Embed Size (px)
Citation preview

BETHANIDINE VS GUANETHIDINE TRIAL/VA Coop Study Group
6. Meyer RA, Kaplan S: Echocardiography in the diagnosis of hypoplasiaof the left or right ventricles in the neonate. Circulation 46: 55, 1972
7. Assad-Morell JL, Tajik AJ, Giuliani ER: Echocardiographic analysis ofthe ventricular septum. Prog Cardiovasc Dis 17: 219, 1974
8. Seward JB, Tajik AJ, Hagler DJ, Ritter DG: Preoperative andpostoperative echocardiographic observations in common ventricle(abstract). Circulation 52 (suppl II): 11-46, 1975
9. Seward JB, Tajik AJ, Spangler JG, Ritter DG: Echocardiographic con-trast studies: Initial experience. Mayo Clin Proc 50: 163, 1975
10. Gramiak R, Shah PM, Kramer DH: Ultrasound cardiography: Contraststudies in anatomy and function. Radiology 92: 939, 1969
11. Hallermann FJ, Davis GD, Ritter DG, Kincaid OW: Roentgenographicfeatures of common ventricle. Radiology 87: 409, 1966
12. Rahimtoola SH, Ongley PA, Swan HJC: The hemodynamics ofcommon(or single) ventricle. Circulation 34: 14, 1966
13. Harley HRS: The embryology of cor triloculare biatriatum with bulbar(rudimentary) cavity. Guy's Hosp Rep 107: 116, 1958
14. Marin-Garcia J, Tandon R, Moller JH, Edwards JE: Single ventriclewith transposition. Circulation 49: 994, 1974
15. Elliott LP, Anderson RC, Edwards JE: The common cardiac ventriclewith transposition of the great vessels. Br Heart J 26: 289, 1964
16. Marin-Garcia J, Tandon R, Moller JH, Edwards JE: Common (single)ventricle with normally related great vessels. Circulation 49: 565, 1974
17. Seward JB, Tajik AJ, Gutierrez F, Hagler DJ, Moodie DS, Ritter DG:Contrast echocardiography: Peripheral vein injection of indocyaninegreen dye for detection and assessment of right-to-left intracardiac shunt-ing (abstract). Am J Cardiol 37: 171, 1976
18. Ruttenberg HD, Neufeld HN, Lucas RV Jr, Carey LS, Adams P Jr,Anderson RC, Edwards JE: Syndrome of congenital cardiac disease withasplenia: Distinction from other forms of congenital cyanotic cardiac dis-ease. Am J Cardiol 13: 387, 1964
19. Gramiak R, Chung KJ, Nanda N, Manning J: Echocardiographicdiagnosis of transpositiofi of the great vessels. Radiology 106: 187, 1973
20. Dillon JC, Feigenbaum H, Konecke LL, Keutel J, Hurwitz RA, DavisRH, Chang S: Echocardiographic manifestations of d-transposition ofthe great vessels. Am J Cardiol 32: 74, 1973
21. Pieroni D, Varghese PJ, Rowe RD: Echocardiography to detect shuntand valvular incompetence in infants and children (abstract). Circulation48 (suppl IV): IV-81, 1973
22. Kerber RE, Kioschos JM, Lauer RM: Use of an ultrasonic contrastmethod in the diagnosis of valvular regurgitation and intracardiac shunts.Am J Cardiol 34: 722, 1974
23. Duff DF, Gutgesell HP: The use of saline for ultrasonic detection of aright-to-left shunt in postoperative period (abstract). Am J Cardiol 37:132, 1976
24. Valdes-Cruz LM, Pieroni DR, Roland J-M, Shematek JP: Recognitionof residual post-operative shunts by contrast echocardiographic tech-niques (abstract). Am J Cardiol 37: 178, 1976
25. Gramiak R, Shah PM: Echocardiography of the aortic root. InvestRadiol 3: 356, 1968
26. Feigenbaum H, Stone JM, Lee DA, Nasser WK, Chang S.: Identifica-tion of ultrasound echoes from the left ventricle by use of intracardiac in-jections of indocyanine green. Circulation 41: 615, 1970
27. Assad-Morell JL, Seward JB, Tajik AJ, Hagler DJ, Giuliani ER, RitterDG: Echo-phonocardiographic and contrast studies in conditionsassociated with systemic arterial trunk overriding the ventricular septum:Truncus arteriosus, tetralogy of Fallot, and pulmonary atresia with ven-tricular septal defect. Circulation 53: 663, 1976
28. Seward JB, Tajik AJ, Hagler DJ, Giuliani ER, Gau GT, Ritter DG:Echocardiogram in common (single) ventricle: Angiographic-anatomiccorrelation. Am J Cardiol, in press
29. Seward JB, Tajik AJ, Ritter DG: Echocardiographic features of strad-dling tricuspid valve. Mayo Clin Proc 50: 427, 1975
30. LaCorte MA, Fellows KE, Williams RG: Overriding tricuspid valve:Echocardiographic and angiocardiographic features. Am J Cardiol 37:911, 1976
Multiclinic Controlled Trial ofBethanidine and Guanethidine in Severe Hypertension
VETERANS ADMINISTRATION COOPERATIVESTUDY GROUP ON ANTIHYPERTENSIVE AGENTS
SUMMARY One hundred and eight patients with initial diastolicblood pressure in the range of 100-124 mm Hg while takinghydrochlorothiazide were assigned randomly and double-blind tohydrochlorothiazide plus either bethanidine or guanethidine. Theaverage reduction of the fifth and sixth months' diastolic bloodpressure was 18.4 mm Hg for guanethidine and 13.6 mm Hg forbethanidine (P < 0.01). The distribution of the individual values wassuch that 68.8% of guanethidine treated patients achieved a diastolic
GUANETHIDINE AND BETHANIDINE are potentantipressor compounds with a similar mode of action in-volving blockade of the post ganglionic adrenergic nerveendings. In clinical practice guanethidine has been employedchiefly when other drugs such as diuretics, hydralazine,reserpine or methyldopa fail to achieve adequate control ofthe hypertension or when their side effects are unaccept-
From participating Veterans Administration Hospitals in Allen Park,Michigan; Jackson, Mississippi; Memphis, Tennessee; Miami, Florida; Rich-mond, Virginia; San Juan, Puerto Rico; and Washington, D.C.A complete list of participants appears in the Addendum at the end of this
article.Address for reprints: Eli A. Ramirez, M.D., Veterans Administration
Hospital, GPO Box 4867, San Juan, P.R. 00936.Received September 13, 1976; revision accepted October 25, 1976.
level below 90 mm Hg, compared to only 45.5% of the bethanidinetreated group (P < 0.025). The degree of orthostatic fall in bloodpressure was greater with bethanidine than with guanethidine(P < 0.05). The diurnal variation of blood pressure was slightlygreater with bethanidine than with guanethidine. The resultssignificantly favor guanethidine. This study failed to demonstrate thatthe shorter action of bethanidine confers significantly better controlof blood pressure than the longer action of guanethidine.
able.", 2 It has also been used as the primary agent to controlmalignant or severe diastolic hypertension in combinationwith diuretics and other antihypertensive drugs.2 8Bethanidine is not commercially available in the UnitedStates, but is widely used in Britain." It is said to have thefollowing advantages over guanethidine:4"1-
1) Following oral administration the onset of antihyper-tensive effect occurs within one or two hours, reaches a max-imum at four to five hours and disappears in 12 hours. Bycontrast, the duration of action of guanethidine is greaterthan 96 hours.9 Because of its short action in comparisonwith guanethidine, bethanidine might avoid the morningorthostatic hypotension as well as the afternoon rise of bloodpressure characteristic of guanethidine. By varying the dosesof bethanidine at different times of the day, it might be
519
by guest on July 24, 2017http://circ.ahajournals.org/
Dow
nloaded from

VOL 55, No 3, MARCH 1977
possible to minimize the diurnal fluctuation of bloodpressure that is seen with guanethidine.
2) Side effects are an inseparable byproduct of the phar-macological action of both drugs, but they are said to bemore severe with guanethidine. Increased frequency ofbowel movements, which may be a troublesome side effect ofguanethidine, is said to be absent with bethanidine.4 Ortho-static faintness, sexual dysfunction and mild depression alsooccur in varying degrees with both guanethidine andbethanidine. However, because of the shorter duration of ac-tion of bethanidine, the ability to control or minimize theside effects by dosage adjustments might be greater thanwith guanethidine.The purpose of the present controlled trial was to ascer-
tain whether bethanidine plus thiazide is more effective thanguanethidine plus thiazide in the control of severe hyperten-sion.
Objectives of Study
The study was designed to determine:1) The antihypertensive effectiveness of bethanidine as
compared to guanethidine (both being combined with hydro-chlorothiazide), using the following criteria: a) the percent-age of patients in each group who at the fifth and sixthmonth postrandomization visits exhibited an average dia-stolic blood pressure below 90 mm Hg; b) the mean changesof diastolic blood pressures between the last two preran-domization visits (hydrochlorothiazide alone), and the fifthand six month postrandomization visits (hydrochlorothi-azide plus either bethanidine or guanethidine).
2) The intrapatient diurnal variation of blood pressureswith both drugs as determined by eight blood pressurereadings during a 24 hour period of hospitalization. Thereadings were obtained during the fifth and sixth monthspostrandomization.
3) The acceptability of the drug combinations over a sixmonth experience to be based on the incidence of toxic reac-tions and side effects.
Plan of Investigation
Selection of Patients
Male patients below age 60 were considered as candidatesfor the trial if their diastolic pressure ranged from 100 to 129mm Hg while receiving treatment, or from 1 10 to 129 mmHg without treatment. Patients were excluded if they hadsurgically curable hypertension, if they were considered un-reliable, or if they were not able to measure their own bloodpressure. Other exclusions were atrial fibrillation or otherarrhythmias making blood pressure readings unreliable,liver disease or recurrent diarrheal disease such as colitis.Patients were also excluded if they had past or present severe
hypertensive complications such as cerebral or subarachnoidhemorrhage, dissecting aneurysm, grade 3 or 4 hypertensiveretinopathy, serum creatinine greater than 3.0 mg/100 ml orrecent acute hypertensive encephalopathy. Exclusions foratherosclerotic complications included cerebral thrombosis,transient ischemic attack, and myocardial infarction or un-
stable angina within the past six months.Patients with a history of gout, peptic ulcer, diabetes
mellitus if under control, congestive heart failure if con-
trolled without thiazides or other antihypertensive drugs,and patients with left ventricular enlargement by ECG or X-ray were permitted in the trial.
Prerandomization Trial Period
At the initial visit the study was explained to the patientby the physician and a signed informed consent was ob-tained.* The patient was instructed in the technique ofmeasuring his own blood pressure at home, and was suppliedwith an apparatus designed for this purpose (Autosphyg-Propper). The history, physical examination and initiallaboratory studies were performed. The laboratory studiesincluded complete blood count, urinalysis, serum creatinine,uric acid, potassium, cholesterol, fasting blood sugar, serumoxaloacetic transaminase, alkaline phosphatase, bilirubin,chest X-ray and ECG.The clinic blood pressures were measured in the right arm
using the Arteriosonde 1010 (Roche) with a cuff of ap-propriate size. After the patient rested undisturbed in thesupine position for 10 to 15 minutes, the blood pressure wasmeasured three times at two minute intervals in each of thefollowing positions: lying, sitting and standing. The pulserate was counted in each position. Blood pressure waschecked additionally by the standard auscultatory method atthe time of randomization, and at the fifth and sixth monthspostrandomization.
If the patient was receiving reserpine, it was discontinuedfor one month, although other antihypertensive drugs werecontinued. If the patient was receiving any other antihyper-tensive agent than reserpine, it was discontinued and he wasgiven a tablet every eight hours containing 35 mg hydro-chlorothiazide plus riboflavine 5 mg, which was used as amarker substance. The patient was asked to record his bloodpressure morning and evening at home.
During the remainder of the prerandomization trialperiod, the patients were seen every two weeks for a max-imum of four visits. At each visit compliance was checked bypill counting and by the presence of riboflavine-inducedurinary fluorescence under ultraviolet light. The require-ments for randomization were two successive visits in which:1) the average Arteriosonde fifth phase sitting diastolicblood pressure was in the range of 100-124 mm Hg; 2) therewere no pill count or urine fluorescence violations; 3) thepatient demonstrated the ability to measure his bloodpressure reliably at home.
Postrandomization Period
This was a double blind trial. Accepted patients wereassigned randomly to either bethanidine or guanethidine un-der the code name "Bethadine." "Bethadine" was suppliedin three strengths in a ratio of 1 mg guanethidine to 1.67 mgbethanidine as follows:
"Bethadine"Strength
I23
Bethanidine(mg)4.212.550.0
Guanethidine(mg)2.57.530.0
*The study protocol was approved by the Human Use Committee of eachparticipating hospital and conformed to the principles of the Helsinki declara-tion.
520 CIRCULATION
by guest on July 24, 2017http://circ.ahajournals.org/
Dow
nloaded from

BETHANIDINE VS GUANETHIDINE TRIAL/VA Coop Study Group
All patients were continued on their usual doses of hydro-chlorothiazide and one tablet every eight hours of the firststrength of "Bethadine" was added.
Patients were seen in the clinic at two week intervals andboth clinic and home records of blood pressure were used inadjusting doses. "'Bethadine" doses were increased slowly bypredetermined increments until an antihypertensive effectwas obtained. For more precise dosage adjustments, thepatients were asked whenever needed to spend from 8:00a.m. to 4:00 p.m. in the clinic where their blood pressure was
recorded every two hours. An attempt was made in eachcase, utilizing home and all day clinic blood pressure
readings, to alter each of the three doses of "Bethadine" inorder to obtain the best possible 24 hour control of thehypertension. For example, at the third and fifth monthclinics, doses were changed in approximately 25% of thepatients. Half of these changes took advantage of bethan-idine's shorter action: either the evening dose was decreasedor the morning or noon dose was increased. The minimumdose was one tablet daily of "Bethadine" strength 1, and themaximum was nine tablets of strength 3.
After the initial dosage adjustment phase, patients were
seen at monthly intervals. At the fifth and sixth month visits,the patients were hospitalized and their blood pressures
measured eight times during the diurnal cycle from 6:00a.m. to 10:00 p.m. At the sixth month, all initial laboratorytests were repeated.The following hypertensive complications were indica-
tions for removal from the study: grade 3 or 4 hypertensiveretinopathy, acute hypertensive encephalopathy, hemor-rhagic stroke, dissecting aneurysm of the aorta, congestiveheart failure and uremia.
Terminating atherosclerotic complications includedcerebral thrombosis, transient ischemic attacks, myocardialinfarction and unstable angina.
Other reasons for removal of the patients were intoleranceto hydrochlorothiazide, inability to tolerate the minimaldose of "Bethadine," discontinuation of protocol drugs fortwo months, and elevation of diastolic blood pressure to 125mm Hg or higher for two successive clinic visits one weekapart.The patients were questioned at each visit about side
effects including increased frequency of bowel movements,failure of ejaculation, orthostatic faintness and others.Protocol treatment could be interrupted for acute illnesses,surgery, or other valid medical reasons providing treatmentwas reinstituted within a period of two months.
Results
From January 1973 to December 1974, 203 patients were
recruited for the study. A total of 95 were rejected for failureto satisfy the criteria for randomization. Forty-nine were
rejected because their diastolic blood pressure during thetrial period was less than 100 mm Hg and two because ofpressures greater than 124 mm Hg. Twenty were rejectedbecause of pill count violations and 13 because they failed tokeep clinic appointments. Four were rejected because of in-tolerance to hydrochlorothiazide, one because he exceededthe age limit and six for miscellaneous medical reasons.
One hundred and eight patients in seven hospitals were
randomized: 56 to guanethidine and 52 to bethanidine.
TABLE 1. Characteristica at Time of Randomization of Pa-tients Completing Six Months of Treatment
Guanethidine BethanidineMean SI Mean BE
Age (yr) 48.8 .8 50.1 .8Weight (lb) 193.3 4.7 180.1 4.0Systolic BP (mm Hg) 155.5 2.4 153.3 2.4
(A-Sonde)Systolic BP (mm Hg) 157.3 2.1 153.5 2.5
(Auscultatory)Diastolic BP (mm Hg) 105.5 .6 105.4 .7
(A-Sonde)Diastolic BP (mm Hg) 110.3 .97 108.7 1.1
(Auscultatory)Pulse/min 79.8 1.4 81.0 1.6Uric acid (mg/100 ml) 8.05 .28 7.82 .26Serum K (mEq/L) 4.06 .07 4.06 .10Creatinine
(mg/100 ml) 1.29 .03 1.27 .04N 48 44
Because of losses occuring during the first six months afterrandomization, 48 patients receiving guanethidine and 44receiving bethanidine completed six months of treatment.The present results cover this period of therapy.
Characteristics of the patients at the time of randomiza-tion are shown in table 1. Except for a slight difference inbody weight, the data were similar in the two groups.At the end of six months of treatment, the distributions of
dose levels reached by titration for both agents were similarin relation to the 1 to 1.67 ratio guanethidine to bethanidinewhich was chosen to equalize tablet potencies (table 2).Patients taking guanethidine were titrated to dose levelsfrom a minimum of 7.5 mg/day to 150 mg/day, with themedian at 30 mg/day. Patients receiving bethanidine weretitrated to dose levels from a minimum of 12.6 mg/day to350 mg/day with the median at 50 mg/day.
Blood Pressure Changes
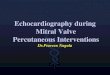
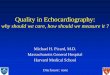
The therapeutic end point was a sitting phase 5 diastolicblood pressure measured with the Arteriosonde of less than90 mm Hg using the average of the readings taken at thefifth and sixth months postrandomization. This end pointwas achieved in 68.8% of patients treated with guanethidineand in 45.5% of the bethanidine treated group (P < 0.025)(fig. 1).The number and percent frequencies of the changes in sit-
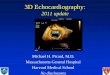
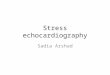
ting pressures before and after treatment are shown in figure2. Eighty-five percent of the patients on guanethidine com-pared to 70.5% of the patients on bethanidine obtained adiastolic pressure reduction exceeding 10 mm Hg. The meanreduction with guanethidine was 18.4 mm Hg, which wassignificantly greater than the 13.6 mm Hg obtained withbethanidine (P < 0.01).
TABLE 2. Number of Patients on Dose Levels at Six MonthsDose level*
1 2 3 4 5 6 7 8 9 10 Total
Guanethidine 4 4 9 12 9 6 3 1 0 0 48Bethanidine 1 7 11 9 4 5 6 0 1 0 44
*Dose levels of guanethidine (daily total) in mg were as follows: 1 = 7.5,2 = 15, 3 = 22.5, 4 = 30, 5 = 45, 6 = 67.5, 7 = 90, 8 = 150, 9 = 210,10 = 270. Equivalent doses of bethanidine were 1.67 times these amounts.
521
by guest on July 24, 2017http://circ.ahajournals.org/
Dow
nloaded from

VOL 55, No 3, MARCH 1977
GUANETHIDINE
50 -
40 - Systolic
,*
30
20-
106 m
%
.initial
100 120 140 160190 200m m Hg
50
40
30
20
10
70 80 90 100 110 120m m Hg
BETHAN I D INE
50 -
40 -
30 -
20 -
10
40
30
20
10
Systolic
I
6 mo/- i al
100 120 140 160 180 200
mm Hg
4030
20
1050
40 - Diastolic
30-
I,' .\initial10 ' 6 mo;-/
70 80 90 100 110 120m m Hg
FIGURE 1. Frequency distributions of Arteriosonde pressures of
patients completing six months of therapy.
Regarding Arteriosonde systolic blood pressure, 83.4% ofthe patients taking guanethidine compared to 70% of thepatients taking bethanidine obtained a reduction exceeding10 mm Hg. The average reduction of systolic blood pressurefor the bethanidine group was 21.8 mm Hg and for theguanethidine group was 15.4 mm Hg.
Using the sitting blood pressure obtained by the standardauscultatory method, the results were similar to those ob-tained with the Arteriosonde. Eighty-one percent of thepatients taking guanethidine and only 50% of those takingbethanidine achieved a 10 mm Hg or greater reduction indiastolic pressure. The mean reduction of diastolic pressurefor guanethidine was 17.1 mm Hg and for bethanidine 10.3mm Hg (P < 0.005). For systolic pressure the mean reduc-tion for guanethidine was 20.6 mm Hg and for bethanidine13.8 mm Hg, which are also significantly different(P < 0.05).
ARTER IOSONDE
Systolic
Guanethidine f:#--<;S- -: Bethanidine
-50 -40 -30 -20 -10 0 10 20 30 40m m. H9
Diastolic
-50 -40 -30 -20 -10 0 10 20 30 40m m. Ha
AUSCULTATORY--
40
30
20
10
40
30
20
10
Systolic
Bethanidine
;uanethidine Bethanidine
-~
-50 -40 -30 -20 -10 0 10 20 30 40m m. Hg
X Average of Change*The baseline pressure for the standard auscultatorymethod was one prerandomization reading whereasthe average of two prerandomization pressures was
used for the Arteriosonde.
FIGURE 2. Frequency distributions ofinitial minus six months sit-ting pressure changes using A rteriosonde and standard auscultatorymethod.
Postural and Diurnal Changes in Blood Pressure
Table 3 shows average systolic and phase 5 diastolicArteriosonde blood pressures for 36 patients in the supineand standing positions. The blood pressures were taken ap-proximately two hours apart from 6:00 a.m. to 10:00 p.m. at
TABLE 3. Average Arteriosonde Systolic and DiastolicPatients on Each Regimen
the fifth and sixth months postrandomization. The purposeof these observations was to determine whether the shorteracting bethanidine did indeed permit less of a differentialbetween supine blood pressure and the blood pressure in theorthostatic position, and less diurnal variation.
Pressures At 5-6 Months Postrandomization in 36
Diastolic (mm Hg) Systolic (mm Hg)Guanethidine Bethanidine Guanethidine Bethanidine
Hour Supine Erect Change Supine Erect Change Supine Erect Change Supine Erect Change
6 80.3 76.3 4.0 85.3 74.5 10.8 137.8 116.9 20.9 136.9 112.1 24.88 82.8 79.9 2.9 85.1 78.2 6.9 135.5 121.8 13.7 136.8 117.2 19.6
10 84.3 83.7 0.6 86.2 78.4 7.8 136.8 125.0 11.8 139.8 115.9 23.912 83.6 83.0 0.6 87.8 82.1 5.7 139.8 127.6 12.2 141.8 120.0 21.814 82.9 82.4 0.5 85.3 81.2 4.1 140.4 129.3 11.1 138.5 120.0 18.516 84.7 82.6 2.1 86.8 82.3 4.5 140.2 128.7 11.5 143.5 120.1 23.419 83.4 80.6 2.8 81.9 77.4 4.5 143.0 129.5 13.5 142.2 117.2 25.022 82.7 80.9 1.8 83.5 77.0 6.5 143.9 126.4 17.5 141.4 116.6 24.8
Mean 83.1 81.2 1.9 85.2 78.9 6.3 139.7 125.7 14.0 140.1 117.4 22.7
522 CIRCULATION
by guest on July 24, 2017http://circ.ahajournals.org/
Dow
nloaded from

BETHANIDINE VS GUANETHIDINE TRIAL/VA Coop Study Group
The average systolic blood pressures in the supine positionwere essentially equal in both groups but in the orthostaticposition, the systolic diurnal range of change averaged 14.0mm Hg for guanethidine and 22.7 mm Hg for bethanidine, a
difference of 8.7 mm Hg (P < 0.05). The diurnal range ofchange in diastolic blood pressure from supine to standingaveraged 1.9 mm Hg for the guanethidine group and 6.3 mmHg for the bethanidine group; the difference of 4.4 mm Hg isalso significant (P < 0.05). In fact, the averages of allsystolic and diastolic supine-erect blood pressure changes atall times of the day were greater with bethanidine than withguanethidine.
Table 4 shows the averages of the lowest and highest dailypressures of the 36 patients in the supine, sitting and erectpositions. The pooled within-patient, within-day standarddeviations of eight observations for each position from 6:00a.m. to 10:00 p.m. are also shown. All differences betweenaverage highest and lowest systolic and diastolic pressures inall positions were greater for bethanidine than for guan-
ethidine. The standard deviations were also uniformlygreater for bethanidine than for guanethidine in all positionsfor both systolic and diastolic blood pressures.
Comparison of Pressure Readings with the Arteriosonde and theStandard Auscultatory Method
Standard auscultatory blood pressures also were taken atthe same time as the Arteriosonde readings at preran-
domization and five and six months postrandomization. Inthe prerandomization determinations it was observed thatthe systolic readings were almost identical for both methodswith an average difference of only 1.04 mm Hg (table 1).However, the diastolic standard auscultatory blood pressure
readings were systematically higher within patients andbetween groups than the Arteriosonde instrument pressures.
The average difference was 4.06 mm Hg.
Losses from Study and Side Effects
Of the 108 patients randomized, 16 were lost from thestudy, eight because of noncompliance and seven because ofterminating events. One patient was improperly ran-
domized. With respect to the noncompliant patients, fivefailed to return for unknown reasons, one moved from thearea, and two were uncooperative in taking the medicationsand following protocol procedures. These noncompliantpatients were equally distributed between regimens.Of the four patients who were lost because of terminating
morbid events, two died, one from myocardial infarctionand one of sudden death. Both were receiving guanethidine.Nonfatal morbid events included a patient with transientischemic attacks and another who exhibited a rising level ofserum creatinine. Both were receiving bethanidine. Lossesdue to real or suspected drug toxicity included depression inone patient and orthostatic dizziness in a second patient.
Side effects elicited and volunteered during the course ofthe study included vertigo, dyspnea, headache, nasalstuffiness, increased frequency of bowel movements, sexualdysfunction, lethargy, joint pains, angina and syncope,among others (table 5). No significant differences betweenthe two drugs were observed although there were fewer com-plaints of dyspnea, depression and sexual dysfunction withbethanidine. However, lethargy was somewhat increased.
TABLE 4. Diurnal Variation of Arteriosonde Pressures for36 Patients on Each Drug at 5 and 6 Months*
Pooledwithin-day
within-patientBlood pressure standard(mm Hg) deviations of 8
Ave daily Ave daily observationslow high Difference from 06:00 to 22:00
Supine systolicGuanethidine 125.0 156.4 31.4 11.9Bethanidine 122.7 158.4 35.7 13.8
Supine diastolicGuanethidine 72.3 92.6 20.3 7.6Bethanidine 73.0 96.1 23.1 8.6
Sitting systolicGuanethidine 119.0 151.4 32.4 12.3Bethanidine 115.3 151.5 36.2 13.5
Sitting diastolicGuanethidine 74.8 95.9 21.1 8.3Bethanidine 75.9 98.8 22.9 8.6
Erect systolicGuanethidine 108.0 141.8 33.8 13.3Bethanidine 96.1 137.3 41.2 16.3
Erect diastolicGuanethidine 69.0 91.6 22.6 8.5Bethanidine 63.8 92.6 28.8 11.2*Averages of the lowest and highest daily Arteriosonde systolic and
diastolic pressures in the supine, sitting and standing positions at 5-6months postrandomization in 36 patients on each regimen
No differences between drugs were noted with respect tofrequency of bowel movements, vertigo and syncope.No significant differences between the groups were noted
in serum potassium or uric acid. There was a trend to aslight increase in serum creatinine averaging less than0.3 mg % with guanethidine, but neither the change nor thedifferences between the regimens were statistically signifi-cant.
It was noted in table 1 that the initial average heart ratefor patients randomized to guanethidine was 79.8/min andfor those on bethanidine 81/min. After six months of treat-ment the average heart rate decreased 6/min withguanethidine and increased 1.2/min with bethanidine. Thisdifference is significant (P< 0.01).
TABLE 5. Number of Patients with Side Effects Noted duringInitial Six Months Postrandomization
Symptom Guanethidine Bethanidine Total
Vertigo 20 23 44Dyspnea 17 6 23Headache 13 9 22Nasal stuffiness 12 10 22Increased bowelmovements 10 11 21
Sexual dysfunction 13 8 21Lethargy 7 11 18Joint pain 7 6 13Angina 6 6 12Syncope 4 6 10Fever 4 5 9Nightmares 4 2 6Wheezing 2 4 6Palpitations 2 4 6Ulcer symptoms 3 3 6Depression 5 0 5Skin rash 3 1 4Other 24 17 41Total 156 132 288
523
by guest on July 24, 2017http://circ.ahajournals.org/
Dow
nloaded from

VOL 55, No 3, MARCH 1977
Discussion
Using the end point of sitting fifth phase diastolic levelsbelow 90 mm Hg after'six months of treatment, it wouldappear that guanethidine was more effective thanbethanidine. Over 23% more patients achieved this end pointwith guanethidine than with bethanidine. Similarly, usingthe end point of fifth phase diastolic blood pressure reduc-tion, guanethidine was more effective. With guanethidine theaverage reduction was 4.8 mm Hg greater than withbethanidine. Both differences were significant statistically.
Guanethidine also showed a greater antihypertensiveeffect than bethanidine according to other indicators. Forexample, 85.3% of guanethidine treated patients achieved areduction of diastolic pressure exceeding 10 mm Hg com-pared to 70.5% of those taking bethanidine. Likewise, sittingsystolic pressure was reduced more effectively and in agreater proportion of patients with guanethidine than withbethanidine. The spread between the two regimens was evengreater with the established, standard auscultatory tech-nique with 81.2% of guanethidine treated patients and only50% of bethanidine treated subjects achieving a reduction indiastolic pressure exceeding 10 mm Hg. These findings arein contrast to previous reports. Gibb et al., in a smaller con-trolled trial, found no essential difference betweenguanethidine and bethanidine.5 These drugs have been con-sidered to be interchangeable in terms of antihypertensiveeffectiveness.'0
Other objectives of the study were to determine whetherone drug induced less orthostatic change than the otherthroughout the day and at different times of the day. Themeans of the values obtained in the throughout-the-daymeasurements indicate that the orthostatic fall obtainedfrom supine to standing with bethanidine averaged 8.7/4.4mm Hg more than that obtained with guanethidine. Thegreater differential between supine and erect blood pressureswith bethanidine was noted throughout the day including theearly morning blood pressures. These results were disap-pointing because it was hoped that with the greater ability toadjust dosages at eight hour intervals, the spread betweensupine and orthostatic levels would be less with bethanidinethan with guanethidine. Prichard et al. in a cross-over studyalso found that bethanidine produced slightly greaterorthostatic hypotension than did guanethidine.6
Contrary to what was anticipated,7 8 the diurnal variationin blood pressure was not significantly different between thedrugs. Indeed, the small differences observed favoredguanethidine. Bethanidine exhibited greater differences thanguanethidine between the means of the highest and lowestsystolic and diastolic blood pressures measured throughoutthe day from 6:00 a.m. to 10:00 p.m. Also, the pooled within-patient, within-day standard deviations of eight observationsthroughout the day were slightly greater with bethanidinethan with guanethidine. These findings were noted in allpositions, but were particularly notable in the orthostaticposition.
Considering the severity of the hypertension, the numberof morbid events was not great. Also, three of the four wereatherosclerotic complications involving the coronary andcerebral vessels. The distribution of morbid events wasabout the same with both treatments. The preponderance of
atherosclerotic complications in this short term study issimilar to that among the treated patients of the VeteransAdministration Study on morbidity," 12 where treatmentappeared to be effective primarily in preventing the so-called"hypertensive" complications of hemorrhagic stroke, con-gestive heart failure, renal failure and malignant phase ofhypertension.No significant differences were noted in the side effects in
our patients. Fewer patients taking bethanidine complainedof dyspnea and depression than was the case withguanethidine. Surprisingly, however, there was no differencein the two groups in regard to increased frequency of bowelmovements, the absence of which is claimed as one of themain advantages of bethanidine. The incidence of sexualdysfunction, lethargy and syncope also were similar in thetwo therapeutic groups.The lack of significant difference in the incidence of com-
plaints of side effects does not necessarily indicate that suchdifferences may not actually exist. In the present study, arelatively high incidence of complaints of side effects wasobserved in both treatment groups. In a previous V.A. drugtrial,'2 it was noted that placebo treated patients can exhibitas high an incidence of suspected side effects as patients tak-ing active drugs. It is our impression that the clinic interviewtechnique yields a large number of false positive responseswhich may result in dilution of actual differences to the ex-tent that they become undetectable.
Guanethidine produced a small but significant lowering ofpulse rate as compared to bethanidine. Prichard et al. notedthe same effect.6 This may be attributed to a more completesympathetic inhibition and consequent increase in para-sympathetic effect by guanethidine as compared tobethanidine. Although both drugs inhibit the release ofnoradrenaline at the sympathetic nerve endings, bethanidinedoes not deplete noradrenaline in nerve tissue until severalmonths have elapsed, and even then to a lesser degree thanguanethidine.8The results of the present study fail to support the claim
that bethanidine provides greater therapeutic benefit thanguanethidine. In fact, the results significantly favor guan-ethidine over bethanidine. The shorter duration of action ofbethanidine apparently does not confer an advantage inmore effective control of blood pressure than the longer ac-tion of guanethidine. It must be emphasized, however, thatthe study was designed and the results analyzed to deter-mine the relative effectiveness of the drugs in two groups ofpatients. It is entirely possible that certain individualpatients may obtain more therapeutic benefit from bethan-idine than from guanethidine and vice versa.
Addendum
Members of the Study Group
Eli A. Ramirez, M.D., ChairmanLeo Elson, M.D.Edward D. Freis, M.D.Arthur S. Gear, M.D.James R. Oster, M.D.Frederick N. Talmers, M.D.J. R. Thomas, M.D.
524 CIRCULATION
by guest on July 24, 2017http://circ.ahajournals.org/
Dow
nloaded from

DOBUTAMINE AFTER OPEN HEART SURGERY/Sakamoto, Yamada
Consultants and Associates
Jack M. BecktelJames A. Hagans, M.D., Ph.D.C. Morton Hawkins, Sc.D.Sibley W. Hoobler, M.D.Arthur F. Johnson, Ph.D.H. M. Perry, M.D.Harold W. Schnaper, M.D.Lawrence W. ShawWilliam M. Smith, M.D.
References
1. Page IH, Hurley RE, Dustan HP: The prolonged treatment of hyperten-sion with guanethidine. JAMA 175: 543, 1961
2. Kelly JJ Jr, Housel EL, Daly JW: Clinical experience with guanethidinein the treatment of hypertension. JAMA 176: 577, 1961
3. Maronde RF, Haywood LJ, Barbour B: Comparison of guanethidine and
guanethidine plus a thiazide diuretic. Am J Med Sci 242: 228, 19614. Editorial: Today's drugs: Bethanidine sulfate. Br Med J 2: 865, 19645. Gibb WE, Malpos JS, Turner P, White RJ: Comparison of bethanidine,
alpha methyldopa and reserpine in essential hypertension. Lancet 2: 275,1970
6. Prichard BNC, Johnston AW, Hill ID, Rosenheim ML: Bethanidine,guanethidine and alpha methyldopa in treatment of hypertension. Awithin patient comparison. Br Med J 1: 135, 1968
7. Gifford RW Jr: Bethanidine sulphate - a new antihypertensive agent.JAMA 193: 901, 1965
8. Editorial: Today's drugs: Bethanidine. Br Med J 1: 285, 19679. Swinyard EA, Harvey SC: Adrenergic blocking drugs. In Remington's
Pharmaceutical Series, edited by Martin EW. Easton, Mack PublishingCo., 1965, pp 988-989
10. Page LB, Sidd JJ: Medical Management of Primary Hypertension.Boston, Little, Brown, 1973, pp 42-46
11. Veterans Administration Cooperative Study Group on AntihypertensiveAgents: Effects of treatment on morbidity in hypertension. Results inpatients with diastolic blood pressures averaging 115 through 129 mmHg. JAMA 202: 116, 1967
12. Veterans Administration Cooperative Study Group on AntihypertensiveAgents: Effects of treatment on morbidity in hypertension. II. Results inpatients with diastolic blood pressures averaging 90 through 114 mm Hg.JAMA 213: 1143, 1970
Hemodynamic Effects of Dobutaminein Patients Following Open Heart Surgery
TOHRU SAKAMOTO, M.D., AND TAKASHI YAMADA, M.D.
SUMMARY Dobutamine, a new synthetic inotropic agent, was ad-ministered by intravenous infusion to 22 patients following open heartsurgery. The dosage of dobutamine started from 2Ag/kg/min andwas increased stepwise to 4, 6, and 8 ,ug/kg/min. Cardiac index in-creased from 2.54 ± 0.13 to 3.11 ± 0.19 and 3.50 ± 0.22 L/min/m2with 4 and 8 ,tg/kg/min, respectively. Heart rate increased from87.6 ± 2.9 to 96.4 ± 2.3 and 108.9 ± 3.2 beats/min with 4 and 8,gg/kg/min, respectively. Systolic and mean aortic pressure andsystolic pulmonary arterial pressure were elevated from 126.0 ± 3.8to 144.6 ± 6.0 mm Hg, from 91.8 ± 2.7 to 96.2 ± 3.2 mm Hg, and
ISOPROTERENOL, a potent beta-adrenergic stimulator,has been widely used for the treatment of cardiac failure,cardiogenic shock, or low output syndrome following openheart surgery.1-3
Although infusion of isoproterenol improves myocardialperformance, occurrence of adverse side effects such astachycardia, ventricular arrhythmia, and reduced perfusionpressure, often necessitates the discontinuation of this drug.Furthermore, isoproterenol has been shown experimentallyto intensify myocardial ischemia and to extend infarct sizeafter coronary narrowing or occlusion resulting in acutemyocardial failure.4An agent with inotropic effect as potent as isoproterenol
but without significant effects on vasomotor tone, heart rate,or rhythm would be desirable for the treatment of myocar-
From the Division of Cardiovascular Surgery, First Department ofSurgery, School of Medicine, Tokyo Medical and Dental University, Tokyo,Japan.
Address for reprints: Tohru Sakamoto, M.D., Division of CardiovascularSurgery, First Department of Surgery, School of Medicine, Tokyo Medicaland Dental University, No. 1-5-45, Yushima, Bunkyo-Ku, Tokyo, Japan.
Received June 23, 1976; revision accepted September 30, 1976.
from 33.4 ± 2.3 to 37.1 ± 2.5 mm Hg with 8 Ag/kg/min, while otherpressures were unchanged. Mean left atrial pressure fell significantlyfrom 15.9 ± 0.6 to 14.8 ± 0.7 mm Hg. Stroke volume index, strokework index, and left ventricular work also increased. Premature ven-tricular beats were observed in only one patient during dobutamine in-fusion, but no other side effect was observed.We conclude that dobutamine is a potent inotropic agent which in-
creases cardiac output without causing significant tachycardia orarrhythmias, and is useful for the treatment of patients followingopen heart surgery.
dial pump failure. Recently, Tuttle and Millis synthesized anew beta-adrenergic stimulator.6 This new beta-adrenergicstimulator, dobutamine, which is synthesized by modifyingthe side-chain of dopamine, is reported to have a strong in-otropic action with a weak chronotropic action and littleeffect on peripheral vessels.7-14
In this study, we examined the acute hemodynamic effectsof dobutamine on patients following open heart surgery andcompared the hemodynamic responses with isoproterenolinfusion.
Method and Materials
The study group (table I) consisted of 22 patientshospitalized at the Tokyo Medical and Dental UniversityHospital for open heart surgery. Their ages ranged from 19to 54 years with a mean of 32.5 years. The surgicalprocedure for aortic valve replacement with the Starr-Edwards ball prosthesis was performed during either cor-onary perfusion or a period of anoxic arrest. For other sur-gical procedures which included mitral valve replacementwith the Starr-Edwards disc prosthesis, an anoxic arrest was
525
by guest on July 24, 2017http://circ.ahajournals.org/
Dow
nloaded from

E A Ramirez, L Elson, A S Gear, J R Oster, F N Talmers and J R ThomasMulticlinic controlled trial of bethanidine and guanethidine in severe hypertension.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1977 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.55.3.519
1977;55:519-525Circulation.
http://circ.ahajournals.org/content/55/3/519the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on July 24, 2017http://circ.ahajournals.org/
Dow
nloaded from