Embed Size (px)
Citation preview

MRI of Congenital and Developmental Abnormalities of the KneeMiller, Angie, M.D., Hernandez, Andrea, M.D., Pena, Andres, M.D., Jaramillo, Diego, M.D., M.P.H.
Departments of Radiology, �e Children’s Hospital of Philadelphia, Philadelphia, PA 19104Congenital and developmental abnormalities of the knee are often initially identified on radiographs, but MRI can be utilized to
detect physeal, epiphyseal, meniscal, ligamentous, and patellar abnormalities not suspected radiographically.
The various congenital and developmental abnormalities of the knee are best understood within the context of its normal development. The epiphyseal ossification center of the distal femur is present at birth, while the proximal tibial epiphysis forms a secondary ossification center during the first to third postnatal months. The normal secondary ossification center of the distal femoral epiphysis during childhood can have rough or serrated margins. The patella is completely cartilaginous at birth. Primary patellar ossification begins at 5 to 6 years, although small foci may be evident at 2 to 3 years of age. The menisci obtain their characteristic shape before birth. Postnatally, the meniscal growth follows the distal femoral and proximal tibial enlargement, allowing for alteration in femorotibial contact and weight bearing with age. The cruciate ligaments blend into the epiphyseal cartilage of the distal femur and proximal tibia in early childhood. It is not until adolescence that the development of Sharpey’s fibers occurs and the ligaments insert directly into the maturing ossification centers.
The alignment of the knee varies during early childhood. Physiologic genu varum reaches a maximum degree at 6 months, and lasts until approximately 24 months. During the 3rd and 4th year, the knee becomes aligned in valgus, and the final alignment of slight genu valgus is reached at approximately 6 years of age.
PhysealBlount DiseaseBlount disease (Infantile tibia vara) is due to a local growth disturbance of the medial aspect of the proximal tibial epiphysis, with failure of endochondral ossification of the medial growth plate. It primarily involves the physis, but ultimately affects the epiphyseal cartilage, the menisci, the secondary ossification centers, and the adjacent metaphyses. More than half of cases are bilateral. It is considered by some to be related to stress on the medial compartment of the knee related to increased patient weight.
RicketsRickets is a disorder of childhood caused by a deficiency of or resistance to vitamin D or its derivative 1,25-dihydroxycholecalciferol. Abnormal endochondral ossification results, with an imaging appearance of widened and irregularly shaped physes, and flaring or cupping of the
metaphyses. There is widening of the physes of the secondary ossification centers, with delay in the appearance of these centers, and absence of the zone of provisional calcification.
EpiphysealTrevor’s DiseaseDysplasia Epiphysealis Hemimelica (Trevor’s disease) is characterized by localized overgrowth of an epiphysis of a long bone, most commonly occurring medially and within the distal tibial or distal femoral epiphyses, and the talus. The lesions may be single or multiple, and ossify with maturation. Premature closure of the physis with resultant deformity and occasional limb discrepancy may also be seen. Articular surface irregularity may lead to early secondary osteoarthritis.
Figure 5: Dysplasia Epiphysealis Hemimelica (Trevor’s disease), 1-year-old boy: AP and lateral view of the left knee (Fig.5A and B) demonstrates faint irregular ossification arising from the distal femoral condyle. Coronal T1 weighted (Fig.5C and D) and Sagittal T2 weighted (Fig.5E and F) images demonstrate overgrowth of the peripheral cartilage mass of the medial femoral epiphysis (arrow). Abnormal signal within the cartilage is suggestive of early ossification.
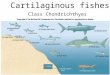
Congenitally Short FemurCongenitally short femur ranges from mild hypoplasia to complete absence of the femur. In childhood it is characterized by anterolateral bowing of the femur and medial cortical thickening. It results in an abnormality of the tibial and femoral condyles, which may be flattened. Unlike in proximal focal femoral deficiency, the hip joint is unaffected.
Figure 8: Congenitally short femur, 28 week gestational age girl:Echo planar images of the right (Fig.8A arrow) and left femur (Fig. 8 B arrow) demonstrate asymmetric femoral length, with the ossified segments of the right and left femora measuring 6.1 cm and 3.4 cm, respectively.
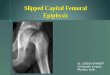
Proximal Focal Femoral Deficiency Proximal Focal Femoral Deficiency (PFFD) describes a spectrum of disorders ranging from hypoplasia to aplasia of the proximal femur. The acetabulum is dysplastic. At the knee, PFFD is associated with flattening of the distal femoral epiphysis and underdevelopment of the intercondylar notch. There is often absence of the cruciate ligaments.
Figure 9: PFFD, 6-year-old girl: Coronal proton density (Fig.9) image of the right hip demonstrates a hypoplastic acetabulum, fibrous connection between the femoral head and the shaft of the femur, and a small but spherical femoral head. The distal femur is also hypoplastic.
MeniscalDiscoid MeniscusDiscoid meniscus is a variant in which the meniscus is more disc-shaped than semicircular shaped, and in which a portion of the meniscus extends to the central portion of the tibial plateau. It occurs more frequently laterally than medially. The incidence of a lateral discoid meniscus is 1.5-3%, whereas that of a medial discoid meniscus is 0.1-0.3%. It is associated with an abnormal attachment of the posterior lateral meniscus to the tibial plateau. A discoid meniscus can be symptomatic, causing joint locking and joint line tenderness. The abnormal biomechanics of the discoid meniscus makes it prone to tearing.
PatellarNail Patella Syndrome
Nail patella syndrome is an autosomal dominant condition characterized by nail dysplasia, patellar aplasia-hypoplasia, arthrodysplasia of the elbows, posterior conical iliac horns, and nephropathy.
Conclusion: MRI is valuable in detecting and characterizing the physeal, epiphyseal, meniscal, ligamentous, and patellar abnormalities associated with congenital and developmental disorders of the knee.
References
Fig.1A Fig.1B Fig.1C Fig.1D
Figure 2: Bilateral Blount’s disease, 5-year-old girl Coronal proton density (Fig.2A and B) images in an older child demonstrate bilateral medial tibial physeal depression with associated bony bridging between the tibial epiphysis and metaphysis (arrow). There is associated widening of the lateral tibial physis. Tibia vara deformity is present with irregularity of the medial epiphyseal and metaphyseal bone. Sagittal proton density (Fig.2C) image demonstrates hypertrophy and increased signal within the medial meniscus, irregularity of the cortex of the posteromedial femoral condyle, and irregularity of the medial proximal tibial physis, through the area of bony bridging.
Figure 3: Rickets, 13-month-old girlSagittal STIR (Fig.3) image demonstrates widening of the distal femoral and proximal tibial physes as well as the physis of the secondary ossification center (arrow). A normal zone of provisional calcification is not visualized.
Figure 4: Rickets, 7-year-old boyCoronal T1 weighted (Fig.4A) image demonstrates loss of the zone of provisional calcification with medial tibial physeal bridging of uncertain etiology. Coronal 3D gradient-echo (Fig.4B and C), sagittal T1 weighted (Fig. 4D), and sagittal STIR (Fig. 4E) images demonstrate widening of the distal femoral and proximal tibial physes with abnormal intraphyseal signal. Pallisading longitudinal vertical hypodense areas within the physis are suggestive of mineralization along the metaphyseal side of the physis.
Fig.2A Fig.2B Fig.2C
Fig.3
Fig.4A Fig.4B Fig.4C Fig.4D Fig.4E
Fig.5A Fig.5B Fig.5C Fig.5D Fig.5E Fig.5F
Fig.6A Fig.6B Fig.7A
Fig.8A Fig.8B
Tibial hemimelia varies from mild hypoplasia to complete absence of the tibia and is associated with other abnormalities of the knee, including patellar and cruciate ligament deformities, absent menisci, and abnormal collateral ligaments.
Figure 6: Tibial hemimelia, newborn male: AP view (Fig. 6A) demonstrates complete tibial hemimelia and inward turning of the foot. Sagittal oblique T2-weighted image (Fig.6B) demonstrates a hypertrophied proximal fibular epiphysis that articulates with the distal femoral epiphysis. The patella is absent. (Image courtesy of Jaramillo D, Hoffer FA. Cartilaginous epiphysis and growth plate: normal and abnormal MR imaging findings. AJR Am J Roentgenol. 1992 May;158(5):1105-10)
Epiphyseal dysplasia is characterized by stippling of the epiphyses and abnormality of development of the secondary ossification centers. In the knee, there is less distinct shaping of the secondary ossification
centers with relative flattening of the distal femoral condylar contours.
Figure 7: Epiphyseal dysplasia, 10 year old girl: Sagittal T1 and T2 weighted images (Fig.7A and 7B) demonstrate abnormal flattening of the distal femoral condylar contours and irregularity of the developing secondary ossification center. There is diffusely abnormal signal within the developing cartilage
Epiphyseal Dysplasia
Fig.9
Fig.10A Fig.10D Fig.10EFig.10CFig.10B
Tibial Hemimelia
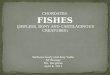
Figure 10: PFFD, 6-year-old boy: Lateral view (Fig.10A) of the femur demonstrates hypoplasia of the intertrochanteric portion of the right femur, with abnormal ossification. Coronal proton density image (Fig.10B) of the pelvis demonstrates a hypoplastic acetabulum without uncovering of the femoral head. Coronal proton density (Fig. 10C) and T1-weighted (Fig. 10D) images of the knee demonstrate lateral dislocation of the patella (Fig. 10D, arrow), and large medial and lateral discoid menisci with associated high signal consistent with degeneration. Sagittal proton density image (Fig.10E) demonstrates absence of the cruciate ligaments and rounding of the femoral and tibial epiphyses. There is absence of a well formed intercondylar notch.
Fig.11A Fig.11B Fig.11C
Fig.12A Fig.12B
Fig.13
Figure 12: Nail patella syndrome, 22-year-old girl: AP view of the pelvis (Fig. 12A) demonstrates flaring of the iliac wings bilaterally. The characteristic iliac horns are not present in this particular patient. Axial 3D gradient-echo (Fig.12B) and Axial T2 weighted images (Fig.12C) demonstrate a hypoplastic patella with thinning of the patellar articular cartilage, particularly of the medial facet, with areas of abnormal signal intensity consistent with chondromalacia. The patellar retinaculum is poorly developed.
Figure 13: Nail patella syndrome, infant girl: Axial gradient echo image of the left knee demonstrates hypoplasia of the patella, a shallow trochlea, and lateral patellar subluxation. (Courtesy of Dr. Tal Laor).
Bipartite patella occurs when the patella develops from two separate ossification centers, resulting in a main and accessory bone. The main and accessory bones are connected by fibrocartilaginous tissue. The findings are usually of no clinical significance.
Figure 14: Bipartite patella, 2-year-old boy: Coronal T1 weighted image (Fig.14A) in a young patient demonstrates a nonossified cartilaginous patella. Coronal T1 weighted fat saturated post-contrast image (Fig. 14B) demonstrates a separate cartilaginous component of the superolateral patella, not yet ossified.
Figure 11: Discoid meniscus, 9-year-old girl: Coronal proton density (Fig. 11A) and Sagittal T2 weighted images ( Fig.11B) demonstrate increased signal within a thickened lateral meniscus, with an intrameniscal cyst within its anteromedial portion (arrow). Sagittal proton density image (Fig 11C) demonstrates markedly irregular contour, thickening and increased signal within the lateral meniscus which also shows evidence of a meniscal flounce(arrow).
Congenital Dislocation of the PatellaCongenital dislocation of the patella represents a spectrum of developmental dysplasia of the patella and of the extensor mechanism. Flattening of the lateral femoral condyle occurs with an
increasing degree of genu valgum and external tibial rotation. The patella is hypoplastic and the intercondylar sulcus is shallow.
Figure 15: Congenital patellar dislocation, 1-year-old boy: Axial PD (Fig.15A) image demonstrates lateral dislocation of the patella and a shallow intercondylar notch. The lateral dislocation of the extensor mechanism is seen on the coronal PD (Fig.15B) image. Coronal 3D (Fig.15 C) reconstructed image further demonstrates the abnormal patellofemoral relationship.
Fig.12C
Bipartite Patella
GlobalVascular MalformationThe most common congenital vascular lesions of the knee are vascular malformations, resulting from abnormal vascular formation during embryonic life. The dilated blood vessels that build up these lesions gradually enlarge and can be classified based on their type of blood flow into slow-flow (capillary, venous, lymphatic) lesions, high-flow (arterial) lesions, and combined slow/fast-flow lesions Clinically, these patients are subject to repeated bouts of hemarthrosis if the lesion is located within a joint space.
Figure 16: Venous malformation, 3-year-old boy: Sagittal PD image (Fig.16A) demonstrates a multilobulated mass in Hoffa’s fat pad. It contains areas of low T2 signal intensity, consistent with phleboliths (arrow). (Fig. 16B) Sagittal contrast enhanced T1 weighted image (Fig.16C) demonstrates heterogeneous enhancement of the multilobulated mass which may be due to a lymphatic component or to delayed filling with contrast.
1. Craig JG, Holsbeeck M, Zaltz I (2002) The utility of MR in assessing Blount disease. Skeletal Radiology 31: 208-2132. Shapiro F. Pediatric orthopedic deformities: basic science, diagnosis, and treatment. Orlando (FL): Academic Press; 2002.3. Strouse PJ, Koujok K (2002) Magnetic Resonance imaging of the pediatric knee. Top Magn Reson Imaging 13(4): 277-944. John A. Ogden. Skeletal injury in the child, 3rd edition. Berlin: Springer Verlag, 2000.
5. Anton CG, Applegate KE, Kuivila TE, Wilkes DC (1999) Proximal femoral focal deficiency (PFFD): more than an abnormal hip. Semin Musculoskelet Radiol 3:215-2266. Laor T, Jaramillo D, Hoffer FA, Kasser JR (1996) MR imaging in congenital lower limb deformities. Pediatr Radiol 26:381-3877. Resnick D. Diagnosis of bone and joint disorders, 3rd edition. Philadelphia: WB Saunders, 1995: 3589.8. Jaramillo D, Hoffer FA (1992) Cartilaginous epiphysis and growth plate: normal and abnormal MR imaging findings. AJR Am J Roentgenol. May;158(5):1105-10
Fig.7B
Figure 1: Bilateral Blount disease, 2-year-old girlAP view of the knees (Fig.1A) demonstrates the initial radiographic changes of irregular metaphyseal ossification with a medial and distal pointing metaphyseal spur, irregular metaphyseal ossification along the medial tibial physis, fragmentation of the adjacent medial femoral epiphysis, and resultant tibia vara deformity. Coronal 3D
gradient-echo (Fig.1B and C) images demonstrate irregularity of metaphyseal ossification along the tibial physis, stippling of the secondary ossification centers, and overgrowth of the cartilage of the medial compartment of the knee. Sagittal 3D gradient-echo (Fig. 1D) image demonstrates stippling of the medial femoral epiphysis and hypertrophy of the medial meniscus.
Fig.14A Fig.14B
Fig.15A Fig.15B Fig.15C
Fig.16A Fig.16B Fig.16C