Embed Size (px)
Citation preview

SCIENTIFIC ARTICLE
MRI characteristics of lipoma and atypical lipomatoustumor/well-differentiated liposarcoma: retrospectivecomparison with histology and MDM2 gene amplification
Mélanie Brisson & Takeshi Kashima & David Delaney &
Roberto Tirabosco & Andrew Clarke & Suzie Cro &
Adrienne M. Flanagan & Paul O’Donnell
Received: 18 March 2012 /Revised: 28 July 2012 /Accepted: 27 August 2012 /Published online: 18 September 2012# ISS 2012
AbstractPurpose To review the reliability of MR imaging featuresfor the purpose of distinguishing lipoma and atypical lipo-matous tumor/well-differentiated liposarcoma (ALT/WDL).Materials and methods A retrospective review of 87 patientswith histologically proven lipomatous tumors was performed.All underwent MR imaging, assessing lipomatous content,septation, and nodules. The associations between these fea-tures and tumor diagnosis based on morphology and thepresence or absence of MDM2 amplification were explored.The age of the patient and the size and location of the lesionwere also recorded for statistical analysis.Results Of the 87 patients, 54 were classified as lipomas and33 as ALT/WDL. MR identified ALT/WDL with a sensitiv-ity of 90.9 % (CI 74.5–97.6) and a specificity of 37.0 % (CI
24.6–51.3). The positive and negative predictive valueswere 46.9 % (CI 34.5–59.7) and 86.9 % (CI 65.3–96.6),respectively. The mean age of patients with ALT/WDL wasgreater (60 years [range 40–83 years]) than those withlipoma (52 years [range 10–79 years]) (p00.025). The meansize of ALT/WDL (18.7 cm [range 5–36 cm]) was signifi-cantly greater than lipoma (13.9 cm [range 3–32 cm]) (p00.003). Features that increased the likelihood of ALT/WDLincluded: patient age over 60 years, maximal lesion dimen-sion over 10 cm, location in lower limb, and presence ofnon-fatty areas, by a factor of 2.61–6.25 times.Conclusions ALT/WDL and lipoma have overlapping MRimaging characteristics. The most reliable imaging discrim-inators of ALT/WDL were size of lesion and lipomatouscontent, but due to the overlap in the MRI appearances oflipoma and ALT/WDL, discrimination should be based onmolecular pathology rather than imaging.
Keywords Atypical lipomatous tumor . Well-differentiatedliposarcoma . Lipoma .Magnetic resonance imaging .
MDM2
Introduction
Liposarcoma is the most frequent soft tissue sarcoma, account-ing for about 20 % of all mesenchymal tumors [1]. The WorldHealth Organization (WHO) Committee for Classification ofSoft tissue Tumors in 2002 subdivided soft-tissue liposarcomasinto five categories: well-differentiated, dedifferentiated, myx-oid, pleomorphic, and mixed liposarcomas [2]. Atypical lipo-matous tumor/well-differentiated liposarcoma (ALT/WDL)represent 40–45 % of liposarcomas and is the most frequentsubcategory of liposarcoma [2, 3]. They occur most frequently
M. Brisson :A. Clarke : P. O’Donnell (*)Department of Radiology, Royal National Orthopaedic Hospital,Stanmore, Middlesex HA7 4LP, UKe-mail: [email protected]
T. Kashima :D. Delaney : R. Tirabosco :A. M. FlanaganDepartment of Histopathology, Royal National OrthopaedicHospital NHS Trust,Stanmore, Middlesex HA7 4LP, UK
A. M. Flanagan : P. O’DonnellInstitute of Orthopaedics and Musculoskeletal Science, UCL,Stanmore, UK
S. CroClinical Trials Unit, Medical Research Council,London, UK
A. M. FlanaganUCL Cancer Institute,Huntley Street,London WC1E 6BT, UK
Skeletal Radiol (2013) 42:635–647DOI 10.1007/s00256-012-1517-z

during the sixth decade of life, with no sex predilection [1, 4],and arise most commonly in the deep soft tissues of the limbs,especially the thigh, followed by the retroperitoneum, the para-testicular area, the mediastinum, and the subcutaneous tissue.They are locally aggressive, with no potential for metastasisunless they contain a dedifferentiated component [2].
The term ALT is preferred to WDL when referring tolesions arising in the limbs and trunk, as a wide excisionmargin is usually curative [5]. In contrast, when tumors arelocated in the retroperitoneum and mediastinum, it is com-monly impossible to obtain a wide excision margin, and localrecurrence, which is frequent, may lead to death. In these sites,the term WDL is often used, but the application of thisterminology can be confusing. In this study, the terms ALT/WDL are considered as synonymous as both have identicalmorphology, karyotype, and biological behavior [2].
It is generally possible to distinguish lipoma and ALT/WDL by histology alone, as the latter consists of a matureadipocytic neoplasm showing unequivocally atypical hyper-chromatic nuclei. [2]. Unlike lipomas, these tumors are oftentraversed by fibrous septa, where the atypical cells tend to bemore numerous and difficult to identify. However, the diag-nosis is sometimes difficult because the atypical stromal cellscan be infrequent and scattered throughout the lesion. In somecases, the identification of unequivocal atypical cells requiresextensive sampling of the tumor [3]. In those particular cases,the difference between lipoma and ALT/WDL may be subtleand subjective [3]. A number of ancillary tools have beendescribed to distinguish these tumors: immunohistochemistry,reverse transcription polymerase chain reaction (RT-PCR) [6,7], fluorescence in situ hybridization (FISH) [8], and anti-bodies to MDM2 and CDK4 [9]. FISH has been shown to
provide a near-perfect correlation between the presence ofsupernumerary ring or giant marker chromosomes in the12q13-15 region and the morphological features of ALT/WDL [10, 11]. These abnormalities result in amplification ofseveral genes (CDK4, SAS, HMGIC, and others) withMDM2,the most frequently amplified gene in ALT/WDL [3, 10, 12].A recent publication shows that in a large series of maturelipomatous tumors, MDM2 is a highly sensitive marker forALT/WDL and that pathologists had a tendency to “overcall”lipomas. The findings were correlated with clinical outcomeproviding additional value to the study [13].
Magnetic resonance imaging has been described as auseful tool for diagnosing lipomatous tumors [4, 14–17]. Itis reported that a confident diagnosis of lipoma can be madeon MR imaging when the entire lesion is isointense tosubcutaneous fat on all sequences, there is complete sup-pression of fatty signal on fat-saturation techniques, and themass contains only a few thin septa [4, 14]. An intramuscu-lar lipoma may present with irregular margins, interdigitat-ing with skeletal muscle, with traversing muscle fiberstypically causing a striated appearance, which is not seenwith other lipomas [4, 18]. Several imaging features arecurrently thought to suggest a diagnosis of ALT/WDL andare widely used by radiologists: these include the size of thelesion (more than 10 cm), thick irregular/nodular septa, non-adipose areas or nodules, and fat content less than 75 %[16]. Other imaging characteristics have also been describedas useful in attempting to distinguish these two lesions, suchas prominent foci of high signal on fluid sensitive sequences[19, 20] and septal enhancement [21, 22].
Just as there are histological similarities between lipomasand ALT/WDL, there is also imaging overlap, with some
A
C D
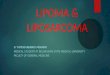
BFig. 1 Transmitted andfluorescent light microscopy ofmature lipomatous tumors.Hematoxylin and eosin (H&E)-stained slides showing repre-sentative tissue sections of ma-ture lipomatous tumor: adult-type fat without atypical cells(a) and with a single cell withan enlarged hyperchromaticnucleus (black arrow) (b). Thecorresponding images showingrepresentative fluorescent insitu hybridization of a nucleusfrom the lipoma showing twored signals and two green sig-nals (c), and the ALT/WDLwith two red signals and >30green signals (d). The red sig-nals represent the centromereand the green signals representMDM2. Bar050 µm
636 Skeletal Radiol (2013) 42:635–647

lipomas sharing the same imaging characteristics tradition-ally described in ALT/WDL [16]. Considering the recentadvances in molecular genetics, which have been exploitedas ancillary tools for diagnosing specific tumors, a morerobust diagnosis is now available to distinguish lipoma fromALT/WDL [13]. The purpose of this study is to review thereliability of MR imaging characteristics of lipoma andALT/WDL, diagnosed on the basis of histopathologicalfeatures and MDM2 amplification.
Table 1 MDM2 amplification status by FISH and histological diag-nosis for each case (n087)
MDM2amplification status
Histologicaldiagnosis
Numberof cases
MDM2 + ALT/WDL 33 (38 %)
MDM2 − Lipoma 54 (62 %)
Total 87
Data is presented asn(%)
A
C
B
D
* *
E F
Fig. 2 Lipomatous content.Homogeneously lipomatous(completely fatty) tumor. aCoronal T1-weighted (T1W)and b T2-weighted MR imageswith fat-saturation (T2W-FS)showing a superficial lipoma-tous mass in the right thigh of a37-year-old male that is com-pletely isointense to subcutane-ous fat in both sequences (blackarrows). Diagnosis: lipoma.Amorphous, non-fatty areas cCoronal T1W and d Short-tauinversion recovery (STIR) MRimages of a deep heterogeneouslipomatous mass in the anteriorcompartment of the left thigh ofa 73-year-old male with non-fatty amorphous areas withinthe mass (*). Diagnosis: lipo-ma. Faint hyperintensity (“al-tered fat”) e Coronal T1W and fSTIR MR images of the leftthigh of a 27-year-old femaleshowing faint hyperintensity ina lipomatous mass in the quad-riceps compartment (“alteredfat” signal, white arrow). Diag-nosis: lipoma
Skeletal Radiol (2013) 42:635–647 637

Materials and methods
This was a retrospective MR imaging review of 102 cases ofprimary soft tissue lipomatous tumors of the extremity andtrunk with a histologically confirmed diagnosis of lipoma orALT/WDL. Cases were retrieved from the histopathologydatabase of the Royal National Orthopaedic Hospital between2003 and 2008. Non-imaging criteria (patient age and gender)were recorded for further statistical analysis but were not usedby the radiologist to distinguish lipoma from ALT/WDL.Recurrent lipomatous tumors and those with inadequate MRimaging were excluded. This study was deemed an audit ofcurrent practice and thus patient consent and institutionalreview was not required.
Histology with MDM2 gene amplification analysis
Representative tissue sections from tissue blocks were exam-ined by fluorescence in situ hybridization (FISH) using theZytoLight SPECMDM2/CEN12 Dual Colour Probe kit (Zyto-Vision GmbH, Bremerhaven, Germany), according to the pro-tocol provided by the manufacturer. This probe cocktailhighlighted the chromosomal region of the humanMDM2geneas a green signal. The centromere of chromosome 12 (CEN12)was detected as a strong and intense red signal (Fig. 1).
Evaluation of the sampled tissue sections was carried out usingfluorescence microscopy on an Olympus BX-50 microscope oron a Mirax viewer (3DHISTECH Kft., Budapest, Hungary)following the digitization of slides using a Zeiss Mirax scanner.Counting a minimum of 50 non-overlapping nuclei per case,the number of each signal for MDM2 and CEN12 wererecorded. A ratio greater than 2.0 was considered to representMDM2 amplification consistent with a diagnosis of ALT/WDL. A ratio of 2 or less was considered to be non-amplified.
Four pathologists, experienced in the examination of softtissue tumors, reviewed the histological sections taken at thetime of resection and provided a consensus diagnosis basedon the World Health Organization criteria [2], in the absenceof knowledge of the relevant clinical information, includingtumor location and size. The microscopic diagnosis wascompared with the fluorescence in situ hybridization(FISH) results and where the histopathology diagnosis didnot concur with the FISH, the slides were reviewed. Thepathologists diagnosed one lipoma that showed extensiveMDM2 amplification and this was reclassified as an ALT/WDL and included in the study. There were six tumorsdiagnosed as ALT/WDL, which revealed normal MDM2and CDK4 copy number and these were excluded from thestudy because for a variety of reasons it was not clear howbest to classify them. Hence, all tumors included in this
AA
C
B
D
Fig. 3 Septations. Thin(“pencil-line”) septa a AxialT1W and b STIR MR imagesshowing a lipomatous mass inthe midline posterior trunk of a43-year-old female that remainsisointense to subcutaneous fatin both sequences and that con-tains thin, delicate septa (blackarrows). Diagnosis: lipoma.Thick septa c Coronal T1W andd STIR MR images of a deepheterogeneous lipomatous massof the posterior compartment ofthe left thigh of a 55-year-oldfemale that is predominantlyisointense to subcutaneous fatin both pulse sequences. Thickseptations are also evident(white arrows). Diagnosis:lipoma
638 Skeletal Radiol (2013) 42:635–647

imaging study that revealed MDM2 amplification (accord-ing to the above definition) were classified as ALT/WDL,and those without atypia (by consensus) and without thisgenetic abnormality were classified as lipoma.
From the initial group of 102 cases where imaging wasavailable for review (Table 1), there were 33 cases whereMDM2 was amplified, 32 of which showed unequivocalcellular atypia and one (mentioned above) with minimalatypia but extensive MDM2 amplification, consistent witha diagnosis of ALT/WDL. There were 54 cases whereMDM2 was not amplified and histological analysis wasconsistent with a diagnosis of lipoma. Finally, 15 cases wereexcluded (six unclassified tumors with normal MDM2 copynumber (as above) and nine cases of dedifferentiated lip-osarcoma [DLS]). A total of 87 cases were included in thisstudy: 50 female and 37 male with a mean age of 55 years(range 10–83 years).
MR image analysis
One radiologist, experienced in bone and soft tissue tumorMRI, without knowledge of the patient history or final patho-logical diagnosis, reviewed MR images of the 87 cases. Asecond radiologist, also blinded to patient history and finaldiagnosis, independently reviewed 90 % of the cases to estab-lish interobserver reliability for the diagnosis of lipoma or ALT/WDL using these MRI criteria. The first radiologist assessedthe images for a second time so that intra-observer variabilitycould be additionally assessed. MR imaging was performed ona variety of high-field systems, as many patients had beenscanned before referral. The MR imaging protocols includeda variety of sequences in sagittal, coronal, and axial planesusing T1-weighted spin echo (T1 W SE), T2-weighted fastspin echo with fat suppression (T2 W FSE FS), and short tauinversion recovery (STIR) sequences. Contrast enhancement
A
C
F
B
D E
G H
E
Fig. 4 Nodules. a Axial T1Wand b STIR MR imagesshowing a deep lipomatousmass in the left gluteal region ofa 68-year-old female with anon-specific nodule (definedarea of non-lipomatous tissue,hypointense on T1W and hy-perintense on STIR (open whitearrows). Diagnosis: ALT/WDL.c Axial T1W and d STIR MRimages of a deep heterogeneouslipomatous mass of the posteri-or compartment of the rightthigh of a 56-year-old malepresenting with a fatty nodule(open white arrows). DiagnosisALT/WDL. e Lateral plain filmin the same patient confirms arim of ossification (black ar-row). f Coronal T1W, g T2W-FS MR and h axial CT imagesof the anterior compartment ofthe right thigh in a 64-year-oldmale patient showing a denselyossified nodule in a heteroge-neous, predominantly fattymass (black arrows). Diagno-sis: ALT/WDL
Skeletal Radiol (2013) 42:635–647 639

was not used in the majority of patients in this study as patientswere referred from a number of hospitals, using different im-aging protocols and was not evaluated in this study. EstablishedMR imaging features were assessed: lipomatous content(Fig. 2) ([a and b] completely fatty; [c and d] amorphous,non-fatty areas within the lipomatous tumor and even faintareas of hyperintensity (“altered fat” signal [e and f]) on fluid-sensitive sequences; solid, non-fatty masses); septa (Fig. 3)(absence, thin (“pencil-line”) [a and b] or thick/nodular [c andd]) and nodules (Fig. 4) (absence or presence, size and signal).The location (upper limb, lower limb, trunk), depth (subcuta-neous or deep to fascia) and maximum dimension of tumorwere recorded but, as with non-imaging criteria, not used todistinguish lipoma from ALT/WDL.
Using strict imaging criteria, anMR diagnosis of lipomawasconsidered for any completely fatty tumor with or without thinsepta and no nodules. Muscle fibers running through the lesionwithout other evidence of thick septa or nodules was considereddiagnostic of an intra-muscular lipoma (Fig. 5). The diagnosisof ALT/WDL was made if the lesion showed: a non-fatty area,thick/nodular septa, or nodule(s), whatever the size or signal.
Statistical analysis
The following analyses were applied to the entire study group(87 patients). Analysis of a subgroup of patients who wereover 40 years old, with large (greater than 10 cm) and deep(subfascial) tumors was also performed.
Table 2 Summary of results foreach imaging and non-imagingvariable in group with ALT/WDL and lipoma
aOmitted as nodules ≥1 cm pre-dicts ALT/WDL perfectly
Variable ALT/WDL (n) Lipoma (n) Odds ratio (95 % CI) p value
Gender Male 15 22 1.21 (0.51–2.91) 0.666Female 18 32
Age >60 years 18 17 2.61 (1.07–6.39) 0.035≤60 years 15 37
Lesion size >10 cm 30 35 5.43 (1.46–20.15) 0.011≤10 cm 3 19
Location Lower limb 28 30 4.48 (1.50–13.36) 0.007Upper limb/trunk 5 24
Septation Thick 15 15 2.17 (0.87–5.37) 0.095Absence/thin 18 39
Nodules Presence 13 12 2.28 (0.88–5.87) 0.089Absence 20 42
Nodules ≥1 cm 9 0 aAbsence/<1 cm 24 54
Fat content Solid/amorphous 29 29 6.25 (1.93–20.22) 0.002Completely fatty 4 25
Signal intensity Increased 5 9 0.89 (0.27–2.94) 0.852Not Increased 28 45
A BFig. 5 Intramuscular lipoma. aCoronal and b axial T1Wimages of a 62-year-old femaleshowing a predominantly fattylesion in the left deltoid withmuscle fibers running throughthe lesion (open black arrows).Diagnosis: lipoma
640 Skeletal Radiol (2013) 42:635–647

Every test performed was two-sided and p values lessthan 0.05 were considered to indicate a statistically signifi-cant difference. The MR imaging diagnoses suggested bythe radiologist were compared to the pathological diagnosesbased on histopathology and MDM2 amplification and thefollowing analyses were performed: sensitivity (the propor-tion of histology/MDM2-amplification positive cases diag-nosed as ALT/WDL, compared with MR diagnosis),specificity (the proportion of histology/MDM2-amplifica-tion negative cases diagnosed as lipoma, compared withMR diagnosis), positive predictive value (proportion ofALT/WDL that were correctly diagnosed using MR criteria)and negative predictive value (proportion of lipomas thatwere correctly diagnosed using MR criteria).
Comparisons of patient age and size of lesion betweenboth groups were performed using unpaired Wilcoxon rank-sum tests for non-normally distributed continuous variables.The univariable association between each of the binaryimaging and non-imaging variables under study and ALT/WDL was analyzed by logistic regression. Odds ratios (OR)were calculated along with 95 % confidence intervals toquantify the relative odds of having an ALT/WDL for anindividual of the marked category, in comparison to thereference category. An OR greater than 1 indicates increasedodds of ALT/WDL while an OR less than 1 indicates de-creased odds of ALT/WDL. A multiple binary logistic re-gression model was built using a stepwise selection methodto confirm the multivariable contribution of the observedimaging and non-imaging variables and determine whichstudy variables best predicted a diagnosis of ALT/WDL.
Reproducibility between each of the two observers wascalculated using Cohen’s kappa statistics with correction forexpected chance agreement. Data analysis was performedusing Prism version 4 for Macintosh (GraphPad Software,San Diego, CA), except for kappa and odds ratios statisticsthat were calculated using Stata/IC v12.0, StataCorp, Col-lege Station, TX, USA.
Results
Using a combination of histology and FISH analysis, out ofa total of 87 mature lipomatous tumors, 33 were diagnosedas ALT/WDL and 54 as lipomas. Using the strict MRimaging criteria described in the Materials and methodssection, 64 ALT/WDL and 23 lipomas were diagnosed bythe radiologist. This represents a sensitivity of 90.9 % (CI74.5–97.6) and a specificity of 37.0 % (CI 24.6–51.3). Thepositive and negative predictive values were 46.9 % (CI34.5–59.7) and 86.9 % (CI 65.3–96.6), respectively.
The mean age for the group with lipomas was 52 years(median053.5, range 10–79 years) and 60 years (median065, range 40–83 years) for the group with ALT/WDL. The
Wilcoxon rank-sum test confirmed that age was significant-ly greater for the ALT/WDL patients (p00.025). The meansize of lipomas was 13.9 cm (median013, range 3–32 cm)and ALT/WDL 18.7 cm (median018.4, range 5–36 cm).The Wilcoxon rank-sum test confirmed that size was alsosignificantly greater for the ALT/WDL patients (p00.003).Only three ALT/WDL measured 10 cm or less.
Table 2 summarizes the associations between ALT/WDLand the important binary imaging and non-imaging varia-bles of interest in this study. Using histology and FISH asthe gold standard, differences between the lipoma and ALT/WDL groups in patient age (>60 years), size of lesion(>10 cm), location, and fat content were statistically
*
Age
of p
atie
nt (
year
s)
lipoma(n=54)
ALT/WDL(n=33)
0102030405060708090
Fig. 6 Comparison of age of patients with lipoma (n054) and ALT/WDL(n033). The continuous lines depict the mean age in both groups.The average age of patients in the lipoma group was 52 years (range10–79 years) and 60 years (range 40–83 years) in the ALT/WDLgroup. The break lines represent the number of patients aged 40 yearsand less (nine lipomas and two ALT/WDL). * indicates p00.02 withunpaired Wilcoxon rank-sum test
lipoma(n=54)
ALT/WDL(n=33)
0
10
20
30
40
*
Max
imum
dim
ensi
on o
f tum
or (
cm)
Fig. 7 Comparison of the size of lipomas (n054) and ALT/WDL(n033). The continuous lines depict the average dimensions in bothgroups. The average tumor dimensions were 13.9 cm (range 3–32 cm) for lipomas and 18.7 cm (range 5–36 cm) for ALT/WDL.The break lines represent the number of tumors measuring 10 cmand less (19 lipomas and three ALT/WDL). * indicates p00.003 withunpaired Wilcoxon rank-sum test
Skeletal Radiol (2013) 42:635–647 641

significant with p values of 0.035, 0.011, 0.007, and 0.002,respectively (Figs. 6 and 7).
The distribution of tumors is presented in Table 3. ALT/WDL were frequently located in the lower limb (n028(85 %)) while lipomas were slightly more evenly distributedbetween the lower limb (n030 (56 %)) and the upper limb/trunk (n024 (44 %)). In this study, all ALT/WDL werelocated in deep locations with only seven of the 54 lipomassited subcutaneously, five located in the trunk/upper limb,and two in the lower limb.
A purely fatty stroma on MRI (100 % lipomatous con-tent), without altered fat signal or non-fatty masses, andcontaining either no or only thin septa was observed in bothlipomas (Fig. 8) and ALT/WDL. Specifically, this patternwas seen in four cases (12 %) of ALT/WDL (Fig. 9a, b), andof these, one case showed muscle fibers running through thelesion and was diagnosed as an intramuscular lipoma basedon MR criteria (Fig. 9c, d). In contrast, 24 lipomas (44 %)showed these appearances.
Areas of increased signal intensity relative to subcutane-ous fat on fluid-sensitive sequences, and/or non-fatty fociwere recorded in the majority of ALT/WDL (n029, 88 %)but were also seen in 29 (54 %) of lipomas. Thereafter, wesubdivided the lesions containing amorphous areas into twocategories: amorphous areas occupying less or more than
50 % of the mass. An amorphous signal occupying morethan 50 % of the tumor was more frequently seen in thegroup with ALT/WDL (ten cases, 30 % of the total numberof ALT) than in the group with lipoma (six cases, 11 %).There were two cases (one lipoma and one ALT/WDL) thatshowed large solid masses within the fatty tumor, suggest-ing a dedifferentiated component (Fig. 10). Histologically,these non-fatty components were described as lipomatoustumors with a major inflammatory component and, in onecase, there was also focal metaplastic bone. Subtle, amor-phous, and faint hyperintensity within the tumor (“alteredfat” signal) on T2 W FSE FS or STIR sequences was alsoassessed as a potential sign of ALT/WDL (Fig. 2e and f).There were 14 cases where a radiological diagnosis of ALT/WDL was based solely on the presence of a subtle amor-phous area of faint increased signal. Nine out of these 14cases were diagnosed as lipomas based on histology andMDM2 amplification status.
Absence, or presence of only thin “pencil-line” septationwas identified in 39 (72 %) lipomas and 18 (55 %) ALT/WDL,while thick/nodular septa were present in 15 (28 %) lipomasand 15 (45 %) ALT/WDL. The presence of nodules was alsodescribed in both groups, but nodules measuring more than1 cm were only seen in nine (27 %) cases of ALT/WDL andwere never observed in lipomas. The signal of individualnodules was unhelpful as we found mineralized (corticatedmargin with fatty marrow centrally or diffusely calcified[Fig. 4c–h]) and non-specific soft tissue nodules (hypointenseon T1-weighted and hyperintense on STIR images relative tofat [Fig. 4a/b]) in both ALT/WDL and lipomas.
In total, 30 out of 54 lipomas (MDM2 amplificationnegative) (56 %) presented with non-fatty areas, nodules,or thick septa. All of these cases revealed unequivocalabsence of cellular atypia although they contained areas of
A B
Fig. 8 Lipoma with MR imaging features of lipoma. a Coronal T1Wand b STIR MR images showing a deep lipomatous mass in theadductor compartment of left thigh of a 38-year-old male. The massis homogenous, completely isointense to subcutaneous fat on T1Wimages, and is completely suppressed on the STIR sequence, consistent
with a radiological diagnosis of lipoma. Some muscle fibers are visibleat the edge of the mass (white arrows). No cellular atypia were reportedand MDM2 was not amplified, which is consistent with a pathologicaldiagnosis of lipoma
Table 3 Body distribution for each case of ALT/WDL (n033) andlipoma (n054)
Distribution ALT/WDL Lipoma
Lower limb 28 (85 %) 30 (56 %)
Upper limb/trunk 5 (15 %) 24 (44 %)
Data is presented as n(%)
642 Skeletal Radiol (2013) 42:635–647

fat necrosis or fibrosis (Fig. 11), resulting in similar MRIappearances to ALT/WDL (Fig. 12).
The odds ratios used to assess the risk of having an ALT/WDL versus lipoma are detailed in Table 2. The non-imaging and imaging features favoring a diagnosis ofALT/WDL in univariable analysis were: age over 60 years
(OR02.61, 95 % CI 1.07–6.39, p00.035), lesion size ofmore than 10 cm (OR05.43, 95 % CI 1.46–20.15, p00.011), mass located in the lower limb (OR04.48, 95 %CI 1.50–13.36, p00.007) and presence of a non-fatty area(solid or amorphous) on MR imaging (OR06.25, 95 % CI1.93–20.22, p00.002).
A BFig. 10 ALT/WDL with anMR imaging appearance ofdedifferentiated liposarcoma(DLS). a Sagittal T1W and bSTIR MR images showing adeep lipomatous mass in theanterior compartment of thethigh of a 75-year-old female.The mass appears heteroge-neous, with a large area of moresolid, non-lipomatous tumorinferiorly (black arrows), sug-gesting a diagnosis of dediffer-entiated liposarcoma. MDM2showed amplification and his-tology an atypical lipomatoustumor with a major inflamma-tory component, consistent withthe diagnosis of ALT/WDL
A B
C D
Fig. 9 ALT/WDL with MRimaging features of lipoma. aAxial T1W and b STIR MRimages showing a deeplipomatous mass in theadductor compartment of theright thigh of a 44-year-oldmale. The mass is homoge-neous, completely isointense tosubcutaneous fat on T1Wimages, and is completely sup-pressed on the STIR sequence,which is consistent with a ra-diological diagnosis of lipoma(white arrows). c Sagittal T1Wand d STIR images show a le-sion in the anterior compart-ment of the arm of a 51-year-old female with signal identicalto subcutaneous fat, containingmuscle fibers, consistent with aradiological diagnosis of intra-muscular lipoma (blackarrows). FISH performed onthese two cases showed numer-ous cells with unequivocalMDM2 amplification consistentwith pathological diagnosis ofALT/WDL
Skeletal Radiol (2013) 42:635–647 643

Using the imaging and non-imaging criteria, a final multi-ple logistic regressionmodel was built and is shown inTable 4.The size of the lesion (cm) and lipomatous content (solid/amorphous relative to completely fatty) were the strongestpredictors of ALT/WDL in the multivariable analysis and,after adjusting for these two variables, none of the othersretained significance. The adjusted OR for size (cm) was1.09 (95 % CI 1.02–1.18, p00.016), and the adjusted ORfor lipomatous content 5.15 (95 % CI 1.54–17.19), p00.008).
The radiological inter-observer reliability was substantialand the intra-observer reliability excellent with Kappa val-ues of 0.71 and 0.89, respectively.
Analysis of large, deep lesions in older patients
A total of 55 cases (32 female, 23 male; mean age 61 years,range 41–83 years) were included in the subgroup analysis ofolder patients (over 40 years old), with large (greater than10 cm), deep (subfascial) tumors. Of the 55 patients, 26 wereclassified as lipomas and 29 as ALT/WDL using a combinationof histology and FISH analysis. Using the strict MR imagingcriteria described in the Materials and methods section, 46
ALT/WDL and nine lipomaswere diagnosed by the radiologist.MR identified ALT/WDL with a sensitivity of 96.6 % (CI80.4–99.8) and a specificity of 30.8 % (CI 15.1–51.9). Thepositive and negative predictive values were 60.9 % (CI 45.4–74.5) and 88.9 % (CI 50.7–99.4), respectively.
The mean age of patients with ALT/WDL was greater(mean062 years, median065 years [range 41–83 years])than those with lipoma (mean060 years, median063 years[range 42–79 years]). However, this was not a significantdifference (p00.473). The mean size of ALT/WDL (mean020.3 cm, median019 cm [range 12–36 cm]) was not signif-icantly greater than lipoma (mean018.1 cm, median018 cm[range 11–32 cm]) (p00.221).
Table 5 summarizes the associations between ALT/WDL(as assessed using the combination of histology and FISHanalysis) and the important imaging and non-imaging vari-ables of interest in this study subgroup. The differencebetween the lipoma and ALT/WDL groups in fat contentwas statistically significant with a p value of 0.006. Thepresence of non-fatty (solid/amorphous) areas increased thelikelihood of ALT/WDL by a factor of 9.90 times (95 % CI1.93–50.71). This was the strongest predictor of ALT/WDL
A BFig. 12 ALT/WDL with MRimaging features of ALT/WDL.a Coronal T1Wand b STIR MRimages showing a deeplipomatous mass in theadductor compartment of theright thigh of a 43-year-old fe-male. The mass is heteroge-neous and shows extensive,amorphous, non-fatty signalconsistent with an MR diagno-sis of ALT/WDL (open whitearrows)
A BFig. 11 Lipoma with MRimaging features of ALT/WDL.a Coronal T1Wand b STIR MRimages showing a deeplipomatous mass in the rightdeltoid of a 53-year-old male,which contains an area of het-erogeneous signal suggestive ofALT/WDL based on radiologi-cal criteria (white arrows). Onhistology review, the lesionshowed areas of fibrosis andnecrosis without MDM2 ampli-fication consistent with a diag-nosis of lipoma
644 Skeletal Radiol (2013) 42:635–647

and, after adjusting for lipomatous content using a multiplelogistic regression model, none of the others variables weresignificant predictors.
Discussion
Just as distinction between lipoma and ALT/WDL on MRimaging often represents a challenge, the same difficulty isnot infrequently encountered by histopathologists. Hereinwe have described the MR imaging features of lipomasand ALT/WDL based on a pathological diagnosis using acombination of histology, and genetic testing (MDM2-am-plification status), which currently represents the most ob-jective method for reaching a diagnosis [13].
The MRI appearances of ALT/WDL in this study aresimilar to those previously described [16] and most fre-quently this tumor presents as a heterogeneous fatty masssimilar to lipoma, containing areas of non-adipose tissue ornodules and areas of non-specific increased signal intensityon STIR or T2 W FSE FS images. However, the presence ofthick and irregular/nodular septa traditionally described inALT/WDL was not statistically significant in this study,although more lesions with thick septa were seen in thisgroup [16, 22]. This finding could be due to a referral bias,
as lipomas presenting with atypical features are more likelyto be referred for consultation. Hosono et al. [22] suggestedthat irregular, thick septa in ALT/WDL showed markedenhancement following intravenous injection of gadopente-tate dimeglumine as opposed to faint enhancement of thin,regular septa in lipomas. Septal enhancement was not in-vestigated in our study as too few patients were imagedfollowing intravenous injection of contrast, but may be amethod of further discriminating tumors with thick septa, asseptal morphology was unhelpful.
It is of interest that four of 33 (12 %) ALT/WDL showedcompletely fatty masses with none or only pencil-line septa onMR imaging. Although these cases were classified as ALT/WDL by the histopathologists on the basis of cellular atypia,which was supported by the presence of numerous cells beingMDM2 amplification-positive, these tumors revealed virtuallyno fibrosis microscopically. The MRI appearances of one ofthese cases presented with the typical appearances of anintramuscular lipoma. Recently, similar findings werereported in two cases of genetically proven intramuscularALT/WDL [23]. These findings imply that the presence ofintralesional muscle fibres is not a reliable sign of a benignlesion as traditionally described [18]. In contrast, nodulesmeasuring more than 1 cm in diameter seem to be an impor-tant discriminator and favors ALT/WDL over a lipoma, al-though the signal of the nodules was not found to be helpful.
Traditionally, lipomas have been described as showinghomogeneous signal intensity identical to subcutaneous fatin all pulse sequences, with complete loss of signal after fatsuppression. Forty-four percent (n024) of tumors classifiedas lipomas in this study presented as a completely fatty masson imaging without any, or only thin (“pencil-line”) septa.However, non-fatty areas, nodules, or thick septa were iden-tified in other lipomas (56 %, n030) and correlation with the
Table 5 Subgroup analysis forpatients >40 years, tumor size>10 cm, deep (subfascial) loca-tion. Summary of results foreach imaging and non-imagingvariable in group with ALT/WDL and lipoma
aOmitted as nodules ≥1 cm pre-dicted ALT/WDL perfectly
Variable ALT/WDL (n) Lipoma (n) Odds ratio (95 % CI) p value
Gender Male 13 10 1.30 (0.44–3.82) 0.633Female 16 16
Age >60 years 18 13 1.64 (0.56–4.79) 0.369≤60 years 11 13
Location Lower limb 25 20 1.88 (0.46–7.57) 0.377Upper limb/Trunk 4 6
Septation Thick 14 8 2.10 (0.69 6.35) 0.189Absence/Thin 15 18
Nodules Presence 12 8 1.59 (0.52–4.84) 0.415Absence 17 18
Nodules ≥1 cm 8 0 aAbsence/<1 cm 21 26
Fat content Solid/Amorphous 27 15 9.90 (1.93–50.71) 0.006Completely fatty 2 11
Signal Intensity Increased 4 5 0.67 (0.16–2.83) 0.588Not Increased 25 21
Table 4 Multiple logistic regression model to predict ALT/WDLa
Odds ratio 95 % CI p value
Size of lesion (cm) 1.09 (1.02–1.18) 0.016
Fat content (solid/amorphousrelative to completely fatty)
5.15 (1.54–17.19) 0.008
a Predictors of ALT/WDL selected from Table 2 by using stepwiselogistic regression
Skeletal Radiol (2013) 42:635–647 645

pathology revealed areas of fat necrosis or fibrosis, whichwould account for the imaging appearances. Kransdorf et al.also noted the existence of non-adipose areas and thick septain lipomas [16], but concluded that nodular, globular, andmass-like non-adipose areas were helpful in differentiatingALT/WDL from lipoma. It is also worthy of note that in onelipoma, the amount of necrosis and inflammation resulted inthe MRI appearances suggesting a diagnosis of dedifferen-tiated liposarcoma. Our findings are likely to reflect biasresulting from a disproportionate number of large, hetero-geneous lipomatous tumors referred to a tertiary center.
We found that MRI showed an overall excellent sensitivitybut a poor specificity for identifying these lipomatous tumorsusing our criteria. Poor specificity was due to a high numberof cases diagnosed as ALT/WDL on imaging but reported aslipoma on histology. The authors assessed “altered fat” signalwithin the tumor as a potential sign of an ALT/WDL, in viewof its uncertain relevance, even though it was thought likely toresult in false-positive diagnoses (over-diagnosis of ALT/WDL). Of the 14 cases where a radiological diagnosis ofALT/WDL was based solely on its presence, nine were diag-nosed as lipomas. The use of this criterion explains at least insome cases our false-positive ALT/WDL imaging diagnoses.
As expected, no gender predilection was identified be-tween the patients diagnosed with lipoma and ALT/WDL, afinding that is consistent with previous reports [2, 5, 12, 15,23]. We found that on average patients were statisticallyolder in the group with ALT/WDL than with lipoma. Nopatient with an ALT/WDL was less than 40 years old and asignificant increased likelihood of a final diagnosis of ALT/WDL in patients over 60 years old was found. This supportsresults reported by others [2, 3, 5, 12, 15, 16]. A similarrange in size for both ALT/WDL and lipomas was observed.However, on average, the maximum dimensions of ALT/WDL were statistically greater than lipomas, which is alsoconsistent with previous studies [2, 5, 12, 15, 16]. While itwas frequent for lipomas to measure less than 10 cm, onlythree ALT/WDL in our study were in this category. Size is ahelpful means of distinguishing the two tumor types.
Our results also suggest that lower limb location is asignificant predictor of ALT/WDL. Most of the tumors inthis study were located in the lower limb but ALT/WDLwere relatively infrequent in the upper limb and trunk.Lipomatous content was also identified as a significantpredictor of ALT/WDL. Specifically, the odds of ALT/WDL were found to be greater for patients with solid/amor-phous content in comparison to those with completely fattycontent. In older patients with large tumors, lipomatouscontent was the only significant predictor of ALT/WDL,with the presence of non-fatty areas increasing the likeli-hood of a malignant diagnosis by a factor of 9.90 times.
In summary, we identified imaging and non-imagingfeatures favoring a diagnosis of ALT/WDL. The most
important features, based on univariable analysis and oddsratios, were: patient age over 60 years, maximum lesiondimension over 10 cm, location in the lower limb, andpresence of non-fatty (solid or amorphous) areas. Kransdorfet al. [16] reported similar results but also included thepresence of thickened septa and nodular areas. The discrep-ancies between these results may be due to the bigger size ofour cohort and a more robust pathological diagnosis. Mul-tivariable analysis revealed that the size of the lesion andlipomatous content were the strongest predictors; afteradjusting for these two variables, none of the other factorsretained significance.
In conclusion, using standard imaging characteristics(thick septa, nodules, and non-fatty areas) compared tohistology and MDM2 amplification status, there was a highsensitivity but poor specificity for the diagnosis of thesetumors due to over-diagnosis of ALT/WDL on imaging.The strongest non-imaging and imaging predictors ofALT/WDL are lesion size and presence of non-fatty areas.This paper highlights the necessity to reassess the applica-tion of traditionally described MR features and the require-ment to use advances in pathology to reach a reliablediagnosis.
Conflict of interest The authors declare that they have no conflictsof interest.
References
1. Dei Tos AP. Liposarcoma: new entities and evolving concepts.Ann Diagn Pathol. 2000;4(4):252–66.
2. Fletcher CDM, Unni KK, Mertens F, >editors. World HealthOrganization Classification of Tumor. Pathology and Genetics ofTumors of Soft Tissue and Bone. Lyon: IARC Press; 2002.
3. Coindre JM, Pedeutour F, Aurias A. Well-differentiated and dedif-ferentiated liposarcomas. Virchows Arch. 2009 Aug 18.
4. MurpheyMD, Arcara LK, Fanburg-Smith J. From the archives of theAFIP: imaging of musculoskeletal liposarcoma with radiologic-pathologic correlation. Radiographics. 2005;25(5):1371–95.
5. Evans HL. Atypical lipomatous tumor, its variants, and its com-bined forms: a study of 61 cases, with a minimum follow-up of 10years. Am J Surg Pathol. 2007;31(1):1–14.
6. Shimada S, Ishizawa T, Ishizawa K, Matsumura T, Hasegawa T,Hirose T. The value of MDM2 and CDK4 amplification levelsusing real-time polymerase chain reaction for the differential diag-nosis of liposarcomas and their histologic mimickers. Hum Pathol.2006;37(9):1123–9.
7. Hostein I, Pelmus M, Aurias A, Pedeutour F, Mathoulin-PelissierS, Coindre JM. Evaluation of MDM2 and CDK4 amplification byreal-time PCR on paraffin wax-embedded material: a potential toolfor the diagnosis of atypical lipomatous tumours/well-differentiat-ed liposarcomas. J Pathol. 2004;202(1):95–102.
8. Sirvent N, Coindre JM, Maire G, Hostein I, Keslair F, Guillou L, et al.Detection of MDM2-CDK4 amplification by fluorescence in situhybridization in 200 paraffin-embedded tumor samples: utility in
646 Skeletal Radiol (2013) 42:635–647

diagnosing adipocytic lesions and comparison with immunohisto-chemistry and real-time PCR. Am J Surg Pathol. 2007;31(10):1476–89.
9. Binh MB, Sastre-Garau X, Guillou L, de Pinieux G, Terrier P,Lagace R, et al. MDM2 and CDK4 immunostainings are usefuladjuncts in diagnosing well-differentiated and dedifferentiated lip-osarcoma subtypes: a comparative analysis of 559 soft tissue neo-plasms with genetic data. Am J Surg Pathol. 2005;29(10):1340–7.
10. Kashima T, Halai D, Ye H, Hing SN, Delaney D, Pollock R, et al.Sensitivity of MDM2 amplification and unexpected multiple faintalphoid 12 (alpha 12 satellite sequences) signals in atypical lipo-matous tumor. Mod Pathol. 2012. doi:10.1038/modpathol.2012.90[Epub ahead of print].
11. Weaver J, Downs-Kelly E, Goldblum JR, Turner S, Kulkarni S,Tubbs RR, et al. Fluorescence in situ hybridization for MDM2gene amplification as a diagnostic tool in lipomatous neoplasms.Mod Pathol. 2008;21(8):943–9.
12. Dei Tos AP, Doglioni C, Piccinin S, Sciot R, Furlanetto A,Boiocchi M, et al. Coordinated expression and amplification ofthe MDM2, CDK4, and HMGI-C genes in atypical lipomatoustumours. J Pathol. 2000;190(5):531–6.
13. Zhang H, Erickson-Johnson M, Wang X, Oliveira JL, NascimentoAG, Sim FH, et al. Molecular testing for lipomatous tumors: criticalanalysis and test recommendations based on the analysis of 405extremity-based tumors. Am J Surg Pathol. 2010;34(9):1304–11.
14. Nishida J, Morita T, Ogose A, Okada K, Kakizaki H, Tajino T, etal. Imaging characteristics of deep-seated lipomatous tumors: in-tramuscular lipoma, intermuscular lipoma, and lipoma-like lipo-sarcoma. J Orthop Sci. 2007;12(6):533–41.
15. Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH,Kransdorf MJ. From the archives of the AFIP: benign musculo-skeletal lipomatous lesions. Radiographics. 2004;24(5):1433–66.
16. Kransdorf MJ, Bancroft LW, Peterson JJ, Murphey MD, FosterWC, Temple HT. Imaging of fatty tumors: distinction of lipomaand well-differentiated liposarcoma. Radiology. 2002;224(1):99–104.
17. Gaskin CM, Helms CA. Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): results of MRI evalu-ations of 126 consecutive fatty masses. AJR Am J Roentgenol.2004;182(3):733–9.
18. Matsumoto K, Hukuda S, Ishizawa M, Chano T, Okabe H. MRIfindings in intramuscular lipomas. Skeletal Radiol. 1999;28(3):145–52.
19. Galant J, Marti-Bonmati L, Saez F, Soler R, Alcala-Santaella R,Navarro M. The value of fat-suppressed T2 or STIR sequences indistinguishing lipoma from well-differentiated liposarcoma. EurRadiol. 2003;13(2):337–43.
20. Doyle AJ, Pang AK, Miller MV, French JG. Magnetic resonanceimaging of lipoma and atypical lipomatous tumour/well-differen-tiated liposarcoma: observer performance using T1-weighted andfluid-sensitive MRI. J Med Imaging Radiat Oncol. 2008;52(1):44–8.
21. Ohguri T, Aoki T, Hisaoka M, Watanabe H, Nakamura K,Hashimoto H, et al. Differential diagnosis of benign peripherallipoma from well-differentiated liposarcoma on MR imaging: iscomparison of margins and internal characteristics useful? AJRAm J Roentgenol. 2003;180(6):1689–94.
22. Hosono M, Kobayashi H, Fujimoto R, Kotoura Y, Tsuboyama T,Matsusue Y, et al. Septum-like structures in lipoma and liposar-coma: MR imaging and pathologic correlation. Skeletal Radiol.1997;26(3):150–4.
23. Donato M, Vanel D, Alberghini M, Mercuri M. Muscle fibersinside a fat tumor: a non-specific imaging finding of benignancy.Eur J Radiol. 2009;72(1):27–9.
Skeletal Radiol (2013) 42:635–647 647








![Large buccal fat pad lipoma: A rare case report...gland lipoma in 2 cases, angiolipoma in 2 cases, and spindle cell lipoma in 3 cases [10]. The most common presentation of BFP lipoma](https://img.pdfslide.us/doc/110x75/5e610a1252021369db53e163/large-buccal-fat-pad-lipoma-a-rare-case-report-gland-lipoma-in-2-cases-angiolipoma.jpg)