Embed Size (px)
Citation preview
Embryo and Implantation Disorders
Bolarinde Ola FRCOG MD

Outline
• Embryo and Embryo grading• Implantation physiology• Implantation failure • (Recurrent) Implantation failure• How to manage (recurrent ) implantation
failure?

Grades of (Day 3) Cleavage Stage Embryos:
Grade DescriptionGrade 1 Cells are of equal size; no fragmentation
seen
Grade 2 Cells are of equal size; minor fragmentation only
Grade 2.5 Cells are mostly of equal size; moderate fragmentation
Grade 3 Cells are of unequal size; no fragmentation to moderate fragmentation
Grade 4 Cells are of equal or unequal size; fragmentation is moderate to heavy

Blastocyst Grading
• Are graded 1 - 4 according to degree of expansion (and 5-6 degree of hatching)
• Blastocysts of grades 3 or higher are further graded A-C for Inner Cell Mass (ICM) and Trophectoderm
A - Tightly packed, many cellsB - Loosely packed, severalC - Very few cells

Blastocyst Stage Embryos: Day 5
.

BASIC IMPLANTATION PHYSIOLOGY


Embryo-Endometrium Communication
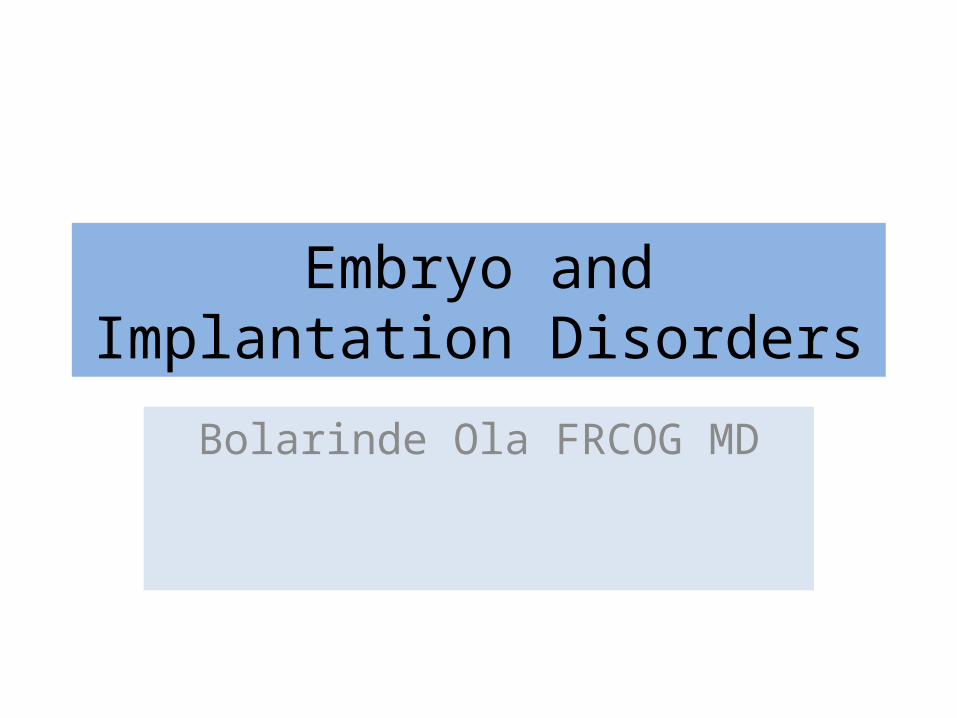
• Day 5 - Free floating blastocyst in utero • Day 6 - Blastocyst hatching – Start of Window• Day 7 - Blastocyst apposition to endometrium at
the beginning of the implantation window • Day 8 - Blastocyst adhesion occurring when LIF is
maximally expressed by the endometrium and blastocyst expresses the LIF receptor
• Day 9 - Blastocyst Invasion• Day 10 - Implantation complete– End of
Window
IMPLANTATION WINDOW AND EMBRYO-MATERNAL CROSSTALK
Justine S. Fitzgerald et al. Hum. Reprod. Update 2008;14:335-344
Free floating blastocyst
Blastocyst hatching
Blastocyst apposition
Blastocyst adhesion
Blastocyst invasion
Implantation complete
START (implantation
window)
END (implantation
window)

• Differentiation of trophoblast cells into inner cyto-trophoblast and outer syncytiotrophoblast layers and invasion into the luminal epithelium, where the blastocyst then commences to secrete cytokines such as IL-1, which in turn stimulates LIF expression in the endometrium
• Implantation is complete,• Implantation window is closed
REPRODUCTIVE FAILURE
• Embryo– Sperm factors– Egg factors
• Endometrium• Uterine• Tubal• Endocrine• Immune• Others

EMBRYO QUALITY
• Poor Sperm– Unexplained– Iatrogenic (surgery, radiation etc)– Chromosomal / Genetic– Congenital / varicocoele
• Reduced Ovarian reserve– Age– Iatrogenic– Chromosomal / Genetic– Congenital
ENDOMETRIUM
• Unexplained• Poor endometrial development• Infections• Polyps• Submucous fibroids• Congenital (Uterine Septa)

UTERINE / TUBAL
Uterine• Fibroids• Adenomyosis• Mullerian dysgenesis
Tubal• Hydrosalpinges

ENDOCRINE
• Hypothyroid• Hyperthyroid• Diabetes Mellitus• Polycystic Ovary Syndrome• Premature ovarian failure

IMMUNE DISORDERS
• Autoimmune thyroid disorders• Auto-immune gonadal diseases• Abnormal endometrial cytokines– Elevated NK cells in endometrium
• Antiphospholipid Syndrome - APS

IMPLANTATION
• Implantation is the series of stages including blastocyst hatching, adhesion, endometrial invasion, embryo differentiation and growth to produce a state of clinical pregnancy
• Measurable over a period by implantation rate:– Number of embryo implanted out of number transferred
over a period– i.e. total number of gestation sacs on scan divided by
total number of embryo transferred

FAILED IMPLANTATION
• Failure to reach a stage in which there is ultrasonographic evidence of intra uterine pregnancy (intra-uterine gestational sac)
IMPLANTATION FAILURE
Failure to achieve a clinical pregnancy • following the transfer of at least four embryos• at least 3 transfer cycles, fresh or frozen • in which embryos were good quality • in women aged <40 years

OUTCOMES OF IVF
• Ongoing clinical pregnancy• Cycle cancellation• Failed fertilisation• Failed implantation• Miscarriage• Ectopic pregnancy
• Implantation failure (repeated)

INVESTIGATIONS OF IMPLANTATION FAILURE
RECOMMENDED INVESTIGATIONS TESTS OF RESEARCH VALUE
• Ovarian reserve tests: FSH, AMH, antral follicle count
• Sperm DNA fragmentation
• Parental karyotype (?aneuploidies) • Natural Killer Cells
• Hereditable/acquired thrombophilia
• Pelvic imaging (TVS/TAS)
• Hysterosalpingography
• Hysteroscopy
• Laparoscopy
Improving the Embryo

IMPROVING EMBRYO QUALITY:GENERAL MEASURES
• Encourage couples to try early• Good diet• Reduce / Cigarette smoking• Reduce alcohol• Weight control
IMPROVING EMBRYO QUALITY, SPECIFIC MEASURES
• Sperm DNA fragmentation tests• Ovarian stimulation protocol• Gamete donation (for parental aneuploidies)• Insemination by ICSI• Careful embryo selection - embryoscope• Blastocyst transfer• Assisted hatching• Improved embryo transfer techniques

Improving the Endometrium

THROMBOPHILIA & IMMUNE DISORDERS
Antiphospholipid syndrome (APS)• A systemic autoimmune disease characterized by
vascular thrombosis and/or pregnancy morbidity in the persistent presence of antiphospholipid antibodies (aPL).
• aPL are currently evaluated by three tests – Abs against beta-2 glycoprotein I (anti-β2GPI abs) – Abs against cardiolipin (aCL), – Lupus anticoagulant (LA)

aPL cause defective placentation by interacting with both sides of the placenta. • At the decidual level, aPL is proinflammatory
with neutrophil infiltration, secretion of cytokines and complement activation
• At trophoblast level, aPL down-regulate hCG,
integrins and cadherins resulting in reduced trophoblast proliferation and growth
THROMBOPHILIA & IMMUNE DISORDERS

THROMBOPHILIA AND IMPLANTATION FAILURE
• APS is strongly linked to recurrent miscarriages (RCMs)
• Treatment of APS improves RCMs
• APS is NOT associated with implantation failure (IF)
• Treatment of APS does not usually improve IF

THYROID AUTOIMMUNITY
• Described as the presence of autoantibodies against thyroid peroxidase (TPO) and/or thyroglobulin (TG)
• Associated with repeated implantation failure (RIF)
• Treatment is Thyroxine supplements

NATURAL KILLER CELLS
• Natural killer (NK) cells are subpopulation of lymphocyte in peripheral blood
• Similar immune cells which are poor killers (uNK) populate the uterine lining at implantation – The functions of these uterine NK (uNK) cells are
essentially unknown – May have a role in regulating placentation and
trophoblast cell invasion

NATURAL KILLER CELLS
• Increasingly, clinicians are testing for uNK– No agreed range of normality
• An increasing number of treatments available– None conclusively proven to be beneficial

PERSISTENT ENDOMETRIAL FLUID

CAUSES OFFLUID WITHIN ENDOMETRIUM
• Ovarian stimulation (uterine or cervical)• High dose Estrogen• Low Estrogen• Tubal - Hydrosalpinges• Endometrial– Polyp or fibroid– Asherman’s synechia– Cervical stenosis– Chronic infection
• Others

POORLY DEVELOPED ENDOMETRIUM

POORLY DEVELOPED ENDOMETRIUM
• Poor ovarian reserve or POF• Iatrogenic (medical, radiation• Endometrial– Asherman’s synechia– Chronic infection
• Uterine fibroids• Adenomyosis• Others
THE ROLE OF DIAGNOSTIC HYSTEROSCOPY
Courtesies RCOG London StratOG

MANAGING IMPLANTATION FAILURE:Levels of evidence
Level 1+ : high quality meta-analyses of RCTs or RCT with a low risk of bias
Level 1- : meta analyses or RCTs or RCT with a high risk of bias
Level 2 : systematic review of case-control or well conducted case control cohort studies or cohort studies Level 3: case reports or case series
Level 4: expert opinion

LIVE BIRTH RATE PER CYCLE FOR ROUTINE HYSTEROSCOPY VERSUS NO
HYSTEROSCOPY PRIOR TO IVF/ICSI
Pundir & El Toukhi Reproductive BioMedicine Online 28, 2, 2014, 151–161
Level 2++ Evidence
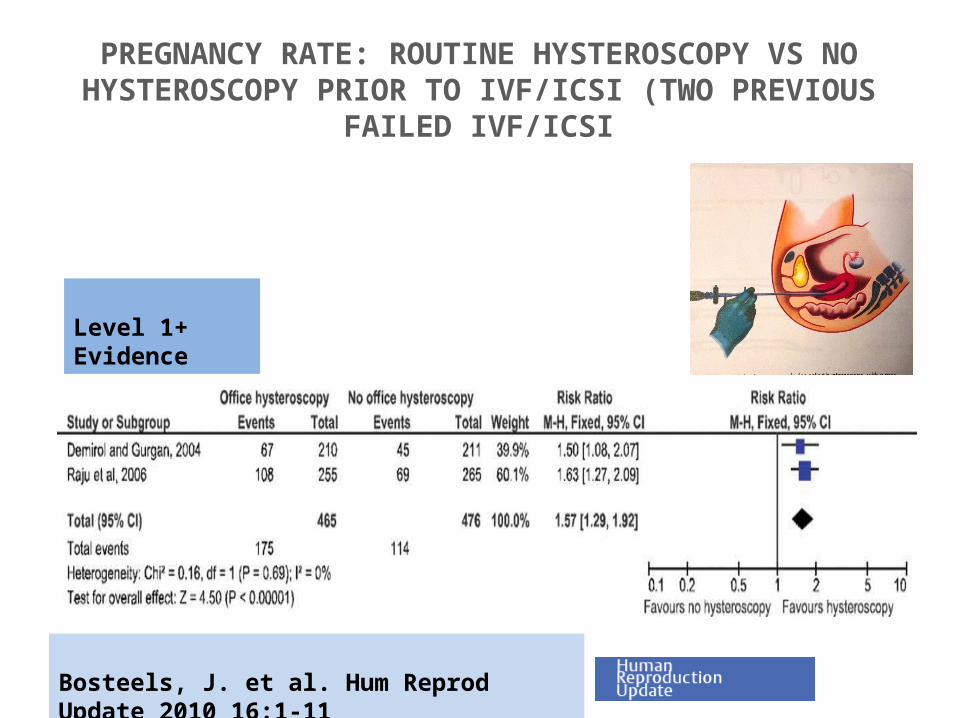
PREGNANCY RATE: ROUTINE HYSTEROSCOPY VS NO HYSTEROSCOPY PRIOR TO IVF/ICSI (TWO PREVIOUS
FAILED IVF/ICSI
Bosteels, J. et al. Hum Reprod Update 2010 16:1-11
Level 1+ Evidence
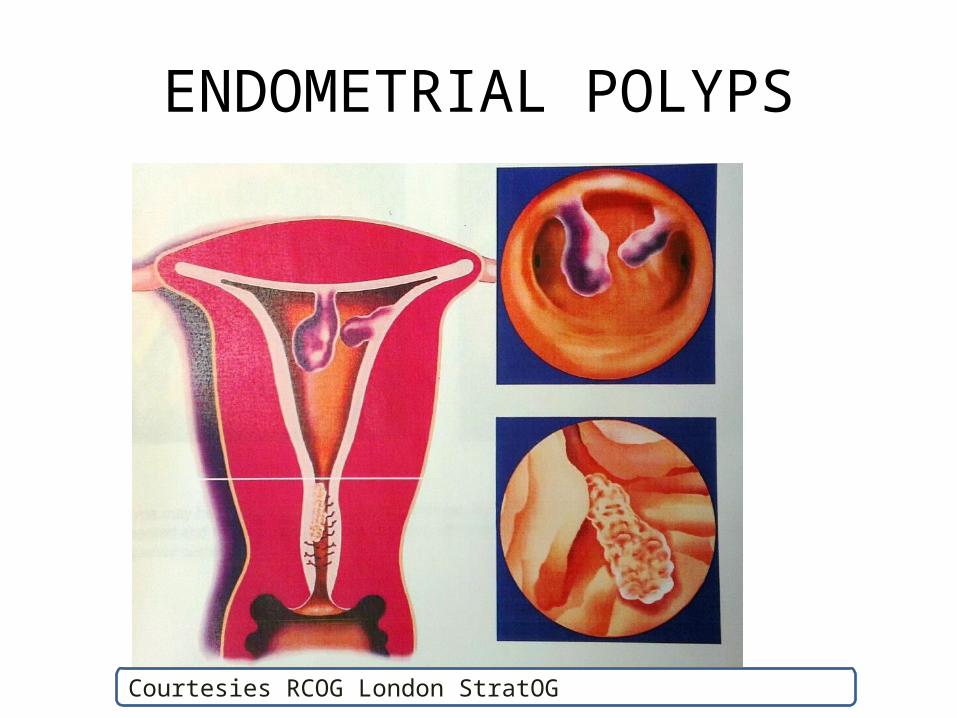
ENDOMETRIAL POLYPS
Courtesies RCOG London StratOG

HYSTEROSCOPIC POLYPECTOMY VS DIAGNOSTIC HYSTEROSCOPY + BIOPSY
ONLY PRIOR TO IUI: CLINICAL PREGNANCY
Level 1+ Evidence
Bosteels J, Cochrane Database of Systematic Reviews 2013, Issue 1.
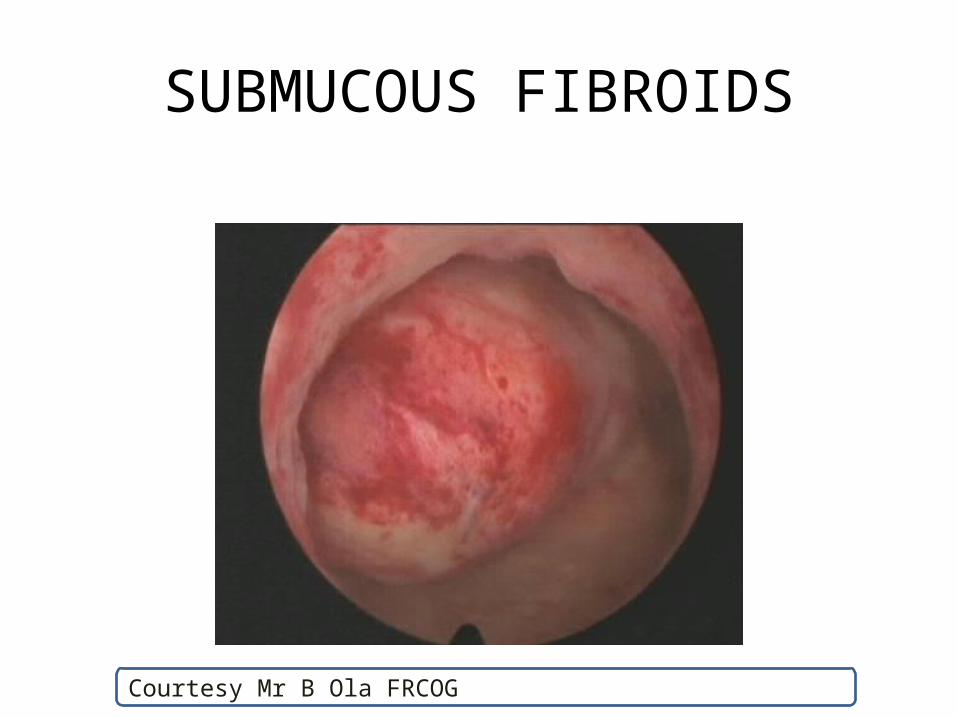
SUBMUCOUS FIBROIDS
Courtesy Mr B Ola FRCOG

HYSTEROSCOPIC MYOMECTOMY VS SEXUAL INTERCOURSE ONLY: CLINICAL PREGNANCY
Bosteels J, Cochrane Database of Systematic Reviews 2015, Issue 1.
Level 1- Evidence
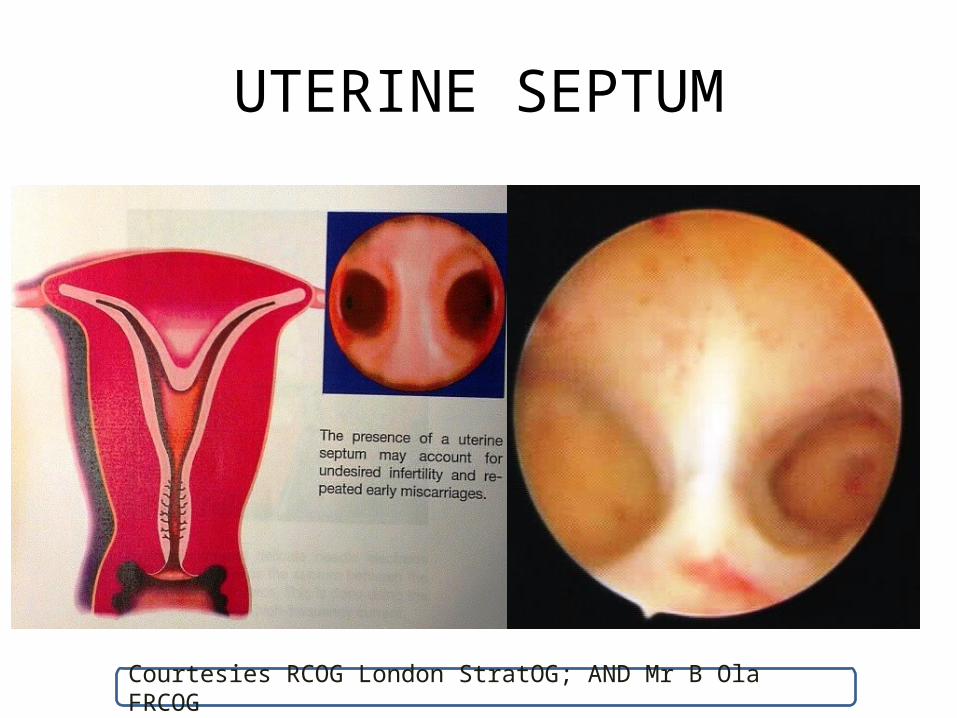
UTERINE SEPTUM
Courtesies RCOG London StratOG; AND Mr B Ola FRCOG
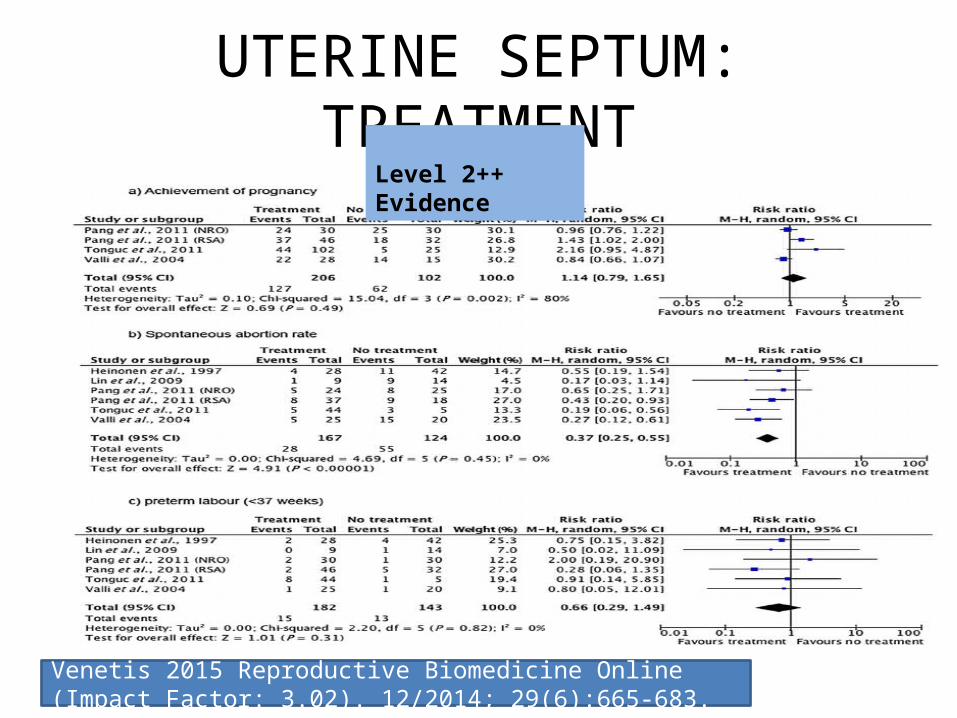
UTERINE SEPTUM: TREATMENTLevel 2++ Evidence
Venetis 2015 Reproductive Biomedicine Online (Impact Factor: 3.02). 12/2014; 29(6):665-683.

UTERINE SYNECHIA
Courtesies RCOG London StratOG

HYSTEROSCOPIC SURGERY FOR ASHERMAN SYNECHIA:
Pregnancy and Live Birth Rates
Total Pregnant Live Births
43 51% 33%
A. Dawood, A. Al-Talib, T. Tulandi (2010). Obstet. Gynaecol. Can., 32 pp. 767–770
Evidence Level 2-

INTRAMURAL FIBROIDS
http://www.medicinenet.com/uterine_fibroids/article.htmhttp://www.advancedfertility.com/myomfoto.htm

EFFECT OF FIBROIDSLevel 2- Evidence

EFFECT OF MYOMECTOMY
Metwally M, Farquhar C, Li TC Cochrane Database of Systematic Reviews 2015, Issue 1.
Level 1- Evidence

ADENOMYOSIS
http://www.sir.net.au/adenomyosis

ADENOMYOSIS AND IVF CLINICAL PREGNANCY RATES
Level 2 Evidence
iVercellini P, et al. Uterine adenomyosis and in vitro fertilization outcome: a systematic review and meta-analysis. Human Reproduction. 2014 Mar 12:deu041.y

ADENOMYOSIS AND IVF MISCARRIAGESLevel 2 Evidence
iVercellini P, et al. Uterine adenomyosis and in vitro fertilization outcome: a systematic review and meta-analysis. Human Reproduction. 2014 Mar 12:deu041.y

ADENOMYOSIS AND IVF SHORT OR LONG PROTOCOL
Level 2 Evidence
iVercellini P, et al. Uterine adenomyosis and in vitro fertilization outcome: a systematic review and meta-analysis. Human Reproduction. 2014 Mar 12:deu041.y

HYDROSALPINGES AND TREATMENTS
Courtesy Mr B. Ola FRCOG

HYDROSALPINGES AND IVF
Salpingectomy prior to IVF in women with hydrosalingesimproves pregnancy, implantation and live birth ratesEvidence Level 1
Strandell et al 1999 Hydrosalpinx and IVF outcome : a prospective randomized multicentre trial in Scandinavia on salpingectomy prior to IVF Human Reprod 14:2762
Level 1+ Evidence
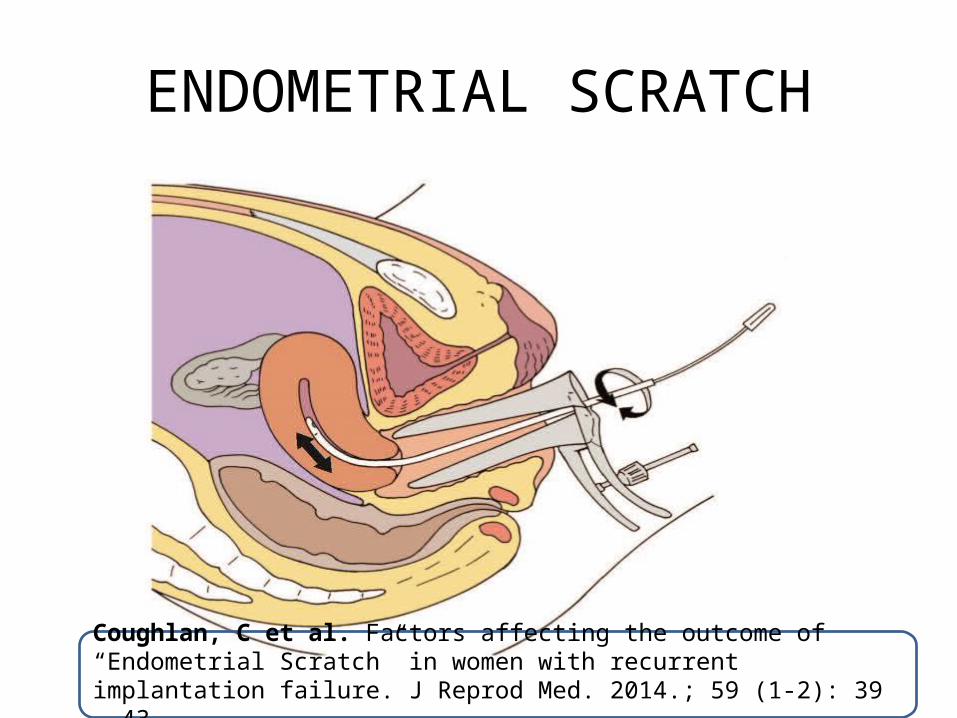
ENDOMETRIAL SCRATCH
Coughlan, C et al. Factors affecting the outcome of “Endometrial Scratch” in women with recurrent implantation failure. J Reprod Med. 2014.; 59 (1-2): 39 – 43

ENDOMETRIAL INJURY AND IMPLANTATION FAILURE
Carolina O Nastri Endometrial injury in women undergoing assisted reproductive techniques Cochrane Database of Systematic Reviews 2015, Issue 3

CONCLUSIONS
• Research is continuously active in the areas of embryo quality and implantation disorders
• There is still a big gap in knowledge
• Currently research is focussing on the roles of MicroRNAs in the regulation of cross-talk between embryo and endometrium