-4 and IL-13 signaling, both of which are crucial in acquired and innate immunity pathways through fast signaltransduction, leading to an early response to treatment. Although rapid improvement within 1–3 days after dupilumabtreatment was observed in moderate-to-severe atopic dermatitis, an early response within 7 days of dupilumab treat-ment in severe asthma has not been reported.Methods: Twelve consecutive patients with severe asthma who were newly treated with dupilumab between July 2019and April 2020 were retrospectively investigated. We evaluated the early response (within 7 days) of patients withsevere asthma receiving dupilumab therapy. Asthma control test (ACT) and the daily ACT, which was modified fromthe ACT to evaluate daily symptoms associated with asthma, were adopted as patient-reported outcomes (PROs) atweek 8 and within 7 days, respectively. Patients were stratified into early responders (7 days), late responders (week8), and non-responders without significant improvement in PROs. Descriptive statistics were adopted due to the lim-ited number of patients.Results: Four of these 12 patients were early responders, with the following baseline characteristics: body mass index,<25 kg/m2; without depression; baseline forced expiratory volume in 1 second, <1.50 L; and more than one exacerba-tion in 1 year. On the other hand, five were late responders, and 44.4% of the nine responders were early responders.The higher the eosinophilic count and/or FeNO did not show any relationship between the early responder and non-responder.Conclusions: The effect of dupilumab on severe asthma in patients with atopic features could be started earlier than2 weeks, similar to atopic dermatitis. Daily ACT may be useful in monitoring the early efficacy of dupilumab in treat-ing severe asthma.
Key words: Asthma; daily ACT (asthma control test); dupilumab; early responder; severe asthma; quality of life.
AB
STR
ACT
Correspondence: Takayuki Takeda, Department of Respiratory Medicine, Japanese Red Cross Kyoto Daini Hospital, 355-5,Haruobi-cho, Kamanza-dori, Marutamachi-agaru, Kamigyo-ku, Kyoto 602-8026, Japan. Tel. +81.75.2315171 - Fax: +81.75.2563451. E-mail: [email protected]
Contributions: NT, TT, designed and wrote the original manuscript; NK, YK, collected data; YT, TS, constructed methodol-ogy; IS, NT, analyzed the data; YO, KH, contributed to the final data curation and visualization; TT, supervised the study,reviewed and edited the manuscript. Each author made a significant contribution to the manuscript, has read and approved thefinal version of the manuscript and agreed to be accountable for all aspects of the work.
Conflict of interest: The authors declare that they have no competing interests, and all authors confirm accuracy.
Funding: None.Availability of data and materials: The datasets analyzed in the current study are available from the corresponding author onreasonable request.
Ethics approval and consent to participate: This study was approved by the Ethics Committee of the Japanese Red CrossKyoto Daini Hospital (approval date: 21 June 2019; approval number: S2019-21). The requirement for written informed con-sent was waived because of the retrospective study design and because patient anonymity was assured. Instead, the opportunityto opt-out was provided on the homepage of our hospital.
Consent for publication: Not applicable.
ORIGINAL RESEARCH ARTICLE
®Multidisciplinary Respiratory Medicine 2021; volume 16:736
MRM_02 original.qxp_Hrev_master 17/03/21 09:21 Pagina 25

13MRM
Multidisciplinary Respiratory Medicine 2021; 16:736 - N. Tani, et al.
IntroductionAsthma is one of the most common respiratory diseases char-
acterized by heterogeneity in symptoms, severity, phenotypes, andendotypes due to the underlying molecular mechanisms [1]. In par-ticular, severe asthma accounts for approximately 5 to 10% of theasthmatic population, and its management is of the utmost impor-tance [2,3]. Severe asthma not only impairs the patient’s quality oflife (QOL), which can be life-threatening [3,4], but also poses ahigh burden for both healthcare resources and society [3,5-7].Thus, a comprehensive approach to effectively manage this condi-tion is crucial.
To achieve this, the investigation into the molecular mechanism ofairway inflammation has provided much-needed insight into the patho-physiology of severe asthma [8-10]. Both adaptive and innate immunesystems are important in the pathogenesis of airway epithelial inflam-mation in asthma and play a pivotal role in type 2 inflammation.Adaptive immunity is mediated by T helper-2 (Th2) cells, eosinophils,immunoglobulin E (IgE)-producing B cells, and mast cells via IgE andTh2 cytokines such as interleukin-4 (IL-4), IL-5, and IL-13. On theother hand, group 2 innate lymphoid cells (ILC2s) play an importantrole via IL-5 and IL-13 in innate immunity. While upstream events inthe airway epithelium, which trigger the production of Th2 cytokines,have been identified as thymic stromal lymphopoietin (TSLP) in adap-tive immunity, and TSLP, IL-25, and IL-33 in innate immunity, respec-tively, biological agents targeting them have not been established inphase 3 trials.
The introduction of biological agents such as monoclonal anti-bodies targeting IgE (omalizumab), IL-5 (mepolizumab), and IL-5receptor-α subunit (IL-5Rα; benralizumab) have revolutionized thetreatment strategy for severe asthma [11-13]. They were appliedaccording to the serum levels of IgE and eosinophil counts.Dupilumab is a monoclonal antibody that targets the anti-IL-4receptor-α subunit (IL-4Rα) of the IL-4 and IL-4 / IL-13 receptorcomplexes, which blocks both IL-4 and IL-13 signaling. This iscrucial in both acquired and innate immunity pathways [14].
Most of the primary endpoints in clinical trials of biologicalagents are established to confirm their long-term efficacy by set-ting endpoints at forced expiratory volume in 1 second (FEV1), theannualized rate of severe asthma exacerbation, and the percentagereduction in the preexisting glucocorticoid dose more than 3months after the treatment. Although these endpoints are signifi-cant in measuring the durable efficacy of biological agents, theearly management of asthma-associated symptoms is equallyimportant. Thus, the palliation of severe asthma-associated symp-toms and an earlier response to biological agents is highly desired.
Although rapid improvement within 1–3 days after dupilumabtreatment was observed in moderate-to-severe atopic dermatitis[15,16], an early response within 7 days of dupilumab treatment insevere asthma has not been reported. We have modified the widely uti-lized asthma control test (ACT), a patient-reported outcome (PRO)[17] consisting of 5 items experienced within 4-weeks before assess-ing the frequency of dyspnea, general asthma-related symptoms, useof rescue medications, the effect of asthma on daily functioning, andoverall self-assessment of asthma control [18]. Moreover, ACT is sim-ple and useful in usual care settings and has been validated to be con-cordant with the Asthma Control Questionnaire (ACQ) [18]. ACT ismore prevalent than ACQ in Japan. The minimal clinically importantdifference in ACT score over time is 3 points [19]. Since ACT wasdesigned to report asthma control with a 4-week recall, it is unfit forthe daily assessment of asthma-associated symptoms. Therefore, inthe current study, ACT was modified for daily usage to report asthmacontrol with a 24-hour recall, named “daily ACT,” which could reflectdaily symptoms and activity very well. Daily ACT was reported every
day to evaluate the early response within 7 days of dupilumab treat-ment in severe asthma. The original ACT was also used to assess asth-ma-associated symptoms and the effect of dupilumab on 4-week asth-ma control. The baseline characteristics were also investigated in rela-tion to the early responders within 7 days as well as responders atweek 8, who showed 3 points or more improvement in the daily ACTand original ACT scores, respectively.
Methods
Patients A retrospective study was performed on 12 consecutive
patients with severe asthma who were newly treated with dupilum-ab between July 2019 and April 2020.
These patients were asked to report both daily ACT and origi-nal ACT, which were routinely conducted at our hospital when bio-logical agents were newly introduced irrespective of clinical study.Therefore, this study was categorized as retrospective. Thosepatients who had been treated with other biological agents andswitched to dupilumab due to their ineffectiveness were notexcluded irrespective of biological agent-free interval. This studywas carried out in accordance with the Declaration of Helsinki andwas approved by the Ethics Committee of the Japanese Red CrossKyoto Daini Hospital (approval date: 21 June 2019; approval num-ber: S2019-21). The requirement for written informed consent waswaived because of the retrospective study design and also becausepatient anonymity was assured. Instead, the opportunity to opt-outwas provided on the homepage of our hospital.
Dupilumab was introduced in patients with severe asthma whowere uncontrolled under medium-to-high dose of inhaled corticos-teroids (ICSs) and long-acting β2-agonist (LABA) and/or long-act-ing muscarinic antagonist (LAMA). The indication criteria fordupilumab at our hospital were as follows: omalizumab was firstintroduced in patients who exhibited an allergic or atopic pheno-type with elevated specific IgE antibodies and serum total IgE val-ues ranging between 30 and 1500 IU/mL, and switched todupilumab when omalizumab was not effective; mepolizumab orbenralizumab were introduced to patients who exhibitedeosinophil counts of 150 cells/μL or higher irrespective of an aller-gic or atopic phenotype, and switched to dupilumab when anti-IL-5/IL-5Rα therapies were ineffective; and dupilumab was preferen-tially introduced as the first-line biological agent to patients whodemonstrated type 2 inflammation with elevated eosinophil countsor fraction of exhaled nitric oxide (FeNO) ≥25 ppb, when accom-panied by atopic dermatitis or eosinophilic chronic rhinosinusitis.
Treatment schedule, baseline characteristics, and evalu-ation of patient-related outcomes
Dupilumab was administered subcutaneously at a dose of 600mg on day 1, followed by a dose of 300 mg every 2 weeks as anadd-on therapy.
The following baseline characteristics were analyzed: sex, age,body mass index (BMI), smoking habits, antigen-specific IgE, thehighest serum total IgE level, and eosinophil counts (≥ 300cells/μL were evaluated as elevated) [20], FeNO (≥25 ppb wasevaluated as elevated) [21]; FEV1; past history of exacerbationrequiring an emergency or urgent medical care visit and systemiccorticosteroid treatment within 1 year before dupilumab introduc-tion, prescription of leukotriene receptor antagonists (LTRAs),proton pump inhibitors (PPIs), macrolides, or oral corticosteroids(OCS), previous use of biological agents, previous bronchial ther-moplasty (BT), and comorbidities including chronic obstructive
MRM_02 original.qxp_Hrev_master 17/03/21 09:21 Pagina 26

14MRM
Multidisciplinary Respiratory Medicine 2021; 16:736 - N. Tani, et al.
pulmonary disease (COPD), allergic rhinitis, eosinophilic chronicrhinosinusitis, atopic dermatitis, and depression.
Daily ACT was created as a 5-item, patient-administered sur-vey evaluating the 24-hour control of asthma-associated symp-toms. Asthma control with a 24-hour recall was evaluated by 5questions in accordance with the original ACT, while some modi-fications were made to questions No. 2, 3, and 4, which dealt withthe frequency of asthma-associated symptoms and rescue inhaleruse (Table 1). Daily ACT was reported by the patient every day for8 successive days starting on the day of dupilumab introduction.The early response to dupilumab was defined as the improvementof 3 points or more in the daily ACT scores within 7 days afterdupilumab introduction, where the daily ACT score on day 1 wasused as the baseline in the evaluation. The definition of the earlyresponse as “3 points or more improvements” was adopted throughthe interpretation of the original ACT [19]. The response todupilumab was also defined as 3 points or more improvement inthe original ACT scores at week 8, where the ACT score on day 1was used as the baseline. The baseline scores were interchangedbetween the daily and the original ACT scores, since the contentsof the daily ACT were modified from the original ACT, resultingin slightly different baseline scores between the two PROs.
Statistical analysisDescriptive statistics were adopted to report the baseline char-
acteristics, the evaluation of PROs, and the prevalence of earlyresponders among the 12 patients in the 7 days period and theresponder to dupilumab at week 8 because of the limited numberof patients enrolled. The data are presented as median (range orstandard deviation; SD) for continuous variables and percentagesfor categorical variables.
Results
Baseline characteristics The baseline characteristics are summarized in Table 2. All the
patients exhibited one or more factors associated with type 2inflammation, that is, positive for antigen-specific IgE, elevatedeosinophil counts, or elevated FeNO levels at baseline. The median
ACT and the daily ACT scores at the baseline were 16 (range: 8–19) and 17 (range: 9–21), respectively. The median ACT and thedaily ACT scores were relatively high since biological agents hadbeen administered previously and were switched to dupilumab in 8
Table 1. Daily asthma control test.
Q1. In the past 24 hours, how much of the time did your asthma keep you from getting as much done at work, school, or at home? All of the time Most of the time Some of the time A little of the time None of the time
1 2 3 4 5Q2. During the past 24 hours, how often have you had shortness of breath? More than once a day Once a day at rest Once a day at night Once a day on exertion Not at all
1 2 3 4 5Q3. During the past 24 hours, how often did your asthma symptom wake you up at night or earlier than usual in the morning? Could not sleep at all Requiring orthopnea More than twice a night Once a night Not at all
1 2 3 4 5Q4. During the past 24 hours, how often have you used your rescue inhaler (SABA)? 3 or more times a day Twice a day Once a day at rest Once a day on exertion Not at all
1 2 3 4 5Q5. How would you rate your asthma control during the past 24 hours? Not controlled at all Poorly controlled Somewhat controlled Well controlled Completely controlled
1 2 3 4 5
Table 2. Baseline characteristics.
Total (n=12)
Age (median; years, range) 51.5 (38 – 77)Sex (women / men; n, %) 10 (83.3%) / 2 (16.7%)BMI (median; kg/m2, range) 24.1 (20.4 – 41.6)Smoking habit + / - (n, %) 6 (50.0%) / 6 (50.0%) Antigen-specific IgE + / - (n, %) 12 (100%) / 0 (0%)Total IgE (median; IU/mL, range) 470 (37 – 2470)Eosinophil counts (median; cells/ L, range) 286.0 (203.0 – 1368.0)FeNO (median; ppb, range) 41 (7 – 300)FEV1 (median; ml, range) 2070 (500 – 3220)ACT score at baseline (median; range) 16 (8 – 19)Daily ACT score at baseline (median; range) 17 (9 – 21)More than one exacerbation + / - (n, %) 7 (58.3%) / 5 (41.7%)High-dose ICS/LABA + / - (n, %) 12 (100%) / 0 (0%)LAMA + / - (n, %) 10 (83.3%) / 2 (16.7%)LTRA + / - (n, %) 11 (91.7%) / 1 (8.3%)PPI + / - (n, %) 6 (50.0%) / 6 (50.0%)Macrolide + / - (n, %) 3 (25.0%) / 9 (75.0%)Daily OCS + / - (n, %) 7 (58.3%) / 5 (41.7%)Biologic agents + / - (n, %) 8 (66.7%) / 4 (33.3%)BT + / - (n, %) 2 (16.7%) / 10 (83.3%)COPD + / - (n, %) 3 (25.0%) / 9 (75.0%)AR + / - (n, %) 2 (16.7%) / 10 (83.3%)ECRS + / - (n, %) 2 (16.7%) / 10 (83.3%)AD + / - (n, %) 1 (8.3%) / 11 (91.7%)Depression + / - (n, %) 3 (25.0%) / 9 (75.0%)
MRM_02 original.qxp_Hrev_master 17/03/21 09:21 Pagina 27

15MRM
Multidisciplinary Respiratory Medicine 2021; 16:736 - N. Tani, et al.
patients, which are described below.At baseline, high-dose ICS/LABA was prescribed for all the
patients, LAMA for 10 (83.3%), LTRAs for 11 (91.7%), PPIs for 6(50.0%), macrolides for 3 (25.0%), daily OCS for 7 (58.3%), andbiological agents had been previously administered in 8 (66.7%;omalizumab and benralizumab in 5 and 3 patients, respectively).The previous biological agents were directly switched to dupilum-ab due to their inadequate effects in all 8 patients. In 2 patients,(16.7%) BT was performed. The comorbidities observed wereCOPD in 3 (25.0%), allergic rhinitis in 2 (16.7%), eosinophilicchronic rhinosinusitis in 2 (16.7%), atopic dermatitis in 1 (8.3%),and depression in 3 (25.0%) patients.
Changes in subjective symptoms of 12 patients via dailyACT within 7 days and the original ACT at weeks 4and 8
The changes in PROs from the baseline of 12 patients via thedaily ACT within 7 days (days 1–8) and the original ACT at weeks4 and 8 are plotted in Figure 1. The median days needed for the sig-nificant improvement in the daily ACT in the 4 early responderswas 5 days (range: 2–7 days), while a significant improvement inthe original ACT was observed for the first time in 7 patients atweek 4 and in 2 patients at week 8 (Figure 1).
The patients were divided into 3 groups according to theresponse pattern: early responders within 7 days via the daily ACT,late responders until week 8, and non-responders without signifi-cant improvement in PROs. The mean changes in the daily and the
original ACT from the baseline (day 1) of these subpopulations areplotted in Figure 2. The fluctuation of the daily or original ACTscores was observed in some cases, while the scores tended toimprove over time in both the early and late responders todupilumab.
Baseline characteristics according to the therapeuticeffects of dupilumab on subjective symptoms within 7days
Four out of 12 patients (33.3%) reported an early response todupilumab within 7 days, while the percentage of 4 early respon-ders increased to 44.4% among 9 responders until week 8. Threewomen and 1 man showed an early response, and all 4 earlyresponders had a BMI <25 and without psychiatric disorders, whilethe median eosinophil counts and FeNO in these three patientswere 391.9 (range: 203.0–1368.0) and 52 (range: 20–117), respec-tively. Three out of 4 early responders had baseline FEV1 less than1.50 L, and all 4 experienced more than 1 exacerbation within 1year. On the other hand, the median eosinophil counts and FeNOin 8 patients without an early response were 286.0 (range, 211.2 –593.6) and 30.5 (range, 7 – 300), respectively. Six out of 8 patientswithout an early response had a baseline FEV1 > 1.50 L, and only3 patients experienced more than 1 exacerbation within 1 year.There was no relationship between a higher eosinophilic countand/or FeNO with early and non-responder to dupilumab via thedaily ACT within 7 days in the current study, due in part to a smallsample size (Table 3).
Figure 1. The changes in patient-reported outcomes from the baseline of 12 patients via the daily asthma control test (ACT) on days1-8 and the original ACT at weeks 4 and 8 are plotted. The black lines (No. 1, 2, 3, 10) represent the early responders within 7 days,the dark gray lines (No. 4, 5, 8, 11, and 12) the late responder until week 8, and the light gray lines (No. 6, 7, and 9) the non-responders,respectively. The median day needed for the significant improvement in 4 early responders was 5 days (range, 2-7 days), while a signif-icant improvement in the early and late responders via the original ACT was observed for the first time in 7 patients at week 4 and in2 patients at week 8.
MRM_02 original.qxp_Hrev_master 17/03/21 09:21 Pagina 28

16MRM
Multidisciplinary Respiratory Medicine 2021; 16:736 - N. Tani, et al.
Baseline characteristics according to the therapeuticeffects of dupilumab on subjective symptoms at week 8
Nine out of 12 patients (75.0%) responded to dupilumab viathe original ACT until week 8, including 4 early responders within7 days. The median eosinophil counts and FeNO in 9 responderswere 287.0 (range, 203.0–1368.0) and 47 (range, 7–300), respec-tively. Although eosinophil counts and FeNO represent a type 2
inflammation, the higher eosinophilic count and/or FeNO did notshow any relationship between responders and non-responders todupilumab until week 8 in the current study because of the smallsample size (Table 4). Three out of 9 responders had baseline FEV1<1.50 L, and 6 out of 9 experienced more than 1 exacerbation with-in 1 year. All 3 non-responders were women, and had characteris-tics of BMI ≥28 and comorbidity of depression, while the medianeosinophil counts and FeNO in these 3 patients were 285 (range:
Table 3. Baseline characteristics according to the therapeutic effects of dupilumab on subjective symptoms within 7 days.
Total (n=12) Early responders (n=4) Late or non-responders (n=8)
Age (median; years, range) 51.5 (38 – 77) 70.0 (38 – 75) 49.5 (41 – 77)Sex (women / men; n, %) 10 (83.3%) / 2 (16.7%) 3 (75.0%) / 1 (25.0%) 7 (87.5%) / 1 (12.5%)BMI (median; kg/m2, range) 24.1 (20.4 – 41.6) 21.9 (20.4 – 24.8) 26.7 (20.7 – 41.6)Smoking habit + / - (n, %) 6 (50.0%) / 6 (50.0%) 1 (25.0%) / 3 (75.0%) 5 (62.5%) / 3 (37.5%)Total IgE (median; IU/mL, range) 470 (37 – 2470) 407 (267 – 2470) 472.5 (37 – 1791)Eosinophil counts (median; cells/ L, range) 286.0 (203.0 – 1368.0) 391.9 (203.0 – 1368.0) 286.0 (211.2 – 593.6)FeNO (median; ppb, range) 41.0 (7 – 300) 52.0 (20 – 117) 30.5 (7 – 300)FEV1 (median; ml, range) 2070 (500 – 3220) 1415 (500 – 3220) 2370 (1240 – 2970)ACT score at baseline (median; range) 16 (8 – 19) 15 (13 – 17) 16 (8 – 19)Daily ACT score at baseline (median; range) 17 (9 – 21) 15 (13 – 17) 17 (9 – 21)More than one exacerbation + / - (n, %) 7 (58.3%) / 5 (41.7%) 4 (100%) / 0 (0%) 3 (37.5%) / 5 (62.5%)Macrolide + / - (n, %) 3 (25.0%) / 9 (75.0%) 2 (50.0%) / 2 (50.0%) 1 (12.5%) / 7 (87.5%)Daily OCS + / - (n, %) 7 (58.3%) / 5 (41.7%) 3 (75.0%) / 1 (25.0%) 4 (50.0%) / 4 (50.0%)Biologic agents + / - (n, %) 8 (66.7%) / 4 (33.3%) 3 (75.0%) / 1 (25.0%) 5 (62.5%) / 3 (37.5%)COPD + / - (n, %) 3 (25.0%) / 9 (75.0%) 1 (25.0%) / 3 (75.0%) 2 (25.0%) / 6 (75.0%)AR + / - (n, %) 2 (16.7%) / 10 (83.3%) 0 (0%) / 4 (100%) 2 (25.0%) / 6 (75.0%)ECRS + / - (n, %) 2 (16.7%) / 10 (83.3%) 0 (0%) / 4 (100%) 2 (25.0%) / 6 (75.0%)AD + / - (n, %) 1 (8.3%) / 11 (91.7%) 0 (0%) / 4 (100%) 1 (12.5%) / 7 (87.5%)Depression + / - (n, %) 3 (25.0%) / 9 (75.0%) 0 (0%) / 4 (100%) 3 (37.5%) / 5 (62.5%)
ACT, asthma control test; AD, atopic dermatitis; AR, allergic rhinitis; BMI, body mass index; BT, bronchial thermoplasty; ECRS, eosinophilic chronic rhinosinusitis; FeNO, a fraction of exhaled nitric oxide;FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroid; IgE, immunoglobulin E; LABA, long-acting β2-agonist; LAMA, long-acting anti-muscarinic antagonist; LTRA, leukotriene receptorantagonist; OCS, oral corticosteroid; PPI, proton pump inhibitors.
Figure 2. The mean changes in the daily and the original asthma control test (ACT) of the early responders within 7 days, the lateresponders until week 8, and the non-responders were plotted. The early responders quickly reached the significant improvement in 2days followed by further improvement. On the other hand, the late responders showed significant improvement at week 4 followed byfurther improvement until week 8. The error bars show an SD of 2.
MRM_02 original.qxp_Hrev_master 17/03/21 09:21 Pagina 29

17MRM
Multidisciplinary Respiratory Medicine 2021; 16:736 - N. Tani, et al.
211.2–378) and 23 (range: 16–38), respectively, without any dif-ference compared to those of the responders. All 3 non-respondershad baseline FEV1 >1.50 L, and only 1 non-responder experiencedmore than 1 exacerbation within 1 year before dupilumab introduc-tion.
DiscussionAn appropriate assessment of asthma control is essential in
clinical practice, which is difficult due to its heterogeneous nature[1]. Therefore, physicians’ underestimation of asthma-associatedsymptoms [22], which can lead to the worsening of the patients’QOL, should be avoided. Incorporation of PROs, including ACTand lung function tests, is essential for appropriate asthma manage-ment, and avoiding patients’-physicians’ discordance in the QOLassessment. Under such circumstances, physical activity, which isoften hampered by asthma-associated symptoms, is very importantin asthma control since it sometimes leads to worsening of asthmacontrol [23]. Therefore, physical activity and QOL should beimproved as soon as possible. Lung function including FEV1, asth-ma-associated symptoms, and QOL often diverges from one anoth-er [18]. Thus, the assessment of asthma control regularly throughPRO as well as FEV1 remains equally important.
Dupilumab demonstrated efficacy in reducing the risk ofsevere asthma exacerbation and maintaining FEV1 in moderate-to-severe uncontrolled asthma, especially in patients with aneosinophil count of 300 or more per mm3 [24], and it also reducedoral glucocorticoid use in steroid-dependent severe asthma [25].
On the other hand, the efficacy of dupilumab in asthma-asso-ciated symptoms, QOL, and productivity in asthmatic patients hasbeen evaluated at week 24 after dupilumab treatment using ACQ-5 and asthma quality of life questionnaire (AQLQ), and dupilumab
significantly improved ACQ-5 and AQLQ scores [26]. However,the early efficiency of dupilumab within 7 days has not beenreported. This could be due to the lack of quantitative assessmentof the QOL daily as well as the administration interval of dupilum-ab every 2 weeks.
In the current study, we evaluated the changes in asthma-asso-ciated QOL on a daily basis for 8 consecutive days, including theday of dupilumab introduction using the daily ACT to detect earlyresponders to dupilumab. The original ACT was also used every 4weeks, and the efficacy was evaluated at week 8 after treatment.Nine patients (75.0%) showed efficacy via the original ACT atweeks 8, and 4 (44.4%) out of 9 responders achieved significantimprovement in daily ACT score within 7 days after dupilumabtreatment. Although descriptive statistics were adopted due to thelimited number of patients, all 4 early responders to dupilumab hadcharacteristics of BMI lower than 25 and were without psychiatricdisorders. All 4 patients had experienced more than 1 exacerbationbefore dupilumab introduction and 3 out of 4 had a baseline FEV1<1.50 L, which was in concordance with the observed results in aprevious phase 2b study investigating the efficacy of dupilumab onsymptoms and QOL in patients with persistent asthma [26]. On theother hand, the higher the eosinophilic count and/or FeNO did notshow any relationship between the early responder and non-responder.
Dupilumab is an anti-IL-4Rα antibody that inhibits both IL-4and IL-13 signaling by inhibiting the IL-13 receptor-α1 subunit(IL-13Rα1) [14]. IL-4 and IL-13 are the key Th2 cytokines, withIL-4 being secreted from Th2 cells and IL-13 from both Th2 cellsand ILC2s. IL-4 plays an important role in polarization and func-tional maintenance of Th2 cells, while IL-13 induces the expres-sion of inducible nitric oxide synthase (iNOS) in the airway epithe-lium as well as plays roles in TSLP promotion, goblet cell hyper-plasia, and airway remodeling through extracellular collagen depo-
Table 4. Baseline characteristics according to the therapeutic effects of dupilumab on subjective symptoms at week 8.
Total (n=12) Responders (n=9) Non-responders (n=3)
Age (median; years, range) 51.5 (38 – 77) 51.0 (38 – 77) 52.0 (41 – 64)Sex (women / men; n, %) 10 (83.3%) / 2 (16.7%) 7 (77.8%) / 2 (22.2%) 3 (100%) / 0 (0%)BMI (median; kg/m2, range) 24.1 (20.4 – 41.6) 22.2 (20.4 – 29.9) 33.7 (28.2 – 41.6)Smoking habit + / - (n, %) 6 (50.0%) / 6 (50.0%) 4 (44.4%) / 5 (55.6%) 2 (75.0%) / 1 (25.0%)Total IgE (median; IU/mL, range) 470 (37 – 2470) 408 (37 – 2470) 537 (280 – 829)Eosinophil counts (median; cells/μL, range) 286.0 (203.0 – 1368.0) 287.0 (203.0 – 1368.0) 285.0 (211.2 – 378.0)FeNO (median; ppb, range) 41 (7 – 300) 47 (7 – 300) 23 (16 – 38)FEV1 (median; ml, range) 2070 (500 – 3220) 2390 (500 – 3220) 1390 (1240 – 2350)ACT score at baseline (median; range) 16 (8 – 19) 16 (12 – 18) 16 (8 – 19)Daily ACT score at baseline (median; range) 17 (9 – 21) 17 (12 – 18) 17 (9 – 21)More than one exacerbation + / - (n, %) 7 (58.3%) / 5 (41.7%) 6 (66.7%) / 3 (33.3%) 1 (33.3%) / 2 (66.7%)Macrolide + / - (n, %) 3 (25.0%) / 9 (75.0%) 2 (22.2%) / 7 (77.8%) 1 (33.3%) / 2 (66.7%)Daily OCS + / - (n, %) 7 (58.3%) / 5 (41.7%) 5 (55.6%) / 4 (44.4%) 2 (75.0%) / 1 (25.0%)Biologic agents + / - (n, %) 8 (66.7%) / 4 (33.3%) 6 (66.7%) / 3 (33.3%) 2 (75.0%) / 1 (25.0%)COPD + / - (n, %) 3 (25.0%) / 9 (75.0%) 2 (22.2%) / 7 (77.8%) 1 (33.3%) / 2 (66.7%)AR + / - (n, %) 2 (16.7%) / 10 (83.3%) 2 (22.2%) / 7 (77.8%) 0 (0%) / 3 (100%)ECRS + / - (n, %) 2 (16.7%) / 10 (83.3%) 2 (22.2%) / 7 (77.8%) 0 (0%) / 3 (100%)AD + / - (n, %) 1 (8.3%) / 11 (91.7%) 1 (11.1%) / 8 (88.9%) 0 (0%) / 3 (100%)Depression + / - (n, %) 3 (25.0%) / 9 (75.0%) 0 (0%) / 9 (100%) 3 (100%) / 0 (0%)
ACT, asthma control test; AD, atopic dermatitis; AR, allergic rhinitis; BMI, body mass index; BT, bronchial thermoplasty; ECRS, eosinophilic chronic rhinosinusitis; FeNO, a fraction of exhaled nitric oxide;FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroid; IgE, immunoglobulin E; LABA, long-acting β2-agonist; LAMA, long-acting anti-muscarinic antagonist; LTRA, leukotriene receptorantagonist; OCS, oral corticosteroid; PPI, proton pump inhibitors.
MRM_02 original.qxp_Hrev_master 17/03/21 09:21 Pagina 30

18MRM
Multidisciplinary Respiratory Medicine 2021; 16:736 - N. Tani, et al.
sition [14,27]. These mechanisms are essential in airway hypersen-sitivity, which is a crucial part of the pathophysiology of severeasthma. Both IL-4Rα and IL-13Rα1 are expressed in B lympho-cytes, eosinophils, antigen-presenting cells, and bronchial epithe-lial cells, and consist of a heterodimeric receptor complex [28].The activation of the heterodimeric complex of IL-4Rα and IL-13Rα1 induces prompt stimulation of Janus kinase 1/2 (JAK 1/2)and tyrosine kinase 2 (Tyk2), followed by phosphorylation of sig-nal transducer and activator transcription 6 (STAT6) [29,30].Signal transduction through the cascade of JAK 1/2, Tyk2, and fol-lowing STAT6 is very quick; therefore, blocking IL-4 and/or IL-13is considered very promising. Anti-IL-13 antibodies tralokinumab[31] and lebrikizumab [32] failed to demonstrate consistent clini-cal benefits in phase 3 trials. On the other hand, treatments thatsolely target IL-4 have never proven efficacy in severe asthma[33,34]. Under circumstances where the inhibition of either IL-4 orIL-13 signaling is not effective in severe asthma, dual inhibition ofIL-4 and IL-13 with dupilumab demonstrated clinical benefit[24,25].
The early responders within 7 days after dupilumab treatment,consisting of 44.4% of all responders, could be explained by thebasic mechanism mentioned earlier. The dual inhibition of IL-4and IL-13 suppresses Th2 cell activation and iNOS induction,resulting in controlled airway hypersensitivity. These effects couldbe quickly noticed by patients considering prompt signal transduc-tion through JAK 1/2, Tyk2, and STAT6. The early efficacy ofdupilumab in moderate-to-severe atopic dermatitis has beenobserved in the pooled analysis of LIVERTY AD SOLO 1 and 2[15] within 1-3 days both subjective (by patient-reported itch) andobjective (by eczema area severity index), and combined analysisof SOLO 1 and 2, AD ADOL, and CHRONOS by day 2 in adultsand by day 5 in adolescents subjectively (daily peak pruritisnumerical rating scale score) [16]. Therefore, the observed earlyresponders to dupilumab treatment in severe asthma are concor-dant with both basic mechanisms and previously confirmed clini-cal effects on moderate-to-severe atopic dermatitis. In addition tothe dual inhibiting effect of dupilumab, the loading dose ofdupilumab on day 1 (600 mg) could have exerted a very rapideffect on asthma-associated symptoms, allowing systemic concen-trations to peak enough for strong suppression of IL-4 and IL-13signals before reaching a steady state.
There are some limitations to the current study. First, since thiswas a retrospective observational study design with limited samplesize and without controls (placebo), the bias may be higher com-pared to prospective studies with larger populations. Second, sincethe daily ACT is different from the original ACT, the definition of3 points of improvement as the minimal clinically important differ-ence over time in the daily ACT score has not been validated andneeds validation through prospective studies. Nevertheless, its def-inition was adopted in accordance with the original ACT. The dailyACT was feasible in the current study, which was in concordancewith the clinical course during the first 7 days, with all of the earlyresponders assessed by the daily ACT, resulting in effective ACTat week 8.
ConclusionsTaken together, the effect of dupilumab on severe asthma with
atopic features was observed within 7 days in 44.4% of the patientswho showed improvement in ACT scores after 8 weeks of treat-ment. Thus, the effect of dupilumab could have started earlier than2 weeks in severe asthma. Daily ACT may be useful in monitoringthe early efficacy of dupilumab in treating severe asthma.
AbbreviationsACT, asthma control test; ACQ, asthma control questionnaire; AQLQ, asthma quality of life questionnaire; BMI, body mass index; BT, bronchial thermoplasty; COPD, chronic obstructive pulmonary disease; FeNO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroid; Ig, immunoglobulin; iNOS, inducible nitric oxide synthase; IL, interleukin; IL-4Rα, IL-4 receptor-α subunit; IL-5Rα, IL-5 receptor-α subunit; IL-13Rα1, IL-13 receptor-α1 subunit; interleukin; ILC2, group 2 innate lymphoid cell; JAK 1/2, Janus kinase 1/2; LABA, long-acting β2-agonist; LAMA, long-acting anti-muscarinic antagonist;LTRA, leukotriene receptor antagonist; OCS, oral corticosteroid; PPI, proton pump inhibitor; PRO, patient-reported outcome; SD, standard deviation; STAT6, signal transducer and activator transcription 6; Th2, T helper-2; TSLP, thymic stromal lymphopoietin; Tyk2, tyrosine kinase 2; QOL, quality of life.
References 1. Global Initiative for Asthma, Global Strategy for Asthma
Management and Prevention. Updated 2020. Accessed on: 26June 2020. Available from: https://ginasthma.org/wp-content/uploads/2020/06/GINA-2020-report_20_06_04-1-wms.pdf
2. Hekking PP, Wener RR, Amelink M, Zwinderman AH, BouvyML, Bel EH. The prevalence of severe refractory asthma. JAllergy Clin Immunol 2015;135:896-902.
3. Chipps BE, Haselkorn T, Paknis B, Ortiz B, Bleecker ER,Kianifard F, et al. Epidemiology and natural history of asthma:Outcomes and Treatment Regimens Study Group. More than adecade follow-up in patients with severe or difficult-to-treatasthma: The epidemiology and natural history of asthma: out-comes and treatment regimens (TENOR) II. J Allergy ClinImmunol 2018;141:1590-7.
4. Kupczyk M, ten Brinke A, Sterk PJ, Bel EH, Papi A, ChanezP, et al. Frequent exacerbators--A distinct phenotype of severeasthma. Clin Exp Allergy 2014;44:212-21.
5. Mazalovic K, Jacoud F, Dima AL, Van Ganse E, Nolin MCD,Zaba C. The Astro-Lab Group. Asthma exacerbations andsocio-economic status in French adults with persistent asthma:A prospective cohort study. J Asthma 2018;55:1043-51.
6. Van Ganse E, Antonicelli L, Zhang, Q, Laforest L, Yin DD,Nocea G, et al. Asthma-related resource use and cost by GINAclassification of severity in three European countries. RespirMed 2006;100:140-7.
7. Sullivan PW, Ghushchyan VH, Globe G, Schatz M. Oral corti-costeroid exposure and adverse effects in asthmatic patients. J
MRM_02 original.qxp_Hrev_master 17/03/21 09:21 Pagina 31

19MRM
Multidisciplinary Respiratory Medicine 2021; 16:736 - N. Tani, et al.
Allergy Clin Immunol 2018;141:110-6.8. Fahy JV. Type 2 inflammation in asthma – present in most,
absent in many. Nat Rev Immunol 2015;15:57-65.9. Hirose K, Iwata A, Tamachi T, Nakajima H. Allergic airway
inflammation: key players beyond the Th2 cell pathway.Immunol Rev 2017;278:145-61.
10. Kuruvilla ME, Lee FE-H, Lee GB. Understanding asthma phe-notypes, endotypes, and mechanism of disease. Clin RevAllergy Immunol 2019;56:219-33.
11. D'Amato G, Stanziola A, Sanduzzi A, Liccardi G, Salzillo A,Vitale C, et al. Treating severe allergic asthma with anti-IgEmonoclonal antibody (omalizumab): a review. MultidiscipRespir Med 2014;9:23.
12. Menzella F, Lusuardi M, Galeone C, Zucchi L. Tailored thera-py for severe asthma. Multidiscip Respir Med 2015;10:1.
13. Busse WW. Biological treatments for severe asthma: A majoradvance in asthma care. Allergol Int. 2019; 68: 158-66.
14. Barranco P, Phillips-Angles E, Dominguez-Ortega J, Quirce S.Dupilumab in the management of moderate-to-severe asthma:the data so far. Ther Clin Risk Manag 2017;13:1139-49.
15. Thaçi, D, L Simpson E, Deleuran M, Kataoka Y, Chen Z,Gadkari A, et al. Efficacy and safety of dupilumab monothera-py in adults with moderate-to-severe atopic dermatitis: Apooled analysis of two phase 3 randomized trials (LIBERTYAD SOLO 1 and LIBERTY AD SOLO 2). J Dermatol Sci2019;94:266-75.
16. Silverberg JI, Yosipovitch G, Simpson EL, Kim BS, Wu JJ,Eckert L, et al. Dupilumab treatment results in early and sus-tained improvements in itch in adolescents and adults withmoderate to severe atopic dermatitis: Analysis of the random-ized phase 3 studies SOLO 1 and SOLO 2, AD ADOL, andCHRONOS. J Am Acad Dermatol 2020;82:1328-36.
17. Swigris JJ, Fairclough D. Patient-reported outcomes in idio-pathic pulmonary fibrosis research. Chest 2012;142:291-7.
18. Schatz M, Sorkness CA, Li JT, Marcus P, Murray JJ, NathanRA, et al. Asthma Control Test: Reliability, validity, andresponsiveness in patients not previously followed by asthmaspecialists. J Allergy Clin Immunol 2006;117:549-56.
19. Schatz M, Kosinski M, Yarlas AS, Hanlon J, Watson ME,Jhingran P. The minimally important difference of the asthmacontrol test. J Allergy Clin Immunol 2009;124:719-23.
20. Yancey SW, Keene ON, Albers FC, Ortega H, Bates S,Bleecker ER, et al. Biomarkers for severe eosinophilic asthma.J Allergy Clin Immunol 2017;140:1509-18.
21. Bjermer L, Alving K, Diamant Z, Magnussen H, Pavord I,Piacentini G, et al. Current evidence and future research needsfor FeNO measurement in respiratory diseases. Respir Med2014;108 830-41.
22. Matsunaga K, Hamada K, Oishi K, Yano M, Yamaji Y, HiranoT. Factors associated with physician-patient discordance in theperception of asthma control. J Allergy Clin Immunol Pract2019;7:2634-41.
23. Panagiotou M, Koulouris NG, Rovina N. Physical activity: Amissing link in asthma care. J Clin Med 2020;9:706.
24. Castro M, Corren J, Pavord ID, Maspero J, Wenzel S, RabeKF, et al. Dupilumab efficacy and safety in moderate-to-severeuncontrolled asthma. N Engl J Med 2018;378:2486-96.
25. Rabe KF, Nair P, Brusselle G, Maspero JF, Castro M, Sher L,et al. Efficacy and safety of dupilumab in glucocorticoid-dependent severe asthma. N Engl J Med 2018;378:2475-85.
26. Corren J, Castro M, Chanez P, Fabbri L, Joish VN, Amin N, etal. Dupilumab improves symptoms, quality of life, and produc-tivity in uncontrolled persistent asthma. Ann Allergy AsthmaImmunol 2019;122:41-9.
27. Barnes PJ. Targeting cytokines to treat asthma and chronicobstructive pulmonary disease. Nat Rev Immunol2018;18:454-66.
28. LaPorte SL, Juo ZS, Vaclavikova J, Colf LA, Qi X, Heller NM,et al. Molecular and structural basis of cytokine receptorpleiotropy in the interleukin-4/13 system. Cell 2008;132:259-72.
29. Oh CK, Geba GP, Molfino N. Investigational therapeutics tar-geting the IL-4/IL-13/STAT-6 pathway for the treatment ofasthma. Eur Respir Rev 2010;19:46-54.
30. Chiba Y, Goto K, Misawa M. Interleukin-13-induced activa-tion of signal transducer and activator of transcription 6 ismediated by activation of Janus kinase 1 in cultured humanbronchial smooth muscle cells. Pharmacol Rep 2012;64:454-8.
31. Panettieri RA Jr, Sjöbring U, Péterffy A, Wessman P, BowenK, Piper E, et al. Tralokinumab for severe, uncontrolled ssthma(STRATOS 1 and STRATOS 2): Two randomized, double-blind, placebo-controlled, phase 3 clinical trials. Lancet RespirMed 2018;6:511-25.
32. Hanania NA, Korenblat P, Chapman KR, Bateman ED,Kopecky P, Paggiaro P, et al. Efficacy and safety of lebrik-izumab in patients with uncontrolled asthma (LAVOLTA I andLAVOLTA II): Replicate, phase 3, randomized, double-blind,placebo-controlled trials. Lancet Respir Med 2016;4:781-96.
33. Wenzel S, Wilbraham D, Fuller R, Getz EB, Longphre M.Effect of an interleukin-4 variant on late-phase asthmaticresponse to allergen challenge in asthmatic patients: results oftwo phase 2a studies. Lancet 2007;370:1422-31.
34. Corren J, Busse W, Meltzer EO, Mansfield L, Bensch G,Fahrenholz J, et al. A randomized, controlled, phase 2 study ofAMG 317, an IL-4Ralpha antagonist, in patients with asthma.Am J Respir Crit Care Med 2010;181:788-96.
Received for publication: 21 November 2020. Accepted for publication: 23 February 2021.This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0).©Copyright: the Author(s), 2021Licensee PAGEPress, ItalyMultidisciplinary Respiratory Medicine 2021; 16:736doi:10.4081/mrm.2021.736
MRM_02 original.qxp_Hrev_master 17/03/21 09:21 Pagina 32
20MRM
Efficacy of low-dose valganciclovir in CMV R+ lung transplant recipients: a retrospective comparative analysisJessica Hunt,1 Kristina M. Chapple,2 Aasya Nasar,1 Lauren Cherrier,1 Rajat Walia3
1Department of Pharmacy; 2Department of Biostatistics and Neurosurgery; 3Department of Pulmonology, St. Joseph’sHospital and Medical Center, Phoenix AZ, USA
Background: Cytomegalovirus (CMV) infection is extremely common after lung transplant and can be associatedwith significant morbidity and mortality. Current practice suggests the use of 900 mg daily of valganciclovir for CMVprophylaxis, but there is no literature assessing whether 450 mg daily of valganciclovir is sufficient in intermediateCMV risk lung transplant recipients. Therefore, we sought to assess the role of low-dose valganciclovir (LDV) versushigh-dose valganciclovir (HDV) prophylaxis in intermediate-risk (R+) recipients. Methods: We conducted a retrospective analysis on lung transplant recipients at the Norton Thoracic Institute inPhoenix, Arizona looking at intermediate-risk patients that received either valganciclovir 450 mg per day (LDV) or900 mg/day (HDV). All patients were followed for 1 year post-transplant for incidence of CMV viremia. The primaryoutcome was the rate of CMV viremia as determined by a positive CMV polymerase chain reaction ([PCR] >2.7 logcopies/mL). Secondary outcomes included rate of adverse events, acute cellular rejection, and mortality. Results: The primary analysis included 103 patients (55 in the LDV group, 48 in the HDV group). In the LDV group,9 patients (16.4%) developed CMV viremia compared to 4 (8.3%) in the HDV group (p=0.221) with no differenceobserved in adverse event rates between groups. Conclusion: There was no statistical difference between groups for the primary outcome. However, the effect sizedemonstrated in this analysis may be of clinical relevance and valganciclovir 450 mg daily would not be recommendedin intermediate risk lung transplant recipients at this time. To confirm our results, further prospective studies enrollinglarger patient populations are necessary.
Key words: Cytomegalovirus; lung transplantation; valganciclovir.
AB
STR
ACT
Correspondence: Lauren Cherrier, PharmD, St. Joseph’s Hospital and Medical Center, 350 W Thomas Rd, Phoenix, AZ85013, USA. Tel. +1.602.406.3000 - Fax: +1.602.512.6647.E- mail: [email protected]
Contributions: All authors made substantial contributions to the conception of the work; the acquisition, analysis, and inter-pretation of data; and the drafting and revision of the article. All authors approved the final version of the article for publica-tion.
Conflict of interest: This study contains no off-label use of valganciclovir, and none of the authors has a financial relationshipwith a commercial entity that has an interest in the subject of the presented material or other conflicts of interest to disclose.
Funding: No funding was received for this study.
Availability of data and materials: Individuals interested in viewing the raw data analyzed in this manuscript are encouraged tocontact the corresponding author.
Ethics approval and consent to participate: This study was approved by the Institutional Review Board at St. Joseph’sHospital and Medical Center in Phoenix, Arizona, USA.
Consent for publication: Not applicable.
ORIGINAL RESEARCH ARTICLE
®Multidisciplinary Respiratory Medicine 2021; volume 16:706
MRM_02 original.qxp_Hrev_master 25/01/21 09:46 Pagina 1

21MRM
Multidisciplinary Respiratory Medicine 2021; 16:706 - J. Hunt et al.
IntroductionCytomegalovirus (CMV) is one of the most common infec-
tions after solid organ transplantation and is associated with highmorbidity and mortality [1]. In addition to the detrimental effectsof CMV tissue invasion, the infection also places transplant recip-ients at a higher risk of rejection. Valganciclovir is currently thestandard of care for CMV prophylaxis and treatment [2]. Whileguidelines recommend 900 mg daily for intermediate risk patients,they also mention the use 450 mg daily, which has been studied inthe kidney transplant population. The guidelines state that there iscurrently no data to support or contradict the use of 450 mg dailydosing for intermediate risk lung transplant patients and the lungtransplant studies referenced do not address varying doses of val-ganciclovir in this population [3]. The lung transplant specificstudies primarily focused on comparing valganciclovir to a histor-ical control (ganciclovir) or assessing the duration of prophylaxiswith 900 mg valganciclovir daily [4-8].
The majority of the data regarding CMV prophylaxis dosing inthe lung transplant population are extrapolated from renal trans-plant studies [9-13]. However, this comparison may not be appro-priate, as pulmonary tissue is inherently more susceptible to CMVinfection. The reported incidence of CMV infection in lung trans-plant patients without prophylaxis has been reported to be as highas 54% to 92% (compared to less than 50% in kidney transplantpatients) [14]; therefore, direct comparisons across transplantedorgans may not be appropriate. Although some studies have shownbenefit with low-dose strategies in low- and intermediate-riskpatients, many of those same studies raise concern for higher ratesof CMV viremia and resistance [10,11,13,15].
In accordance with the renal transplant findings, and in anattempt to limit drug costs and adverse events such as leukopenia,our center used 450 mg valganciclovir daily as prophylaxis inintermediate-risk patients beginning in 2010. In 2017, our centerincreased our prophylaxis dose to 900 mg daily due to suspectedhigher rates of CMV viremia in this population. This study was
conducted to review the change in protocol, to evaluate the mostappropriate prophylactic regimen, and to determine whether val-ganciclovir 450 mg daily can be used effectively in intermediaterisk lung transplant patients.
MethodsThis study was approved by the Institutional Review Board at
St. Joseph’s Hospital and Medical Center in Phoenix, Arizona,USA. We retrospectively assessed the difference between 2 groupsof lung transplant recipients who received different valganciclovirCMV prophylaxis protocols after undergoing a lung transplant atthe Norton Thoracic Institute (NTI) in Phoenix, Arizona, USA.Patients were assigned to regimens based on their risk of CMV asdetermined by their pre-transplant CMV serology. The focus ofthis analysis was on intermediate risk (R+) patients. Patientsundergoing transplant between March 2016 and December 2016were designated as the low dose valganciclovir (LDV) CMV pro-phylaxis group and received 450 mg daily. In February 2017, NTIrevised its institutional protocol to a high dose valganciclovir(HDV) regimen, where intermediate recipients received 450 mgtwice daily. This group was classified as patients that underwenttransplant from March 2017 to December 2017 (Figure 1). Datafrom January and February of 2017 were excluded for simplicityto allow for appropriate time for education and implementation ofthe new protocol. In both protocols, valganciclovir began on day 4posttransplant, and continued indefinitely. Baseline characteristics,efficacy, adherence, and adverse events were all collected retro-spectively for both groups. The primary outcome was the rate ofCMV viremia as determined by a positive CMV polymerase chainreaction ([PCR] >2.7 log copies/mL). Secondary outcome meas-ures included leukopenia (white blood cell nadir and quarterlyaverages), renal function (peak serum creatinine, quarterly aver-ages, and associated creatinine clearance), biopsy-confirmed rejec-tion (Grade A1-A4), and mortality. CMV PCR was assessed week-
Figure 1. Study groups. HDV, high-dose valganciclovir; LDV, low-dose valganciclovir.
MRM_02 original.qxp_Hrev_master 25/01/21 09:46 Pagina 2

22MRM
Multidisciplinary Respiratory Medicine 2021; 16:706 - J. Hunt et al.
ly while patients were in the hospital and with routine labs post-transplant at months 1, 3, 6, and 12.
Protocol adherence was monitored both inpatient and at outpa-tient clinic visits based on whether patients were receiving the cor-rect dose of valganciclovir. However, due to the retrospectivenature of this study, it was not possible to accurately assess patientcompliance. Therefore protocol adherence was based solely onprovider adherence to the specified protocol. Although there is nospecific renal adjustment protocol for valganciclovir at our institu-tion, patients with a regimen adjusted for renal function using stan-dardized creatinine clearance cutoffs were considered adherent.Adjustments for hepatic dysfunction, or thrombocytopenia, how-ever, were considered non-adherent to the protocol, as these adjust-ments were not considered standard for valganciclovir.
Means and standard deviation were used for continuous vari-able data. Percentages were used for categorical variables, includ-ing baseline characteristics. Chi-square and t-tests were used toassess primary and secondary outcomes. A p-value of <0.05 indi-cated statistical significance.
ResultsA total of 103 intermediate-risk patients (55 in the LDV group
and 48 in the HDV group) were included in the primary analysis.Patients were well matched for age, pre-transplant diagnosis, andlung allocation scores (Table 1). The majority of patients under-went bilateral lung transplant and received either basiliximab orthe combination of rituximab and intravenous immunoglobulin forinduction therapy. All patients were started on prednisone,mycophenolate mofetil, and tacrolimus for maintenance immuno-suppression. Overall, no difference was seen in the rate of protocoladherence for either group in the first year posttransplant. In theLDV and HDV groups, patients were prescribed the appropriateper-protocol prophylaxis regimen more than 80% of the time
(85.3% vs 81.29% respectively, p=0.47). For the primary efficacyoutcome, 9 of 55 (16.4%) patients in the LDV group developedCMV viremia (positive CMV PCR); whereas 4 of the 48 patientsin the HDV group developed CMV viremia (8.3%; p=0.221; Table2). At the time of the primary outcome there were disparitiesbetween groups for protocol adherence. Of the HDV patients whodeveloped a positive CMV PCR, only 2 out of 4 were adherentwith the protocol regimen at the time of the positive PCR result.The other two patients had not started valganciclovir therapy: onepatient had a positive PCR at day 3 posttransplant (prior to ourstandard initiation on day 4); the other patient had a positive PCRat day 11 posttransplant - this patient had valganciclovir withhelddue to postoperative leukopenia. Given the few number of patients(only 50%) in the intervention group on therapy at the time of thepositive PCR, an exploratory outcome was conducted. In the perprotocol analysis nine LDV patients (16.4%) had a positive PCR,compared to 2 patients (4.16%) in the HDV group (p=0.054).
There were no major differences in secondary outcomes forboth groups. Average peak serum creatinine in the year followingtransplant were similar: 1.94 mg/dL in the LDV group vs 1.92mg/dL in the HDV group (p=0.95). The average worst creatinineclearance throughout the year was consequently well matched.Leukopenia was similar between groups, with an average nadir of3.82 and 2.82 in the LDV and HDV groups, respectively(p=0.211). Rejection and mortality rates remained consistent forboth patient populations. Biopsy-confirmed rejection rates weresimilar at 38.2% (21/55) in the LDV and 41.6% (20/48) in theHDV groups (p=0.65). The rate of mortality was less than 10% ineach group; LDV group: 7.3%; HDV group: 8.3% (p=0.84).
DiscussionOverall, this study showed a numerical reduction in the rate of
CMV viremia after implementation of the new protocol. Though
Table 1. Baseline data for 103 patients at intermediate risk for developing CMV infection after lung transplant.
Clinical characteristics LDV (n=55) HDV (n=48) p
Mean age, years ± SD 59.22 ± 13.3 60.52 ± 15.4 0.65Mean lung allocation score ± SD 43.7 ± 15.1 44.3 ± 16.7 0.84Mean serum creatinine, mg/dl ± SD 0.68 ± 0.2 0.63 ± 0.1 0.12Mean creatinine clearance, ml/min ± SD 92.89 ± 36.5 90.9 ± 43.4 0.80Transplant type Unilateral, n (%) 0 (0.0) 2 (4.2) - Bilateral, n (%) 55 (100.0) 45 (93.8) - Retransplant, n (%) 6 (10.9) 4 (8.3) -Pre-transplant diagnosis, n (%)* Pulmonary fibrosis 25 (45.5) 24 (50.0) 0.65 Pulmonary hypertension 5 (9.1) 5 (10.4) 0.82 COPD 17 (30.9) 12 (25.0) 0.51 Cystic fibrosis 4 (7.3) 4 (8.3) 0.84 Rejection 6 (10.9) 4 (8.3) 0.66 Other 3 (5.5) 8 (16.7) 0.07Induction agents, n (%) 0.029° Rituximab/IVIG 21 (38.2) 9 (18.8) -- Basiliximab 30 (54.5) 38 (79.2) -- Thymoglobulin 4 (7.3) 1 (2.1) - Cytomegalovirus immune globulin use, n (%) 26 (47.3) 3 (6.3) <0.001
LDV, low-dose valganciclovir; HDV, high-dose valganciclovir; *some values total more than 100% due to overlap in disease categories; °the overall χ2 was significant; however, based on standardized resid-uals there were no statistical differences for individual induction agents; COPD, chronic obstructive pulmonary disease; IVIG, intravenous immunoglobulin.
MRM_02 original.qxp_Hrev_master 25/01/21 09:46 Pagina 3

23MRM
Multidisciplinary Respiratory Medicine 2021; 16:706 - J. Hunt et al.
the primary outcome was not statistically significant, the findingsin this analysis may have clinical relevance. This study demon-strated a roughly 50% reduction in the rate of CMV viremia forpatients receiving HDV.
A major strength of the present study was its closely matchedbaseline characteristics, which increases the internal validity of ourpatient population. In addition, our patient population has goodexternal validity. In accordance with national trends, the mostcommon pre-transplant diagnosis in our cohort was fibrotic lungdisease, followed by chronic obstructive pulmonary disease [16].In addition, the present study evaluated multiple parameters thatmay influence development of CMV viremia, including protocoladherence, immunosuppression, and medication adjustments inresponse to leukopenia, renal dysfunction, or rejection. Adherencewith the prophylaxis regimen was previously reported.Discrepancies between groups were adjusted for with the assess-ment of the exploratory outcome, per-protocol CMV viremia. Inaddition, differences in the amount of immunosuppressionbetween groups did not appear to be a confounding factor in thepresent study as all patients with a positive CMV PCR received thesame maintenance immunosuppression with tacrolimus, mycophe-
nolate mofetil, and prednisone. In those patients who developedCMV viremia, just 1 patient in each group had a tacrolimus levelabove the goal at the time of the positive PCR (levels were still lessthan 14 ng/ml), so excessive immunosuppression does not appearto be a major confounder in this analysis. During the period ofincreased immunosuppression immediately posttransplant, the riskof infection is consequently higher [2,14]. As expected, this wasdemonstrated in our study, as CMV viremia was more commonearly after transplant. The average onset of CMV viremia was 32days posttransplant (range: 3-113).
The present study has some limitations. Its retrospective non-randomized design made it difficult to control for potential con-founding variables. One potential confounder was the difference inthe use of CMV immunoglobulin between groups. Our institution’snew protocol also involved stopping the administration of CMVimmunoglobulin. Within the LDV group, 47.3% of patientsreceived cytomegalovirus immune globulin versus just 7% in theHDV group (p≤0.001). Based on the described mechanism ofCMV immunoglobulin, it is reasonable to expect this discrepancyto influence reduced rates of CMV viremia in the LDV group;however, this was not the case. High-risk and low-risk patients at
Table 2. Outcomes of 103 patients at intermediate risk for CMV infection, based on prophylaxis protocol used.
Variable* LDV (n=55) HDV (n=48) p
Percent adherence 85.3 ± 27.6 81.3 ± 28.3 0.47CMV viremia, n (%) 9 (16.4) 4 (8.3) 0.22Following protocol at the time of positive PCR, n (%) 9/9 (100.0) 2/4 (50.0) -Per-protocol CMV viremia, n (%) 9 (16.4) 2 (4.2) 0.05Biopsy-confirmed rejection, n (%) 21 (38.2) 20 (41.7) 0.65Death, n (%) 4 (7.3) 4 (8.3) 0.84Peak serum creatinine, mg/dl 1.94 ± 1.1 1.92 ± 1.3 0.95Lowest creatinine clearance, ml/min 45.4 38.3 0.29Mean SCr Quarter 1, mg/dl 1.0 ± 0.6 0.9 ± 0.3 0.29Mean SCr Quarter 2, mg/dl 1.2 ± 0.3 1.1 ± 0.6 0.46Mean SCr Quarter 3, mg/dl 1.8 ± 3.8 3.4 ± 12.8 0.47Mean SCr Quarter 4, mg/dl 1.9 ± 4 2.8 ± 9.5 0.59Mean WBC nadir, cells/µl 3.4 X 103 ± 2.4 X 103 2.8 X 103 ± 2.17 X 103 0.21Mean time to WBC nadir, days 157 ± 114.1 165 ± 115.4 0.74Nadir categories, n (%) 0.76 ≥ 3000 cells/µl 18 (32.7) 13 (27.1) - 2000-2999 cells/µl 20 (36.3) 16 (33.3) - 1000-1999 cells/µl 13 (23.6) 13 (27.1) - <1000 cells/µl 4 (8.0) 6 (12.5) -Mean WBC Quarter 1, cells/µl 10.3 X 103 ± 2.5 X 103 9.9 X 103 ± 2.9 X 103 -Mean WBC Quarter 2, cells/µl 5.2 X 103 ± 1.8 X 103 5.1 X 103 ± 2.5 X 103 -Mean WBC Quarter 3, cells/µl 4.8 X 103 ± 1.9 X 103 4.3 X 103 ± 1.6 X 103 -Mean WBC Quarter 4, cells/µl 5.0 X 103 ± 1.8 X 103 4.4 X 103 ± 1.9 X 103 -Renal adjustments: Decreased, n (%) Valganciclovir 16 (29.1) 25 (52.1) - Sulfamethoxazole/trimethoprim 28 (50.9) 18 (37.5) - Immunosuppression goals 11 (20.0) 4 (8.3) -Leukopenia adjustments Decreased valganciclovir 8 (14.5) 12 (25.0) - Adjusted other medications° 19 (34.5) 23 (47.9) -
*Values shown as mean ± SD, unless indicated otherwise; LDV, low-dose valganciclovir; HDV, high-dose valganciclovir; CMV, cytomegalovirus; PCR, polymerase chain reaction; SCr, serum creatinine; WBC,white blood cells; °adjustments included decreasing or holding mycophenolate mofetil; decreasing or holding sulfamethoxazole/trimethoprim, changing sulfamethoxazole/trimethoprim to atovaquoneor pentamidine, or giving a granulocyte-colony stimulating factor.
MRM_02 original.qxp_Hrev_master 25/01/21 09:46 Pagina 4

24MRM
Multidisciplinary Respiratory Medicine 2021; 16:706 - J. Hunt et al.
our institution (who did not undergo valganciclovir dose adjust-ments), demonstrated no change in rates of CMV viremia from onestudy period to the next, regardless of institutional adjustments tocytomegalovirus immunoglobulin. Previously published studiesalso support our findings, demonstrating a lack of benefit in termsof CMV infection rates after cytomegalovirus immunoglobulinadministration [17-19]. This finding suggests that immunoglobulinuse did not act as a major confounder in our analysis, as anticipat-ed. Given the lack of demonstrated benefit in our study and in theliterature, we currently recommend against its regular use forCMV prophylaxis in lung transplant recipients. Although our insti-tution has general recommendations for adjusting valganciclovirfor renal function, adjustments could not be entirely controlled fordue to the retrospective nature of this analysis. Ultimately, adjust-ments occurred according to provider discretion and not a speci-fied protocol. In the HDV group, valganciclovir appeared morelikely to be reduced secondary to renal dysfunction than in theLDV group, in which sulfamethoxazole/trimethoprim, immuno-suppression, and other nephrotoxic agents were typically adjustedfirst. On the other hand, there did not appear to be a major differ-ence between groups in adjustments made secondary to leukope-nia. The present study was not sufficiently powered to detect a dif-ference in the primary outcome (current power calculation: 15%).It is anticipated that 282 intermediate-risk patients would berequired in each treatment group in order to achieve 80% power forthe primary outcome. Our institution performs between 80 and 100transplants per year; therefore, it would take roughly 3 years ofpatient enrollment in each group to achieve adequate power,according to the above calculation (4 years total, including follow-up). To date, the new protocol has been in effect for 2 years.Despite the power limitation, this study does have a much largersample size compared to previously published literature in the lungtransplant population.
Overall, this analysis showed a trend toward benefit with thehigh-dose valganciclovir regimen. This benefit was evidenced byfewer cases of CMV viremia with no increase in adverse events.Even though the literature in kidney transplant has shown utility indosing valganciclovir 450 mg daily for their intermediate risk pop-ulation, we did not find the same outcome in the lung transplantpopulation. This research provides further insight into prophylacticdosing in lung transplant patients (specifically those classified asintermediate risk based on pre transplant serology), with an effectsize for the primary outcome that may be clinically relevant andthat adds to the body of literature supporting higher doses of val-ganciclovir for these patients. Future analyses will target largerpatient populations in a prospective trial design to correct forpotential confounders in the present study (i.e., immunoglobulinuse, medication adjustments, and compliance). Study outcomeswill further assess high dose vs low dose efficacy in addition tooptimum duration of therapy.
AbbreviationsCMV: cytomegalovirus;HDV: high-dose valganciclovir;LDV: low-dose valganciclovir;PCR: polymerase chain reaction.
References1. Avidan Y, Paul M, Rahamimov R, Bishara J, Samra Z, Edna S,
et al. Selective low-dose valganciclovir for prevention ofcytomegalovirus disease following kidney transplantation. JInfect 2008;57:236-40.
2. Kotton C, Kumar D, Caliendo A, Huprikar S, Chou S,Danziger-Isakov L, et al. The Third International ConsensusGuidelines on the Management of cytomegalovirus in solid-organ transplantation. Transplantation 2018;102:900-31.
3. Razonable R, Humar A. Cytomegalovirus in solid organ trans-plantation. Am J Transplant 2013;13:s93-106.
4. Finlen Copeland C, Davis W, Snyder L, Banks M, Avery R,Davis R, et al. Long-term efficacy and safety of 12 months ofvalganciclovir prophylaxis compared with 3 months after lungtransplantation: A single-center, long-term follow-up analysisfrom a randomized, controlled cytomegalovirus preventiontrial. J Heart Lung Transpl 2011;30:990-6.
5. Humar A, Kumar D, Preiksaitis J, Boivin G, Siegal D, FentonJ, et al. A trial of valganciclovir prophylaxis forcytomegalovirus prevention in lung transplant recipients. Am JTransplant 2005;5:1462-8.
6. Jaksch P, Zweytick B, Kerschner H, Hoda A, Keplinger M,Lang G, et al. Cytomegalovirus prevention in high-risk lungtransplant recipients: Comparison of 3- vs 12-month valganci-clovir therapy. J Heart Lung Transplant 2009;28:670-5.
7. Palmer S, Limaye A, Banks M, Gallup D, Chapman J,Lawrence E, et al. Extended valganciclovir prophylaxis to pre-vent cytomegalovirus after lung transplantation. Ann of InternMed 2010;152:761.
8. Zamora M, Nicolls M, Hodges T, Marquesen J, Astor T, GraziaT, et al. Following universal prophylaxis with intravenous gan-ciclovir and cytomegalovirus immune globulin, valgancicloviris safe and effective for prevention of CMV infection follow-ing lung transplantation. Am J Transplant 2004;4:1635-42.
9. Chamberlain C, Penzak S, Alfaro R, Wesley R, Daniels C,Hale D, et al. Pharmacokinetics of low and maintenance dosevalganciclovir in kidney transplant recipients. Am J Transplant2008;8:1297-302.
10. Heldenbrand S, Li C, Cross R, DePiero K, Dick T, Ferguson K,et al. Multicenter evaluation of efficacy and safety of low-doseversus high-dose valganciclovir for prevention ofcytomegalovirus disease in donor and recipient positive(D+/R+) renal transplant recipients. Transpl Infect Dis2016;18:904-12.
11. Khan S, Sullivan T, Ali M, Dunn D, Patel G, Huprikar S. Low-dose valganciclovir for cytomegalovirus prophylaxis in inter-mediate-risk liver transplantation recipients. Liver Transpl2018;24:616-2. A
12. Le Page A, Jager M, Kotton C, Simoons-Smit A, Rawlinson W.International survey of cytomegalovirus management in solidorgan transplantation after the publication of consensus guide-lines. Transplantation 2013;95:1455-60.
13. Stevens D, Sawinski D, Blumberg E, Galanakis N, Bloom R,Trofe-Clark J. Increased risk of breakthrough infection amongcytomegalovirus donor-positive/recipient-negative kidneytransplant recipients receiving lower-dose valganciclovir pro-phylaxis. Transpl Infect Dis 2015;17:163-73.
14. Azevedo L, Pierrotti L, Abdala E, Costa S, Strabelli T, CamposS, et al. Cytomegalovirus infection in transplant recipients.Clinics 2015;70:515-23.
15. Eid A, Arthurs S, Deziel P, Wilhelm M, Razonable R.Emergence of drug-resistant cytomegalovirus in the era of val-ganciclovir prophylaxis: therapeutic implications and out-comes. Clin Transplant 2007;22:162-70.
16. Egan T, Edwards L. Effect of the lung allocation score on lungtransplantation in the United States. J Heart Lung Transplant
MRM_02 original.qxp_Hrev_master 25/01/21 09:46 Pagina 5

25MRM
Multidisciplinary Respiratory Medicine 2021; 16:706 - J. Hunt et al.
2016;35:433-9. 17. Kruger R, Paranjothi S, Storch G, Lynch J, Trulock E. Impact
of prophylaxis with cytogam alone on the incidence of CMVviremia in CMV-seropositive lung transplant recipients. JHeart Lung Transplant 2003;22:754-63.
18. Rea F, Potena L, Yonan N, Wagner F, Calabrese F.Cytomegalovirus hyper immunoglobulin for CMV prophylax-is in thoracic transplantation. Transplantation 2016;100:S19-
26. 19. Aguado J, Gomez-Sanchez M, Lumbreras C, Delgado J,
Lizasoain M, Otero J, et al. Prospective randomized trial ofefficacy of ganciclovir versus that of anti-cytomegalovirus(CMV) immunoglobulin to prevent CMV disease in CMV-seropositive heart transplant recipients treated with OKT3.Antimicrob Agents Chemother 1995;39:1643-5.
Received for publication: 3 August 2020. Accepted for publication: 21 December 2020.This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0).©Copyright: the Author(s), 2021Licensee PAGEPress, ItalyMultidisciplinary Respiratory Medicine 2021; 16:706doi:10.4081/mrm.2021.706
MRM_02 original.qxp_Hrev_master 25/01/21 09:46 Pagina 6

26MRM
The Global Usability Score Short-Form for the simplified assessment of dry powderinhalers (DPIs) usabilityMassimiliano Povero,1 Paola Turco,2 Luca Bonadiman,3 Roberto W. Dal Negro3
1AdRes Health Economics and Outcome Research, Turin2Research & Clinical Governance, Verona 3National Centre for Respiratory Pharmacoeconomics and Pharmacoepidemiology, Verona, Italy
Background: The choice of the Dry Powder Inhaler (DPI) to prescribe is a critical issue. The estimation of DPIsusability depends on the objective assessment of several indices related to both subjective and objective determinants.The Global Usability Score (GUS) Questionnaire is a comprehensive tool usable for checking, comparing, and rankinginhalers’ usability objectively in real life, but it takes some time to fill. Aim: The aim of this study was to favour the quicker check of DPIs usability in clinical practice by means of a sim-plified short-form GUS (S-GUS) Questionnaire, while maintaining the high specificity and sensitivity of the original,extended version of the Questionnaire (O-GUS questionnaire). Methods: The usability of the six most prescribed DPIs was assessed in 222 patients with persistent airway obstructionand needing long-term inhalation treatments. LASSO regression and multicollinearity test were used to select the sub-set of questions of the O-GUS questionnaire, with the highest information power. Each item was then scored using thecorresponding coefficient in the linear regression (normalized at 50 as the O-GUS score). Agreement between the orig-inal and the short-form questionnaire was evaluated using the Cohen’s kappa statistic (κ). The overall S-GUS valuesobtained for each DPI were then compared to those from the O-GUS, in the same patients, using a Bayesian indirectcomparison (IC) model. Results: After the statistical selection of the items mostly contributing to the overall score, the novel S-GUS question-naire consists of twelve items only. Nine items are related to patients’ opinion before DPIs handling, and three to thenurse’s assessment after DPIs practicality. O-GUS and S-GUS score were strongly correlated (R2=0.9843, p<0.0001)and the usability score calculated for each DPI by means of the O- and of S- GUS overlapped almost completely(κ=84.5%, 95% CI 81.3% to 89.2%). Furthermore, S-GUS was much faster to complete than O-GUS (mean time 6.1vs 23.4 minutes, p<0.001). Estimates of S-GUS, obtained from the IC model, allowed to propose a simple classifica-tion of usability: “good” by GUS values >25; “pretty good” by values ≤25≥15, and “insufficient” by values <15.Conclusions: The S-GUS proves as much specific and suitable as the extended O-GUS questionnaire in measuringDPIs usability, while maintaining the same high sensitivity. As the time required for its use is quite shorter, S-GUS isalso particularly suitable and helpful in current clinical practice.
Key words: Inhalation devices; dry powder inhalers; usability; global usability score; GUS; GUS short-form;bronchial asthma; COPD.
Correspondence: Massimiliano Povero, AdRes Health Economics and Outcome Resources, Via Vittorio Alfieri 17, 10121Torino, Italy. E-mail: [email protected]: All authors read and approved the final manuscript.Conflict of interest: The authors declare that they have no competing interests. RWD is Associate Editor of MultidisciplinaryRespiratory Medicine.Funding: Not applicable.Availability of data and materials: Authors do not wish to share their data without their permission.Ethics approval and consent to participate: This study was approved by the Ethical and Scientific Commission of theNational Centre for Respiratory Pharmacoeconomics and Pharmacoepidemiology during the session of January 4th, 2016 (# RD011/G01/16). All subjects gave their written informed consent.Consent for publication: All subjects gave their written informed consent to the study.
ORIGINAL RESEARCH ARTICLE
Multidisciplinary Respiratory Medicine 2020; volume 15:659A
BST
RA
CT
MRM_01 original.qxp_Hrev_master 22/07/20 10:44 Pagina 48

27MRM
Multidisciplinary Respiratory Medicine 2020; 15:659 - M. Povero et al.
Introduction The evidence that inhalers, and Dry Powder Inhalers (DPIs) in
particular, may affect per sé therapeutic outcomes independentlyof the drug(s) prescribed is consolidated [1-5]. On the other hand,it has also been stated that patients are not able to use all DPIsequally well [5-8]. As a consequence, the achievement of a deeperawareness of inhalers’ usability should then be increasingly pur-sued together with a dedicated specific training as priority issues[6-9]. The empowerment of patients who need inhalation therapyhas risen remarkably in the last decade, particularly in favour ofthose individuals requiring long-term treatments for managingtheir persistent airway obstruction (such as: Bronchial Asthma andChronic Obstructive Pulmonary Disease - COPD).
The choice of the convenient DPI to prescribe still represents acrucial issue in real-life because it is too frequently affected byhighly empiric decisions in clinical practice [7-8].
The critical factors contributing to the effectiveness of inhalationtreatments via DPIs are various and of different origin (Figure 1).Differently from the past, the primary role of patients’ viewpointgreatly concentrated the attention in recent years, and the determi-nants of incorrect inhalation were frequently investigated [9-10].Patients’ preference, acceptance, and satisfaction were mostlyassigned to criteria strictly related to their current subjectivity andbeliefs (such as: age, psychological profile, socio-economic status,cognition, educational level, physical limitations) [11-17], despitethe low number of studies assessing the objective correspondencebetween the patients’ beliefs and the real-life usability of inhalersby means of quantitative tools [11,14,18]. However, unlike thosebelonging to the domain of subjectivity, other criteria are involvedin determining the appropriate utilization of DPIs, particularlythose that are almost completely independent of the sole patients’point of view: the intrinsic structure of the device, the number andthe complexity of manoeuvres required for their actuation, thequality and the duration of the educational training received, etc.
Novel and more comprehensive instruments of investigationshould then be suggested and expected in order to provide a moreobjective check of inhalers usability. At present, the Global
Usability Score (GUS), which is obtained by means of the specificGUS Questionnaire, represents the first comprehensive tool forassessing, ranking, and comparing inhalers’ usability objectively,thus greatly contributing to the effective and motivated standard ofchoice in real life [19-23]. However, even if characterized by a>97% comprehension at the first reading, the original, extendedversion of GUS Questionnaire (O-GUS) consisting of 27 ques-tions, obviously requires some time to be properly filled, and thisfact may likely limit its wider use in clinical practice.
Aim of the present study was the definition and the validationof the simplified short-form GUS Questionnaire (S-GUS) in orderto favour the effective and quick assessment of DPIs usability indaily clinical activities, while maintaining the same high specifici-ty and sensitivity of the O-GUS Questionnaire.
Materials and MethodsA cluster of 222 original, extended GUS questionnaires (con-
sisting in 27 items; 22 questions requiring the patients’, and theremaining 5 the nurse’s direct involvement) already used in a pre-vious investigation [24] aimed to assess and compare the usabilityof the six most used DPIs (Breezhaler, Diskus, Ellipta, Nexthaler,Spiromax, and Turbohaler randomly grouped) was used. Thisstudy was approved by the Ethical and Scientific Commission ofthe National Centre for Respiratory Pharmacoeconomics andPharmacoepidemiology during the session of January 4th, 2016 (#RD 011/G01/16).
The association between the 27 items of the O-GUS question-naire and the GUS scores was investigated using a Least AbsoluteShrinkage and Selection Operator (LASSO) regression model.The LASSO regression minimizes the residual sum of squares sub-jects to the sum of the absolute value of the coefficients being lessthan a constant [25]. Because of the nature of this constraint, ittends to produce some coefficients that are exactly zero and henceit permits to discard redundant covariates. LASSO regression isrecommended with respect to automated variable selection algo-rithms as backward elimination, forward selection or stepwise
Figure 1. The multiple aspects affecting DPIs usability.
MRM_01 original.qxp_Hrev_master 22/07/20 10:44 Pagina 49
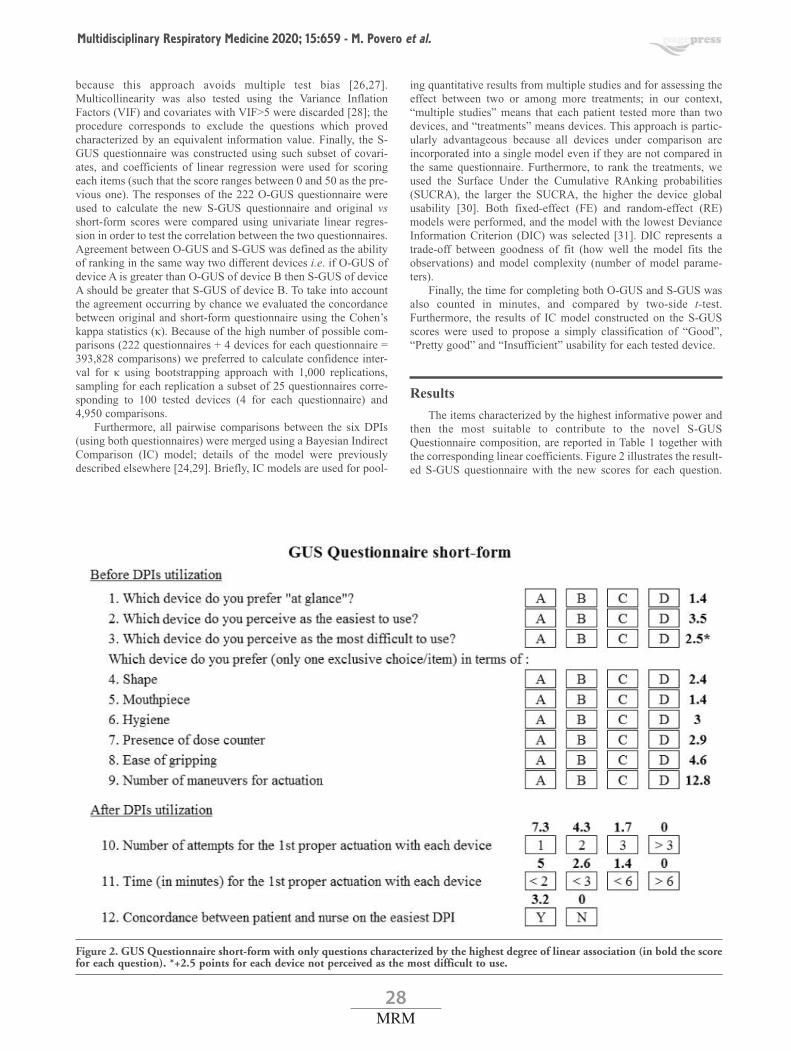
28MRM
Multidisciplinary Respiratory Medicine 2020; 15:659 - M. Povero et al.
because this approach avoids multiple test bias [26,27].Multicollinearity was also tested using the Variance InflationFactors (VIF) and covariates with VIF>5 were discarded [28]; theprocedure corresponds to exclude the questions which provedcharacterized by an equivalent information value. Finally, the S-GUS questionnaire was constructed using such subset of covari-ates, and coefficients of linear regression were used for scoringeach items (such that the score ranges between 0 and 50 as the pre-vious one). The responses of the 222 O-GUS questionnaire wereused to calculate the new S-GUS questionnaire and original vsshort-form scores were compared using univariate linear regres-sion in order to test the correlation between the two questionnaires.Agreement between O-GUS and S-GUS was defined as the abilityof ranking in the same way two different devices i.e. if O-GUS ofdevice A is greater than O-GUS of device B then S-GUS of deviceA should be greater that S-GUS of device B. To take into accountthe agreement occurring by chance we evaluated the concordancebetween original and short-form questionnaire using the Cohen’skappa statistics (κ). Because of the high number of possible com-parisons (222 questionnaires + 4 devices for each questionnaire =393,828 comparisons) we preferred to calculate confidence inter-val for κ using bootstrapping approach with 1,000 replications,sampling for each replication a subset of 25 questionnaires corre-sponding to 100 tested devices (4 for each questionnaire) and4,950 comparisons.
Furthermore, all pairwise comparisons between the six DPIs(using both questionnaires) were merged using a Bayesian IndirectComparison (IC) model; details of the model were previouslydescribed elsewhere [24,29]. Briefly, IC models are used for pool-
ing quantitative results from multiple studies and for assessing theeffect between two or among more treatments; in our context,“multiple studies” means that each patient tested more than twodevices, and “treatments” means devices. This approach is partic-ularly advantageous because all devices under comparison areincorporated into a single model even if they are not compared inthe same questionnaire. Furthermore, to rank the treatments, weused the Surface Under the Cumulative RAnking probabilities(SUCRA), the larger the SUCRA, the higher the device globalusability [30]. Both fixed-effect (FE) and random-effect (RE)models were performed, and the model with the lowest DevianceInformation Criterion (DIC) was selected [31]. DIC represents atrade-off between goodness of fit (how well the model fits theobservations) and model complexity (number of model parame-ters).
Finally, the time for completing both O-GUS and S-GUS wasalso counted in minutes, and compared by two-side t-test.Furthermore, the results of IC model constructed on the S-GUSscores were used to propose a simply classification of “Good”,“Pretty good” and “Insufficient” usability for each tested device.
ResultsThe items characterized by the highest informative power and
then the most suitable to contribute to the novel S-GUSQuestionnaire composition, are reported in Table 1 together withthe corresponding linear coefficients. Figure 2 illustrates the result-ed S-GUS questionnaire with the new scores for each question.
Figure 2. GUS Questionnaire short-form with only questions characterized by the highest degree of linear association (in bold the scorefor each question). *+2.5 points for each device not perceived as the most difficult to use.
MRM_01 original.qxp_Hrev_master 22/07/20 10:44 Pagina 50
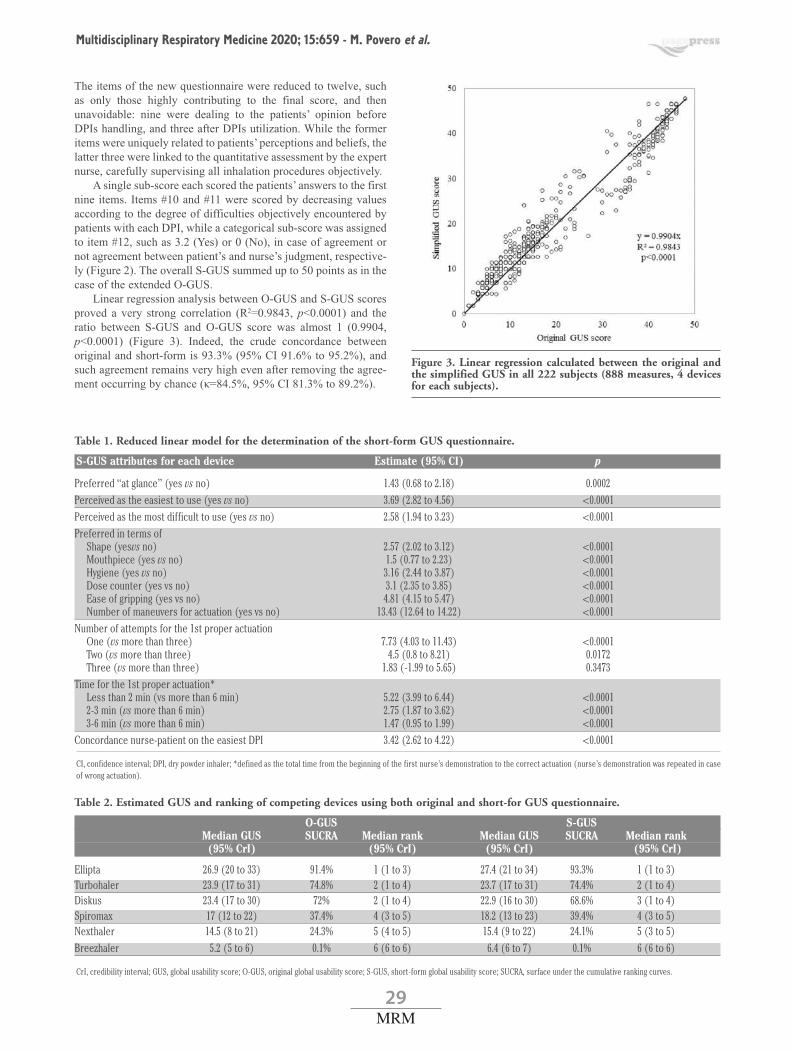
29MRM
Multidisciplinary Respiratory Medicine 2020; 15:659 - M. Povero et al.
The items of the new questionnaire were reduced to twelve, suchas only those highly contributing to the final score, and thenunavoidable: nine were dealing to the patients’ opinion beforeDPIs handling, and three after DPIs utilization. While the formeritems were uniquely related to patients’ perceptions and beliefs, thelatter three were linked to the quantitative assessment by the expertnurse, carefully supervising all inhalation procedures objectively.
A single sub-score each scored the patients’ answers to the firstnine items. Items #10 and #11 were scored by decreasing valuesaccording to the degree of difficulties objectively encountered bypatients with each DPI, while a categorical sub-score was assignedto item #12, such as 3.2 (Yes) or 0 (No), in case of agreement ornot agreement between patient’s and nurse’s judgment, respective-ly (Figure 2). The overall S-GUS summed up to 50 points as in thecase of the extended O-GUS.
Linear regression analysis between O-GUS and S-GUS scoresproved a very strong correlation (R2=0.9843, p<0.0001) and theratio between S-GUS and O-GUS score was almost 1 (0.9904,p<0.0001) (Figure 3). Indeed, the crude concordance betweenoriginal and short-form is 93.3% (95% CI 91.6% to 95.2%), andsuch agreement remains very high even after removing the agree-ment occurring by chance (κ=84.5%, 95% CI 81.3% to 89.2%).
Table 1. Reduced linear model for the determination of the short-form GUS questionnaire.
S-GUS attributes for each device Estimate (95% CI) p
Preferred “at glance” (yes vs no) 1.43 (0.68 to 2.18) 0.0002Perceived as the easiest to use (yes vs no) 3.69 (2.82 to 4.56) <0.0001Perceived as the most difficult to use (yes vs no) 2.58 (1.94 to 3.23) <0.0001Preferred in terms of
Shape (yesvs no) 2.57 (2.02 to 3.12) <0.0001Mouthpiece (yes vs no) 1.5 (0.77 to 2.23) <0.0001Hygiene (yes vs no) 3.16 (2.44 to 3.87) <0.0001Dose counter (yes vs no) 3.1 (2.35 to 3.85) <0.0001Ease of gripping (yes vs no) 4.81 (4.15 to 5.47) <0.0001Number of maneuvers for actuation (yes vs no) 13.43 (12.64 to 14.22) <0.0001
Number of attempts for the 1st proper actuation One (vs more than three) 7.73 (4.03 to 11.43) <0.0001Two (vs more than three) 4.5 (0.8 to 8.21) 0.0172Three (vs more than three) 1.83 (-1.99 to 5.65) 0.3473
Time for the 1st proper actuation* Less than 2 min (vs more than 6 min) 5.22 (3.99 to 6.44) <0.00012-3 min (vs more than 6 min) 2.75 (1.87 to 3.62) <0.00013-6 min (vs more than 6 min) 1.47 (0.95 to 1.99) <0.0001
Concordance nurse-patient on the easiest DPI 3.42 (2.62 to 4.22) <0.0001
CI, confidence interval; DPI, dry powder inhaler; *defined as the total time from the beginning of the first nurse’s demonstration to the correct actuation (nurse’s demonstration was repeated in caseof wrong actuation).
Table 2. Estimated GUS and ranking of competing devices using both original and short-for GUS questionnaire.
O-GUS S-GUS Median GUS SUCRA Median rank Median GUS SUCRA Median rank (95% CrI) (95% CrI) (95% CrI) (95% CrI)
Ellipta 26.9 (20 to 33) 91.4% 1 (1 to 3) 27.4 (21 to 34) 93.3% 1 (1 to 3)Turbohaler 23.9 (17 to 31) 74.8% 2 (1 to 4) 23.7 (17 to 31) 74.4% 2 (1 to 4)Diskus 23.4 (17 to 30) 72% 2 (1 to 4) 22.9 (16 to 30) 68.6% 3 (1 to 4)Spiromax 17 (12 to 22) 37.4% 4 (3 to 5) 18.2 (13 to 23) 39.4% 4 (3 to 5)Nexthaler 14.5 (8 to 21) 24.3% 5 (4 to 5) 15.4 (9 to 22) 24.1% 5 (3 to 5)Breezhaler 5.2 (5 to 6) 0.1% 6 (6 to 6) 6.4 (6 to 7) 0.1% 6 (6 to 6)
CrI, credibility interval; GUS, global usability score; O-GUS, original global usability score; S-GUS, short-form global usability score; SUCRA, surface under the cumulative ranking curves.
Figure 3. Linear regression calculated between the original andthe simplified GUS in all 222 subjects (888 measures, 4 devicesfor each subjects).
MRM_01 original.qxp_Hrev_master 22/07/20 10:44 Pagina 51

30MRM
Multidisciplinary Respiratory Medicine 2020; 15:659 - M. Povero et al.
Table 2 displays the results produced by pairwise IC both usingO-GUS and S-GUS scores. There is absolute perfect agreementbetween the results obtained using O-GUS score and thoseobtained using S-GUS score. Furthermore, devices are ranked inthe same order, the value of SUCRA for each DPI is almost equaland the cumulative ranking probability curves overlap for eachDPI (Figure 4). Mean values of the overall S-GUS proved stablefor all DPIs and characterized by a well comparable variability.This stability allows the suggestion of a quantitative ranking ofDPIs based on the mean GUS value. In particular, a “good” usabil-ity can be highly presumed for S-GUS values >25, and a “prettygood” usability for S-GUS values ≥15 ≤25, while an “insufficient”usability can be likely suggested for S-GUS values <15 (Figure 5)
Finally, the mean time spent for filling O-GUS properly was23.4 min (standard deviation 3.3), while that for completing the S-GUS was 6.1 min (standard deviation 2.2), respectively (p<0.001).
Figure 4. Cumulative ranking probability plots for competing DPIs drawn by extrapolating at the middle of each interval of the stepfunction: on the horizontal axis is the possible rank of each device (from the first best rank to worse according to the global usabilityscore), on the vertical axis is the cumulative probability for each device to be the best option, among the best two options, among thebest three options, and so on.
Figure 5. The thresholds for ranking DPIs usability by means ofthe estimated S-GUS scores: white points represent the medianGUS while the bars indicate the 95% credibility interval; we cal-culated such statistics considering the GUS score of each devicewhen the device was ranked 1st to 2nd, 3rd to 4th and 5th to 6th,respectively.
MRM_01 original.qxp_Hrev_master 22/07/20 10:44 Pagina 52

31MRM
Multidisciplinary Respiratory Medicine 2020; 15:659 - M. Povero et al.
Discussion The choice of the most convenient DPIs to prescribe is too fre-
quently empiric in real life, being the role of effective criteria ofchoice often underestimated or neglected [5,13,15,16].
Usually, the patients’ skill of the operational manoeuvres lead-ing to the proper inhalation of the drug from DPIs is usually inad-equate and only occasionally checked before their prescription: itis regarded as a time-consuming procedure that also requires a pre-scribers’ specific knowledge [5, 13]. This represents a crucial pointparticularly in long-term inhalation treatments, as in the case ofpersistent airway diseases (i.e. bronchial asthma and chronicobstructive airway disease – COPD), when the personalization oftherapy is absolutely relevant in terms of patients’ adherence totreatments and then of outcomes to achieve. Even if DPIs presentlyavailable are highly effective, nonetheless it is known that patientsare not able to use all of them equally well [5,6,21,24]. Moreover,the sophisticated engineering of present DPIs would increasinglyrequire the contribution of advanced health professional roles orspecific knowledge for teaching, training and supporting patientsproperly [6,7,32]. Despite these critical aspects, inhalation abso-lutely remains the route to prefer for delivering and assuming res-piratory drugs effectively. Consequently, usability should beregarded as the most important parameter contributing to the moti-vated and convenient choice of the DPI to prescribe [19-21].
The term “usability” was sometimes merely used in the litera-ture as a synonymous of “ease of use”, or “intuitivity”, or “prefer-ence at glance”, even if usability itself does represent a much morecomplex and comprehensive concept than expected. Actually,usability mirrors the role of a much wider panel of variables under-lying and affecting proper inhalation. In other words, usabilityreflects the influence of those factors depending of the patients’point of view (i.e., preference, attractivity, etc.) [12,15], but also ofthose related to the effects of intrinsic technological characteristicsof the DPIs, of which patients are usually almost completelyunaware (i.e., emission velocity, lung deposition, dose consistency,etc.). The careful assessment of DPIs usability through quantitativeand specific indices should then be increasingly favoured as a pri-ority issue also in the aim of comparing and ranking their usabilityobjectively.
Nevertheless, the great majority of recent investigationalinstruments has been mostly (or uniquely) developed in order tomainly focus patients’ intuitiveness, preference, and satisfactionrelated to DPIs [11,14,16-18]. Unfortunately, even if these instru-ments proved to be reliable tools for checking patients’ personalbeliefs, the role of an independent assessment by a third-partexpert observer (i.e., by an expert supervising nurse or doctor) wassometimes lacking, or not valued systematically [16,17]. In ourcenter, two nurses, equally expert, motivated in educational pro-grams, and familiar with the technical and the psychologicalaspects of the GUS Questionnaire, played this role. They werespecifically dedicated to patients’ interviews, and to supervise,check, assess, and validate all patients’ procedures for inhalation.However, this figure could be generalizable and extended to anyhealthcare professional or other caregiver, but only after a specifictraining.
Furthermore, specificity and suitability represent the mostimportant qualities, which should characterize the investigationalinstruments to use in clinical studies for investigating DPIs perfor-mances. If O-GUS allowed for the first time to discriminate DPIsin terms of their effective usability [24], the same extent of inter-DPIs differences was also equally documented with the S-GUS:not only in terms of patients’ perceptions and beliefs, but mostly in
terms of number of attempts and of time required for achieving thefirst proper actuation of DPIs. In particular, data from the presentstudy strongly confirm the good suitability of the novel S-GUS inclinical practice as they are super-imposable to those obtained withthe extended O-GUS and prove the almost absolute correspon-dence between patients’ and nurse’s opinions.
The role of time to spend for checking one more DPIs objec-tively and to overcome the difficulties encountered by patientsprior to their prescription still represents a key parameter in clini-cal practice. To emphasize that the novel S-GUS consents the rank-ing of DPIs in a very short time, thus highly favouring the regularcheck of patients’ DPIs usability in current clinical practice.Furthermore, the short-form questionnaire can be easily convertedinto a mobile application that represents one of the more usefulinstruments in medical practice.
ConclusionsDPIs were further confirmed to be characterized by different
degrees of usability. S-GUS proved as a quite specific tool for assess-ing DPIs usability in short time. The availability of this suitable,reproducible, smart and quick operational tool should be regarded asa valuable progress in this particular field of investigation.
AcknowledgementsNone.
References1. Newman SP, Busse WW. Evolution of dry powder inhaler
design, formulation, and performance. Respir Med 2002;96:93-304.
2. Wieshammer S, Dreyhaupt J. Dry powder inhalers: which fac-tors determine the frequency of handling errors? Respiration2008;75:18-25.
3. Chapman KR, Fogarty CM, Peckitt C, Lassen C, Jadayel D,Dederichs J, et al. Delivery characteristics and patients’ han-dling of two single-dose dry powder inhalers used in COPD.Int J Chron Obstruct Pulmon Dis 2011;6:353-6.
4. Barrons R, Pegram A, Borrens A. Inhaler device selection: spe-cial considerations in elderly patients with chronic obstructivepulmonary disease. Am J Health Syst Pharm 2011;1221-32.
5. Barry PW, O’Callagnan C. The influence of inhaler selectionon efficacy of asthma therapies. Adv Drug Deliv Res2003;55:879-923.
6. Gustafsson P, Taylor A, Zanen P, Chrystyn H. Can patients useall dry powder inhalers equally well? Int J Clin Pract Suppl2005;59:13-18.
7. Melani AS. Inhalatory therapy training: a priority challenge forthe physician. Acta Biomed 2007;78:233-45.
8. Thomas M, Williams AE. Are outcomes the same with all drypowder inhalers? Int J Clin Pract Suppl 2005;149:33-5.
9. Chrystyn H. Do patients show the same level of adherencewith all dry powder inhalers? Int J Clin Pract Suppl2005;149:19-25.
10. Franks M, Briggs P. Use of a cognitive ergonomics approachto compare usability of a multidose dry powder inhaler and acapsule dry powder inhaler: an open label, randomized, con-trolled study. Clin Ther 2004;26:1791-9.
MRM_01 original.qxp_Hrev_master 22/07/20 10:44 Pagina 53

32MRM
Multidisciplinary Respiratory Medicine 2020; 15:659 - M. Povero et al.
11. Virchow JC, Crompton GK, Dal Negro R, Pedersen S, MagnanA, Seidenberg J, et al. Importance of inhaler devices in themanagement of airway disease. Respir Med 2008;102:10-9.
12. Lenney J, Innes JA, Crompton GK. Inappropriate inhaler use:assessment of use and patient preference of seven inhalationdevices. EDICI. Respir Med 2000;94:496-500.
13. Anderson P. Patient preference for and satisfaction with inhalerdevices. Eur Respir Rev 2005;96:109-16.
14. Tordera PM, Viejo JL, Sanchis J, Badia X, Cobos N, Picado C,et al. Assessment of patient satisfaction and preferences withinhalers in asthma with the FSI-10 Questionnaire. ArchBroncopneumol 2008;44:346-52.
15. Schulte M, Osseiran K, Betz R, Wenker M, Brand P, Meyer T,et al. Handling of and preferences for available dry powderinhaler systems by patients with asthma and COPD. J AerosolMed Pulm Drug Deliv 2008;21:321-8.
16. Hodder R, Price D. Patient preferences for inhaler devices inchronic obstructive pulmonary disease: experience withRespimat Soft Mist Inhaler. Int J Chron Obstruct Pulmon Dis2009;4:381-90.
17. van der Polen J, Ginko T, Kroker A, van der Valk P, GoosensM, Padullés L, et al. Preference, satisfaction and errors withtwo dry powder inhalers in patients with COPD. Expert OpinDrug Deliv 2013;10:1023-31.
18. Hantulik P, Wittig K, Henschel Y, Ochse J, Vahteristo M, RytilaP. Usage and usability of one powder inhaler compared to otherinhalers at therapy start: an open, non-interventional observa-tional study in Poland and Germany. Pneumol Allergol Pol2015;83:365-77.
19. Kozma CM, Slaton TL, Monz BU, Hodder R, Reese PR.Development and validation of a patient satisfaction and pref-erence questionnaire for inhalation devices. Treat Respir Med2005;4:41-52.
20. Rajan SK, Gogtay JA. Ease-of-use, preference, confidence,and satisfaction with Revolizer, a novel dry powder inhaler, inan Indian population. Lung India 2014;31:366-37.
21. Zervas E, Samitas K, Gaga M. Assessment of satisfaction withdifferent dry powder inhalation devices in Greek patients with
COPD and asthma: the ANASA study. Int J Chron ObstructPulmon Dis 2016;11:1845-55.
22. Dal Negro RW, Turco P, Povero M. The Global UsabilityScore: A novel comprehensive tool for assessing, ranking, andcompare usability of inhalers in patients requiring airway treat-ments. Pulm Respir Med 2017;7:2.
23. Dal Negro RW, Povero M. Usability and cost-of-usability ofthree Dry powder inhalers (DPIs) in patients with ChronicObstructive Pulmonary Disease (COPD): may these variablesinfluence the health technology assessment of DPIs? ChronicObstr Pulm Dis 2016;1:2-12.
24. Dal Negro RW, Turco P, Povero M. Patients’ usability of sevenmost used dry-powder inhalers in COPD. Multidiscip RespirMed 2019;14:30.
25. Tibshirani R. Regression Shrinkage and Selection via Lasso. JR Statist Soc B 1996;58:267-88.
26. Altman DG, Andersen PK. Bootstrap investigation of the sta-bility of a Cox regression model. Stat Med 1989;8:771-83.
27. Derksen S, Keselman HJ. Backward, forward and stepwiseautomated subset selection algorithm: Frequency of obtainingauthentic and noise variables. Brit J Math Stat Psychol1992;45:265-82.
28. Sheather SJ. A modern approach to regression with R. NewYork, NY; Springer; 2009.
29. Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis fordecision making 2: A generalized linear modeling frameworkfor pairwise and network meta-analysis of randomized con-trolled trials. Med Decis Making 2013;33:607-17.
30. Salanti G, Ades AE, Ioannidis PA. Graphical methods andnumerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J ClinEpidemiol 2011;64:163-71.
31. David J, Spiegelhalter, NGB, Bradley PC, van der Linde A.Bayesian measures of model complexity and fit. J R Statist SocB 2002;64:583-639.
32. Self TH, Arnold LB, Csosnowski LM, Swanson JM, SwansonH. Inadequate skill of health care professionals in using asthmainhalation devices. J Asthma 2007;44:593-8.
Received for publication: 24 March 2020. Accepted for publication: 27 April 2020.This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0).©Copyright: the Author(s), 2020Licensee PAGEPress, ItalyMultidisciplinary Respiratory Medicine 2020; 15:659doi:10.4081/mrm.2020.659
MRM_01 original.qxp_Hrev_master 22/07/20 10:44 Pagina 54

33MRM
Respiratory symptoms and associated risk factors among under-five children in Northwest, Ethiopia: community based cross-sectional studyZewudu Andualem,1 Asefa Adimasu Taddese,2 Zelalem Nigussie Azene,3 Jember Azanaw,1 Henok Dagne1
1Department of Environmental and Occupational Health and Safety, Institute of Public Health, College of Medicine andHealth Sciences, University of Gondar2Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences,University of Gondar3Department of Women’s and Family Health, School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Ethiopia
Introduction:Acute respiratory infections are still a major public health problem resulting in morbidity and mortalityamong under-five children. This study aims to assess the extent of respiratory symptoms and associated risk factorsamong under-five children in Gondar city, Northwest Ethiopia.Methods:A community-based cross-sectional study was carried out from February to June 2019. From 792 study par-ticipants, data were collected via face to face interviews by using a semi-structured pre-tested questionnaire. Data wereentered in Epi Info version 7, then exported to Stata 14.00 for analysis. Binary (Bivariable and Multivariable) logisticregression analysis was used to test the association of explanatory and outcome variables. Variables with p<0.05 wereconsidered as significantly associated with the outcome variable.Results: The prevalence of respiratory symptoms among under-five children was 37.5% at [95% (CI: 34.3-41)].Uterine irritability during pregnancy [AOR = 1.89 at 95% CI: (1.11-3.23)], physical exercise during pregnancy [AOR= 0.60 at 95% CI: (0.41-0.89)], using wood and coal for heating [AOR = 2.42 at 95% CI: (1.65-3.53)], cockroachesinfestation [AOR = 1.95 at 95% CI: (1.36 – 2.90)], presence of new carpets [AOR = 2.38 at 95% CI: (1.33-4.29)],damp stain [AOR = 2.45 at 95% CI: (1.02-2.69)], opening windows during cooking [AOR = 0.58 at 95% CI: (0.36 -0 .93)], living less than 100 m heavy traffic [AOR = 1.94 at 95% CI: (1.16-3.27)], and living less than 100 m (unpavedroads/streets) [AOR= 2.89 at 95% CI: (1.89-4.55)] were significantly associated with respiratory symptoms.Conclusion: The prevalence of respiratory symptoms among under-five children was relatively high in the study area.Personal and environmental characteristics influencing symptom occurrence were identified. Respiratory symptomswill be minimized by reducing exposure to indoor and outdoor air pollution and enhancing housing quality.
Key words: Air pollution; respiratory symptoms; cross-sectional study; under-five children; Ethiopia.
AB
STR
ACT
Correspondence: Zewudu Andualem, Department of Environmental and Occupational Health and Safety, Institute of PublicHealth, College of Medicine and Health Sciences, University of Gondar, Ethiopia. E-mail: [email protected]: All stated authors were involved in the study from the inception to design, acquisition of data, analysis andinterpretation, and drafting of the manuscript. All authors read and approved the final manuscript.Conflict of interest: The authors declare that they have no competing interests.Funding: The authors received no specific funding for this work. Availability of data and materials: The dataset analyzed during the current study is available from the corresponding author uponreasonable request.Ethics approval and consent to participate: The study was conducted after obtaining ethical clearance from the InstitutionalReview Board of University of Gondar with IRB number of (O/V/PRCS/05/369). An official letter of cooperation was written toGondar city administration. After a clear and detailed explanation of the purpose, risks, and benefits of the study, written informedconsent was obtained from each of the mothers/study participants. Mothers were told that participation was voluntary and that theycould withdraw at any time if they were not comfortable during the interview. During data collection, under-five children identifiedwith clear acute respiratory infection were referred to the health institutions for appropriate treatment. Personal identifiers were notincluded in the written tool to ensure confidentiality. The ethical statement was carried out in accordance with the principles of theDeclaration of Helsinki.
Consent for publication: Not applicable.
ORIGINAL RESEARCH ARTICLE
Multidisciplinary Respiratory Medicine 2020; volume 15:685
MRM_01 original.qxp_Hrev_master 28/09/20 15:35 Pagina 108

34MRM
Multidisciplinary Respiratory Medicine 2020; 15:685 - Z. Andualem et al.
Introduction Acute respiratory infections (ARI) are still a major public
health problem resulting in morbidity and mortality among under-five children. Worldwide, it is estimated that about 7.6 million chil-dren died before celebrating their fifth year of birthday attributedto respiratory tract infections [1,2]. About more than half (i.e.,55%) of deaths due to ARI symptoms are from 15 low and middle-income countries (LMICs) and nine of these countries are locatedin sub-Saharan African (SSA) region [3]. From an estimated, 5.4million under-five children that died in 2017 roughly half of thosedeaths occurred in sub-Saharan Africa and ARIs contributed to thehighest number of deaths [4].
Finding from Urban Slums of Gulbarga city found ARI inci-dence of 27.25% among under-five age group children [5]. Amulti-country study conducted over sub-Saharan African countrieshas also reported the magnitude of acute lower respiratory infec-tion (ALRI) for all the countries was 25.3%, Congo (39.8%),Gabon (38.1%), Lesotho (35.2%), and Tanzania (35.2%) were thecountries with the highest prevalence of ALRIs [6].
Indoor air pollution is one of the most important contributorsto the global burden of disease, particularly in developing coun-tries including Ethiopia, being children one of the most vulnerablegroups [7]. The high incidence of ARI in children less than fiveyears of age is one of the main reasons for pediatric outpatients’visits and hospitalization in developing countries [8]. Besidesresulting in substantial morbidity and mortality, ARI also yields inmultifaceted adverse consequences. Economic losses as a result ofthe use of healthcare resources, use of health personnel’s time, dis-ruption of the family, long time hospitalization and loss in produc-tivity are some of them [9].
Ethiopia has made ample investments to reduce the burden ofmorbidity and mortality posed by ARI in the pediatrics segment ofthe population. Integrated management of common childhood ill-ness and community case management are among the program ini-tiatives scaled up nationally to address ARI in the country [10].Previous studies have identified different factors linked with respi-ratory symptoms among children of under-five. Age and gender ofthe child, nutritional status, wealth index, parental educational sta-tus, large family size, exposure to biomass fuel, and parental smok-ing status, insufficient breastfeeding practice, poor immunizationstatus, attendance to daycare centers, and overcrowding wereimportant predictors of ARI among under-five children[3,8,11,12].
This study aims to determine the extent of respiratory symp-toms and associated risk factors among under-five children inGondar city, Northwest Ethiopia.
Methods
Study design, period, and areaA community-based cross-sectional study was conducted from
February 15, 2019, to June 20, 2019, in Gondar city, NorthwestEthiopia. The city is divided into 12 administrative areas (sub-cities) which consist of 21 kebeles (the smallest administrativeunits in Ethiopia). It has an estimated total population of 324, 000with about 23,929 under-five children.
Sample size calculation and sampling procedureThe sample size was determined by using a single population
proportion formula [13] considering the following assumptions: p= 50% proportion of children with respiratory symptoms (there isno previous study in the study area), 95% confidence interval, 5%
margin of error (d) and design effect 2
Since we used multi-stage sampling technique, it demands usto use design effect of 2 and we used 5% non-response rate, thus,final sample size (2×384+ 768×0.05) = 806.
Multi-stage sampling was used as an assumption of being aheterogeneous population in the 12 administrative areas of thecities. Fifty percent of total sub-cities were randomly selected fromthe 12 administrative areas and all eligible study participants pres-ent in the selected sub-cities were included in the study. Study par-ticipants were selected through simple random sampling tech-nique.
Data collection tools and procedures Through a face-to-face interview at the participants’ home,
data were collected using a pretested semi-structured question-naire. The questionnaire was developed by reviewing different lit-eratures [12,14-16]. The questionnaires include the outcome vari-able i.e. respiratory symptoms (such as cough, shortness of breath,wheezing, chest tightness, phlegm, and a problem in the chestincluding blocked, or running nose) and the explanatory variables:such as socio-demographic factors (age of a child, age of mothers,average monthly income, mothers and spouse educational level,etc.) and household air pollutants (such as type of fuels for cook-ing, types of fuel for heating, pesticide application, contact withfarm animals (e.g. cattle, pigs, goats, sheep or poultry), smoke cig-arettes (mothers/guardians),cockroach infestation in a household(HH), painting/staining done in the last 6 months HH, new carpets,drapes or other textiles in the last 6 months and using air freshen-ers, etc.) and house characteristics such as floor construction mate-rials, wall surface water-based paint, ceiling surface, damp stains,visible mold, place of cooking, open doors during cooking, openwindows during cooking, and time of spending indoors on an aver-age day.
The questionnaire was first prepared in English and then trans-lated to Amharic (local language) and back to English to maintainconsistency of the tool. In the data collection process, six licentiatenurses and one BSc nurse were involved. Data collectors andsupervisors have received two-days training.
Operational definitions The outcome variable of this study was respiratory symptoms.
Respiratory symptoms were defined in this study as to whether thechildren under-five years of age had been suffering from cough,shortness of breath, wheezing, chest tightness, phlegm, and a prob-lem in the chest including blocked, or running nose [17,18].Under-five children who have experienced at least one of theabove-mentioned symptoms for the last 12 months prior to thestudy were considered as having respiratory symptoms.
Data processing and analysisData were first checked manually for completeness and then
coded and entered into Epi Info version 7, then exported to Stata14.00 for data checking, cleaning, and analysis. Descriptive statis-tics were performed to describe the study population with depend-ent and independent variables. Model fitness was checked with theassumptions of the Hosmer and Lemeshow goodness of fit test.Bi-variable and multivariable logistics regressions were computedto identify the presence and strength of associations. Variables witha p<0.2 [19] in the bivariable binary logistic regression analysis
MRM_01 original.qxp_Hrev_master 28/09/20 15:35 Pagina 109

35MRM
Multidisciplinary Respiratory Medicine 2020; 15:685 - Z. Andualem et al.
were included in the multivariable binary logistic regression analy-sis. Odds ratios with 95% CI were computed and variables havinga p less than 0.05 in the multivariable binary logistic regressionmodels were considered significantly associated with the depend-ent variable.
Results
Socio-demographic characteristics of the study partici-pants
A total of 806 study participants were aimed in this study. Out ofthese, 792 participants were enrolled with a response rate of 98.26%.The median age of under-five children was 24 months ± 12.24(SD)and about 431 (54.4%) were males. 28.65% of the study partici-pants’ mothers were in the age of 18-25 years and 22.98% wereabove 33 years. The majority (77.02%) of the study participantswere Orthodox Christian by their religious affiliation (Table 1).
Household air quality and housing characteristicsThree-fifth (60.48%) of the study participants reported the use
of charcoal for cooking food. Only few (2.15%) of fathers and
(3.03%) of mothers smoked cigarettes and 47.85% of householdswere infested by cockroaches. Out of the study participants, 250(31.57%) have spent their time between 6 to 11 h, 179 (31.57%)>15 h, and 198 (25%) <6 h indoors in home, respectively. Abovehalf (55.56%) of the study participants used wood and coal forheating their house during humid weather condition and 43.06%did not use any fuel for heating (Table 2).
Prevalence of respiratory symptoms among under-fivechildren
The prevalence of respiratory symptoms among under-fivechildren in Gondar city was 37.5% at [95% (CI: 34.3-41)]. Themost common respiratory symptoms were runny nose (25.63%),phlegm (10.48%), and wheezing (9.72%). The lowest reportedrespiratory symptom was chest tightness 3.03% (Figure 1).
Factors associated with respiratory symptoms amongunder-five children
In multivariable analyses, problems during pregnancy (e.g.hyperirritability of uterus), regular physical activity during preg-nancy, the heredity of respiratory disease, fuel type usually usedfor heating, cockroach infestation in home, presence of new car-pets, damp stains, opening windows during cooking, living less
Table 1. Socio-demographic characteristics of study participants in Gondar city, Northwest Ethiopia, 2019.
Variables Frequency (n=792) %
Sex of child Female 361 45.6Age of child 12 months 204 25.76 13-24 months 213 26.89 25-36 months 181 22.85 37-48 months 152 19.19 49-59 months 42 5.30 Median age of children 24±12.24 (SD)Education level of mothers Unable to read and write 121 15.55 Read and write 90 11.57 Primary 100 12.85 Secondary 253 32.52 Graduate from vocational 30 3.86 Diploma and above 184 23.65Age of mothers 18-25 years 227 28.66 26-28 years 206 26.01 29-32 years 177 22.35 >33 years 182 22.98 Median age of mothers 28±5.86 (SD) Religion Orthodox 610 77.02 Muslim 140 17.68 Others* 42 5.30Occupation of mother (n=784) Housewife 533 67.98 Farmer 4 0.51 Student 8 1.02 Private employee 52 6.63 Government employee 142 18.11 Merchant 35 4.46 Others (specify) 10 1.28Occupation of father (n=723) Farmer 18 2.49 Student 8 1.11 Private employee 310 42.88 Government employee 232 32.09 Merchant 88 12.17 Others 67 9.27
*Protestants, Jewish.
MRM_01 original.qxp_Hrev_master 28/09/20 15:35 Pagina 110

36MRM
Multidisciplinary Respiratory Medicine 2020; 15:685 - Z. Andualem et al.
than 100 m from heavy traffic, and living less than 100 m fromunpaved roads/streets were significantly associated with under-five children’s respiratory symptoms.
Among children of under-five years, those children whosemother had a problem of uterine overstimulation at the time oftheir pregnancy were 2.20 at times heightened risk of sufferingfrom respiratory symptoms as compared to their counterparts[AOR=2.20 at 95% CI: (1.25-2.89)]. Children from a mother whohad done a regular exercise during their pregnancy period had a40% lesser likelihood of developing respiratory symptoms thanchildren whose mothers had been sedentary during pregnancy[AOR = 0.60 at 95% CI: (0.41-0.89)]. The adjusted odds of respi-ratory symptoms were 1.89 times higher among under-five chil-dren whose mothers had a hereditary respiratory disease whencompared with their counterparts [AOR=1.89 at 95% CI: (1.11-
Table 2. Household air quality and housing characteristics of the study participants in Gondar city, Northwest Ethiopia, 2019.
Variables Frequency (n= 792) %
Types of fuel usually used for cooking Charcoal 479 60.48 Electricity 273 34.47 Open fires 40 5.05Types of fuel usually used for heating None 341 43.06 Wood, coal 440 55.56 Electricity 11 1.39History of contact with farm animals Yes 47 5.93Cigarettes smoking (mothers/guardians) Yes 24 3.03Cockroach infestation in household Yes 379 47.85Painting/staining done in the last 6 months Yes 110 13.89Presence of new carpets, in the last 6 months Yes 110 13.89Using air fresheners Yes 48 6.06Presence of a kitchen exhaust fan Yes 40 5.05A pesticide application Yes 157 19.82Floor construction materials Wood and mud 542 68.43 Brick and concrete| 250 31.57Wall surface water-based paint Yes 174 21.97Ceiling surface (n=749) Wooden 576 76.90 Painted 131 17.49 Cement 42 5.61Damp stains Yes 63 7.95Visible mould Yes 67 8.46Place of cooking (n=775) Inside 461 59.48 Outside 314 40.52Open doors during cooking (n= 680) Yes 241 35.44Open windows during cooking (n=676) Yes 214 31.66Length of time spend indoors on an average day <6 hours 198 25.00 6 to 11 hours 250 31.57 11 to 15 hours 165 20.83 >15 hours 179 22.60Presence of attached garage within 100 m of household Yes 46 5.81Frequency of trucks passing through the nearby street Never 397 50.13 Seldom 254 32.07 Frequently 93 11.74 Almost the whole day 48 6.06Living in less than 100 m heavy traffic Yes 162 20.45Living in less than 100 m (unpaved roads/streets) Yes 194 24.49Exposure to animal allergens in early childhood Yes 38 4.80Exposure to animal allergens in the present time Yes 45 5.68
Figure 1. Prevalence of respiratory symptoms among under-fivechildren in Gondar city, Northwest Ethiopia, 2019.
MRM_01 original.qxp_Hrev_master 28/09/20 15:35 Pagina 111

37MRM
Multidisciplinary Respiratory Medicine 2020; 15:685 - Z. Andualem et al.
3.23)]. When compared to children whose parents did not usewood and coal, those who used wood and coal for heating indoorsduring humid weather conditions were 2.42 times more likely todevelop respiratory symptoms [AOR=2.42 at 95% CI: (1.65-3.53)]. Children living in households infested by cockroaches were1.95 times more likely to suffer from respiratory symptoms whencompared with their counterparts [AOR=1.95 at 95% CI: (1.36-2.90)]. Children whose parents used new carpets in HH were 2.38times more likely to suffer from respiratory symptoms comparedwith their counterparts [AOR=2.38 at 95% CI: (1.33-4.29)].Children living in a damp house were 1.66 times more likely tosuffer from respiratory symptoms when compared with their coun-terparts [AOR=1.66 at 95% CI: (1.02-2.69)]. In households wherewindows were open at the time of cooking, the risk of experiencingrespiratory symptoms among under-five children was 42% timesless likely as compared to those households which remained closedduring cooking time [AOR = 0.58 at 95% CI: (0.36 0.93)].Children living less than 100 m from heavy traffic areas were 1.94times more likely to suffer from respiratory symptoms [AOR=1.94at 95% CI: (1.16-3.27)]. Children living less than 100 m fromunpaved roads/streets were 2.89 times more likely to develop res-piratory symptoms when compared with their counterparts[AOR=2.89 at 95% CI: (1.89-4.55)] (Table 3).
Discussion This study found that a number of housing characteristics,
indoor air pollution, and outdoor air pollution significantly con-tributed to an increase in the prevalence of respiratory symptomsamong under-five children. In this study, we have found that theoverall prevalence of respiratory symptoms among under-five chil-dren was 37.5% at [95% (CI: 34.3-41)], of these (runny nose(25.63%), phlegm (10.48%), and wheezing (9.72 were commonlyreported respiratory symptoms. This finding [37.5%] was highercompared with previous studies in Ethiopia [20], India [15,21],Nepal [22], and Bangladesh [17]. The possible explanation couldbe the variation of the study setting, in which some of the studieswere institutional-based, whereas our study was community-based,the study period, and the variability in socio-economic, housing,and environmental inequalities.
In regard to the independent factors affecting the respiratorysymptoms among children of under-five years, those childrenwhose mother had a problem of uterine overstimulation at the timeof their pregnancy were 2.20 times at heightened risk of sufferingfrom respiratory symptoms as compared to their counterparts. Thisfinding may be related to the fact that whenever there is uterineoverstimulation, the spiral artery which is responsible for supply-ing blood to the uterus tends to be ligated/ tied off and this leadsthe fetus to develop asphyxia due to uteroplacental insufficiency.Birth asphyxia has numerous long term impacts on the baby tillchildhood including multiple organ damage involving lungs andpoor brain stem reflexes like breathing problems which finallypose children at a greater risk of experiencing respiratory symp-toms [23].
Regular exercise during pregnancy was another determinant ofunder-five respiratory symptoms. Accordingly, children frommothers who had done a regular exercise during their pregnancyperiod had a 40% lesser likelihood of developing respiratorysymptoms than children whose mothers had been sedentary duringpregnancy. This could probably be explained by well-documentedevidence that reports the benefits of exercise during pregnancy forthe mother and the fetus with benefits persisting for the child intoadulthood. Regular exercise during pregnancy decreases the risk ofdisease for children including respiratory symptoms in that the
babies’ hearts most likely had sped up and synchronized with theirmothers’ during exercise, allowing children to enjoy the same heartbenefits, thereby having better-conditioned cardiac muscles whichin turn mitigating their risk of respiratory symptoms [24,25]. Theadjusted odds of respiratory symptoms were 1.98 times higheramong under-five children whose mothers had hereditary respira-tory disease. Infection and genetic factors affect the developmentof the lungs, either directly or indirectly, which can cause respira-tory symptoms [26].
When comparing children whose parents did not use wood andcoal, those who used wood and coal for heating indoors duringhumid weather conditions were 2.42 times more likely to developrespiratory symptoms. Evidence has shown that respiratory symp-toms are a common problem with wood smoke exposure [27].Studies suggest that wood smoke particles cause harm to humanhealth through oxidative stress, cell toxicity, defects in cell regen-eration, resulting in lung damage, and genotoxicity [28,29].Children living in households infested by cockroaches were 1.95times more likely to suffer from respiratory symptoms when com-pared with their counterparts. Cockroach exposure has been linkedto cockroach sensitization and allergic respiratory symptoms [30].Exposure to cockroaches can increase the risk for frequent wheez-ing of children with allergic or asthmatic parents in the first year oflife even if cockroach infestation is not clear and a relatively lowconcentration is measured. While the cockroaches in the kitchenare most abundant, their presence in the bedroom and the livingroom may be more important for the induction of repeated wheezein infancy [31]. Research in Ethiopia demonstrated that cockroach-es are the potential source of multiresistant strains of bacterialpathogens and they are carriers of Klebsiella pneumonia [32]. Thismight enlighten the enhanced associations of respiratory symp-toms with a cockroach infestation.
Under-five children whose parents used new carpets at homewere 2.38 times more likely to suffer from respiratory symptomscompared with their counterparts. A possible explanation could bethat a new carpet can be a source of chemical emissions. In addi-tion to the carpet, the padding and adhesives all emit volatileorganic compounds and some people report symptoms such asupper respiratory irritations, skin rash, shortness of breath, cough,and fatigue, which they associate with the new carpet installation,and the distinct odor of new carpet is usually attributed to thechemicals 4-phenyl cyclohexane (4-PC) [33]. Children living in adamp house were 1.66 more likely to suffer from respiratory symp-toms. This study confirms previously-reported associationsbetween a damp stain and current respiratory symptoms in children[34,35]. Damp living conditions have adversely affected children’srespiratory health. Since both fungi and household dust mitesthrive in humid environments, an allergic reaction to one or both ofthese allergens is suggested as a significant contributing factor inthe development of more respiratory symptoms among childrenliving in humid homes [36]. In households where windows wereopen at the time of cooking, the risk of experiencing respiratorysymptoms among under-five children was 42% times less likely ascompared to those households which remained closed duringcooking time. Similar findings were reported to support this result[37,38]. Although most households reported opening windowsduring cooking, this study was conducted during winter and springseasons. The ventilation level will likely decrease over the summerseason as windows are often kept closed to minimize energy loss,which can contribute to higher summer indoor air pollutants thanthose found in this report [39]. Children living less than 100 mfrom heavy traffic were 1.94 times more likely to suffer from res-piratory symptoms. Moving traffic is highly associated with higheremissions of organic carbon, elemental carbon, carbon monoxide,nitric oxide, hydrocarbons, and soot. This might explain the fact
MRM_01 original.qxp_Hrev_master 28/09/20 15:35 Pagina 112
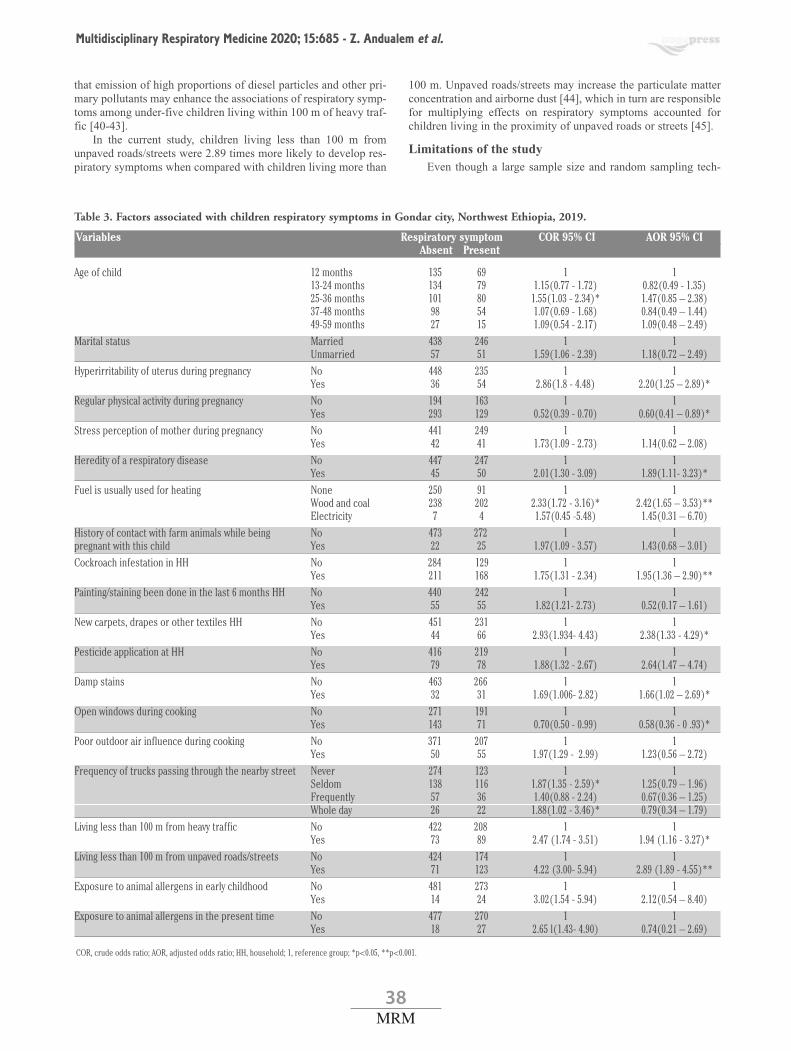
38MRM
Multidisciplinary Respiratory Medicine 2020; 15:685 - Z. Andualem et al.
that emission of high proportions of diesel particles and other pri-mary pollutants may enhance the associations of respiratory symp-toms among under-five children living within 100 m of heavy traf-fic [40-43].
In the current study, children living less than 100 m fromunpaved roads/streets were 2.89 times more likely to develop res-piratory symptoms when compared with children living more than
100 m. Unpaved roads/streets may increase the particulate matterconcentration and airborne dust [44], which in turn are responsiblefor multiplying effects on respiratory symptoms accounted forchildren living in the proximity of unpaved roads or streets [45].
Limitations of the studyEven though a large sample size and random sampling tech-
Table 3. Factors associated with children respiratory symptoms in Gondar city, Northwest Ethiopia, 2019.
Variables Respiratory symptom COR 95% CI AOR 95% CI Absent Present
Age of child 12 months 135 69 1 1 13-24 months 134 79 1.15(0.77 - 1.72) 0.82(0.49 - 1.35) 25-36 months 101 80 1.55(1.03 - 2.34)* 1.47(0.85 – 2.38) 37-48 months 98 54 1.07(0.69 - 1.68) 0.84(0.49 – 1.44) 49-59 months 27 15 1.09(0.54 - 2.17) 1.09(0.48 – 2.49)Marital status Married 438 246 1 1 Unmarried 57 51 1.59(1.06 - 2.39) 1.18(0.72 – 2.49)Hyperirritability of uterus during pregnancy No 448 235 1 1 Yes 36 54 2.86(1.8 - 4.48) 2.20(1.25 – 2.89)*Regular physical activity during pregnancy No 194 163 1 1 Yes 293 129 0.52(0.39 - 0.70) 0.60(0.41 – 0.89)*Stress perception of mother during pregnancy No 441 249 1 1 Yes 42 41 1.73(1.09 - 2.73) 1.14(0.62 – 2.08)Heredity of a respiratory disease No 447 247 1 1 Yes 45 50 2.01(1.30 - 3.09) 1.89(1.11- 3.23)*Fuel is usually used for heating None 250 91 1 1 Wood and coal 238 202 2.33(1.72 - 3.16)* 2.42(1.65 – 3.53)** Electricity 7 4 1.57(0.45 -5.48) 1.45(0.31 – 6.70)History of contact with farm animals while being No 473 272 1 1pregnant with this child Yes 22 25 1.97(1.09 - 3.57) 1.43(0.68 – 3.01) Cockroach infestation in HH No 284 129 1 1 Yes 211 168 1.75(1.31 - 2.34) 1.95(1.36 – 2.90)**Painting/staining been done in the last 6 months HH No 440 242 1 1 Yes 55 55 1.82(1.21- 2.73) 0.52(0.17 – 1.61)New carpets, drapes or other textiles HH No 451 231 1 1 Yes 44 66 2.93(1.934- 4.43) 2.38(1.33 - 4.29)*Pesticide application at HH No 416 219 1 1 Yes 79 78 1.88(1.32 - 2.67) 2.64(1.47 – 4.74)Damp stains No 463 266 1 1 Yes 32 31 1.69(1.006- 2.82) 1.66(1.02 – 2.69)*Open windows during cooking No 271 191 1 1 Yes 143 71 0.70(0.50 - 0.99) 0.58(0.36 - 0 .93)*Poor outdoor air influence during cooking No 371 207 1 1 Yes 50 55 1.97(1.29 - 2.99) 1.23(0.56 – 2.72)Frequency of trucks passing through the nearby street Never 274 123 1 1 Seldom 138 116 1.87(1.35 - 2.59)* 1.25(0.79 – 1.96) Frequently 57 36 1.40(0.88 - 2.24) 0.67(0.36 – 1.25) Whole day 26 22 1.88(1.02 - 3.46)* 0.79(0.34 – 1.79)Living less than 100 m from heavy traffic No 422 208 1 1 Yes 73 89 2.47 (1.74 - 3.51) 1.94 (1.16 - 3.27)*Living less than 100 m from unpaved roads/streets No 424 174 1 1 Yes 71 123 4.22 (3.00- 5.94) 2.89 (1.89 - 4.55)**Exposure to animal allergens in early childhood No 481 273 1 1 Yes 14 24 3.02(1.54 - 5.94) 2.12(0.54 – 8.40)Exposure to animal allergens in the present time No 477 270 1 1 Yes 18 27 2.65 l(1.43- 4.90) 0.74(0.21 – 2.69)
COR, crude odds ratio; AOR, adjusted odds ratio; HH, household; 1, reference group; *p<0.05, **p<0.001.
MRM_01 original.qxp_Hrev_master 28/09/20 15:35 Pagina 113

39MRM
Multidisciplinary Respiratory Medicine 2020; 15:685 - Z. Andualem et al.
nique employed in this study help for greater generalizability, thelack of measurements i.e. pulmonary function test was one of thelimitations. Furthermore, recall bias and social desirability biasesmight be high in such types of self-reported cross-sectional studies.
ConclusionsIn this study, the overall prevalence of respiratory symptoms
among under-five children was relatively high. Personal and envi-ronmental characteristics influencing symptom occurrence wereidentified. Respiratory symptoms will be minimized by reducingexposure to indoor and outdoor air pollution and enhancing hous-ing characteristics.
AcknowledgmentsWe are very indebted to Gondar City Health Office for permit-
ting to conduct the study and providing the necessary preliminaryinformation while conducting this study. We do wish to extend ourgratitude to the study participants, supervisors, and data collec-tors.
Abbreviations ALRIs: acute lower respiratory infections; AOR: adjusted odds ratio;ARI: acute respiratory infections;COR: crude odds ratio;HH: household;OR: odd ratio;SSA: sub-Saharan African.
References1. Rudan I, Tomaskovic L, Boschi-Pinto C, Campbell H. Global
estimate of the incidence of clinical pneumonia among chil-dren under five years of age. Bull World Health Organ2004;82:895-903.
2. Leowski J. Mortality from acute respiratory infections in chil-dren under 5 years of age: global estimates. World Health StatQ 1986;39:138-44.
3. Adesanya OA, Darboe A, Rojas BM, Abiodun DE, Beogo I.Factors contributing to regional inequalities in acute respirato-ry infections symptoms among under-five children in Nigeria:a decomposition analysis. Int J Equity Health 2017;16:140.
4. Accinelli RA, Leon-Abarca JA, Gozal D. Ecological study onsolid fuel use and pneumonia in young children: A worldwideassociation. Respirology 2017;22:149-56.
5. Ramani VK, Pattankar J, Puttahonnappa SK. Acute respiratoryinfections among under-five age group children at urban slumsof gulbarga city: A longitudinal study. J Clin Diagn Res2016;10:LC08.
6. Seidu AA, Dickson KS, Ahinkorah BO, Amu H, Darteh EKM,Kumi-Kyereme A. Prevalence and determinants of acute lowerrespiratory infections among children under-five years in sub–Saharan Africa: evidence from demographic and health sur-veys. SSM Popul Health 2019;8:100443.
7. Nandasena S, Wickremasinghe AR, Sathiakumar N. Indoor airpollution and respiratory health of children in the developingworld. World J Clin Pediatr 2013;2:6.
8. Akinyemi JO, Morakinyo OM. Household environment and
symptoms of childhood acute respiratory tract infections inNigeria, 2003–2013: a decade of progress and stagnation.BMC Infect Dis 2018;18:296.
9. Quintussi M, Van de Poel E, Panda P, Rutten F. Economic con-sequences of ill-health for households in northern rural India.BMC Health Serv Res 2015;15:179.
10. Miller NP, Amouzou A, Tafesse M, Hazel E, Legesse H,Degefie T, et al. Integrated community case management ofchildhood illness in Ethiopia: implementation strength andquality of care. Am J Trop Med Hyg 2014;91:424-34.
11. Kolawole O, Oguntoye M, Dam T, Chunara R. Etiology of res-piratory tract infections in the community and clinic in Ilorin,Nigeria. BMC Rese Notes 2017;10:712.
12. Ujunwa F, Ezeonu C. Risk Factors for acute respiratory tractinfections in under-five children in Enugu Southeast Nigeria.Ann Med Health Sci Res 2014;4:95-9.
13. Arifin WN. Introduction to sample size calculation. Educ MedJ 2013;5:130.
14. Woldeamanuel BT, Gebreyesus HL. Prevalence and risk fac-tors for chest-related symptoms of acute respiratory tract infec-tions among under five children: Case of Ethiopia. J Tre BioRes 2019;2:1-7.
15. Sharma D, Kuppusamy K, Bhoorasamy A. Prevalence of acuterespiratory infections (ARI) and their determinants in underfive children in urban and rural areas of Kancheepuram dis-trict, South India. Ann Trop Med Public Health 2013;6:513.
16. Yousef FM, Hamed AF. Prevalence of acute respiratory infec-tion and related risk factors in school-age children in Egypt: across-sectional study. Int J Curr Res Med Sci 2016;2:50-8.
17. Hasan M, Tasfina S, Haque SR, Saif-Ur-Rahman K,Khalequzzaman M, Bari W, et al. Association of biomass fuelsmoke with respiratory symptoms among children under 5years of age in urban areas: results from Bangladesh UrbanHealth Survey, 2013. Environ Health Prev Med 2019;24:65.
18. Benefits Bridge. United Concordia [Internet]. 6 common respi-ratory disease symptoms to be aware of. 2019. Accessed on: 8February 2019. Available from: https://benefitsbridge.united-concordia.com/6-common-respiratory-disease-symptoms-to-be-aware-of/
19. Mickey RM, Greenland S. The impact of confounder selectioncriteria on effect estimation. Am J Epidemiol 1989;129:125-37.
20. Dagne H, Andualem Z, Dagnew B, Taddese AA. Acute respi-ratory infection and its associated factors among childrenunder-five years attending pediatrics ward at University ofGondar Comprehensive Specialized Hospital, NorthwestEthiopia: institution-based cross-sectional study. BMC Pediatr2020;20:1-7.
21. Savitha AK, Gopalakrishnan S. Determinants of acute respira-tory infections among under five children in a rural area ofTamil Nadu, India. J Family Med Prim Care 2018;7:1268-73.
22. Maharjan PL, Sharma Y. Prevalence and determinants of acuterespiratory infection among children under age five in GorkhaMunicipality, Gorkha. Glob J Pharmaceu Sci 2017;2:555588.
23. Nagdyman N, Kömen W, Ko HK, Müller C, Obladen M. Earlybiochemical indicators of hypoxic-ischemic encephalopathyafter birth asphyxia. Pediatr Res 2001;49:502-6.
24. Moyer C, Reoyo OR, May L. The influence of prenatal exer-cise on offspring health: A review. Clin Med Insights WomensHealth 2016;9:37-42.
25. The New Work Times [Internet]. Exercise during pregnancymay have lasting benefits for babies (G. Reynolds). 2019.Accessed on: 19 August 2019. Available from:https://www.nytimes.com/2019/08/07/well/move/exercise-during-pregnancy-may-have-lasting-benefits-for-babies.html
26. National Center for Biotechnology Information (US). Genes
MRM_01 original.qxp_Hrev_master 28/09/20 15:35 Pagina 114

40MRM
Multidisciplinary Respiratory Medicine 2020; 15:685 - Z. Andualem et al.
and Disease [Internet]. 1998. Accessed on: 15 March 2020.Available from: https://www.ncbi.nlm.nih.gov/books/NBK22167/
27. Triche EW, Belanger K, Beckett W, Bracken MB, Holford TR,Gent J, et al. Infant respiratory symptoms associated withindoor heating sources. Am J Respir Crit Care Med2002;166:1105-11.
28. WHO. Residential heating with wood and coal: health impactsand policy options in Europe and North America. 2015.Avilable from: https://www.euro.who.int/__data/assets/pdf_file/0009/271836/ResidentialHeatingWoodCoalHealthImpacts.pdf
29. Riddervold I, Bønløkke J, Olin AC, Grønborg T, SchlünssenV, Louring-Skogstrand K, et al. Effects of wood smoke parti-cles from wood-burning stoves on the respiratory health ofatopic humans. ParticFibre Toxicol 2012;9:12.
30. Do DC, Zhao Y, Gao P. Cockroach allergen exposure and riskof asthma. Allergy 2016;71:463-74.
31. Gold DR, Burge HA, Carey V, Milton DK, Platts-Mills T,Weiss ST. Predictors of repeated wheeze in the first year oflife: the relative roles of cockroach, birth weight, acute lowerrespiratory illness, and maternal smoking. Am J Respir CriticCare Med 1999;160:227-36.
32. Moges F, Eshetie S, Endris M, Huruy K, Muluye D, Feleke T,et al. Cockroaches as a source of high bacterial pathogens withmultidrug resistant strains in Gondar town, Ethiopia. BioMedRes Int 2016;2016:2825056.
33. MedicineNet [Internet]. New carpet allergy. 2017. Accessedon: 15 March 2020. Available from: https://www.medi-cinenet.com/script/main/art.asp?articlekey=21803
34. WHO. Report of the International Conference onEnvironmental threats to the health of children: Hazards andvulnerability, Bangkok, 3-7 March 2002. Genwva: WorldHealth Organization; 2002.
35. Garrett MH, Rayment PR, Hooper MA, Abramson MJ,Hooper BM. Indoor airborne fungal spores, house dampness
and associations with environmental factors and respiratoryhealth in children. Clin Exp Allergy 1998;28:459-67.
36. Li CS, Hsu LY. Home dampness and childhood respiratorysymptoms in a subtropical climate. Arch Environ Health1996;51:42-6.
37. Abuka T. Prevalence of pneumonia and associated factorsamong children 2-59 months old in Wondo Genet district,Sidama zone, SNNPR, Ethiopia. Curr Pediatr Res 2017;21.
38. Fekadu GA, Terefe MW, Alemie GA. Prevalence of pneumo-nia among under-five children in Este Town and the surround-ing rural Kebeles, Northwest Ethiopia: a community basedcross sectional study. Sci J Public Health 2014;2:150-5.
39. Rumchev K, Spickett J, Brown H, Mkhweli B. Indoor air pol-lution from biomass combustion and respiratory symptoms ofwomen and children in a Zimbabwean village. Indoor Air2008;17:468-74.
40. Shah SD, Cocker DR, Miller JW, Norbeck JM. Emission ratesof particulate matter and elemental and organic carbon fromin-use diesel engines. Environ Sci Technol 2004;38:2544-50.
41. Tong H, Hung W, Cheung C. On-road motor vehicle emissionsand fuel consumption in urban driving conditions. J Air WasteManage Assoc 2000;50:543-54.
42. Ryan PH, LeMasters G, Biagini J, Bernstein D, GrinshpunSA, Shukla R, et al. Is it traffic type, volume, or distance?Wheezing in infants living near truck and bus traffic. J AllergyClin Immunol 2005;116:279-84.
43. Garshick E, Laden F, Hart JE, Caron A. Residence near amajor road and respiratory symptoms in U.S. veterans.Epidemiology 2003;14:728-36.
44. Khan RK, Strand MA. Road dust and its effect on humanhealth: a literature review. Epidemiol Health2018;40:e2018013.
45. Sarmiento-Suárez R, Medina K. Prevalence of respiratorysymptoms associated with outdoor and indoor air pollution inBogota 2012. WIT Transactions on the built environment.2013;134:713-24
Received for publication: 6 May 2020. Accepted for publication: 10 August 2020.This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0).©Copyright: the Author(s), 2020Licensee PAGEPress, ItalyMultidisciplinary Respiratory Medicine 2020; 15:685doi:10.4081/mrm.2020.685
MRM_01 original.qxp_Hrev_master 28/09/20 15:35 Pagina 115

41MRM
Primary care management of allergic rhinitis: a cross-sectional study in four ASEANcountriesBaharudin Abdullah,1 Kornkiat Snidvongs,2 Marysia Recto,3 Niken Lestari Poerbonegoro,4 De Yun Wang5
1Department of Otorhinolaryngology – Head and Neck Surgery, School of Medical Sciences, Universiti Sains Malaysia,Kelantan, Malaysia2Endoscopic Nasal and Sinus Surgery Excellence Center Chulalongkorn Hospital, Department of Otolaryngology, Faculty ofMedicine, Chulalongkorn University, Thailand 3Adult and Pediatric Division of Allergy and Immunology, University of the Philippines - Philippine General Hospital,Manila, Philippenes4Department of Otorhinolaryngology-Head and Neck Surgery, Faculty of Medicine Universitas Indonesia/Dr. CiptoMangunkusumo Hospital, Jakarta 5Department of Otolaryngology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Background: In primary care, general practitioners (GPs) and pharmacists are tasked with the frontline responsibilityof identifying and managing allergic rhinitis (AR) patients. There are currently no consolidated data on current treat-ment practices, patient compliance, and usage of guidelines within Southeast Asian Nations (ASEAN).Objective: To assess the attitudes and practices on AR of GPs and pharmacists in 4 ASEAN countries (Philippines,Indonesia, Thailand, and Malaysia).Methods: A cross-sectional survey of 329 GPs and 548 pharmacists was conducted from May to November 2019.Participants answered a questionnaire focused on their i) current practice in the management of AR, ii) views onpatient compliance, iii) understanding and usage of guidelines. Results: Clinical history was the most preferred method to diagnose AR by 95.4% of GPs and 58.8% of pharmacists.Second-generation antihistamines were the most widely available treatment option in GP clinics and pharmacies(94.8% and 97.2%) and correspondingly the most preferred treatment for both mild (90.3%, 76.8%) to moderate-severe rhinitis (90.3%, 78.6%) by GPs and pharmacists, respectively. Loratadine was ranked as the most preferred 2nd
generation antihistamines (GP vs pharmacists: 55.3% vs 58.9%). More than 90% of GPs and pharmacists rankedlength and efficacy of treatment as important factors that increase patient compliance. Awareness of the ARIA guide-lines was high among GPs (80%) and lower among pharmacists (48.4%). However, only 63.3% of GPs and 48.2% ofpharmacists knew how to identify AR patients. Conclusions: The survey in the 4 ASEAN countries has identified a need to strengthen the awareness and use of ARIAguidelines among the primary care practitioners. Adherence to ARIA guidelines, choosing the appropriate treatmentoption and prioritizing factors that increases patient compliance may contribute to better management outcomes of ARat the primary care practiceKey words: Allergic rhinitis; management; ASEAN; primary care; general practitioners; multidisciplinary.
AB
STR
ACT
Correspondence: Professor Baharudin Abdullah, Department of Otorhinolaryngology – Head and Neck Surgery, School ofMedical Sciences, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia. Tel. +60.97676416 - Fax: +60.97676424. E-mail: [email protected]
Contributions: All the authors made a substantive intellectual contribution. All the authors have read and approved the finalversion of the manuscript and agreed to be accountable for all aspects of the work. Conflict of interest: All authors declare no conflict of interest.Financial support: Bayer Consumer Health ASEAN (Malaysia, Thailand, Philippines, Indonesia) provided logistic support inorganizing the education symposiums where the surveys were conducted. Bayer Co. (Malaysia) Sdn. Bhd. further provided supportin respect of publication costs but had no influence on the content of the work. Availability of data and materials: The data used to support the findings of this study are available from the corresponding authorupon request.
Ethic approval and consent to participate: Ethical approval was obtained from Human Research Ethics Committee USM(Universiti Sains Malaysia) (USM/JEPeM/ 19050284).
Consent for publication: Not applicable.
ORIGINAL RESEARCH ARTICLE
Multidisciplinary Respiratory Medicine 2020; volume 15:726
MRM_01 original.qxp_Hrev_master 07/12/20 21:10 Pagina 154

42MRM
Multidisciplinary Respiratory Medicine 2020; 15:726 - B. Abdullah et al.
Introduction Allergic rhinitis (AR) is defined as an IgE-mediated symp-
tomatic disorder of the nose induced after allergen exposure [1].AR affects approximately 40% of the population globally, withprevalence rates on the rise and records the highest ones in the AsiaPacific [2,3]. As of 2011, the prevalence is reported to be 8.7%across eight Asia Pacific regions [3]. A survey conducted inSingapore revealed that AR was the key complaint of patients (10-40%) visiting primary care clinics [4]. With this high patient load,it becomes pertinent to establish a strong healthcare ecosystem,comprising of a spectrum of healthcare professionals – specialists,general practitioners (GPs) and pharmacists, to come together andoptimize AR management. In the primary care environment, GPsand pharmacists are key healthcare providers. GPs are responsiblefor diagnosis, treatment recommendations and patient counselling.Pharmacists, on the other hand, are responsible for dispense ofmedications and identification of AR patients for further referraland diagnosis by doctors. With overlap symptoms amongst AR andcolds, as well as increasing availability of over-the-counter (OTC)drugs in AR management, pharmacists’ understanding in AR man-agement and identification of AR patients becomes a critical stepin the healthcare ecosystem for AR management [1].
The allergic rhinitis and its impact on asthma (ARIA) guide-lines aim to provide evidence-based recommendations to cliniciansfor the management of AR and asthma [1,5]. It has previously beenreported that adherence to guidelines such as ARIA for the treat-ment of AR yielded better patient outcomes [6]. Nonetheless,despite the recognized importance of guidelines, current literaturepinpoints to low-level awareness on the ARIA guidelines amongboth the GPs and pharmacists [7]. Consistently, within the AsiaPacific, another survey conducted on more than 500 MalaysianGPs; ear, nose, and throat (ENT) specialists and pharmacistsdemonstrated that 42% of the pharmacists and 11% of the GPswere not satisfied with ARIA guidelines mainly due to the lack ofstepwise guidance for management of AR in the primary care set-ting. This study also revealed that antihistamines remained themost preferred choice for mild AR treatment, as recommended by51% GPs, 45% ENT specialists, and 78% pharmacists [8].
Most recently, an expert consensus article from Malaysia iden-tified gaps between the current guidelines and real-world practice,with emphasis at the primary management level. Specific to anti-histamine treatments, the authors presented guidance for primarycare practitioners by introducing a three-step approach: i) profileeach patient; ii) review patient-specific considerations based onprofile; iii) recommend and monitor treatment responses andalways escalate up to specialist care in more severe or difficult-to-treat cases [9].
Compared to other regions of the world, data on primary careattitudes and practices in the management of AR is still limited inthe Association of Southeast Asian Nations (ASEAN). To closethis gap, focusing on primary care in Malaysia, Indonesia,Philippines, and Thailand, our study seeks to better understand pri-mary care in terms of: i) their current practice in the managementof AR in primary care; ii) their views on patient compliance; andiii) their understanding and usage of guidelines.
Methods
SubjectsThis cross-sectional survey involving GPs and pharmacists, in
four ASEAN countries (Philippines, Indonesia, Thailand, andMalaysia) was conducted from May to November 2019. Ethicalapproval was obtained from Human Research Ethics CommitteeUSM (USM/JEPeM/ 19050284). Each survey was conductedbefore allergy-focused education symposiums and workshops. Weused a probability-based sampling methodology to obtain a repre-sentative national sample of GPs and pharmacists across regions ineach country, comprising approximately 100 GPs and 100 pharma-cists per country (50% GPs and 50% pharmacists) giving a totaltarget sample size of 800. A total of 902 responses were received,of which 887 (GPs: 329, pharmacists: 548) were considered. Thereason for any exclusion of responses from the data analysis wasprofession other than primary care practice.
QuestionnaireThe questionnaire for this study entitled ‘ASEAN Primary
Care Survey for Allergy Rhinitis Care’ was designed, followingpreviously conducted survey publications [8,10,11]. It consisted of32 questions divided into five sections:1. Demographics/Screener2. Pharmacy practice/clinical practice followed3. Perception of antihistamines in primary care4. Understanding of AR and the guidelines5. Understanding of ARIA guidelines
The questionnaire was uploaded on an online platform usingthe Google form (https://www.google.com/forms/about/) and had astatement at the beginning, briefing participants about the purposeof conducting this survey. No personal data was collected duringthis survey study. The link of the survey was shared with partici-pants at allergy-focused education symposiums and workshops.
Statistical analysisAfter the closure of access to the survey, the data for each
country survey was downloaded directly from Google Forms in theMicrosoft© Excel form. The data on responses of GPs and pharma-cists for each country were extracted, and then the data were clus-tered for all the four ASEAN countries for GP and pharmacists. Forevaluation of the responses to all survey questions, the count andpercentages of each option of the questions were calculated. Therewere some questions in the survey where participants may selectmore than one option. Categorical data was analyzed using theChi-square/Fisher exact test, and the continuous data variableswere assessed with a t-test for two independent variables/Mann-Whitney U test depending upon the distribution of the data. T-testwas used for two independent samples with normal distributionwhile Mann-Whitney U test was used for data with huge variation(not-normally distributed data). Statistical significance wasassessed at p<0.05 adjusted with Bonferroni correction for multi-ple tests. SPSS v23.0 software was used for data analysis.
Results
Characteristics of respondentsIn the ‘GPs’ group, all respondents are certified medical doc-
tors who see patients in the community. Taken together, they see amedian of 100 patients/week. The clinical experience and addition-al profile details of participants are given in Table 1. In the‘Pharmacists’ group, most of the respondents were retail and com-munity pharmacists (83%), while a few were hospital pharmacists(14%). The pharmacists see a median 200 patients/week(p<0.001). The clinical experience and additional profile details ofthe participating pharmacists are given in Table 1.
MRM_01 original.qxp_Hrev_master 07/12/20 21:10 Pagina 155

43MRM
Multidisciplinary Respiratory Medicine 2020; 15:726 - B. Abdullah et al.
Diagnosis of allergic rhinitis Overall, 95% percent of the GPs and 58.8% of pharmacists
used clinical history to identify AR patients (p<0.001). Less than15% of GPs chose other diagnostic techniques such as imagingparanasal sinuses, and nasal endoscopy. In comparison, becausepharmacists are not professionally trained to diagnose the condi-tion, less than 10% of pharmacists utilized diagnosis methods suchas anterior rhinoscopy, allergy testing, imaging paranasal sinusesand nasal endoscopy, and only 48.2% of pharmacists respondedthat they knew how to identify AR patients (Table 2).
Treatment of allergic rhinitisIn both GP clinics and pharmacies, there is a good range of
treatment options for AR, comprising of single and combinationdrugs, as well as non-drug options such as saline douching.Noteworthy, almost all GP clinics and pharmacies have 1st and 2nd
generation antihistamines in stock, and nearly all pharmacies havethe combination of oral antihistamines and decongestants in stock.This is indicated by agreement levels of more than 90% respond-
ing “yes” to all listed treatment options. Corresponding to treat-ment availability, 2nd generation antihistamines are the most pre-ferred treatment option for AR patients regardless of disease sever-ity, as selected by both GPs and pharmacists responding “alwaysrecommend” based on the listed treatment options (90.2% and76.3% for mild AR; 90.2% and 78.6% for moderate-severe ARpatients), respectively. This was statistically more significant than1st generation antihistamines or the combination of oral antihis-tamines and decongestants (p<0.001). For moderate-severe ARpatients compared to mild AR patients, there is also an increasedpreference among GPs to recommend intranasal corticosteroids(67.8% vs. 40.1%) and the combination of oral antihistamines anddecongestants (68.1% vs 59%). Non-drug treatment are also pre-ferred treatment options for both mild and moderate-severe ARpatients including saline douching (46.1% and 53% for GP; 42%and 48.5% for pharmacist) and allergen avoidance (71% and71.3% for GP; 57.7% and 58.4% for pharmacist). Taken together,these data demonstrate that antihistamines, particularly 2nd genera-tion antihistamines, are still the mainstay of AR treatment in pri-mary care practice within ASEAN. With 2nd generation antihis-
Table 1. Demographics details of the respondents who participated in this survey study.
Profile Malaysia Thailand Philippines Indonesia Total (N) General practitioners / Medical doctors
N of respondents, n (%) 57 (100) 89 (100) 108 (100) 63 (100) 317 Composition, n (%) Years of practice, n (%) <5 years 1 (1.8) 63 (70.8) 41 (37.9) 19 (30.1) 132 5-10 years 6 (10.5) 19 (21.4) 35 (32.4) 11 (17.5) 75 11-20 years 21 (36.8) 6 (6.7) 21 (19.4) 23 (36.5) 71 >20 years 29 (50.9) 1 (1.1) 11 (10.2) 10 (15.9) 51 Place of practice, n (%) Private sector 54 (94.7) 8 (9) 70 (64.8) 34 (54) 177 Public sector 3 (5.3) 81 (91) 38 (35.2) 29 (46) 152 Median number of patients seen/week (range), IQR 150 (7-501), 200 150 (1-500), 180 60 (3-1000), 70 100 (6-700), 120 100 (1-1000), 160Median number of patients with AR seen/week (range), IQR 20 (0-2020), 23 10 (1-80), 15 10 (0-60), 15 10 (1-100), 10 10 (0-2020), 15Median number of patients with asthma seen/week (range), IQR 7 (0-77), 14 3 (0-50), 11 9 (0-120), 10 5 (0-100), 8 5 (0-120), 8Median number of patients with both AR and asthma seen/week 5 (0-70), 8 5 (0-50), 9 5 (0-100), 7 2 (0-100), 4 5 (0-100), 8(range), IQR Pharmacists
N. of respondents (%) 194 (100) 39 (100) 216 (100) 99 (100) 548Composition (%) Retail/community pharmacist 141 (72.7) 29 (74.4) 206 (95.4) 96 (97) 472 Hospital pharmacist 53 (27.3) 10 (25.6) 10 (4.6) 3 (3.1) 76Years of practice, n (%) <5 years 85 (43.8) 12 (30.8) 97 (44.9) 84 (84.9) 278 5-10 years 52 (26.8) 17 (43.6) 58 (26.9) 12 (12.1) 139 10-20 years 40 (20.6) 10 (25.6) 35 (16.2) 1 (1) 86 >20 years 17 (8.8) - 26 (12) 2 (2) 45Place of practice, n (%) Private sector 134 (69.0) 30 (76.9) 189 (87.5) 4 (4) 357 Public sector 60 (31.0) 9 (23.1) 27 (12.5) 95 (96) 191 Median number of patients seen/week (range), IQR 150 (0-4000), 335 300 (7-1500), 420 150 (4-10000), 200 400 (7-2000), 550 200 (0-10000)*, 300 Median number of patients with AR seen/week (range), IQR 30 (0-1500), 60 40 (0-350), 70 30 (2-2000), 70 30 (1-300), 45 30 (0 – 2000)*, 70 Median number of patients with asthma seen/week (range), IQR 20 (0-1000), 34 10 (0-150), 25 30 (1-2000), 50 10 (1-200), 45 20 (0 – 2000)*, 40 Median number of patients with both AR and asthma seen/week 10 (0-500), 20 10 (0-100), 16 25 (2-2000), 39 10 (0-300), 22 15 (0 – 2000)*, 25 (range), IQR
AR, Allergic rhinitis; GP, general practitioner; IQR, interquartile range; *represent p<0.001 comparing GP with pharmacists.
MRM_01 original.qxp_Hrev_master 07/12/20 21:10 Pagina 156

44MRM
Multidisciplinary Respiratory Medicine 2020; 15:726 - B. Abdullah et al.
tamines selected as the most preferred treatment option for ARpatients (mild to severe) in primary care practice both GPs andpharmacists agreed that antihistamines are always effective in thetreatment of patients with mild-moderate AR (91.8 % and 92%),respectively. It is further demonstrated that out of the six common-ly-available 2nd generation antihistamines in ASEAN, loratadine isranked as the most preferred choice amongst GPs and pharmacists(55.2 %% and 58.9%).This is followed by cetirizine (41% and40.5%) .When it comes to primary care considerations prior to therecommendation of antihistamines, GPs are mostly concerned withthe efficacy of the drug (94.6%), whilst pharmacists are furtherconcerned with use during pregnancy and breastfeeding (91.6%)and side effects such as somnolence (90%), aside from efficacy ofdrug (96.7%).
Patient compliance and management in primary carepractice
From a predetermined list of factors, both GPs (Figure 1A) andpharmacists (Figure 2B) in Malaysia, Philippines, Thailand andIndonesia listed length of treatment (95.9 % and 93.4%), treatmentefficacy (94.1 % and 94.7%) and route of administration (91.8 %and 92.2%) as the top 3 factors influencing patient’s compliance toAR treatment. Noteworthy, majority of the pharmacists think thatpatients’ phobia of steroids (72.6% pharmacists vs 62.5 % GPs;p<0.001) is the other key factor influencing patient compliance(Figure 1 A,B).
With a preliminary understanding of primary care practice, aquestion was included in the survey on ‘what else is needed to opti-mize AR management in primary care’. A predetermined list offactors was provided to respondents: i) accurate diagnosis of AR;ii) availability of allergy testing; iii) allergen avoidance measures;iv) disease awareness and health education for patients; v) accessi-bility and cost of treatment; vi) recommended length of treatment;vii) dedicated guidelines for primary care. More than 90% of bothGPs and pharmacists agreed that all these factors, except for (ii)availability of allergy testing, are needed to optimize AR manage-ment in primary care practice (Figure 2 A,B). Specific to allergytesting, it is noteworthy that more pharmacists agreed that this fac-tor is needed, as compared to GPs (84.3% of pharmacists vs 63.8%of GPs; p<0.001) (Figure 2 A,B). This corresponds to less than halfof both GPs and pharmacists agreeing that specific allergy testingis necessary to distinguish between AR and non-AR conditions(45.7 % vs 47.6%), respectively (Table 2).
Awareness and perception of guidelines in primary carepractice
Within Malaysia, Philippines, Thailand and Indonesia, theauthors are well aware that GPs play a major role in diagnosis ofAR, which explain more GPs than pharmacists (80.8 % vs 48.4%;p<0.001) are aware of the ARIA guidelines that govern treatmentrecommendations for patients diagnosed with AR (Table 2). Thislevel of awareness was similar for the Global Initiative for Asthma
Table 2. General practitioners and pharmacists’ agreement on statements pertaining to their understanding and management of allergicrhinitis. The percentage of respondents who chose “Agree”, “Neutral” or “Disagree” to specific questions asked is shown.
Responses GP n (%) Pharmacists n (%) p, N=317 N=548 comparing GP to pharmacists
Do you know ARIA guidelines? Yes 256 (80.8) 265 (48.4) <0.001 No 22 (6.9) 115 (20.9) Not Sure 39 (12.3) 168 (30.7) Do you know GINA guidelines? Yes 242 (76.3) 223 (40.7) <0.001 No 25 (7.9) 144 (26.3) Not Sure 50 (15.8) 181 (33) Do you know other guidelines for AR? Yes 56 (17.7) 47 (8.6) <0.001 No 118 (37.2) 208 (38) Not Sure 143 (45.1) 293 (53.5) Do you know rhinitis can be classified into AR and non-AR? Yes 215 (67.8) 270 (49.3) <0.001 No 42 (13.2) 98 (17.9) Not Sure 60 (18.9) 180 (32.8) Is specific allergy testing necessary to distinguish between AR and non-AR? Yes 145 (45.7) 261 (47.6) <0.001 No 76 (24) 82 (15) Not Sure 96 (30.3) 205 (37.4) In your opinion, is an evaluation of asthma necessary for AR patients? Yes 254 (80.1) 356 (65) <0.001 No 20 (6.3) 53 (9.6) Not sure 43 (13.6) 139 (25.4) Do you know how to identify AR patients? Yes 259 (81.7) 264 (48.2) <0.001 No 10 (3.2) 85 (15.5) Not sure 48 (15.1) 199 (36.3) Do you know the common symptoms of AR? Yes 286 (90.2) 380 (69.3) <0.001 No 4 (1.3) 43 (7.8) Not sure 27 (8.5) 125 (22.8) Do you know how to classify allergic rhinitis based on severity? Yes 236 (74.4) 236 (43.1) <0.001 No 26 (8.2) 100 (18.2) Not sure 55 (17.4) 212 (38.7)
AR, Allergic rhinitis; ARIA, allergic rhinitis and its impact on asthma; GINA, global initiative for asthma; GP, general practitioner.
MRM_01 original.qxp_Hrev_master 07/12/20 21:10 Pagina 157

45MRM
Multidisciplinary Respiratory Medicine 2020; 15:726 - B. Abdullah et al.
Figure 1. Factors influencing patient compliance to allergic rhinitis treatment. A) General practitioners; B) Pharmacists. Respondentswere asked to review the listed factors that may influence patient compliance to allergic rhinitis treatment. The percentage of respon-dents who chose “Agree”, “Neutral” or “Disagree” to specific factors is shown.
Figure 2. Factors needed to optimize AR management in primary care practice. A) General practitioners; B) Pharmacists. Respondentswere asked to review the listed factors that are needed to optimize allergic rhinitis management in primary care practice. The percentageof respondents who chose “Agree”, “Neutral” or “Disagree” to specific factors is shown.
MRM_01 original.qxp_Hrev_master 07/12/20 21:10 Pagina 158

46MRM
Multidisciplinary Respiratory Medicine 2020; 15:726 - B. Abdullah et al.
(GINA) guidelines (76.3 % vs 40.7%; p<0.001) (Table 2). GPs alsohad more knowledge on differentiating rhinitis into AR and non-AR, as compared to pharmacists (67.8% vs 49.3%; p<0.001),respectively (Table 2). A modest percentage of both GPs and phar-macists agree that the evaluation of asthma is necessary for AR(80.1 % and 65%), respectively (Table 2).
Amongst those who have a moderate to full understandingARIA (respondents who selected ‘not sure’ or ‘yes’), a high per-centage of both GPs and pharmacists still agreed that the ARIAguidelines are useful in the diagnosis and treatment of AR patients(Table 3). Additionally, both GPs and pharmacists agreed that ARcan be classified into ‘mild’ or ‘moderate/severe’ depending on theseverity of the symptoms and quality of life outcomes, alignedwith ARIA guidelines (Table 3). Almost 80% of GPs and pharma-cists agreed that the diagnosis of AR should be based upon the con-cordance between a typical history of allergic symptoms and aller-gy tests (Table 3).
Discussion This survey presents findings on the attitudes and current prac-
tices of primary healthcare providers (GPs and pharmacists) man-aging AR in four ASEAN countries. The survey findings showedthat a majority of GPs and only 50% of pharmacists rely on clinicalhistory to identify AR, irrespective of the severity of the disease.Despite the many new treatment options available for AR, second-generation oral antihistamines remained the mainstay treatmentoption preferred by both GPs and pharmacists, with loratadinebeing the most recommended antihistamine option. Several factorsand considerations were regarded as key to influencing patientcompliance and optimizing AR management at a primary carelevel. Lastly, on guidelines, most GPs and pharmacists agreed thatguidelines such as ARIA are useful in the treatment and diagnosisof AR.
Management of AR in primary care practice still heavily relieson clinical history for diagnosis. Clinical history is the most pre-
ferred method by 95 % of GPs in this study. Clinical history of AR,non-AR, chronic rhinosinusitis may be different, and thus clinicalhistory may be helpful to differentiate AR from other upper respi-ratory diseases. The symptoms-based diagnosis of CRS has mod-erate reliability of around 60% [12-14]. Similarly, complete anddetailed history taking can result in prompt AR diagnosis of up to>80% [15]. However, clinical history is still inadequate in makinga definitive diagnosis of type of allergies. For example, in a studyconducted in the Philippines on 85 children, the sensitivity of clin-ical symptoms to diagnose AR was >80% and specificity was<30% compared to skin prick testing [15]. More pharmacists thanGPs, agreed that allergy testing is needed to make a definitive diag-nosis of AR (84.3% of pharmacists vs 63.8% of GPs; p<0.001).The detection of specific IgE through skin prick or in vitro allergytesting is mandatory for diagnosing allergic disease. There aremany differential diagnoses of AR, which are non-allergic (forexample, vasomotor rhinitis, rhinitis medicamentosa, NARES andthe very common infectious rhinitis), and are often mistaken forAR. Therefore, the risk of overdiagnoses of AR is present if werely on clinical history alone. Nonetheless, the relevance, andimplementation of allergy testing in primary care is controversial.Serum specific IgE testing is also expensive, not readily availableand requires handling by laboratory technicians. As such, allergytesting is best done in tertiary settings by specialists. Thus, at a spe-cialist level, allergy testing should be made more widely availableand affordable for the specialist centers to utilize optimally. Onother diagnostic methods, less than 15% of GPs chose imagingparanasal sinuses and nasal endoscopy. Imaging is not a recom-mended modality for diagnosis of AR and it is technically chal-lenging to perform a nasal endoscopy examination at a primarycare clinic. The majority of GPs would perform anteriorrhinoscopy, which is relatively simpler to assess nasal congestionand nasal discharge. Despite varied preferences on diagnosis meth-ods, it is an interesting observation that almost 80% of GPs andpharmacists agreed that the diagnosis of AR needs to be basedupon the concordance between a typical history of allergic symp-toms and allergy tests. Therefore, for primary care, the best
Table 3. GPs and pharmacists’ agreement on statements pertaining to guidelines for allergic rhinitis management. The percentage ofrespondents who chose “Agree”, “Neutral” or “Disagree” to specific statements listed is shown.
Responses GP n (%) Pharmacists n (%) p-value, N = 301* N = 433* comparing GP to pharmacists
The ARIA guidelines are useful in diagnosing AR patients Agree 273 (90.7) 361 (83.4) 0.011 Neutral 27 (9) 69 (15.9) Disagree 1 (0.3) 3 (0.7) The ARIA guidelines are useful for the treatment of your AR patients Agree 280 (93.6) 368 (85) <0.001 Neutral 17 (5.7) 65 (15) Disagree 2 (0.7) 0 Aligned with the ARIA guidelines, allergic rhinitis can be sub-divided into Agree 266 (88.4) 348 (80.4) 0.013"intermittent" or "persistent" based on duration of symptoms Neutral 33 (11) 80 (18.5) Disagree 2 (0.7) 5 (1.2) Aligned with the ARIA guidelines, the severity of allergic rhinitis can be Agree 276(91.7) 357 (82.4) <0.001classified as “mild” or “moderate/severe” depending on the severity Neutral 23 (7.6) 73 (16.9)of the symptom and quality of life outcomes life outcomes Disagree 2 (0.7) 3 (0.7) The diagnosis of allergic rhinitis is based upon the concordance between Agree 229 (76.1) 343 (79.2) 0.035a typical history of allergic symptoms and allergy tests Neutral 58 (19.3) 84 (19.4) Disagree 14 (4.7) 6 (1.4)
*Only respondents who stated “yes/ not sure” to the question “Do you know allergic rhinitis and its impact on asthma (ARIA) guidelines?” responded to these questions; AR, Allergic rhinitis; ARIA, aller-gic rhinitis and its impact on asthma; GP, general practitioner.
MRM_01 original.qxp_Hrev_master 07/12/20 21:10 Pagina 159

47MRM
Multidisciplinary Respiratory Medicine 2020; 15:726 - B. Abdullah et al.
approach may be to conduct more education programs to promotesymptoms-based evaluation and escalation to specialists for diag-nosis.
The survey results demonstrated that antihistamines, particu-larly 2nd generation antihistamines, are still the mainstay of ARtreatment in primary care practice within Malaysia, Philippines,Thailand and Indonesia. This correlated with a survey from thePhilippines [11] that assessed the specialists’ and GPs’ attitudesand practices followed for the treatment of the AR patients. Theauthors showed that monotherapy, mainly antihistamines, was thepreferred choice for mild AR treatment. For moderate-severepatients, both monotherapy (intranasal corticosteroid spray; INCS)and combination therapy with antileukotrienes, antihistamines,INCS were preferred. The choice of these therapeutic regimes wasprimarily attributed to efficacy and cost-effectiveness [11]. In con-trast, the Current Allergic Rhinitis Experiences Survey (CARES)[16], which assessed the AR management practices followed bythe primary healthcare professionals (HCPs) in the U.S., demon-strated that more than 80% of the HCPs stated intranasal corticos-teroids as the gold standard for the treatment of AR. In this samestudy, HCPs also feedback that around 63% to 77% of patients canmanage the disease after the treatment establishment, and around70% of HCPs further agreed that over-the-counter (OTC) medicineshould be tried before prescribed medicine for AR management[16]. It is a consensus that intranasal steroids are more effectivethan antihistamines. However, it is not suggested that intranasalsteroids are the most cost-effective treatment options. Cost-effec-tiveness is especially relevant in ASEAN countries without amplepublic healthcare support such as the Philippines. The cost-effec-tiveness of antihistamines is a key contributing factor to primarycare favoring the recommendations of antihistamines. Currentresearch development has also demonstrated that second-genera-tion antihistamines do have anti-inflammatory effects alongsidetheir anti-histaminic effects, by decreasing the release of keycytokines and the migration of inflammatory cells [17].Noteworthy, the survey results showed that there are still some pri-mary care practitioners who would recommend 1st generation anti-histamines to AR patients. This may also be attributed to costeffectiveness, with 1st generation typically priced cheaper than 2nd
generation antihistamines. More education is required at a primarycare level to increase awareness of potential side effects associatedwith 1st generation antihistamines.
The survey further revealed that non-drug treatment optionssuch as saline douching and allergen avoidance are also preferredtreatment options in both GP clinics and pharmacies. These non-drug treatment options are recommended in the ARIA guidelinesas adjuncts to supplement the main treatments. However, thesenon-drug options have low evidence and should not replace stan-dard treatments. The best treatment regimen is to employ multiplecontrol measures comprising of allergen avoidance, mainstreamtreatments, and non-drug adjunct therapies.
The length and efficacy of treatment are viewed as essential byprimary care for the long-term control of AR. Preference for theoral route of administration may also be due to the faster onset ofaction of oral 2nd generation antihistamines (1-2 hours) comparedwith intranasal steroids (6 hours). Running out and dripping downof intranasal treatment resulting in patient discomfort is also a keyconsideration for patients. In addition, more pharmacists than GPsthink that patients’ phobia of steroids (72.6% pharmacists vs 62.5% GPs; p<0.001) is the other key factor influencing patient com-pliance. This may correlate with the high prescription/usage ofantihistamines in primary care. Adverse events from corticos-teroids treatment are real and can be life-threatening if not man-aged well. Although intranasal steroids today are generally tolera-
ble in safety profiles, especially the new generation molecules, theevidence is still based off on safety studies of a trial period lessthan one year. There is currently no evidence demonstrating safetyif patients were to use intranasal steroids longer than one year. Thiswas also pointed out by the expert consensus statement inMalaysia, where it was noted that current guidelines are still vaguein recommending the length of treatment of steroids in AR patients[9]. More clinical evidence is required to provide stronger guid-ance to primary care.
In this survey, 80.8 % of GPs were aware of the ARIA guide-lines, while only 48.4% of pharmacists were aware. This correlatedwith 81.7% of GPs and only 48.2% of pharmacists who know howto identify AR patients. Out of those who are aware of ARIA,90.7% of GPs and 83.4% of pharmacists agreed that the ARIAguidelines are useful in the diagnosis of AR patients. Whilst theauthors acknowledged the distinct roles of GPs and pharmacists inAR management (diagnosis versus dispensing respectively), itshould be noted some patients visiting the pharmacy would havehad AR previously diagnosed by physicians, some self-diagnosedand some without any diagnosis or inaccurate diagnosis (e.g., aviral infection or cold). Hence, pharmacists must be in good steadto identify the symptoms of AR and to recommend appropriatetreatment [1]. The strong agreement from both GPs and pharma-cists on the relevance of the ARIA guidelines validates the ongoingefforts to increase awareness and usage of ARIA. Several reasonsmay account for the pharmacist respondents having low awarenessof the ARIA guidelines. Pharmacists are not exposed to the guide-lines in their pharmacy curriculum, and dissemination of ARIA ismostly targeted to GPs as the emphasis is on diagnosis, an arearestricted to medical doctors in most ASEAN countries. ARIA alsohas language barriers in some ASEAN countries. It will be mostoptimal to have either a translated version of ARIA or a nationalguideline (or ASEAN guideline), which is in line with ARIA.There is also an opportunity to leverage technology. Currently, anEU backed initiative termed as “Next Generation ARIA care path-ways” is using digital technology to enable a patient-centeredapproach in allergy care in order to bridge the existing gap [18].Western countries such as the U.S., UK, France, and Japan havebrought ARIA into mobile applications such as MACVIA [19].Care of AR patients are most optimal when we have a healthyecosystem comprising of various healthcare professionals such aspharmacists, GPs, allergists, ENTs, nutritionists/dietitians even.Overall, ARIA has already adapted itself to meet the real world andto guide primary care practitioners. VAS score is introduced andreplaced ‘mild’ and ‘moderate to severe’ for severity assessment.The stepwise approach has been developed with the aim that ARIAwill be more practical [1].
There are several limitations to this study. Despite a large totalsample size of 887, this survey was an aggregate of 4 ASEANcountries, with an average of 82 GPs and 127 pharmacists percountry. This may be regarded as a rather small sample size percountry, and thus, the findings cannot be used to over-generalizeeach country. The survey results should be interpreted at anASEAN level. Lastly, because the responses of the respondentswere based on their own experience and perceptions, not on theobjective assessment from the patient cohort or registry, the resultsof this study might be different from the real-world assessments.
In conclusion, our survey results have identified a need tostrengthen the awareness and use of ARIA guidelines among pri-mary care practitioners in the 4 ASEAN countries. Adherence toARIA guidelines, choosing the appropriate treatment option andprioritizing factors that increase patient compliance may con-tribute to better management outcomes of AR at the primary carepractice.
MRM_01 original.qxp_Hrev_master 07/12/20 21:10 Pagina 160

48MRM
Multidisciplinary Respiratory Medicine 2020; 15:726 - B. Abdullah et al.
AcknowledgementsThe authors acknowledge Turacoz Healthcare Solutions
(https://www.turacoz.com/) for the medical writing assistance.
References1. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ,
Togias A, et al. Allergic Rhinitis and its Impact on Asthma(ARIA) 2008 update (in collaboration with the World HealthOrganization, GA(2)LEN and AllerGen). Allergy 2008;63:S8-160.
2. Tong MCF, Lin JSC. Epidemiology of allergic rhinitis through-out the world. In: Akdis CA, Hellings PW, Agache I, editors.EAACI Global atlas of allergic rhinitis and chronic rhinosi-nusitis. Zurich: European Academy of Allergy and ClinicalImmunology; 2015. p. 62-3.
3. Katelaris CH, Lai CK, Rhee CS, Lee SH, Yun WD, Lim-Varona L, et al. Nasal allergies in the Asian-Pacific population:results from the allergies in Asia-Pacific survey. Am J RhinolAllergy 2011;25:S3-15.
4. Wang DY, Chan A, Smith JD. Management of allergic rhinitis:a common part of practice in primary care clinics. Allergy2004;59:315-9.
5. Brozek JL, Bousquet J, Agache I, Agarwal A, Bachert C,Bosnic-Anticevich S, et al. Allergic Rhinitis and its Impact onAsthma (ARIA) guidelines-2016 revision. J Allergy ClinImmunol 2017;140:950-8.
6. Bousquet J, Lund VJ, van Cauwenberge P, Bremard-Oury C,Mounedji N, Stevens MT, et al. Implementation of guidelinesfor seasonal allergic rhinitis: a randomized controlled trial.Allergy 2003;58:733-41.
7. Canonica GW, Triggiani M, Senna G. 360 degree perspectiveon allergic rhinitis management in Italy: a survey of GPs, phar-macists and patients. Clin Mol Allergy 2015;13:25.
8. Prepageran N, Wang de Y, Nair G, Maurer M. The status quoand unmet needs in the management of allergic rhinitis andchronic rhinosinusitis: a Malaysian perspective. Asia PacAllergy 2014;4:142-8.
9. Baharudin A, Abdul Latiff AH, Woo K, Yap FB, Tang IP,Leong KF, et al. Using patient profiles to guide the choice of
antihistamines in the primary care setting in Malaysia: Expertconsensus and recommendations. Ther Clin Risk Manag2019;15:1267-75.
10. Abdullah B, Kandiah R, Husna Nik Hassan NF, Ismail AF,Mohammad ZW, Wang DY. Assessment of perception, atti-tude, and practice of primary care practitioners towards aller-gic rhinitis practice guidelines: Development and validation ofa new questionnaire. World Allergy Organization J 2020;13:100482.
11. Navarro-Locsin CG, Romualdez JA. Attitudes, practices onallergic rhinitis of generalists and specialists in PhilippineNational Capital Region. Asia Pac Allergy 2015;5:203-9.
12. Tahamiler R, Canakcioglu S, Ogreden S, Acioglu E. The accu-racy of symptom-based definition of chronic rhinosinusitis.Allergy 2007;62:1029-32.
13. Ferguson BJ, Narita M, Yu VL, Wagener MM, Gwaltney JM,Jr. Prospective observational study of chronic rhinosinusitis:environmental triggers and antibiotic implications. Clin InfectDi. 2012;54:62-8.
14. Tomassen P, Newson RB, Hoffmans R, Lotvall J, Cardell LO,Gunnbjornsdottir M, et al. Reliability of EP3OS symptom cri-teria and nasal endoscopy in the assessment of chronic rhinos-inusitis--a GA(2) LEN study. Allergy 2011;66:556-61.
15. Castor MAR, Recto MT, Sumpaico MW. Correlation of skinprick test with symptoms and physical examinations finding inallergic rhinitis among Filipino Children. Phil J AllergyAsthma Immunol 2016;19:19-28.
16. Blaiss MS, Fromer LM, Jacob-Nara JA, Long RM, MannionKM, Lauersen LA. Current Allergic Rhinitis ExperiencesSurvey (CARES): Health-care practitioners' awareness, atti-tudes and practices. Allergy Asthma Proc 2014;35:316-22.
17. Marshall GD, Jr. Therapeutic options in allergic disease: anti-histamines as systemic antiallergic agents. J Allergy ClinImmunol 2000;106:S303-9.
18. Bousquet J, Pham-Thi N, Bedbrook A, Agache I, Annesi-Maesano I, Ansotegui I, et al. Next-generation care pathwaysfor allergic rhinitis and asthma multimorbidity: a model formultimorbid non-communicable diseases - Meeting Report(Part 1). J Thorac Dis 2019;11:3633-42.
19. Bousquet J, Schunemann HJ, Fonseca J, Samolinski B,Bachert C, Canonica GW, et al. MACVIA-ARIA SentinelNetworK for allergic rhinitis (MASK-rhinitis): the new gener-ation guideline implementation. Allergy 2015;70:1372-92.
Received for publication: 7 October 2020. Accepted for publication: 19 November 2020.This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0).©Copyright: the Author(s), 2020Licensee PAGEPress, ItalyMultidisciplinary Respiratory Medicine 2020; 15:726doi:10.4081/mrm.2020.726
MRM_01 original.qxp_Hrev_master 07/12/20 21:10 Pagina 161

49MRM
Value of modified Burns Wean Assessment Program scores in the respiratory intensive care unit: an Egyptian studyNermeen A. Abdelaleem,1 Sherif A.A. Mohamed,1 Azza S. Abd ElHafeez,2 Hassan A. Bayoumi1
1Department of Chest Diseases and Tuberculosis2Department of Medical Physiology, Faculty of Medicine, Assiut University, Assiut, Egypt
Background: There is no consensus on the most useful predictive indicator for weaning patients from mechanical ven-tilation (MV). We aimed to evaluate the utility of the modified Burns Wean Assessment Program (m-BWAP) in pre-dicting the weaning success in patients with respiratory disorders admitted to the respiratory intensive care unit(RICU).Methods: Patients with respiratory failure requiring MV for longer than 48 hours were included. They were weanedby pressure support ventilation and spontaneous breathing trails. Patients were divided into successful and unsuccess-ful weaning groups according to their outcomes. Results: A total of 91 patients were enrolled. The majority had chronic obstructive pulmonary diseases (COPD): 40%,overlap syndrome (24%), and obesity hypoventilation syndrome (OHS): 15%. The successful group had significantlyhigher m-BWAP scores than that in the unsuccessful group (median 65; range 35 to 80 vs. median 45; range 30 to 65;p=0.000), with area under the curve (AUC) of 0.854; 95% CI 0.766 to 0.919), p<0.001. At cut-off value of ≥55, thesensitivity and specificity of m-BWAP to predict successful weaning were 73.77% and 84.85%, respectively. The AUCfor m-BWAP was significantly higher than that for rapid shallow breathing index (RSBI).Conclusion: We conclude that m-BWAP scores represent a good predictor of weaning success among patients withchronic respiratory disorders in the RICU. The m-BWAP checklist has many factors that are closely related to the weaningoutcomes of patients with chronic respiratory disorders. Further, large-scale, multicenter studies are warranted.
Key words: Modified Burns Wean Assessment Program scores; respiratory; ICU; Egypt; weaning.
AB
STR
ACT
Correspondence: Dr. Sherif A.A. Mohamed, Department of Chest Diseases and Tuberculosis, Faculty of Medicine, AssiutUniversity, 71516 Assiut, Egypt. Tel. +20.882413713. Fax: +20.88241333327. E-mail: [email protected]
Contributions: NAA, SAAM, HAB, contributed to the draft of the submitted article, revised it critically for important content,and made substantial contributions to conception and design, as well as data acquisition, analysis, and interpretation; SAAM,NAA, ASA, contributed to the draft of the submitted article and made substantial contributions to acquisition, analysis, andinterpretation of clinical and physiological data. All authors have provided approval of the manuscript to be published and haveagreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any partof the work are appropriately investigated and resolved.
Conflict of interest: The authors have no competing interests.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Availability of data and materials: The datasets used and/or analyzed during the current study are available from the correspon-ding author on reasonable request.
Ethics approval and consent to participate: The study was approved by the Ethical Committee of the Faculty of Medicine,Assiut University, Egypt.
Consent for publication: Not applicable.
ORIGINAL RESEARCH ARTICLE
Multidisciplinary Respiratory Medicine 2020; volume 15:691
MRM_01 original.qxp_Hrev_master 04/08/20 11:20 Pagina 96

50MRM
Multidisciplinary Respiratory Medicine 2020; 15:691 - N.A. Abdelaleem et al.
IntroductionMechanical ventilation (MV) is an integral part of manage-
ment for patients with respiratory failure, due to different respira-tory disorders, in the intensive care unit (ICU) [1,2]. Weaning cov-ers the entire process of liberating the patient from mechanicalsupport as well as from endotracheal tube, which can take morethan 56% - 90% of the time of MV [3]. Determining the patient’sreadiness for the process of weaning from MV is of crucial impor-tance. However, it is not an easy task to wean a patient with respi-ratory failure due to respiratory disorder from the MV. BecauseMV itself is associated with many complications, as well as wean-ing patients improperly from MV can lead to respiratory failureand re-intubation, the decision of weaning still represents a chal-lenge to the respiratory physician [2,4].
Early weaning and unsuccessful extubation can lead to trachealreintubation, which potentially leads to airway trauma, aspiration,acute lung injury, and increases the risk of nosocomial pneumoniaand the mortality rates [5]. On the other hand, late weaning expos-es the patients to pneumonia, ventilator-induced lung injury (VILI)and higher mortality [6].
Despite the fact that many weaning parameters and predictorshave been reported in the literature, there is no consensus on themost useful predictive indicators [7-9], particularly in patients withrespiratory disorders [4,10].
A comprehensive clinical weaning checklist and scoringinstrument, the Burns Wean Assessment Program (BWAP) scorewas designed to assist the clinicians in the management of patientswho require prolonged MV [11]. Moreover, a modified version ofthe BWAP score (m-BWAP) has been developed, which makes thescoring more convenient, and proved effective as a good indicatorof weaning and extubation outcome in patients with long-termmechanical ventilation (LTMV) [12]. However, no study had eval-uated this score in patients with respiratory failure due to respira-tory disorder. Therefore, this study aimed to evaluate the modifiedBurns Wean Assessment Program (m-BWAP) score in predictingweaning success in mechanically ventilated respiratory patientsdue to respiratory failure for more than 48 h.
Materials and Methods
Study design and subjects Assiut University Hospital (AUH) is a large tertiary hospital in
Upper Egypt, to which many patients with respiratory disorders arereferred. This prospective, observational study was conducted in a24-bed respiratory ICU at AUH, from the period of January 2019to July 2019.
Inclusion criteria were; adult subjects with the diagnosis of res-piratory failure due to a respiratory disorder who are mechanicallyventilated for ≥48 h with the absence of uncontrolled respiratoryinfection, and in a clinical and neurological stable state. Subjectsaged younger than 18 years, those with irreversible brain injury,acute or chronic neuromuscular diseases, LTMV prior to ICUadmission, and those who received tracheostomy before the firstspontaneous breathing trial (SBT) were excluded. A ventilatorweaning protocol, based on doc umented guidelines, has beendeveloped [1,4], and successfully implemented in our respiratoryICU (Figure 1).
All patients were monitored with ECG, blood pressure andpulse oximetry. Patients were assigned for a spontaneous breathingtrial (SBT) for 30 min when they met the following criteria:PaO2/FiO2 >150, PEEP ≤8 mmHg, stable neurological state, meanblood pressure ≥60 mmHg and adequate cough. All patients were
weaned by low level of pressure support (5-8 cmH2O) and FiO2levels decreased gradually until ≤40%. Patients showed good tol-erance for the trial: acceptable arterial blood gas (pH ≥7.35,PaO2/FiO2 >150 with a FiO2 ≤40%, respiratory rate ≤35breaths/min), they were extubated and followed for 48 h. Weaningsuccess means the ability to maintain spontaneous ventilationwithout the need for reintubation and invasive mechanical ventila-tion for 48 h after extubation. If signs of intolerance happened(altered mental state, respiratory rate >35 breaths/min, pH <7.32,increase in PaCO2 >10 mmHg, heart rate >140 beats/min, systolicblood pressure >180 or <90 mmHg) turn the ventilator to full sup-port. The study was approved by the Ethical Committee of theFaculty of Medicine, Assiut University.
Data collection and definitions Demographic and clinical data were collected for each subject;
age, gender, body mass index (BMI), and ICU admission diagno-sis. The latter was determined according to the well-known inter-national guidelines and agreements. Chronic obstructive pul-monary disease (COPD) was defined as per the Global Initiativefor Chronic Obstructive Lung Disease (GOLD) guidelines [13].The overlap syndrome was defined as the combination of COPDand sleep apnea-hypopnea syndrome (SAHS) [14]. Obesityhypoventilation syndrome (OHS) was defined by the combinationof obesity (BMI ≥30 kg·m−2), sleep disordered breathing and day-
Figure 1. Weaning protocol at the RICU.
MRM_01 original.qxp_Hrev_master 04/08/20 11:20 Pagina 97

51MRM
Multidisciplinary Respiratory Medicine 2020; 15:691 - N.A. Abdelaleem et al.
time hypercapnia (arterial carbon dioxide tension (PaCO2) ≥45mmHg at sea level) during wakefulness occurring in the absence ofan alternative neuromuscular, mechanical or metabolic explanationfor hypoventilation [15].
The severity of illness within 24 h of ICU admis sion was mea-sured using the Acute Physiology and Chronic Health Evaluation(APACHE) II score [16]; ICU and hospital length of stay, durationof MV, and hospital mortality were also recorded.
The m-BWAP checklists, as previously reported [12], wereused in this study. Enrolled subjects were grouped according to thesuccess of the first spontaneous breathing trial (SBT), into success-ful and unsuccessful liberation from MV groups, respectively. Wealso evaluated traditional weaning parameters [rapid shallowbreathing index (RSBI), maximal inspiratory pressure (Pimax)] atfirst SBT to compare predicting successful liberation at first SBTwith m-BWAP score. The primary outcome was successful libera-tion from MV at first SBT, and successful liberation was definedas complete weaning from MV lasting more than 48 h.
Statistical analysis Continuous variables were expressed as median (range),
whereas categorical variables are presented as number (%). TheStudent t-test or the Mann-Whitney U-test were used for compar-isons of continuous variables. The Chi-square or Fisher exact test(for small numbers) was used to compare categorical variables. Toestimate the performance of the m-BWAP score in terms of pre-dicting successful weaning from MV, receiver operating character-istic curves were constructed and the area under the curve (AUC)was determined; identification of an optimal cut-off value for thisscore was based on the maximum Youden’s index [17]. All tests ofsignificance were two-tailed, and p-values of <0.05 were consid-ered to be statistically significant.
ResultsOut of the 125 patients included, 21 (16.8%) died before start-
ing the first weaning trials. Moreover, nine patients (7.2%) wereself-extubated or had unplanned weaning (Figure 2). The remaining95 patients (76%) were divided into two groups; i) successful wean-ing group, 62 (65.3%) patients, and ii) unsuccessful weaning group,33 (34.7%) patients. The majority of patients (66/95, 69.5%) weremales. At ICU admission, the majority (38/95, 40%) of patients hadthe diagnosis of COPD, followed by those with overlap syndrome(23/95, 24%), and those with OHS (14/95, 15%).
Patients in the unsuccessful group were older (60.16 ±13.13 vs57.98 ±13.39; p=0.427) with higher APACHE II score than thesuccessful one (23.43±4.49 vs 20.04 ±4.56; p=0.428). The distri-bution of respiratory disorders within successful and unsuccessfulgroups revealed significant differences. Patients with asthma, over-lap syndrome and pneumonia/ARDS were significantly higheramong the successful weaning group than in the unsuccessfulgroup (p=0.008, p=0.000, and p=0.031), respectively). Whilepatients with COPD and bronchiectasis were significantly higheramong the unsuccessful weaning group than in the successfulgroup (p=0.000, and p=0.031, respectively). Mortality rate wassignificantly higher in unsuccessful group (30.3% vs 12.9%;p=0.000). There were significant differences between the 2 groupswith regards to partial pressure of oxygen (PaO2), mechanical andventilatory parameters (airway resistance, minute ventilation, max-imal inspiratory pressure, lung compliance, and rapid shallowbreathing index), as well as modified Burns Wean AssessmentProgram (m-BWAP). The successful group had significantly high-er m-BWAP scores than that in the unsuccessful group (median 65;range 35 to 80 vs median 45; range 30 to 65; p=0.000), respective-
ly. Table 1 details the differences between successful and unsuc-cessful weaning groups.
By analyses according to all m-BWAP scoring checklist ele-ments [12], the successful group had a significantly higher rate innine factors of all checklist elements when compared with theunsuccessful group (i.e., stable heart rhythm, general body strengthand condition, ability to clear airway, amount and consistency ofsecretion, good lung compliance, low airway resistance (Raw), lowPimax, low RSBI, and appropriate minute ventilation) (Table 2)
The m-BWAP score was higher in patients with successfulweaning using a cut-off value of ≥55. At this cut-off value, the sen-sitivity and specificity of the m-BWAP to predict successful wean-ing were 73.77% and 84.85%, respectively (AUC 0.854; 95% CI0.766 to 0.919), p<0.001 (Figure 3).
Figure 2. Flow chart of the studied patients.
Figure 3. Receiver operating characteristic curves for modifiedBurns Wean Assessment Program (m-BWAP) score and rapidshallow breathing index (RSBI) for predicting successful weaningfrom mechanical ventilation in RICU patients. The areas underthe curve (AUCs) for m-BWAP and RSBI were 0.854 (95% CI:0.766 to 0.919), p<0.001, and 0.740 (95% CI: 0.637 to 0.823),p<0.001, respectively.
MRM_01 original.qxp_Hrev_master 04/08/20 11:20 Pagina 98

52MRM
Multidisciplinary Respiratory Medicine 2020; 15:691 - N.A. Abdelaleem et al.
Table 1. Clinico-physiological features of patients with successful and unsuccessful weaning from mechanical ventilation.
Successful group (n=62) Unsuccessful group (n=33) p
Age (median ± SD, years) 57.98 ±13.39 60.16 ±13.13 0.427Gender (n, %) Female 17 (27.4%) 12 (36.4%) 0.251 Male 45 (72.6%) 21 (63.6%) Severity of illness at ICU admission APACHE II score 20.04 ±4.56 23.43±4.49 0.488 Time between ICU admission and weaning (days)* 2.67±1.30 3.78±1.82 0.002Underlying respiratory disorder (n,%) Asthma 5 (8.1%) 0 (0%) 0.008 COPD 22 (35.5 %) 16 (48.5%) 0.000 Bronchiectasis 3 (4.8%) 3 (11.0%) 0.031 Overlap syndrome 18 (29.0%) 5 (15.2%) 0.000 OHS 8 (12.9%) 6 (18.2%) 0.063 Pneumonia/ ARDS 4 (6.5%) 0 (0%) 0.031 Others° 2 (3.2%) 3 (11.0%) 0.008Laboratory and functional parameters Hemoglobin 13.16±2.25 12.32±2.58 0.095 Albumin 28.65±5.04 26.11±4.78 0.014 pH 7.45±0.04 7.44±0.06 0.255 PaCO2 54.08±10.62 56.22±12.51 0.369 PaO2 74.86±13.98 67.40±12.93 0.008 Raw 8.68±3.09 15.91±3.47 0.000 Pimax 21.19±5.53 13.97±4.43 0.000 MV 7.02±2.45 11.75±2.57 0.000 RR 23.26±5.35 35.82±3.20 0.000 LC 42.21±10.73 28.22±7.61 0.000 RSBI 78.59±26.886 121.33±18.45 0.000 m-BWAP 65 (35-80) 45 (30-65) 0.000Length of stay in the ICU# 6.51±4.58 12.89±8.64 0.000Hospital mortality 8 (12.9%) 10 (30.3%) 0.000
APACHE II, Acute Physiology and Chronic Health Evaluation II score; WBC, White blood cells; ALB, serum albumin; PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon dioxide; MV, minuteventilation; Hg, hemoglobin; PLT, platelets; Na, sodium; K, potassium; Raw, airway resistance; Pimax, maximal inspiratory pressure; RR, respiratory rate; LC, lung compliance; COPD, chronic obstructivepulmonary disease; OHS, obesity hypoventilation syndrome; ARDS, acute respiratory distress syndrome; *duration before weaning was defined as the time from intubation until first spontaneous breath-ing trial; ° Others; 2 post-pulmonary TB sequelae; 2 interstitial lung disease; and one pulmonary embolism; #length of stay in ICU was defined as the time from intubation until ICU discharge. Data pre-sented as mean ± SD; median (range); number (%).
Table 2. Comparison of m-BWAP scoring tools between patients with successful and unsuccessful groups.
Item Successful group (n=62) Unsuccessful group (n=33) p
Age <65 years 37 (59.7%) 23 (69.7%) 0.343Without heart failure 56 (90.3%) 27 (81.8%) 0.235Stable heart rhythm 53 (85.5%) 18 (54.5%) 0.001Stable blood pressure 56 (90.3%) 26 (78.8%) 0.058Free from factors that will increase or decrease metabolic rate 52 (83.9%) 24 (72.7%) 0.196Stable arterial blood gases pH 41 (66.1%) 18 (54.5%) 0.066Stable PaO2 and PaCO2 33(53.2%) 17 (51.1%) 0.874Good consciousness 0 (0%) 0 (0%) -Stable sodium, potassium, calcium, and phosphate concentration 46 (74.2%) 21(63.6%) 0.053Stable fluid status 0 (0%) 0 (0%) -Good nutritional status 23 (37.1%) 12(36.4%) 0.944General body strength and condition 20 (32.3%) 4 (12.1%) 0.032Ability to clear airway 26 (41.9%) 2 (6.1%) 0.000Amount and consistency of secretion 54 (87.1%) 17 (51.1%) 0.000Good lung compliance 58 (93.5%) 21 (63.6%) 0.000Low Raw 58 (93.5%) 13 (39.4%) 0.000Low Pimax 46 (74.2%) 11 (33.3%) 0.000Low RSBI 54 (87.1%) 19 (57.6%) 0.000Appropriate minute ventilation 55 (88.7%) 11 (33.3%) 0.000
This table shows the comparison between patients with successful and unsuccessful liberation of ventilator care at the time of first SBT in total patients regardless of whether they had 5 points or notaccording to the definition of each category. m-BWAP, modified Burns Wean Assessment Program; PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon dioxide; Raw, airway resistance;Pimax, maximal inspiratory pressure; RSBI, rapid shallow breathing index. Values are presented as number (%).
MRM_01 original.qxp_Hrev_master 04/08/20 11:20 Pagina 99

53MRM
Multidisciplinary Respiratory Medicine 2020; 15:691 - N.A. Abdelaleem et al.
Upon comparing the m-BWAP score with other weaningparameters (RSBI), at a cut-off value of ≥83 for RSBI, the AUCwas 0.740 (95% CI: 0.637 to 0.823), p <0.001. The sensitivity andspecificity of RSBI to predict successful weaning were 51.61%and 93.94%, respectively. The AUC for m-BWAP was significant-ly higher than that for RSBI (Figure 3).
DiscussionTo the best of our knowledge, this is the first study that evalu-
ates the m-BWAP score in weaning from mechanical ventilation ofa well-characterized group of adult patients with different respira-tory disorders admitted to RICU. We had observed that the m-BWAP score could be successfully applied to Egyptian adultpatients with different respiratory disorders. The m-BWAP scorewas higher in patients with successful weaning using a cut-offvalue of 55, with sensitivity and specificity of 73.77% and 84.85%,respectively. Moreover, upon comparing the m-BWAP score withother weaning parameters (RSBI), m-BWAP proved to be moreeffective tool for predicting weaning from mechanical ventilationin patients with chronic respiratory disorders.
Our demographic data showed that days of mechanical venti-lation before weaning, and length of ICU stays affected weaningsuccess. This was in accordance with the findings of Wu, et al [18].Also, in agreement with Shin et al. [19], we had reported thatAPACHE II score was significantly lower in the successful wean-ing group.
In patients with chronic respiratory disorders, systematic track-ing of factors associated with successful weaning remains impor-tant for care planning and to determine the weaning potential. Thisis of particular importance because almost all chronic respiratorydisorders affect -in a way or another- the lung mechanics and/orthe ventilatory control [20], so the preparation for weaning apatient with chronic respiratory disorder is of crucial importanceand represents a challenging task for the pulmonologist and/or theintensivist. This task will be harder in patients with combined res-piratory disorders (e.g., overlap syndrome, obesity hypoventilationsyndrome) [9,20,21]. Our study included considerable numbers ofpatients with different respiratory disorders. Moreover, patientswith asthma, overlap syndrome and pneumonia/ARDS were sig-nificantly higher among the successful weaning group than thosein the unsuccessful group. On the contrary, patients with COPDand bronchiectasis were significantly higher among the unsuccess-ful weaning group than those in the successful one.
Patients with COPD are well known to have pathophysiologicabnormalities like airway obstruction, dynamic hyperinflation,diaphragmatic muscle abnormalities, ventilation-perfusion mis-match [13]. The overlap syndrome can contribute to worsenedsymptoms and oxygen desaturation at night. Alveolar hypoventila-tion, ventilation-perfusion mismatch and intermittent hypercapnicevents resulting from apneas and hypopneas contribute to the finalclinical picture of overlap syndrome, which is quite different fromthe “usual” COPD [22]. On the other hand, the pathophysiology ofOHS results from complex interactions, among which are respira-tory mechanics, ventilatory control, sleep-disordered breathing andneurohormonal disturbances, such as leptin resistance, each ofwhich contributes to varying degrees in individual patients to thedevelopment of obesity hypoventilation [22,22]. Spontaneousbreathing assessment was a routine practice carried out for allmechanically ventilated patients [23]. Different techniques wereused to decide if a patient was able to breathe independently. If
patients needed more time on the ventilator, the initial requirementfor ventilator support was rarely the only reason for continueddependence on a ventilator. Rather, it was mostly the effect of othercomplications or comorbidities that emerge over time. Thus, acomprehensive assessment of these patients was necessarily need-ed [24]. The original checklist of Burns wean assessment program(BWAP) was developed as tool to measure patient’s readiness forweaning from the ventilator. This tool evaluates parameters ofpatients’ weaning from the ventilator systematically and examinesall parameters related to pulmonary function, gas changes, physio-logical and psychological conditions of patients [9,11]. It is aneasy-to-use checklist, and its parameters could be measured within10 minutes [25]. The modified version of BWAP was developed byJiang et al. [12] who proved that this tool was a good predictor ofsuccessful weaning and extubation in patients requiring LTMV forlonger than 21 days. Their results also suggested that a m-BWAPscore ≥60 is associated with successful extubation outcomes.Jeong and coworkers [4] prospectively enrolled 103 patients in amedical ICU and concluded that m-BWAP score was a good pre-dictor of weaning success in patients with an endotracheal tube inplace at first SBT. The current study confirms the findings of Janget al. [12] and Jeong et al. [4], and observed that m-BWAP scoreincreased the likelihood of successful weaning among patientswith different respiratory disorders in the RICU. Moreover, m-BWAP score was superior to another traditional weaning index(RSBI). Blackwood et al. [26] reported that daily assessment forcriteria of readiness to wean based on weaning protocols coulddecrease the duration of mechanical ventilation and length of hos-pital stay, reduce costs and reduce rates of weaning failure. Thus,our findings could have important clinical and financial impacts,particularly in the setting of developing countries, like Egypt.
In the current study, the successful group showed a significantdifference in nine factors of the m-BWAP checklist elements whencompared with the unsuccessful group. These factors were; stableheart rhythm, general body strength and condition, ability to clearairway, amount and consistency of secretion, good lung compli-ance, low Raw, low Pimax, low RSBI, and appropriate minute ven-tilation.
In their analysis, Jeong and coworkers [4] found different fivefactors to be significantly different between the successful andunsuccessful groups of weaning. Our results suggest that it is likelythat there are more effective factors among the m-BWAP scoringchecklist elements among patients with chronic respiratory disor-ders that can predict successful weaning liberation from MV.Furthermore, we think that one of the major advantages of m-BWAP is that parts of the m-BWAP are better suited for predictingweaning success (mechanics, gas exchange and image studies)while other parts are better for predicting the ability to protect theairway and thus ensure safe extubation (cough ability, secretioncontent and consciousness). Further multicenter studies with largernumbers of patients with different chronic respiratory disorders areessentially needed.
The current study has several strength points. First, it is thefirst study that addresses the utility of m-BWAB in “pure” patientswith chronic respiratory disorders and admitted in a “respiratoryICU”. The pathophysiology of these respiratory disorders is ulti-mately related to the lung mechanics and the process of weaningfrom MV. Second, it is a prospective study. Third, our results high-lighted the importance of using m-BWAB with the use of moreeffective factors among its checklist that are more likely to predict,and closely related to the successful weaning among patients withchronic respiratory disorders. Inevitably, our study has some limi-tations. The study sample size was relatively small and the studywas performed at a single centre.
MRM_01 original.qxp_Hrev_master 04/08/20 11:20 Pagina 100

54MRM
Multidisciplinary Respiratory Medicine 2020; 15:691 - N.A. Abdelaleem et al.
ConclusionsWe concluded that m-BWAP scores represent a good predictor
of weaning success among patient with chronic respiratory disor-ders in the respiratory intensive care unit. The m-BWAP checklisthas many factors that are closely related to the weaning outcomesof patients with chronic respiratory disorders. Additional, large-scale, multicenter studies are needed to further evaluate the clinicalutility of m-BWAP scores in patients with chronic respiratory dis-orders.
AcknowledgmentsThe authors thank the nursing and technician teams of the
Department of Chest Diseases and Tuberculosis, Assiut UniversityHospital, for their kind support to this work.
AbbreviationsAPACHE II: Acute Physiology and Chronic Health Evaluation;ARDS: acute respiratory distress syndrome; AUC: area under the curve; BMI: body mass index; CI: confidence interval; COPD: chronic obstructive pulmonary diseases; FiO2: fracture of inspired oxygen; LC: lung compliance; LTMV: long-term mechanical ventilation; OHS: obesity hypoventilation syndrome; OS: overlap syndrome; m-BWAP: modified Burns Wean Assessment Program; MV: mechanical ventilation; PaCO2: partial pressure of carbon dioxide; PaO2: partial pressure of oxygen; PEEP: positive end expiratory pressure; Pimax: maximal inspiratory pressure; Raw: airway resistance; RICU: respiratory intensive care unit; RR: respiratory rate;RSBI: rapid shallow breathing index; SBT: spontaneous breathing trial; VILI: ventilator-induced lung injury; WBC: white blood cells.
References1. Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C,
et al. Weaning from mechanical ventilation. Eur Respir J2007;29:1033-56.
2. Hussein K, Mohamed S, Ahmed Y. Airway pressure releaseventilation in management of acute respiratory distress syn-drome: a 2-years experience from upper Egypt. Int J Sci Res2015;4:265-8.
3. Keykha A, Dahmardeh AR, Khoshfetrat M. Comparison ofsuccess rate of weaning from mechanical ventilation usingBurn’s Wean Assessment Program and routine method. CritCare Nurs J 2017;10:e12557.
4. Jeong ES, Lee K. Clinical application of modified burns weanassessment program scores at first spontaneous breathing trial
in weaning patients from mechanical ventilation. Acute CritCare 2018;33:260-8.
5. Ely EW, Meade MO, Haponik EF, Kollef MH, Cook DJ,Guyatt GH, et al. Mechanical ventilator weaning protocolsdriven by nonphysician health-care professionals: evidence-based clinical practice guidelines. Chest 2001;120:454S–63S.
6. Esen S, Leblebicioglu H. Prevalence of nosocomial infectionsat intensive care units in Turkey: a multicentre 1-day pointprevalence study. Scand J Infect Dis 2004;36:144-8.
7. Macintyre NR. Evidence-based assessments in the ventilatordiscontinuation process. Respir Care 2012;57:1611-8.
8. McConville JF, Kress JP. Weaning patients from the ventilator.N Engl J Med 2012;367:2233-9.
9. Baptistella AR, Sarmento FJ, da Silva KR, Ferla Baptistella S,Taglietti M, Zuquello RA, et al. Predictive factors of weaningfrom mechanical ventilation and extubation outcome: A sys-tematic review. J Crit Care 2018;48:56-62.
10. Vassilakopoulos T, Zakynthinos S, Roussos Ch. Respiratorymuscles and weaning failure. Eur Respir J 1996;9:2383-400.
11. Burns SM, Marshall M, Burns JE, Ryan B, Wilmoth D,Carpenter R, et al. Design, testing, and results of an outcomes-managed approach to patients requiring prolonged mechanicalventilation. Am J Crit Care 1998;7:45-57.
12. Jiang JR, Yen SY, Chien JY, Liu HC, Wu YL, Chen CH.Predicting weaning and extubation outcomes in long-termmechanically ventilated patients using the modified BurnsWean Assessment Program scores. Respirology 2014;19:576-82.
13. Global Initiative for Chronic Obstructive Lung Disease[Internet]. Global Strategy for the diagnosis, management andprevention of COPD 2017. Available from: https://goldcopd.org/
14. Flenley DC. Sleep in chronic obstructive lung disease. ClinChest Med 1985;6:51-61.
15. Mokhlesi B, Kryger MH, Grunstein RR. Assessment and man-agement of patients with obesity hypoventilation syndrome.Proc Am Thorac Soc 2008;5:218-25.
16. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHEII: a severity of disease classification system. Crit Care Med1985;13:818-29.
17. Perkins NJ, Schisterman EF. The inconsistency of “optimal”cutpoints obtained using two criteria based on the receiveroperating characteristic curve. Am J Epidemiol 2006;163:670-5.
18. Wu YK, Kao KC, Hsu KH, Hsieh MJ, Tsai YH. Predictors ofsuccessful weaning from prolonged mechanical ventilation inTaiwan. Respir Med 2009;103:1189-95.
19. Shin HJ, Chang JS, Ahn S, Kim TO, Park CK, Lim JH, et al.Clinical factors associated with weaning failure in patientsrequiring prolonged mechanical ventilation. J Thorac Dis2017;9:143-50.
20. Verbraecken J, McNicholas WT. Respiratory mechanics andventilatory control in overlap syndrome and obesity hypoven-tilation. Respir Res 2013;14:132.
21. Mohamed S, Bayoumi H, Abd El-Aziz N, Mousa E, Gamal Y.Prevalence, risk factors, and impact of lung Cancer on out-comes of idiopathic pulmonary fibrosis: a study from theMiddle East. Multidiscip Respir Med 2018;13:37.
22. Weitzenblum E, Chaouat A, Kessler R, Canuet M. Overlapsyndrome. Obstructive sleep apnea in patients with chronicobstructive pulmonary disease. Proc Am Thorac Soc2008;5:237-41.
23. Alía I, Esteban A. Weaning from mechanical ventilation. CritCare 2000;4:72-80.
24. Burns SM, Fisher C, Tribble SE, Lewis R, Merrel P, ConawayMR, et al. The relationship of 26 clinical factors to weaning
MRM_01 original.qxp_Hrev_master 04/08/20 11:20 Pagina 101

55MRM
Multidisciplinary Respiratory Medicine 2020; 15:691 - N.A. Abdelaleem et al.
outcome. Am J Crit Care 2012;21:52-8; quiz 59.25. Dehghani A, Abdeyazdan G, Davaridolatabadi E. An overview
of the predictor standard tools for patient weaning frommechanical ventilation. Electron Physician 2016;8:1955-63.
26. Blackwood B, Alderdice F, Burns K, Cardwell C, Lavery G,
O'Halloran P. Use of weaning protocols for reducing durationof mechanical ventilation in critically ill adult patients:Cochrane systematic review and meta-analysis. BMJ2011;342:c7237.
Received for publication: 16 June 2020. Accepted for publication: 17 July 2020.This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0).©Copyright: the Author(s), 2020Licensee PAGEPress, ItalyMultidisciplinary Respiratory Medicine 2020; 15:691doi:10.4081/mrm.2020.691
MRM_01 original.qxp_Hrev_master 04/08/20 11:20 Pagina 102

56MRM
Novel therapeutic approaches for the management of cystic fibrosisRyan Jaques, Arslan Shakeel, Cameron HoyleCentre for Atherothrombosis and Metabolic Disease, Hull York Medical School, University of Hull, UK
Cystic fibrosis (CF) is a genetic condition characterised by the build-up of thick, sticky mucus that can damage manyof the body’s organs. It is a life-long disease that results in a shortened life expectancy, often due to the progression ofadvanced lung disease. Treatment has previously targeted the downstream symptoms such as diminished mucus clear-ance and recurrent infection. More recently, significant advances have been made in treating the cause of the diseaseby targeting the faulty gene responsible. Hope for the development of potential therapies lies with ongoing researchinto new pharmacological agents and gene therapy. This review gives an overview of CF, and summarises the currentevidence regarding the disease management and upcoming strategies aimed at treating or potentially curing this con-dition.
Key words: Cystic fibrosis; CFTR; treatment; infection; gene therapy.
AB
STR
ACT
Correspondence: Ryan Jaques, Molecular Physiology Laboratory, Centre for Atherothrombosis & Metabolic Disease, HullYork Medical School, University of Hull Cottingham Road, Hull HU6 7RX, UK. Tel. +44.1482.465008. E-mail: [email protected]
Contributions: RJ, concepted the design of the paper and wrote most of the main text. AS, wrote significant portions of thepaper, specifically within the emerging molecular therapies section; he also revised and edited the final draft. CH, providedadditional information, revising, and helping draft the article. All contributors are satisfied with all aspects of the work.Conflict of interest: RJ, AS and CH, have no competing interests, as we wrote this manuscript entirely by ourselves, and donot work for any corporation or government.Funding: There was no funding for this manuscript. It was written and put together by RJ, AS and CH. Availability of data and materials: Data was only gathered from previously published clinical trials, as referenced in the paper.This data was mainly used in the tables to highlight the efficiencies of treatment. No data was taken by the authors as this is a reviewarticle.Ethics approval and consent to participate: As this was a review article it does not require consent due to the absence ofparticipants.
REVIEW
Multidisciplinary Respiratory Medicine 2020; volume 15:690
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 48

57MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
IntroductionCystic fibrosis (CF) is a life-long condition characterised
primarily by a build-up of mucus in the lungs and digestive tracts[1]. The body’s failure to remove this often leads to breathingdifficulties and frequent lung infections [2]. Unfortunately, thesemanifestations become chronic as patients progress through life,with pulmonary disease and respiratory failure remaining the majorcause of morbidity and mortality [3]. Currently, there is no cure forCF, however with good management, patients often live well intoadulthood with the average predicted survival standing at 48 yearsfor males and 43 years for females [4]. Yet, the demanding routinepatients must go through to control their symptoms often hasdeleterious effects on their physical and mental wellbeing. Ongoingresearch is trying to explore how we can minimise these problems,focusing on how best to manage, treat and possibly cure CF.
The aim of this review is to critically discuss the currentevidence on the therapeutic strategies for managing CF. Firstly, weprovide an overview of CF in relation to its clinical presentation andpathophysiology and then look at the current options available fortreatment. We will then explore future therapies, where emphasismay be given towards how we can target the underlyingmechanisms of this genetic condition by focusing onpharmacological interventions that are currently undergoinginvestigation.
Prevalence of CFVarious countries have introduced registers which track the
number of patients diagnosed with CF [5-7]. These help to measure,appraise and compare aspects of cystic fibrosis, its diagnosis, andits treatment regimen, thereby encouraging new procedures to dealwith this disease. Most countries within Africa, South America andparts of Asia have a limited or non-existent system due to healthauthorities prioritising other important public health issues; poverty,malnutrition, civil war, and outbreaks of infectious diseases aregiven greater emphasis [8]. For these reasons, the most accurate dataconcerning the prevalence of CF is usually found in countries withinEurope and North America.
Each year, the European Cystic Fibrosis Society PatientRegistry collects data on CF patients and causative mutations fromEurope and neighbouring countries [5]. In the 2017 report [9], thenumber of CF patients registered totalled 48,204, though the amountis certain to be higher due to coverage varying from differentcountries [10]. In Romania for example, there is an estimated 35%coverage in comparison to the UK which has a coverage of morethan 95% [9]. Overall, the F508del mutation is the most frequent,with approximately 80% of patients detected as being F508delheterozygous and around 40% as being F508del homozygous. Thisis in comparison to the G542X allele mutation, the second mostcommon, for which 2.69% of patients tested positive and N1303Kwith 2.19%, although it should be noted that the geographicaldistributions of these variants can differ.
The frequency of CF in North America is similar to Europe,affecting 1 in 2,500-3,500 people [11,12]. However, there aredifferences in its distribution across the North American continent.This is primarily linked to ethnic group; the Caucasian populationhas a higher prevalence than other ethnicities, including Hispanics,Native Americans and those of African or Caribbean ancestry [8].Consequently, as with Europe, North America’s most prevalentmutation is the F508del mutation. The 2018 US Cystic FibrosisFoundation Patients Registry report found that, in those genotyped,84.7% of those in the registry had at least one F508del mutation,with 44.2% of those being homozygous for F508del [13]. There is
a substantial drop in the next prevalent mutations which are G542X,G551D and R117H. These are found to be at a prevalence of 4.6%,4.4% and 3.0% of the CF population, respectively. Due to its highfrequency among Caucasian populations, it is the most common,potentially lethal inherited condition in this demographic [14].
PathophysiologyCystic fibrosis is an autosomal recessive disorder caused by a
mutation on chromosome 7 at position q31.2 [15]. This locationcontains the cystic fibrosis transmembrane conductance regulator(CFTR) gene which is 189 kb in length with 27 exons and 26introns. The protein itself is made of 1,480 amino acids and consistsof five domains. There are two transmembrane domains that areeach connected to a nucleotide binding domain (NBD) in thecytoplasm. The first NBD is connected to the secondtransmembrane domain by a regulatory ‘R’ domain. For the channelto open, serine residues on the ‘R’ domain must be phosphorylatedby a cAMP-dependent protein kinase and ATP must bind to bothNBDs and be subsequently hydrolysed [16]. In its open state, thechannel is responsible for the transport of anions, specificallybicarbonate and chloride ions, across the cell membrane [17].Physiologically, chloride and bicarbonate ions are secreted onto theepithelial surface by the CFTR channel resulting in the secretion offluid through osmosis. Any impairment in CFTR function maytherefore lead to a decrease in CFTR-mediated chloride andbicarbonate secretion. Water resorption follows, creating a thick,viscous mucus which accumulates on the epithelial surfaces ofbodily organs such as the lungs, liver, intestines and pancreas [18].The CFTR channel is also involved in the regulation of the epithelialsodium channel (ENaC), otherwise known as the amiloride-sensitive sodium channel, found in the airways of the lungs [19].
While CF is a multi-organ disease, the dominant cause ofmorbidity and mortality is its effects on the lungs [20]. In theairways of the lungs, CFTR is highly expressed, where the build-up of mucus often causes breathing difficulties and increases therisk of infections. The airways are predominantly lined bypseudostratified columnar epithelium [21]. This epithelium iscomposed of numerous cell types including basal cells, club cells,ciliated cells, goblet cells, and pulmonary neuroendocrine cells(PNECs) amongst others. The pulmonary ionocytes are of particularimportance to CF. These cells are derived from basal cells and areresponsible for most of the CFTR expression in the airwayepithelium. It is therefore thought that pulmonary ionocytes areheavily involved in fluid regulation and may play a critical role inthe pathogenesis of CF [22].
Mucus build-up is primarily driven by dehydration of the airwaysurface liquid (ASL) that coats the epithelial cells of the airways.Hydration of the ASL is primarily regulated by CFTR-mediatedanion secretion and ENaC-mediated sodium absorption. In CF, anincrease in ENaC-mediated sodium absorption into the airwayepithelial cells has been found alongside CFTR dysfunction,contributing to the dehydration of ASL [23]. This is thought to bedue to the abolition of ENaC regulation by the CFTR channel, whenCFTR is mutated and dysfunctional, as seen in CF [24]. The ASL iscomposed of a periciliary layer (PCL) that is covered with a mucuslayer (ML) [25]. The ML is composed of mucins that form a gel-like structure and are involved in trapping inhaled particles, whilethe PCL covers the cilia, preventing penetration by those inhaledparticles. This allows the cilia to beat to remove inhaled particlesthrough mucociliary clearance. Dehydration of the ASL leads to adecrease in PCL volume, resulting in the dehydrated MLcompressing the cilia. This ultimately results in a decrease in theability of the cilia to beat, thickened mucus, mucus stasis, and
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 49

58MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
recurrent infections [26]. Over time this may progress into chroniclung disease and an overall decline in lung function.
CFTR is also strongly expressed in the sebaceous and eccrinesweat glands [15,27]. Defective CFTR results in reduced transportof sodium chloride in the absorptive duct and therefore results insaltier sweat. In the digestive tract, nutrition and vitamindeficiencies are common as mucus clogs the pancreas, preventingdigestive enzymes from reaching the gut. Blockages of the smallducts in the liver and biliary system can lead to problems such asgallstones and liver disease, with the latter affecting roughly 30%of CF sufferers [28]. The reproductive systems are also not sparedas the destruction of the vas deferens and epididymis are responsiblefor 95% of male CF patients being infertile [29]. In females, themajority are fertile but have thicker cervical mucus and may haveovulation issues due to poor nutrition.
There are 2,102 known mutations of the CFTR gene [30], over1,850 of which are known to be disease-causing [31]. These areseparated into classes I-VI as shown in Table 1. Patients with ClassI-III mutations often have more severe clinical features due to eitherthe absence of the CFTR protein at the cell surface, or the lack ofefficient gating of the channel [32]. The most common mutation isthe F508del mutation, which is a frameshift mutation caused by adeletion of phenylalanine at codon 508. As a class II mutation, itcauses the misfolding of the CFTR protein, which is subsequentlypolyubiquitinated and destroyed by the cell proteasome [33]. Eachmutation class confers a different defect in CFTR production and/orfunction, and therefore unique approaches are required whendesigning treatments that can target these alterations.
Diagnosis of CFThere are several tests that can be utilised for diagnosing CF.
Babies are screened for CF using the heel prick test and, as a result,most children are diagnosed shortly after birth. The test itselfinvolves taking blood from the baby’s heel at around 5 days of age,which is then sampled for several conditions including CF. The firststage of testing involves the measurement of ImmunoreactiveTrypsinogen (IRT) levels, which are raised in CF patients due toblockages of the pancreatic ducts [34]. If IRT is raised, mutationanalysis of the CFTR gene is undertaken. To test positive, twocopies of the faulty gene need to be identified, though further testsare required to confirm a diagnosis [35]. In this case, a sweat testwill be ordered which measures the salt levels on the skin, as thosewith CF have higher chloride levels compared to the generalpopulation. The values of chloride and sodium in sweat are around10-50 mmol/L in normal subjects, but in the patients with CF theyare usually above 60 mmol/L and can be as high as 120 mmol/L[36].
Antenatal testing can be offered for potential parents who areaware they are both carriers. This may involve a chorionic biopsyor amniocentesis during pregnancy to identify the condition of thebaby. Benefits of early diagnosis allow treatment to begin at birth,although these procedures can carry an increased risk ofmiscarriage.
New non-invasive techniques are available and can aid earlydiagnosis, although these are only accessible privately. Thedevelopment of safer prenatal screening has been developed by theidentification of circulating free foetal DNA in the maternal plasmain early gestation [37]. DNA reflecting both maternal and foetalmaterial is collected from the maternal plasma, which is molecularlyamplified by PCR and subsequently sequenced. The foetal DNAwill be analysed to assess the inheritance of the CFTR mutation.Tests that can be offered include the paternal mutation exclusionwhen the parents carry different CF mutations, or where bothparents are carriers of the same CF mutation. If the baby hasinherited the paternal mutation, an invasive test may be required tosee if the maternal mutation has also been inherited.
Cystic fibrosis can also be diagnosed later in life. This isbecause rarer mutations are not screened early on and may presentwith delayed symptoms that mimic other lung pathologies such asbronchitis, thus making an accurate diagnosis more challenging.Individuals may choose to get tested to determine if they carry afaulty CFTR gene, especially if they have a relative or history ofCF in their family.
The nasal potential difference (NPD) test measures how wellsodium and chloride flow across the mucous membrane lining thenasal cavity. NPD gives an in vivo measurement of CFTR functionand sodium channel function in the respiratory epithelium [38]. Thisis helpful in distinguishing individuals with non-classic forms ofCF with evidence of CFTR dysfunction, from individuals withnormal CFTR function that are unlikely to have CF. This cantherefore be used alongside sweat tests, especially in those with anintermediate sweat result and who may carry a rare or unknownmutation.
Clinical assessment of disease progressionRoutine monitoring and assessments are crucial to assess any
changes that can occur as patients progress through life.Comprehensive annual reviews are offered which includepulmonary, nutritional and psychological assessments [39]. Lungfunction is primarily singled-out as this has a significant impact onthe patient’s quality of life, especially if their lung disease hassignificantly advanced. To assess this, pulmonary testing is carriedout through spirometry. This measures forced expiratory volume in1 second (FEV1), forced expiratory flow (FEF)25-75% and forced vital
Table 1. CFTR mutation classes and required strategies for treating cystic fibrosis.
Classification CFTR defect Mutation examples Required approaches Drug required (Approved?)
Class I No functional CFTR protein/mRNA G542X, W1282X, R553X Salvage protein synthesis Bypass therapy (no), Read through agents (no)Class II CFTR trafficking defect ΔΔF508, ΔI507, N1303K Correct protein folding Corrector (yes) Class III Impaired gating G551D, V520F, S549N Recover channel conductance Potentiator (yes)Class IV Decreased channel conductance R334W, R117H, S1235R Recover channel conductance Potentiator (only for R117H)Class V Reduced production of CFTR A455E, 1680-886A→G Improve maturation/correct splicing Antisense oligonucleotides (no), Corrector (no), Amplifier (no)Class VI Decreased CFTR stability Q1412X, 4279 insA Promote protein stability Stabilisers (no)
CFTR, cystic fibrosis transmembrane conductance regulator.
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 50

59MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
capacity (FVC), with oxygen saturation measured to furtherdetermine lung condition. Weight and height are used as keyindicators in evaluating growth and nutritional status. These goalongside tests that look for CF-related disorders such as diabetesand liver disease [40]. Sputum samples are also taken formicrobiological analysis or, if this is not possible, cough swabs ornasopharyngeal aspirates can be used. Any significant abnormalitiesfound in any of these tests may call for clinicians to alter treatment.
Alongside this, regular routine reviews are carried out. Theseare more frequent in earlier life and start immediately afterdiagnosis. In the first month of life these reviews occur weekly,progressing to monthly during the first year, and then incrementingto every 3 to 6 months as patients progress into adulthood. Thesereviews look at treatment adherence, quality of life and anycomplications or concerns patients may have [41]. Sudden onset ofpulmonary exacerbations can regularly appear, and they arenormally caused by an acute pulmonary infection. These often needto be clinically managed, and so chest X-rays may be beneficial inlooking for radiological abnormalities.
Non-pharmacological managementPatients can implement several techniques that may help to
improve their symptoms. Physiotherapy is performed daily, whichhelps to clear the airways and loosens mucus in the lungs. It canalso be adapted to individual needs, as certain techniques canimprove problems such as urinary incontinence and inhaledmedication compliance [42,43]. Frequent exercise is stronglyadvised as this can loosen up sputum, increase respiratory muscleendurance and reduce lung residual volume [44,45].
It is highly important for patients to maintain good nutrition, asa healthy body weight has been directly linked to better lungfunction and fewer chest infections [46]. Unfortunately, due to theGI tract being congested, malabsorption is a common problemespecially in early life [15,47]. To help manage this, more caloriesneed to be consumed and digestive enzyme replacements are givento help aid the breakdown of food [48]. Even with supplementation,CF can increase the body’s energy requirements by over 100%which is challenging for many, particularly for those with poorappetite [49]. Performing these tasks can be a burden, whichpartially explains why psychological distress is frequently seenamong sufferers. Recent studies highlight the vast increase insymptoms of depression and anxiety in both individuals with CFand their caregivers [50,51]. Prevalence data shows that theseproblems are 2-3 times more prevalent than in the generalbackground population [52-54]. To combat this, countries such asthe UK have introduced guidelines where annual reviews assesswellbeing, quality of life and treatment adherence [55].
Established drug therapiesUntil recently, patients have relied on therapies that treat the
symptoms rather than the underlying cause. Such options haveincluded the inhalation of mucoactive agents such as hypertonicsaline, rhDNase and mannitol powder. These aim to help thin themucus on the lung epithelium, making it easier to cough out.
Hypertonic saline works by increasing the amount of salt in theairways, which attracts water and thins the mucus [56]. It isavailable in different concentrations of 3%, 3.5% and 7%. Peoplewho are 6 years or older or those with FEV1 greater than 40%percent predicted can be offered this. Although the guidelines donot advocate for its use among those younger than 6, a recent studyhas shown that inhaled hypertonic saline improved lung clearance
in children aged 3-6 years and could be a suitable early intervention[57].
rhDNase (Dornase alfa; Pulmozyme®) is approved for people5 years and older. It works as an enzyme which hydrolyzes the DNAin the mucus and reduces sputum viscoelasticity [58]. Comparisonsto hypertonic saline show superiority in improving lung function inseveral trials, with one indicating that rhDNase given on alternativedays rather than daily is equally effective [59-61]. Mannitol powderhas also been recommended as an option, although stricter criteriahave been put on its usage. The criteria are as follows: inadequateresponse to rhDNase, declining lung function (>2% decline in FEV1annually), and where other osmotic agents are not appropriate. Theexact mechanism of action is unknown, though it is thought tochange the viscoelastic properties of mucus. It does this byrehydrating the PCL, thereby increasing clearance throughmucociliary activity [62].
Bronchodilators can be used alongside mucolytics as thesewiden the airways, allowing mucus to move easily from smallerairways to larger ones. These also help with bronchospasms whichare a common side effect of inhaled treatments [63].
Molecular therapies for CFRecently, a number of new drugs have been made available
which have shown favourable results in several Phase III clinicaltrials [64-79], as shown in Table 2. These have been designed totarget the underlying mechanism responsible for creating theineffective CFTR protein.
The first therapeutic drug that has demonstrated significantclinical effects is Ivacaftor (Kalydeco®). Developed by VertexPharmaceuticals, it is the first of its kind to target the underlyinggene defect. It works by modulating inefficient CFTR channels atthe cell surface causing them to open [80]. The main target is theG551D mutation, a Class III defect and the most prevalent gatingmutation [81]. Several completed studies highlight the significantimprovements in percent predicted forced expiratory volume in onesecond (ppFEV1) and other clinical outcomes in class III and IVmutations [64-68]. The main drawback of Ivacaftor is that there isno supportive evidence that it is effective for those with a F508delmutation, which accounts for the majority of cases in Europe andNorth America [4,10,13]. This Class II mutation causes ineffectiveprotein folding. To target this, Vertex has designed Lumacaftorwhich acts as a chaperone during protein folding, increasing thenumber of efficient CFTR proteins at the cell surface [82]. Evidenceshows that as a monotherapy, it is ineffective at providing significantimprovements in lung function, but may have potential for use incombination with other drugs [83]. To fully combat the F508delmutation, Vertex has created co-formulated combinations aimed atmaximising the number of effective CFTR channels. The first ofthese is Ivacaftor/Lumacaftor (Orkambi®), which utilises the dualaction of both drugs by helping the protein fold correctly and thenmodulating the channel after it has reached the cell membrane.Some Phase III studies involving Orkambi® have demonstratedsignificant improvements in ppFEV1 [72-74], although others havenot identified such significance [69-71]. Another combinationtreatment is Tezacaftor/Ivacaftor (Symdeko® in US, Symkevi® inEU). Tezacaftor has been designed to facilitate the processing andtrafficking of the CTFR protein towards the cell surface. In the twobiggest completed Phase III studies, EVOLVE and EXPAND, theTezacaftor/Ivacaftor group showed significant improvements inppFEV1 [76-77], although a smaller study showed no significantincrease in ppFEV1 [75].
Vertex has recently produced a triple combination therapyconsisting of a combination of Elexacaftor/Tezacaftor/Ivacaftor
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 51

60MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
(Trikafta® in US, Kaftrio® in EU) that is used in a combinationregimen with ivacaftor. Elexacaftor, like Tezacaftor, is a CFTRcorrector but binds to a different site and facilitates the cellularprocessing and trafficking of the CFTR protein to the cell surface[84]. Of the two completed Phase III clinical trials shown in Table2, greater improvements have been shown in the average ppFEV1and CFT-R score than either Orkambi® or Symkevi® [78-79].Significant reductions in sweat chloride concentration have alsobeen shown compared to trials involving the other dual therapies.
Although these molecular therapies have shown great benefit,there are several side effects that need to be considered beforestarting treatment. Common side effects associated with these drug
therapies include headaches, upper respiratory tract infections, nasalcongestion, abdominal pain, nasopharyngitis, diarrhoea, rash,nausea, and dizziness [64-79]. One of the more severe side effectsis the worsening of liver function, as these treatments have beenshown to increase blood liver enzyme levels [85,86]. This isindicative of hepatic impairment. Blood tests assessing liverfunction must be undertaken before initiation, then every 3 monthsduring the first year, followed by annual appointments. Thesetherapies have also been shown to increase the risk of cataracts insome children and adolescents [87-90], so an eye examinationshould be performed before and during treatment. The therapeuticeffectiveness of these therapies can vary if in concomitant use with
Table 2. Published phase III clinical trials for new drug therapies for cystic fibrosis (up to June 2020).
Drug Study Name Outcome(s) Age Length Mutation Main finding in treatment group Ref.
Ivacaftor KONDUCT I. Safety ≥6 Yrs 24W R117H Mean absolute ppFEV1 significantly 64(Kalydeco®) (n=69) II. Change in ppFEV1 increased for those >18 years by 5.0% (95% CI 1.15-8.78%), not in those aged 6-11 years. KONNECTION I. Change in ppFEV1 ≥6 Yrs 24W Non-G551D Gating Significant improvement in BMI and sweat chloride. ppFEV1 65 (n=39) with model-adjusted absolute mean increased by 10.7% (95% CI 7.3-14.1%) at 8W and was maintained through 24W. ENVISION I. Change in ppFEV1 6-11 Yrs 48W G551D Significant increase in adjusted ppFEV1 when compared 66 (n=52) to placebo (10.7% vs. 0.7%, P < 0.001). Mean gain of 2.8 kg more than placebo with sweat chloride levels significantly reduced. PERSIST I. AE's ≥6 Yrs 144W G551D Well tolerated. Sustained improvements in ppFEV1 67 (n=192) II. Change in ppFEV1 and weight in all ages. PEx remained suppressed in adult/ adolescents versus placebo. STRIVE I. Change in ppFEV1 ≥12 Yrs 48W G551D Significant increase in ppFEV1 at 24W (10.6%) and maintained 68 (n=161) at W48. PEx reduced by 55% and sweat chloride was significantly reduced. Mean gain of 2.7kg compared to placebo. Lumacaftor/ VX15-809-115 I. AE 2-5 Yrs 24W 2 F508del Both drugs well tolerated. Mean sweat chloride 69Ivacaftor (n=60) II. Sweat chloride concentrations decreased on average 31.7 mmol/L. (Orkambi®) VX13-809-011 I. AE 6-11 Yrs 24W 2 F508del Well tolerated. No significant change in ppFEV1, but significant 70 (n=58) II. Change in ppFEV1 improvements in BMI, CFQ-R scores and sweat chloride level reduced by 24.8 mmol/L. VX14-809-106 I. AE ≥12 Yrs 24W 2 F508del Severe lung disease patients receiving half dose had less 71 (n=46) II. Change in ppFEV1 respiratory events with shorter duration. ppFEV1 was similar to baseline from 4W onward. TRAFFIC and I. Change in ppFEV1 ≥12 Yrs 24W 2 F508del Significant improvements in ppFEV1 in those with varying degrees 72 TRANSPORT of lung function. Significant improvements in BMI and PEx. (n=1108) Some AEs were higher in intervention groups. VX14-809-109 I. Lung clearance 6-11 Yrs 24W 2 F508del Significant improvement in lung function; change in LCI2.5 by -1.09 73 (n=206) II. Change in ppFEV1 units (95% CI -1.43 to -0.75) and absolute change ppFEV1 by 2.4% (95% CI 0.4-4.4%) using least square mean analysis. PROGRESS I. AE ≥12 Yrs 96W 2 F508del ppFEV1 was maintained from continued treatment. PEx rate 74 (N=1030) II. Change in ppFEV1 remained lower than placebo. Annual ppFEV1 decline was reduced. Tezacaftor/ VX15-661-113 I. Safety 6-11 Yrs 24W ≥1 F508del + 1 F/RF Well tolerated. Significantly improved sweat chloride levels 75Ivacaftor (n=70) II. Change in ppFEV1 and CFQ-R scores. Mean absolute change ppFEV1 remained stable. (Symdeko® in US, EVOLVE I. Change in ppFEV1 ≥12 Yrs 24W 2 F508del PEx were 35% lower. Absolute and relative mean changes in ppFEV1 76Symkevi® in EU (n=510) II. PEx significantly improved by 4.0% (95%CI 3.1-4.8%) and 6.8% (95% CI 5.3-8.3) respectively (P<0.001 for both). EXPAND I. Change in ppFEV1 ≥12 Yrs 24W 1 F508del + 1 F/RF Absolute change ppFEV1 was significantly increased in 77 (n=248) Tezacaftor/Ivacaftor group by 6.8% (95% CI 5.7-7.8%) and Ivacaftor group by 4.7% (95% CI, 3.7-5.8%) compared to placebo. Elexacaftor/ VX17-445-102 I. Change in ppFEV1 ≥12 Yrs 24W1 F508del + 1 F/MF ppFEV1 was significantly higher at 4W (13.8%) and 24W (14.3%) 78Tezacaftor/Ivacaftor (n=403) checkpoints. PExs were 63% lower with sweat chloride (Trikafta® levels significant reduced.in US/Kaftrio® VX17-445-103 I. Change in ppFEV1 ≥12 Yrs 4W 2 F508del Elexacaftor/Tezacaftor/Ivacaftor group had significant 79in EU) (n=113) II. Sweat Chloride increase in ppFEV1 of 10.0% (95% CI 7·4-12·6%) and significant improvement in sweat chloride levels by 45·1 mmol/L (95% CI -50·1 to -40·1) compared to Tezacaftor/Ivacaftor group.Ref., Reference; n, number of enrolled participants; ppFEV1, percent predicted forced expiratory volume in one second; CI, confidence intervals; Yrs, years; W, weeks; BMI, body mass index; AE,adverse effects; PEx, pulmonary exacerbations; CFQ-R, cystic fibrosis questionnaire-revised; LCI, lung clearance index; RCT, randomised control trial; F/RF, residual function mutation; F/MF, minimalfunction mutation.
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 52

61MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
other medications that induce or inhibit CYP3A4 enzymes.Therefore, a drug history and review would have to be undertakenbefore starting any treatment.
The therapeutic indications for these new molecular therapiesare shown in Table 3. These include the authorised use from the USFood and Drug administration, and European Medicines Agency.Currently in the EU, Kalydeco’s approval covers the medication’suse in children as young as six months, while the approval forSymkevi® allows its use in patients aged 12 or older. This may soonbe reduced to 4 months for Kalydeco® and 6 years for Symkevi®as this has been recommended to be green lighted by the EuropeanMedicines Agency [91,92].
Use of bronchodilatorsBronchodilators are primarily used in the treatment of chronic
obstructive diseases, but their role in CF is less clear. Measurementsof FEV1 and FVC amongst CF patients can change up to 20%throughout the day, so assessing the effects bronchodilators isdifficult [93]. The mechanism by which CF causes airwayinflammation differs from asthma, resulting in a progressive non-reversible airflow obstruction [94]. In some cases, asthma can occuralongside CF, but obtaining a diagnosis is difficult due the similarityof symptoms these conditions present with. Furthermore, there isno universal definition of asthma which makes it harder to confirma concomitant diagnosis. According to the European EpidemiologicRegistry of Cystic Fibrosis and the North American EpidemiologicStudy of Cystic Fibrosis databases, the prevalence of asthma in CFpatients is around 17% and 19% respectively, with identicalproportions seen amongst children and adults [95]. It could beassumed this would translate into the CF population; however, thisassumption cannot be made as there are ongoing discussions overwhether CF gene heterozygosity predisposes asthma development[96,97].
Only a limited number of trials show short acting beta-2 agonists
increasing ppFEV1 in the short term, with increases in peakexpiratory flow rate mostly seen in the long term in those withbronchial hyperreactivity and/or bronchodilator responsiveness[98]. Contrary to this, there have been other trials that have shownno clinical benefit. To further evaluate the use of this therapy, aninvestigation is underway examining the effects of a short actingbeta-2 agonist (Salbutamol) on shortness of breath, exerciseperformance and breathing responses in adults with CF(NCT03522831).
A recent Cochrane review into the use of long-termbronchodilators suggests that neither beta-2 agonists nor muscarinicantagonists produce significant improvements in ppFEV1, adverseevents or quality of life [99]. The only suggested benefit was that itmay help reduce the burden for CF patients as they can be takenless frequently. These conclusions have led some experts torecommend that these drugs should not be prescribed [100].
One area of similarity between CF and asthma is theinvolvement of the small airways (airways <2mm). In both CF andasthma, the small airways are thickened due to inflammation, andare now thought to a play a central role in CF lung disease [101].The small airways have traditionally been referred to as the “silentzone” of the lungs due to their relatively small contribution to totalrespiratory resistance. As a consequence, any damage to the smallairways may not result in symptoms until the damage is advanced[102]. Recent evidence suggests that this “silent zone” may play amuch greater role in airway pathology than previously thought andpossibly could be used as a prognostic indicator [103]. Due to thecentral role of the small airways in CF lung pathology, they mayserve as a target for future therapies. This could be particularlyimportant for patients who suffer with asthma alongside CF.
Inhaled corticosteroidsThe use of inhaled corticosteroids (ICS) as anti-inflammatory
agents in both adults and children with CF is not often
Table 3. Authorised use of new drug therapies in the EU and US.
Drug (trade name) EMA therapeutic indication US FDA therapeutic indication
Ivacaftor (Kalydeco®) Kalydeco® is used on its own to treat cystic Kalydeco® is used on its own to treat cystic fibrosis in patients aged 4 fibrosis in patients aged 6 months and above months and over who have one of 10 mutations in the CFTR gene: G551D, who have one of the following mutations in the G178R, S549N, S549R, G551S, G1244E, S1251N, S1255P, G1349D or R117H. CFTR gene: R117H, G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N and S549R. Lumacaftor/ivacaftor Orkambi® tablets are indicated for the treatment of CF Orkambi® tablets are indicated for the treatment of CF in patients (Orkambi®) in patients aged 2 years and older who are homozygous for the aged 2 years and older who are homozygous for the F508del mutation F508del mutation in the CFTR gene. Orkambi® granules are in the CFTR gene. Orkambi® granules are indicated for the treatment indicated for the treatment of CF in children aged 2 years and of cystic fibrosis CF in children aged 2 years and older who are older who are homozygous for the F508del mutation in the CFTR gene. homozygous for the F508del mutation in the CFTR gene.Tezacaftor/Ivacaftor Symkevi® is indicated in a combination regimen with ivacaftor for the Symdeko® is indicated in a combination regimen with ivacaftor for the (Symdeko® in US, treatment of patients with CF aged 12 years and older who are treatment of patients with CF aged 6 years and older who are homozygous Symkevi® in EU) homozygous for the F508del mutation or who are heterozygous for the F508del mutation or have a single copy of the following mutations for the F508del mutation and have one of the following mutations in the CFTR gene: A455E, E56K, R74W, A1067T, E193K, R117C, D110E, in the CFTR gene: P67L, R117C, L206W, R352Q, A455E, D579G, 711+ F1052V, R347H, D110H, F1074L, R352Q, D579G, K1060T, R1070W, D1152H, 3A→G, S945L, S977F, R1070W, D1152H, 2789+5G→A, 3272 26A→G, L206W, S945L, D1270N, P67L, S977F, 711+3A→G, 3272-26A→G, and 3849+10kbC→T. E831X, 2789+5G→A, 3849+10kbC→T.Elexacaftor/Tezacaftor/ Kaftrio® is indicated in a combination regimen with ivacaftor for the Trikafta® is indicated in a combination regimen with ivacaftor for the Ivacaftor (Trikafta® treatment of CF in patients aged 12 years and older who are treatment of CF in patients aged 12 years and older who have at least one in US/Kaftrio® in EU) homozygous for the F508del mutation in the CFTR gene or F508del mutation in the CFTR gene.
heterozygous for F508del in the CFTR gene with a minimal function mutation.
EMA, European Medicines Agency; US FDA, United States Food and Drug Administration; CF, cystic fibrosis; CFTR, cystic fibrosis transmembrane conductance regulator.
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 53

62MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
recommended. There is no evidence to suggest that these improvelung function or quality of life [104]. In fact, there is some evidenceto suggest there is an adverse effect on growth at high dosages [105].Therefore, the use of corticosteroids should be restricted to thosewith symptomatic wheezing if deemed to be beneficial. Regularassessments will be needed to identify if the treatment is working,as well as to identify any side effects. However, it is important toconsider that corticosteroids are heterogeneous, resulting in differentside-effect profiles. An example of this is the increased risk ofpneumonia in patients taking fluticasone, alone or in combinationwith salmeterol, whilst there is no similarly reported increased riskof pneumonia in patients taking a budesonide/formoterolcombination. The use of some steroids can therefore be safer thanothers and careful attention must be paid to the side effect profilesof individual ICS [106].
Lung transplantationDue to the absence of a cure, there may be a point where
conventional treatments no longer work. In this scenario, medicalstaff may then have to decide whether a lung transplant is the mostviable option. Other organs such as the liver or pancreas are alsoexamined for possible transplantation, but only if necessary. Thereis no way to determine how long a patient will have to wait for atransplant. This would depend upon how the transplant team haveevaluated their condition, but also on the availability of a donor thatis a good match for the patient. For most, this takes several monthswhere only two in three will be successful in having a transplant[107]. Survival rates at 5 years after the procedure are approximately60% among CF patients, with many of these living for at least 10years [108].
Antibiotic treatment and prophylaxis As well as airway obstruction, CF is characterised by chronic
bacterial infections and inflammatory exacerbations [15,109]. It isnot known whether the predisposition to infection is caused bydecreased ASL alone, or whether environmental factors or evenimmunological defects are at play. What becomes clear however, isthat CF lung pathogenesis begins with the altered lung environmenttriggered by the abnormal CFTR.
The microbiome of the lung environment in CF is different fromthat of healthy people, as the diversity changes as patients get olderand their lung disease progresses [110]. The traditional viewproposes that bacterial communities become less diverse withantibiotic usage and advancing lung disease [111]. The communitythereby becomes dominated with bacteria such as Staphylococcusaureus (S. aureus) or opportunistic pathogens such as Pseudomonasaeruginosa (P. aeruginosa), Haemophilus influenzae (H.influenzae), Stenotrophomonas maltophilia (S. maltophilia),Burkholderia cepacian (B. cepacian), and Achromobacterxylosoxidans (A. xylosoxidans), with P. aeruginosa being thepredominate lung infection in CF [112]. All of these, with theexception of S. aureus, are gram negative and are associated withsteep declines in lung function, increased risk of exacerbations andgreater risk of mortality [113].
Recognition of the diverse microbiota raises questions on howbest to approach antibiotic treatment. In terms of antibioticresistance, S. maltophilia, B. cepacia and P. aeruginosa have beenfound to be difficult to kill due to their vast array of resistancemechanisms [114]. These include Beta-lactamases, efflux pumps,and biofilm formation which increase their resistance to
aminoglycosides, flouroquinolones and Beta-lactams [115]. In somecases, especially in early life, antibiotic prophylaxis may be givento prevent infection and lung damage. Any changes to the treatmentregimen will have to be evaluated beforehand. This will look at thepotential side effects that may arise, such as the possibility of drugtoxicity when using drugs such as Streptomycin, Kanamycin andAmikacin to treat non-tuberculous mycobacteria. These drugs canhave adverse effects on auditory, vestibular, renal andneuromuscular function [116]. These also have been shown tointerfere with CY3PA4 enzymes, and therefore patients beingtreated with the new molecular therapies (Kalydeco®, Orkambi®,Symkevi®/Symdeko®, or Trikafta®/Kaftrio®) need to be closelymonitored.
Ongoing clinical trialsIn the first part of this review we have discussed the current
management of CF. Next, we will expand into novel treatmentpossibilities, exploring how these could improve upon treating theunderlying mechanism of CF. Many clinical trials are currentlyunderway, which look at treatments that aim to improve pulmonaryfunction, as shown in Table 4. This does not include trials aimingto treat pulmonary exacerbations or lung infections, but thecompounds may reduce the number of these as a secondary effect.
Emerging molecular therapiesThere is ongoing development on a variety of new potentiators
and correctors. Alongside this, entirely new classes of CFTRmodulators are in development, primarily read-through agents andCFTR amplifiers. Potentiators and correctors currently indevelopment are shown in Table 4. ABBV-3067 (formerly knownas GLPG-3067) has completed Phase I clinical trials(NCT03128606) and preliminary results seem to indicate that thedrug was well tolerated [117]. As shown in Table 4, it is now inPhase II clinical trials alone and in combination with ABBV-2222(formerly known as GLPG-2222), a corrector that demonstratedadvantages over the first generation correctors Lumacaftor andTezacaftor in preclinical studies [118]. The new CFTR modulatorsPTI-801, PTI-808 and PTI-428 are being tested in combination, asseen in Table 4. PTI-801 is a corrector, PTI-808 is a potentiator, andPTI-428 is a novel class of CFTR modulator known as an“amplifier”. This triple combination has completed Phase II trialsin patients with at least one copy of the F508del mutation(NCT03251092), with a reported significant improvement inppFEV1 and reduction in sweat chloride concentration [119].Thereare now plans to move ahead with two Phase III clinical trials; theMORE (Modulator Options to RestorE CFTR) trial for subjects thatare homozygous for F508del to confirm the efficacy of the triplecombination and the CHOICES (Crossover trial based on HumanOrganoid Individual response in CF) trial that aims to develop thearea of personalised medicine in CF [120].
CFTR amplifiersOf particular significance is the amplifier PTI-428. Amplifier
agents work to increase the levels of CFTR protein by stabilisingCFTR mRNA. The very early experimental compound known asPTI-CH acted in a mutation-agnostic fashion and demonstratedefficacy in preclinical studies [121]. The development of PTI-428,a first-in-class amplifier, followed. In a Phase II study assessing thesafety and efficacy of PTI-428 in patients taking Orkambi®, the testgroup exhibited a 5.2% increase in mean absolute improvement in
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 54

63MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
Table 4. Current active and/or recruiting studies for drug therapies for cystic fibrosis (up to June 2020).
Intervention Age Phase Drug action Allele mutation Trial no. Status Sponsordrug(s) criteria
ELX-02 ≥18 years II ERSG ≥ 1 G542X NCT04126473 Recruiting Eloxx PharmaceuticalsOrkambi® ≥12 years - Potentiator/corrector 2 F508del NCT03894657 Recruiting Assistance Publique - Hôpitaux de ParisTEZ/IVA ≥ 6 years III Potentiator/corrector ≥ 1 F508del NCT03537651 Active, not recruiting Vertex PharmaceuticalsELX/TEZ/IVA ≥ 12 years III Potentiator/corrector ≥ 1 F508del + 1 (F/MF) NCT03447262 Active, not recruiting Vertex PharmaceuticalsELX/TEZ /IVA ≥ 12 years III Potentiator/corrector 1 F508del + 1 (F/G and F/RF) NCT04058366 Enrolling by invitation Vertex PharmaceuticalsELX/TEZ/IVA ≥ 12 years III Potentiator/corrector 1 F508del + 1 (F/G and F/RF) NCT04058353 Recruiting Vertex PharmaceuticalsELX/TEZ/IVA ≥ 12 years III Potentiator/corrector ≥ 1 F508del NCT04043806 Recruiting Vertex PharmaceuticalsELX/TEZ/IVA ≥ 12 years III Potentiator/corrector ≥ 1 F508del NCT03525574 Active, not recruiting Vertex PharmaceuticalsELX/TEZ/IVA ≥ 12 years III Potentiator/corrector 2 F508del NCT04105972 Active, not recruiting Vertex PharmaceuticalsELX/TEZ/IVA ≥ 6 years III Potentiator/corrector 2 F508del or 1 F508del + 1 (F/F or F/MF) NCT04183790 Enrolling by invitation Vertex PharmaceuticalsELX/TEZ/IVA 6-11 years III Potentiator/corrector 2 F508del or 1 F508del + 1 (F/F or F/MF) NCT03691779 Active, not recruiting Vertex PharmaceuticalsELX/TEZ/IVA ≥ 12 years II Potentiator/corrector Partial function mutations NCT03506061 Recruiting Emory UniversityPOL6014 18 - 55 years Ib/IIa NEI No specific mutation specified NCT03748199 Recruiting Santhera PharmaceuticalsCHF 6333 ≥ 18 years I NEI No specific mutation specified NCT04010799 Recruiting Chiesi Farmaceutici S.p.A.PTI-801 18 - 55 years I Corrector 2 F508del NCT03140527 Recruiting Proteostasis TherapeuticsABBV-3067 +/- ABBV-2222 ≥ 18 years II Potentiator/corrector 2 F508del NCT03969888 Recruiting AbbVieIONIS-ENaCRx 18 - 50 years Ib/IIa ENaC blocker No specific mutation specified NCT03647228 Recruiting Ionis PharmaceuticalsARO-ENaC 18-55 years I/II ENaC blocker No specific mutation specified NCT04375514 Recruiting Arrowhead PharmaceuticalsPTI-808/PTI-428/PTI-801 18 - 99 years Ib/IIa Potentiator/amplifier/ ≥ 1 F508del NCT03251092 Active, Proteostasis corrector not recruiting TherapeuticsLAU-7b ≥ 18 years II Anti-inflammatory No specific mutation specified NCT03265288 Recruiting Laurent Pharmaceuticals BI 1265162 ≥ 12 years II ENaC blocker ≥ 2 CF mutations NCT04059094 Recruiting Boehringer IngelheimLenabasum ≥ 12 years II Anti-inflammatory No specific mutation NCT03451045 Active, not Corbus (20 mg; 5mg) specified recruiting PharmaceuticalsOligoG Dry ≥ 12 years II/III Mucolytic No specific mutation NCT03698448 Not yet recruiting AlgiPharma ASpowder specified OligoG Dry ≥ 18 years II/III Mucolytic No specific mutation NCT03822455 Recruiting AlgiPharma ASpowder specified CB-280 ≥ 18 years Ib Anti-inflammatory No specific mutation NCT04279769 Not yet recruiting Calithera specified BiosciencesMRT5005 ≥ 18 years I/II mRNA therapy Two Class I or II NCT03375047 Recruiting Translate Bio mutations VX-561/IVA ≥ 18 years II Potentiator 1 of either: G551D, G178R, NCT03911713 Recruiting Vertex S549N, S549R, G551S, G1244E, Pharmaceuticals S1251N, S1255P, or G1349D ERSG, Eukaryotic ribosomal selective glycoside; TEZ, Tezacaftor; IVA, Ivacaftor; ELX, Elexacaftor; F, F508del mutation; MF, minimal function mutation; G, gating mutation; RF, residual function mutation; NEI, neutrophil elastase inhibitor; ENaC, epithelial sodium channel.
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 55

64MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
ppFEV1 [122]. It continues to be tested in combination with PTI-808 and PTI-801.
Readthrough agentsAttention has also been given to the potential usage of
readthrough agents, a novel type of CFTR modulator, in patientswith CF resulting from nonsense mutations. These are pointmutations that result in the introduction of a premature terminationcodon (PTC), resulting in the production of a truncated anddysfunctional protein. This problem can be bypassed using thenatural process of translational readthrough (TR). TR involves thesuppression of a PTC which allows for translation to continuebeyond that PTC, subsequently resulting in the development of thefull-length protein. Readthrough agents seek to exploit this naturalphenomenon to allow for the frequent production of a full-length,fully functional protein [123]. Such agents are therefore potentiallyuseful for patients that have CF caused by nonsense mutations, alarge subset of CFTR mutation Class I, that cause the production ofa truncated CFTR protein [124]. One readthrough agent that hadbeen given particular attention is Ataluren, a readthrough agent thathas been shown to be effective in nonsense mutation Duchennemuscular dystrophy (nmDMD) and is currently being used to treatspecific patients with nmDMD [125]. However, Phase III trialsshowed no significant difference in mean relative change in FEV1,or sweat chloride concentrations, when comparing Ataluren toplacebo for the treatment of CF resulting from nonsense mutations,and clinical development was subsequently halted [126,127].Another readthrough agent known as ELX-02 demonstrated that itwas able to produce readthrough of PTCs whilst preserving thefidelity of native stop codons (NSCs) in preclinical studies [128]. Itis currently in Phase II clinical trials in CF patients with G542Xnonsense mutations (NCT04126473).
ENaC as an alternative targetThere is also potential to target other channels that contribute
to the pathogenesis of CF. Due to the heavy role that ENaC plays inthe dehydration of ASL in CF, there has been a focus on the potentialfor ENaC as a therapeutic target, for which there are no currenttherapeutics. Theoretically, the therapeutic inhibition of ENaC canreduce the hyperabsorption of sodium ions seen in CF, thereforerehydrating the ASL [129]. A variety of strategies can potentiallybe used to target ENaC. One established strategy is to simplydirectly inhibit ENaC, for which particular attention is being givento BI 1265162, a highly potent ENaC inhibitor that has shownefficacy in preclinical testing. Phase I clinical trials alsodemonstrated that the molecule was safe and well tolerated. It iscurrently the only ENaC inhibitor in Phase II clinical trials, in whichit must now demonstrate clinical efficacy [130].
Another strategy is to inhibit channel activating proteases (CAP)which increase ENaC activation in CF and therefore contribute tosodium hyperabsorption [131]. Camostat was a CAP inhibitorinitially used to provide proof of concept that CAP inhibition canbe used to attenuate ENaC function [132]. This has prompted thedevelopment of further compounds which may have the potentialof replicating this effect. The two key inhibitors of ENaC-activatingCAPs in development are QUB-TL1 and NAP858, both of whichhave been shown to improve ASL height and mucociliary clearancein preclinical studies. These compounds are only in pre-clinicaldevelopment and their efficacy in vivo cannot be attested to [133].
Attention has also been given to the therapeutic potential of aprotein called Short Palate Lung and Nasal Epithelial Clone 1(SPLUNC1). SPLUNC1 is secreted by the airway epithelium andacts an autocrine inhibitor of ENaC, a process which has thepotential to be exploited [134]. SPX-101 is a key compound thatwas tested as a mimetic of SPLUNC1 as an attempt to replicateSPLUNC1’s ENaC-inhibitory effects [135]. Preclinical studies
showed that SPX-101 acts to internalise all of ENaC’s subunits,leading to its inhibition [136]. Phase I trials on SPX-101 seemed toshow that the compound was well tolerated and did not havesystemic effects [137]. However, no further development on thecompound is currently being undertaken and no other SPLUNC1mimetics are currently in development [138]. Despite this, this isan area of inquiry that is relatively novel and therefore may haveuntapped potential.
Other lines of inquiry are looking into how ENaC productionitself could be curtailed. One method to achieve this involves theusage of antisense oligonucleotides (ASOs). These have been shownto be efficacious in decreasing levels of mRNA that encode ENaC’ssubunits, even in the presence of mucus, and reversing CF-likesymptoms in mouse models [139]. The only antisense therapeuticfor CF in development is IONIS-ENaC-2.5Rx, which finished PhaseI trials in June 2020 (NCT03647228). It was demonstrated to causea mean 55.6% decrease in ENaC mRNA expression at a dose of75mg in healthy patients, although full results are yet to bepublished [140]. As an alternative to ASOs, small interfering RNA(siRNA) can be delivered to the lung’s epithelial cells. In pre-clinical studies, these siRNAs have demonstrated efficacy inreducing ENaC mRNA levels, resulting in a decrease in the numberof ENaC channels [141]. The key siRNA-based therapeutic indevelopment is ARO-ENaC, which is currently in Phase I clinicaltrials (NCT04375514).
Gene delivery approachesIn contrast to a mutation specific approach, genetic
manipulation has the potential to treat CF patients with mutationsin any class. This strategy involves introducing the correct copiesof CFTR DNA into the epithelial cells in the airways [142]. Thereare two components that are required for this. The first is a normalcopy of the CFTR gene, along with the required regulatoryconstructs, and the second is a transfer agent capable of efficienttransfection.
The biggest challenge with this therapy will be how best todeliver the genetic material to the target cells. Lung cell turnoverand the immune response have prevented many proposed vectorsfrom delivering the CFTR gene into the epithelial cells [143,144].Focus was previously placed on viral approaches such asadenoviruses, adeno-associated viruses and Sendai virus, but thesehave proved ineffective due to the inefficient transduction of theCFTR gene [145]. Lentiviruses look more favourable, as they haveshown sufficient capacity for a CFTR expression cassette andgreater transducing capabilities [146]. Additionally, unlikeadenoviral vectors, lentiviral vectors display low immunogenicityand are more amenable to repeated dosing [147]. In individuals withsevere lung disease who may not respond to existing prescribedCFTR modulators, such as those with nonsense mutations, lentiviralvectors may offer certain advantages. However, lentiviruses do notnaturally possess the surface proteins capable of recognisingreceptors on respiratory epithelia. To get around this, the UK CFGene Therapy Consortium has created a simian immunodeficiencyvirus (SIV) pseudotyped with F and HN envelope proteins takenfrom a Sendai virus [148]. Currently, the Consortium is trying todesign a Phase I/IIa trial using nasal epithelium as a surrogate organ,which will allow for easy monitoring of gene expression and safety.As well as the lungs, CFTR is expressed in other organs and virusesmay have potential in targeting these. This is because viruses canonly deliver DNA to specific cell types. The subsequent positiveeffects in nutritional and metabolic requirements are likely to reduceclinical problems and significantly improve quality of life.
More recently, attention has shifted towards non-viral vectors.
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 56

65MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
The most promising has been a formulation of Plasmid DNAexpressing CFTR (pGM169) complexed with cationic liposome(GL67A). This biological agent was the first non-viral based genetherapy to undergo a clinical trial to detect functional changes.Following 12 monthly nebulised doses of PGM169/GL67A, therewas a mild yet significant increase in ppFEV1 of 3.7% (0.1-7.3%,95% Confidence Intervals; p<0.05) and the therapy was generallywell tolerated [149]. This is only a modest increase, especially whencompared to other new drugs which show equal or better clinicaloutcomes [64-68,72-74,76-79]. It is therefore unlikely that theformulation will be suitable for use without further improvement inefficacy. In addition to this, increasing the frequency or dosage of thistreatment could be explored, along with the addition of a CFTRpotentiator. There were no treatment attributable adverse events seen,which could encourage the introduction of more potent vectors.
One of the main obstacles to the successful delivery of the DNAis the thick and tenacious mucus seen in CF, which acts as a barrieragainst penetration by exogenous molecules [150]. The answer tothis problem may lie with compressing DNA into small, densestructures called nanoparticles (NPs) [151,152]. NPs, due to theirsize, can feasibly be utilised to overcome this obstacle as they areless likely to be hindered by the mucus mesh. To further enhancepenetration, NPs can be coated with the electrostatically neutralmolecules like polyethylene glycol (PEG) to reduce electrostaticinteractions with mucins. They can also be coated in mucolytics,agents that cleave mucin fibres, to enhance mucus penetration [153].This ultimately results in a greater amount of the DNA reaching thetarget epithelial cells, enhancing the efficacy and viability of genetherapy [154].
mRNA-based therapyAnother new proposal is MRT5005. This is designed to restore
CFTR function by delivering correct copies of CFTR-encodedmRNA, via a nebuliser, to the lung epithelial cells. It is the firstclinical stage mRNA product candidate developed to treat allpatients regardless of their underlying genetic mutation, includingthose with limited or no CFTR protein. A Phase I/II trial is nowunderway [155], with interim data of the first single ascending dosephase having been published [156]. Twelve Participants, eleven ofwhom had at least one copy of F508del mutation, were split intofour groups receiving different dosages (8, 16, and 24 mg) with onegroup receiving a placebo. In the eight-day period after dosing, theplacebo group and 8 mg dose group showed no markedimprovement in ppFEV1. In the 16 mg dose group, the meanmaximum increase from baseline was 15.7% (5.8% StandardDeviation), with two participants in this group on a CFTRmodulator during this period. In the 24 mg dose group, one patientexperienced a maximum ppFEV1 increase of 21.4%, whilst twopatients did not show any significant increase from their baseline.
CRISPR/Cas9 gene editingCRISPR/Cas-9 based genome editing is a recent discovery with
potential for correcting mutations in the CFTR gene [157]. Cas9 isa natural nuclease used for accurate DNA editing. It achieves thisby complexing with a guide RNA (gRNA) that is specific to thetarget DNA, localising to the targeted DNA sequence, and thenintroducing a doubled-strand break (DSB) at the targeted site. Thisthen activates the DNA DSB repair processes known asnonhomologous end-joining (NHEJ) and homology-directed repair(HDR), the latter of which most commonly utilises homologousrecombination [158]. Donor DNA can then be provided, and this is
used to repair the DSB, resulting in transgenic DNA [159].Designing and testing gRNA has been met with high success ratesand this technology has shown great promise for editing the humangenome to treat CF [160].
Induced pluripotent stem cells with a CFTR mutation have beencorrected using the CRISPR/Cas9 approach [161]. Stem cell nicheshave been described within the lungs, so it could be possible toobtain these cells from patients and correct the CFTR mutations,before reinserting them back into their environmental niches [157].Alternatively, viral and non-viral vehicles could be used fordelivering CRISPR/Cas9 into pulmonary epithelial cells, althoughtransfection issues will have to be overcome.
A new tool in CRISPR technology has been the developmentof Cpf1, also known as Cas12a. This differs from Cas9 as Cpf1gRNA is shorter and requires only one single gRNA molecule,compared to Cas9 that requires two gRNAs [162]. This makes iteasier to synthesise gRNA in vitro and package it into vectors. Cpf1also cuts DNA to leave ‘sticky ends’, which allows DNA insertionto be more controllable and easier to work with, unlike Cas9 whichleaves ‘blunt’ ends [163]. This method has shown great success inother genetic conditions such as Duchenne muscular dystrophy,where Zhang et al. successfully corrected the faulty gene in bothmouse models and cells derived from affected patients [164]. Mauleet al. provided proof of concept for the use of Cas12a in editingCFTR mutations. A minigene model was used to demonstrate thatCas12a could be utilised to effectively repair two mutations in theCFTR gene that result in splicing defects. Primary airway epithelialcells were also used to validate the efficacy of Cas12a as deliveredby a lentiviral vector [165].
Using intravenous administration for delivery is not preferentialas vectors will reach the alveoli, an area devoted for gas exchange,and not the surface epithelium of the bronchial tree, where theCFTR protein is more frequently expressed [166]. Therefore,inhaled deliveries are viewed as a suitable strategy of deliveringthese vectors.
ConclusionBy managing the symptoms with established therapies, CF
patients are living longer than ever before, and with the approval ofCFTR modulators, this is only likely to increase. At this moment,several new treatments are being evaluated through clinical trials,which aim to improve lung function by directly interacting withCFTR or by altering its downstream effects. These may give rise toa new generation of therapies which reduce the symptomaticproblems that are frequently seen amongst sufferers.
Gene manipulating techniques and new molecular targets arealso being explored. The use of genome editing using CRISPR/Cas9technology has great potential, although it is still in the early stagesof development, with obstacles in deliverance still needing to beovercome. There should also be more attention drawn to otherorgans and glands expressing CFTR mutations, as this will have vastnutritional and metabolic benefits if targeted successfully. Overall,there has been significant progress in the treatment of cystic fibrosisby attempting to restore the airways to a natural phenotype, eitherthrough restoring the function of existing CFTR proteins, modifyingepithelial cells to produce normal CFTR, or by targeting alternativechannels.
AcknowledgementsWe would like to acknowledge Katie Jaques and William Secrett
for proof-reading and editing.
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 57

66MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
AbbreviationsCF: cystic fibrosis; CFTR: cystic fibrosis transmembrane conductance regulator; NBD: nucleotide binding domain; ENaC: epithelial sodium channel; PNEC: pulmonary neuroendocrine cells; ASL: airway surface liquid; PCL: periciliary layer; ML: mucus layer; IRT: immunoreactive trypsinogen; NPD: nasal potential difference; FEV1: forced expiratory volume in 1 second; FEF: forced expiratory flow; FVC: forced vital capacity; ppFEV1: percent predicted forced expiratory volume in one second; ICS: inhaled corticosteroids; PTC: premature termination codon; TR: translational readthrough; nmDMD: nonsense mutation Duchenne muscular dystrophy; NSC: native stop codons; CAP: channel activating proteases; SPLUNC1: short palate lung and nasal epithelial clone 1; ASO: antisense oligonucleotides; siRNA: small interfering RNA; SIV: simian immunodeficiency virus; NP: nanoparticle; PEG: polyethylene glycol;gRNA: guide RNA; DSB: doubled-strand break; NHEJ: nonhomologous end-joining; HDR: homology-directed repair.
References1. Kreda SM, Davis CW, Rose MC. CFTR, mucins, and mucus
obstruction in cystic fibrosis. Cold Spring Harb Perspect Med2012;2:a009589.
2. Filkins LM, O'Toole GA. Cystic fibrosis lung infections:Polymicrobial, complex, and hard to treat. PLoS Pathog2015;11:e1005258.
3. Lyczak JB, Cannon CL, Pier GB. Lung infections associatedwith cystic fibrosis. Clin Microbiol Rev 2002;15:194-222.
4. Keogh RH, Szczesniak R, Taylor-Robinson D, Bilton D. Up-to-date and projected estimates of survival for people withcystic fibrosis using baseline characteristics: A longitudinalstudy using UK patient registry data. J Cyst Fibros2018;17:218–27.
5. European Cystic Fibrosis Society Patient Registry. Databasefor CF information in 35 participating countries. Availablefrom: https://www.ecfs.eu/ecfspr
6. US CF Foundation Registry. Annual Reports for detailedinformation on CF Care and treatment outcomes. Availablefrom: https://www.cff.org/Research/Researcher-Resources/Patient-Registry/
7. Australian Cystic Fibrosis Data Registry. Annual Reports forHealth outcomes and information. Available from:https://www.cysticfibrosis.org.au/dataregistry
8. Mirtajani SB, Farnia P, Hassanzad M, Ghanavi J, Farnia P,Velayati AA. Geographical distribution of cystic fibrosis; Thepast 70 years of data analyzis. Biomed Biotech Res J2017;1:105-12.
9. ECFS Patient Registry Annual Data Report 2017. PDF
Available from: https://www.ecfs.eu/sites/default/files/general-content-images/working-groups/ecfs-patient-registry/ECFSPR_Report2017_v1.3.pdf
10. Burgel PR, Bellis G, Olesen HV, Viviani L, Zolin A, Blasi F,et al. Future trends in cystic fibrosis demography in 34European countries. Eur Respir J 2015;46:133-41.
11. Lao O, Andrés AM, Mateu E, Bertranpetit J, Calafell F. Spatialpatterns of cystic fibrosis mutation spectra in Europeanpopulations. Eur J Hum Genet 2003;11:385-94.
12. Kosorok MR, Wei WH, Farrell PM. The incidence of cysticfibrosis. Stat Med 1996;15:449-62.
13. US Cystic Fibrosis Foundation. Registry Annual Data Report2018. Available from: https://www.cff.org/Research/Researcher-Resources/Patient-Registry/2018-Patient-Registry-Annual-Data-Report.pdf
14. Davies JC, Geddes DM, Alton EW. Gene therapy for cysticfibrosis. J Gene Med 2001;3:409–17.
15. Elborn JS. Cystic fibrosis. Lancet 2016;388:2519–31.16. Ma J, Zhao J, Drumm ML, Xie J, Davis PB. Function of the R
domain in the cystic fibrosis transmembrane conductanceregulator chloride channel. J Biol Chem 1997;272:28133-141.
17. Tang L, Fatehi M, Linsdell P. Mechanism of direct bicarbonatetransport by the CFTR anion channel. J Cyst Fibros2009;8:115-21.
18. Ehre C, Ridley C, Thornton DJ. Cystic fibrosis: an inheriteddisease affecting mucin-producing organs. Int J Biochem CellBiol 2014;52:136-45.
19. Mall MA, Hartl D. CFTR: cystic fibrosis and beyond. EurRespir J 2014;44:1042-054.
20. Cutting GR. Cystic fibrosis genetics: from molecularunderstanding to clinical application. Nat Rev Genet2015;16:45-56.
21. Tam A, Wadsworth S, Dorscheid D, Man SF, Sin DD. Theairway epithelium: more than just a structural barrier. Ther AdvRespir Dis 2011;5:255-73.
22. Montoro DT, Haber AL, Biton M, Vinarsky V, Lin B, BirketSE, et al. A revised airway epithelial hierarchy includes CFTR-expressing ionocytes. Nature 2018;560:319-324.
23. Moore PJ, Tarran R. The epithelial sodium channel (ENaC) asa therapeutic target for cystic fibrosis lung disease. Expert OpinTher Targets 2018;22:687-701.
24. Saint-Criq V, Gray MA. Role of CFTR in epithelial physiology.Cell Mol Life Sci 2017;74:93-115.
25. Derichs N, Jin BJ, Song Y, Finkbeiner WE, Verkman AS.Hyperviscous airway periciliary and mucous liquid layers incystic fibrosis measured by confocal fluorescencephotobleaching. FASEB J 2011;25:2325-32.
26. Haq IJ, Gray MA, Garnett JP, Ward C, Brodli M. Airwaysurface liquid homeostasis in cystic fibrosis: pathophysiologyand therapeutic targets. Thorax 2016;71:284-7.
27. Hanukoglu I, Boggula VR, Vaknine H, Sharma S, Kleyman T,Hanukoglu A. Expression of epithelial sodium channel (ENaC)and CFTR in the human epidermis and epidermal appendages.Histochem Cell Biol 2017;147:733-48.
28. Al Sinani S, Al-Mulaabed S, Al Naamani K, Sultan R. Cysticfibrosis liver disease: Know more. Oman Med J 2019;34:482-9.
29. de Souza DAS, Faucz FR, Pereira-Ferrari L, Sotomaior VS,Raskin Sl. Congenital bilateral absence of the vas deferens asan atypical form of cystic fibrosis: Reproductive implicationsand genetic counseling. Andrology 2018;6:127-35.
30. Cystic Fibrosis Mutation Database Statistics [Internet].CFMDB statistics. Accessed: October 2020. Available from:http://www.genet.sickkids.on.ca/StatisticsPage.html
31. Karimi N, Pour AB, Alibakhshi R, Almasi S. Haplotypeanalysis of the CFTR gene on normal and mutant CFTR genes.
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 58

67MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
Mutat Res 2020;821:11170832. Castellani C, Cuppens H, Macek M Jr, Cassiman JJ, Kerem E,
Durie P, et al. Consensus on the use and interpretation of cysticfibrosis mutation analysis in clinical practice. J Cyst Fibros2008;7:179-96.
33. Fraser-Pitt D, O’Neil D. Cystic fibrosis-a multiorgan proteinmisfolding disease. Future Sci OA 2015;1:FSO57.
34. Castellani C, Massie J. Newborn screening and carrierscreening for cystic fibrosis: alternative or complementary? EurRespir J 2014;43:20-3.
35. Farrell PM, Rosenstein BJ, White TB, Accurso FJ, CastellaniC, Cutting GR, et al. Guidelines for diagnosis of cystic fibrosisin newborn through older adults: Cystic Fibrosis FoundationReport. J Pediatr 2008;153:S4-14.
36. Mishra A, Greaves R, Massie J. The relevance of sweat testingfor the diagnosis of cystic fibrosis in the genomic era. ClinBiochem Rev 2005;26:135–53.
37. Shaw J, Scotchman E, Chandler N, et al.PREIMPLANTATION GENETIC TESTING: Non-invasiveprenatal testing for aneuploidy, copy-number variants andsingle-gene disorders. Reproduction 2020;160:A1-A11.
38. Rowe SM, Clancy JP, Wilschanski M. Nasal potentialdifference measurements to assess CFTR ion channel activity.Methods Mol Biol 2011;741:69-86.
39. Long JM, Fauset-Jones J, Dixon MJ, Worthington-Riley D,Sharma V, Patel L, et al. Annual review hospital visits forpatients with cystic fibrosis. J R Soc Med 2001;94(s40):S12–6.
40. Kamal N, Surana P, Koh C. Liver disease in patients with cysticfibrosis. Curr Opin Gastroenterol 2018;34:146-51.
41. Bishay L, Sawicki G. Strategies to optimize treatmentadherence in adolescent patients with cystic fibrosis. AdolescHealth Med Ther 2016;7:117-24.
42. McVean RJ, Orr A, Webb AK, Bradbury A, Kay L, Philips E,et al. Treatment of urinary incontinence in cystic fibrosis. JCyst Fibros 2003;2:171-6.
43. Agent P, Parrott H. Inhaled therapy in cystic fibrosis: agents,devices and regimens. Breathe (Sheff) 2015;11:110-8.
44. Scherer TA, Spengler CM, Owassapian D, Imhof E, BuotellierU. Respiratory muscle endurance training in chronicobstructive pulmonary disease: impact on exercise capacity,dyspnea, and quality of life. Am J Respir Crit Care Med2000;162:1709-14.
45. Button BM, Button B. Structure and function of the mucusclearance system of the lung. Cold Spring Harb Perspect Med2013;3:a009720.
46. Mauch RM, Kmit AH, Marson FA, Levy CE, Barros-Filho A,Ribeiro JD. Association of growth and nutritional parameterswith pulmonary function in cystic fibrosis: a literature review.Rev Paul Pediatr 2016;34:503-9.
47. Lai HJ, Shoff SM. Classification of malnutrition in cysticfibrosis: implications for evaluating and benchmarking clinicalpractice performance. Am J Clin Nutr 2008;88:161-6.
48. Cohen-Cymberknoh M, Shoseyov D, Kerem E. Managingcystic fibrosis: strategies that increase life expectancy andimprove quality of life. Am J Respir Crit Care Med2011;183:1463-71.
49. Parsons HG, Beaudry P, Dumas A, Pencharz PB. Energy needsand growth in children with cystic fibrosis. J PediatrGastroenterol Nutr 1983;2:44-9.
50. Quittner AL, Goldbeck L, Abbott J, Duff A, Lambrecht P, SoléA, et al. Prevalence of depression and anxiety in patients withcystic fibrosis and parent caregivers: Results of TheInternational Depression Epidemiological Study across ninecountries. Thorax 2014;69:1090-7.
51. Quittner AL, Abbott J, Georgiopoulos AM, Goldbeck L, Smith
B, Hempstead SE, et al. International Committee on mentalhealth in cystic Fibrosis: Cystic fibrosis Foundation andEuropean cystic fibrosis Society consensus statements forscreening and treating depression and anxiety. Thorax2016;71:26-34.
52. Martin A, Rief W, Klaiberg A, Braehler E. Validity of the briefpatient health questionnaire mood scale (PHQ-9) in the generalpopulation. Gen Hosp Psychiatry 2006;28:71–7.
53. Dierker LC, Albano AM, Clarke GN, Heimberg RG, KendallPC, Merikangas KR, et al. Screening for anxiety anddepression in early adolescence. J Am Acad Child AdolescPsychiatry 2001;40:929-36.
54. Eisenberg D, Gollust SE, Golberstein E, Hefner JL. Prevalenceand correlates of depression, anxiety, and suicidality amonguniversity students. Am J Orthopsychiatry 2007;77:534-42.
55. National Institute for Health and Care Excellence (NICE).Cystic fibrosis: diagnosis and management – NICE guideline[NG78]. Available from: https://www.nice.org.uk/guidance/ng78/chapter/recommendations
56. Elkins MR, Bye PT. Mechanisms and applications ofhypertonic saline. J R Soc Med 2011;104:S2-5.
57. Ratjen F, Davis SD, Stanojevic S, Kronmal RA, HinckleyStukovsky KD, Jorgensen N, et al. Inhaled hypertonic salinein preschool children with cystic fibrosis (SHIP): a multicentre,randomised, double-blind, placebo-controlled trial. LancetRespir Med 2019;7:802-9.
58. Pressler T. Review of recombinant human deoxyribonuclease(rhDNase) in the management of patients with cystic fibrosis.Biol Targets Ther 2008;2:611.
59. Suri R, Metcalfe C, Lees B, Grieve R, Flather M, Normand C,et al. Comparison of hypertonic saline and alternate-day ordaily recombinant human deoxyribonuclease in children withcystic fibrosis: a randomised trial. Lancet 2001;358:1316-21.
60. Suri R, Grieve R, Normand C, Metcalfe C, Thompson S, WallisC, Bush A. Effects of hypertonic saline, alternate day and dailyrhDNase on healthcare use, costs and outcomes in childrenwith cystic fibrosis. Thorax 2002;57:841-6.
61. King M, Dasgupta B, Tomkiewicz RP, Brown NE. Rheologyof cystic fibrosis sputum after in vitro treatment withhypertonic saline alone and in combination with recombinanthuman deoxyribonuclease I. Am J Respir Crit Care Med1997;156:173-7.
62. Flume PA, Aitken ML, Bilton D, Agent P, Charlton B, ForsterE, et al. Optimising inhaled mannitol for cystic fibrosis in anadult population. Breathe Sheff Engl 2015;11:39-48.
63. Trapnell BC. Inhaled dry powder mannitol: a solution for cysticfibrosis. Am J Respir Crit Care Med 2012;185:596-8.
64. Moss RB, Flume PA, Elborn JS, Cooke J, Rowe SM, McColleySA, et al. Efficacy and safety of ivacaftor in patients with cysticfibrosis who have an arg117his-CFTR mutation: a double-blind, randomised controlled trial. Lancet Respir Med2015;3:524-33.
65. De Boeck K, Munck A, Walker S, Faro A, Hiatt P, GilmartinG, et al. Efficacy and safety of ivacaftor in patients with cysticfibrosis and a non-G551D gating mutation. J Cyst Fibros2014;13:674-80.
66. Davies JC, Wainwright CE, Canny GJ, Chilvers MA,Howenstine MS, Munck A, et al. Efficacy and safety ofivacaftor in patients aged 6 to 11 years with cystic fibrosis witha G551D mutation. Am J Respir Crit Care Med 2013;187:1219-25.
67. McKone EF, Borowitz D, Devinek P, Griese M, Konstan MW,Wainwright C, et al. Long-term safety and efficacy of ivacaftorin patients with cystic fibrosis who have the Gly551Asp-CFTRmutation: a phase 3, open-label extension study (PERSIST).Lancet Respir Med 2014;2:902-10.
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 59

68MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
68. Ramsey BW, Davies J, McElvaney NG, Tullis E, Bell SC,Dřevínek P, et al. A CFTR potentiator in patients with cysticfibrosis and the G551D mutation. N Engl J Med 2011;365:1663-72.
69. McNamara JJ, McColley SA, Marigowda G, Liu F, Tian S,Owen CA, et al. Safety, pharmacokinetics andpharmacodynamics of lumacaftor and ivacaftor combinationtherapy in children aged 2-5 years with cystic fibrosishomozygous for F508del-CFTR: ah open-label phase 3 study.Lancet Respir Med 2019;7:325-35.
70. Milla CE, Ratjen F, Marigowda G, Liu F, Waltz D, RosenfeldM, et al. Lumacaftor/ivacaftor in patients aged 6-11 years withcystic fibrosis and homozygous for F508del-CFTR. Am JRespir Crit Care Med 2017;195:912-20.
71. Taylor-Cousar JL, Jain M, Barto TL, Haddad T, Atkinson J,Tian S, et al. Lumacaftor/ivacaftor in patients with cysticfibrosis and advanced lung disease homozygous for F508del-CFTR. J Cyst Fibros 2018;17:228-35.
72. Elborn JS, Ramsey BW, Boyle MP, Konstan MW, Huang W,Marigowda G, et al. Efficacy and safety of lumacaftor/ivacaftorcombination therapy in patients with cystic fibrosishomozygous for phe508del CFTR by pulmonary functionsubgroup: a pooled analysis. Lancet Respir Med 2016;4:617-26.
73. Ratjen F, Hug C, Marigowda G, Tian S, Huang X, StanojevicS, et al. Efficacy and safety of lumacaftor and ivacaftor inpatients aged 6-11 with cystic fibrosis homozygous forF508del-CFTR: a randomized, placebo-controlled phase 3 trial.Lancet Respir Med 2017;5:557-67.
74. Konstan MW, McKone EF, Moss RB, Marigowda G, Tian S,Waltz D, et al. Assessment of safety and efficacy of long-termtreatment with combination lumacaftor and ivacaftor therapyin patients with cystic fibrosis homozygous for the F508del-CFTR mutation (PROGRESS): a phase 3, extension study.Lancet Res Med 2017;5:107-18.
75. Walker S, Glume P, McNamara J, Solomon M, Chilvers M,Chmiel J, et al. A phase 3 study of tezacaftor in combinationwith ivacaftor in children aged 6 through 11 years with cysticfibrosis. J Cyst Fibros 2019:18:708-13.
76. Taylor-Cousar JL, Munck A, McKone EF, van der Ent CK,Moeller A, Simard C, et al. Tezacaftor-Ivacaftor in patients withcystic fibrosis homozygous for Phe508del. N Eng J Med2017;377:2013-23.
77. Rowe SM, Daines C, Ringshausen FC, Kerem E, Wilson J,Tullis E, et al. Tezacaftor-Ivacaftor in residual-functionheterozygotes with cystic fibrosis. N Eng J Med2017;377:2024-34.
78. Middleton PG, Mall MA, Drevínek P, Lands LC, McKone EF,Polineni D, et al. Elexacaftor-tezacaftor-ivacaftor for cysticfibrosis with a single phe508del allele. N Eng J Med2019;381:1809-19.
79. Heijerman HGM, McKone EF, Downey DG, Van Braeckel E,Rowe SM, Tullis E, et al. Efficacy and safety of the elexacaftorplus tezacaftor plus ivacaftor combination regimen in peoplewith cystic fibrosis homozygous for the F508del mutation: adouble-blind, randomised, phase 3 trial. Lancet 2019;394:1940-8.
80. Csanády L, Töröcsik B. Cystic fibrosis drug ivacaftorstimulates CFTR channels at picomolar concentrations. Elife2019;8:e46450.
81. Guigui S, Wang J, Cohen RI. The use of ivacaftor in CFTRmutations resulting in residual functioning protein. Resp MedCase Rep 2016;19:193-5.
82. Carlile GW, Yang Q, Matthes E, Liao J, Radinovic S,Miyamoto, et al. A novel triple combination of pharmacologicalchaperones improves F508del-CFTR correction. Sci Rep
2018;8:11404.83. Clancy JP. Rapid therapeutic advances in CFTR modulator
science. Pediatr Pulmonol 2018;53:S4-11.84. Ridley K, Condren M. Elexacaftor-Tezacaftor-Ivacaftor: The
first triple-combination cystic fibrosis transmembraneconductance regulator modulating therapy. J Pediatr PharmacolTher 2020;25:192-7.
85. LiverTox: Clinical and Research Information on Drug-InducedLiver Injury [Internet]. Bethesda (MD): National Institute ofDiabetes and Digestive and Kidney Diseases; 2012. CysticFibrosis Agents. Available from: https://www.ncbi. nlm.nih.gov/books/NBK547889/
86. Chaudary N. Triplet CFTR modulators: future prospects fortreatment of cystic fibrosis. Ther Clin Risk Manag2018;14:2375-2383.
87. Vertex Pharmaceuticals, Inc. Kalydeco [Product Monograph]2012. Laval, Quebec: Available from: https://pi.vrtx.com/files/uspi_ivacaftor.pdf
88. Vertex Pharmaceuticals, Inc. Orkambi [Product Monograph]2015. Laval, Quebec: Available from: https://pi.vrtx.com/files/uspi_lumacaftor_ivacaftor.pdf
89. Vertex Pharmaceuticals, Inc. Symdeko [Product Monograph]2018. Laval, Quebec: Available from: https://pi.vrtx.com/files/uspi_tezacaftor_ivacaftor.pdf
90. Vertex Pharmaceuticals, Inc. Trikafta [Product Monograph]2019. Laval, Quebec: Available from: https://pi.vrtx.com/files/uspi_elexacaftor_tezacaftor_ivacaftor.pdf
91. European Medicine Agency. Pending EC decision for Ivacaftor– Committee for Medicinal Products for Human Use (CHMP).Available from: https://www.ema.europa.eu/en/ medicines/human/summaries-opinion/kalydeco-3#key-facts-section
92. European Medicine Agency. Pending EC decision for Symkevi– Committee for Medicinal Products for Human Use (CHMP).Available from: https://www.ema.europa.eu/en/ medicines/human/summaries-opinion/symkevi-0
93. Flume PA, O’Sullivan BP, Robinson KA, Goss CH, MogayzelPJ Jr, Willey-Courand B, et al. Cystic fibrosis pulmonaryguidelines: chronic medications for maintenance of lung health.Am J Respir Crit Care Med 2007;176:957-69.
94. De Rose V, Molloy K, Gohy S, Pilette C, Greene CM. Airwayepithelium dysfunction in cystic fibrosis and COPD. MediatorsInflamm 2018;2018:1309746.
95. Balfour-Lynn IM, Elborn JS. "CF asthma": what is it and whatdo we do about it? Thorax 2002;57:742-8.
96. Dahl M, Tybjærg-Hansen A, Lange P, Nordestgaard BG.DeltaF508 heterozygosity in cystic fibrosis and susceptibilityto asthma. Lancet 1998;351:1911-3. Erratum in Lancet1998;352:1230.
97. Schroeder SA, Gaughan DM, Swift M. Protection againstbronchial asthma by CFTR delta F508 mutation: aheterozygote advantage in cystic fibrosis. Nat Med 1995;1:703-5.
98. Halfhide C, Evans HJ, Couriel J. Inhaled bronchodilators forcystic fibrosis. Cochrane Database Syst Rev 2005:CD003428.
99. Smith S, Edwards CT. Long-acting inhaled bronchodilators forcystic fibrosis. Cochrane Database Syst Rev 2017:CD012102.
100. Barry PJ, Flume PA. Bronchodilators in cystic fibrosis: acritical analysis. Expert Rev Respir Med 2017;11:13-20.
101. Eckrich J, Zissler UM, Serve F, Leutz P, Smaczny C, Schmitt-Grohé S, et al. Airway inflammation in mild cystic fibrosis. JCyst Fibros 2017;16:107-15.
102. Konstantinos Katsoulis K, Kostikas K, Kontakiotis T.Techniques for assessing small airways function: Possibleapplications in asthma and COPD. Respir Med 2016;119:e2-9.
103. Scichilone N, Contoli M, Paleari D, Pirina P, Rossi A,
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 60

69MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
Sanguinetti CM, et al. Assessing and accessing the smallairways; implications for asthma management. PulmPharmacol Ther 2013;26:172-9.
104. Balfour-Lynn IM, Welch K. Inhaled corticosteroids for cysticfibrosis. Cochrane Database Syst Rev 2016:CD001915.
105. De Boeck K, De Baets F, Malfroot A, Desager K, Mouchet F,Proesmans M. Do inhaled corticosteroids impair long-termgrowth in prepubertal cystic fibrosis patients? Eur J Pediatr2007;166:23-8.
106. Latorre M, Novelli F, Vagheggini B, Braido F, Papi A, SanduzziA, et al. Differences in the efficacy and safety among inhaledcorticosteroids (ICS)/long-acting beta2-agonists (LABA)combinations in the treatment of chronic obstructive pulmonarydisease (COPD): Role of ICS. Pulm Pharmacol Ther2015;30:44-50.
107. Lynch JP III, Sayah DM, Belperio JA, Weigt SS. Lungtransplantation for cystic fibrosis: results, indications,complications, and controversies. Semin Respir Crit Care Med2015;36:299-320.
108. Meachery G, De Soyza A, Nicholson A, Parry G, Hasan A,Tocewicz K, et al. Outcomes of lung transplantation for cysticfibrosis in a large UK cohort. Thorax 2008;63:725-31.
109. Davies JC, Alton EWF, Bush A. Cystic fibrosis. BMJ2007;335:1255-9.
110. Coburn B, Wang PW, Diaz Caballero J, Clark ST, Brahma V,Donaldson S, et al. Lung microbiota across age and diseasestage in cystic fibrosis. Sci Rep 2015;5:10241.
111. Huang YJ, LiPuma JJ. The microbiome in cystic fibrosis. ClinChest Med 2016;37:59-67.
112. Bhagirath AY, Li Y, Somayajula D, Dadashi M, Badr S, DuanK. Cystic fibrosis lung environment and Pseudomonasaeruginosa infection. BMC Pulm Med 2016;16:174.
113. Coutinho HDM, Falcao-Silva VS, Goncalves GF. Pulmonarybacterial pathogens in cystic fibrosis patients and antibiotictherapy: a tool for the health workers. Int Arch Med 2008;1:24.
114. Brooke JS. Stenotrophomonas maltophilia: An emerging globalopportunistic pathogen. Clin Microbiol Rev 2012;25:2–41.
115. Tamma PD, Cosgrove SE, Maragakis LL. Combination therapyfor treatment of infections with gram-negative bacteria. ClinMicrobiol Rev 2012;25:450-70.
116. Peloquin CA, Berning SE, Nitta AT, Simone PM, Goble M,Huitt GA, et al. Aminoglycoside toxicity: daily versus thrice-weekly dosing for treatment of mycobacterial diseases. ClinInfect Dis 2004;38:1538-44.
117. Petkova M, Gesson C, De Vos S, Conrath K, Corveleyn S,Geller D, et al. safety, tolerability and pharmacokinetics of anovel CFTR potentiator GLPG3067 in healthy volunteers.Galapagos Biotech 2017 Poster. Available at:https://www.glpg.com/docs/view/59fc5ef4102ec-en
118. Singh AK, Fan Y, Balut C, Alani S, Manelli AM, Swenses AM,et al. Biological characterization of F508delCFTR proteinprocessing by the CFTR corrector ABBV-2222/GLPG2222. JPharmacol Exp Ther 2020;372:107-18.
119. Lopes-Pacheco M. CFTR modulators: The changing face ofcystic fibrosis in the era of precision medicine. FrontPharmacol 2020;10:1662.
120. Proteostasis Therapeautics, Inc. Recent positive phase 2 and exvivo organoid study data support initiation of MORE andCHOICES trials in 2020 proteostatis therapeutics regulatoryupdate 2020. Available from: https://www.prnewswire.com/news-releases/proteostasis-therapeutics-regulatory-update-following-scientific-advice-meeting-with-mhra-300985498.html
121. Molinski SV, Ahmadi S, Ip W, Ouyang H, Villella A, Miller JP,et al. Orkambi® and amplifier co-therapy improves functionfrom a rare CFTR mutation in gene-edited cells and patient
tissue. EMBO Mol Med 2017;9:1224-43.122. Matos AM, Matos P. Combination therapy in Phe508del CFTR:
how many will be enough? J Lung Health Dis 2018;2:9-16. 123. Dabrowski M, Bukowy-Bieryllo Z, Zietkiewicz E. Advances
in therapeutic use of a drug-stimulated translationalreadthrough of premature termination codons. Mol Med2018;24:25.
124. Wilschanski M. Class 1 CF Mutations. Front Pharmacol 2012;3:117.
125. Mercuri E, Muntoni F, Osorio AN, Tulinius M, Buccella F,Morgenroth LP, et al. Safety and effectiveness of ataluren:comparison of results from the STRIDE Registry and CINRGDMD Natural History Study. J Comp Eff Res 2020;9:341-60.
126. Abidi NZ, Haq IJ, Gardner AI, Brodlie M. Ataluren in cysticfibrosis: development, clinical studies and where are we now?Expert Opin Pharmacother 2017;18:1363-71.
127. Aslam AA, Higgins C, Sinha IP, et al. Ataluren and similarcompounds (specific therapies for premature termination codonclass I mutations) for cystic fibrosis. Cochrane Database SystcRev2017;1:CD012040. rawford DK, Alroy I, Sharpe N,Goddeeris MM, Williams G. Premature versus native stopcodon read-through by ELX-02. J Pharmacol Exp Ther2020;374:264-72.
128. Moore PJ, Robert Tarran R. The epithelial sodium channel(ENaC) as a therapeutic target for cystic fibrosis lung disease.Expert Opin Ther Targets 2018;22:8:687-701.
129. Mall MA. ENaC inhibition in cystic fibrosis: potential role inthe new era of CFTR modulator therapies. Eur Respir J2020;2000946.
130. Reihill JA, Walker B, Hamilton RA, Ferguson TE, Elborn JS,Stutts MJ, et al. Inhibition of protease-epithelial sodiumchannel signaling improves mucociliary function in cysticfibrosis airways. Am J Respir Crit Care Med 2016;194:701-10.
131. Rowe SM, Reeves G, Hathorne H, Solomon GM, Abbi S,Renard D, et al. Reduced sodium transport with nasaladministration of the prostasin inhibitor camostat in subjectswith cystic fibrosis. Chest 2013;144:200-7.
132. Strug LJ, Stephenson AL, Panjwani N, Harris A. Recentadvances in developing therapeutics for cystic fibrosis. HumMolr Genet 2018;27:R173–86.
133. Hobbs CA, Blanchard MG, Alijevic O, Da Tan C, KellenbergeS, Bencharit S, et al. Identification of the SPLUNC1 ENaC-inhibitory domain yields novel strategies to treat sodiumhyperabsorption in cystic fibrosis airway epithelial cultures.Am J Physiol Lung Cell Mol Physiol 2014;1;306:L708.
134. Lennox A, Myerburg MM. SPX-101 is a promising and novelnebulized ENaC inhibitor. Am J Respir Crit Care Med2017;196:671-2.
135. Scott DW, Walker MP, Sesma J, Wu B, Stuhlmiller TJ, SabaterJR, et al. SPX-101 is a novel epithelial sodium channel-targetedtherapeutic for cystic fibrosis that restores mucus transport. AmJ Respir Crit Care Med 2017;196:734-44.
136. Couroux P, Farias P, Rizvi L, Griffin K, Hudson C, CrowderT, et al. First clinical trials of novel ENaC targeting therapy,SPX-101, in healthy volunteers and adults with cystic fibrosis.Pulm Pharmacol Ther 2019;58:101819.
137. Cystic Fibrosis Foundation. Drug Development Pipeline: SPX-101. Available from: https://www.cff.org/Trials/Pipeline/details/10128/SPX-101
138. Crosby JR, Zhao C, Jiang C, Bai D, Katz M, Greenlee S, et al.Inhaled ENaC antisense oligonucleotide ameliorates cysticfibrosis-like lung disease in mice. J Cyst Fibros 2017;16:671-80.
139. Ionis Pharmaceuticals, Inc. Ionis' inhaled antisense medicinedemonstrates potential as a novel treatment for cystic fibrosis.Ionis Pharmaceuticals, Inc. Update 2020. Available from:
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 61

70MRM
Multidisciplinary Respiratory Medicine 2020; 15:690 - R. Jaques et al.
https://ir.ionispharma.com/news-releases/news-release-details/c-o-r-r-e-c-t-i-o-n-ionis-pharmaceuticals-inc-0
140. Manunta MDI, Tagalakis AD, Attwood M, Aldossary AM,Barnes JL, Munye MM, et al. Delivery of ENaC siRNA toepithelial cells mediated by a targeted nanocomplex: atherapeutic strategy for cystic fibrosis. Sci Rep 2017;7:700.
141. Burney TJ, Davies JC. Gene therapy for the treatment of cysticfibrosis. Appl Clin Genet 2012;5:29-36.
142. Karda R, Buckley SMK, Waddington SN. Gene therapy withadeno-associated virus for cystic fibrosis. Am J Respir CritCare Med 2016;193:234–6.
143. Donnelley M, Parsons DW. Gene therapy for cystic fibrosislung disease: overcoming the barriers to translation to theclinic. Front Pharmacol 2018;9,1381.
144. Griesenbach U, Inoue M, Hasegawa M, Alton EWFW. Viralvectors for cystic fibrosis gene therapy: What does the futurehold? Dove Press 2010;2:159-71.
145. Naldini L, Blomer U, Gage FH, Trono D, Verma IM. Efficienttransfer, integration, and sustained long-term expression of thetransgene in adult rat brains injected with a lentiviral vector.Proc Natl Acad Sci USA 1996;93:11382-8.
146. Griesenbach U, Inoue M, Meng C, Farley R, Chan M, NewmanNK, et al. Assessment of F/HN-pseudotyped lentivirus as aclinically relevant vector for lung gene therapy. Am J RespirCrit Care Med 2012;186,846-56.
147. Moradali MF, Ghods S, Rehm BH. Pseudomonas aeruginosalifestyle: a paradigm for adaptation, survival, and persistence.Front Cell Infect Microbiol 2017;7:39.
148. Alton E, Armstrong DK, Ashby D, Bayfield KJ, Bilton D,Bloomfield EVm et al. Repeated nebulisation of non-viralCFTR gene therapy in patients with cystic fibrosis: arandomised, double-blind, placebo-controlled, phase 2b trial.Lancet Respir Med 2015;3-:684–91.
149. Lai SK, Wang YY, Hanes J. Mucus-penetrating nanoparticlesfor drug and gene delivery to mucosal tissues. Adv Drug DelivRev 2009;61:158-71.
150. Suk JS, Lai SK, Boylan NJ, Dawson MR, Boyle MP, Hanes J.Rapid transport of muco-inert nanoparticles in cystic fibrosissputum treated with N-acetyl cysteine. Nanomedicine (Lond)2011;6:365-75.
151. Lababidi N, Sigal V, Koenneke A, Schwarzkopf K, Manz A,Schneider M . Microfluidics as tool to prepare size-tunablePLGA nanoparticles with high curcumin encapsulation forefficient mucus penetration. Beilstein J Nanotechnol2019;10:2280-2293.
152. Ong V, Mei V, Cao L, Lee K, Chung EJ. Nanomedicine for
cystic fibrosis. SLAS Technol 2019;24:169-80.153. Velino C, Carella F, Adamiano A, Sanguinetti N, Vitali A,
Catalucci D, et al. Nanomedicine approaches for the pulmonarytreatment of cystic fibrosis. Front Bioeng Biotechnol2019;7:406.
154. Sahu I, Haque AKMA, Weidensee B, Weinmann P, KormannMSD. Recent developments in mRNA-based proteinsupplementation therapy to target lung diseases. Mol Ther2019;27:803-23.
155. Translate Bio, Inc. Translate Bio announces interim resultsfrom phase 1/2 clinical trial of MRT5005 in patients with cysticfibrosis, 2019. Available from: http://investors. translate.bio/node/7101/pdf
156. Marangi M, Pistritto G. Innovative therapeutic strategies forcystic fibrosis: moving forward to CRISPR technique. FrontPharmacol 2018;9:396.
157. Hsu PD, Lander ES, Zhang F. Development and applicationsof CRISPR-Cas9 for genome engineering. Cell 2014;157:1262-78.
158. Hille F, Charpentier E. CRISPR-Cas: biology, mechanisms andrelevance. Philos Trans R Soc Lond B Biol Sci 2016;371:20150496.
159. Hodges CA, Conlon RA. Delivering on the promise of geneediting for cystic fibrosis. Genes Dis 2019;6:97–108.
160. Suzuki S, Chosa K, Lee A, Yezzi M, Kai H, Gruenert D.Seamless correction by donor DNA of a class I CFTR mutationfacilitated by a double nicking CRISPR/Cas9 in CF-iPSCs.Mol Therapy 2016;24:S51
161. Park J, Bae S. Cpf1-database: web-based genome-wide guideRNA library design for gene knockout screens using CRISPR-Cpf1. Bioinformatics 2017;34:1077-79.
162. Ledford H. Alternative CRISPR system could improve genomeediting. Nature 2015;526:17.
163. Zhang Y, Long C, Li H, McAnally JR, Baskin KK, Shelton JMet al. CRISPR-Cpf1 correction of muscular dystrophymutations in human cardiomyocytes and mice. Sci Adv2017;3:e1602814.
164. Maule G, Casini A, Montagna C, Ramalho AS, De Boeck K,Debyser Z, et al. Allele specific repair of splicing mutations incystic fibrosis through AsCas12a genome editing. NatCommun 2019;10:3556. Author Correction in: Nat Commun2020;11:5457.
165. Katz MG, Fargnoli AS, Bridges CR. Myocardial gene transfer:routes and devices for regulation of transgene expression bymodulation of cellular permeability. Hum Gene Ther2013;24:375-92.
Received for publication: 16 June 2020. Accepted for publication: 6 November 2020.This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0).©Copyright: the Author(s), 2020Licensee PAGEPress, ItalyMultidisciplinary Respiratory Medicine 2020; 15:690doi:10.4081/mrm.2020.690
MRM_01 review.qxp_Hrev_master 26/11/20 09:27 Pagina 62

71MRM
What makes flunisolide different among inhaled corticosteroids used for nebulization: a close look at the role of aqueous solubility Ahmad KantarPediatric Asthma and Cough Center, Istituti Ospedalieri Bergamaschi, Bergamo, Italy
Evidence-based management of bronchial asthma and wheezing in children and adults recommends the employmentof inhaled corticosteroids (ICSs). Difficulty in using some inhalation devices for ICS delivery, such as pressurizedmetered-dose and dry-powder inhalers, is common among young children and in the elderly, and for that reason, theyare replaced with nebulizers. We reviewed comparative studies that evaluated funisolide with other ICSs currentlyavailable on the market, including beclomethasone dipropionate, fluticasone propionate, and budesonide. Moreover,we assessed the physicochemical properties of these ICSs in determining drug fate in the lung. Data indicate that theflunisolide output in respirable particles by any type of pneumatic nebulizer (traditional, open breath or breath-enhanced) is superior to the output of other ICSs. This is principally attributed to the higher water solubility of flu-nisolide. Furthermore, in vivo simulation studies demonstrate that the intersubject variability of the inhaled doseamong asthmatic children was much greater for suspensions of fluticasone propionate and beclomethasone dipropi-onate than for those of flunisolide. The physicochemical properties and pharmacokinetic profile of flunisolide favorits employment in nebulization.
Key words: Inhaled corticosteroids; flunisolide; nebulization; drug output; particle size.
AB
STR
ACT
Correspondence: Ahmad Kantar, Pediatric Asthma and Cough Center, Istituti Ospedalieri Bergamaschi, Gruppo OspedalieriSan Donato, Via Forlanini 15, 24036 Ponte San Pietro (BG), Italy. E-mail: [email protected]
Contributions: AK is the only author that contributed to the preparation of this manuscript.
Conflict of interest: AK received lecture fees from Valeas, Menarini, Chiesi, Italchimici, Merck Sharp & Dohme, Sanofi andNovartis (Italy). AK is a member of the Editorial Board of Multidisciplinary Respiratory Medicine.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Availability of data and materials: Qualified researchers may request access to study documents and data reported in this manuscript.
Ethics approval and consent to participate: Not applicable.
REVIEW
®Multidisciplinary Respiratory Medicine 2021; volume 16:719
MRM_02 review.qxp_Hrev_master 15/01/21 12:38 Pagina 1

72MRM
Multidisciplinary Respiratory Medicine 2021; 16:719 - A. Kantar
IntroductionInhaled corticosteroids (ICSs) are anti-inflammatory drugs that
are largely indicated in the first-line management of subjects withvarious respiratory diseases. Among ICSs, four are currentlyaccessible on the market for nebulization: budesonide (BUD), flu-ticasone propionate (FP), flunisolide (FLU), and beclomethasonedipropionate (BDP). These ICSs possess different chemical struc-tures and distinct physicochemical properties that form the basis oftheir different pharmacokinetic (PK) and pharmacodynamic (PD)properties. To better comprehend the safety and efficacy of theseICSs, it is important to examine the fate of drug molecules in thebody during nebulization and inhalation. ICSs exhibit therapeuticeffects after deposition and distribution in pulmonary tissues at thesite of action. Depending on the size of the particles, the deliverydevice used as well as the patient respiratory pattern, distinct frac-tions of the ICS are deposited in the upper respiratory tract(oropharynx), central airways (bronchi and bronchiole), or deeppulmonary tissues (alveoli) [1,2]. Deposition of the ICS in thelungs allows the targeted delivery and induction of the desiredtherapeutic effects. Guidelines for the treatment of respiratory dis-eases as well as for aerosol therapy do not provide detailed guid-ance on the choice of the most appropriate device in a particularclinical setting [3]. Therefore, according to local practices andaccessibility, there is great inconsistency among countries in theemployment of different devices for administering aerosol therapy[4,5]. An outstanding tendency in pediatric aerosol therapy is theliberal decline in the choice of nebulizers in favor of pressurizedmetered dose inhalers (pMDIs) and dry-powder inhalers (DPIs);nevertheless, over 70 countries worldwide still use nebulization todeliver ICSs for both children and adults for asthma and chronicobstructive pulmonary disease [6]. In this article, we review ourexisting knowledge of ICSs for nebulization with a focus on FLUby responding to frequently asked questions regarding why thisdrug is the most appropriate for nebulization.
Are all ICSs born equally?ICSs are synthetic corticosteroid analogs created from basic
steroid molecules. In 1972, BDP became the first corticosteroid tobe developed as a therapeutic aerosol [7]. Formulations of ICSproducts share numerous properties to enhance local potency andminimize systemic exposure. Specific ICS molecules have distinc-tive properties that affect their formulation and use. In terms ofpharmacology, they differ in physicochemical properties that dic-tate their PK and PD characteristics. In the clinical setting, balanc-ing favorable and unfavorable properties presents challenges indetermining whether a molecule offers significant advantages ineither efficacy or safety.
In general, the PK and PD properties of an ICS dictate its effi-cacy and safety; nevertheless, because there are several character-istics of individual agents that influence these properties, the glob-al effect is sometimes uncertain and often controversial [1]. Theoptimal ICS would be an agent that displays significant local andsustained effects in the airways with negligible systemic effectsowing to limited bioavailability and prompt systemic clearance [8].
The preferred drug would exert selective topical effects withminimal systemic absorption or rapid inactivation after absorption[9]. Several PK and PD features of ICSs have been identified ashaving a role in their overall efficacy and safety profile. Due to thenumerous properties that concomitantly influence ICS action andsafety, it is difficult to determine the precise effect of any distinctproperty. For example, the receptor binding affinity of available
ICS agents varies 10–100-fold, and oral bioavailability varies 20-fold. Although the protein binding of available agents is relativelyconsistent, ranging from 71% to 99%, lipophilicity varies over100-fold, and half-lives generally vary between 5 to 14 h. Perhapsbecause of the similarities or the numerous differences amongmolecules, no single agent seems to have significant advantages orconfers additional risks over any other in clinical practice.Moreover, the behavior of the therapeutic formulation duringdelivery can vary between devices.
The exponential relationship between in vitro glucocorticoidreceptor binding affinity and therapeutic dose for ICS is evidencethat more potent molecules can be administered at much lowerdoses to achieve similar clinical efficacy. Furthermore, the struc-tural features of ICS that give rise to more potent molecules alsodrive lower systemic exposure, and together these factors canimprove the therapeutic index. Relative glucocorticoid receptorbinding affinity relative to dexamethasone (affinity of 100) is 2989for fluticasone furoate (FF) DPI, 2100 for mometasone furoateDPI, 1775 for FP DPI, 53 for BDP pMDI, 1345 for beclometha-sone 17-monopropionate, 935 for BUD, 190 for FLU pMDI and 12for oral prednisolone [7].
Enhanced inhaled ICS potency leads to greater lipophilicity,slower dissolution and pulmonary absorption of inhaled drug par-ticles with longer retention times in the airways. This also resultsin a longer duration of action and permits less frequent dosing.Once absorbed, more potent inhaled corticosteroids have higherplasma protein binding, lower unbound fractions in the plasma andlarger volumes of distribution. These molecules are also good sub-strates for drug-metabolizing enzymes and have high systemicclearance, high first-pass metabolism and low oral bioavailabilityof the swallowed dose [7].
A prolonged pulmonary residence time is apparent when theelimination half-life following inhaled administration is signifi-cantly longer than found following intravenous administration.This tendency has been noted for the more lipophilic inhaled cor-ticosteroids. The main consequence of this appears to be a longerduration of action rather than greater efficacy per se, with the cor-ticosteroid with the longest lung retention time (such as FF) beingsuitable for once daily dosing, and those with shorter lung reten-tion times (such as FP) requiring twice daily dosing regimens [7].
An advantage of ICSs is their high potency, which allowsoccupancy of a glucocorticoid receptor at a lower dose than that ofless potent agents. The potency of topical corticosteroids variesamong different agents, and characterizing the relative potency ofavailable therapies is challenging and imperfect. For example, FPis marketed in all pMDI, DPI and nebulization formulas and has ahigh therapeutic index and efficacy [10,11]. For several years, FPhas been employed successfully for all severities of asthma and hasproven to be well tolerated. No clinically important systemiceffects are reported for its normal therapeutic dose range [10-13].By contrast, pharmacokinetic studies have suggested hypothalam-ic-pituitary-adrenal suppression with higher doses. However, thosehigh-dose studies involve normal volunteers [14-19] or subjectswith mild asthma who were receiving inappropriately high doses,well in excess of those normally recommended to obtain diseasecontrol [20,21]. In patients with moderate or severe asthma requir-ing higher doses of ICSs, factors such as airflow obstruction andventilation-perfusion mismatch could alter drug deposition in thelung and alter systemic absorption. Brutshe et al. [22] demonstrat-ed through a double-blind, randomized, crossover study that thesystemic availability of FP is substantially less in patients withmoderate to severe asthma than in healthy controls. There is littleinformation on factors that influence the systemic bioavailabilityof ICSs, especially for drugs with minimum oral bioavailability,such as FP, in which drug delivery and pulmonary deposition have
MRM_02 review.qxp_Hrev_master 15/01/21 12:38 Pagina 2

73MRM
Multidisciplinary Respiratory Medicine 2021; 16:719 - A. Kantar
key roles. Almost all FP present in the systemic circulation isabsorbed in an unchanged active form via the lungs [23,24]. Oncepresent in the bloodstream, this drug remains potent, with a highbinding affinity to the extrapulmonary corticosteroid receptor.Until now, despite the characteristic differences that arise in theairways in asthma, it had been assumed that drug deposition, pul-monary drug absorption, and systemic effects measured in healthyindividuals could predict outcomes in people with asthma. Asthmais, however, characterized by reversible and nonhomogeneous air-flow obstruction, leading to ventilation-perfusion mismatch.Several studies, some by using three-dimensional imaging tech-niques [25], have shown that the uniformity of deposition in thelungs is greater in healthy individuals than in patients with airwaydisease. It is suggested that the narrowing of airways in asthmaresults in reduced penetration of the drug particles and subsequent-ly increased deposition in the central rather than in peripheral air-ways. In asthma, inflammation definitely involves large airways,but histopathological evidence has clearly shown that the inflam-mation involves small airways as well. Drug particles that aredeposited in the conducting airways are more subject to mucocil-iary clearance than those deposited in the alveoli, which are com-pletely absorbed. Consequently, for a drug with a relatively slowdissolution rate in the lung, such as FP [24], drug deposited in theairways is more likely to be removed from the lung by mucociliaryclearance and then swallowed, leading to a lower degree of sys-temic exposure than that seen in healthy subjects.
How is a nebulizer chosen?There has been substantial progress in drug delivery technolo-
gy over the last decades. New devices that are outstandinglyimproved in delivering respirable drugs to the airways have beenpromoted. Since the introduction of pMDIs, there has been a trendof progressive decrease in the use of traditional nebulizers in favorof smart and more portable devices. Nevertheless, in various coun-tries, traditional nebulizers continue to be commonly employed,somewhat for historical and economic motives.
Nebulizers allow drug delivery to very young children andelderly adults through passive inhalation and are less reliant onpatient synchronization, cooperation and acceptance. Delivery ofICSs by nebulization represents a valid and alternative method ofaerosol therapy for infants and elderly adults, who are unable orrefuse to use pMDIs with spacers or DPIs.
In a review article, Melani indicated that nebulizers may beconsidered as an effective alternative to inhalers for deliveringICSs and can be recommended to asthmatic and COPD subjectswho are unwilling or unable to use inhalers [6]. Results of thereview showed that nebulized BDP, FP and FLU are effective alter-natives to nebulized BUD in asthma and COPD. From a pharma-ceutical perspective, a primary advantage of nebulizers is the useof water-based formulations, which are relatively simple to preparefor aqueous soluble drugs making them less expensive comparedwith the processing required for pMDI and DPI aerosol formula-tions.
The cheapest and most commonly used devices are pneumaticnebulizers characterized from old atomizers by their means of pre-venting delivery and recycling of large particles [26]. Baffles orimpaction sites are assembled to block the primary spray emergingfrom the atomizer jet. Cycling of the fluid and baffling control thevelocity, size and volume flow of the delivered drug, permitting therelease of a cloud of respirable particles [27].
New technical innovations for nebulizers have drasticallyreduced drug wastage and increased output. Innovative categoriesof nebulizers have been promoted, among which are the open vent,
breath-enhanced open vent, breath-activated devices and meshnebulizers [28,29]. Although ultrasonic nebulizers are more effi-cient and compact than jet nebulizers, they are entirely inadequateto deliver ICS suspensions.
Vibrating mesh technology is an alternative innovation to jetnebulizers. Numerous recent electronic nebulizers that employ avibrating mesh or plate with multiple holes to generate monodis-persing, fine-particle, low-velocity aerosol clouds are beingreleased in the market and are increasingly used to deliver specificdrugs. These devices are highly efficient in delivering aerosols tothe peripheral airways, such that the nominal dose of drugs to beaerosolized could be substantially reduced. Moreover, the residualvolume of the formulation left in these devices after nebulizationis negligible, leading to prominent improvements in the cost-effec-tiveness of administering costly medications. Since these devicesnebulize at a faster rate than conventional jet or ultrasonic nebuliz-ers, the duration of each treatment is reduced. These devices effi-ciently nebulize solutions and suspensions and have overcomemany of the limitations associated with forerunning nebulizers,and they offer the adaptability to adjust the aerosol characteristicsaccording to the clinical need for which they are employed [30].
Jet and ultrasonic nebulizers entered the market severaldecades before mesh devices. Therefore, the mesh nebulizer hashad to compete for a share of the pre-existing market since thelaunch of the first mesh nebulizer in 1993. In an ever-growing neb-ulizer market, perhaps as a consequence of lower prices and theincrease in respiratory diseases worldwide, the jet nebulizer con-tinues to dominate the market in several countries. Moreover,many pharmaceuticals have been developed and packaged for jetnebulizer use; thus, mesh nebulizers are not designed as an imme-diate substitution for jet nebulizers.
Drug formulations can have a key impact on the aerosol outputrate and the output of drug in respirable particles. Suspensions witha high surface tension, such as BUD, can decrease the performanceof vibrating mesh nebulizers regarding the output rate and theinhaled mass. Moreover, obstruction of mesh holes during nebu-lization has been reported with drug suspensions [30].
The usage of mesh nebulizers to deliver ICS is scarce due tothe limited number of studies in this field and the lack of clinicalexperience. In addition, their higher cost remains a limiting factorin their expansion in the market. Moreover, even if the best nebu-lizer is selected based on cost, ease of use, and clinical efficacy, acritical factor is the patient’s ability to use the device.
A wide range of micro- and nanoemulsion-based formulationshave been proposed for oral, topical and parenteral administration,which, by mimicking the physicochemical properties of solutions,“solubilize” poorly water-soluble drugs in an aqueous formulation,indicating potential for use in drug delivery systems [31,32].Nanoemulsions, because of their high solubilizing and drug protec-tion features have the potential to deliver active drug compoundsto the lungs. With the advantage of solution-like physicochemicalproperties of nanoemulsions, it is hypothesized that nanoemulsionsperform as a solution when nebulized and will demonstrateimproved aerosolization performance over suspension formula-tions. Amani et al. evaluated in vitro performance of a nebulizednanoemulsion-based formulation containing budesonide withrespect to budesonide suspension formulation delivered from a jetand mesh nebulizers. A smaller MMAD with improved aerosoloutput was observed in the nanoemulsion preparations [31].
Mixing nebulizable medications for simultaneous inhalation isan obvious way to reduce the duration of nebulization and is acommonly used procedure. The problem of compatibility ofinhalation admixtures received little attention and has been sporad-ically researched. Even if the admixtures are physically and chem-ically compatible in the nebulizer, the aerodynamic behavior and
MRM_02 review.qxp_Hrev_master 15/01/21 12:38 Pagina 3

74MRM
Multidisciplinary Respiratory Medicine 2021; 16:719 - A. Kantar
out-put may be influenced by mixing [33]. Melani [34] evaluatedthe effect of mixinig BUD or BDP with albuterol and ipratropiumbromide from an open-vent and breath-enhanced nebulizer.Results demonstrated that mixing did not substantially reduced therespirable mass of the examined drugs. In our previously study,using a conventional and an open-vent nebulizer, we have demon-strated that mixing FLU or BDP with salbutamol did not decreasedrug out or modified particle size [35]. Droplet and particle sizedistribution in the delivered aerosol and incompatibilities arisingduring nebulization of the admixtures should be addressed for eachmixture before prescription.
Prescribing the most appropriate nebulized therapy should takeinto consideration the available drug formulations, combinations,and devices, as well as the patients’ pulmonary function, skills, andpreferences [36].
There are many challenges with the use of inhalers and nebu-lizers, and no one device suits all patients [37]. Each nebulizer hasdifferent technical properties that dictate its performance.Knowledge of nebulization procedures and of the behavior of adrug during nebulization is essential for drug-device matching.Patient factors to consider in device selection include disease sta-tus, physical and mental capabilities, past experiences withinhalers, preferences and satisfaction with their inhalers [37].However, several drawbacks have been reported with using nebu-lizers including considerable heterodispersity in concertation ofdelivered drug, device preparation, possible contamination,lengthy treatment time, drug waste or high cost. In a nation-widesurvey Melani et al. demonstrated that the use of nebulizers in Italyis widespread, with either occasional or regular use for upper orlower airways diseases. However, the use and maintenance ofhome nebulizers were heterogenous and not optimal [38].
Why is flunisolide appropriate for nebulization?The physicochemical features of the preparation and its com-
portment during the process of nebulization are essential aspects tobe considered when prescribing inhalation therapy. Not all drugsare appropriate for the nebulization process. Water solubility andformulation viscosity govern the quantity of drug delivered in par-ticles able to reach the therapeutic target. If a drug solution in a neb-ulizer chamber is homogeneously distributed, each aerosol dropletis likely to have a relatively uniform drug concentration during neb-ulization. Nevertheless, water in the drug formulation evaporatesduring nebulization, and consequently, the drug concentration in thedelivered cloud will increase [39,40]. Corticosteroids available fornebulization, depending on their water solubility, may either be insolution, such as FLU, or in suspension, such as FP, BUD and BDP.Högger and Rohdewald rated the water solubility of ICSs at 37°Cas 140 μg/ml for FLU, 16 μg/ml for BUD, 0.14 μg/mL for FP and0.13 μg/mL for BDP [41]. Most solution formulations are a mixtureof the active drug and a diluent forming a continuous phase. On theother hand, suspensions form two phases become challenging tonebulize. The high solubility of FLU yields a drug advantage innebulization. Studies comparing the output of different ICSs fromthe same nebulizer are still lacking. In our previous studies, the out-put from two nebulizers (traditional and open vent) for FLU, BDP,and BUD delivery was investigated using a multistage liquidimpinger method [42-44]. The data showed that FLU output wassuperior to that of the other two drugs. Moreover, the mass medianaerodynamic diameter (MMAD) of nebulized FLU was smallerthan that of BDP and BUD. The drug output in respirable particles<4.3 µm as a percentage of the nominal doses of FLU, BUD andBDP were 25.7%, 14.7%, and 11.5%, respectively, from the tradi-tional nebulizer and 24.7%, 11.6%, and 7.2%, respectively, from theopen-vent nebulizer (Figure 1).
Figure 1. Output in particles <6.8 µm and <4.3 µm as percentages of the nominal dose of nebulized flunisolide (nominal dose 600 µg);red bars, budesonide (nominal dose 500 µg); blue bars; beclomethasone DP (nominal dose 800 µg); green bars, from two different neb-ulizers. The jet nebulizers used were Nebula (a conventional pneumatic device, Markos-Mefar, Bovezzo, Italy) and BimboNeb (an open-vent nebulizer, Markos-Mefar) (data from references 47-49).
MRM_02 review.qxp_Hrev_master 15/01/21 12:38 Pagina 4

75MRM
Multidisciplinary Respiratory Medicine 2021; 16:719 - A. Kantar
In another study, we investigated the inhaled doses of threeICSs delivered via nebulization for asthmatic children [45]. Theinteraction of a child with a device has an overwhelming effect onthe inhaled dose. The aim of that study was to investigate whetherchildren with asthma inhale the same ratios of the prescribed dosedelivered by the same nebulizer for FP, BDP and FLU. A ‘breath-enhanced, open vent’ nebulizer (Pari TurboBOY, Germany) wasused, and the following drug formulations were employed: FP sus-pension (500 μg/2 ml nebule) BDP suspension (0.8 mg/2 ml neb-ule) and FLU solution (30 mg/30 ml solution). The children inhaledeach of the drug preparations for 5 min. The results revealed thatthe prescribed dose bears little resemblance to the proportion ofdrug the children actually inhale and that this is largely dependenton the formulation of the drug. Following nebulization, the chil-dren in the study would have inhaled 13% of the prescribed doseof FP, 21% of BDP and 25% of FLU. However, the percentage ofthe dose inhaled by drug particles that were less than 5 μm andtherefore more likely to reach the lungs were only 5% and 8% ofthe prescribed doses of FP and BDP, respectively. Hitherto, theamount of FLU inhaled in particles less than 5 μm was significant-ly greater at 16%. These variances were augmented further whenthe amount of drug contained in particles less than 3 μm was com-pared. Surprisingly, the variation in the quantity of drug inhaledwas larger among children who inhaled the suspensions of BDPand FP than those of FLU. This fact has not been previously report-ed and suggests that drug dispersion in the nebulizer mixture, drugbehavior during nebulization or the child’s breathing patternthrough the nebulizer may have noteworthy effects on the amountof drug delivered from suspensions and that this is not predictable.It is of interest that a currently discontinued preparation of BDPresulted in very little drug exiting the nebulizer in particles smallenough to reach the lower airways [46,47]. and that this was asso-ciated with a poor clinical effect [48,49]. Other factors, such as thechoice of nebulizer, may have a profound effect on the dose of neb-ulized corticosteroids a patient may inhale. For example, in vitrostudies have demonstrated that the dose of budesonide that a 10-year-old is likely to inhale from breath-enhanced, open-vent nebu-lizers is almost four times greater than that from an open-vent neb-ulizer and twice greater than that from a conventional nebulizer[50].
How is nebulized flunisolide handled in the lungs?The target of ICS treatment is to achieve an appropriate anti-
inflammatory outcome in the airways while outstandingly reduc-ing adverse local and systemic effects.
Common means of retaining inhaled drugs in the lungs includetissue entrapment (e.g., water soluble di-bases) and the slow disso-lution of particles of poorly soluble drugs such as corticosteroids
[51]. For compounds with high water solubility, sustained local tis-sue concentration and hence the therapeutic effect is influencedmainly by the extent of tissue binding or tissue entrapment, whichis governed by molecular properties rather than material or formu-lation properties. For slowly dissolving compounds, the extent ofthe therapeutic effect is sensitive to the material properties govern-ing the solubility and/or dissolution rate. This principle has beendemonstrated experimentally: a difference in systemic exposurebetween two formulations with similar aerodynamic particle sizedistributions was found to be consistent with the predicted differ-ence in the dissolution rate [52]. A relationship between dissolutionrate and the rate of detection of drug in the plasma has also beenreported [53]. Dissolution in vivo is influenced not only by theproperties of the drug, such as solubility and specific surface area- which can be controlled and measured in an in vitro setting - butalso by physiological factors, including the composition of airway-lining fluid, permeability of the airway epithelium, and rate of par-ticle clearance, all of which vary between different regions of thelung. For example, epithelial permeability for many compounds(depending upon the molecular properties) is significantly greaterin respiratory districts than in the conducting airways, and perme-ation could conceivably substitute dissolution as the rate limitingstep as the deposition site moves from the peripheral to the centrallung. The causality between the rate of dissolution and the clinicalperformance of an ICS is complex, but differences in the dissolu-tion rate between ICSs with otherwise similar aerosol performance(with potential effects on local and systemic bioavailability anddrug safety) have been demonstrated [54,55].
Sakagami et al. [56] evaluated the dissolution of various res-pirable ICSs in ≤ 5.8 or 6.5 μm particles in a simulated lung liningfluid. Dissolution in 10 ml of the simulated lung lining fluid wasdetermined over time in a Transwell dish. The results demonstratedthat while ICSs with high-to-intermediate solubility [FLU, triam-cinolone acetonide (TAA) and BUD] were capable of first order“sink” and complete dissolution in 6 h, ICSs with poor solubility,including FP (FP, BDP, mometasone furoate, and ciclesonide),resulted in pseudozero-order “non-sink”, slow and limited dissolu-tion. The aerosol dissolution rate constant was well correlated withsolubility. For FP, but not for highly soluble FLU, dissolution waskinetically aerosol mass dependent.
Wiedemann et al. evaluated the aqueous solubility and the rel-ative affinity of some CSs (BUD, TAA, dexamethasone, and FLU)for lung surfactant using a native extract of bovine lung (Survanta)[57]. The aqueous solubility of the drugs at 37°C was 19.6, 35.8,104, and 120 µg/mL, respectively. The quantity of drug dissolvedin Survanta was amplified with solubilization of 0.019, 0.023,0.014, and 0.02 µg of the drug per µg of Survanta. The amount ofsurfactant per kg of body weight was estimated to be between 8-24mg [58]. The residence time of a drug in the lung is reliant on itssolubilization in the surfactant (Table 1).
Table 1. Solubility and dissolution of ICSs in water and in bronchial fluid in vitro.
ICS Water solubility, µg/ml Solubilization in Survanta, Dissolution time (ref 46) a native extract of bovine lung, µg/ml (human bronchial fluid in vitro) (ref 68) (ref 46)
Beclomethasone dipropionate 0.13 - 5 hBeclomethasone 17-propionate 15.5 - -Triamcinolone acetonide 21 35.8 -Budesonide 16 19.6 6 minFlunisolide 140 120 2 minFluticasone 17-propionate 0,14 - 8 h
MRM_02 review.qxp_Hrev_master 15/01/21 12:38 Pagina 5

76MRM
Multidisciplinary Respiratory Medicine 2021; 16:719 - A. Kantar
Pulmonary residence time is governed by the release rate of theinhaled particle, the degree of absorption of the dissolved drugacross the pulmonary membranes and the mucociliary clearance[59]. The mean absorption times are 5-9 hours for FP and 0.3-1.8hours for BUD [18]. The prolonged extracellular pulmonary resi-dence of FP, as indicated by the rather prolonged mean absorptiontime, is a result of its extremely low solubility. The formation ofintracellular ester depots is an alternative mean of protracting pul-monary residence. Long residence times in the extracellular envi-ronment have been estimated for FP and TAA, whereas BUD andFLU tend to fade quickly [53,60]. These properties are correlatedto pulmonary solubility, which seems to be the rate-limiting step inpulmonary absorption [60,61]. Laboratory studies have demon-strated that a substantial portion of BUD undergoes intracellularesterification [61]. Corticosteroids that lack the free C21 hydroxylgroup, such as FP and BDP, do not form free fatty acid esters [62].The reversible esterification leads to the slow release of the activedrug at the targeted site of action [63]. FLU contains a free hydrox-yl group at C21 and can potentially undergo esterification, as itwas demonstrated for ciclesonide and TAA [64]. FLU, TAA, andciclesonide all contain a free hydroxyl group at C21 and can poten-tially undergo esterification. FLU, like BUD, is characterized by abrief pulmonary residence time, and it is assumed that inside thecell, it might be subjected to esterification due to the presence of afree C21 hydroxyl group. The intrapulmonary retention time ofFLU is not known. In a study, we assessed the concentration of flu-nisolide in rat lungs after inhalation using gas chromatography[65]. Our study demonstrated a prolonged retention of inhaledFLU in rat lung tissue. In particular, retention in the lung wouldenhance the therapeutic index, either due to slow dissolution or theability to form esters in the airways. The study demonstrated reten-tion of FLU in rat lungs. This may be attributed to nonspecificbinding processes, esterification, or gradient formation in the cell.
The absorption of drugs from the lungs to the systemic circu-lation is generally rapid, with high bioavailability for compoundswith a wide range of physicochemical properties [66,67]. Differentregions of the lungs are thought to have varying permeabilities todrugs according to their molecular properties, which dictate theirinteraction with the extracellular environment, including the liningfluid composition, cellular type and thickness, the extent anddimensions of intercellular junctions, blood flow, and competingclearance mechanisms. For example, the absorption of a small,hydrophilic molecule in human subjects was greatly enhanced bycoapplying an absorption enhancer for a more peripheral delivery[68]. Although they may be delivered predominately to central orperipheral regions, current inhaled drugs do not exclusively targeta particular region of the lungs, and clinical absorption profiles arecomposites of those of drug deposited and absorbed in differentregions.
ConclusionFLU, which was discovered in 1965 and used initially for neb-
ulization, was approved in the United States in a CFC-pMDI forthe treatment of asthma in 1981. Flunisolide was subsequentlyreformulated with a hydrofluoroalkane propellant. The reformulat-ed flunisolide HFA with an integrated spacer is the most recent ICSproduct for asthma on the market in the United States and is theonly product that combines an extrafine corticosteroid aerosol anda built-in spacer. The physical and chemical properties of FLUfavor its prescription for nebulization. Clinical studies havedemonstrated that nebulized FLU, at the commonly prescribeddosages, is efficient for asthma treatment in infants and that nonlo-cal or systemic side effects have been reported [69].
AcknowledgementsNot applicable
Abbreviations ICS: inhaled corticosteroid;BUD: budesonide;FP fluticasone propionate;FLU: flunisolide;TAA: triamcinolone acetonide; BDP: beclomethasone dipropionate;PK: pharmacokinetic; PD: pharmacodynamic; DPI: dry-powder inhaler;pMDI: pressurized metered dose inhalers; MMAD: mass median aerodynamic diameter.
References1. Derendorf H, Nave R, Drollmann A, Cerasoli F, Wurst W.
Relevance of pharmacokinetics and pharmacodynamics ofinhaled corticosteroids to asthma. Eur Respir J 2006;28:1042-50.
2. Hubner M, Hochhaus G, Derendorf H. Comparative pharma-cology, bioavailability, pharmacokinetics, and pharmacody-namics of inhaled glucocorticosteroids. Immunol Allergy ClinNorth Am 2005;25:469-88.
3. Dolovich MB, Ahrens RC, Hess DR, Anderson P, Dhand R,Rau JL, et al. Device selection and outcomes of aerosol thera-py: evidence- based guidelines: American College of ChestPhysicians/ American College of Asthma, Allergy, andImmunology. Chest 2005;127:335-71.
4. Vermeire P. European trends in inhalation therapy. Eur RespirRev 1994;4:89-91.
5. Lavorini F, Corrigan CJ, Barnes PJ, Dekhuijzen PR, Levy ML,Pedersen S, et al. Retail sales of inhalation devices in Europeancountries: so much for a global policy. Respir Med2011;105:1099-103.
6. Melani AS. Nebulized corticosteroids in asthma and COPD.An Italian appraisal. Respir Care 2012;57:1161-74.
7. Daley-Yates PT. Inhaled corticosteroids: potency, dose equiva-lence and therapeutic index. Br J Clin Pharmacol 2015;80:372-80.
8. Derendorf H, Hochhaus G, Meibohm B, Mo¨llmann H, BarthJ. Pharmacokinetics and pharmacodynamics of inhaled corti-costeroids. J Allergy Clin Immunol 1998;101:S440-6.
9. Lipworth BJ. Clinical pharmacology of corticosteroids inbronchial asthma. Pharamcol Ther 1993;58:173-209.
10. Fabbri L, Burge PS, Croonenborgh L, Warlies F, Weeke B,Ciaccia A, et al. Comparison of fluticasone propionate withbeclomethasone dipropionate in moderate to severe asthmatreated for one year. Thorax 1993;48:817-23.
11. Ayres JG, Bateman ED, Lundback B, Harris TA. High dosefluticasone propionate, 1 mg daily versus fluticasone propi-onate, 2 mg daily, or budesonide, 1.6 mg daily, in patients withchronic severe asthma. Eur Respir J 1995;8:579-86.
12. Agertoft L, Pedersen S. A randomised, double-blind dosereduction study to compare the minimal effective dose ofbudesonide Turbohaler and fluticasone propionate Diskhaler. JAllergy Clin Immunol 1997;99:773-80.
13. Yiallouros PK, Milner AD, Conway E, Honour JW. Adrenal
MRM_02 review.qxp_Hrev_master 15/01/21 12:38 Pagina 6

77MRM
Multidisciplinary Respiratory Medicine 2021; 16:719 - A. Kantar
function and high dose inhaled corticosteroids for asthma.Arch Dis Child 1997;76:405-10.
14. Lönnebo A, Grahnén A, Jansson B, Brundin RM, Ling-Andersson A, Eckernäs SA. An assessment of the systemiceffects of single and repeated doses of inhaled fluticasone pro-pionate and inhaled budesonide in healthy volunteers. Eur JClin Pharmacol 1996;49:459-63.
15. Grahnén A, Eckernäs SA, Brundin RM, Ling-Andersson A. Anassessment of the systemic activity of single doses of inhaledfluticasone propionate in healthy volunteers. Br J ClinPharmacol 1994;38:521-5.
16. Grahnén A, Jansson B, Brundin RM, Ling-Andersson A,Lönnebo A, Johansson M, et al. A dose-response study com-paring suppression of plasma cortisol induced by fluticasonepropionate from Diskhaler and budesonide from Turbohaler.Eur J Clin Pharmacol 1997;52:261-7.
17. Thorsson L, Dahlström K, Edsbäcker A, Källén A, Paulson J,Wirén JE. Pharmacokinetics and systemic effects of inhaledfluticasone propionate in healthy subjects. Br J Clin Pharmacol1997;43:155-61.
18. Boorsma M, Andersson N, Larsson P, Ullman A. Assessmentof the relative systemic potency of inhaled fluticasone andbudesonide. Eur Respir J 1996;9:1427-32.
19. Clark DJ, Grove A, Cargill RI, Lipworth BJ. Comparativeadrenal suppression with inhaled budesonide and fluticasonepropionate in adult asthmatic patients. Thorax 1996;51:262-6.
20. Clark DJ, Lipworth BJ. Adrenal suppression with chronic dos-ing of fluticasone propionate compared with budesonide inadult asthmatic patients. Thorax 1997;52:55–8.
21. Derom E, Van Schoor J, Verhaeghe W, Vincken W, Pauwels R.Systemic effects of inhaled fluticasone propionate and budes-onide in adult patients with asthma. Am J Respir Crit Care Med1999;160:157-61.
22. Brutsche MH, Brutsche IC, Munavvar M, Langley SJ,Masterson CM, Daley-Yates PT, et al. Comparison of pharma-cokinetics and systemic effects of inhaled fluticasone propi-onate in patients with asthma and healthy volunteers: a ran-domised crossover study. Lancet 2000;356:556-61.
23. Möllman H, Wagner M, Meibohm B, Hochhaus G, Barth J,Stöckmann R, et al. Pharmacokinetic and pharmacodynamicevaluation of fluticasone propionate after inhaled administra-tion. Eur J Clin Pharmacol 1998;53:459-67.
24. Yanai M, Hatazawa J, Ojima F, Sasaki H, Itoh M, Ido T.Deposition and clearance of inhaled 18FDG powder in patientswith chronic obstructive pulmonary disease. Eur Respir J1998;11:1342-8.
25. Melchor R, Biddiscombe M, Mak V, Short M, Spiro S. Lungdeposition patterns of directly labelled salbutamol in normalsubjects and in patients with reversible airflow obstruction.Thorax 1993;48:506-11.
26. Niven RW. Atomization and nebulizers. In: Hickey AJ, editor.Inhalation aerosol: Physical and biological basis for therapy.New York: Marcel Dekker; 1996. p. 273-312.
27. O'Callaghan C, Barry PW. The science of nebulised drug deliv-ery. Thorax 1997;52:531-44.
28. Dalby RN, Tiano SL, Hickey AJ. Medical devices for thedelivery of therapeutic aerosols to the lungs. In: Hickey AJ,editor. Inhalation aerosol: Physical and biological basis fortherapy. New York: Marcel Dekker; 1996. p 441-73.
29. Dhand R. Nebulizers that use a vibrating mesh or plate withmultiple apertures to generate aerosol. Respir Care2002;47:1406-146. discussion 1416-8.
30. Fink JB, Simmons R. Nebulization of steroid suspension: an invitro evaluation of the Aeroneb®Go nebulizer and thePari®LC+ nebulizers. Chest 2004;126:816S-7.
31. Amani A, York P, Chrystyn H, Clark BJ. Evaluation of ananoemulsion-based formulation for respiratory delivery ofbudesonide by nebulizers. AAPS Pharm Sci Tech 2010;11:1147-51.
32. Lawrence MJ, Rees GD. Microemulsion-based media as noveldrug delivery systems. Adv Drug Deliv Rev 2000;45:89-121.
33. Kamin W, Schwabe A, Krämer I. Inhalation solutions: whichone are allowed to be mixed? Physico-chemical compatibilityof drug solutions in nebulizers. J Cyst Fibros 2006;5:205-13.
34. Melani AS. Effects on aerosol performance of mixing of eitherbudesonide or beclomethasone dipropionate with albuterol andipratropium bromide. Respir Care 2011;56:319-26.
35. O'Callaghan CL, White JA, Jackson JM, Barry PW, Kantar A.Nebulisation of corticosteroid suspensions and solutions with abeta(2) agonist. J Pharm Pharmacol 2008;60:601-5.
36. Tashkin DP. A review of nebulized drug delivery in COPD. IntJ Chron Obstruct Pulmon Dis 2016;11:2585-96.
37. Pleasants RA, Hess DR. Aerosol delivery devices for obstruc-tive lung diseases. Respir Care 2018;63:708-33.
38. Melani AS, Sestini P, Aiolfi S, Barbato N, Canessa P, DeAngelis G, et al. GENebu Project: home nebulizer use andmaintenance in Italy. Eur Respir J 2001;18:758-63.
39. Wood JA, Wilson RS, Bray C. Changes in salbutamol concen-tration in the reservoir solution of a jet nebulizer. Br J DisChest 1986;80:164-9.
40. McCallion ON, Taylor KM, Thomas M, Taylor AJ.Nebulization of fluids of different physicochemical propertieswith air-jet and ultrasonic nebulizers. Pharm Res 1995;12:1682-8.
41. Högger P, Rohdewald P. Glucocorticoid receptors and flutica-sone propionate. Rev. Contemp Pharmacother 1998;9:501-22.
42. O'Callaghan C, White J, Barry P, Kantar A. Analysis of the out-put of beclomethasone dipropionate from different nebulisers.Riv Ital Pediatr 2000;26:821-4.
43. O'Callaghan C, White J, Jackson J, Barry P, Kantar A. Theoutput of flunisolide from different nebulisers. J PharmPharmacol 2002;54:565-9.
44. O'Callaghan C, White J, Jackson J, Barry PW, Kantar A.Delivery of nebulized budesonide is affected by nebulizer typeand breathing pattern. J Pharm Pharmacol 2005;57:787-90.
45. O'Callaghan C, White JA, Kantar A. Nebulization of corticos-teroids to asthmatic children: large variation in dose inhaled.Respirology 2014;19:276-9.
46. O’Callaghan C. Particle size of beclomethasone dipropionateproduced by two nebulisers and two spacing devices. Thorax1990;45:109-11.
47. Todd GR. Nebulised fluticasone. Thorax 2000;55:346-47.48. Storr J, Lenney CA, Lenney W. Nebulised beclomethasone
dipropionate in preschool asthma. Arch Dis Child 1986;61:270-3.
49. Webb MS, Milner AD, Hiller EJ, Henry RL. Nebulisedbeclomethasone dipropionate suspension. Arch Dis Child1986;61:1108-10.
50. Barry PW, O’Callaghan C. An in vitro analysis of the output ofbudesonide from different nebulizers. J Allergy Clin Immunol1999;104:1168-73.
51. Heyder J, Svartengren MU. Basic principles of particle behav-ior in human respiratory tract. In: Bisgaard H, O'Callaghan C,Smaldone GC, Editors. Drug delivery to the lung. New York:Marcel Dekker; 2002. p. 21-45.
52. Bäckman P, Adelman H, Petersson G, Jones CB. Advances ininhaled technologies: understanding the therapeutic challenge,predicting clinical performance, and designing the optimalinhaled product. Clin Pharmacol Ther 2014;95:509-20.
53. Grainger CI, Saunders M, Buttini F, Telford R, Merolla LL,
MRM_02 review.qxp_Hrev_master 15/01/21 12:38 Pagina 7

78MRM
Multidisciplinary Respiratory Medicine 2021; 16:719 - A. Kantar
Martin GP, et al. Critical characteristics for corticosteroid solu-tion metered dose inhaler bioequivalence. Mol Pharm2012;9:563-9.
54. Riley T, Christopher D, Arp J, Casazza A, Colombani A,Cooper A, et al. Challenges with developing in vitro dissolu-tion tests for orally inhaled products (OIP’s). AAPS Pharm SciTech 2012;13:978-89.
55. Buttini F, Miozzi M, Balducci AC, Royall PG, Colombo P,Brambilla G, et al. Differences in physical chemistry and dis-solution rate of solid particle aerosols from solution inhalers.Int J Pharm 2014;465:42-51.
56. Sakagami M, Li H, Venitz J. In vivo-relevant transwell dish-based dissolution testing for orally inhaled corticosteroid prod-ucts. Pharm Res 2019;36:95.
57. Wiedmann TS, Bhatia R, Wattenberg LW. Drug solubilizationin lung surfactant. J Control Release 2000;65:43-7.
58. Hallman M. Recycling of surfactant: A review of human amni-otic fluid as a source of surfactant for treatment of respiratorydistress syndrome. Rev Perinat Med 1989;6:197-226.
59. Derendorf H, Hochhaus G, Krishnaswami S, Mol̈lmann H.Systemic disposition and effects of inhaled corticosteroids. In:Schleimer RP, O'Byrne PM, Szefler SJ, and Brattsand R, edi-tors. Inhaled steroids in asthma. Optimizing effects in the air-ways. New York: Marcel Dekker; 2002. p. 247-72.
60. Derendorf H, Hochhaus G, Rohatagi S, Möllmann H, Barth J,Sourgens H, et al. Pharmacokinetics of triamcinolone ace-tonide after intravenous, oral, and inhaled administration. JClin Phramacol 1995;35:302-5.
61. Miller-Larsson A, Mattsson H, Hjertberg E, Dahlbäck M,Tunek A, Brattsand R. Reversible fatty acid conjugation of
budesonide: Novel mechanism for prolonged retention of top-ically applied steroid in airway tissue. Drug Metab Dispos1998;26:623-30.
62. Hochberg RB. Biological esterification of Steroids. EndocrRev 1998;19:331-48.
63. Miller-Larsson A, Janssen P, Runstròm A, Brattsand R.Prolonged airway activity and improved selectivity of budes-onide possibly due to esterification. Am J Respir Crit CareMed 2000;162:1455-1461.
64. Kelly HW. Comparative potency and clinical efficacy ofinhaled corticosteroids. Respir Care Clin N Am 1999;5:537-53.
65. Kantar A, Carloni M, Kulkarni N, Fedeli D, Falcioni G.Retention of flunisolide in rat lungs after single inhalation.Europ J inflamm 2012;10:127-31.
66. Mathias NR, Timoszyk J, Stetsko PI, Megill JR, Smith RL.Wall epithelial cells: in vitro/in vivo correlation to predict lungabsorption in rats. J Drug Target 2002;10:31-40.
67. Tronde A, Norden B, Marchner H, Wendel A-K, Lennernas H,Bengtsson UH. Pulmonary absorption rate and bioavailabilityof drugs in vivo in rats: structure-absorption relationships andphysicochemical profiling of inhaled drugs. J Pharm Sci2003;92:1216-33.
68. Bondesson E, Bengtsson T, Nilsson LE, Wollmer P. Effects ofsodium taurocholate on the absorption of inhaled Tc-99m-DTPA. Pharm Res 2006;23:2122-8.
69. Kantar A, Mroueh S, Fiocchi A. A reappraisal of the clinicalefficacy of nebulized flunisolide in pediatric asthma: theItalian experience. Allergy Asthma Proc 2007;28:671-87.
Received for publication: 19 June 2020. Accepted for publication: 15 December 2020.This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0).©Copyright: the Author(s), 2021Licensee PAGEPress, ItalyMultidisciplinary Respiratory Medicine 2021; 16:719doi:10.4081/mrm.2021.719
MRM_02 review.qxp_Hrev_master 15/01/21 12:38 Pagina 8

79MRM
Cardiopulmonary exercise pattern in patients with persistent dyspnoea after recovery from COVID-19Arno Mohr,1 Laura Dannerbeck,1 Tobias J. Lange,2 Michael Pfeifer,1,2 Stefan Blaas,1 Bernd Salzberger,3Florian Hitzenbichler,3 Myriam Koch2
1Center for Pneumology, Donaustauf Hospital, Donaustauf2Department of Internal Medicine 2, University Medical Center, Regensburg3Department of Infection Control and Infectious Diseases, University Medical Center Regensburg, Germany
Cause and mechanisms of persistent dyspnoea after recovery from COVID-19 are not well described. The objective isto describe causal factors for persistent dyspnoea in patients after COVID-19. We examined patients reporting dysp-noea after recovery from COVID-19 by cardiopulmonary exercise testing. After exclusion of patients with pre-existinglung diseases, ten patients (mean age 50±13.1 years) were retrospectively analysed between May 14th and September15th, 2020. On chest computed tomography, five patients showed residual ground glass opacities, and one patientshowed streaky residua. A slight reduction of the mean diffusion capacity of the lung for carbon monoxide was notedin the cohort. Mean peak oxygen uptake was reduced with 1512±232 ml/min (72.7% predicted), while mean peakwork rate was preserved with 131±29 W (92.4% predicted). Mean alveolar-arterial oxygen gradient (AaDO2) at peakexercise was 25.6±11.8 mmHg. Mean value of lactate post exercise was 5.6±1.8 mmol/l. A gap between peak workrate in (92.4% predicted) to peak oxygen uptake (72.3% pred.) was detected in our study cohort. Mean value of lactatepost exercise was high in our study population and even higher (n.s.) compared to the subgroup of patients withreduced peak oxygen uptake and other obvious reason for limitation. Both observations support the hypothesis ofanaerobic metabolism. The main reason for dyspnoea may therefore be muscular.
Key words: CPET; COVID-19; postdischarge dyspnoea; post-COVID-19 syndrome.
AB
STR
ACT
Correspondence: Dr. Myriam Koch, Klinik und Poliklinik für Innere Medizin II, Universitätsklinikum Regensburg, Franz-Josef-Strauß Allee 11, D-93053 Regensburg, Germany. Tel. +49.941/944-0. E-mail: [email protected]
Contributions: All authors made a substantive intellectual contribution, read and approved the final version of the manuscriptand agreed to be accountable for all aspects of the manuscript.
Conflict of interest: LD, MP and MK have nothing to disclose; AM reports grants from Gilead Sciences, outside the submittedwork; TJL reports personal fees from Actelion, personal fees from Janssen-Cilag, personal fees from BMS, personal fees fromMSD, personal fees from Pfizer, personal fees from GSK, personal fees from Acceleron Pharma, outside the submitted work;SB reports personal fees and non-financial support from Roche, personal fees and non-financial support from BoehringerIngelheim, non-financial support from Teva, personal fees and non-financial support from Bayer, non-financial support fromGilead, personal fees and non-financial support from Novartis, personal fees from Merck Serono, non-financial support fromLucane Pharma, non-financial support from Actelion, non-financial support from CSL Behring, non-financial support fromVertex, outside the submitted work; BS reports personal fees from Roche Ag, personal fees from Sanofi, personal fees fromFalk Foundation, outside the submitted work; FH reports grants from Gilead Sciences, personal fees from MSD, outside thesubmitted work.
Funding: The authors received no specific funding for this work.Availability of data and materials: The dataset analysed during the current study is available from the corresponding authorupon reasonable request.
Ethics approval and consent to participate: The retrospective study was approved by the local ethics committee (No. 20-1773-104) at the University of Regensburg.
Consent for publication: Not applicable.
SHORT REPORT
®Multidisciplinary Respiratory Medicine 2021; volume 16:732
MRM_02 short.qxp_Hrev_master 10/02/21 08:53 Pagina 1

80MRM
Multidisciplinary Respiratory Medicine 2021; 16:732 - A. Mohr et al.
IntroductionCOVID-19 has led to more than 2 millions deaths in less than
12 months [1]. Mankind is challenged by this new disease, whichin many aspects and characteristics is different to other respiratoryviral infections [2-4]. Manifestations range from asymptomaticinfection to severe ARDS. Some survivors suffer from symptoms,attributable to ICU care and some show persisting symptomswhich are still unclear [5]. Some patients do not report dyspnoeadespite hypoxemia in severe COVID-19 [2,6]. Interestingly afterrecovery from acute infection with SARS-CoV2 dyspnoea andfatigue are the most frequent symptoms [7-10]. However, the causeand pathophysiologic mechanisms of persistent dyspnoea afterrecovery from COVID-19 are not well described. In this study wesought to analyse our cohort of post COVID-19 patients with per-sistent dyspnoea using a thorough clinical workup including car-diopulmonary exercise testing (CPET).
Methods
Study population, study design and data collectionThe study was conducted at the Centre of Pneumology in
Donaustauf, Germany. The hospital is a quaternary care providerfor pneumology, where patients from the eastern region of Bavariaare seen for specialized care.
All available medical reports from patients, that presented tothe outpatient’s clinic or on Non-ICU ward with persistent symp-toms after recovery from COVID-19 (post-COVID-19) betweenMay 14th and September 15th 2020 were retrospectively analysed.
StatisticsSummary statistics of continuous variables are presented as
mean ± standard deviation. Data were analysed using MicrosoftExcel (version 2016, Redmond, USA) and IBM SPSS (version24.0, IBM, Armonk, USA).
PatientsThe following eligibility criteria were applied: 18 years of age
or older, post COVID-19, still symptomatic with dyspnoea.Patients were excluded from the study if any of the above criteriawas not fulfilled or if no CPET was performed or any other reasonfor dyspnoea became evident. Abnormal spirometry was not astrict exclusion criterion except reflecting an underlying lung dis-ease judged responsible for patient’s dyspnoea.
ExaminationsPatients received a comprehensive assessment of dyspnoea
including blood gas analysis, lung function test, 6-min walk test,echocardiography, computed chest tomography (CT) scan, tho-racic sonography, and CPET. Due to the retrospective nature of ourstudy, examinations mentioned (except CPET) were not performedin the entire patient population.
Results
Baseline characteristicsIn the time period 42 patients post COVID-19 were seen at our
hospital, 31 patients were excluded because no CPET was per-formed. Ten patients met the eligibility criteria. Mean age of thesepatients was 50±13.1 years and four patients were female. In the
acute phase of COVID-19 six patients had been hospitalized, fivepatients needed oxygen, two patients needed high-flow oxygentherapy, and in two patients invasive ventilation was necessary.Mean hospital stay was 23.4±22.0 days; mean time to presentationto our outpatient’s clinic after hospital discharge were 115 days.None of the participants had a history of lung disease, congestiveheart failure, diabetes mellitus or malignancy. There were fivepatients with known “arterial hypertension”, one patient had anACE inhibitor in his regular medication.
Ejection fraction in transthoracic echocardiography was nor-mal in all patients. One patient showed a slightly dilated right ven-tricle with a mild tricuspid valve insufficiency (PAP elevation 60mmHg over central venous pressure). No other patient showedsigns of an acute right heart strain. Thorax sonography was per-formed in two patients showing normal diaphragm function. ChestCT scan was performed in all patients. Five patients showedground glass opacities and one patient showed streaky residua.Pulmonary embolism, as possible reason for the dyspnoea, wasexcluded by CT scan in nine patients (one patient had a CT scanwithout contrast agent but a low likelihood in Wells-Score andnegative d-dimer testing).
No participant had obstructive lung disease. A nominal reduc-tion of the diffusion capacity of the lung for carbon monoxide(DLCO) of 73% was recognized in the cohort.
Cardiopulmonary exercise testingPeak oxygen uptake (Peak-VO2) was measured by CPET with
1512±232 ml/min (72.7% predicted) at a mean peak work rate of131±29 W (92.4% pred.). Mean alveolar-arterial oxygen gradient(AaDO2) at peak exercise was 25.6±11.8 mmHg, mean peak ven-tilation was 64.7 l/min and mean breathing reserve (BR) was35.1±19.0%. Mean heart rate during exercise was 133±19 /min(78.1±7.3 pred.), oxygen pulse 11.9±2.6 (96.0±15.5% pred.).Mean EQCO2 and mean EQO2 at VT1 were measured with35.4±6.5 and 28.7±10.4. Mean value of lactate post exercise was5.6±1.8 mmol/l. A detailed description of all patients is presentedin Table 1.
In detail CPET detected a nearly normal performance(VO2max ≥ 85%) in two of the patients (No 3 and No 8), eightpatients (beside No 1 and No 10) had elevated (>30) EQCO2 val-ues at VT1. Limitation was cardiac in one patient (No 5) and ven-tilatory (BR <30%) in two patients. AaDO2 was elevated in threepatients (No 3, No 4 and No 8). Dyspnoea during CPET was quan-tified via RPE scale (range 3-9).
DiscussionTo our knowledge, this is the first study examining patients
with persistent dyspnoea after COVID-19. Persistent dyspnoea inpatients, who recovered from acute COVID-19 infection has beendescribed [7-9].
The gap between reached peak work rate (92.4% predicted) topeak oxygen uptake (72.3% pred.) in our study population canmost likely be explained by an early switch to anaerobicmetabolism. This would explain why mean value of lactate postexercise was high in our study population and even higher (n.s.)compared to the subgroup of patients with reduced peak oxygenuptake and other obvious reason for limitation.
In two patients the limitation was ventilatory. Critical-illness-polyneuropathy may have contributed in patient Nos 7 and 8.AaDO2 was elevated in three patients (No 3, No 4 and No 8), all ofthem had ground-glass opacity or streaky residua on the CT-scan.Finally, even with the use of CPET, dyspnoea could not be
MRM_02 short.qxp_Hrev_master 10/02/21 08:53 Pagina 2

81MRM
Multidisciplinary Respiratory Medicine 2021; 16:732 - A. Mohr et al.
Tabl
e 1.D
etai
led ch
arac
teris
tics o
f all
10 p
atien
ts.
Patie
nt
Gen
der/
Tim
e in
Oxy
gen
/
CT
Lu
ng fu
nctio
n
6 m
in
CPE
T:
CPE
T:
CP
ET:
CPE
T:
CPET
:
CPE
T:
CPE
T:
CPE
T:
CPE
T: EQ
O 2 CP
ET:R
ER
CP
ET:
num
ber /
ag
e /
hos
pita
l/
hig
h-flo
w
sca
n
Z-sc
ores
w
alk
po
wer
VE/
VCO 2
V’
O 2AT
/
m
ax.
aa
do2
BR
R
MV
ox
ygen
EQC
O 2
m
ax.
La
ctat
e m
ax.
occu
patio
n /
B
MI
on
ICU
NI
V / i
nvas
ive
an
d
slop
e /
V
O 2m
ax
HR
(
rest
/
pu
lse
dea
d sp
ace
(
post
-
(p
ost-
smok
ing
ve
ntila
tion
TLC
O SB
/
VE
/VCO
2
e
xerc
ise)
vent
ilatio
n e
xerc
ise)
ex
ercis
e)st
atus
h
aem
oglo
bin
in
terc
ept
(e
xerc
ise)
[mm
ol/l]
1 / nu
rse /
F /
52 a
/
0 da
ys
No o
xygen
No
abno
rmali
ties;
FEV /
FVC:
441 m
(91%
)
9
8 W
28.
2 /
731 m
l / mi
n
12
9 / m
in
1
7 mmH
g /
19
%
4
0 l/m
in
1
0 ml
23.0
1.5
5,
93for
mer s
moke
r 3
6.3 kg
/m²
the
rapy
no pu
lmon
ary
nor
mal
1
06%
2 l /
min
12
88 m
l/min
(78%
)
77%
29 m
mHg
10
2%
27.7
since
2018
emb
olism
TLC:
-2.23
9%
(30 p
y)
TLC
O SB
: 76%
H
b 13.6
g/dl
2 /
innk
eepe
r /
F / 3
6 a /
0 days
N
o oxyg
en
No ab
norm
alitie
s;
FE
V / FV
C:
n.
a.
99 W
3
1. 2 /
6
60 m
l/min
162
/ min
21 m
mHg /
51%
49 l
/min
7.5
ml
3
1.3
1.7
3,35
no sm
oker
20.7
kg/m
²
therap
y
ther
apy
no pu
lmon
ary
no
rmal
85%
4 l / m
in
1221
ml/m
in (7
4%)
8
8%
25 m
mHg
8
3%
42
.4
embo
lism
T
LC: n
orma
l
13%
TL
CO SB
: 88%
H
b 15.1
g/dl
3 /
cler
k / fo
rmer
F / 5
4 a /
2
2 days
/
Oxyg
en th
erap
y
G
roun
d-glas
s
FEV /
FVC:
norm
al
n
.a.
100 W
25
.8 /
64
9 ml/m
in
1
29 / m
in
2
1 mmH
g /
36
%
6
1 l/m
in
11
.2 ml
34.5
1.3
4,
17sm
oker
sinc
e
29.0
kg/m
²
6 da
ys
hig
h-flow
-ther
apy
op
acity
;
TLC
: nor
mal
107
%
2
l / m
in
1355
ml/m
in (8
5%)
7
8%
35
mmH
g
116%
38.1
20
13 (1
0 py)
No n
oninv
asive
no
pulm
onary
TLC
O SB
: 63%
1
5%
venti
lation
emb
olism
H
b 14.2
g/dl
N
o inv
asive
venti
lation
4 / fa
ctory
M
/ 58 a
/
56 da
ys /
O
xygen
ther
apy
Gro
und-g
lass
FE
V / FV
C: no
rmal
621 m
154
W
26.7
/
839 m
l/min
107
/ min
4.8
mmHg
/
43%
67 l
/min
13.7
ml
26
.7
1.9
8,78
worke
r /
33
.0 kg
/m²
42
days
No
high
-flow
-ther
apy
opac
ity;
TLC:
-1.71
(
126%
)
10
8%
3
l / m
in
1368
ml/m
in (6
4%)
6
6%
37
mmH
g
102%
35.5
no sm
oker
N
o non
invas
ive
CT
-scan
with
out
TL
CO SB
: 70%
1
6%
venti
lation
c
ontra
st ag
ent
Hb 1
4.4 g/
dl
Invas
ive ve
ntilat
ion
5 / nu
rse /
M
/ 44 a
/
1 da
y /
No
oxyge
n the
rapy
No a
bnor
maliti
es;
F
EV / F
VC: n
orma
l
395
m
1
62 W
30
.7 /
108
0 ml /
min
1
60 / m
in
1
2 mmH
g /
58
%
6
9 l/m
in
11.6
24.7
1.
6
5
,00no
smok
er
21.0
kg/m
²
0 da
ys
n
o pulm
onary
TLC
: nor
mal
(54
%)
78%
2 l
/ min
18
40 m
l/min
(68%
)
91%
20 m
mHg
7
5%
36.7
em
bolis
m
TLCO
SB: 7
9%
14%
H
b 16.3
g/dl
6 /
n / a
/
M
/ 61 a
/ 49 d
ays /
0
days
Oxyg
en th
erap
y
G
roun
d-glas
s
FEV /
FVC:
norm
al
53
4 m
1
50 W
28
.9 /
89
1 ml/m
in
1
16 / m
in
1
1 mmH
g /
38
%
7
2 l/m
in
14.9
23.8
1.
6
6
,15no
smok
er
29.0
kg/m
²
No h
igh-fl
ow-th
erap
y
op
acity
;
TLC
: nor
mal
(97
%)
98%
4 l
/ min
16
70 m
l/min
(74%
)
73%
29 m
mHg
10
6%
3
1.3
No n
oninv
asive
venti
lation
no pu
lmon
ary
T
LCO
SB: 9
2%
16%
N
o inv
asive
venti
lation
embo
lism
H
b 16.7
g/dl
7 / cl
erk /
M / 5
8 a /
7
days
/
Oxyg
en th
erap
y
G
roun
d-glas
s opa
city;
FE
V / FV
C: no
rmal
n.a.
10
2 W
38.5.
1 /
779 m
l / mi
n
11
7 / m
in
1
0 mmH
g /
14
%
6
8 l/m
in
11
,4. m
l
54.4
1.
1
3
,97no
smok
er
22.3
kg/m
²
0 da
ys
No h
igh-fl
ow-th
erap
y
no pu
lmon
ary
T
LC: n
orma
l
5
9%
3 l / m
in
1320
ml/m
in (5
6%)
7
3%
7
mmH
g
77%
48
.5
No n
oninv
asive
venti
lation
em
bolis
m
TLCO
SB: 6
3%
17%
No i
nvas
ive ve
ntilat
ion
H
b 14.6
g/dl
8 /
denti
st /
M / 5
9 a /
2
6 days
/ 23 d
ays
Ox
ygen t
herap
y
Stre
aky r
esidu
a;
F
EV / F
VC: n
orma
l
n.a
.
1
68 W
38
.1 /
110
7 ml/m
in
1
27 / m
in
2
5 mmH
g /
8
%
9
1 l/m
in
15
.4 ml
29.0
1.7
4,
69no
smok
er
23.0
kg/m
²
H
igh-fl
ow-th
erap
y
no p
ulmon
ary
TLC
: -2.44
1
13%
3 l /
min
18
50 m
l/min
(89%
)
79%
45 m
mHg
11
9%
3
5.7
No n
oninv
asive
venti
lation
em
bolis
m
TLCO
SB: 5
4%
17%
In
vasive
venti
lation
H
b 12.7
g/dl
9 / ba
nk
M / 5
8 a
0
days
N
o oxyg
en th
erap
y
Gro
und-g
lass o
pacit
y;
FEV /
FVC:
norm
al
44
2 m
1
50 W
33
.1 /
93
7 ml/m
in
1
29 / m
in
1
3 mmH
g /
21
%
9
0 l/m
in
14
.3 ml
23.6
1.6
8,
43em
ploye
e /
/
32.0
kg/m
²
n
o pulm
onary
TLC
: nor
mal
(77
%)
89%
3 l
/ min
18
20 m
l/min
(74%
)
80%
17 m
mHg
9
4%
30.1
no sm
oker
embo
lism
TL
CO SB
: 93%
1
2%
Hb 1
5.5 g/
dl10
/ stud
ent /
F / 21
a /
0
days
N
o oxyg
en th
erap
y
N
o abn
orma
lities
;
FEV
/ FVC
: nor
mal
5
53 m
128
W
24.9
/
576 m
l/min
150
/ min
23 /
6
3%
4
0 l / m
in
9,
3 ml
15.8
1,6
5,
78no
smok
er
32.0
kg/m
²
n
o pulm
onary
TLC
: nor
mal
(71
%)
81%
2 l
/ min
14
13 m
l/min
(66%
)
75%
12 m
mHg
8
6%
28.3
em
bolis
m
TLCO
SB: 7
9%
11%
H
b 15.5
g/dl
F, fe
male
M, m
ale; B
MI, b
ody-m
ass-i
ndex
; ICU,
inte
nsive
care
unit;
HR, h
eart
rate
; AaD
O2, a
lveola
r-arte
rial o
xyge
n gra
dient
; ARD
S acu
te re
spira
tory
distre
ss sy
ndro
me; B
R, br
eath
ing re
serve
; n.a.
, not
avail
able;
TLCO
, diff
usion
capa
city o
f the
lung
for c
arbo
n mon
oxide
; CPE
T, sp
iroer
gome
try; R
MV,
resp
irato
ry mi
nute
volum
e, py
, pac
k yea
rs.
MRM_02 short.qxp_Hrev_master 10/02/21 08:53 Pagina 3

82MRM
Multidisciplinary Respiratory Medicine 2021; 16:732 - A. Mohr et al.
explained by cardiac, pulmonary or ventilatory limitation in allpatients. Muscular deficiency and thus metabolic limitation mighthave contributed to dyspnoea in most patients. As in other viraldiseases in adults (e.g., EBV) and in acute respiratory distress syn-drome (ARDS), complete clinical recovery might be prolonged inCOVID-19 [7,11-13]. However, the reason for muscular deficien-cy itself is unclear. It could either be due to atrophy as a conse-quence of insufficient physical load or critical-illness-polyneu-ropathy or direct damage of muscle or central nervous system bySARS-Cov2 [14].
LimitationsOur study has many limitations. First of all, it is retrospective
and the number of patients being included is very small. Second, itis a single centre study; on the other hand, this is the first study atall analysing persistent dyspnoea in patients with COVID-19 viaCPET.
ConclusionDespite the use of CPET, dyspnoea could not be explained by
cardiac, pulmonary or ventilatory limitation in all patients. A gapbetween peak work rate in (92.4% predicted) to peak oxygenuptake (72. % pred.) was detected in our study cohort. Mean valueof lactate post exercise was high in our study population and evenhigher (n.s.) compared to the subgroup of patients with reducedpeak oxygen uptake and other obvious reason for limitation. Bothobservations support the hypothesis of anaerobic metabolism.Muscular deficiency and thus metabolic limitation might con-tribute to dyspnoea in most patients. Further prospective studieswith more participants are needed to evaluate the aetiology of dys-pnoea post COVID-19.
References1. WHO. Coronavirus Disease (COVID-19) Dashboard 2020
[updated 09.09.2020]. Available from: https://covid19.who.int/2. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al.
Clinical characteristics of coronavirus disease 2019 in China.
N Engl J Med 2020;382:1708-20. 3. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early
transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med 2020;382:1199-207.
4. Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S,Müller MA, et al. Virological assessment of hospitalizedpatients with COVID-2019. Nature 2020;581:465-9.
5. Kaye R, Chang CWD, Kazahaya K, Brereton J, Denneny JC,3rd. COVID-19 anosmia reporting tool: Initial findings.Otolaryngology--head and neck surgery : official journal ofAmerican Academy of Otolaryngol Head Neck Surg2020;163:132-4.
6. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinicalfeatures of patients infected with 2019 novel coronavirus inWuhan, China. Lancet 2020;395:497-506.
7. Halpin SJ, McIvor C, Whyatt G, Adams A, Harvey O, McLeanL, et al. Postdischarge symptoms and rehabilitation needs insurvivors of COVID-19 infection: A cross-sectional evalua-tion. J Med Virol 2020;93:1013-22.
8. Carfì A, Bernabei R, Landi F. Persistent symptoms in patientsafter acute COVID-19. JAMA 2020;324:603-5.
9. Wang X, Xu H, Jiang H, Wang L, Lu C, Wei X, et al. The clin-ical features and outcomes of discharged coronavirus disease2019 patients: A prospective cohort study. QJM 2020;113:657-65.
10. Garrigues E, Janvier P, Kherabi Y, Bot AL, Hamon A, GouzeH, et al. Post-discharge persistent symptoms and health-relatedquality of life after hospitalization for COVID-19. J Infect2020;81:e4-6.
11. Dunmire SK, Verghese PS, Balfour HH, Jr. Primary Epstein-Barr virus infection. J Clin Virol 2018;102:84-92.
12. Balfour HH Jr, Dunmire SK, Hogquist KA. Infectiousmononucleosis. Clin Transl Immunology 2015;4:e33.
13. Brandstetter S, Dodoo-Schittko F, Brandl M, Blecha S, Bein T,Apfelbacher C. Ambulatory and stationary healthcare use insurvivors of ARDS during the first year after discharge fromICU: findings from the DACAPO cohort. Ann Intensive Care2019;9:70.
14. Orsucci D, Ienco EC, Nocita G, Napolitano A, Vista M.Neurological features of COVID-19 and their treatment: areview. Drugs Contex 2020;9:2020-5-1.
Received for publication: 1 November 2020. Accepted for publication: 29 January 2021.This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0).©Copyright: the Author(s), 2021Licensee PAGEPress, ItalyMultidisciplinary Respiratory Medicine 2021; 16:732doi:10.4081/mrm.2021.732
MRM_02 short.qxp_Hrev_master 10/02/21 08:53 Pagina 4

IMRM
Congress report
RUBRICA
Diversamente dalla consuetudine adottata nelle malattie eponimiche, la sindrome di Pickwick non è stata definita con il nome del medico che per primo l’ha descritta, bensì è stata così denominata in ricordo del personaggio di Joe, inventato (o meglio descritto) da Charles Dickens, che si caratterizzava per la seguente combinazione di segni e sintomi: obesità, sonnolenza, ipoventilazione, faccia ple-torica e che compariva nel suo libro I quaderni postumi del Pickwick Club. Forse proprio per quest’insolita scelta semantica, che aveva privilegiato la celebrità del nome Pickwick, tale sindrome è diventata una tra le più note; a essa si è probabilmente ispirato anche Walt Disney per il personaggio di Ciccio di Nonna Papera. Detto questo, giù il cappello davanti a Mr. Pickwick, e mi rivolgo a voi, amanti della lettura, che volete uscir da voi stessi e calarvi in un mondo diverso, dove riconoscere però tutti i co-lori dell’umano. Giù il cappello davanti al mite e serafico uomo d’affari a riposo, enciclopedico dilettante, che con tre amici, Winkle lo sportivo, Snodgrass il poeta e Tup-man l’aspirante Casanova (tutti con fisici e prestazioni impari alle ambizioni) vagabonda per l’Inghilterra del primo Ottocento per riferire al Circolo da lui fondato su
caratteri, usanze, curiosità naturali e artistiche, storia lo-cale e così via. Ai quattro si aggiunge Sam Weller, il San-cio Panza di Pickwick, uno dei personaggi memorabili di Dickens, domestico astuto e fedele, esperto del mondo e della vita, accorto consigliere dell’ingenuo padrone. E
L’angolo della Cultura (non solo Medicina…)a cura della Redazione
email: [email protected]
L’eterna giovinezza del Circolo Pickwick
Francesco IodiceGià Direttore U.O. s.c. di Fisiopatologia Respiratoria, Ospedale A. Cardarelli, Napoli, Italia
email address: [email protected]
“I princìpi non servono, sono cose acquisite,sono stracci che volano via alla prima scrollata.
Quello che ci vuole è un credo convinto”. Joseph Conrad, Cuore di tenebra
“I malintesi sono il sale della terra.Senza di essi non vi sarebbe più niente da dire”.
Augusto Frassinetti, Tutto sommato, 1985
Figura 1 I quaderni postumi del Pickwick Club.

IIMRM
Rubrica
inesauribile fonte di comicità, col suo spirito “cockney”, da proletario londinese, coi suoi aneddoti bizzarri, i pa-ragoni spiazzanti, o nei duetti col padre, il vetturino Tony. Dal “Circolo” ora si sprigiona – in una nuova traduzione recentemente pubblicata da Einaudi – un senso di inde-finito: come se si svolgesse in un tempo ciclico e i perso-naggi vagassero ancora nella campagna inglese, un’opera torrenziale.
Ai tempi della regina Vittoria, e anche un po’ prima, alla fine del fascicolo si leggeva: “Arrivederci alla pros-sima puntata”. Infatti, in Gran Bretagna i romanzi usci-vano periodicamente a fascicoli e solo in un secondo mo-mento raccolti in volume. Da parte dell’editore era questo un modo di controllare le spese e, da parte dell’autore, un impegno a tenere desta l’attenzione del pubblico. La fine di ogni puntata creava una forte suspense, come davanti all'orlo di un precipizio, e la cosa prese infatti il nome di “cliffhanger ending” o “suspenseful ending”, (letteral-mente finale sospeso a un baratro o finale in sospeso) tuttora in uso nel gergo dei critici televisivi quando par-lano di programmi, come I Soprano o Melrose Place. I romanzieri, e Charles Dickens ne è un esempio, furono costretti a chiedere alla Musa di tener conto dei gusti del lettore e, al pari della gente di teatro e del circo, dovettero imparare – applausi o fischi, fiori o pomodori – che il cliente ha sempre ragione. Dopo un breve tirocinio come ragazzo di bottega in uno studio legale, Dickens divenne cronista parlamentare. Ebbe occasione di seguire la cam-pagna elettorale di un candidato e ne fece un resoconto, più tardi ripreso in un episodio del Circolo Pickwick, che aveva tutta l’aria di un carnevale in maschera. Firmò una serie di bozzetti per il Morning Chronicle, in seguito pub-blicati dall’editore John Macrone come Sketches by Boz, tradotti di recente in italiano. Il libro fu notato da Chap-man e Hall della omonima casa editrice, i quali chiesero a Dickens di scrivere brevi testi in prosa per riempire gli spazi tra le vignette che Robert Seymour avrebbe dise-gnato per una prossima pubblicazione mensile a fasci-coli. Scene di vita campestre con cavalli che si piantano in mezzo alla strada e non vogliono ripartire; un fucile che spara a casaccio – e nemmeno a salve – per l’im-perizia del cacciatore che lo imbraccia; ami e lenze che volteggiano nell’aria e finiscono per agganciare la canna al cappello o al fondo dei pantaloni del pescatore vicino. Episodi umoristici nella cornice di un’Inghilterra soprav-vissuta alla minaccia napoleonica, che sembra essere an-cora – con postiglioni e locande, strade sterrate e villaggi addormentati nel verde – quella dei tempi passati. Dopo soli due numeri, Seymour morì e il giovane Dickens prese in mano la situazione. Le pagine dei fascicoli diventarono trentadue e gli schizzi che dovevano essere un riempitivo diventarono il testo di un corposo romanzo, ambientato tra il 1827 e 1828. Dopo il terzo numero, fu Phiz, al se-colo Hablot Knight Brown, a illustrare il romanzo che ri-
fletteva un mondo perfettamente dickensiano composto da avidi cacciatori di dote, truffatori e furfanti, gioviali signorotti di campagna con relativo codazzo di nipoti, so-relle, servette e servitori, e un irresistibile grassone, Fat Joe, probabilmente affetto da narcolessia, che si addor-menta non appena smette di parlare. A questi bisogna ag-giungere affittacamere e cameriere, cocchieri e facchini, guardacaccia e villani, viaggiatori anonimi e azzeccagar-bugli dal volto e dal nome ben definiti, per un totale di più di 300 personaggi (c’è chi li ha contati, ndr.) che sono i primi abitanti di quella che sarà la brulicante Città di Dickens. Il primo fascicolo di Pickwick ebbe una tiratura di 400 copie; il quindicesimo arrivò a 40 mila. Il successo clamoroso consentì di raggiungere tutto il pubblico pos-sibile all’epoca; di ogni puntata si facevano letture collet-tive all’ora del tè in appartamenti privati dietro modesto esborso al padrone di casa. La pubblicazione sviluppò un notevole indotto (lo “spin-off” o prodotto secondario di oggi, ora però pianificato a tavolino dal marketing edito-riale prima ancora dell’uscita del libro): bastoni, cappelli, sigari, giacche alla Pickwick; imitazioni, parodie, sequels, adattamenti teatrali; nacque l’aggettivo “pickwickiano”; sorsero club di appassionati.
L’introduzione di questo cambio di passo favorì la con-tinuità narrativa e l’unitarietà del testo. Si sviluppò allora una specie di trama principale: la tragicomica contesa giu-diziaria fra Pickwick e la sua padrona di casa, la vedova Bardell, che per un surreale equivoco lo cita per mancata promessa di matrimonio: il rifiuto di pagare un inden-nizzo truffaldino porterà Pickwick nelle carceri di Fleet Street. A questo filone principale si intrecciano poi temi ricorrenti, come l’amicizia fra Pickwick e la famiglia di Mr. Wardle o le gustose vicende dei Weller padre e figlio.
Il Circolo Pickwick, in cui confluisce la tradizione pi-caresca (Tom Jones di Fielding, Moll Flanders di Defoe, ecc), costituì un laboratorio di quanto Dickens scriverà in
Figura 2 Il Circolo Pickwick, acquerello 1929, Charles Di-ckens Museum.

IIIMRM
Rubrica
seguito, fino all’acre denuncia sociale dei grandi romanzi della maturità. Qui – l’abbiamo detto – c’è una galleria di centinaia di personaggi, spesso caricature o tipizzazioni più che figure a tutto tondo; ma ci sono la folla di Londra e le “country houses”, le case di campagna della borghesia, ci sono taverne e locande, fuoco nei camini e boccali di birra, cocchieri e imbroglioni, avvocati lestofanti, impie-gati fannulloni, zitelle e vedove, ragazze da marito, bimbi dispettosi, fanciulli maltrattati, una misera umanità car-cerata, servette maliziose e lustrascarpe ammiccanti.
Dickens a 24 anni divenne famoso, se non dalla sera alla mattina, dopo tre o quattro mesi dall’inizio, quando entrò in azione il personaggio di Sam Weller, l’arguto
servitore che divertirà i lettori fino alla fine della sto-ria et ultra, se è vero, com’è vero, che ancora qualche decennio fa si aveva l'impressione di risentirne la voce in certe battute dei bigliettai sugli autobus di Londra. Vecchi e giovani, il giorno dell’uscita di una nuova pun-tata andavano incontro al portalettere percorrendo a piedi due o tre miglia di strada. E persino gli analfa-beti, raccontano i biografi, provvedevano a mettere da parte qualche soldino per poter pagar da bere a chi gli leggesse l’ultima puntata. Ma se, come sappiamo, di ar-rivare a tirature stellari, oggi, sono ormai buoni un po’ tutti (si fa per dire), Pickwick deve considerarsi un caso a parte. Infatti, non nasce nel gabinetto dell’alchimista specializzato in best-seller con fusione a freddo – una dose di questo, una di quello, sesso in abbondanza e una spolverata di humour –, ma è un’opera torrenziale in cui i singoli personaggi cominciano a muoversi assai prima che lo stesso autore abbia avuto modo di progettarli. Hanno la forza della verità perché provengono dalla sede naturale dell’immaginazione, che è l'inconscio – se collettivo o del solo autore non si può dire – e ognuno di loro, grandi e piccoli, buoni e cattivi, ha le fattezze di un eroe o di una divinità del folklore inglese. Alcuni critici hanno ritenuto che Pickwick non sia nemmeno un romanzo, ma una creazione che è all’origine di un mito; e questo in quanto i romanzi hanno una trama e arrivano a una conclusione, mentre Pickwick lascia dietro di sé un senso di indefinito e di eterna giovinezza; come se si svolgesse in un tempo ciclico e non lineare e i suoi personaggi stessero tuttora vagando nella campagna in-glese. Non è insomma né un best-seller né un long-seller, Pickwick, ma un monumento, e se qualcuno ancora non lo conoscesse può ora recuperare il tempo perduto leg-gendo la recente traduzione stampata da Einaudi. Con Pickwick ci troviamo davanti a un universo raccontato con strabiliante freschezza di invenzione e osservato con benevola ironia. Un brulichio da formicaio, un moto in-cessante cui fanno da contrappeso la gentile bontà e la placida tranquillità del protagonista. Una narrazione che intende offrire, parole dell’autore, “una visione più lieta e luminosa della natura umana”. In due parole: si ride ad alta voce anche leggendo in solitudine.
Figura 3 Sam Weller, personaggio memorabile di Di-ckens.

IVMRM
Congress report
RUBRICA
WHEN WHERE WHAT WHO TO CONTACT
2021
April 6th International Conference: “Sleep and Breathing” – https://sleepandbreathing.org/ 15-17 virtual event
May American Thoracic Society International Conference – https://conference.thoracic.org/ 14-19 online event
May Course: “Masterclass on pulmonary and pleural infections” https://www.ersnet.org 27-28
May Course: “Masterclass on pulmonary and pleural infections – https://www.ersnet.org 29 Focus on tuberculosis”
June CHEST Congress Italy 2021 – online event https://congress.chestnet.org/ 24-26
September ERS International Congress 2021 – virtual event https://www.ersnet.org 4-8
November Lisbon Research seminar: “Innovative 3D models for understanding https://www.ersnet.org 4-5 (Portugal) mechanisms underlying lung diseases: powerful tools for translational research”
November Krakow Seminar: “Cystic fibrosis” https://www.ersnet.org 18-20 (Poland)
November Kyoto APSR 2021 – The 25th Congress of the Asian Pacific Society [email protected] 20-21 (Japan) of Respirology – hybrid event
November Budapest Course: “Lung transplantation: Sharing experience https://www.ersnet.org 25-27 (Hungary) across Europe”
Meeting Calendar


Volume 16 - N
umber 1-2 - A
pril 2021M
ultid
isciplin
ary Resp
iratory M
edicin
e