Embed Size (px)
Citation preview

AirAsthma
in theAirAsthma
in the
Multidisciplinary clinic offers hope
to inner city children suffering
from asthma

School of Medicine Administration
Robert R. Frank, M.D.Interim Dean
Kertia Black, M.D.Assistant Dean for Student Affairs
Patrick Bridge, Ph.D.Assistant Dean for Medical Evaluation and Education Research
Joseph Brocato, Ph.D.Assistant Dean for Community Education
Donna DauphinaisChief of Staff
Kenneth Ginsburg, M.D.Assistant Dean for Clinical Science Education
Michael HerbertAssistant Dean of Administration and Finance
Matthew Jackson, Ph.D.Interim Assistant Dean for Basic Science Education
Mark Juzych, M.D.Assistant Dean for Graduate Medical Education
Stephen Lerner, M.D.Associate Dean for Faculty Affairs
Helene Lycaki, Ph.D.Assistant Dean for Health Affairs
John Malone Jr., M.D.Associate Dean for Medical Center Relations
Silas Norman, M.D.Assistant Dean for Admissions
Kenneth Palmer, Ph.D.Assistant Dean for Graduate Programs
David Pieper, Ph.D.Assistant Dean for Continuing Medical Education
J. Edson Pontes, M.D.Assistant Dean for International Affairs
John Ruckdeschel, M.D.Associate Dean for Cancer Programs
Basim Dubaybo, M.D.Assistant Dean for Veterans Administration Affairs
Maryjean Schenk, M.D.Interim Associate Dean for Academic & Student Programs
Daniel Walz, Ph.D.Associate Dean for Research
Charles Whitten, M.D.Associate Dean Emeritus for Special Programs
Wayne State University Executive Officers
Irvin ReidPresident
Nancy BarrettProvost and Senior Vice President for Academic Affairs
Susan BurnsVice President for Development and Alumni Affairs, and President for the Wayne State University Foundation
John DavisVice President, Treasurer and Chief Financial Officer
Meredith GibbsExecutive Vice President; Chief of Staff
Harvey Hollins IIIVice President for Government Affairs
Louis LessemVice President and General Counsel
Julie MillerSecretary to the Board of Governors and Executive Assistant to the President
John OliverVice President for Research
Wayne State University Board of Governors
Tina AbbottRichard BernsteinEugene DrikerDiane DunaskissElizabeth HardyPaul MassaronAnnetta MillerJacquelin Washington
Irvin ReidEx-Officio
Julie MillerSecretary
School of Medicine Board of Visitors
Karen BatchelorJan BertschBeth ChappellJulius Combs, M.D.John ConwaySteve EwingOscar FeldmanMelvin Hollowell Jr.Arthur Johnson, Ph.D.Mary KramerTaylor Lewis, M.D.Robert Lucas, M.D.W. Ralph MabryGwen MacKenzieFlorine MarkMariam NolandWilliam O’Neill, M.D.Jack Ryan, M.D.Howard SimsCharly VickeryRichard Webb
Dean’s Distinguished Advisors/ConsultantsTrudy DunCombe ArcherGeorge Dambach, Ph.D.Deborah DingellSteve Larned, M.D.David PageJohn Schwarz, M.D.Margaret SmithGary Valade
This publication was produced by the Office of theDean through the Office of Public Affairs andPublications. Your comments are welcome. Feel freeto email the editor at [email protected] orsend your correspondence to the following address:
Public Affairs & PublicationsWayne State University School of MedicinePublic Affairs and Publications5D University Health Center4201 St. AntoineDetroit, MI 48201(313) 577-1429(313) 993-4333 fax
Director of Public Affairs and PublicationsKathleen Wedemire, APR
Managing Editor/Senior WriterAmy DiCresce
Contributing WritersAndrea GreskoLeslie Mertz
DesignMidnite Oil Creative
PhotographyRobert Stewart Photography Ltd.Tom Owoc, Biomedical Communications

Contents Asthma in the air
What began as a clinical trial for
asthmatic inner city children has
become a multidisciplinary clinic
offering well-rounded treatment
programs to patients and their
families. Dr. Elizabeth Secord is
providing care to kids suffering
from asthma, one of the most
common chronic diseases.
Neurorecovery and innovation prompt therapiesfor traumatic injuriesThere’s no shortage of ambition
with Dr. Jay Meythaler. He’s
found windows of opportunity
where none existed for spinal
cord and brain injuries.
His goal: getting therapeutics
across the blood-brain barrier
and stimulating the healing of
neurons.
Shattering the shame of the uninsuredMedical student John Stasko’s
award-winning photography
exhibit, “People of Detroit: A
Living Project,” features portraits
and excerpted interviews from
citizens of Detroit sharing their
health care experiences.
Grad student trades in fieldjournal for flow cytometerSarah Krueger celebrates
success in the cancer biology
Ph.D. program.
Smart shunt warns of wear and tear in the brainResearchers from neurosurgery
and engineering are developing
an electronic chip that provides
a warning signal when a brain
shunt needs replacement or
retuning.
Zebrafish provide prettymodel to study ugly bacteriaDr. Melody Neely learns about
deadly strains of strep infections
using the 1.5-inch-long zebrafish
as a model.
Doing the double-take of chemo and radiationResearchers at Wayne State
University and the Karmanos
Cancer Institute are helping
patients with head and neck
cancers live longer lives and
avoid cosmetic and functional
deformities by using combined
chemotherapy and radiation.
Think tank spurs action for underserved peopleFrom poverty to homelessness
to health care access, Dr. Iltefat
Hamzavi advocates for community
health issues as co-founder and
interim executive director of the
Institute for Social Policy and
Understanding.
Act like a better doctor, be a better doctorStandardized patients are
trained actors who portray a
clinical scenario, providing a safe
environment for medical students
to perfect their clinical skills.
Protease knowledge gives Stefanie Roshy bargaining powerGraduate student Stefanie Roshy
is on to something big, studying
complex proteases that play a
role in the progression of breast
cancer.
Wayne Medicine 2005
2 Wayne Medicine 2005
Air
Asthma is one of the most common chronic diseases among chil-dren. According to the American Lung Association, an estimated 4million children under the age of 18 have had an asthma attackover the past year, and many others have non-symptomatic orundiagnosed asthma. Childhood asthma is the chronic disease thatcauses the most school absences in the United States.
For minority children, especially those who live in the inner city, asthma can causemuch more than just a missed day of school. The number of diagnosed cases contin-ues to rise in urban areas and more African Americans suffer abrupt and unexpecteddeath from asthma than asthmatics of any other ethnic group.
Fortunately, a Wayne State University doctor and her multi-disciplinary researchteam are working to help change and save the lives of children who are most at risk.
For a little more than a year, Elizabeth Secord, M.D., assistant professor in theDivision of Immunology, Allergy and Rheumatology within the Department ofPediatrics, has been part of a clinical trial with moderate and severe asthmatic innercity children and their families. She has created a clinic that offers a well-rounded, all-inclusive treatment program to its patients.
“We have approximately 75 subjects enrolled and we’re looking to enroll up to 150.We want it open to the high-risk kids and as many moderate-risk kids as we canaccommodate,” Dr. Secord said.
During its study, Dr. Secord’s team has found that a lack of adherence to treatmentis a common thread connecting many patient cases, although genetic and environ-mental factors also come into play.
“There is a high morbidity among children in urban areas. Children who arealready asthmatic and are exposed to mold, dust and cockroaches don’t do as well,”Dr. Secord said. “Lack of adherence is a big issue among high-risk asthmatics. Kidsthat aren’t so bad can get away with not taking their medications once in a while, but
Multidisciplinary clinic offers hope to inner city children suffering from asthma.
Asthma
By Andrea Gresko
in the

Dr. Elizabeth Secord understandsthat children in urban settings mayhave trouble adhering to asthmatreatments because of complicatingenvironmental or lifestyle issues likethe presence of mold, dust, cock-roaches, smokers or pets in thehome.

4 Wayne Medicine 2005
the severe ones can’t.”Dr. Secord’s patients and their families
often struggle with many stresses ofpoverty and inner city life, and the addi-tional burden of coping with a chronicillness becomes overwhelming for them.This is why providing a full-range of ser-
vices is so important.When entering the study,
subjects receive full medical,environmental, psychological,social, and pharmacologicalevaluations.
The patient’s family thenparticipates in an educationalprogram designed to fit itsspecific needs. Topics ofteninclude making environmental changesin the home, medication education andreview, and general information aboutasthma. The team then formulates anaction plan for the family.
Subjects are re-evaluated until theirasthma is under control. The patientsand families who are considered most atrisk are offered additional servicesincluding home environmental assess-ments and motivational enhancementtherapy (MET).
MET focuses on the needs of youngparents, pre-adolescents, and adoles-cents, who are often not able to addresstheir children’s or their own health careneeds while confronted with many otherpsychosocial issues.
According to Dr. Secord, the subjects
seem very happy with the care they’rebeing given – with one exception.
“They’re not happy with the question-naires they have to fill out, but we try tomake it worth their while because theyget more services,” she said.
A distinct facet of the program is the
relationship the clinic has with theFamily Independence Agency (FIA). Aspecially trained FIA supervisor, who isfamiliar with asthma, supervises allreferred cases and is part of monthly clin-ic care meetings.
This allows any FIA workers whoreport to the supervisor access to clinicrecommendations on environmentalcontrol and medication management.The ability of FIA workers to recognizelack of adherence to asthma treatments isan added insurance to help protectpatients from medical neglect.
Dr. Secord’s study has four specificgoals: to reduce the number of asthma-related hospitalizations and emergencyroom visits; to increase patient and fami-ly adherence with asthma therapies; to
improve the overall health of childrenwith moderate and high-risk asthma; andto demonstrate a reduction in health carecosts.
“Our hope is that we can demonstrateenough of a benefit to Children’sHospital of Michigan (CHM) and to the
insurance companies that itwill be worth their while tohelp continue funding the pro-gram. We’ve already shown adecrease in hospitalizationsand it’s a significant enoughsavings that it warrants to paythe extra staff,” she said.
Original funding for thestudy came from the
Children’s Research Center of Michigan.The trial was recently refunded for con-tinuation over several years through ahealthcare disparity grant throughMedicare.
Dr. Secord feels that a multi-discipli-nary approach to health care in an urbansetting is a win-win situation for allinvolved.
“The concept is very simple. We usedto have many more multi-disciplinaryclinics at CHM and the Medicare reim-bursements stopped coming so the hos-pital cut out the programs,” she said.“Patients would really benefit from theextra care. I think the idea is simple andwe’re just trying to show that it’s benefi-cial to the insurance companies, thepatients and the hospital as well.” �
The number of diagnosed asthmacases continues to rise in urban
areas and more African Americanssuffer abrupt and unexpected death
from asthma than asthmatics ofany other ethnic group.

52005 Wayne Medicine
Neurorecovery and innovation prompt therapies for traumatic injuries
There’s no shortage of ambitionwith Dr. Jay Meythaler. He’sfound windows of opportunitywhere none existed before andhe’s breathing fresh air into theresearch arena for spinal cordand brain injuries.
By Amy Dicresce
Picture the injured brain asthe hip new nightclub intown, requiring special VIPpasses for entry. Mostresearchers are waiting out-
side in the cold, trying to figure out howto gain access. More often than not, JayMeythaler, M.D., J.D., finds himself in theA-list line, getting past the protectiveguards and slipping through the blood-brain barrier to the hot-spot.
Wayne State University’s new chair ofthe Department of Physical Medicineand Rehabilitation is slipping new thera-pies into traumatically injured brains byfinding breaks in the barriers that aredesigned to keep out foreign intruders.Trouble is, some of those foreign sub-stances may be beneficial in healing peo-
ple with head injuries, spinal cordinjuries, stroke, Alzheimer’s and otherneurologic diseases.
In developing new therapies for brainand spinal cord injuries, it’s all aboutaccess and neurorecovery, Dr. Meythalersaid. “We’ve got to get across that blood-brain barrier and stimulate healing of theneurons. We need to know what mole-cules pass through, and attach ourselvesto them; or we can find the weak spots inthe wall and take them by storm; butwe’ve got to get across it and stimulateneuron recovery.”
With six drug patents and a seeminglyendless list of research publications, Dr.Meythaler has sent his compounds intobattle a number of times, and they aremaking substantial headway. His strategy
With a research interest in neuropharma-cology and neurorecovery, Dr. Meythaler issearching for targeted windows of opportu-nity to provide maximum healing effect forbrain and spinal cord injuries.

6 Wayne Medicine 2005
is to keep it simple, although that some-times makes him unpopular. Rather thandesign a most elegant experiment with asingular focus, he likes to take what isalready known and run with it in anoth-er direction.
“We are taking off-the-shelf technolo-gy and using it in new ways,” he said. Takefor example, the drug 4-AP or 4-aminopyridine. This drug has beenknown to help with improving nerveconduction through the injured nerves ofthe central nervous system in multiplesclerosis. Dr. Meythaler has applied it tothe peripheral nervous system as well inGullain-Barre syndrome (GBS).
“At first, I didn’t think it would workin GBS. We tried it and have foundpromising results,” Dr. Meythaler said.
Another example is baclofen, whichhas been used to relax muscles that areprone to spasticity in spinal cord injuriesor multiple sclerosis. Dr. Meythaler wasone of the original researchers to cham-pion a change in the delivery mechanism.For years, baclofen was taken orally, buthad only limited usefulness because themedication got dispersed and watereddown throughout the body. When Dr.Meythaler delivered it directly to thespinal canal through an implantedintrathecal pump, the results were dra-matically better. In addition, he was oneof the first to look at its use for headinjuries. Again, the results are very good,and a new study is showing that the drugtizanidine may be another alternative tobaclofen for reducing spasticity via direct
delivery into the spinalcanal.
“Our approach is tolook at proven com-pounds, in analogous sit-uations, and then try toparallel that success with anew delivery approach—either through an innov-ative system or as theresult of an add-on mole-cule—designed to over-come the blood-brain orblood-nerve hurdles,” hesaid.
Dr. Meythaler’s cur-rent research in drugdevelopment is operatingunder two basic tenets.First, he says, there is awindow of opportunityfor neuroprotection totake place. New animalstudies show specifictreatment windows forrats with spinal cordinjuries. After that briefperiod, spasticity maystart; however, new stud-ies are finding that thespasticity process may bereversed with appropri-ate therapy interventionsand motor function maybe enhanced. This timeperiod is an ideal opportunity for inter-ventions by medication and therapy toenhance recovery.
Targeting the exact time and locationfor therapies in the continuum of com-plex injuries and secondary symptoms istricky. Dr. Meythaler points out that youcan lose up to 80 percent of your neuronsand still be fairly functional for shortperiods of time. On the other hand, ifyou lose 90 percent of your neurons, youhave only trace functioning that is barelydiscernable. Somewhere in that 10 per-cent difference lies a complex area ofresearch.
Current drug trials have indicated thatmedications may target specific neuronsand must be administered in varioustime windows during the recovery fromCNS injury. If these medications areadministered outside this window, it
Physical therapy is a necessary part of rehabilitation follow-ing injury, Dr. Meythaler said. “You can use state-of-the-artmedications and procedures to help heal brain and spinalcord injuries, but without therapy, you don’t get better.”
Dr. Meythaler joined Wayne State University and theRehabilitation Institute of Detroit in 2004 after serving asco-director of the Traumatic Brain Injury Care System atthe University of Alabama at Birmingham and director ofBrain Injury Services at Spain Rehabilitation Center. Hewas particularly impressed with WSU’s contributions as acenter of excellence in brain injury research through itsparticipation in the Southeastern Michigan TraumaticBrain Injury System, funded by the National Institute onDisability and Rehabilitation Research.

72005 Wayne Medicine
could cause more damage, and result incomplications such as convulsions or lossof motor control. “Timing becomes veryimportant as we consider the variousneurotransmitters and neuropathways.But as we learn more about chemicalcomposition and complex biologicalprocesses, we can try new interventionsat just the right time to perhaps find newsuccess where it didn’t exist previously.”
This leads to Dr. Meythaler’s secondtenet, which is: “What you use early, youdon’t use late and vice versa.” He usessimple logic to explain. “When you havetrauma to the head or spine, it sets off aneurochemical cascade of inflammationand the release of glutamate and otherexcitatory neural transmitters that arereleased in high concentrations afterinjury and this may be toxic to neuronsthat have already been injured. Drugsthat block glutamate and these otherexcitatory neural transmitters should begiven early during these high concentra-tion times, but they should not be givenlater. This is because you learn and haveneural plasticity in part due to these verysame neural transmitters. Balance needsto be resumed or you’ll have a differentset of problems to deal with.”
This early/late principle is violated allthe time, Dr. Meythaler said. “Anti-seizure drugs are generally administeredearly after injury, and they should be. But
after the first week, they need to bestopped or they will slow neurorecovery.”Similarly, anti-psychotics are often usedfor agitation following TBI, but long-term, they interfere with healing.
Also critical to remember is this: thetherapy is as critical as the drug, said Dr.Meythaler. “New research shows we maybe wrong to get people up and into ther-apy too quickly in the first few days after
injury. The brain and spinal cord need 48hours of quiet rest, with no therapy, toallow the excitatory responses to calmdown,” he said.
These innovative ideas, though ques-tioned by some colleagues, often havesuccessful patients to champion them. Inthe 1990s, Landon Miller overcame asevere closed head injury and coma withthe innovative use of the drug piracetam.This patient inspired Dr. Meythaler to
establish Neurorecovery,Inc., a start-up companythat develops com-pounds and devices toaid injuries of thehuman brain, spinalcord and peripheral ner-vous system.
Gregory Scott Daniel,who is bedridden and paralyzed afterbeing hit by a drunk driver in Alabama,was the first person in the world toreceive a baclofen pump to control hismuscle spasticity following a traumaticbrain injury. His father, Tommy, said,“When Dr. Meythaler put an injectioninto Scott’s spine he relaxed and went tosleep. This was the first time I had seenScott completely relax since he came out
of his coma. Due to the assistance ofSenator Richard Shelby of Alabama, theprocedure was approved through theFDA in about six months.”
Currently, Dr. Meythaler is touting theuse of adult stem cell transplants to helpreverse paralysis. The surgery, calledolfactory mucosa transplantation, takescells from the roof of the nasal cavity andtransplants them to the spinal cord,where they transform into nerve cells andhelp repair injured tissue. Dr. Meythalerand Dr. Steven Hinderer, director ofSpinal Cord Injury Recovery at theRehabilitation Institute of Michigan, areusing successful patient cases to speedexperimental research like this.
“Spinal cord injuries and brain injuriesare extremely complex and there is nosingle silver bullet. Some of the best tra-ditional drugs we have in these areas areonly helpful to 10 percent of patients orthey only offer a slight benefit in theoverall reduction of injury. We need tofind better therapies to treat the com-plexities of these injuries,” Dr. Meythalersaid. “I believe the key is a series of treat-ments that are focused on different cellpopulations delivered at the proper timeafter injury.” �
The Brasza Outpatient Center located at the Rehabilitation Institute of Michigan is a26,000 square foot facility that houses orthopedic and sports medicine programs, women’srehab, and the Center for Spinal Cord Injury Recovery.
Our approach is to look at proven compounds, in analogoussituations, and then try to parallel that success with a newdelivery approach.
Medical student John Stasko says public health
John Stasko, a medical student and public health advocate, won an Outstanding Project Award from the American MedicalStudent Association for his People of Detroit exhibit, which uses photography to raise awareness of the uninsured and underinsured citizens of the city.
ˆ
ˆ

92005 Wayne Medicine
shattering the shame
By Amy DiCresce
visionaries are too far removed from those they serve
Doctors in Detroit know that health carecan get a little gritty. Thirty-eight year oldWayne State University medical studentJohn Stasko doesn’t shy away from thedark little secrets of inner city hospitals—
namely, patients who are homeless, uninsured,impoverished or severely ill. He sits with them, buysthem coffee, listens to their complaints about thesystem, photographs them, and most importantly,gives them a voice.
of the uninsured
ˆ

10 Wayne Medicine 2005
A staunch advocate for better public health services, Staskolives in a burned out inner-city neighborhood among the“undesirables” as they are often called and frankly, he is morethan a little frustrated at the health disparities and inadequatetreatment he witnesses regularly.
Rather than collapse under the weight of the situation, how-ever, he plugs away by competing for small grants, launching artexhibits, hosting conferences and initiating projects that shedlight on the problem of health care access. In the meantime, heis earning his medical degree so he can lend more than a voiceto disadvantaged citizens. He looks forward to the day when he
can lend medical expertise and the clout of medical colleagueswho can build a groundswell of support for meaningful change.
“The health care crisis here is huge,” said Stasko who has livedin several urban areas during his lifetime, most recently, Dallas,Albuquerque, New Mexico, and Washington D.C. “First of all,Detroit is a very segregated metropolitan city. The lack of amass transit system and the clear division between the havesand the have-nots means that people aren’t forced to interact.The bureaucrats and politicians who make decisions aboutfunding and health care coverage drive in from the suburbs,have their meeting, and get the heck out of the city. They don’tlive next door to these people. They don’t ride the bus withthem. If they did, I think they’d be a little more concerned aboutpublic health, because it would be more personal.”
For Stasko, it has become very personal. He recently debutedhis own photography exhibit called “People of Detroit: A LivingProject.” In it, he features photographs and excerpted interviewsin which citizens of Detroit share their experiences accessinghealth care services. With guidance from Marilyn Zimmerman,associate professor in WSU’s Department of Art and ArtHistory, and Maryjean Schenk, M.D., chair of WSU’sDepartment of Family Medicine, Stasko and collaborating
medical student Meegan Green used this exhibit to give a voiceto those frustrated and uninsured people whose input is usual-ly left unheard.
“Photography is used to explore and magnify the humanityof these average citizens, making their stories more alive,”Stasko said. ‘We are using photography for societal change.” Indoing so, Stasko learned that the necessary changes go farbeyond hospitals and medicine. A theme echoed throughoutthe interviews was this: The people who have trouble accessinghealth care tend to be people who also are unemployed or havemenial jobs, lack transportation, have bad credit, endure sub-
par housing and dangerous neighborhoods, arechronically ill and are often in pain.
One interviewed citizen summed it up this way.“[They are] spending millions of dollars on stuff wedon’t need. It’s as simple as that, you know, because weneed education, we need transportation, we need ourstreets fixed, we need our police officers, and that’s
where the issue’s coming in at, and that’s what my concern is.”Over and over again, Stasko’s project shows the faces of
Detroiters and the descriptions of their plight. There were manycommonalities that went far beyond health insurance.• “I broke my back three times in three places. I keep
respraining it and nobody will cover me.”• “I can’t go to the doctor because it will cost me money. I
keep getting those doctor bills that I can’t pay, got my creditall messed up and I am screwed for the rest of my life.”
• “I have never been more, how do I say, broke and homeless,beat up and robbed.”
• “I have a problem getting to a doctor because I don’t got adriver’s license. I don’t got a car, so I gotta take the buseverywhere or walk.”Dr. Schenk, research advisor on the People of Detroit project
and chair of family medicine, says, “These problems are regu-larly encountered by WSU physicians. Oftentimes, a patient’ssocioeconomic problems are either directly related to or exacer-bate the patient’s medical problem. While the physician is ableto work with the patient and reduce the professional fee associ-ated with the patient’s visit, there is no such mechanism for areduced fee for the medical tests and treatments that may be
... it shows incredible contrasts between theemployed and unemployed, the safe andunsafe, and the general disparate conditionof those with little or no income.
ˆ
ˆ
ˆ
ˆ
ˆˆ
ˆ

necessary to either cure or control the patient’s disease andsymptoms. It has been a great privilege and honor to work withthe medical students on this project. This project has height-ened our awareness of these issues and has brought in otherconcerned groups.”
In punctuating his point through art, Stasko paid attention toevery detail. In fact, the easels that were used to display the pho-tographs were made personally by Stasko out of rotten woodfrom abandoned houses in his neighborhood. And whether heknows it or not, his own compassion is seen in the care he showsfor his subjects. A former paramedic, auto company worker, sci-entific research consultant, dabbler in Russian studies, andholder of a Ph.D. in nuclear physics, Stasko himself is a study incontrasts.
“I thought initially that this exhibit would show the contrastbetween the insured and the uninsured. As it turns out, it showsincredible contrasts between the employed and unemployed,the safe and unsafe, and the general disparate condition of thosewith little or no income,” he said.
As written in his project description, Stasko says socioeco-nomic status is a fundamental cause of disease. “For example,the absence of grocery stores in poor neighborhoods reducesaccess to food products that are required for good health.Unsafe neighborhood streets and dumped materials influencepeople to stay indoors and reduce physical activity.Deteriorating neighborhood infrastructures erode social rela-tionships which might help protect against stressful life condi-tions. Low-income children are exposed to greater levels of vio-lence, family disruption and neighborhood crime.”
WSU School of Medicine Dean Robert R. Frank, M.D., feelsthat this medical school fills a critical gap in caring for the poorand uninsured. Although he’d love to see more resources madeavailable, he is proud of the school’s longstanding commitmentto the community. “When other institutions turned away unin-sured citizens, we took care of them. We did not turn our backson them,” Dr. Frank said. But the bottom line is this: “A kid inBloomfield Hills should not get more money spent on him thana kid in Detroit.”
The People of Detroit project has garnered much supportlocally, and public health officials are brainstorming ways to useit as a traveling advocacy piece on a national scale. “Somebodyeven mentioned that this had potential to grow like the AIDSquilt, where people in cities throughout the country would addtheir photos and personal experiences, and eventually, we’dhave this massive volume of personal experiences that could notbe ignored,” he said.
“The project is timely and urgent. National debate merelysimmers over universal health care, yet just as the debate seemsto start percolating, the field shifts and the public is bewilderedand must regroup. Solutions seem long in coming and weak ineffect. The city of Detroit itself tries to assemble its own PublicHealth Authority, yet is foiled by the unknown. Our project willbe a catalyst for change.” �
Following are excerpts from interviews with Detroit citizens about their health care experiences and issues.
“I broke my back three times in 3 places; and I keeprespraining it and nobody will cover me.”
“I have a problem getting to a doctor because I don’tgot a driver’s license; I don’t got a car so I gotta takethe bus everywhere or walk.”
I can’t go to the doctor because it will cost me money; I keep getting those doctor bills that I can’t pay; got mycredit all messed up and I am screwed for the rest ofmy life.’’
‘‘One of the basic issues that I believe that faces a lot ofthe young people in the state of Michigan, particularlyin Detroit, is air quality.’’
‘‘We get cold and hungry and lonely just like everyoneelse; you know we need love too; there it is.’’
of the people of detroitvoices
ˆ
ˆ
ˆ
ˆ
12 Wayne Medicine 2005
Grad studenttrades in field journal for
flow cyometer Sarah Krueger celebrates success in the cancer biology Ph.D. program
By Amy Dicresce

132005 Wayne Medicine
Sarah Krueger’s day job is a farcry from just a few summersago when she found herselfsnorkeling with stingrays inthe Florida Keys and calling
to frogs in mid-Michigan forests in thedead of night. As an undergraduate biol-ogy major with an interest in marinebiology, Krueger has since found practi-cality and application in a less out-doorsey, but equally fascinating area ofstudy—cancer and radiation biology.
Although canoeing and kayaking wereher real summer calling, she took a sea-sonal research assistant position in thelab of Dr. Kaladhar Reddy, upon the urg-ing of her brother who completed his
doctoral degree in that lab in 2002.Joseph Krueger knew that his self-described mildly obsessive-compulsiveand highly motivated sister would getcaught up in academic research. She did,of course, and was accepted into WSU’sPh.D. program the same year her broth-er finished.
“I just became fascinated with thebreast cancer research we were doingand I knew that this was a more broad-based and practical career path for me.I’m still a naturalist who’s interested inoceanic warming and protecting theenvironment, but I feel I can make a pos-itive impact in turning cancer patientsinto cancer survivors through my work,”she said.
Now Krueger works exclusively as agraduate research assistant in theKarmanos Cancer Institute’s RadiationBiology Department led by Dr. MichaelJoiner. Her research project concentrateson defining a link between overall cellsurvival and cellular proliferation fol-lowing low-dose radiation exposure.With mentoring from Brian Marples,Ph.D., Krueger is helping to find themechanism and proteins involved in thephenomenon that makes cells more sen-sitive to radiation therapy when they areexposed to lower doses.
“Low-dose hyper-radiosensitivity is aresponse in which cells die from agreater than anticipated sensitivity tosmall single doses of ionizing radiation,generally at doses less than 0.5 Gray. Webelieve this happens because of a three-component system of damage recogni-tion, signal transduction and damagerepair,” Krueger said.
Interestingly, the Joiner group hasfound cells are most sensitive to lowdoses of radiation during G2 phase, justbefore mitosis, which is the key elementof low-dose hypersensitivity underinvestigation by Krueger. For a briefwindow of time, there seems to be adelay in the cell cycle whereby DNArepair is allowed to occur, but in certaincells this response appears to be defec-
tive, which leads to reduced survival atlow doses of radiation. Much ofKrueger’s time in the lab is spent gettingcells into G2 phase in an effort to try andinducing the defined low dose responseand subsequent repair mechanisms forcritical investigation.
“Elucidating these processes will pro-vide a more complete understanding oflow-dose radiation sensitivity. We hopethat one day this research will allow fordesign strategies to overcome the activa-tion of radiation resistance, which mayimpact the evolution of clinical radio-therapy.”
Krueger has already presented keyfindings at research meetings in France,St. Louis and Toronto, and was awardedfirst-place in the 2004 Graduate StudentResearch Day at the WSU School ofMedicine. In recognition of her research,she has received a travel award, allowingher to attend additional meetings for theAmerican Association for CancerResearch (AACR) and the joint meetingof the Radiation Research Society (RRS)American Society for TherapeuticRadiology and Oncology (ASTRO). Infact, she has applied for an RRS scholar-in-training award and is expected to be afront-runner.
Dr. Marples can attest to the workethic and talent of Krueger. “Sarah is aself-motivating student with an affinityfor experimental research. She has a pas-sion for excellence that is evident in allher academic endeavors. On a more per-sonal level, Sarah’s well-developed senseof humor and sharp wit make her a plea-sure to work with.”
Krueger is expected to complete herPh.D. in 2006 and is considering severalcareer directions. She says she’s veryinterested in an academic career, becauseshe enjoys the teaching and learningsymbiosis of a university.
“In any case, I see myself near water,”she said. With her kayak and canoestrapped to the roof of her car, you maysee her between experiments somewherein Michigan or California or beyond. �
Sarah Krueger expects to complete her Ph.D. in 2006.
‘‘ I feel I can make apositive impact inturning cancerpatients into cancersurvivors throughmy work.’’

14 Wayne Medicine 2005
By incorporating advanced technology with a tra-ditional medical treatment, a multidisciplinaryteam of researchers hopes to offer a much-improved prognosis for children and older adultsliving with hydrocephalus, or “water on the
brain.” The team is developing a device that will sense increasesin pressure within the brain, control a valve in a shunt to drainthe excess cerebrospinal fluid (CSF) as necessary, and providewarning when the shunt needs replacement or an electronic“tune up.”
The proposed device, called a smart shunt, will be useful intreating the well-known infantile/children’s hydrocephalus aswell as the less-familiar condition called normal pressurehydrocephalus, which mainly affects older adults and mimicssome of the symptoms of Alzheimer’s disease. Both forms ofhydrocephalus can cause brain damage and sometimes death,said Pat McAllister, Ph.D., who is the principal investigator of
warns of wear and tear in the brain
BY L E S L I E M E R TZ
Electronic chip provides warning signal when shunt needs replacement or retuning
152005 Wayne Medicine
the research project and WSUprofessor of neurologicalsurgery. The research team, withguidance from Drs. Steve Ham(chief) and Sandeep Sood, pedi-atric neurosurgeons at the
Children’s Hospital of Michigan, is in the process of creating asmart shunt equipped with a tiny, pressure-sensing electronicchip built right into the shunt’s wall. It is also testing a numberof novel, neuroprotective materials that will discourage thebody’s typical inflammatory response, dissuade infection, andprolong the shunt’s lifespan.
“Children need the smart shunts for a couple of reasons,” saidDr. McAllister, who has studied the pathophysiology of hydro-cephalus for more than 20 years, and holds joint appointmentsin WSU’s physiology, anatomy and cell biology, and ophthal-mology departments. First, the currently used shunt frequentlybecomes obstructed when brain tissues grow over the deviceand into its draining holes. “This blockage usually leads to dan-gerous increases in intracranial pressure (ICP), which if nottreated quickly, can lead to escalating neurological deficits andsometimes death. The problem is that we do not have pressuresensors that can detect these changes con-tinuously and warn the physician in timeto prevent brain damage,” he said. A solu-tion is the implantable sensor and elec-tronic chip under development byGregory Auner, Ph.D., of the Departmentof Electrical and Computer Engineeringand a key member of the research team.Dr. Auner is also professor and director ofthe WSU Smart Sensors and IntegratedMicrosystems Program.
The researchers hope to embed this tiny,
1.0 mm x 1.0 mm x 0.25 mm electronic device in the wall of theshunt where it can detect rising pressure early on when it is theleast dangerous, Dr. McAllister said. Neurophysiologist PaulFinlayson, Ph.D., of WSU’s otolaryngology department, isassisting the project by directly measuring ICP in the brain andcomparing these findings with measurements reported by theprototype implantable sensors.
Once a blocked shunt is identified, the typical treatment is itsreplacement, also known as revision, Dr. McAllister said. Inmany patients, the revisions and associated surgery cause thenormally compliant brain to become stiff and inflexible, andtherefore even less able to absorb excess fluid or to withstandICP spikes. WSU chemical engineer Dr. Simon Ng and post-doctoral fellow Dr. Anfeng Wang are working on the root of thatproblem by coating the shunts with specially designed poly-mers. These materials discourage the tissue adhesion that makesthe revisions necessary in the first place.
Dr. McAllister’s lab is currently conducting 30-, 60- and 90-day in vivo studies to determine the biocompatibility andbiostability of the polymers. “Our preliminary results show thatsome of these coatings diminish the inflammatory response inthe brain as well as the amount of tissue build-up on samples,”
he said. The researchers, lead by postdoc-toral fellow Dr. Xuemei Liang, are alsoexploring the possibility of adding slow-release antibiotics to the coatings or to thesilicone wall of the catheter to resist infec-tion, a common problem with shunts.Together, these actions would prolong thelife of the shunt, thereby reducing thenumber of revisions, he said.
On a day-to-day basis, the smart shunt’ssensor would be able to monitor ICP con-stantly and control the shunt’s valve to
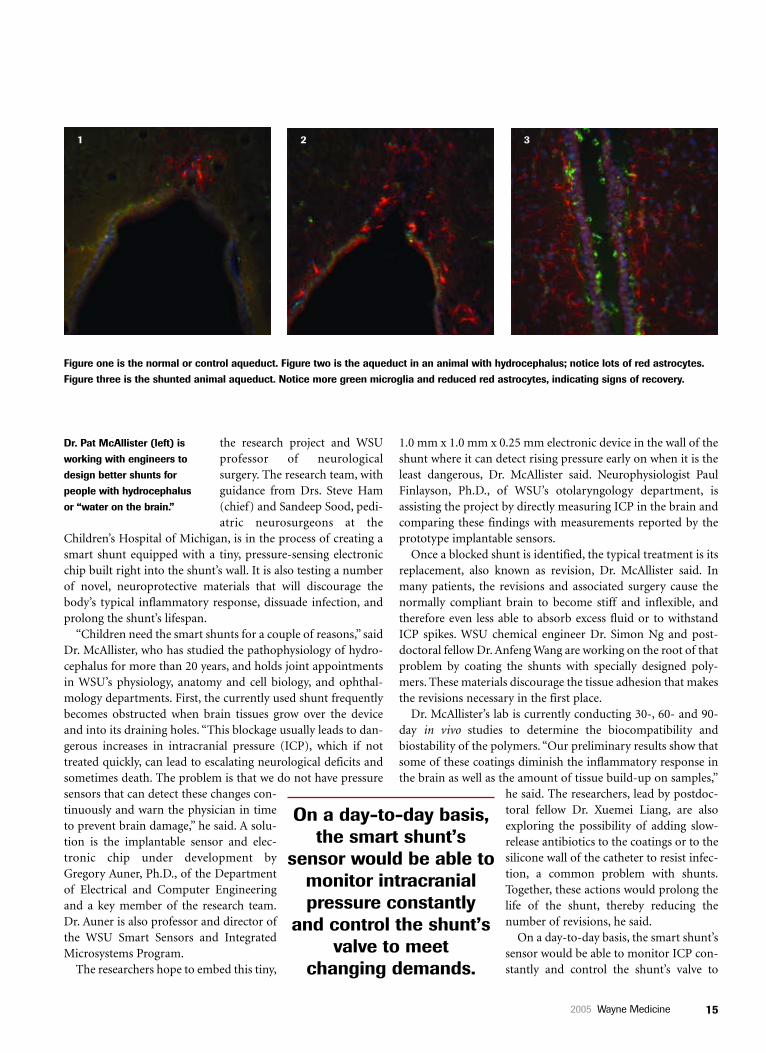
Figure one is the normal or control aqueduct. Figure two is the aqueduct in an animal with hydrocephalus; notice lots of red astrocytes.Figure three is the shunted animal aqueduct. Notice more green microglia and reduced red astrocytes, indicating signs of recovery.
Dr. Pat McAllister (left) isworking with engineers todesign better shunts forpeople with hydrocephalusor “water on the brain.”
On a day-to-day basis,the smart shunt’s
sensor would be able tomonitor intracranialpressure constantly
and control the shunt’svalve to meet
changing demands.
1 2 3

16 Wayne Medicine 2005
meet changing demands. He explainedthat plane trips, travel to areas with differ-ent elevations and therefore differentatmospheric pressures, and simple shiftsin posture from sitting to standing canincrease or decrease ICP levels and poseproblems for patients with currently usedshunts. A smart shunt, on the other hand,would give the patients newfound free-dom, he remarked, as well as a bigger safe-ty margin.
Older adults who develop normal-pres-sure hydrocephalus would benefit, too. In this condition, thepatient has a normal ICP for all but a few minutes a day, Dr.McAllister said. “These patients will spike a pressure in the mid-dle of the night, maybe for three minutes, and then it will goback to normal, which makes it very difficult to detect. What wenow believe is these spikes in pressure are just like some littleguy with a hammer banging on the roof of the cerebral ventri-cles (the chambers within the brain that house CSF). Over time,that gradually causes brain damage.” Some researchers believethree of every 50 patients with dementia actually suffer fromnormal-pressure hydrocephalus, and Dr. McAllister suspectsthe rate may be much higher. At any rate, he said, “It’s a signifi-cant problem.”
The transient nature of the ICP increases in this condition
has presented obstacles for its treatment.“It’s very difficult to design a CSF shuntsystem for people with normal-pressurehydrocephalus, because you don’t knowwhat their pressure is at any particularmoment,” Dr. McAllister said. “If, howev-er, we could have a pressure sensor in theshunt that’s draining the CSF, and thatsensor was feeding information back tothe valve, then we should be able to man-age their pressure changes much, muchbetter.” Some members of the research
team are also considering the possibility of adding pressure-sensitive proteins or other particles to the shunt’s walls, perhapsin lieu of a sensor chip.
Another potential addition to the shunt is one of drug-deliv-ery. “The main drug that we’re investigating is called minocy-cline, a derivative of tetracycline that has been shown in strokemodels and in some neurodegenerative disorders, likeParkinson’s disease, to inhibit inflammation,” he said. “It’s neverbeen tried in hydrocephalus, but it’s a very attractive candidatefor inhibiting the brain’s inflammatory response, and in partic-ular the accumulation of glial cells. During her graduate stud-ies, Dr. Janet Miller, now a postdoctoral fellow in the lab,showed that glial cells increase during hydrocephalus, and wesuspect this is one of the major reasons that the brain becomes
stiff,” he said. The research team is workingon new drug-delivery implants, possibly inconjunction with the shunts, that can conveymedications on an as-needed basis anddirectly to targeted tissues in the central ner-vous system.
The research team’s work will likely haveapplications beyond hydrocephalus, headded. “The drug-delivery system and, infact, all of the technology developed forhydrocephalus can also be used to improvethe treatment of many other medical prob-lems, including stroke, cardiovascular dis-ease, bladder and bowel dysfunction, andother neurological disorders, such as infec-tions, tumors, and brain trauma.”
Dr. McAllister credits the research group’ssuccesses so far to its multidisciplinarynature. “I had been thinking about a way toimprove shunts for many years, but it wasonly a year ago when I started talking toengineers that I realized it could actually bedone,” he said. “Now, with this multidiscipli-
nary approach, we can go all the way from the neurosurgeonswho are putting these things in the patients to the engineerswho are designing the implants. It has certainly allowed us tobuild a better team and make a meaningful clinical impact.” �
The researchers are exploring adding
slow-release antibioticsto the coatings or
to the silicone wall ofthe catheter to resistinfection, a commonproblem with shunts.
Dr. McAllister and postdoctoral fellow Dr. Janet Miller are workingon new drug-delivery implants that can convey medications on anas-needed basis and directly to targeted tissues in the central ner-vous system.

172005 Wayne Medicine
T he small, striped fish in Melody Neely’s four aquariaflash iridescent blue-green colors when the light hits
them just right. They may also hold the answers to some ofthe most common and deadliest of human pathogens.
Dr. Neely, assistant professor of immunology and microbi-ology, is using the 1.5-inch-long zebrafish as a model tostudy two streptococcal bacteria: Streptococcus pyogenes,which the media has publicized as the “flesh-eating bacte-ria”; and Streptococcus iniae, which once only infected fish,
Zebrafish bacteriaprovide pretty model
BY L E S L I E M E R T Z
Dr. Melody Neely learns about deadly strains of strep infections
The zebrafish in Dr. Melody Neely’s lab (above) provide a window into the progression ofstreptococcal bacteria in humans.
to study ugly
Zebrafish bacteriaprovide pretty modelto study ugly
18 Wayne Medicine 2005
but has recently jumped the species bar-rier to humans. “Streptococci are thecausative agents of a large group of dis-eases, a lot of them being fatal,” Dr. Neelysaid.
Streptococcus pyogenes affects morethan 20 million people a year in theUnited States alone, she said. Most of theinfections result in strep throat, a usual-ly short-lived condition that patientstypically describe as a severe sore throat,but sometimes the infections lead todangerous diseases, including necrotiz-ing faciitis, or flesh-eating disease, andstreptococcal toxic shock syndrome, orSTSS. Both have mortality ratesapproaching 50 percent, she noted.Necrotizing faciitis spreads very quicklyand results in massive tissue destructionaccompanied by fever and excruciatingpain, often ending in death within 24-48hours. STSS can lead to an extreme dropin blood pressure, organ failure, andother symptoms, and can result in deathin as little as 24 hours. “We want todetermine which pathogenesis mecha-nisms allow this to happen so rapidly,”Dr. Neely said. “If there were a way inwhich we could modulate one of themechanisms through either thepathogen or the host, we might be ableto develop a new therapy to combatthese very fatal diseases.”
Streptococcus iniae is troubling foranother reason. It was considered strict-ly a fish pathogen until 1995-1996, whenfour people in Canada became ill afterhandling infected fish. The infection ledto meningitis, septic arthritis, cellulitis,fever, confusion, and/or endocarditis inthe patients.
Dr. Neely believes an understanding ofthe mechanisms used by the two bacteriato infect and proliferate in zebrafish willalso provide a window to their progres-sion in humans. “There are lots of rea-sons we’re using zebrafish,” Dr. Neelysaid. “First, the genome for the zebrafishwas recently sequenced. Now that weknow all of the genes that are in the
organism, we found that zebrafish have avery similar genetic makeup to mam-mals, which is quite interesting. Thesefish also have a very well-developedimmune system, including all of theimmune-type molecules that humansdo, so they respond (to bacterial infec-tion) in the same way.” For many dis-eases, including those she is studying, thefish’s symptoms even parallel humansymptoms. In addition, zebrafish areinexpensive, easy to keep, and the perfectsize for study. “One ofthe biggest advantagesis that they’re about1.5 inches long, whichmeans you can take anentire transverse orlongitudinal section ofa zebrafish and put iton a single microscopeslide. Since we canthen look at the wholebody in a single ani-mal, we can see the site
of the initial infection, as well as whereand how it spreads throughout the bodyat different time points.”
Dr. Neely’s team is studying 1) howthe bacteria initially colonize a host; 2)what genes are involved in causing dif-ferent outcomes, such as systemic vs.localized necrotizing disease; and 3)which interactions occur between thepathogen and the host tissue. The last isparticularly challenging, she said. “Welook at it this way. In infection, bacteria
The zebrafish is an excellent animal model —and one of the few animalmodels available — to studythe progression ofmeningeal disease.
The zebrafish is an excellent animal model —and one of the few animalmodels available — to studythe progression ofmeningeal disease.

192005 Wayne Medicine
find themselves in a new environmentonce they come inside the host. Theysense the environment and based on thatnew environment, they change theirgene expression so they can survive. Thehost then senses the presence of the bac-teria and upregulates its own defenses,such as cytokines, oxygen radicals andlysozymes, to combat the invadingpathogens.” The battle doesn’t end there,she said. “Now the bacteria have to fightoff all these other molecules that are try-ing to kill them, so they have to changetheir gene regulation again to survivethat onslaught.”
Neely’s in vivo system captures all thesubtle steps in this complex, back-and-forth exchange. “In our live system, wenot only get to look at that dynamicinterplay between the host andpathogen, but we also have the opportu-nity to look at multiple tissues, and that’sparticularly important in systemicpathogens like these that can disseminatefrom the site of infection to multiple
organs and tissues within the body,” shesaid.
To determine the role of host andpathogen in disease progression, Dr.Neely’s research group, which includesfour graduate students and a technician,makes a random or a targeted mutationto shut down genes in the bacteria, andthen screens the mutated bacteriathrough the zebrafish to find those thatno longer cause disease. This way, theycan deduce which genes are essential todisease progression. “Then we look atwhat’s known about the gene or aboutthe protein that it makes to determinewhat role it plays in the disease process.”She and her research group have alreadyidentified several genes with thismethod and are now doing additionalin vitro experiments to home in on theirspecific mechanisms.
On the host side, the researchers are
concentrating on immune factors andtheir effects on the course of the disease.One method involves placing the fishunder a stress condition, which is knownto dampen the immune response in fishand in humans, and testing whether thefish are more susceptible to disease evenwhen disease-related genes are knockedout.
Pictured is Dr. Neely’s fluorescent micrograph of intracellular (green) and extracellular (red) streptococci with RAW 264.7 macrophages.
An understanding of the mechanismsof S. iniae and S. pyogenes infections mayhave implications beyond flesh-eatingdisease and STSS, she remarked. “S. iniaehas shown similarities to another set ofhuman pathogens, called group B strep-tococcal bacteria, which cause meningi-tis in human newborns and have a simi-lar effect on zebrafish. This makeszebrafish an excellent animal model —and one of the few animal models avail-able — to study the progression ofmeningeal disease. In addition, thesebacteria have gained notoriety the last 10years for causing systemic and bac-teremic infections in the elderly and inimmunocompromised human patients.”
The work will also likely extend toother gram-positive bacteria, such asListeria and Staphylococcus. “We’re hop-ing that by using the zebrafish and our invivo model, we can look at general infec-
tion pathways that all of the gram-posi-tive pathogens use. Since these pathwaysseem to be highly conserved, we’re hop-ing that we can use the zebrafish and ourin vivo model to determine how the gen-eral infection pathways work. If we candetermine what the mechanisms are, wewould be able to devise strategies tocombat multiple species.” �
Streptococcus pyogenes affectsmore than 20 million people a year inthe United States alone. Most of theinfections result in strep throat, butsometimes the infections lead todangerous diseases.
Streptococcus pyogenes affectsmore than 20 million people a year inthe United States alone. Most of theinfections result in strep throat, butsometimes the infections lead todangerous diseases.
20 Wayne Medicine 2005

212005 Wayne Medicine
No cancer is pretty, but head and neck cancers are literally in your face,so there is greater potential for the problems to become downrightugly. Continuing a long-history of medical innovations, researchersat Wayne State University and the Karmanos Cancer Institute arehelping cancer patients live longer lives and avoid cosmetic and func-
tional deformities by advancing new treatment standards.Organ preservation and combined chemoradiation therapies form the core philos-
ophy of the WSU/Karmanos head and neck cancer team which includes Drs. JohnEnsley, professor of internal medicine/oncology, John Jacobs, professor of otolaryn-gology, and Harry Kim, assistant professor of radiation oncology. The team is aresearch powerhouse that gets published in the most prestigious medical journals,challenges dogma with their presentations at national research meetings and sets newagendas for treatment standards with their research protocols. Most importantly, theybring their work directly to cancer survivors, significantly improving the way theylook, talk, eat, breathe and live.
Head and neck cancers are hard to ignore. They can affect the oral cavity (mouthand tongue), oropharynx (the middle of the throat), salivary glands, larynx (voice-box), nasopharynx, (air passageway at the upper part of the throat), the nose, or theparanasal sinus cavities around the nose. This disease set is particularly uncomfortablebecause it aggravates sensitive areas that are used for base functions like eating, swal-lowing and breathing.
For decades, WSU and Karmanos researchers have tested new therapies in an areaof cancer that has gone largely ignored. “In the past, conventional therapy consisted ofthe surgical removal of the cancer-ridden organs as primary treatment. Many peoplelost their voice boxes, or other organs important for swallowing such as the tongueand throat tissues,” Dr. Ensley said. As director of the medical oncology portion of thehead and neck cancer multidisciplinary team, he is championing new treatment stan-dards and urging clinicians to use chemotherapy and radiation in combination to stop
By Amy DiCresce
Dr. John Ensleyurges clinicians touse chemotherapyand radiation incombination to stopcancer growth andto preserve theorgans wheneverpossible
Doing the double-take of chemo and radiation
Head and neck cancers are hard to ignore. They can aggravate sensitive areas that are used for base functions like eating,swallowing and breathing.
Aggressive combination therapy radically improves outcomes for head and neck cancer

22 Wayne Medicine 2005
cancer growth, and to preserve the organswhenever possible.
“Take breast cancer, for example. Ittook 20 years to stop doctors from per-forming mastectomies as primary treat-ment for breast cancer. With the help ofDr. Bill Powers, in fact, from our ownRadiation Oncology Center, we got statelaws passed requiring surgeons to pro-vide non-surgical radiation options thatwould treat the cancer and preserve thebreast. We are undergoing similar battlesnow as we have defined alternative, non-surgical therapies to treat squamous cellcarcinomas of the oral cavity, pharynxand larynx. These treatments are beingaccepted as new standards and are slowlybeing instituted in cancer clinics acrossthe country.”
These regimens have also improved theoutcome for patients who still undergosurgery as the primary treatment fortheir cancers. In May 2004, Drs. Ensley,Jacobs and Kim co-authored a NewEngland Journal of Medicine report estab-lishing a combined regimen ofchemotherapy and radiation followingsurgery as the gold standard for high-risk, advanced stage squamous cell carci-noma of the head and neck. This nation-al phase III trial enlisted the participationof 459 patients through the U.S.A. Headand Neck Cancer Intergroup and was
administered by the Radiation TherapyOncology Group. The need for aggressivetreatment has been critical, because evenafter surgical removal of affected areas,these high-risk cancers in the head andneck frequently recur in the originaltumor bed. Patients who had chemora-diotherapy (combined treatment) post-operatively did better than those withonly radiotherapy in local and regionalcontrol (no recurrence) and disease-freesurvival.
This study and a similar trial conduct-ed in Europe with corresponding results,including improvements in overall sur-vival, are just two in a long list that vali-date the work begun by Drs. Ensley andJacobs and the head and neck cancermultidisciplinary team in the 1980s. Atthat time, they piloted head and neckcancer studies combining thechemotherapy drug cisplatin with con-tinuous infusion 5-fluorourcil (5-FU)which has been called “the Wayne Stateregimen.” They proposed this protocolbecause a similar approach usingchemotherapy and concurrent radiationworked so successfully for anal squamous
cancers in the 1970s in a study led by Dr.Vainutis Vaitkevicius, who is now presi-dent emeritus of Karmanos.
According to Dr. Jacobs, they believedconcurrent radiation and chemothera-pies would make cancer cells more sus-ceptible to radiation and destroy moretumor cells. The results of this post-oper-ative Wayne State regimen were first pre-sented in 1989 at the American Society ofClinical Oncology meeting. This concur-rent regimen has been tested at the coop-
erative and now the intergroup levels inthe past decade in esophageal cancer, lar-ynx and pharynx, and tongue cancer aswell as nasopharyngeal tumors. In eachlarge scale study, this regimen has provid-ed improved survival and/or organpreservation.
“These chemotherapy regimens werefirst identified and tested right here atWSU. They were subsequently taken tonational cooperative groups where, basedupon the WSU data, phase III trials wereconducted resulting in new national andinternational standards for the treatmentof all groups of advanced stage head andneck cancers. These studies have resulted
in WSU being inter-nationally recog-nized for its exper-tise in head andneck cancer,” Dr.Jacobs said.
In November2003, Dr. Ensley
was senior author on another NewEngland Journal of Medicine study usingthe WSU cisplatin-radiation regimen forlaryngeal preservation and regional con-trol. The results of the trial showed a 20percent reduction in the number ofadvanced-stage patients requiringremoval of their voice box compared toradiation alone. Most recently, theSouthwest Oncology Group, usingWayne State/Karmanos Cancer Centerregimens, reported successful organ
Radiation oncologist Dr. Harry Kim has expertise in treating advanced and unusual cancers in the head and neck.
We have defined alternative, non-surgical therapies to treat squamous cell carcinomas of the oral cavity, pharynx and larynx.These treatments are being accepted as new standards and arebeing instituted in cancer clinics across the country.
232005 Wayne Medicine
preservation for advanced cancer of thetongue (70-80 percent) and hypophar-ynx (50 percent). “This is significantbecause we are making strides in improv-ing patients’ quality of life and avoidingdysfunctional surgery,” Dr. Ensley said.
Although these trials have resulted innew standards of therapy, Dr. Ensley said,challenges still remain. The combinedtherapy presents high levels of toxicityand can produce severe adverse effectsranging from dry mouth, pain, and tastedysfunction to serious infection of themucosal lining and fatal toxicity. Thepeople who benefit most from chemora-diation are those with late-stage, high-risk cancer for whom the benefits ofaggressive therapy generally outweigh therisks. Dr. Ensley said that these head andneck cancers are usually discovered lateand therefore run a high risk for prob-lematic cosmetic and functional conse-quences from both the tumor and con-ventional treatment. In these cases,aggressive treatments, both surgical andnon-surgical, are the only hope.
“Advanced head and neck cancerremains a therapeutic challenge and thecollaboration of multidisciplinary teamsis, more than ever, essential,” Dr. Jacobssaid. “The technological development ofnew radiological and biological tools,coupled with the introduction of newcytotoxic and non-cytotoxic compoundsoffer encouraging possibilities.”
Dr. Kim, the radiation oncology experton the team, is trying to overcometumors that respond poorly to the cis-platin-based chemotherapy. “In sometumors, pre-exposure of head and necksquamous carcinoma cells to photonradiation increases resistance to subse-quent cisplatin treatment. Similarly, cis-platin-resistant tumors also respondpoorly to subsequent photon radiationtreatment. We are trying to learn moreabout the molecular basis underlying cis-platin and photon radiation resistanceand hope to design more multimodalityprotocols to answer these questions,” Dr.Kim said.
The Radiation Oncology Center offers
state-of-the-art photon radiation treat-ment techniques such as intensity modu-lated radiation therapy (IMRT), intersti-tial brachytherapy, gamma knife radio-therapy, and neutron radiotherapy,which is available in only two centers inthe U.S.
“With such unique therapeutic capa-bilities, the Radiation Oncology Center isnot only a major referral center through-out the state of Michigan, but also fromout of state for many difficult-to-treat,advanced and unusual cancers in thehead and neck,” Dr. Kim said.
The head and neck multidisciplinaryteam is leading some of the national clin-ical research cooperative groups such asRTOG and SWOG, and is pioneeringinnovative treatments such as periopera-tive p53 gene therapy and a newchemotherapy of cisplatin and taxoterewith radiation therapy.
The team continues to build uponhead and neck cancer treatment develop-ments that have advanced at WSU andKarmanos through the decades. �
Dr. John Jacobs takes pride in WSU’s leadership role in developing cancer protocols and taking them to nationalcooperative groups where they are testedand established as gold-star treatments.

24 Wayne Medicine 2005
Dr. Hamzavi believes physicians should be more active in combating poverty andinadequate health care access for theirpatients; otherwise, they’re just leaving the situation for the next generation ofyoung doctors with no end in sight.
Dr. Hamzavi believes physicians should be more active in combating poverty andinadequate health care access for theirpatients; otherwise, they’re just leaving the situation for the next generation ofyoung doctors with no end in sight.

252005 Wayne Medicine
“Our dermatology clinic takes 25 percent of the uninsured inMichigan. There were days when we would have 120 patientsduring a three-hour clinic and we would have to pick whichones to treat. I had to wonder, is this the United States or is thissub-Saharan Africa?” said Iltefat Hamzavi, M.D., WSU clinicalassistant professor of dermatology. He is also a co-founder andinterim executive director of a Michigan-based think tank,known as the Institute for Social Policy and Understanding(ISPU). “Physicians need toengage in discussions of whythese patients show up atour doorsteps. We need totake the initiative to do morethan put a Band-Aid onwhat is a systemic problem.”
Toward this end, Dr.Hamzavi and the ISPU havepartnered with WSU’s PaulToro, Ph.D., an internation-ally known expert in home-lessness issues, to raiseawareness of the plight ofthis large segment of societyand to spur policy changes.
Dr. Toro summarized theproblem: “On the one hand,we as health care profession-als can complain about how(people who are homeless)are underinsured or unin-sured, and they’re difficultto deal with, and they cost usmoney, but from my stand-point, they’re underserved. I
don’t care that they’re uninsured. They are people in our soci-ety who are dramatically underserved.”
His recent study of homeless adults in Wayne County illus-trates the problem. “If you look at this representative sample ofhow many health problems they have on average, you will bequite amazed,” said Toro, WSU associate professor of clinicalpsychology. “About two thirds of these people report at least 10health problems in the last six months. This is out of a checklist
of 50–60. Half of those peo-ple have 10 to 19 healthproblems, another thirdhave more than 20, and 13percent have 30 or morehealth symptoms.” Just oneor two of the milder symp-toms on the checklist wouldbe enough to send mostpeople to the doctor’s office,he noted, but homeless peo-ple typically lack thatoption. “Their health prob-lems stem from extremepoverty, living on thestreets, not eating well, anda lack of access to healthcare. They have a very hardlife.”
Dr. Toro is now compil-ing his findings into a seriesof policy briefs which willbe publicized by the ISPU,Dr. Hamzavi said. The first,which is now availablethrough the ISPU website
Dr. Hamzavi advocates for homeless and impoverished people through the Institute for Social Policy and Understanding
BY LESLIE MERTZ
FOR UNDERSERVED PEOPLE
THINK TANK SPURS ACTION

26 Wayne Medicine 2005
(www.ispu.us), is titled “Foster Care: A National Problem.” Theeight-page document lists numerous steps to prevent the 20,000U.S. children who “age out” of foster care each year from wind-ing up homeless, as so many of them do. “The ISPU likes to takeon issues that most people don’t put a lot of resources andthought into, and homelessness in America is one of them,” Dr.Hamzavi said.
The ISPU originated a few months after the fall of the WorldTrade Centers in September 2001, when Dr. Hamzavi and 10other concerned individuals, including then-Congressman andnow WSU professor David Bonior, began discussing percep-tions of Muslims in the United States and particularly inMichigan, where many live. The dia-logue soon expanded to U.S. policy andhow well it reflects the issues facing itsMuslim citizens, as well as Americansof other minorities. “I’m a nativeMichiganian, and a lot of the people Iknow are native Michiganians, butwe’re not all Caucasians or all AfricanAmericans. We come from differentbackgrounds, and we want a voice inthe way the country and the communi-ty are shaped. We simply want to pro-vide ideas about how we can possiblylive in the future, and that’s what athink tank does.” Headquartered inClinton Township, the ISPU definesitself as an independent, nonprofit, research organization com-mitted to studying U.S. domestic and foreign policy. It now col-laborates with about 30 scholars, including Dr. Toro, on issuesranging from politics and religion to genetically modifiedfoods.
One of the ISPU’s first major efforts was a national confer-ence, called “Islam in America,” which was jointly hosted by theISPU and the WSU College of Liberal Arts and Sciences. “Wegot a lot of scholars as well as policy makers to come down, andwe had a simultaneous press conference in Washington, D.C.,and Detroit. That conference brought a lot of internationalrecognition for the university,” Dr. Hamzavi said. Afterward,college dean Robert L. Thomas and development officer SusanEmfinger approached Dr. Hamzavi about working with Dr.Toro to disseminate his research findings and recommendationsto key policy makers. The idea struck home, Dr. Hamzavi said.“We have always talked about how ISPU could encourage a pol-icy of inclusion in our country, and Detroit especially, and thattheme was continued with the poverty/homelessness issue.
Now, Dr. Toro writes these policy briefs based on his research,and we create the forums for him to express himself and tellpolicy makers what’s happening.”
While Dr. Toro is working on additional briefs for the ISPUin the hopes of swaying national policy, he encourages the med-ical community to do its part, as well. During a recent presenta-tion to first- and second-year medical students at Wayne State,Dr. Toro reminded them of their obligation to society. “Thereality is that all people who go to medical school are subsi-dized, and those at a public university, like Wayne State, areheavily subsidized. They get a pretty low tuition for what thetraining costs,” he said, adding that he also reaped the rewards
of subsidization through his doctoralprogram in clinical psychology. “I don’twant to guilt-trip people too much, butthe reality is that we owe society. Weshould give back to society in someway, and we should do pro bono work.Perhaps we can give free care everymonth to help indigent people, like Dr.Hamzavi does. It’s a good thing, and Ithink all physicians should do it.”
Dr. Hamzavi also urged medical pro-fessionals to become active advocatesof policies that will solve or at leastreduce poverty and homelessness. Thelong-term benefits are many andinclude improved medical care overall.
“Here in the Detroit Medical Center, for example, a lot of ourproblems with patients are due to the poverty issue. For exam-ple, if your child has a little rash, you go see a doctor. Well, if youhave no access to care, or you don’t have the transportation toget to a doctor, that little rash can progress and get infected, andsuddenly that child has this horrible condition, can no longer goto school, and ends up being admitted to the hospital. This allcould have been avoided if we had treated it in the early stages.”The medical community currently faces such cases as they arise,he said, but such crisis management is not enough. “As medicalprofessionals, we’re the end game, but we need to know whatcaused this and what things as a community we can do to pre-vent it from happening.”
He added, “If those things aren’t addressed, it becomes up tothe physician to handle social issues on a case by case basis. Heor she can handle this for only so long, and after a while movesto the suburbs and enjoys a nice life, leaving the situation for thenext generation of younger doctors to face. And the people whosuffer the most are the patients.” �
I don’t want to guilt-trippeople too much, but the
reality is that we owe society. Perhaps we can
give free care every monthto help indigent people,like Dr. Hamzavi does. It’s a good thing, and I think all physicians
should do it.
272005 Wayne Medicine
Practice makes perfect is a fine motto for some professions. Baseballplayers take batting practice before the big game. Chefs sample andtaste recipes before serving them in restaurants. But where is thepractice field for doctors to treat sick people? How do they rehearsebreaking bad news to loving families? How do they learn to interpretthe pumping and breathing sounds they hear through a stetho-scope? And how many patients are willing to see a doctor at the
practice stage of their training rather than the expert phase? Approximately 300 people at Wayne State University have proven that they are
happy to be practice patients for novice doctors. In fact, they even get paid for itthrough an innovative Standardized Patient Program, directed by Ron Spalding andcoordinated by Maurice Kavanagh in the School of Medicine’s Conjoint Teaching
By Amy DiCresce
Act like a better doctor, be a
Better Doctor
Standardized patients provide safe environment for medical students to perfect clinical skills
Standardized patients provide safe environment for medical students to perfect clinical skills

28 Wayne Medicine 2005
Services. Spalding andKavanagh train people to playpatient roles with specific setsof symptoms and specificmedical histories that are pre-sented to medical students fordiscussion and diagnosis. Theprogram ensures that all stu-dents have uniform trainingand acquire the necessary clin-ical skills.
Lori McParlane was an office managerand nursing student when she was turnedon to a new part-time job at WSU: a stan-dardized patient (SP). One of her firstassignments was to play the part of Ms.Cooper, a fast-living woman with multi-ple risk factors for heart disease. The Biclighter sticking out of her pocket was adead giveaway that she was a smoker, andit served as a planted cue to prompt med-ical students to ask questions about herhealth behaviors and health history.
“The students are grateful that theyhave a safe place to practice and get out
their jitters and anxiety. For me, it is real-ly enriching to know that I am helping totrain the next generation of physicians. Iam able to guide doctors to better meetthe needs of patients like myself,” saidMcParlane who is no longer a standard-ized patient, but an administrator and SPinstructor for WSU. She helps train SPteaching associates—another level of SPswho not only present scenarios, but alsooffer students guidance, evaluation andpersonal instruction during their focusedphysical examinations.
Since 1971, WSU has used lay per-formers for courses in patient interview-ing and history taking. Beginning in1995, SPs were used much more exten-sively for the Objective StructuredClinical Exam (OSCE), a hands-on test ofclinical skills that students take at the end
of their third year. This exam not onlytests the students’ clinical abilities, butalso prepares them for the Step 2 ClinicalSkills Exam they are required to pass aspart of the United States MedicalLicensing Exam. Through the mid 1990s,standardized patient experiences wereformally integrated throughout the med-ical curriculum to teach students infor-mation gathering, diagnostics, clinicalmedicine, interpersonal communicationskills, physical exam techniques, compas-sion and professionalism. Now, Spalding,Kavanagh and McParlane tailor a variety
of SP programs for training residents,genetic counselors and other health careworkers throughout southeast Michigan,in addition to their work with medicalstudents.
In fact, Spalding and Kavanagh havebuilt a true academic research and med-ical education specialty out of the SP pro-gram. They are among the foundingmembers of the Association ofStandardized Patient Educators (ASPE),an international group that publishesresearch on the validity and methodologyof such training programs. The demandfor this reliable teaching tool is continu-ally growing, particularly as core clinicalcompetencies are required and assessedby the Accreditation Council forGraduate Medical Education and otheraccrediting agencies.
Spalding said SPs enhancestudent education, becauseyou can’t always count on thefull spectrum of learning whenyou observe patients in a hos-pital setting. “The SPs are notactually sick or worried abouttheir care. They won’t getwhisked out of the room for anx-ray or feel too groggy from
surgery to undergo an evaluation.Teaching efforts can be concentratedmore on student learning rather than theside effects of the sick patient’s condition.And the situation is a little more compre-hensive and predictable,” he said.
Student David Edwards said it didn’tmatter that the SP wasn’t a “real patient”he examined during the musculoskeletalportion of his training. “It’s a body you’reexamining. That’s what counts most. Itdoesn’t matter if it’s in a hospital or asimulated doctor’s office. I just need tolearn the range of motion tests, theanatomy and the techniques. I see this asa way to learn the mechanics of doctor-ing.”
Andrea O’Boyle agreed saying, “In thehospital, you see what’s wrong withpatients, but it’s hard to see what’s right.This helps us learn how a normal physi-cal exam should be.”
From a bank of video monitors downthe hall, Dr. Michael Stellini, professor ofinternal medicine, can watch the student-patient interactions and jot down notesfor discussion and feedback after theencounter. Whether they are being evalu-ated on their interviewing skills or tech-nical clinical skills, each student has achecklist of things he or she must com-plete. If the faculty member sees that astudent is weak in a particular area, thestudent can get access to “master clini-cians” through extra time spent in train-ing situations. And, because the interac-tions are videotaped, the student canreview his or her own skills.
“This interactive learning experience isvaluable for the students and the faculty.In the hospital, students generally justobserve and report what they learn to theresidents. Here, they practice, they feel a
The students are grateful that they have a safe placeto practice and get out their jitters and anxiety. Forme, it is really enriching to know that I am helpingto train the next generation of physicians.
Medical student Ticaria Jackson perfects her examination skillson Lori McParlane who worked as a part-time standardizedpatient for WSU and is now an instructor and administrator forthe SP program.

292005 Wayne Medicine
person’s joints to check for inflamma-tion, they learn to take a proper bloodpressure, they listen to heart sounds, theyexamine the body from head to toe, andthey begin to learn how the systems ofthe body work together,” he said. “Theybegin to assess the difference betweenwhat a normal baseline is and what mightbe suspicious.”
There are many indications that thetraining works. In fact, this semester, aparticularly observant student heard amurmur or abdominal bruit in an SPthat could be indicative of an aortic flowproblem. “After listening to these normalsounds a few times, he discovered some-thing that just didn’t sound right,” DrStellini said. “I went over to take a listenand the student was right on.” While SPexams are not meant to be diagnostic orto take the place of professional medicalcare, this is an instance where discoveryreally benefited the SP and it was a trueindication that the training worked forthe student.
Another advantage of standardizedpatients is the predictability of the train-ing experience, regardless of geographiclocation. Beginning with academic year2002-2003 a new course called ClinicalMedicine was introduced into the firstyear curriculum. As part of the course,10-12 students are assigned to a smallgroup to get an introduction to theknowledge, skills and attitudes needed inclinical practice. Course facilitators are
made up of faculty and volunteer com-munity hospital physicians. This means,faculty members are training WSU stu-dents in more than 20 sites from AnnArbor to Pontiac. SPs can go to these off-site locations and accommodate training.This cadre of SPs, known colloquially asthe Parachute Club, are assigned to rotatebetween sites and “parachute” into theteaching setting as needed.
SPs in the Parachute Club bring rating
forms and other supplemental materialsas needed to aid with the exercises. “Bothfaculty and students have reacted favor-ably to these interactions, citing as most
beneficial the opportunity to practiceinterviewing skills and techniques in asafe non-threatening environment. Andthey value the patient generated feed-
From a bank of video monitors down thehall, instructors can watch the student-patient interactions and jot down notes fordiscussion and feedback after the encounter.The Standardized Patient Program, directedby Ron Spalding and coordinated byMaurice Kavanagh, ensures that all WSUmedical students have uniform training andacquire the necessary clinical skills.
WSU’s pool of standardized patients include people from all walks of life—teachers,auto workers, nursing students, aspiring actors, volunteers, and a host of other part-time job seekers who feel like doing something interesting and valuable to the com-munity while earning $10-$14 per hour. No medical expertise is required and all
training is done by qualified WSU faculty.If you would like to learn more about participating in the Standardized PatientProgram, please call (313) 577-1414 or visitwww.med.wayne.edu/conjoint/sp_programs/index.asp.
Could you play the role of
standardized patient?

30 Wayne Medicine 2005
back,” Kavanagh said. “In fact, the stu-dents who don’t get an SP experienceand have only ‘real’ clinic or hospitalpatients have commented that they areat a disadvantage. Clearly, the SPs play anecessary role in education. Our stu-dents and faculty are requesting themregularly now.”
Professor Anne Greb in the Center forMolecular Medicine and Genetics hasincorporated SP methodology into thecurriculum of the genetic counselingprogram to help monitor students’progress in developing the nationallydefined practice-based competencies.The first SP encounter, a pregnantwoman at risk of carrying a gene muta-tion for Duchene Muscular Dystrophy,occurs at the end of the first semester.The second encounter, which occurs atthe end of the second semester, involveshaving the same patient return to reviewher carrier results. Students are expectedto present “bad news” genetic testresults, provide appropriate informationon risks and management, and address
Students say patient actors help them learn the mechanics of doctoring.
The new Richard J. Mazurek, M.D.,Medical Education Commons to bebuilt adjacent to the ShiffmanMedical Library will house theexpanding Standardized PatientProgram. With more than 20 roomsequipped with audio and videoequipment, students will be able topractice their clinical skills and laterreview them with advisors and facultymembers. Eventually, all students willcreate their own learning portfoliosthat will contain video footage of thework they’ve accomplished and theskills they’ve learned. This will be oneof the largest clinical skills labs in thecountry and will be a teaching toolfor medical educators and healthcare workers across the state.
The new Education Commons willalso house other educational toolsincluding computerized patient simu-lators similar to those in the pharma-cy program, and life-like models thatallow students to perfect basic skillslike suturing, intubation, giving injec-tions, CPR, etc.
If you’d like to support this programwith a contribution to the EducationCommons, please contact the Schoolof Medicine’s Office of Developmentand Alumni Affairs at (313) 577-1495.
psychosocial, coping, support, and dis-closure issues as appropriate. The com-plexity of psychosocial and other con-founding factors incorporated into theSP portrayal, is increased with eachencounter.
In a pilot study to test the program,Greb found the following to be true.
“The results from the first encountershowed that students’ communicationskills were on target. However, their skillsrelated to taking targeted family history,understanding the importance of con-firming a diagnosis, and nondirectivecounseling were not, prompting specificcurriculum adjustments. Overall, the useof SP encounters has been valuable inhelping us determine if our curriculumgoals, with regard to clinical skills devel-opment, are being met,” Greb said.
The Standardized Patient Program isa true test of our curriculum, Spaldingsaid. “We can make sure our futuredoctors are getting the right messages,the right information and the righttraining.” �
In the hospital, you see what’s wrong with patients,but it’s hard to see what’s right. This helps us learnhow a normal physical exam should be.
The new Richard J. Mazurek, M.D., MedicalEducation Commons will house theexpanding Standardized Patient Program.
Medical EducationCommons to houseSP program

312005 Wayne Medicine
Graduate student Stefanie Roshy is on to some-thing big. In the past, scientists wonderedabout the importance of proteases; but nowtheir complexity has been validated and Roshyis part of the exploration.
“We know now that proteases are more than just housekeep-ing genes. My particular work has elucidated their importancein the development of the normal mammary gland and theprogression of breast cancer,” Roshy said. This work won herfirst place in the 2004 Graduate Student Research Day and itfuels multiple career opportunities when she completes herPh.D. later this year.
Under the tutelage of Bonnie Sloane, Ph.D., professor andchair of pharmacology, Roshy is learning her trade thoroughlyand is being recruited by several members of the proteolysisresearch societies across the country. Research on proteolyticenzymes, their inhibitors, and their substrates has grown to thepoint where it has become difficult to keep up to date, and newresearchers like Roshy are being welcomed into the field.
Roshy uses a 3D in vitro system to look at the roles of cys-teine proteases, specifically cathepsin B and matrix metallopro-teinases (MMPs), in the malignant progression of cancer in themammary acini, or parts of the breast glands where milk andfluid is produced. By learning moreabout selective inhibitors, she and hercolleagues hope to find ways to blockcancer progression.
With the supportive and assertiveDr. Sloane guiding her research, Roshy
has already made more than a dozen research presentationsfrom Colorado to Slovenia to Japan. She has co-authored aCancer Research article, a review article in Cancer MetastasisReviews and a handful of abstracts, and has been honored as ayoung investigator several times by her peers.
“I was scared to death the first time I had to present myresearch in front of all these senior investigators, but now I amvery comfortable with it. I’ve learned a ton about my fieldbased on input and feedback from colleagues and I’ve learnednew and interesting avenues to pursue with this work,” Roshysaid.
Roshy is exploring opportunities for post doctoral positionsand interviewed at a few labs at the National Institutes ofHealth. Newly married to a patent lawyer, Roshy said she andher husband would love to live in the Washington D.C. area forboth of their careers, but they are open to new opportunities.
“Stefanie is a bright student and an outstanding scientistwith much to contribute,” said Dr. Sloane. “It has been delight-ful seeing her develop into a skilled and innovative researcher.
We will all miss her when she moveson to her postdoctoral position, yet welook forward to watching her careerevolve and to spending time with heragain at national and internationalmeetings.” �
Nationally acclaimed colleagues have honored Stefanie Roshy as an outstanding young investigator. She expects to complete her Ph.D. later this year.
By learning more aboutselective inhibitors, Roshy
hopes to find ways to block cancer progression.
Recruitment is already underway for graduate student
with expertise in proteolysis
BY A M Y D I C R E S C E

GAN KRESGE EYE INSTITUTE HARPER UNIVERSITY HOSPITAL HURON VALLEY-SINAI HOSPITAL
1-888-DMC-2500 www.dmc.org
BARBARA ANN KARMANOS CANCER INSTITUTE MICHIGAN ORTHOPAEDIC SPECIALTY HOSPITAL
When health professionals are immersed in a powerful academic environment, the result is anastonishing pace of life-saving discoveries.Developments that used to occur once a decade have accelerated into continuous breakthroughsand they are happening here, in the heart of the Detroit Medical Center/Wayne StateUniversity system.
The DMC is the only health care center withinMetro Detroit with this crucial research affiliation.Direct access to state-of-the-art research at Wayne State Medical School creates the differencebetween the care you’d find at any hospital and the advanced care you can only find at the DMC.
Gateway to the DMCI-75 at MackOne exit north of the stadiums
REAKTHROUGHS HAPPEN WHERE RESEARCH HAPPENS.
B CAMPUSREAKTHROUGHSB CAMPUSREAKTHROUGHS
WSU School of Medicine fuels the DMCWSU School of Medicine fuels the DMC
B CAMPUSREAKTHROUGHSB CAMPUSREAKTHROUGHS
WSU School of Medicine fuels the DMCWSU School of Medicine fuels the DMC
CHILDREN’S HOSPITAL OF MICHIGAN:where the first successful pediatric bone marrowtransplant in Michigan occurred.
DETROIT RECEIVING HOSPITAL:where Michigan’s first Level I Trauma Center was established.
HARPER UNIVERSITY HOSPITAL:where the world’s first open-heart surgery was performed.
HUTZEL WOMEN’S HOSPITAL:home of the nation’s only National Institutes of Health Perinatology Research Branch.
KARMANOS CANCER CENTER:developed the first human breast cancer cell lines, facilitating worldwide breast cancer research.
KRESGE EYE INSTITUTE:where the first radial keratotomy procedure in the U.S. was performed.
SINAI-GRACE HOSPITAL:established the nation’s first comprehensive program for sickle cell anemia.
WAYNE STATE UNIVERSITY: the Center for Urban African-American Health is one of only eight sites in the nation designated by theNational Institutes of Health to address racialdisparities in health care.
RIGHT HERE

332005 Wayne Medicine

Nonprofit OrganizationU.S. Postage
PAIDPermit No. 3844Detroit, Michigan
Public Affairs5D University Health Center4201 St. AntoineDetroit, MI 48201
www.med.wayne.edu