Embed Size (px)
Citation preview

CLIN. CHEM. 35/6, 1005-1010 (1989)
CLINICAL CHEMISTRY, Vol. 35, No. 6, 1989 1005
Multicenter Evaluation of TDx Test for Assessing Fetal Lung Maturity
John C. Russell,’ Carol M. Cooper,’ CatherIne H. Ketchum,2 John S. Torday,3 Douglas K. Richardson,3 John A. HoIt,4 LawrenceA. Kaplan,5 J. Robert Swanson, and W. Michael lyle6
“TDx Fetal Lung Maturity,” an automated assay that mea-sures the relative concentrations of surfactant and albumin in
amniotic fluid, was compared with the lecithin/sphingomyelin(L/S) ratio and phosphatidylglycerol determination at fiveclinical sites. A total of 695 amniotic fluid samples wereanalyzed, of which 312 were followed by delivery of the infantwithin three days of sample collection. Of these 312, 24developed respiratory distress syndrome and seven devel-oped transient tachypnea. With the cutoff for maturity set at a
surfactant/albumin value of 50 mg/g, the assay showed asensitivity of 0.96 and a specificity of 0.88 for all samples,compared with a sensitivity of 0.96 and a specificity of 0.83for the US ratio. The combination of rapid assay (30 mm),accurate results, and uniformity among testing centersmakes the TDx assay a very promising method.
AddItIonal Keyphrases: amniotic fluid fluorescence polanza-
tion lecithin/sphingomyelin ratio, phosphatidyiglycerol compared
Thin-layer chromatographic methods are generally re-garded as the most nearly accurate for assessing fetal lungmaturity. The lecithin/sphingomyelin (LIS) ratio (1), quan-tification of the major surfactant phospholipids as in thelung profile (2), and saturated phosphatidylcholine deter-mination (3,4) have shown the highest predictive values inassessing the likelthood of respiratory distress syndrome(RDS). Although accurate, these methods have inconve-nient features: long turnaround times, use of toxic chemi-cals, and the requirement for much technical expertise. Anadditional problem has been standardization of procedures,so that results determined at one laboratory agree withthose from other laboratories (5). Thus a laboratory mustrely primarily on its own experience with a method todetermine its cutoff value for maturity. Consequently, lungmaturity is tested in relatively few hospitals. To offer thetest, a laboratory must have sufficient demand both tojustil�r training the personnel and to generate a largeenough database of results to maintain quality control ofthe procedure.
“TDx Fetal Lung Maturity” (FLM; Abbott Laboratories,North Chicago, IL) is a new method that avoids much of thetechnician involvement in sample preparation and mea-surement (6, 7). The fluorescence polarization of a dyeadded to a solution of amniotic fluid in buffer is comparedwith values on a standard curve to determine the relativeconcentrations of surfactant and albumin in the sample
(milligrams of surfactant per gram of albumin). The sample
‘Department 9TP AP2O, Abbott Laboratories,Abbott Park, IL60064.
2University of Alabama at Birmingham, Birmingham, AL.
3Brigham and Women’s Hospital, Boston, MA.4Chicago Lying-In Hospital, Chicago, IL.6Umversity of Cincinnati, Cincinnati, OH (present address:
Medical Research Laboratories, Cincinnati, OH).#{176}OregonHealth Sciences University, Portland, OR.Received January 30, 1989; accepted March 24, 1989.
is prepared by ifitering; all pipetting and measurementsteps are performed by the instrument; the result is printedout approximately 30 mm after the assay has been started.Because the method involves minimal technician input,and is run in a calibrated mode on a standard instrument,results should be highly comparable between laboratories.
Five laboratories, allassociated with centers specializing inhigh-risk pregnancies, participated in the study. Specimens ofamniotic fluid collected at these sites were tested both by TDxFLM and by the methods in use at the laboratories. If theinfant was delivered within three days of sample collection,the respiratory status was reported. Of the 312 samplesfitting this description, TDx FLM results were available for308, US ratios for 301, and phosphatidylglycerol for 244.
Materials and Methods
The TDx FLM assay was run in the Abbott TDx instru-ment as previously described (7). The precision of the assaywas determined by running the controls at each site in
replicates of five on 10 days. The results were compiled, andthe mean, standard deviation, and critical variance amongall laboratories were calculated.
Each site was requested to include only those samplesthat were collected specifically for fetal lung maturitytesting, and to use only that portion that remained aftercompletion of the tests in use at the site.TDx results werenot to be used for making clinical decisions.
Samples to be used for TDx testing were divided into two
aliquots to test the effect of different pretreatments on theresult. One was filtered through a 13-mm-diameter glassfiber ifiter provided with the reagents (Abbott; cat. no.85-2600) and the other was centrifuged 10 mm at 500 x gina calibrated centrifuge, provided for the clinical trials. Eachpreparation was tested in duplicate, and the mean reported.Additionally, the albumin in the sample was measured aspreviously described, to enable calculation of the surfactantconcentration from the surfactantlalbumin value (7).
The US ratio procedures at all sites were based onthin-layer chromatography. The amniotic fluid sample wascentrifuged to remove cellular debris, and the phospholip-ida were extracted from the supernate with methanol andchloroform. After evaporation of the chloroform, the resi-due was applied to the thin-layer chromatography plates;in some cases, acetone precipitation was used. After devel-oping, the plates were dried and the phospholipids made
visible by charring or chemical treatment. The spots werequantified by densitometry or planometry. Differences inmethodology between clinical sites are noted in Table 1.
Chart review was performed separately at each institu-tion. RDS was diagnosed on the basis of physical signs suchas flaring, retractions, and tachypnea requiring supplemen-tal oxygen for at least 24 h, and chest roentgenogramsconsistent with hyaline membrane disease. Cases requir-ing supplemental oxygen for less than 24 h were diagnosedas transient tachypnea. Cases of sepsis and serious congen-ital pulmonary or cardiac abnormalities were excludedfrom the study.
SIte: A B C 0 E
Eastman6061
WhatmanLK5
2.1 2.6 2.2
Solvent System 4
VisualIzation
acid/water (65/25/8/4).
Char Cupricacetate
0
0
0
a
a0
0
8
sitaS
8
0
Aa8
0
0 a
o a
A0
01 00 0o 0
000
o g08000
36 38 40
1000 CLINICAL CHEMISTRY, Vol. 35, No. 6, 1989
L/S Ratio Cond�lons
Table 1. US Ratio Methods Used at ParticipatIng Clinical Sites
CentritugatlonRCF(G) 700Time (mln) 5
AcetonePrecIpitatIon yes
TLC Plate Silica Gel withAmmonhim sulfate
Solvent System 1
Visualization Char
QuantIfIcation Dens�ometry Densitometry
Maturity cutoff 2.5
Phosphatidytglycerol conditions
Dimensions
Plate
500 1000 500 100010 10 5 5
no yes noyes
Silica Gel H Eastman13179
2 2 2 3Bromothymol Bromothymol Bromothymof char Cupric
blue blue blue acetate
Planometty Planometry Planometry
2 noldone
Same as L/S
2.0
1 1
SameasL/S MerkSilica Gel 60
2
Same as US
5 6 4
Char Iodine v�or UV Irradiationdlchlorolluoresceln
Solvent systems (by vol): (1) chlorofornVmethanol/water/acetlc acId (68/27/4/0.2); (2) chloroform/methanol/water (65/25/4); (3) chloroform/methanoliisopropanoVtrlathvlamln&watGr (30/9/25/25Th: (4t tetrRhvdroturan/mathvlaVmethanol/ammonium hydroxide. 2.0 mot/L (120/90/35/101: (ff1 thlornform/methennl/weter (55/25/41:
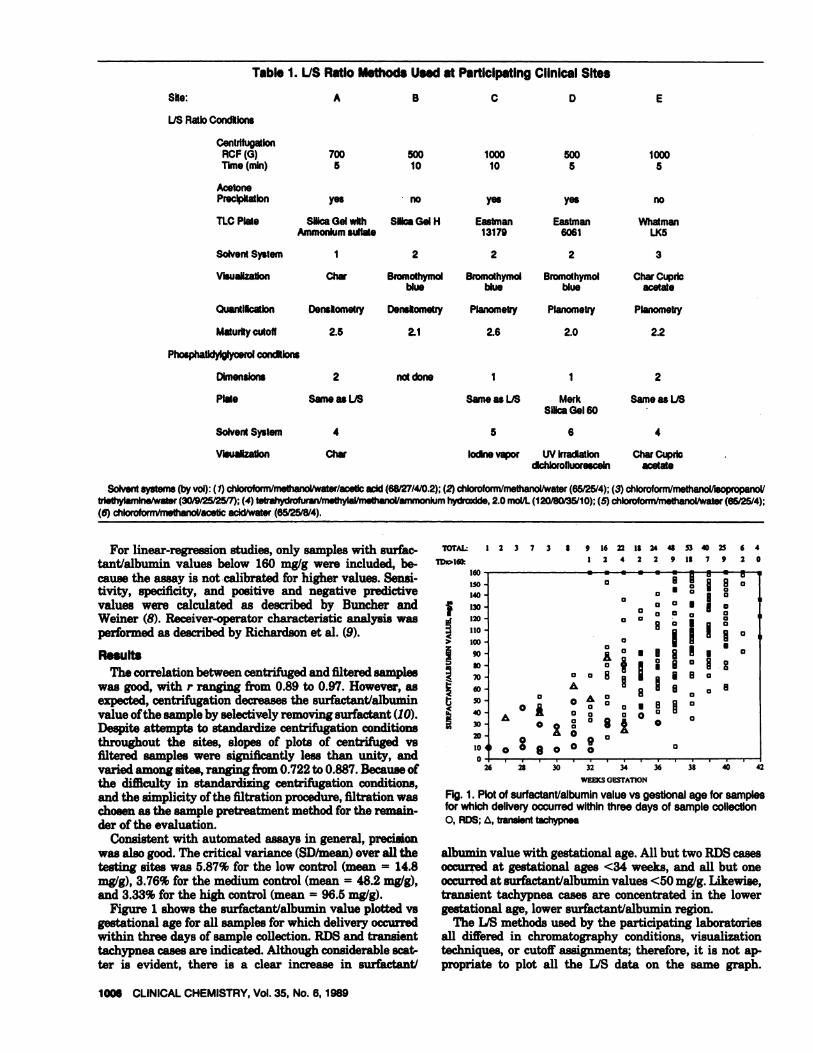
For linear-regression studies, only samples with surfac-tant/albumin values below 160 mg/g were included, be-cause the assay is not calibrated for higher values. Sensi-tivity, specificity, and positive and negative predictivevalues were calculated as described by Buncher andWeiner (8). Receiver-operator characteristic analysis was
performed as described by Richardson et al. (9).
ResultsThe correlation between centrifuged and filtered samples
was good, with r ranging from 0.89 to 0.97. However, asexpected, centrifugation decreases the surfactantlalbuininvalue of the sample by selectively removing surfactant (10).Despite attempts to standardize centrifugation conditionsthroughout the sites, slopes of plots of centrifuged vsfiltered samples were significantly less than unity, andvaried among sites, ranging from 0.722 to 0.887. Because ofthe difficulty in standardizing centrifugation conditions,and the simplicity of the filtration procedure, filtration waschosen as the sample pretreatment method for the remain-der of the evaluation.
Consistent with automated assays in general, precisionwas also good. The critical variance (SD/mean) over all thetesting sites was 5.87% for the low control (mean = 14.8
mg/g), 3.76% for the medium control (mean = 48.2 mg/g),and 3.33% for the high control (mean = 96.5 mg/g).
Figure 1 shows the surfactantlalbumin value plotted vsgestational age for all samples for which delivery occurredwithin three days of sample collection. RDS and transienttachypnea cases are indicated. Although considerable scat-ter is evident, there is a clear increase in surfactantl
TOTAL: 12373 8 9 16fl182448534023 64
1DD160 I 2 4 2 2 9 IS 7 9 2 0
160
150
140
130
ISO
110
160
90
*1
70
60
50
40
30
20
10
0230 32 34
WEEKS GESTA110N
Fig. 1. Plotof surfactant/albumin value vs gestional age for samplesfor whIch delivery occurred within three days of sample collection0, ADS; �, transient tachypnea
albumin value with gestational age. All but two RDS casesoccurred at gestational ages <34 weeks, and all but oneoccurred at surfactantlalbumin values <50 mg/g. Likewise,transient tachypnea cases are concentrated in the lowergestational age, lower surfactantlalbumin region.
The US methods used by the participating laboratoriesall differed in chromatography conditions, visualizationtechniques, or cutoff assignments; therefore, it is not ap-propriate to plot all the US data on the same graph.

L/S RATIO
SRI1<
SRI
.J
>
z
RI
tRIC,
LIS RATIO
IOU
‘Soc140
- . pp
. p #{149}#{149} � #{149}U
0U
130 a
120 0#{149} U
110 U s#{149}I �.
100 I �U U
90 0605 #{149}S60 U Up
70 #{149}U U60 Ao �50 �Q8 #{149}40 #{149}‘U
30 P
20
10 c �Xl �
02 4 6
1.13 RATIO
160
‘�o140
130
120
110
100
90�
70
60
50
40
30
20
10
A.
E�
0A
8
�o�
�5reo
0c��
U �#{149},UP -.
#{149}U . P
.:,J’ U
0�cP. a U
0 U
0 U
UC1�� U a U
�
#{149}.�a
b�
�#{149}a
.
I
1.13RATIO
1.15 RATIO
I 2 4 6
Fig. 2. Plots of surfactant/albumin value vs IfS ratio for clinical trial sites A, B, C, D, E (see Table 1)+, delivery occurred within three days of sample collectIon; 0, ADS; & transient tachypnea
CLINICAL CHEMISTRY, Vol. 35, No. 6, 1989 1007
Instead, a separate graph is shown for each site in Figure 2(A-E). The US cutoff value or intermediate range in use ateach laboratory is indicated, and results are shown for allsamples for which both US and surfactantialbumin (ifi-tered) values were obtained. Although there are significantbetween-laboratory differences in appearance, resultingprincipally from differences in chromatographic methods,all show a strong trend of increasing surfactantialbuminvalue with increasing US ratio. Linear-regression param-
eters also reflect these differences, with slopes varying by afactor of three and intercepts ranging from -51 to 16 mg/g.The maturity cutoff value for surfactantlalbumin value (asestimated from linear regression, with use of the associatedL/S ratio cutofi), ranged from 45 to 83 mg/g.
Figure 3 shows receiver-operator characteristic analysisfor samples in which delivery occurred within three days ofsample collection. Results for surfactantlalbumin values
are shown for the 108 samples at gestational ages 26-36

0.9
0.5
0.7
0.6
0.3
0.2
0.1
RRNN
SonsSpecPPVNPV
E
Fig. 3. Receiver-operator characteristic curve analysis for samples inwhich deliveryoccurred withinthree days of sample collection#{149},Surfactant/albumin value for all samples; + surfactant/albumin value forsamples with gestatlonal ages 26-36 weeks; 0, surfactant concentration forsamples with gestational ages 26-36 weeks
R 23d 23N 32 52R 1 1N 245 225
0.96 0.960.88 0.810.42 0.310.996 0.996
22
46
2250.960.83
0.32
0.996
FALSI1 posmvs RATE
1547
177
0.940.790.240.994
Gestatlonal ages 26-36 weeksA R 21
1425
1900.930.88
0.36
0.995
1216
390.920.710.43
0.975
RNN
Sens
SpecPPVNPV
6 510 5
R 0 0 0 0 0N 47 45 42 36 19
10 20 3)) 40 50 64) 70 4)0 90 00 110 ISO 130 141) 50 160
suRFAcrM(r/ALBuMIN VALUE. mg/g
1008 CLINICAL CHEMISTRY, Vol. 35, No. 6, 1989
weeks, and for all 312 samples regardless of gestationalage, including a number for which gestational age was notknown. Because no RDS cases occurred at gestational ages>36 weeks, this category was not treated separately. Sen-sitivity for using a surfactantialbumin cutoff of 50 mg/g formaturity was 0.96 at a false-positive rate of 0.27 for thelow-gestational-age group and 0,12 for the general popula-
tion. Receiver-operator characteristic analysis for surfac-tant concentration, determined by multiplying the surfac-tant/albumin value by the albumin concentration, is alsoshown for gestational ages 26-36 weeks (7). The surfactantconcentration is not as good a predictor of RDS as thesurfactantlalbumin value, with only a 0.86 sensitivity at afalse-positive rate of 0.33.
Table 2 compares surfactantlalbumin value, US ratio,and phosphatidylglycerol with respect to their abilities topredict the presence or absence of RDS. Only those cases forwhich delivery occurred within three days of sample collec-tion are included in the analysis. US or surfactantlalbuminresults were not obtained for a few samples, and phospha-tidylglycerol results were not obtained for several samples,
which accounts for the different totals seen. For purposes ofthe evaluation, transient tachypnea cases are excluded.Two different cutoff values for the surfactantlalbumin ratioare compared. Optimizing sensitivity and specificity withthe cutoff set at 50 mg/g leaves little margin for error; themore conservative cutoff, 70 mglg, is closer to the mean ofthe cutoff values estimated from linear regression. For theUS ratio, samples with values greater than the cutoff (thehigher cutoff in the case of sites that use an intermediaterange) are considered mature. Simple presence or absenceof phosphatidylglycerol is used as predictor. For the onesite that provided semiquantitative results for phosphatid-ylglycerol, a concentration �5 ,ug/L is considered positive.In the column labeled “US + PG,” samples with an inter-mediate US ratio and a positive test for phosphatidylglyc-erol are also considered mature.
For all the cases in which delivery occurred within threedays of sample collection, we prepared a bar chart (Figure4) showing the number of patients with and without RDSas a function of surfactantlalbumin value. These barsrepresent result-specific predictive values. When surfac-tantialbumin was <30 mg/g, two-thirds of the patientsdeveloped RDS; between 30 and 50 mglg, about one-fourth
Table 2. ComparIson of PredIctive Abilities of MethodsPredlct.d� Found#{176}S/A5OC S/A70c U/S PG IJS+PG
All samples
21 20 12N 23 36 28 25R 1 1 1 1
N 63 50 56 300.96 0.96 0.95 0.920.73 0.58 0.67 0.550.48 0.37 0.44 0.320.984 0.980 0.982 0.968
Samples from vaginal pool: all gestational agesR R 8 8 7R N 5 7 9NN
SonsSpecPPVNPV
1.00 1.00 1.00 1.00 1.000.90 0.87 0.82 0.78 0.790.62 0.53 0.44 0.38 0.501.000 1.000 1.000 1.000 1.000
Test prediction of ADS (A), or no ADS (N). b Outcome of the delivery.
C Surfactant/albumin value with maturity cutoff of 50 or 70 mg/g. d Number of
cases In this category. PG, phosphatidylglycerol; PPV, predictive value of apositive result;NPV, predictive value of a negative result.
59
26
24
22
20
IS
16
4
12
10
0
Fig. 4. Plot of number of patients vs surfactant/albumin value forsamples for which delivery occurred within three days of samplecollectionBlao1#{231}RDS; hatched, transient tachypnea; white, normal respiratory outcome
developed RDS. Of 64 deliveries for which TDx values werebetween 50 and 90 mglg, only one RDS case was seen, andnone above 90 mg/g.
Of the 312 samples representing delivery within threedays of sample collection, 21 were visibly contaminatedwith blood, and 10 with meconium. Of these, all but onewere given the same maturity assessment by US ratio andsurfactantialbumin value. The one exception was a blood-

Case Gestation, S/A,C AlbumIn, Surfactant cones,She Id. weeks US#{176} p�b mg/g 9/U mg/Ld
29 - 6 1.91
27 8 5.29
32 8 1.86
30 8 2.9329 - 9 4.1326 - 10 6.4228 1.3 - 10 2.62
31 1.4 - 11 1.45
32 1.3 - 17 2.82
Comments
Vaginal pool sample
Vaginal pool sample
2.4#{176} - 49 0.72
1.9 + 81 1.97
‘Immature values except where noted. 0Phosphatidylglycerol: -, absent; + present; or (blank),not assayed. C Surfactant/albumlnvalue, #{176}Product of S/A valueand albumin concentration. #{149}Intermediate maturity value. ‘Mature value.
CLINICAL CHEMISTRY, Vol.35, No. 6, 1989 1009
stained sample that was associated with a mature outcome;outcome was predicted as immature by US ratio andmature by surfactantlalbumin value.
Table 3 lists the RDS cases encountered in the study, inorder of increasing surfactantlalbumin value. Cases E68and C136 were falsely predicted as mature by US ratio andphosphatidylglycerol determination, respectively. Case
C136 would also be predicted as mature by surfactantlalbumin value. Interestingly, cases C136 and C128, whichhave the highest surfactantlalbumin values of the RDScases, involved fetal anomalies affecting the urinary tract:the former infant had hydronephrosis due to a blocked
ureteropelvic junction, and the latter an unspecified uri-
nary tract blockage and renal failure.
Discussion
In the majority of pregnancies, there is no need fordetermination of lung maturity. But when preterm deliv-ery is being considered, such measurement is highly valu-able. The cutoff value in a test used to predict maturitydepends on what risk of RDS may be tolerated, and this isdetermined by other risk factors in the pregnancy. Inpregnancies complicated by premature rupture of mem-branes, Rh incompatibility, placenta previa, pre-eclampsia,and other conditions, the danger of RDS due to prematuredelivery must be balanced against the risks to mother orfetus from the complicating factor.
TDx FLM is based on an earlier method in which thefluorescence polarization of a dye dissolved in amniotic fluidwas used as the index of lung maturity (11). After modifica-tion of the dye to improve stability and working characteris-tics, the method was studied to determine the factors that
contribute to the signal (7). Phospholipid and albumin were
found to be the only amniotic-fluid components needed tomodel its behavior, so results were expressed as the phospho-
lipid/albumin ratio. Ivie and Swanson (12), studying the effectof surfactant and albumin isolated from amniotic fluid on thefluorescence polarization of the dye, demonstrated that sur-factant components other than phospholipid also contribute tothe signal. Results are best understood as the ratio of surfac-t.ant to albumin, indexed to primary standards consisting ofdioleylphosphatidylcholine and human albumin. Measure-ment of modified samples demonstrated that low amounts ofadded blood and meconium have relatively little effect,whereas the effects of greater contamination can be rational-
ized in terms of contribution of phospholipid and albuminfrom the contaminant (7).
The wide range of linear-regression parameters in the plotsof surfactantlalbumin value vs US ratio among the reportinginstitutions underscores the variability in US ratio methodscurrently in use. This is to be expected in any such complexprocess. Centrifugation of amniotic fluid, extraction of thephospholipid fraction, acetone precipitation, activation ofthin-layer chromatography plates, techniques for applyingsamples, developing solvents, visualization procedures, andmethod of quantifying the density or area of the spots may all
vary between labs. The relatively low frequency with whichthe test is performed makes it difficult to determine thematurity cutoff value for each laboratory, but the lack ofstandardization of techniques makes it essential. TDx FLMoffers a simplicity of operation that ensures replicabiity,permitting unqualified exchange of results between laborato-ries. Because the required instrumentation is currently pre-
sent in many laboratories, assessment of fetal lung maturitymay become available at sites where it was previously toocumbersome to perform.
Table 3. CharacteristIcs of RDS Cases
C 159B 102
A 46
B 55C 148
E 58C 48
C 149
E 19B 24C 38B 42B 97C 56A 109
A 94
A 113C 98
C 95
A 28
E 68B 120
C 128
C 136
0.91.40.91.3
1.4
28 1.4
31 1.1
30 1.7
33 0.729 1,834 1.6
36 1.5
0.833 2.4#{176}
35 1.71.6
29 2.6’
28 1.5
31
34
17 4.55
- 22 1.9428 3.04
29 1.23- 30 1.47
30 5.26
- 31 2.25- 33 2.97
- 33 1.50
- 37 1.46- 41 1.25
- 42 3.82
44
12
4115
2538
652716
47764385
3644
158
709850
5551
160
35159
Rh isoimmunization
Vaginal pool sampleVaginal pool sample
Vaginal pool sample
Maternal diabetesVaginal pool sampleVaginal pool sampleVaginal pool sample
Fetal urinary obstructionFetal hydronephrosls

1010 CLINICAL CHEMISTRY, Vol. 35, No. 6, 1989
The most informative way to show the relationship
between sensitivity and specificity of a diagnostic assay is
through receiver-operator characteristic curve analysis (9).This method showed TDx FLM to have its optimum sensi-tivity and specificity at a surfactant/albumin cutoff of 50mglg. However, linear-regression results suggested that asurfactantlalbumin value of 70 mg/g corresponds moreclosely with the US cutoffs in use at most sites. Because theTDx FLM and US methods measure different features,only indirectly related, of the amniotic fluid, we suggestthat greater weight be given to the receiver-operator char-
acteristic analysis, which relates assay performance to
actual outcome. With the cutoff for maturity set at 50 or 70mg/g, TDx FLM predicted RDS and its absence as well asthe US ratio and significantly better than did phosphatid-ylglycerol. Samples obtained from vaginal pooi were aspredictive as amniocentesis samples. Performance of TDxFLM was somewhat decreased at lower gestational ages;however, its results stillcompared favorably with US ratioand phosphatidylglycerol determination.
The bar chart of Figure 4 is probably the most practicallyuseful result of this study, by providing an indication of the
probability of RDS, given a particular surfactantialbumin
ratio. The chart can be divided into roughly four ranges of
surfactantlalbumin values:#{149}a value <30 mg/g should be considered definitely im-
mature#{149}a value between 30 and 50 mg/g should be consideredrisky (though other conditions may weigh more heavilyin the decision of whether to deliver)
#{149}a value in the range 50-70 mg/g should be treated withcaution, pending further studies, and
#{149}a value >70 mg/g indicates a small likelihood of RDS.More data, especially in the 30 to 70 mg/g range, are
clearly desirable. Although samples of intermediate matu-rity are obtained less frequently than the more-definitivesamples, use of the standardized TDx FLM method permitsaccumulation of data from a large number of labs. Figure 4was prepared with data from all samples with knownoutcome and delivery within three days of sample collec-tion. Further studies would also be useful to generatesimilar charts for pregnancies with various complications,and by gestational age group, given that the specificity ofall tests appears less at lower gestational ages.
Significant disagreement in prediction is apparent fromthe plots of surfactantialbumin value vs US ratio. This is to
be expected, because the two tests measure different mate-rials. Thus a clinician might use a combination of the two
to improve either sensitivity or specificity. In the presentstudy, there were insufficient cases to analyze adequatelythe value of such a combination.
The two infants in the study with both RDS and urinarytract blockages also had the highest surfactant/albuminvalues associated with RDS. The presence of fetal urinary
tract blockage is strongly correlated with delayed lungdevelopment, often resulting in RDS after delivery at arelatively advanced gestational age (13). In the absence offetal urine output, a larger portion of the amniotic fluidwould consist of lung effluent, which may explain thediscrepant TDx results in these cases. Fluid accumulationdue to blockage of the kidney or urinary tract is easily seenby ultrasound, which is routinely performed as an adjunctto amniocentesis. Until further studies have unambig-uously characterized the effect of urinary tract blockages
on the assay performance, such a finding should be consid-ered an indication for confirmation of mature test resultsby alternative means.
In amniocentesis, occasionally the urinary bladder is punc-tured by mistake, and urine is collected instead of amnioticfluid. In this case, chromatography will show no spots corre-sponding to phospholipids, and no result can be obtained.Fluorescence polarization, however, will give a surfactantialbumin result,which may be in the mature or the immatureregion, depending on the minute amounts of material carriedover from the previous sample. However, the fluorescenceintensity will be much lower than that of an amniotic-fluidsample, and so the result can be invalidated.
Note that the surfactant concentration is not as good anindicator of lung maturity as the surfactantialbumin ratio.This is consistent with earlier findings that total phospho-lipid concentration is less accurate than US ratio at pre-dicting lung maturity (14). Albumin appears to work as aninternal standard in the Thx method, accounting forchanges in the overall amniotic-fluid concentration due tonormal variations in patterns of fetal swallowing andurination. Sphingomyelin was originally included in theUS ratio to account for variations in the efficiency ofextraction of phospholipids from the amniotic fluid. Appar-ently, its role is even more extensive, accounting for vari-ations in overall phospholipid concentration in the amnio-tic fluid. This suggests that other tests for fetal lungmaturity that base their prediction on a simple concentra-
tion may improve their predictive ability by measuring aninternal standard as well.
References1. Gluck L, Kulovich MV, Borer RC, Brenner PH, Anderson GG,Spellacy WN. Diagnosis of the respiratory distress syndrome byamniocentesis. Am J Obstet Gynecol 197 1;109:440-5.2. Kulovich MV, Hallman MB, Gluck L. The lung profile. I.Normal pregnancy. Am J Obstet Gynecol 1979;135:57-63.3. Torday J, Carson L, Lawson E. Saturated phosphatidylcholinein amniotic fluid and prediction of the respiratory-distress syn-
drome. N Engi J Med 1979;301:1013-8.4. Tsai MY, Shultz EK, Williams F?, et al. Assay of disaturatedphosphatidylcholine in amniotic fluid as a test of fetal lungmaturity: experience with 2000 analyses. Clin Chem 1987;33:1648-51.5. Statland BE, Sher G. Reliability of amniotic fluid surfactantmeasurements. Am J Clin Pathol 1985;83:382-4.6. Russell JC. An easy method for assessment of fetal lungmaturity. Clin Chem 1986;32:1097.7. Russell JC. A calibrated fluorescence polarization assay forassessment of fetal lung maturity. Clin Chem 1987;33:1177-84.8. Buncher CR, Weiner D. Reference values. In: Kaplan LA, PesceAJ, eda. Clinical chemistry. St. Louis: CV Mosby Co., 1984:301-9.9. Richardson DK, Schwartz JS, Weinbaum PJ, Gabbe SG. Diag-nostic tests in obstetrics: a method for improved evaluation. Am J
Obstet Gynecol 1985;152:613-8.10. Oulton M. The role of centrifugation in measurement of sur-
factant in amniotic fluid. Am J Obstet Gynecol 1979;135:337-43.11. Tait JF, Franklin RW, Simpson JB, Ashwood ER. Improvedfluorescence polarization assay for use in evaluating fetal lungmaturity. I. Development of the assay procedure. Clin Chem1986;32:248-.54.12. Ivie WM, Swanson JR. Effect of albumin and lamellar bodieson fluorescence polarization of amniotic fluid. Clin Chem 1987;33:1194-7.13. Furlong LA, Williamson RA, Bonsib 5, Epley 5, Pringle K.Pregnancy outcome following ultrasound diagnosis of fetal urinarytract anomalies andior oligohydramnios. Fetal Ther 1986;1:134-45.14. Schreyer P, Tamir I, Bukovski I, Weinraub Z, Caspi E.Amniotic fluid total phospholipids versus lecithinlsphingomyelinratio in the evaluation of fetal lung maturity. AmJ Obstet Gynecol1974;120:909-17.





























