-
7/31/2019 MR Pulse Sequences
1/125
MR PulseMR PulseSequencesSequences
-
7/31/2019 MR Pulse Sequences
2/125
ObjectiveObjective
Physic overviewPhysic overview Basic sequencesBasic sequences
Clinical ApplicationClinical Application
-
7/31/2019 MR Pulse Sequences
3/125
MRIMRI
MRI: Magnetic resonance imagingMRI: Magnetic resonance
imaging
Excellent anatomic and pathologicExcellent anatomic and
pathologicdetaildetail
Recent technologic advancesRecent technologic advances
-
7/31/2019 MR Pulse Sequences
4/125
Commom symbols of pulseCommom symbols of pulsesequence
diagramssequence diagrams
-
7/31/2019 MR Pulse Sequences
5/125
MRIMRIThe basis conceptThe basis concept
T1 recoveryT1 recoveryT2 and T2* decayT2 and T2* decay
Repetition time: TRRepetition time: TR Echo time: TEEcho time:
TE Contrast weightingContrast weighting
-
7/31/2019 MR Pulse Sequences
6/125
Physics overview
(Net magnetization vector)
-
7/31/2019 MR Pulse Sequences
7/125
Magnetization relaxationMagnetization relaxationand decayand
decay
-
7/31/2019 MR Pulse Sequences
8/125
-
7/31/2019 MR Pulse Sequences
9/125
Fat: Shorter T1 (recovers faster)Fat: Shorter T1 (recovers
faster)
Shorter T2 (decays faster)Shorter T2 (decays faster) Water (long
T1 and T2)Water (long T1 and T2) T2*T2*
- depends on the magnetic enviroment- depends on the magnetic
enviroment
(external field)(external field)- Decay of both fat and water
occurs very- Decay of both fat and water occurs
veryquiklyquikly
-
7/31/2019 MR Pulse Sequences
10/125
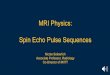
Definitions: TR and TEDefinitions: TR and TE
Two key parametersTwo key parameters
TR(ms) and TE(ms) are key to theTR(ms) and TE(ms) are key to
the
creation of image contrastcreation of image contrast
TR: The time between the applicationTR: The time between the
applicationof an RF excitation pulse and theof an RF excitation
pulse and thestart of the next RF pulsestart of the next RF
pulse
TE: the time between the applicationTE: the time between the
applicationof RF pulse and the peak of echoof RF pulse and the peak
of echodetecteddetected
-
7/31/2019 MR Pulse Sequences
11/125
-
7/31/2019 MR Pulse Sequences
12/125
-
7/31/2019 MR Pulse Sequences
13/125
MR Signal Localization-MR Signal
Localization-GradientsGradients
Gradients are linear variations of theGradients are linear
variations of themagnetic field strength in a selectedmagnetic
field strength in a selectedregion.region.
Three types of Gradients are appliedThree types of Gradients are
applied
- The section-selective gradient:The section-selective
gradient:
-
The phase-encoding gradient:The phase-encoding gradient:- The
frequency-encoding gradientThe frequency-encoding gradient
-
7/31/2019 MR Pulse Sequences
14/125
ImagingPlane
Sliceselection
Encoding
Phase Frequency
Coronal Gy Gx GzAxial (bodyimaging)
Gz Gy Gx
Axial (headimaging)
Gz Gx Gy
Sagital Gx Gy Gz
-
7/31/2019 MR Pulse Sequences
15/125
It can compute the exact location andIt can compute the exact
location andamplitude of the signalamplitude of the signal
K- Space and the Image Matrix- >K- Space and the Image
Matrix- >
Fourrier: ImageFourrier: Image
-
7/31/2019 MR Pulse Sequences
16/125
-
7/31/2019 MR Pulse Sequences
17/125
Tissue ContrastTissue Contrast
-
7/31/2019 MR Pulse Sequences
18/125
Tissue ContrastTissue Contrast
-
7/31/2019 MR Pulse Sequences
19/125
Tissue ContrastTissue Contrast
-
7/31/2019 MR Pulse Sequences
20/125
Tissue ContrastTissue Contrast
-
7/31/2019 MR Pulse Sequences
21/125
DPTR : 2000ms.
TE : 20ms
T2TR : 2000ms. TE : 120ms.
-AT : 4 min. 25 sec.
T1TR : 500ms.
TE :15ms.
AT: 4 min.
Tissue contrastTissue contrast
-
7/31/2019 MR Pulse Sequences
22/125
Effect of TR and TE on MREffect of TR and TE on MRimaging
contrastimaging contrast
Imagingtechnique
TR TE
T1 weighting Short Short
T2 weighting Long Long
Proton-densityweighting
Long Short
-
7/31/2019 MR Pulse Sequences
23/125
Typical TR and TE valuesTypical TR and TE valuesfor SE and
GREfor SE and GRETR (ms) TE (ms)
Sequence Short Long Short Long
SE 250-700>2000 10-20 >60
GRE 100 1-5 >10
-
7/31/2019 MR Pulse Sequences
24/125
Basis SequencesBasis Sequences
Spin-echoSpin-echo Gradient-echoGradient-echo
Inversion-recoveryInversion-recovery Echo-planar imagingEcho-planar
imaging
MR angiographicMR angiographic
-
7/31/2019 MR Pulse Sequences
25/125
SE SequencesSE Sequences
-
7/31/2019 MR Pulse Sequences
26/125
-
7/31/2019 MR Pulse Sequences
27/125
-
7/31/2019 MR Pulse Sequences
28/125
-
7/31/2019 MR Pulse Sequences
29/125
Tissue contrastTissue contrast
T1: AnatomyT1: AnatomyT1 +Gd: PathologyT1 +Gd: Pathology
T2 : PathologyT2 : Pathology Density proton WI: Both Anatomy
andDensity proton WI: Both Anatomy and
PathologyPathology
-
7/31/2019 MR Pulse Sequences
30/125
Hypersignal on T1Hypersignal on T1
Sub-acute Hematome: (MetHb).Sub-acute Hematome: (MetHb).
Fat.Fat.
Artifacts.Artifacts.
Post-hypophyse.Post-hypophyse.
ProteinProtein Melanine (metastase of melanoma).Melanine
(metastase of melanoma).
Manganse.Manganse.
calcifications.calcifications.
-
7/31/2019 MR Pulse Sequences
31/125
The signal intensity ofThe signal intensity ofvarious tissue T1
SEvarious tissue T1 SE
Air, mineral rich tissue (cortical bone, stones), fast
flowing blood
Collagenous tisue (ligament, tendons, scars)
High free water tissue: Kidneys, liver, muscle...
Proteinaceous tissue (abcess, complex
cysts, sylnovial)
Fat, blood products (metHb), slow-flowing blood,
radiation change, contrast agent
-
7/31/2019 MR Pulse Sequences
32/125
The signal intensity ofThe signal intensity ofvarious tissue on
T2 SEvarious tissue on T2 SE
Air, mineral rich tissue, fast-flowing blood
Collagenous tissue, bone islands
Hight bound water tissues (liver, pancreas,adrenals)
Fat, fatty bone marrow
High free water tissue, proteinceous tissue, blood
products
-
7/31/2019 MR Pulse Sequences
33/125
Advances in MR imaging technology haveAdvances in MR imaging
technology have
enabled a reduction in acquisition time withenabled a reduction
in acquisition time withthe use of Fast SE sequencesthe use of Fast
SE sequences
-
7/31/2019 MR Pulse Sequences
34/125
Fast SEFast SE
Echo train
N: Echo train length
-
7/31/2019 MR Pulse Sequences
35/125
SE and Fast SESE and Fast SE
Fast SE: 36s7min 17s
-
7/31/2019 MR Pulse Sequences
36/125
Sequentially increasing the TE of aSequentially increasing the
TE of asequence weights it more heavily towardsequence weights it
more heavily toward
T2:T2:
- MR cholangiopancreatography: Bile ductsMR
cholangiopancreatography: Bile ductsand Pancreatic ductsand
Pancreatic ducts
- MRI: Hemangiomas and CystsMRI: Hemangiomas and Cysts
Fast SEFast SE
-
7/31/2019 MR Pulse Sequences
37/125
Fast SE: T2W (TE= 650)
Fast SE: T2W (TE= 83)Fast SE: T2W (TE= 180)
Hemangiomas or
Cysts
-
7/31/2019 MR Pulse Sequences
38/125
SE and Fast SESE and Fast SESequencesSequences
-
7/31/2019 MR Pulse Sequences
39/125
GRE SequencesGRE Sequences
RF pulse is applied thatRF pulse is applied thatpartly flips the
NMVpartly flips the NMVinto the tranverseinto the tranverseplane
(variable flipplane (variable flip
angle).angle). Gradients, as opposedGradients, as opposedto RF
pulses, are usedto RF pulses, are usedto dephase (negativeto
dephase (negativegradient) and rephasegradient) and rephase
(positive gradient)(positive
gradient)tranversetranversemagnetizationmagnetization
-
7/31/2019 MR Pulse Sequences
40/125
GRE SequenceGRE Sequence
Sensitive to magnetic susceptibility differences between
tissues.
T2*W: (TR : 800ms; TE : 15 ms), 3 min.
-
7/31/2019 MR Pulse Sequences
41/125
GRE SequenceGRE Sequence
HemorrhagicHemorrhagic Pigmented villonodular synovitisPigmented
villonodular synovitis CalcificationCalcification T2* + Gd:
Perfusion studyT2* + Gd: Perfusion study Mapping of human brain
function:Mapping of human brain function:
Blood oxygenation level-dependent imaging:Blood oxygenation
level-dependent imaging:BOLDBOLD
Deoxyhemoglobin in the vasculatureDeoxyhemoglobin in the
vasculature-> Reflection of neuronal activity-> Reflection of
neuronal activity
GRE SequenceGRE Sequence
-
7/31/2019 MR Pulse Sequences
42/125
GRE SequenceGRE SequencePigmented villonodularPigmented
villonodular
synovitissynovitis
Coronal PD FSE, fat
suppression
Coronal T2*-weighted GRE:
Blooming artifact Hemosiderin
-
7/31/2019 MR Pulse Sequences
43/125
GRE SequenceGRE SequencePerfusionPerfusion
-
7/31/2019 MR Pulse Sequences
44/125
GRE SequenceGRE Sequence
Partially Refocused GRE:Partially Refocused GRE:+ MR
angiography+ MR angiography+ Pathology of Internal auditory canal+
Pathology of Internal auditory canal
Fully Refocused GREFully Refocused GRE
- All the gradients are refocused- All the gradients are
refocused--> Signal improvement--> Signal improvementSSFP:
Steady-state free precession:SSFP: Steady-state free
precession:
+ Typical fast+ Typical fast
+ Hight Signal-to-noise ratio+ Hight Signal-to-noise ratio+
Useful for Cardiac imaging, High resolution of IAC :+ Useful for
Cardiac imaging, High resolution of IAC :
Spoiled GRE: T1 + GdSpoiled GRE: T1 + Gd
-
7/31/2019 MR Pulse Sequences
45/125
Oblique sagital T2WSSFP
T1W Spoiled GRE
-
7/31/2019 MR Pulse Sequences
46/125
CISS: State steady interference constructionCISS: State steady
interference construction
- Hight resolution, 3D- Hight resolution, 3D- Acquisition Time:
5min- Acquisition Time: 5min
- Pathology:- Pathology:
+ Cranial nerve: Tumor, neuro-vascular+ Cranial nerve: Tumor,
neuro-vascularconflictconflict
+ Meningo-os fistula+ Meningo-os fistula
GRE SequenceGRE SequenceFully Refocused GREFully Refocused
GRE
CISS/ FIESTACISS/ FIESTA
-
7/31/2019 MR Pulse Sequences
47/125
T2 SE
CISS
-
7/31/2019 MR Pulse Sequences
48/125
-
7/31/2019 MR Pulse Sequences
49/125
CISS TOF 3D
Common names for GRECommon names for GRE
-
7/31/2019 MR Pulse Sequences
50/125
Common names for GRECommon names for GRESequences Used by
MajorSequences Used by Major
VendorsVendors
C ti l I iC ti l I i
-
7/31/2019 MR Pulse Sequences
51/125
Conventional InversionConventional InversionRecoveryRecovery
TI: The interval between the
180 pulse and the 90 pulse
Fluid is dark
C ti l I iC ti l I i
-
7/31/2019 MR Pulse Sequences
52/125
Conventional InversionConventional InversionRecoveryRecovery
STIR: Short TI inversion-recoverySTIR: Short TI
inversion-recovery FLAIR: Fluid attenuated inversion-FLAIR: Fluid
attenuated inversion-
recoveryrecovery TIR (Turbo Inversion Recuperation)
Conventional InversionConventional Inversion
-
7/31/2019 MR Pulse Sequences
53/125
Conventional InversionConventional InversionRecovery
STIRRecovery STIR
Coronal STIRFracture of the distal tibial
Fast SE with spectral fat
suppression
STIR
To null signal from the
Fat : TI 140 msec
TE 140-150 msec
Bone marrow edema
-
7/31/2019 MR Pulse Sequences
54/125
FLAIRFLAIR
To null signal fromthe Fluid
Technics
TR : 8000 ms.TE : 105 ms.
Acquisition time : 3 min
Lung cancer
-
7/31/2019 MR Pulse Sequences
55/125
FLAIR SequenceFLAIR Sequence
-Interest: very sensibility-Interest: very sensibility
+ White matter pathology (SEP,+ White matter pathology
(SEP,Inflammation, infection, tumor,Inflammation, infection,
tumor,vascular).vascular).
+ Epidermoid Kysts.+ Epidermoid Kysts.
- Disadvantage: No specific, artifarctDisadvantage: No specific,
artifarctof flow at the posterior fossaof flow at the posterior
fossa
TIRTIR (T b(Turbo
-
7/31/2019 MR Pulse Sequences
56/125
TIRTIR
(Turbo(TurboInversionInversionRecuperation)Recuperation)-Advantage:
Good-Advantage: Good
contrast white/graycontrast white/graymattermatter
- Application:- Application:
+ Study hippocampe:+ Study hippocampe:(seizure)(seizure)
+ Malformative+ MalformativePathologyPathology (anormal
of(anormal ofneuronal migration,neuronal migration,
Gyration, Heterotopies)Gyration, Heterotopies)
-
7/31/2019 MR Pulse Sequences
57/125
Echo-Planar ImagingEcho-Planar Imaging
A single echo train is used to collectA single echo train is
used to collectdata from all lines of k-space duringdata from all
lines of k-space duringone TR -> shortents the acquisitionone TR
-> shortents the acquisition
timetime 2 types of EPI: SE and GRE2 types of EPI: SE and
GRE
sequencessequences
Technique of choice forTechnique of choice for
+ Diffusion-weighted imaging: EPI SE+ Diffusion-weighted
imaging: EPI SEsequencesequence
+ Cerebral Perfusion Ma netic
-
7/31/2019 MR Pulse Sequences
58/125
EPIEPI
EPI GRE
-
7/31/2019 MR Pulse Sequences
59/125
DWIDWI
To distinguish betweenTo distinguish between+ Rapid diffusion of
protons: unrestriction+ Rapid diffusion of protons:
unrestriction
Diff.Diff.
+ Slow diffusion of protons: restriction Diff.+ Slow diffusion
of protons: restriction Diff.Principle: Either GRE or Fast SE+
Supplement Gradient to dephase:B0, B1000(millitesla/mm2)
+ Gradient to rephase
(equal gradient pulses applied on each side ofthe 180 RF pulse
in EPS)
DWDW
-
7/31/2019 MR Pulse Sequences
60/125
DWDWStrokeStroke
RestrictionHight
signal
intensity
-
7/31/2019 MR Pulse Sequences
61/125
EPI -DWEPI -DWNo net movement:Rephase (-) Hight signal
intensityNet movement: Rephase (+) Signal intensity decrease
Cytotoxique edema, abcess Hyposignal: Fluid, LCR
-
7/31/2019 MR Pulse Sequences
62/125
DW and ADCDW and ADC
Cart ADC: Apparent diffusionCart ADC: Apparent
diffusioncoefficientcoefficient
For the calculation of ADC mapsFor the calculation of ADC
maps
2 sets of images2 sets of images
+ One obtained without application of+ One obtained without
application ofa Diffusion gradient: T2WI or B0a Diffusion gradient:
T2WI or B0
+ One obtained with a diffusion+ One obtained with a
diffusiongradientgradient
-
7/31/2019 MR Pulse Sequences
63/125
Cart ADCCart ADC
Dark and white image : Dark and white image :- ADC decrease
dark, viscosite- ADC decrease dark, viscosite
increase:increase:+ Recent infarction+ Recent infarction
+ Abcess+ Abcess+ Recent hematome+ Recent hematome- ADC
increase, white, mobile fluid:- ADC increase, white, mobile
fluid:
+ LCR+ LCR+ Tumor kysts+ Tumor kysts
Color image:Color image:- ADC decrease = blue- ADC decrease =
blue- ADC increase = red- ADC increase = red
-
7/31/2019 MR Pulse Sequences
64/125
DW and ADCDW and ADC
Whats the purpose?Whats the purpose?
DW and ADCDW and ADC
-
7/31/2019 MR Pulse Sequences
65/125
DW and ADCDW and ADCIschemia ?Ischemia ?
DW ADCDW ADC
-
7/31/2019 MR Pulse Sequences
66/125
DW-ADCDW-ADCIschemiaIschemia
Cytotoxique EdemaCytotoxique EdemaDWI
DW-ADCDW-ADC
-
7/31/2019 MR Pulse Sequences
67/125
Arachnoide and EpidermoideArachnoide and Epidermoide
Kyst ?Kyst ?
DW-ADC
-
7/31/2019 MR Pulse Sequences
68/125
DW ADC
Primary Tumors:Glioblastoma ?
DW ADCDW-ADC
-
7/31/2019 MR Pulse Sequences
69/125
DW-ADCDW-ADCMetastase ?Metastase ?
Metastase: Breast Cancer
DW ADCDW-ADC
-
7/31/2019 MR Pulse Sequences
70/125
DW-ADCDW-ADCMetastase ?Metastase ?
55 years old, man. Metastase bronchal epidermoid carcinome
DW-ADCDW-ADC
-
7/31/2019 MR Pulse Sequences
71/125
DW-ADCDW-ADCAbces ?Abces ?
Rana and al. AJNR 2002
Sensibility +++
Specific: +++
DW-ADCDW-ADC
-
7/31/2019 MR Pulse Sequences
72/125
DW-ADCDW-ADCAbcesAbces
Different Diagnosis:
Metastase: Carcinome epidermoid
Radionecrosis
Hemorrhage in tumor
-
7/31/2019 MR Pulse Sequences
73/125
MR AngiographyMR Angiography
- Exploration of vessel: No invasive- Exploration of vessel: No
invasivetechniquetechnique
- Principle : Creation of contrast- Principle : Creation of
contrast
Blood flow: hypersignalBlood flow: hypersignalSuppression of
stational tissueSuppression of stational tissue
- 4 Principle sequences:- 4 Principle sequences:
+ TOF: Time Of Flight + TOF: Time Of Flight
+ MOTSA: Multiple onerlapping thin-slab+ MOTSA: Multiple
onerlapping thin-slabacquisitionacquisition
+ Contrast-enhanced MRA (Fast GRE 3D+Gd;+ Contrast-enhanced MRA
(Fast GRE 3D+Gd;FISP
MRAMRA
-
7/31/2019 MR Pulse Sequences
74/125
MRAMRATOF and MOTSATOF and MOTSA
Multiple RF pulses applied with shortsMultiple RF pulses applied
with shortsTRs saturate the spin in stationaryTRs saturate the spin
in stationarytissues:tissues:
Suppression of the signal fromSuppression of the signal
fromstationary tissues in the imaging slabstationary tissues in the
imaging slab 2D: section-by-section2D: section-by-section
3D: larger volume3D: larger volume MOTSA: Hybrid result of 2D
and 3DMOTSA: Hybrid result of 2D and 3D
the Thinner slab -> the Lessthe Thinner slab -> the
Lessdeleteriously affected by distaldeleteriously affected by
distal
-
7/31/2019 MR Pulse Sequences
75/125
TOFTOF
GRE: Shorts TR: 40-50msec
Exploration of circulate Flow: Artery or Vein
TOFTOF
-
7/31/2019 MR Pulse Sequences
76/125
TOFTOF- 2D- 2D ::
- Many Acquisitions by continuous coups (Section-by- Many
Acquisitions by continuous coups (Section-bySection)Section)-
Favorage:Favorage:+ Slow flow: Veins, before of severe stenosis.+
Slow flow: Veins, before of severe stenosis.+ Exam for large zone+
Exam for large zone
- 3D- 3D ::- Exam the Volume on only timesExam the Volume on
only times
The volumes acquisition limited 5-10cm.The volumes acquisition
limited 5-10cm.- Precise the anatomy better than 2D.- Precise the
anatomy better than 2D.
- Saturate the slow flow.Saturate the slow flow. Exam the
arteryExam the arteryReconstruction all of the plan:
MIPReconstruction all of the plan: MIPAcquisition time:
7Acquisition time: 7
-
7/31/2019 MR Pulse Sequences
77/125
Original Coup: TOF
-
7/31/2019 MR Pulse Sequences
78/125
MIP Reconstructions
Exam the veins (Dural sinus). Interest:
Thrombophlebite
Bilan extension the veins of Meningioma
-
7/31/2019 MR Pulse Sequences
79/125
Polygone TOFPolygone TOF
Exam the arteries intra-cranial: polygoneExam the arteries
intra-cranial: polygoneof Willisof Willis
- Vascular Malformations:Ane., MAV- Vascular Malformations:Ane.,
MAV- Bilan extension vessel of tumor- Bilan extension vessel of
tumor
- Nervo-vascular conflict (Original- Nervo-vascular conflict
(Original
coups)coups)
Original Coups
-
7/31/2019 MR Pulse Sequences
80/125
Original Coups
-
7/31/2019 MR Pulse Sequences
81/125
MIP Reconstructions
MRAMRA
-
7/31/2019 MR Pulse Sequences
82/125
Contrast-enhanced MRContrast-enhanced MR
angiographyangiographyT1+ Gd: Shorten the T1 of Blood ->T1+
Gd: Shorten the T1 of Blood ->
Hight signal intensity on T1WIHight signal intensity on T1WI
Fast GRE, 3D (Short AcquisitionFast GRE, 3D (Short
Acquisitiontimes:44sec)times:44sec)
Interest: Exploration of cervical vesselsInterest: Exploration
of cervical vesselsfrom their origins to cranial base.from their
origins to cranial base.
Original Coups
-
7/31/2019 MR Pulse Sequences
83/125
Original Coups
MIP Reconstructions
-
7/31/2019 MR Pulse Sequences
84/125
MIP Reconstructions
MRAMRA
-
7/31/2019 MR Pulse Sequences
85/125
MRAMRA
Contrast
MRAMIP on Contrast
MRA
ARM by Phase of ContrastARM by Phase of Contrast
-
7/31/2019 MR Pulse Sequences
86/125
ARM by Phase of ContrastARM by Phase of Contrast
- To dephase of mobile protons, using- To dephase of mobile
protons, usingtwo inverse pole gradients:two inverse pole
gradients:
+ Immobile Protons, dephase and+ Immobile Protons, dephase
andrephage: No signalrephage: No signal
+ Mobile Protons+ Mobile Protons: signal: signal
- The different levels of phase depend on- The different levels
of phase depend onthe velocity of circulated protonthe velocity of
circulated proton
Necessary to select the encode ofNecessary to select the encode
of
potential speed to analyze the vesselpotential speed to analyze
the vessel
MRA by Phase ofMRA by Phase ofCC t t
-
7/31/2019 MR Pulse Sequences
87/125
yyContrastContrast
MRAMRA
-
7/31/2019 MR Pulse Sequences
88/125
MRAMRAPhase-contrast ImagingPhase-contrast Imaging
Providing information about the phaseProviding information about
the phase(direction) and the velocity (magnitude) of(direction) and
the velocity (magnitude) offlowflow
2D and 3D2D and 3D Hight signal: Flow moves fromHight signal:
Flow moves from
RT->LTRT->LT
Sup-> InfSup-> Inf
Ant-> PosAnt-> Pos No signal: Flow moves from:No signal:
Flow moves from:
-
7/31/2019 MR Pulse Sequences
89/125
Phase-contrast
Subclavian steal
Fat-related ImagingFat-related Imaging
-
7/31/2019 MR Pulse Sequences
90/125
Fat related Imagingg gTechniquesTechniques
Fat Signal Suppression: 3 waysFat Signal Suppression: 3 ways
+ RF- uncoherent gradient: MRI +Gd+ RF- uncoherent gradient: MRI
+Gd
+ Inversion-recovery pulse: STIR+ Inversion-recovery pulse:
STIR
+ Water-excitation technique:+ Water-excitation
technique:Spectral-spatial RF pulseSpectral-spatial RF pulse
Fat-related ImagingFat-related ImagingT h iT h i
-
7/31/2019 MR Pulse Sequences
91/125
TechniquesTechniques
STIR
Water excitation
fat suppressionT1 fat suppression
Fat-saturated T1WIFat-saturated T1WI
-
7/31/2019 MR Pulse Sequences
92/125
InterestInterest
- To confirm the fat in the lesion.- To confirm the fat in the
lesion.- Bilan lesions extension to the- Bilan lesions extension to
the
vessel and the space containingvessel and the space
containing
fat:fat:- Arterial dissection- Arterial dissection
Fat saturated T1WIFat saturated T1WI
-
7/31/2019 MR Pulse Sequences
93/125
Lipome
-
7/31/2019 MR Pulse Sequences
94/125
Original 3DTOF.
Fat-saturated T1W images.
In-phase and Out-of-PhaseIn-phase and Out-of-Phase
-
7/31/2019 MR Pulse Sequences
95/125
ppImagingImaging
Different chemical environments of 1H inDifferent chemical
environments of 1H infat ( CH2) and water (H2O)fat ( CH2) and water
(H2O)
Spoiled GRE: Fat and WaterSpoiled GRE: Fat and Water
In-phase: TE =4,2-4,5 msec (1.5 T)In-phase: TE =4,2-4,5 msec
(1.5 T)
Out of phase: TE = 2,1-2,3 msecOut of phase: TE = 2,1-2,3 msec
To depict microscopic fat:To depict microscopic fat:
Adrenal adenomas # Adrenal carcinomasAdrenal adenomas # Adrenal
carcinomas
SteatosisSteatosisFat + -> null on out of phaseFat + ->
null on out of phase
In-phase and Out-of-PhaseIn-phase and Out-of-Phase
-
7/31/2019 MR Pulse Sequences
96/125
ppImagingImaging
T1 W Spoiled GRE: In-phase:
TE= 4.2
T1 W Spoiled GRE: Out of phase:
TE= 2.1
Adrenal adenoma
-
7/31/2019 MR Pulse Sequences
97/125
T1
T2 T1 Fat sat
-
7/31/2019 MR Pulse Sequences
98/125
T1
T2
T1 +Gd
-
7/31/2019 MR Pulse Sequences
99/125
MR SpectroscopyMR Spectroscopy
MR SpectroscopyMR Spectroscopy
-
7/31/2019 MR Pulse Sequences
100/125
MR SpectroscopyMR Spectroscopy
MRS provides a measure of Brain chemistry:MRS provides a measure
of Brain chemistry:
1H, 23Na; 31P: (1H higher signal-to-noise)1H, 23Na; 31P: (1H
higher signal-to-noise)
Each metabolite appears at a specific ppm, andEach metabolite
appears at a specific ppm, andeach one reflects specific cellular
and biochemicaleach one reflects specific cellular and
biochemicalprocessesprocesses
Biochemical changes in Tumors, Stroke, Epilepsy,Biochemical
changes in Tumors, Stroke, Epilepsy,Metabolic disorders, Infections
andMetabolic disorders, Infections and
Neurodegenerative diseasesNeurodegenerative diseases
Interpretation: MRI and MRSInterpretation: MRI and MRS
(ppm: Parts per millions)
-
7/31/2019 MR Pulse Sequences
101/125
Observable Proton Metabolites
0.9-1.4 Lipids Products of brain destruction
1.3 Lactate Product of anaerobic glycolysis
2.0 NAA Neuronal marker
2.2-2.4 Glutamine/GABA Neurotransmitters
3.0 Creatine Energy metabolism
3.2 Choline Cell membrane marker
3.5 myo-inositol Glial cell marker, osmolyte
hormone receptor mechanisms
1.2 Ethanol Triplet
1.48 Alanine Present in meningiomas
3.4&3.8 Glucose Increased in diabetes
3.8 Mannitol Rx for increased ICP
ppm Metabolite Properties
-
7/31/2019 MR Pulse Sequences
102/125
NAA: Decreases with any disease thatNAA: Decreases with any
disease thatadversely affects neuronal integ-rityadversely affects
neuronal integ-rity
Creatine provides a measure of energyCreatine provides a measure
of energy
storesstores Choline: measure of increased cellularCholine:
measure of increased cellular
turnoverturnover
Elevate in tumors,Elevate in tumors,
Inflammatory processesInflammatory processes Myoinositol:
located primarily in astrocytesMyoinositol: located primarily in
astrocytes
Increased in hypernatremia, in tubers andIncreased in
hypernatremia, in tubers and
Alzeimer D.Alzeimer D.
Basis physical PrinciplesBasis physical Principles
-
7/31/2019 MR Pulse Sequences
103/125
Basis physical PrinciplesBasis physical Principles
The resonant frequencies of Protons:The resonant frequencies of
Protons:
10MHz at 0.3 T10MHz at 0.3 T
300MHz at 7 T300MHz at 7 T
63-64 MHZ at 1.5 T63-64 MHZ at 1.5 T
Higher field strength, Higher signal-to-Higher field strength,
Higher signal-to-noise and better separation of thenoise and better
separation of themetabolite peaksmetabolite peaks
-
7/31/2019 MR Pulse Sequences
104/125
Study the biochemical structure of theStudy the biochemical
structure of thedisovle molecule in the waterdisovle molecule in
the water
Aanalyze the character of chemicalAanalyze the character of
chemicalmovement of the molecules aftermovement of the molecules
aftersuppression the signal of water bysuppression the signal of
water by
supplemental magnetique fieldsupplemental magnetique field
-
7/31/2019 MR Pulse Sequences
105/125
Water and Fat is suppressed by:Water and Fat is suppressed
by:Technics:Technics:
CHESS (CHEmical-Shift Selective)CHESS (CHEmical-Shift
Selective)IR (Inversion Recorvery)IR (Inversion Recorvery)
STEAM or PRESS pulse sequenceSTEAM or PRESS pulse
sequence(Stimulated Echo Acquisition Mode): Refocuses(Stimulated
Echo Acquisition Mode): Refocuses
9090(Point Resolved SpectroScopy): Refocuses 180(Point Resolved
SpectroScopy): Refocuses 180
CSI (Chemical Shift Imaging) refers to multi-voxelCSI (Chemical
Shift Imaging) refers to multi-voxelMRSMRS
SI (Spectroscopic Imaging) displays the dataSI (Spectroscopic
Imaging) displays the datadepending on the concentration of a
particulardepending on the concentration of a particular
metabolitemetabolite
PRESS (pointPRESS (point STEAMSTEAM
( i l d h( ti l t d h
-
7/31/2019 MR Pulse Sequences
106/125
(p(presolvedresolvedspectroscopy)spectroscopy)
Double spin-echoDouble spin-echotechniquetechnique
Subject to T2 lossSubject to T2 loss
(stimulated echo(stimulated echoacquisitionacquisition
mode):mode): Can use shorterCan use shorter
TE, allow to seeTE, allow to seemore metabolitesmore
metabolites
such assuch asmyoinositolmyoinositol
Less SNR thanLess SNR thanPRESSPRESS
SETTING UP MRSETTING UP MR
-
7/31/2019 MR Pulse Sequences
107/125
SPECTROSCOPYSPECTROSCOPY Choose the right sequenceChoose the
right sequence+ Homogeneous lesion: single voxel+ Homogeneous
lesion: single voxel
+ Heterogeneous lesion (ring-enhancing,+ Heterogeneous lesion
(ring-enhancing,
edema): multivoxeledema): multivoxel Choose the volume (4-8
cmChoose the volume (4-8 cm33)) Avoid skull, sinus, fat, blood
products,Avoid skull, sinus, fat, blood products,
vasogenic edema, water, foreign bodies andvasogenic edema,
water, foreign bodies andradioactive seedsradioactive seeds
-
7/31/2019 MR Pulse Sequences
108/125
Short TE of 30msec: Metabolites withShort TE of 30msec:
Metabolites withboth short and long T2 relaxationboth short and
long T2 relaxationtimes are observed:times are observed:
Long TE of 270 msec, onlyLong TE of 270 msec, onlymetabolites
with a long T2 are seen:metabolites with a long T2 are seen:NAA,
Creatinin and CholineNAA, Creatinin and Choline
TE of 144 msec: Lactate at 1.3 ppmTE of 144 msec: Lactate at 1.3
ppm
Normal MR Spectrum2
http://www.ajnr.org/content/vol21/issue9/images/large/ajnr-21-09-04-f01.jpeg
-
7/31/2019 MR Pulse Sequences
109/125
1
WM
1
2
GM
Huntersangle
Hunters Angle:
NAA/Cr, NAA/Cho, and Cho/Cr
Normal Abnormal
NAA/Cr 2.0 < 1.6
NAA/Cho 1.6 < 1.2
Cho/Cr 1.2 > 1.5
MRSMRSBrain Tumors: Degree ofBrain Tumors: Degree of
http://www.ajnr.org/content/vol21/issue9/images/large/ajnr-21-09-04-f01.jpeg
-
7/31/2019 MR Pulse Sequences
110/125
Brain Tumors: Degree ofBrain Tumors: Degree
ofMalignancyMalignancy
Malignancy increases:Malignancy increases: NAA and Creatine
decreaseNAA and Creatine decrease
+ Displaces or destroys neurons+ Displaces or destroys neurons+
Very malignancy: Hight metabolic activity+ Very malignancy: Hight
metabolic activity
and deplete the energy stores -> Reduceand deplete the energy
stores -> ReduceCreatineCreatine
Choline, Lactate and Lipid increaseCholine, Lactate and Lipid
increase+ Very hypercellular tumors with rapid growth+ Very
hypercellular tumors with rapid growth
elevate the Cholin levelselevate the Cholin levels+ Lipid: in
necrotic portions of tumors+ Lipid: in necrotic portions of tumors+
Lactats appears when tumors out grow their+ Lactats appears when
tumors out grow theirblood supply and start ultilizing
anaerobicblood supply and start ultilizing anaerobic
glycosisglycosis
MRSMRS
-
7/31/2019 MR Pulse Sequences
111/125
GliomblastomaGliomblastoma
Elevation of Cho and Decrease NAA
Lactat doublet
Glial tumor or Non-glialGlial tumor or Non-glial
-
7/31/2019 MR Pulse Sequences
112/125
tumorstumors
Gliomas: Elevation of Cholin beyond the margin ofGliomas:
Elevation of Cholin beyond the margin ofenhancementenhancement
High grade astrocytoma # metastasis: the presence ofHigh grade
astrocytoma # metastasis: the presence ofhigh choline in the
peritumoral region.high choline in the peritumoral region.
Non glial tumors: Have little or no NAANon glial tumors: Have
little or no NAA Meningoma: Elevation of Alanine at
1.48ppm:Meningoma: Elevation of Alanine at 1.48ppm: PNET or
medulloblastomas have higher elevations ofPNET or medulloblastomas
have higher elevations of
Choline than astrocytomaCholine than astrocytoma Lymphomas have
higher elevated lipids compared toLymphomas have higher elevated
lipids compared to
GBM.GBM. Craniopharyngiomas have a peak in the
lactate-lipidCraniopharyngiomas have a peak in the
lactate-lipid
range.range.
Tumor recurrence after RadiTumor recurrence after Radi
-
7/31/2019 MR Pulse Sequences
113/125
or Sur.or Sur.
Elevated cholin is a marker forElevated cholin is a marker
forrecurrent tumorrecurrent tumor
Radiation change generally exhibits lowRadiation change
generally exhibits low
NAA, Creatine and Cholin onNAA, Creatine and Cholin
onSpectroscopySpectroscopy
If radiation necrosis is present, theIf radiation necrosis is
present, the
spectrum may reveal elevated lipidsspectrum may reveal elevated
lipidsand lactateand lactate
TUMOR VS RADIATIONTUMOR VS RADIATION
-
7/31/2019 MR Pulse Sequences
114/125
NECROSISNECROSIS Radiation necrosis have high lactateRadiation
necrosis have high lactate
and lipids (which may be also foundand lipids (which may be also
foundafter radiotherapy)after radiotherapy)
MRSMRSh i d f i
http://www.ajnr.org/content/vol21/issue2/images/large/ajnr-21-02-13-f02.jpeg
-
7/31/2019 MR Pulse Sequences
115/125
Ischemia and InfectionIschemia and Infection
IschemiaIschemia
+ Anaerobic glycosis and lactate accumulates -> Hight+
Anaerobic glycosis and lactate accumulates ->
HightLactateLactate
+ Infarction: Lipid increase+ Infarction: Lipid increase Brain
abcesses destroy or displace brain tissueBrain abcesses destroy or
displace brain tissue
+ NAA: not present+ NAA: not present
+ Bacterial abcesses: Lactate, cytosolic acid, alanine+
Bacterial abcesses: Lactate, cytosolic acid, alanine
and Acetateand Acetate+ Toxoplasmosis and Tuberculomas:
Prominent peaks+ Toxoplasmosis and Tuberculomas: Prominent
peaksfrom Lactate and Lipidsfrom Lactate and Lipids
Infections DiseasesInfections Diseases
-
7/31/2019 MR Pulse Sequences
116/125
Infections DiseasesInfections Diseases
Brain abcesses destroy or displaceBrain abcesses destroy or
displacebrain tissuebrain tissue
NAA: not presentNAA: not present
Bacterial abcesses: Lactate, cytosolicBacterial abcesses:
Lactate, cytosolicacid, alanine and Acetateacid, alanine and
Acetate
Toxoplasmosis and Tuberculomas:Toxoplasmosis and
Tuberculomas:
Prominent peaks from Lactate andProminent peaks from Lactate
andLipidsLipids
-
7/31/2019 MR Pulse Sequences
117/125
-
7/31/2019 MR Pulse Sequences
118/125
How about protocols MRIHow about protocols MRI
for each disease ?for each disease ?
-
7/31/2019 MR Pulse Sequences
119/125
Thank you for yourThank you for yourattentions!attentions!
-
7/31/2019 MR Pulse Sequences
120/125
Protocol dIRM dansProtocol dIRM dansl ti h ll ti h l
-
7/31/2019 MR Pulse Sequences
121/125
exploration encphaleexploration encphale
Standard: T1 sagitalStandard: T1 sagitalT2 axialT2 axial
Flaire axialFlaire axial
Comitialit : T1 sag-T1 Stir CoronalComitialit : T1 sag-T1 Stir
Coronal
T2* axialT2* axial
Flaire coronalFlaire coronal+/- T1 axial ou coronal+/- T1 axial
ou coronal
avec Gdavec Gd
Protocol dIRM dansProtocol dIRM dansl ti h ll ti h l
-
7/31/2019 MR Pulse Sequences
122/125
exploration encphaleexploration encphale
Dmence: T1 sag-T1 Stir coronalDmence: T1 sag-T1 Stir
coronal(hippo)(hippo)
Flaire axialFlaire axial
T1 axial GdT1 axial Gd Hypophyse: T1 sag et coronalHypophyse: T1
sag et coronal
T1 sag et coronal avecT1 sag et coronal avec
GdGdT2 coronalT2 coronal
ARM post Embolisation: T2 axialARM post Embolisation: T2
axial
TOFTOF
Protocol dIRM dansProtocol dIRM dansl ti h ll ti h l
-
7/31/2019 MR Pulse Sequences
123/125
exploration encphaleexploration encphale Surdit rtrocochlaires,
VertigesSurdit rtrocochlaires, Vertiges
T1 sagT1 sagT2 axial coupes fines encphalesT2 axial coupes fines
encphalesCISS 3D axialCISS 3D axialT1 axial FS pre et post GdT1
axial FS pre et post Gd
+/-Coro+/-Coro Controle Neurinome de lacoustique non oprControle
Neurinome de lacoustique non opr
T1 Gd axial et coro : VolumeT1 Gd axial et coro : VolumeT2
axialT2 axial
Controle Neurinome oprControle Neurinome oprT1 pre et post Gd
FST1 pre et post Gd FST2 axialT2 axial
Protocol dIRM dansProtocol dIRM dansl ti h ll ti h l
-
7/31/2019 MR Pulse Sequences
124/125
exploration encphaleexploration encphale
Orbites: T1 PNOOrbites: T1 PNOT2 PNOT2 PNO
T2 coro StirT2 coro Stir
+/-T1 avec Gd FS+/-T1 avec Gd FS
Conflit Vasculo-nerveuxConflit Vasculo-nerveux
T1 sagT1 sag
T2 axial coupes fines encphalesT2 axial coupes fines
encphales
CISS 3D axialCISS 3D axialTOF PolygoneTOF Polygone
ArtifactArtifact
-
7/31/2019 MR Pulse Sequences
125/125
ArtifactArtifact