-
J. clin. Path., 1973, 26, 413-421
Mucinous cystadenoma and cystadenocarcinomaof the vermiform
appendix with particularreference to mucocele and
pseudomyxomaperitoneiN. M. GIBBS
From the Area Laboratory, St Luke's Hospital, Guildford, and the
Research Department,St Mark's Hospital, Londont
SYNOPSIS Ten cases of mucocele of the vermiform appendix are
described. Eight cases were ofmucinous cystadenoma of the appendix
and six cases showed acute inflammation. Two of the sixcases showed
pseudoinvasion of the appendix and in a further case the appendix
had perforatedwith extrusion of a misplaced neoplasm. Two cases
were of mucinous cystadenocarcinoma and oneof these was diagnosed
as 'pseudomyxoma peritonei'. 'Pseudomyxoma peritonei' is a misnomer
andis caused by dissemination of a mucinous cystadenocarcinoma
within the peritoneal cavity. Thespecial problems of histological
diagnosis are discussed.
Mucocele of the appendix is an uncommon butmysterious condition
about which a large volume ofliterature has accumulated without
much clarifica-tion of the underlying pathology. There are two
maintheories of causation. The first can be termed the'obstructive'
theory because it is thought that thedistal mucosa of the appendix
is stimulated toproduce an excessive secretion of mucin, as a
resultof proximal obstruction of the lumen by faeces,inflammatory
fibrosis, or the presence of a neoplasm(Elliott, 1957). The second
theory, which is anextension of the first, asserts that the mucosa
of theobstructed appendix undergoes an ill definedneoplastic change
which has been termed 'adeno-carcinoma grade I' (Woodruff and
McDonald,1940) or papillary mucus-secreting carcinoma in
situ(Scimeca and Dockerty, 1955).The mystery deepens when
'pseudomyxoma
peritonei', which is a complication of mucocele ofthe appendix,
is considered. The original hypothesis(Werth, 1884) postulates that
peritoneal irritation,produced by the leakage of mucus from a
burstmucocele, causes a metaplastic reaction to takeplace in the
mesothelial cells so that mucin is formedlocally in the peritoneal
cavity. Other hypothesesaccept that malignant adenocarcinomas of
theappendix can produce pseudomyxoma peritonei, butthere is also
the opinion that it may occur in theReceived for publication 5
April 1973.
presence of a neoplasm which is not invasive orwhere there is an
abnormal epithelium which is notneoplastic.The object of this paper
is to describe the histology
of 10 appendices and to consider the underlyingpathology with
particular relation to mucocele andpseudomyxoma peritonei.
Materials and Methods
The appendices were fixed in 10% formal saline.Coronal blocks in
sequence were taken so that theentire appendix was examined in each
case with theexception of cases 3, 6, and 10. Sections were cut
at5,u and stained routinely by Ehrlich's acid haema-toxylin and
counterstained with eosin. Specialstains included phloxine
tartrazine for Paneth cells,the diazo method, and Fontana's silver
impregna-tion for enterochromaffin granules, alcian blue, andPAS
(pH 2 6) for mucin.The cases are summarized in table I.
Histology
The histological details of cases 1-10 are given intable II.
Cases 1-8 showed a replacement of the liningepithelium of the
surface and the glands by tallcolumnar mucinous epithelium which
characteris-413
on April 5, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.26.6.413 on 1 June 1973.
Dow
nloaded from
http://jcp.bmj.com/
-
Case No. Date Sex Age in Clinical History Follow UpYears
1 March 1972 76 Incidental finding at necropsy for basilar
arterialthrombosis
2 March 1971 V 59 Presented with acute abdominal pain, and
laparotomy Complete recoveryrevealed perforated diverticulum of the
caecum and amucocele of the appendix. The appendix was removed.
3 November 1957 54 Presented with acute abdominal pain and
Complete recoveryappendicectomy was done followed by an
intervalright hemicolectomy.
4 June 1972 47 Acute abdominal pain followed by appendix mass
for Complete recoverysix weeks, and appendicectomy
5 September 1972 37 Acute appendicitis and appendix mass
followed by Complete recovery'interval' appendicectomy three months
later
6 January 1957 70 Acute appendicitis associated with localized
abscess Alive and well whenfilled with mucoid pus last seen in
1963
7 March 1972 70 Acute appendicitis and appendicectomy Complete
recovery8 October 1972 71 Abdominal pain followed by a mass in the
abdomen Complete recovery
for four months; this was explored and an inflamedperforated
distended appendix was removed.
9 June 1965 54 Two-day history of abdominal pain and distension;
Complete recoveryan appendicectomy was done. A right
hemicolectomywas done six weeks later
10 May 1971 d 45 There was abdominal pain and swelling for two
Disseminated intra-months; an abscess in the lower abdomen was in-
abdominal adeno-cised and drained in May 1971. This recurred and
much carcinomamucus was evacuated. A diagnosis of
pseudomyxomaperitonei was made and a right hemicolectomy wasdone.
Further accumulation of mucin occurred anda metastasis in the
abdominal wall was biopsied inJune 1972.
Table I Clinical details of cases I to 10
tically showed basal crowding of nuclei and thepresence of
numerous mitoses. The epitheliumlooked neoplastic, and villous
processes weredeveloped in some cases (cases 4 and 5) with
anappearance identical to the villous adenomas of thelarge
intestine. In addition the glands were tortuousand showed lateral
branching and budding of cystictubules (figs 1, 2, and 3). There
were numerousmitoses and the basi-glandular cells of the
cryptstended to be displaced by mucinous epithelium. Thusthe Paneth
cells disappeared and argentaffin cellswere diminished and
displaced, a common factor inneoplasms of the intestine which
distinguishes themfrom hyperplasias and heterotopias (Gibbs,
1967).Polypoid mucosal hyperplasia (metaplasia) mayoccur in the
appendix (MacGillivray, 1972) but theepithelium, although tall,
only shows occasionalgoblet cells whilst the surface epithelial
cells have aveiled or fronded appearance.
Cases 1 and 2 showed 'sac-like' dilatations(mucoceles) and here
there was widespread pressureatrophy of the lining epithelium (fig
4) and partialreplacement by granulation tissue with a
'foreign-body' giant cell reaction. The glands were stretchedby
accumulated mucin and many had disappeared.Nevertheless the
characteristic neoplastic epitheliumwas preserved in occasional cul
de sacs. It would seem
that further development of the tumours wasimpeded by mucus
retention.
Cases 1, 2, 4, and 5 showed partial or completeorganic
obstruction of the proximal lumen byfibrous tissue which had
replaced or constricted theepithelial lining. It is possible that
obstruction wasdue to congenital absence of part of the mucosa
orpossibly to an episode of localized proximal inflam-mation. It
seems more likely, however, that the viscidmucin secreted by the
tumour was unable to draininto the caecum so that the adjacent
normal mucosaunderwent pressure atrophy. The thickened tumourmucosa
may have blocked the proximal lumen but ineither event the normal
mucosa will be subject tocompression and inflammation with eventual
atrophyand reactive fibrosis as sequelae. Alternativelyblockage
could result from calcified inspissatedmucus (case 5, fig 5). It
seems that if free drainage ofmucin from the tumour were possible a
saculardilatation (mucocele) of the appendix would notdevelop.
Cases 3, 4, and 5 did not show diffuse dilatation ofthe
appendices but instead developed diverticulaThese diverticula
bulged through and betweenthe muscle coats and formed lakes of
mucus lined inpart by mucinous epithelium. Acute inflammationhad
occurred with consequent perforation and
414 N. M. Gibbs
on April 5, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.26.6.413 on 1 June 1973.
Dow
nloaded from
http://jcp.bmj.com/
-
415Mucinous cystadenoma and cystadenocarcinoma of the vermiform
appendix
Case Macroscopic Lumen Microscopic Description Appendix Other
InformationNo. Description Diverticulum
I Appendix (6 x 2 Proximal half of The distal mucosa was
replaced bycm) showed gross lumen showed columnar mucinous
epithelium which wasdistension of distal fibrous obliteration.
stretched and flattened. Most of the cryptshalf by mucus. had
disappeared.
2 Appendix (6 x 1-5 Proximal lumen The distal mucosa was
replaced by tallcm) showed gross showed fibrous columnar mucinous
epithelium. The glanddistension of distal obliteration. crypts had
disappeared.part by mucus.
3 Appendix showed The mucosa of the dilated part wasdistension
of the replaced by tall columnar mucinousmiddle part by epithelium
which showed areas of flatteningmucin and pus. and
inflammation.
4 Appendix (4 x 0-8 Proximal lumen The distal mucosa was
replaced by tallcm) showed distal showed fibrous columnar mucinous
epithelium showingdilatation (1-5 x I obliteration. branched
papillary processes, but foci ofcm) and globules atrophy and
inflammation were present.of mucin could beseen beneath
theperitoneal coat.
5 Appendix (5 x 2 Proximal lumen The distal mucosa was replaced
by tallcm) showed distal obliterated by mucinous columnar
epithelium whichdilatation and was fibrous tissue; formed papillary
processes projecting intofilled with mucin distal lumen the lumen.
The glands were elongated andand pus. There was contained a showed
pronounced lateral branching andan old perforation calculus mitotic
activity.with adhesion to thecaecum and adeposit of
jelly-likemucin.
6 Appendix was The distal mucosa was replaced bydistended with
pus disrupted tall columnar mucinous epitheliunand mucus and There
was diffuse acute purulentthere was a perfora- inflammation.tion
and abscess.
7 Appendix distended Acute purulent inflammation of theby pus
and mucin; appendix; crypts were replaced by atypicaladherent to
caecum tall columnar mucinous epithelium whichwhich showed showed a
surface villous pattern andgangrenous necrosis. tortuous
glands.
8 Appendix was There was marked inflammatory thickeningdistended
with pus and the mucosa was replaced by talland mucus and was
mucinous columnar epithelium. There wereperforated. surface villous
processes and hyperplastic
9 Appendix (6 x 3 Patentcm) was sealed withomentum and hadnot
perforated.The distal three-quarters of theappendixwere distended
bymucin and the wallwas thickened.
10 Appendix wasfragmented andinvolved by atumour mass and
anabscess.
glands although in places the epitheliumwas stretched and
attenuated.The proximal glands were normal but theremainder were
hyperplastic and replacedby tall columnar
mucin-secretingepithelium. The distal half was infiltratedby
mucinous adenocarcinoma showing alarge glandular pattern;
'signet-ring' cellswere present; numerous argentaffincells in both
large tubules and 'signet-ring'cells.
There was a primary mucinousadenocarcinoma of the appendix with
acomplex acinar pattern, and surrounded by'lakes' of mucin.
Argentaffin cells were notseen.
Absent
Absent
Present No residual growthfound in caecum andascending colon
Present
Rupture of diverti-culum into theinterstitial tissues ofthe
appendix and'displacement' offragmented mucosa
No extension ofgrowth into caecum;lymph glands inappendix
mesenterydid not containmetastases.
m.
Absent
Epithelium was dis-placed into the musclecoats at the site
ofperforation but nodiverticulum.
Absent An interval righthemicolectomy wasdone and the
ileo-caecal lymph glandscontained metastases.
Diffuse invasion ofthe peritoneum; nodiverticulum
Interval right hemi-colectomy showedcarcinoma of theappendix
invading thecaecum; developedmetastases inabdominal wall.
Table II Histology ofappendices
9
on April 5, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.26.6.413 on 1 June 1973.
Dow
nloaded from
http://jcp.bmj.com/
-
j , v -j Fig 2
Fig I
Si ~ ~ A
Fig 3
W x,s,, :' '~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~4
Fig 4
on April 5, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.26.6.413 on 1 June 1973.
Dow
nloaded from
http://jcp.bmj.com/
-
Mucinous cystadenoma and cystadenocarcinoma of the
vermiformappendix4
v.g.4 fjK,
A :iS, -4X fN
VI.
s v\" 9 ~Fig 7
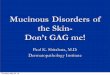
'\t Fig 1 Case 5: mucinous cystadenoma of the appendixlined by
tall columnar mucinous epithelium
N\ (haematoxylin and eosin x 100).
Fig 2 Case 4: mucinous cystadenoma of the appendixshowing
replacement of surface and glandular epithelium
8'23% by tall mucinous epithelium (haematoxylin and eosinx
80).Fig 3 Case 3: inflamed mucocele showing distorted
i villous epithelium (haematoxylin and eosin x 63).
L s * Fig 4 Case 1: mucocele of the appendix showingprogressive
flattening of the lining epithelium (haema-
F 'f j toxylin and eosin x 63).F Fig 5 Case 5: mucinous
cystadenoma ofappendix
showing villous processes and calcified secretion(calculus)
(haematoxylin and eosin x 63).
Fig 6 Case 5: epithelial displacement and_ pseudoinvasion in a
perforated mucocele ofappendix
(haematoxylin and eosin x 63).
Fig 7 Case 5: epithelial displacement andpseudoinvasion in a
perforated mucocele ofappendix(haematoxylin and eosin x 100).
*.:
-. m
Fig 6
417
on April 5, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.26.6.413 on 1 June 1973.
Dow
nloaded from
http://jcp.bmj.com/
-
418
. y#.'*
;P\4
¶sft.
t~~~~~~~4
VA4
$
41
i Fig 8 Case 4: interstitial'. t ** mucin showing muciphages
q ' 0 Jr (haematoxylin and eosinIC I x 80).
O.
f..
i'
.
U't
Fig 9 Fig 10Fig 9 Case 9: mucinous cystadenocarcinoma of
appendix showing junction with normal epithelium and the
formationoj'surface villous processes (haematoxylin and eosin x
100).Fig 10 Case 9: mucinous cystadenocarcinoma of appendix
(haemstoxylin and eosin x 100).
N. M. Gibbs
v.
. -'s 0.0 Ar0 . to..
..r .,:r
W
on April 5, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.26.6.413 on 1 June 1973.
Dow
nloaded from
http://jcp.bmj.com/
-
Mucinous cystadenoma and cystadenocarcinoma of the vermiform
appendix
Fig 11 Fig 12Fig 11 Case 9: mucinous cystadenocarcinoma of
appendix showing numerous argentaffin cells (Fontana's sill
ercounterstained with saffranin, x 100).Fig 12 Case 10: mucinous
cystadenocarcinoma of appendix with abdominal metastasis
(haematoxylin and cosinx 63).
disruption of the lining epithelium. Strips of
displacedepithelium could be seen lying interstitially producinga
semblance of invasion (figs 6 and 7) and mucinousepithelium had
grown through the perforationtracks in cases 4 and 5. Large numbers
of macro-phages were present in the interstitial mucin and
thiscomplicated the histology (fig 8).
Cases 1-8 cover the histological 'spectrum' of anepithelial
neoplasm of the appendix which isconsidered to be a primary
mucinous cystadenoma.It can be seen that considerable variations in
his-tology occur in these neoplasms which appear to bethe result of
local factors influencing tumourgrowth.Case 9 was an invasive
mucinous neoplasm of the
appendix forming large numbers of argentaffin cellsand was
considered to be a primary mucinous cysta-denocarcinoma of the
appendix (figs 9, 10, and 11).
There was acute appendicitis wihout perforation sothat
peritoneal dissemination had not occurredalthough there were
lymphatic metastases. Case 10was a similar tumour but perforation
and appendixabscess had occurred which was followed by
dis-se;mination of the mucinous cystadenocarcinomawithin the
peritoneal cavity and 'pseudomyxomaperitonei' (fig 12).
Discussion
Mucinous cystadenoma of the appendix is anuncommon tumour which
secretes viscid mucus thattends to accumulate within the lumen so
that itbecomes distended to produce a mucocele. If thelumen
proximal to the tumour is narrow, the mucusmay not drain. However,
four of the mucocelesdescribed here are associated with severe
narrowing
419
on April 5, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.26.6.413 on 1 June 1973.
Dow
nloaded from
http://jcp.bmj.com/
-
N. M. Gibbs
or complete obstruction of their lumina which isprobably related
to abnormalities in development ofthe organ or subclinical episodes
of acute inflam-mation. It is evident that epithelial displacement
andpseudoinvasion are related to definite clinicalepisodes of acute
appendicitis. In longstanding casescalcification of inspissated
mucus (case 5) may resultin the formation of an appendiceal
calculus (Bunch,1945) which may be detected
radiographically(Marshak and Gerson, 1960).Mucinous cystadenoma of
the intestine is found,
it seems, only in the appendix. However, it sharesmany of the
morphological characteristics of villousadenoma of the colon and it
can be argued that thetumours described are in fact villous
adenomas whichhave been altered by the confines of the
appendix.Nevertheless it is known that epithelial neoplasms ofthe
appendix show significant differences fromneoplasms elsewhere in
the intestine. For example,the appendix is the most common site of
carcinoidtumours which, in this situation, are almost alwaysbenign,
often show mucin secretion, and may con-tain Paneth cells.
Furthermore some primaryadenocarcinomas of the appendix show
histologicalfeatures not found in other organs.The cases of
mucocele described in this paper show
the characteristic epithelial abnormalities common toreports in
the literature when a detailed examinationof the appendix has been
made. The nature of theabnormalities, however, has been fogged by
muchdubious and imprecise terminology. Many authorshave been unable
to decide whether the epitheliallesion is metaplastic or
neoplastic, benign ormalignant, and others diagnose carcinoma in
situ,which is a concept best avoided in the considerationof
neoplasms of the intestine. The reasons for theapparent
contradictions seem to depend on specialproblems of interpretation.
The neoplastic epitheliumforming the mucocele may undergo
deformation dueto pressure of accumulated mucus so that
theepithelium may become flattened or atrophic. Thusthe neoplastic
epithelium of the mucocele may passunrecognized unless a detailed
histological examina-tion of the appendix is undertaken.
Furthermore, theneoplastic cells of the mucocele, whether invasive
ornot, usually do not show cytological proof ofmalignancy, a
finding in common with otherneoplasms of the intestinal tract. The
presence oflarge pools of mucin may distort local anatomy andwhen
perforation takes place the epithelium may bedisplaced and extruded
into the peritoneal cavitysimulating invasion. A similar problem of
inter-pretation is encountered in adenomatous polyps ofthe colon,
which may show displacement of glan-dular tissue into the stalk.
This displacement may bemistaken for malignant transformation and
invasion.
It can be seen, therefore, that a distinction betweenbenign and
malignant mucinous cystadenoma maybe a difficult problem. This
provides an explanationfor the observation made by Hilsabeck, Judd,
andWoolner (1951) that the majority of cases
diagnosedhistologically as malignant failed to progress oncethe
mucocele was removed and that only two of 18patients with mucocele
developed pseudomyxomaperitonei and died. The clinical diagnosis
may alsobe problematic as a very large pseudocyst filled withmucin
may form around a perforated mucocelewhich may be mistaken for
'pseudomyxoma peri-tonei' (Early, Stephenson, and Davis,
1968).However, the problem of interpretation is simplifiedif the
histologist is aware of the possibility ofpseudoinvasion by
displaced islands of neoplasticepithelium in an area of
inflammation. Conclusiveevidence of tissue invasion must be found
before adiagnosis of mucinous cystadenocarcinoma is madeand this
was readily available in the examplesdescribed (cases 9 and 10).
Benign mucinouscystadenomas (mucoceles) should be treated
byappendicectomy and more radical procedures
areunnecessary.Mucinous cystadenocarcinoma behaves as an
invasive neoplasm (cases 9 and 10). Such tumours,in common with
other mucinous adenocarcinomasof the intestinal tract, may produce
by differentiationlarge numbers of argentaffin cells and have
beenmistaken for carcinoids (Evans and Murphy, 1959).A tumour which
invades and disseminates within theperitoneal cavity after the
appendix has been totallyremoved must be regarded by definition as
malig-nant.The alarming clinical features produced by dis-
semination of a mucinous carcinoma within theperitoneal cavity
were described by Fraenkel (1901)in relation to mucocele of the
appendix. He used theterm 'pseudomyxoma peritonei', which had
originallybeen given by Werth (1884) to describe a similarclinical
picture associated with 'cystadenoma' ofthe ovary. Certainly
pseudomyxoma peritonei is amisnomer with emotive connotations which
eventoday causes histologists and clinicians to cast
asiderecognized precepts of disease. It should be leftbehind with
the past.
I wish to thank Dr B. C. Morson and the surgeonsof St Luke's
Hospital, Guildford, St Peter's Hospital,Chertsey, and St Mark's
Hospital, London, forpermission to study their patients, and Dr G.
F. Rossfor pathological material of two cases.References
Bunch, G. H. (1945). Mucoid disease of the appendix. Ann. Surg.,
121.704-709.
Earls, K. S., Stephenson, D. V., Jr., and Davis, W. C. (1968).
Giant
420
on April 5, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.26.6.413 on 1 June 1973.
Dow
nloaded from
http://jcp.bmj.com/
-
Mucinous cystadenoma and cystadenocarcinoma of the vermiform
appendix
retroperitoneal mucocele simulating pseudomyxoma peritoneiand
mucinous adenocarcinoma. Amer. J. Surg., 116, 439-443.
Elliott, C. E. (1957). Two cases of pseudomyxoma peritonei
frommucocele of the appendix. Brit. J. Surg., 45, 15-18.
Evans, R. W., and Murphy, A. F. (1959). Pseudomyxoma
peritoneiassociated with an appendix obstructed by an
argentaffinoma(carcinoid) in a male. Brit. J. Surg., 47,
166-172.
Fraenkel, E. (1901). Uber das sogenannte pseudomyxoma
peritonei.Munch. med. Wschr., 48, 965-970.
Gibbs, N. M. (1967). Incidence and significance of argentaffin
andPaneth cells in some tumours of the large intestine. J.
clin.Path., 20, 826-831.
Hilsabeck, J. R., Judd, E. S., Jr., and Woolner, L. B. (1951).
Sym-posium on surgical aspects ofcancer problem: carcinoma of
the
vermiform appendix. Surg. Clin. N. Amer., 31,
995-1011.MacGillivray, J. B. (1972). Mucosal metaplasia in the
appendix. J.
clin. Path., 25, 809-81 1.Marshak, R. H., and Gerson, A. (1960).
Mucocele of the appendix.
Amer. J. dig. Dis., 5, 49-54.Scimeca, W. B., and Dockerty, M. B.
(1955). Carcinoma of the vermi-
form appendix: a review of the literature and report of a
case.Proc. Mayo Clin., 30, 527-534.
Werth, R. (1884). Klinische und anatomische Untersuchungen
zurLehre von den Bauchgeschwiilsten und der Laparotomie.
Arch.Gynik., 24, 1)0-118.
Woodruff, R., and McDonald, J. R. (1940). Benign and
malignantcystic tumors of the appendix. Surg. Gynec. Obstet., 71,
750-755.
Reports and Bulletins prepared by the Association of Clinical
Biochemists
The following reports and bulletins are published by the
Association of Clinical Biochemists. They may be obtainedfrom The
Administrative Office, Association of Clinical Biochemists,
7Warwick Court, Holborn, London, WC1R5DP.The prices include
postage, but airmail will be charged extra. Overseas readers should
remit by British Postal or MoneyOrder. If this is not possible the
equivalent of 50p is the minimum amount that can be accepted.
SCIENTIFIC REPORTS3 Automatic Dispensing Pipettes. An assessment
of 35commercial instruments 1967 P. M. G. BROUGHTON,A. H.
GOWENLOCK, G. M. WIDDOWSON, and K. A. AHLQULIT80p ($2)
4 An Evaluation of five Commercial Flame Photometerssuitable for
the Simultaneous Determination of Sodiumand Potassium March 1970 P.
M. G. BROUGHTON andJ. B. DAWSON 80p ($2)
SCIENTIFIC REVIEWS
1 The Assessment of Thyroid Function March 1971F. V. FLYNN and
J. R. HOBBS 60p ($1.50)
2 Renal Function Tests Suitable for Clinical PracticeJanuary
1972 F. L. MITCHELL, N. VEALL, and R. W. E.WATTS 60p ($1.50)
TECHNICAL BULLETINS
9 Determination of Urea by AutoAnalyzer November1966 RUTH M.
HASLAM 40p ($1)
11 Determination of Serum Albumin by AutoAnalyzerusing
Bromocresol Green October 1967 B. E. NORTHAMand G. M. WIDDOWSON 40p
($1)
13 An Assessment of the Technicon Type H SamplerUnit March 1968
B. C. GRAY and G. K. MCGOWAN40p ($1)
14 Atomic Absorption Spectroscopy. An outline of itsprinciples
and a guide to the selection of instrumentsMay 1968 J. B. DAWSON
and P. M. G. BROUGHTON40p ($1)
15 A Guide to Automatic Pipettes (2nd edition) June1968 P. M. G.
BROUGHTON 40p ($1)
16 A Guide to Automation in Clinical Chemistry May1969 P. M. G.
BROUGHTON 60p ($1.50)17 Flame Photometers (2nd edition) 1969 P.
WILDINO60p ($1.50)18 Control Solutions for Clinical Biochemistry
(4thedition) March 1970 P. M. 0. BROUGHTON 60p($1.50)19
Spectrophotometers. A comparative list of low-pricedinstruments
readily available in Britain May 1970C. E. WILDE and P. SEWELL 60p
($1.50)20 Quantities and Units in Clinical Biochemistry June1970 P.
M. G. BROUGHTON 60p ($1.50) More than30 copies in units of 10 at
20p21 Filter Fluorimeters: A comparative list of 18 instru-ments
September 1970 H. BRAUNSBERG and s. s.BROWN 60p ($1.50)22 Bilirubin
standards and the Determination of Bilirubinby Manual and Technicon
AutoAnalyzer MethodsJanuary 1971 BARBARA BILLING, RUTH HASLAM,
andN.WALD 60p ($1.50)23 Interchangeable Cells for
Spectrophotometers andFluorimeters September 1971 E. S. BROWN and
A. H.GOWENLOCK 60p ($1.50)
24 Simple Tests to Detect Poisons March 1972 B. W.MEADE et al.
60p ($1.50)25 Blood Gas Analysers May 1972 K. DIXON 60p($1.50)26
Kits for Enzyme Activity Determination September1972 s. B. ROSALKI
and D. TARLOW 80p ($2.00)27 Assessment of Pumps Suitable for
Incorporation intoExisting Continuous Flow Analytical Systems
November1972 A. FLECK et al 60p ($1.50)
421
on April 5, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.26.6.413 on 1 June 1973.
Dow
nloaded from
http://jcp.bmj.com/