Embed Size (px)
Citation preview
M.R.SHOJAM.R.SHOJA 11
GOOD MORNING &GOOD MORNING & CONGRATULATION CONGRATULATION

M.R.SHOJAM.R.SHOJA 22
M.R. SHOJAM.R. SHOJAProfessor Of Professor Of Ophthalmology Ophthalmology
M.R.SHOJAM.R.SHOJA 33
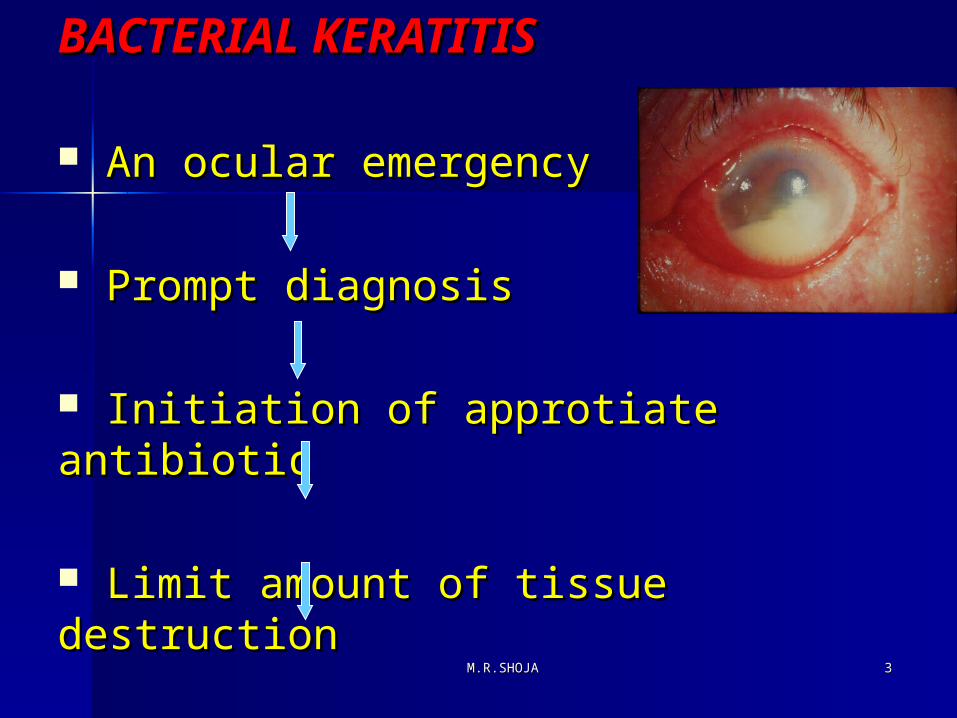
BACTERIAL KERATITISBACTERIAL KERATITIS
An ocular emergencyAn ocular emergency
Prompt diagnosisPrompt diagnosis
Initiation of approtiate antibioticInitiation of approtiate antibiotic
Limit amount of tissue destructionLimit amount of tissue destruction
Improve patient,s visual prognosisImprove patient,s visual prognosis
M.R.SHOJAM.R.SHOJA 44
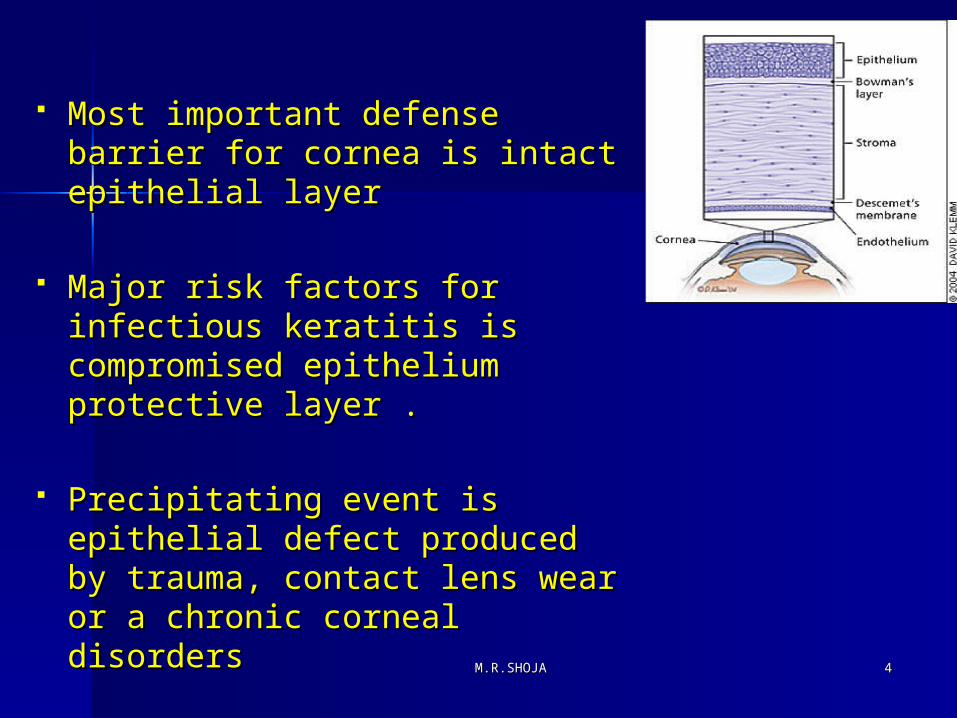
Most important defense Most important defense barrier for cornea is intact barrier for cornea is intact epithelial layerepithelial layer
Major risk factors for infectious Major risk factors for infectious keratitis is compromised keratitis is compromised epithelium protective layer .epithelium protective layer .
Precipitating event is epithelial Precipitating event is epithelial defect produced by trauma, defect produced by trauma, contact lens wear or a chronic contact lens wear or a chronic corneal disorderscorneal disorders
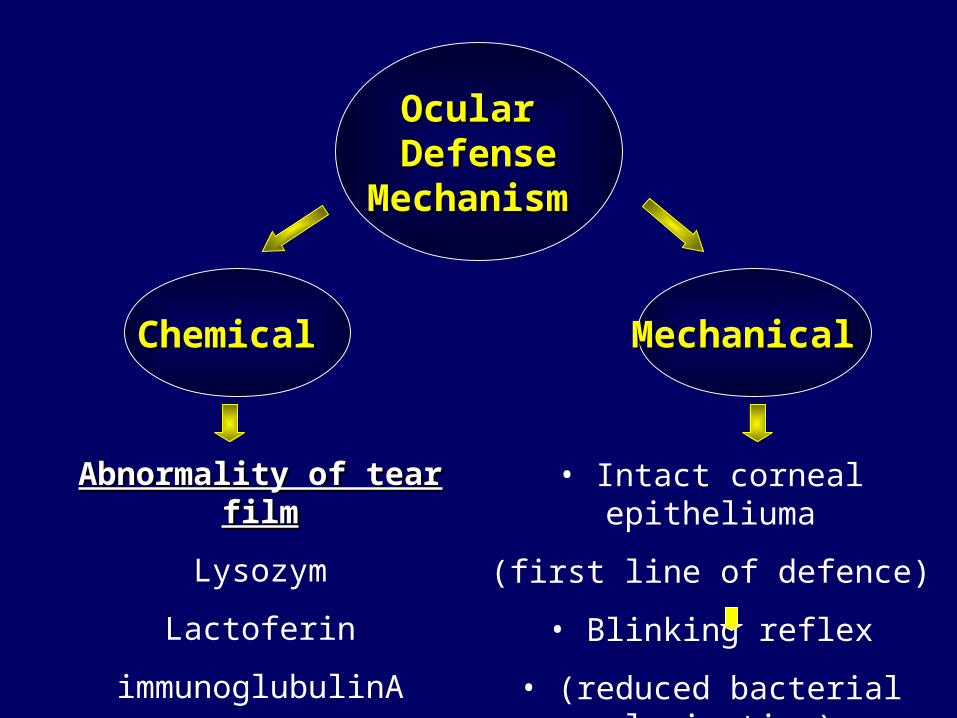
Ocular Ocular DefenseDefense
Mechanism Mechanism
Chemical Chemical Mechanical Mechanical
Abnormality of tear filmAbnormality of tear film
Lysozym
Lactoferin
immunoglubulinA
Mucin deficiency
• Intact corneal epitheliuma
(first line of defence)
• Blinking reflex
• (reduced bacterial colonization)
M.R.SHOJAM.R.SHOJA 66
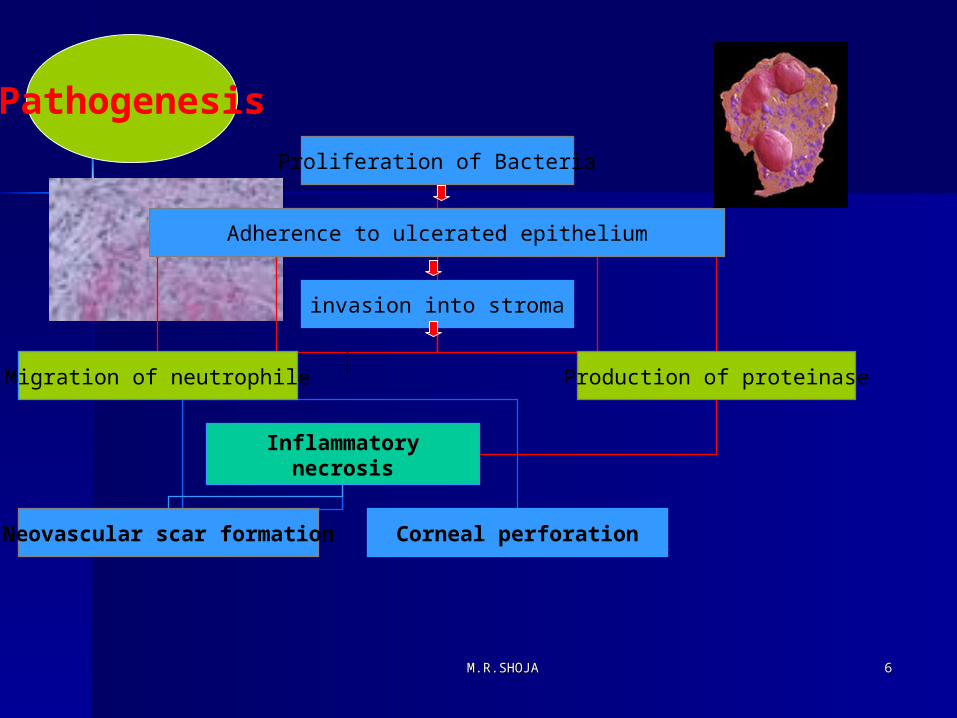
Pathogenesis
Proliferation of Bacteria
Adherence to ulcerated epithelium
invasion into stroma
Migration of neutrophile Production of proteinase
Inflammatorynecrosis
Neovascular scar formation Corneal perforation
M.R.SHOJAM.R.SHOJA 77
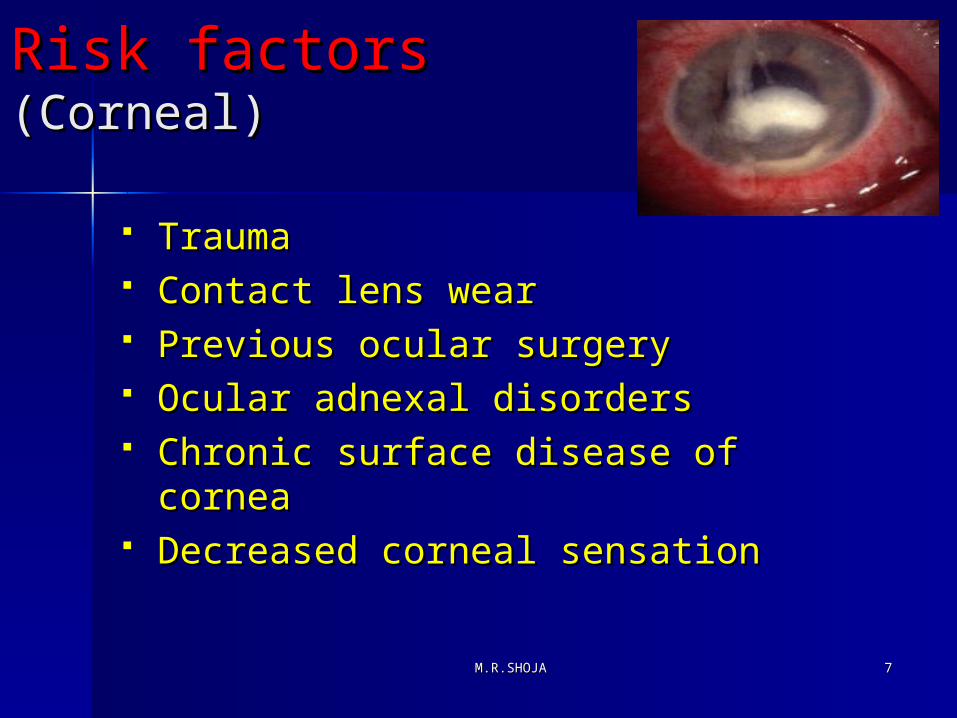
RiskRisk factorsfactors (Corneal)(Corneal)
TraumaTrauma Contact lens wearContact lens wear Previous ocular surgeryPrevious ocular surgery Ocular adnexal disordersOcular adnexal disorders Chronic surface disease of Chronic surface disease of
corneacornea Decreased corneal sensation Decreased corneal sensation
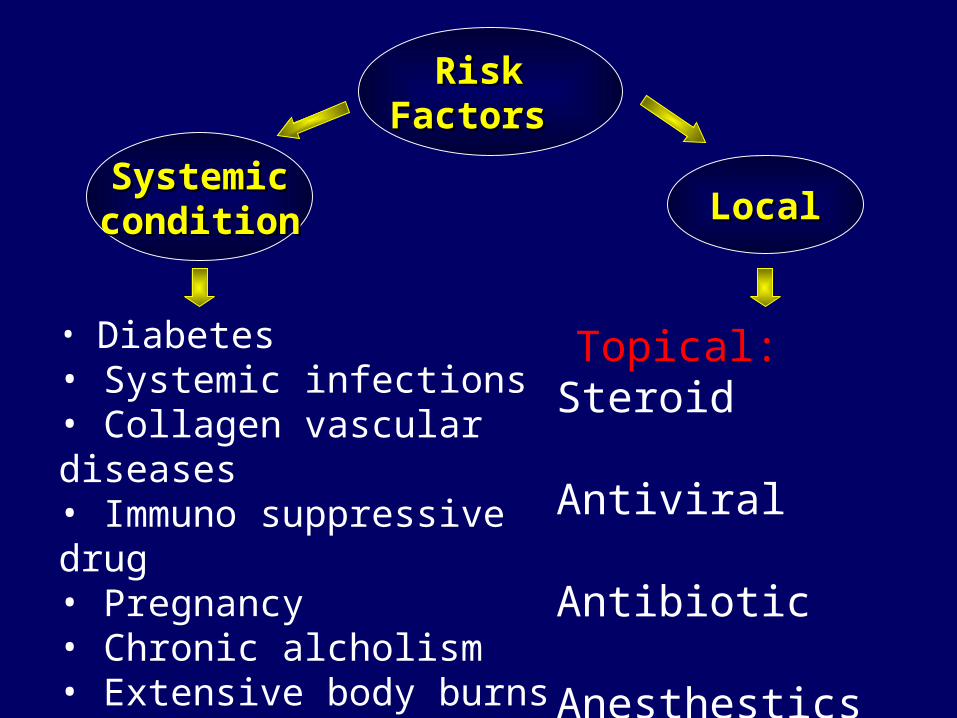
Risk Risk Factors Factors
SystemicSystemicconditioncondition LocalLocal
• Diabetes• Systemic infections• Collagen vascular diseases• Immuno suppressive drug• Pregnancy• Chronic alcholism• Extensive body burns• Drug addiction• AIDS
Topical: Steroid Antiviral
Antibiotic Anesthestics
M.R.SHOJAM.R.SHOJA 99
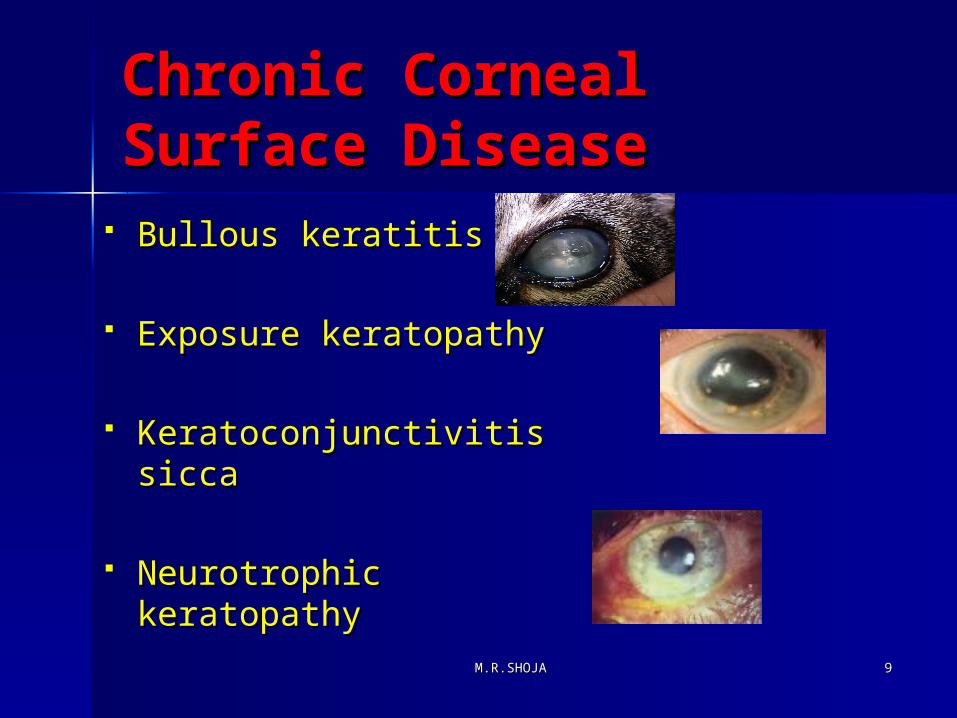
Chronic Corneal Chronic Corneal Surface Disease Surface Disease
Bullous keratitisBullous keratitis
Exposure keratopathyExposure keratopathy
Keratoconjunctivitis siccaKeratoconjunctivitis sicca
Neurotrophic keratopathy Neurotrophic keratopathy
M.R.SHOJAM.R.SHOJA 1010
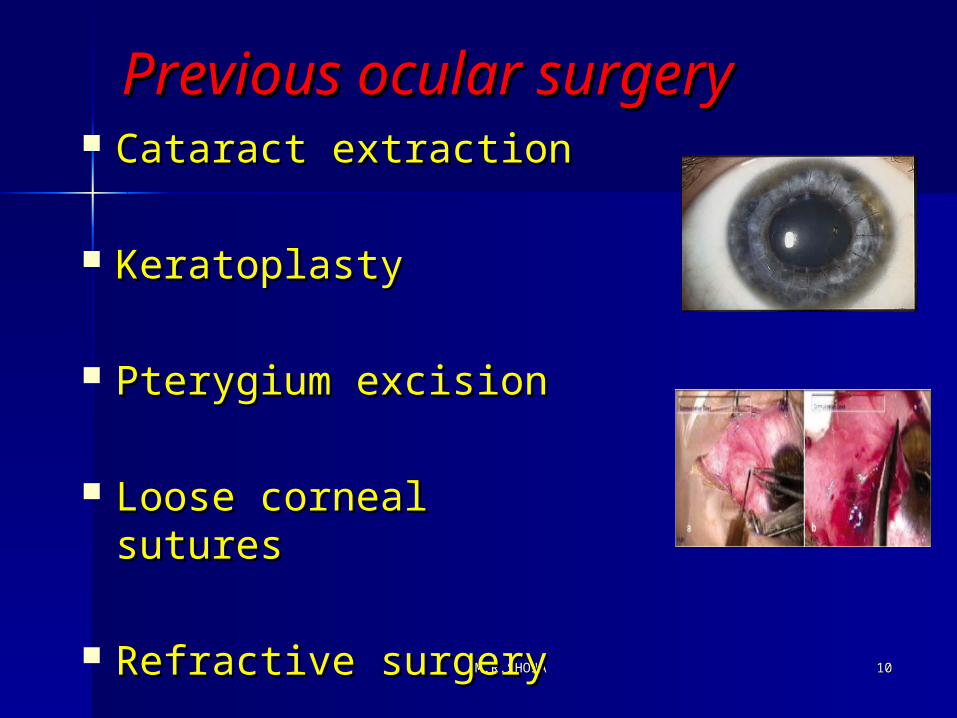
Previous ocular surgeryPrevious ocular surgery Cataract extractionCataract extraction
KeratoplastyKeratoplasty
Pterygium excisionPterygium excision
Loose corneal suturesLoose corneal sutures
Refractive surgeryRefractive surgery
M.R.SHOJAM.R.SHOJA 1111
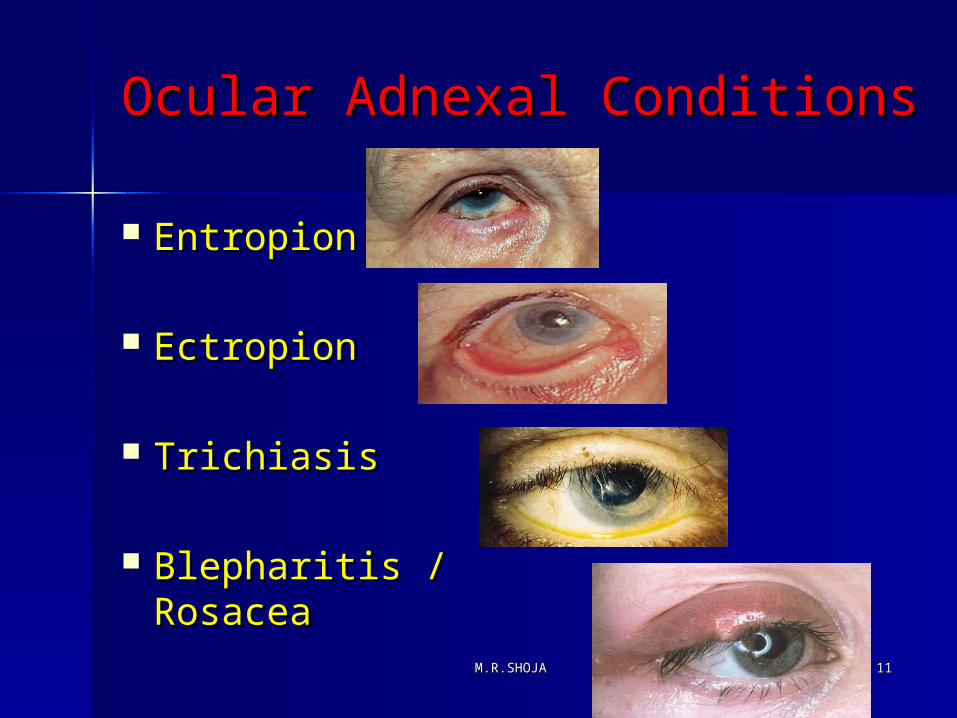
Ocular Adnexal ConditionsOcular Adnexal Conditions
EntropionEntropion
EctropionEctropion
TrichiasisTrichiasis
Blepharitis / Blepharitis / RosaceaRosacea
M.R.SHOJAM.R.SHOJA 1212
Normal flora of ocular surfaceNormal flora of ocular surface GRAM POSITIVE:GRAM POSITIVE: Staphylococcus Aureus (more common)Staphylococcus Aureus (more common) Staphylococcus Epidermidis (more common)Staphylococcus Epidermidis (more common) Propionibacterium acnes.Propionibacterium acnes. Streptococcus ViridansStreptococcus Viridans GRAM NEGATIVEGRAM NEGATIVE (less common) (less common) Escheria ColiEscheria Coli KlebsiellaKlebsiella ProteusProteus MoraxellaMoraxella
M.R.SHOJAM.R.SHOJA 1313
Causes of Bacterial keratitis Causes of Bacterial keratitis (87%)(87%)
Staphylococcus aureus Staphylococcus aureus
Staphylococcus epidermidisStaphylococcus epidermidis
Streptococcus pneumonieaStreptococcus pneumoniea
Pseudomonas aeruginosa Pseudomonas aeruginosa
Most common organism in soft contact Most common organism in soft contact lenslens
Enterobacteriaceae Enterobacteriaceae (proteus, (proteus, enterobacter)enterobacter)
M.R.SHOJAM.R.SHOJA 1414
Now yorkNow york LondonLondon
S.aureus S.aureus S.aureusS.aureus Pseudomonas Moraxella Pseudomonas Moraxella S.pneumonia S.pneumonia PseudomonasPseudomonas
ETIOLOGY
M.R.SHOJAM.R.SHOJA 1515
OrOrgganismsanisms penetrate intact penetrate intact epitheliumepithelium
Neisseria gonorroae Neisseria gonorroae
Haemophilus agegyptius Haemophilus agegyptius
Corynebacterium diphteria Corynebacterium diphteria
Listeria Listeria

M.R.SHOJAM.R.SHOJA 1616
Clinical presentationClinical presentation
Rapid onset of painRapid onset of pain Conjunctival injection (Conjunctival injection (RednessRedness)) PhotophobiaPhotophobia Decreased visionDecreased vision Discharge and lid edemaDischarge and lid edema
M.R.SHOJAM.R.SHOJA 1717
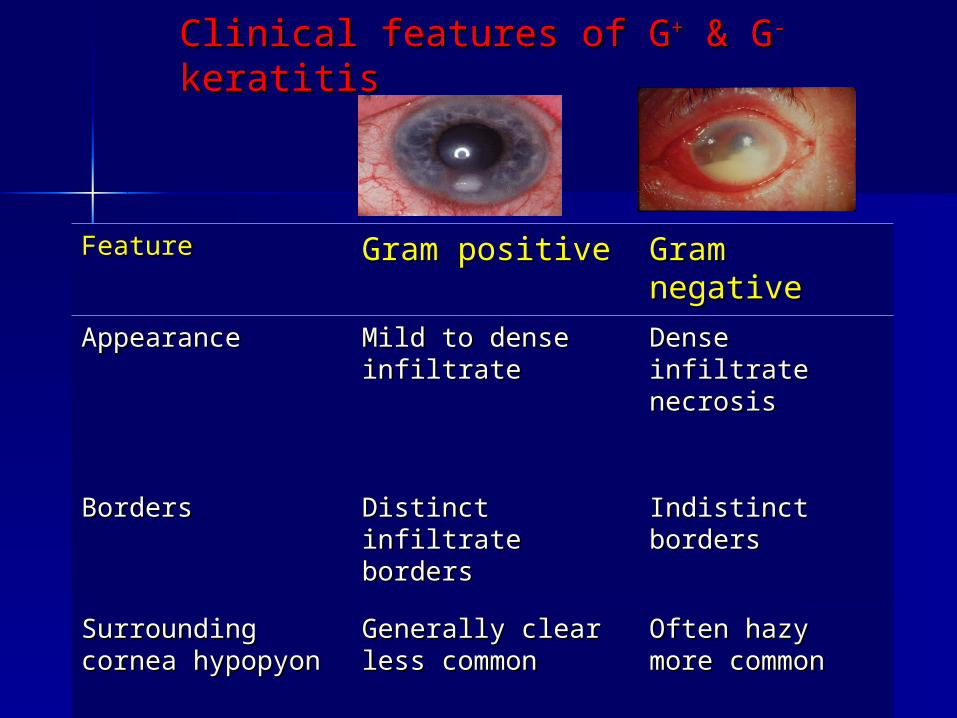
Clinical features of GClinical features of G++ & G & G-- keratitis keratitis
Feature Feature Gram positiveGram positive Gram Gram negativenegative
AppearanceAppearance Mild to dense Mild to dense infiltrateinfiltrate
Dense infiltrate Dense infiltrate necrosisnecrosis
BordersBorders Distinct infiltrate Distinct infiltrate bordersborders
Indistinct bordersIndistinct borders
Surrounding Surrounding cornea hypopyon cornea hypopyon
Generally clear less Generally clear less commoncommon
Often hazy more Often hazy more commoncommon
M.R.SHOJAM.R.SHOJA 1818
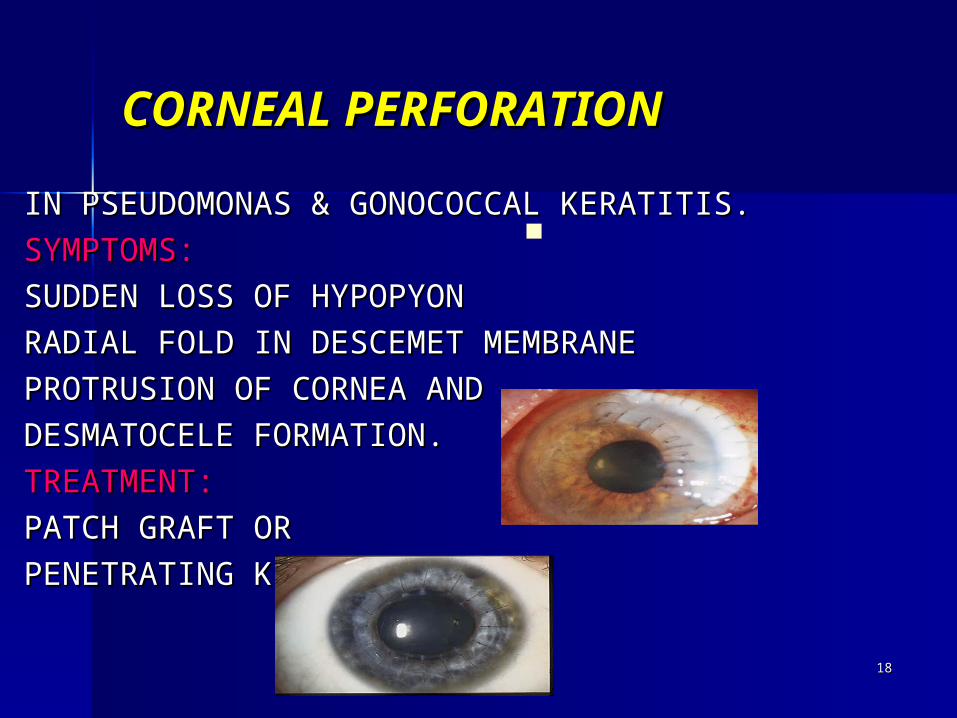
CORNEAL PERFORATIONCORNEAL PERFORATION
IN PSEUDOMONAS & GONOCOCCAL KERATITIS.IN PSEUDOMONAS & GONOCOCCAL KERATITIS.
SYMPTOMS:SYMPTOMS:
SUDDEN LOSS OF HYPOPYONSUDDEN LOSS OF HYPOPYON
RADIAL FOLD IN DESCEMET MEMBRANERADIAL FOLD IN DESCEMET MEMBRANE
PROTRUSION OF CORNEA AND PROTRUSION OF CORNEA AND
DESMATOCELE FORMATION.DESMATOCELE FORMATION.
TREATMENT:TREATMENT:
PATCH GRAFT OR PATCH GRAFT OR
PENETRATING K.PENETRATING K.
M.R.SHOJAM.R.SHOJA 1919
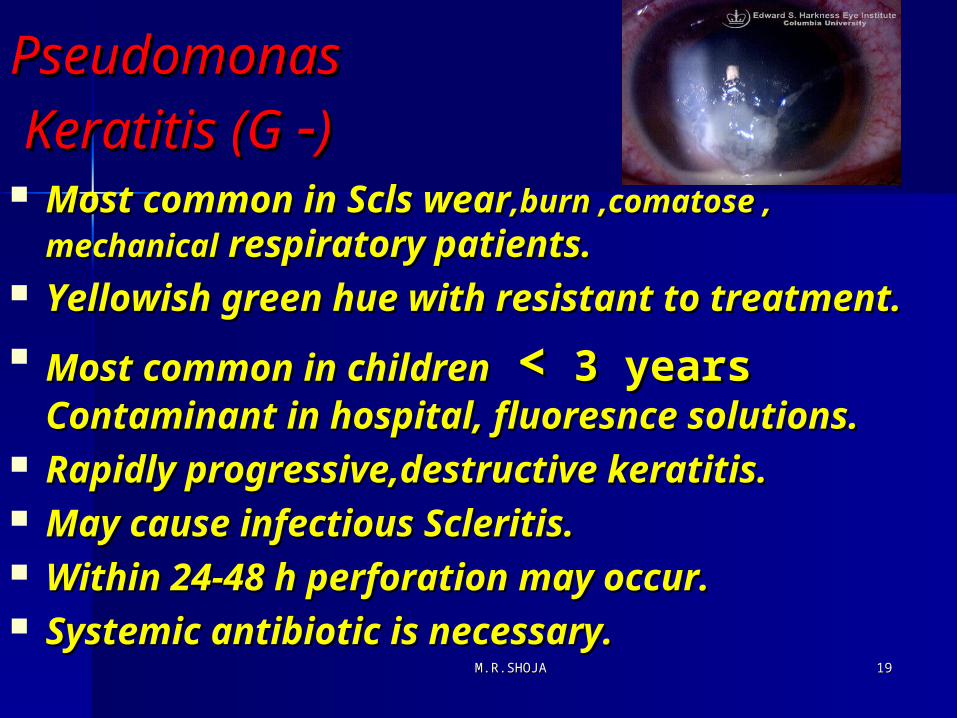
PseudomonasPseudomonas Keratitis (G Keratitis (G --)) Most common in Scls wearMost common in Scls wear,burn ,comatose , ,burn ,comatose ,
mechanicalmechanical respiratory patients. respiratory patients. Yellowish green hue with resistant to Yellowish green hue with resistant to
treatment.treatment.
Most common in childrenMost common in children << 3 years 3 years Contaminant in hospital, fluoresnce Contaminant in hospital, fluoresnce solutions.solutions.
Rapidly progressive,destructive keratitis.Rapidly progressive,destructive keratitis. May cause infectious Scleritis.May cause infectious Scleritis. Within 24-48 h perforation may occur.Within 24-48 h perforation may occur. Systemic antibiotic is necessary.Systemic antibiotic is necessary.
M.R.SHOJAM.R.SHOJA 2020
Gonococci KeratitisGonococci Keratitis
Hyperacute conjunctivitis , preauricular Hyperacute conjunctivitis , preauricular adenopathyadenopathy
PPenetrate intact epithelium ,produce rapid enetrate intact epithelium ,produce rapid corneal ulceration and perforation as 24 to corneal ulceration and perforation as 24 to 48 hours after infection.48 hours after infection.
Choice of treatment is 1 g ceftriaxone IM or Choice of treatment is 1 g ceftriaxone IM or IV for 3 to 5 days for keratitis.IV for 3 to 5 days for keratitis.
Frequent irrigation is necessary.Frequent irrigation is necessary. Sexual partners should be evaluated.Sexual partners should be evaluated. In all hyperacute conjunctivitis the entire In all hyperacute conjunctivitis the entire
cornea must be evaluated for ulcerationcornea must be evaluated for ulceration

M.R.SHOJAM.R.SHOJA 2121
Gonococci CGonococci Conjunctivitisonjunctivitis & &
KeratitisKeratitis
M.R.SHOJAM.R.SHOJA 2222
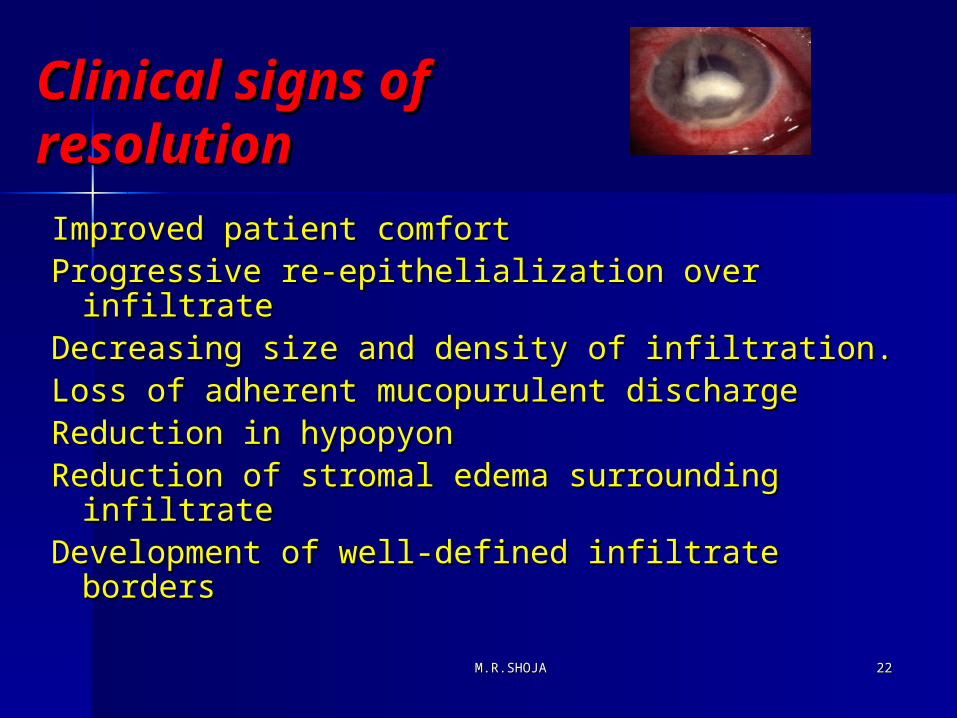
Clinical signs of Clinical signs of resolutionresolution
Improved patient comfortImproved patient comfortProgressive re-epithelialization over infiltrate Progressive re-epithelialization over infiltrate Decreasing size and density of infiltration.Decreasing size and density of infiltration.Loss of adherent mucopurulent dischargeLoss of adherent mucopurulent dischargeReduction in hypopyon Reduction in hypopyon Reduction of stromal edema surrounding Reduction of stromal edema surrounding
infiltrateinfiltrateDevelopment of well-defined infiltrate Development of well-defined infiltrate
bordersborders

M.R.SHOJAM.R.SHOJA 2323
Stain or culture media Stain or culture media
StainsStains Gram stainGram stain Giemsa stainGiemsa stain Calcofluor white stainCalcofluor white stain Acid fast stainAcid fast stain
Culture mediaCulture media Blood agarBlood agar Sabourauds agarSabourauds agar Chocolate agarChocolate agar Thioglycolate brothThioglycolate broth
M.R.SHOJAM.R.SHOJA 2424
Goals of therapyGoals of therapy Rapid elimination of bacteriaRapid elimination of bacteria Reduction of inflammatory Reduction of inflammatory responseresponse Prevent of structural damagePrevent of structural damage Promotion healing of epithelial Promotion healing of epithelial
M.R.SHOJAM.R.SHOJA 2525
Treatment
Hospitalization
Systemic Antibiotic Corneal Graft
Fortified combined drops
Monotherapy Fluroquinolone
Drug penetartion in to cornea increased with higher concentration and frequent application
M.R.SHOJAM.R.SHOJA 2626
Treatment Treatment ((ImpricalImprical))
Loading dose : 5 application every 2 Loading dose : 5 application every 2 MinMin
Frequent instillation every 30 MinFrequent instillation every 30 Min
Fortified cephalosporin (Fortified cephalosporin (50mg/dl) +50mg/dl) +
gentamycin or tobramycin (gentamycin or tobramycin (15mg/ml)15mg/ml)
Modification of initial AB is based on Modification of initial AB is based on culture results and clinical responseculture results and clinical response
For (G +) Vancomycin is alternativeFor (G +) Vancomycin is alternative
For (G-) Ceftazidime or AmikacineFor (G-) Ceftazidime or Amikacine
M.R.SHOJAM.R.SHOJA 2727
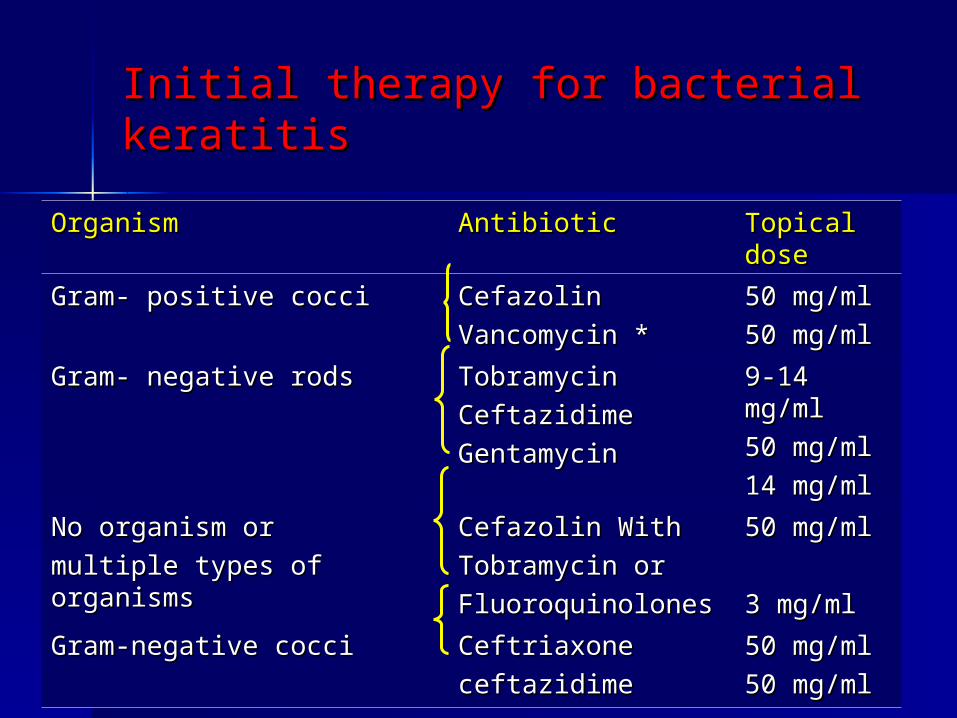
Initial therapy for bacterial keratitisInitial therapy for bacterial keratitis
OrganismOrganism Antibiotic Antibiotic Topical Topical dose dose
Gram- positive cocciGram- positive cocci CefazolinCefazolin
Vancomycin *Vancomycin *50 mg/ml50 mg/ml
50 mg/ml50 mg/ml
Gram- negative rodsGram- negative rods TobramycinTobramycin
Ceftazidime Ceftazidime
Gentamycin Gentamycin
9-14 9-14 mg/mlmg/ml
50 mg/ml50 mg/ml
14 mg/ml14 mg/ml
No organism or No organism or
multiple types of organismsmultiple types of organismsCefazolin With Cefazolin With
Tobramycin orTobramycin or
FluoroquinolonesFluoroquinolones
50 mg/ml50 mg/ml
3 mg/ml3 mg/ml
Gram-negative cocciGram-negative cocci Ceftriaxone Ceftriaxone
ceftazidimeceftazidime50 mg/ml50 mg/ml
50 mg/ml50 mg/ml
M.R.SHOJAM.R.SHOJA 2828
AntibioticsAntibiotics The choice of antibiotics is standard The choice of antibiotics is standard
topical, commercially unavailable, topical, commercially unavailable, fortified aminoglycoside and fortified fortified aminoglycoside and fortified cephalosporin drops (ie gentamicin 1.5% cephalosporin drops (ie gentamicin 1.5% and cefuroxime 5%) or the new regime and cefuroxime 5%) or the new regime of fluoroquinolone monotherapy with of fluoroquinolone monotherapy with commercially available ciprofloxacin or commercially available ciprofloxacin or ofloxacin 0.3%.ofloxacin 0.3%.
Currently both the standard and Currently both the standard and fluoroquinolone regimen encounter fluoroquinolone regimen encounter bacterial resistance in about 5% of casesbacterial resistance in about 5% of cases
M.R.SHOJAM.R.SHOJA 2929
TreatmentTreatment
Subconjunctival injectionSubconjunctival injection for for impending corneal perforationimpending corneal perforation
Hydrophilic soft contact lensHydrophilic soft contact lens ParenteralParenteral 1-Impending perforation1-Impending perforation 2-Perforated infection2-Perforated infection 3-Scleral involvement3-Scleral involvement
M.R.SHOJAM.R.SHOJA 3030
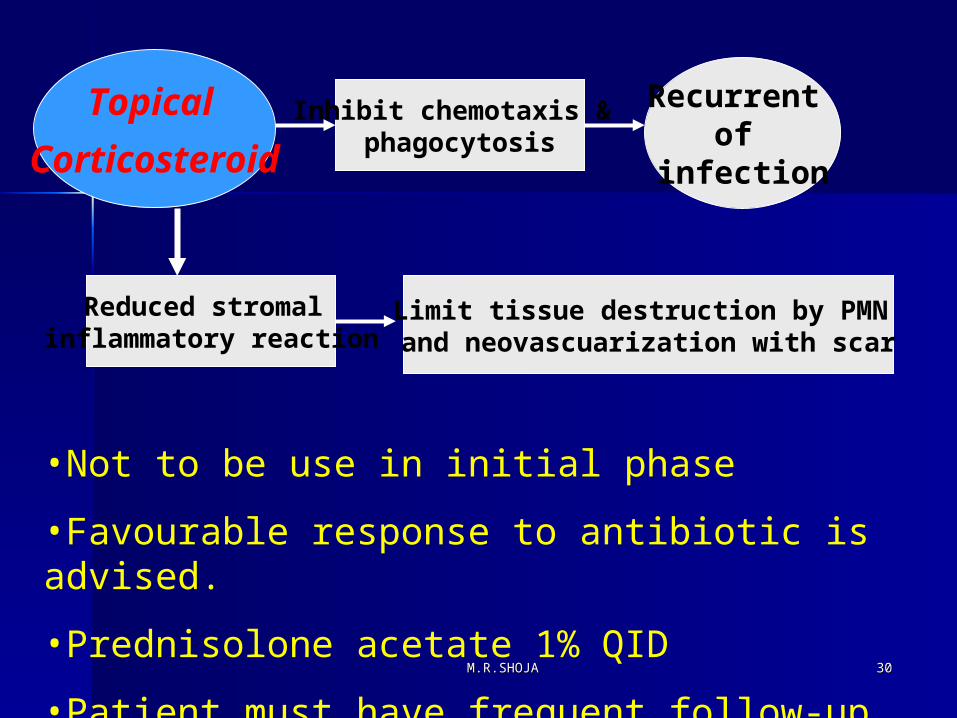
•Not to be use in initial phase
•Favourable response to antibiotic is advised.
•Prednisolone acetate 1% QID
•Patient must have frequent follow-up
Topical
Corticosteroid
Inhibit chemotaxis & phagocytosis
Recurrent of
infection
Reduced stromal inflammatory reaction
Limit tissue destruction by PMN and neovascuarization with scar
M.R.SHOJAM.R.SHOJA 3131
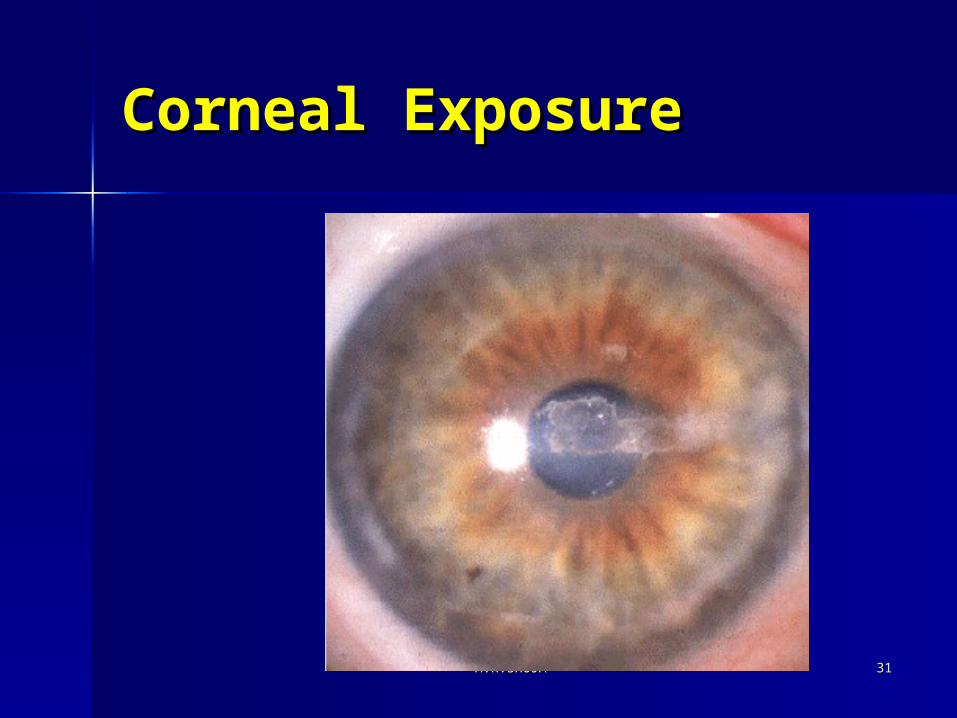
Corneal ExposureCorneal Exposure
M.R.SHOJAM.R.SHOJA 3232
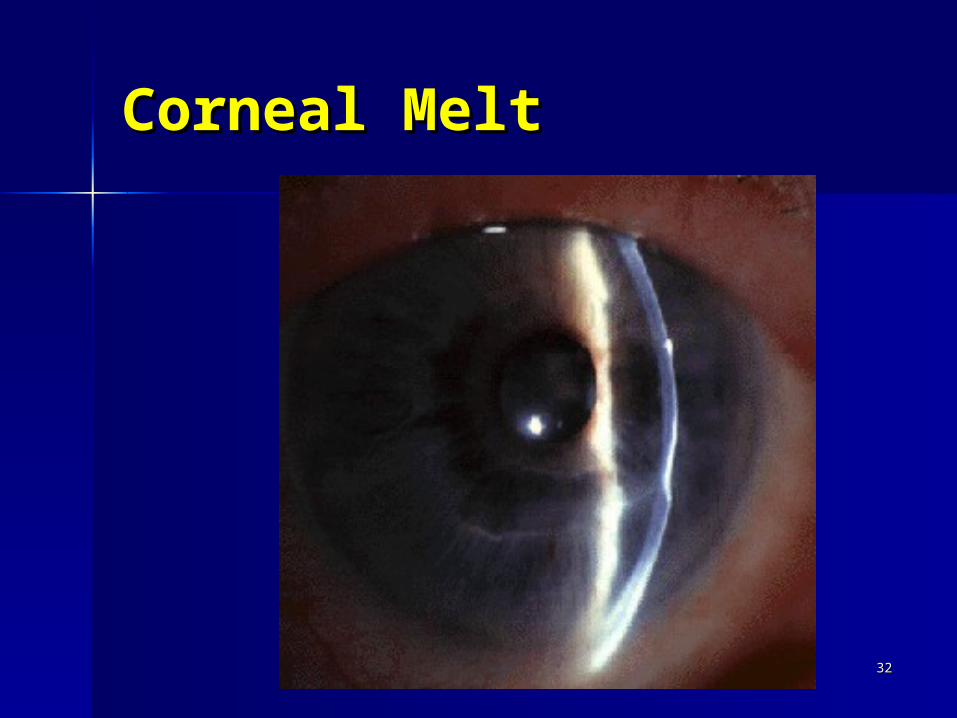
Corneal MeltCorneal Melt

M.R.SHOJAM.R.SHOJA 3333
Corneal UlcerCorneal Ulcer
M.R.SHOJAM.R.SHOJA 3434
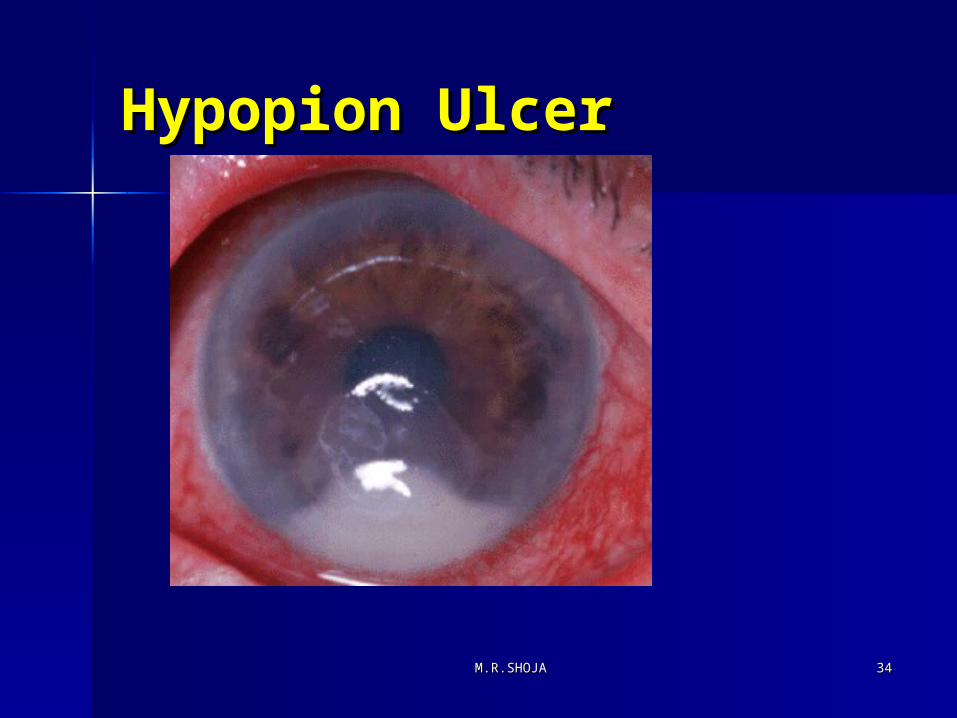
Hypopion UlcerHypopion Ulcer
Fungal KeratitisFungal Keratitis
Fungal keratitis is challenging corneal Fungal keratitis is challenging corneal disease and presents as very difficult form disease and presents as very difficult form bacterial keratitis. Difficulty arise in making bacterial keratitis. Difficulty arise in making correct clinical and laboratory diagnosis. The correct clinical and laboratory diagnosis. The treatment of fungal keratitis is also difficult treatment of fungal keratitis is also difficult due to poor availability of antifungal drugs due to poor availability of antifungal drugs and delay in starting treatment. and delay in starting treatment.
Treatment is required on long term basis, Treatment is required on long term basis, intensively and often cases require intensively and often cases require therapeutic keratoplasty. therapeutic keratoplasty.
3535M.R.SHOJAM.R.SHOJA
Fungal KeratitisFungal Keratitis
Fungi enter into corneal stroma through Fungi enter into corneal stroma through epithelial defect, which may be due to epithelial defect, which may be due to trauma, contact lens wear, bad ocular trauma, contact lens wear, bad ocular surface or previous corneal surgery.surface or previous corneal surgery.
In stroma fungi multiply and causes tissue In stroma fungi multiply and causes tissue necrosis and inflammatory reaction.necrosis and inflammatory reaction.
Organisms enter deep into the stroma and Organisms enter deep into the stroma and through an intact Descemets membrane through an intact Descemets membrane into the anterior chamber and iris. They into the anterior chamber and iris. They can also involve Sclera. can also involve Sclera.
3636M.R.SHOJAM.R.SHOJA
Risk FactorsRisk Factors
1.1. Trauma outdoor/ or the one which Trauma outdoor/ or the one which involves plant matter (including contact involves plant matter (including contact lenses)lenses)
2.2. Topical medications:Topical medications:
3.3. corticosteroids, corticosteroids,
4.4. anaesthetic drug abuse anaesthetic drug abuse
5.5. topical broad spectrum antibiotics use topical broad spectrum antibiotics use for long timefor long time
3737M.R.SHOJAM.R.SHOJA
Risk FactorsRisk Factors
6. Systemic use of steroids 6. Systemic use of steroids
7. Corneal surgeries (Penetrating keratoplasty, 7. Corneal surgeries (Penetrating keratoplasty, refractive surgery)refractive surgery)
8. Chronic keratitis (herpes simplex, herpes 8. Chronic keratitis (herpes simplex, herpes zoster, Vernal or allergic keratoconjunctivitis, zoster, Vernal or allergic keratoconjunctivitis, and neurotrophic ulcer) and neurotrophic ulcer)
9. Diabetes , Chronically ill / hospitalised 9. Diabetes , Chronically ill / hospitalised patients, AIDS and leprosypatients, AIDS and leprosy
3838M.R.SHOJAM.R.SHOJA
Causative fungi Causative fungi
I.I. Yeast: Candida species (albicans), Yeast: Candida species (albicans), CryptococcusCryptococcus
II.II. Filamentous septated Filamentous septated A. Non-pigmented hyphae: Fusarium A. Non-pigmented hyphae: Fusarium species (solani), Aspergillus species species (solani), Aspergillus species (fumigatus, flavus, niger)(fumigatus, flavus, niger)
3939M.R.SHOJAM.R.SHOJA
Causative fungiCausative fungi
III. Filamentous non-septated : III. Filamentous non-septated : Mucor and Rhizopus species Mucor and Rhizopus species
IV. Diphasic forms: Histoplasma, IV. Diphasic forms: Histoplasma, Coccidiodes, BlastomycesCoccidiodes, Blastomyces
4040M.R.SHOJAM.R.SHOJA
SymptomsSymptoms
Onset is slowOnset is slow Symptoms are less compared to Symptoms are less compared to
signssigns Diminution of vision, pain, foreign Diminution of vision, pain, foreign
body sensation body sensation
4141M.R.SHOJAM.R.SHOJA
SignsSigns
Diminution of vision, depending on Diminution of vision, depending on location of ulcerlocation of ulcer
Conjunctival and ciliary congestionConjunctival and ciliary congestion Epithelial defectEpithelial defect Stromal infiltratesStromal infiltrates Elevated areas, hypate (branching) Elevated areas, hypate (branching)
ulcers, irregular feathery marginsulcers, irregular feathery margins Dry and rough texture Dry and rough texture
4242M.R.SHOJAM.R.SHOJA
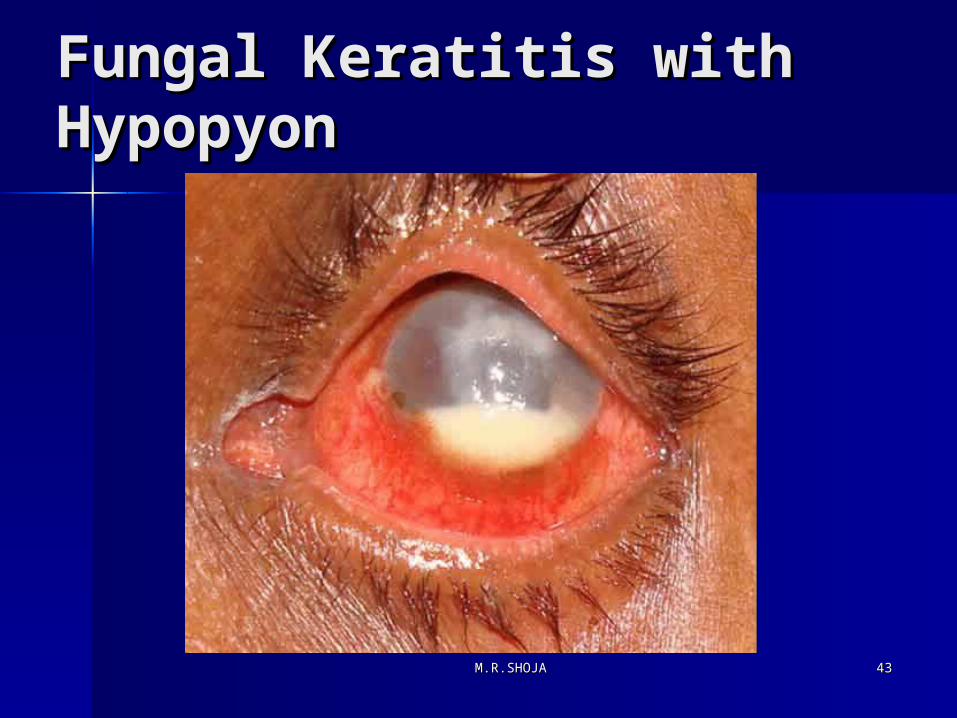
Fungal Keratitis with Fungal Keratitis with HypopyonHypopyon
4343M.R.SHOJAM.R.SHOJA
SignsSigns
Satellite lesionsSatellite lesions Brown pigmentation due to Brown pigmentation due to
dematiaceous fungus (Curvularia dematiaceous fungus (Curvularia lunata)lunata)
Intact epithelium with stromal Intact epithelium with stromal infiltratesinfiltrates
Anterior chamber reaction Anterior chamber reaction
4444M.R.SHOJAM.R.SHOJA

Fungal KeratitisFungal Keratitis
Fungal Keratitis – Pigmented Lesion
4545M.R.SHOJAM.R.SHOJA
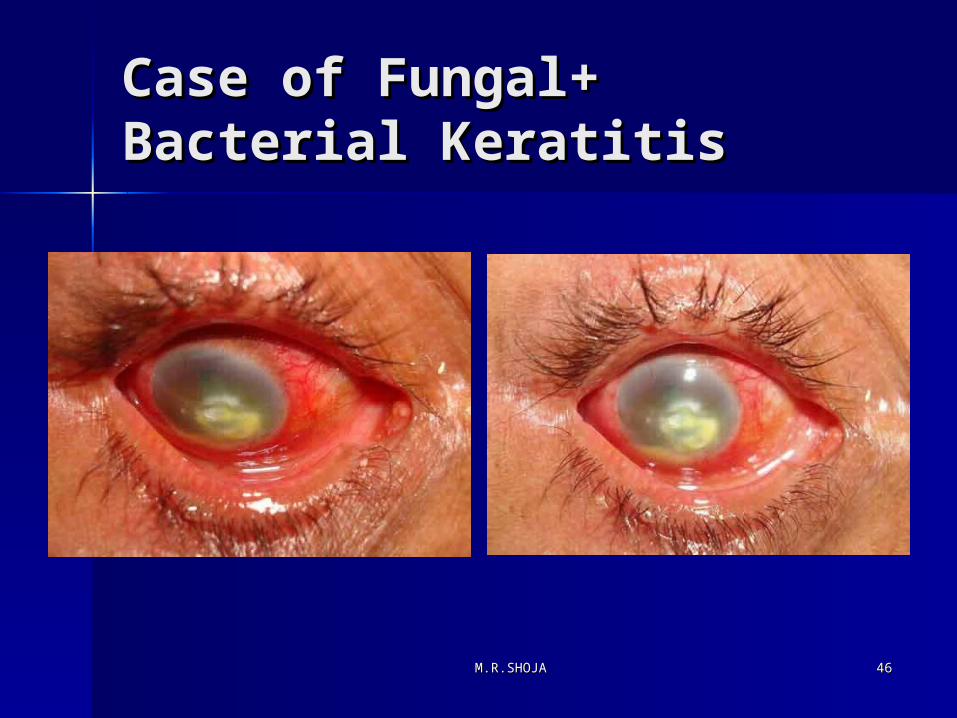
Case of Fungal+ Case of Fungal+ Bacterial KeratitisBacterial Keratitis
4646M.R.SHOJAM.R.SHOJA
Laboratory DiagnosisLaboratory Diagnosis
The Gram and Giemsa stains are used as The Gram and Giemsa stains are used as initial stains initial stains
Potassium Hydroxide (10-20 %) wet Potassium Hydroxide (10-20 %) wet mounts mounts
Culture Media: Sheep blood agar, Culture Media: Sheep blood agar, Chocolate agar, Sabouraud dextrose agar, Chocolate agar, Sabouraud dextrose agar, Thioglycollate broth Thioglycollate broth
Anterior chamber tap under aseptic Anterior chamber tap under aseptic conditions to aspirate hypopyon and or conditions to aspirate hypopyon and or endothelial plaqueendothelial plaque
4747M.R.SHOJAM.R.SHOJA
TreatmentTreatment
Natamycin 5% suspension: Natamycin 5% suspension: Candida species respond better to Candida species respond better to Amphotericin B 0.15%Amphotericin B 0.15%
Fluconazole 2%Fluconazole 2% Miconazole 1%Miconazole 1% Scrapping every 24 to 48 hours Scrapping every 24 to 48 hours Treatment is required for 4 – 6 Treatment is required for 4 – 6
weeks weeks
4848M.R.SHOJAM.R.SHOJA
TreatmentTreatment
Sub-conjunctival injection of Sub-conjunctival injection of Miconazole 5 – 10 mgm of 10 mgm/ml Miconazole 5 – 10 mgm of 10 mgm/ml suspension (indicated in severe form suspension (indicated in severe form of keratitis, scleritis and of keratitis, scleritis and endophthalmitis) endophthalmitis)
Systemic: Systemic:
Fluconazole or Ketoconazole is Fluconazole or Ketoconazole is indicated in severe form of keratitis, indicated in severe form of keratitis, scleritis and endophthalmitisscleritis and endophthalmitis
4949M.R.SHOJAM.R.SHOJA
Surgical TreatmentSurgical Treatment
1.1. Daily debridement with spatula/ blade every Daily debridement with spatula/ blade every 24 – 48 hours 24 – 48 hours
2.2. Surgical treatment is required in Surgical treatment is required in approximately 1/3approximately 1/3rdrd cases of fungal keratitis cases of fungal keratitis due to failure of medical treatment or due to failure of medical treatment or perforation perforation
3.3. Surgical treatment in the form of :Surgical treatment in the form of :therapeutic keratoplasty, conjunctival flap or therapeutic keratoplasty, conjunctival flap or lamellar keratoplasty lamellar keratoplasty
5050M.R.SHOJAM.R.SHOJA
Surgical TreatmentSurgical Treatment
Surgery is usually indicated within 4 Surgery is usually indicated within 4 weeks due to failure of medical weeks due to failure of medical treatment or recurrence of infection treatment or recurrence of infection
Unfavorable outcome is due to scleritis, Unfavorable outcome is due to scleritis, endophthalmitis and recurrence endophthalmitis and recurrence
Cryotherapy with topical antifungal Cryotherapy with topical antifungal treatment or corneoscleral graft in cases treatment or corneoscleral graft in cases of fungal scleritis and keratoscleritis of fungal scleritis and keratoscleritis
5151M.R.SHOJAM.R.SHOJA
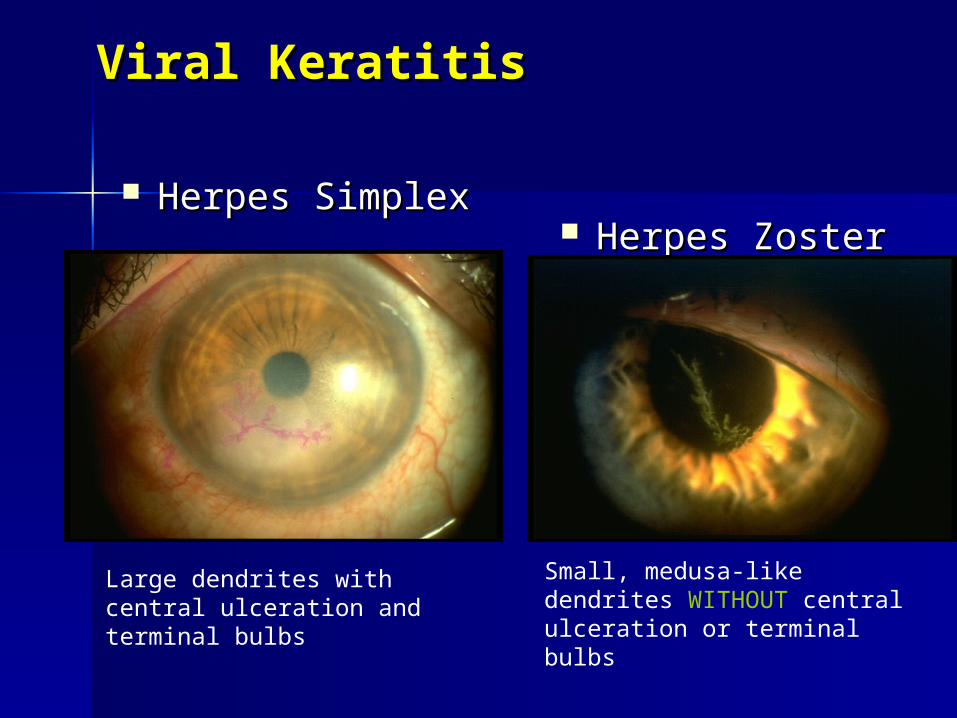
Viral KeratitisViral Keratitis
Herpes SimplexHerpes Simplex Herpes ZosterHerpes Zoster
Large dendrites with central ulceration and terminal bulbs
Small, medusa-like dendrites WITHOUT central ulceration or terminal bulbs
Herpes Simplex Keratitis:Herpes Simplex Keratitis:PathogenesisPathogenesis
HSV is a DNA virus that commonly HSV is a DNA virus that commonly infects humansinfects humans
Two distinct strains existTwo distinct strains exist– HSV-1: orofacial and ocularHSV-1: orofacial and ocular– HSV-2: orogenital STD, neonatalHSV-2: orogenital STD, neonatal
Recurrent HSV keratitis is one of the Recurrent HSV keratitis is one of the most frequent causes of infective most frequent causes of infective corneal blindness in the UScorneal blindness in the US

Herpes Simplex Keratitis:Herpes Simplex Keratitis:Primary Ocular InfectionPrimary Ocular Infection
Most commonly occurs on the Most commonly occurs on the mucocutaneous areas of the head mucocutaneous areas of the head innervated by CN Vinnervated by CN V
Manifests as a nonspecific URIManifests as a nonspecific URI May travel to the sensory ganglion and May travel to the sensory ganglion and
remain in a latent nonpathogenic stateremain in a latent nonpathogenic state
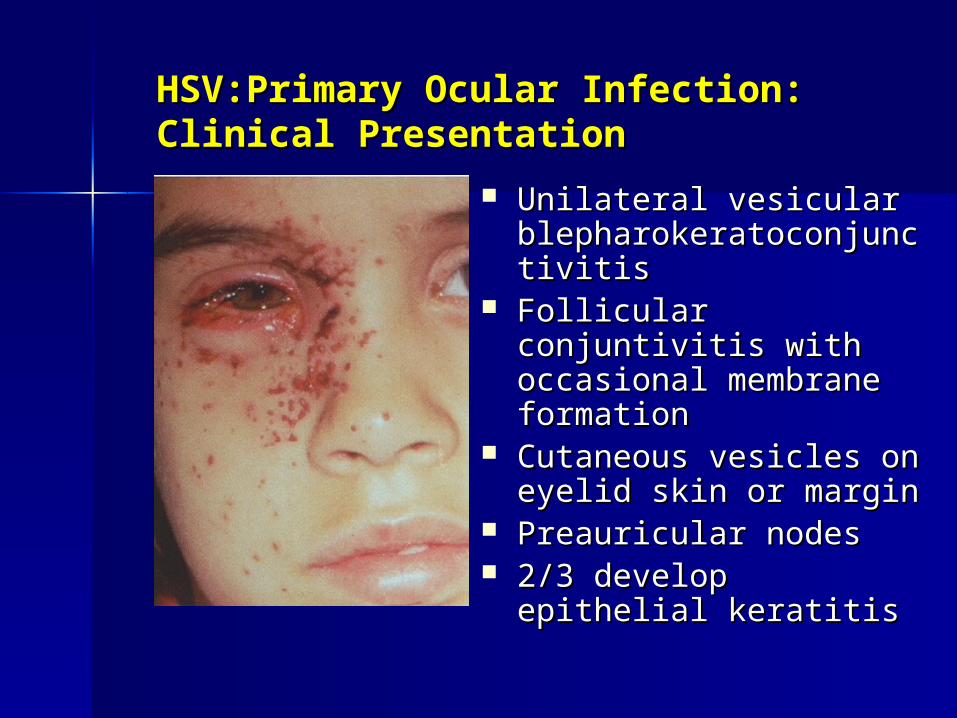
HSV:Primary Ocular Infection:HSV:Primary Ocular Infection:Clinical PresentationClinical Presentation
Unilateral vesicular Unilateral vesicular blepharokeratoconjunctivblepharokeratoconjunctivitisitis
Follicular conjuntivitis Follicular conjuntivitis with occasional with occasional membrane formationmembrane formation
Cutaneous vesicles on Cutaneous vesicles on eyelid skin or margineyelid skin or margin
Preauricular nodesPreauricular nodes 2/3 develop epithelial 2/3 develop epithelial
keratitiskeratitis
HSV: Primary Ocular InfectionHSV: Primary Ocular InfectionTreatmentTreatment
Self-limited conditionSelf-limited condition Topical antiviral therapyTopical antiviral therapy
– Trifluridine (Viroptic)Trifluridine (Viroptic)– Vidarabine Vidarabine
Oral antiviral therapy (one week)*Oral antiviral therapy (one week)*– Acyclovir 400mg 5x/dayAcyclovir 400mg 5x/day– Famcyclovir 500mg 3x/dayFamcyclovir 500mg 3x/day*may reduce recurrence rate*may reduce recurrence rate





























