Embed Size (px)
Citation preview
Vascular Graft InfectionsInfected Prosthetic Graft
Mr P SomaiyaMr P SomaiyaMr P SomaiyaSpecialist Registrar, General
Mr P SomaiyaSpecialist Registrar, General
Surgery, London DeanerySurgery, London Deanery
Part OnePart OnePart OneVascular Graft Infections
Part OneVascular Graft Infections
HistoryHistoryHistoryHistory• the history of vascular grafts is closelythe history of vascular grafts is closely
linked to popliteal aneurysms and was influenced by Alexis Carrel’s publishedinfluenced by Alexis Carrel s published work in 1902
• the first vascular grafts were done as follows:Goyanes – 1906 – popliteal vein was used in situ to replaced a popliteal aneurysmin situ to replaced a popliteal aneurysm Enderlen – 1907 – end to end anastamosisPringle 1913 reversed saphenous vein
HistoryHistoryHistoryHistory• the Korean War influenced emergence ofthe Korean War influenced emergence of
reconstructive surgery for arterial injuries initiated by Schumaker and reported byinitiated by Schumaker and reported by Hughes and Bowers – 1952
• Voorhees also in 1952 reported his initial work in dogs using Vinyon-N cloths to g g ybridge arterial defects.
• work done by DeBakey in the 1950 ‘s and• work done by DeBakey in the 1950 s and 1960’s firmly established the use of Dacron grafts for arterial reconstruction
• 1970’s saw the introduction of ePTFE
UsesUsesUsesUses• for bridging of arterial defects openfor bridging of arterial defects open
vascular surgery in the following forms:t b ft- tube grafts
- trouser graftsg- patch repair of arteries
i t l b t i• as internal by-pass systems in endovascular surgery in the following forms:
- covered stents for peripheral arteries- covered stents for peripheral arteries- EVAR stents for aorta
TypesTypesTypesTypes• natural materials:natural materials:
- autologous:in-situin situreversed
- homologous – human umbilical vein (HUV)- heterologous – bovine or porcine patches- heterologous – bovine or porcine patches - genetically engineered tissue grafts
TypesTypesTypesTypes• prosthetic:prosthetic:
- Dacronwovenwovenknitted
- ePTFE or Teflon(both can come with and without external(both can come with and without external
support)• hybrid
when to choose what?when to choose what?when to choose what?when to choose what?• prosthetic: • natural:
- medium to large vessel reconstruction
- small vessel reconstructionvessel reconstruction
- extra-anatomic reconstruction
reconstruction
anatomicreconstruction- absence of natural
materials
- anatomic reconstruction
materials- suprageniculate
- presence of infection- infrageniculate
bypasses- patch repair of
bypasses- cuffs in hybrid grafts

what can go wrong?what can go wrong?what can go wrong?what can go wrong?
• re-stenosis• thrombosisthrombosis• graft infections
the general rule is try and use autologousthe general rule is try and use autologous materials if possible, especially when doing reconstr ction after infection and fordoing reconstruction after infection and for infra-geniculate by passes.
graft infections a few factsgraft infections a few factsgraft infections-a few factsgraft infections-a few facts
• size of the problem:varies from 1-5% dependant on graft sizevaries from 1 5% dependant on graft size and patient populationit i hi h t f i f i i l bit is highest for infra-inguinal bypasses with rates of upto 12% reported in some studiesaorto-femoral and aortic repairs areaorto-femoral and aortic repairs are associated with lower graft infection rates f 1 2%of approx. 1-2%
graft infections a few factsgraft infections a few factsgraft infections-a few factsgraft infections-a few facts
• causes:most of the graft infections occur at themost of the graft infections occur at the time of surgery. Breakdown of sterility is the commonest cause of graft infectionthe commonest cause of graft infection. Other causes include presence of pre-existing aneurysms (mycotic aneurysms), extension from superficial woundextension from superficial wound infections and a haematogenous spread
graft infections a few factsgraft infections a few factsgraft infections-a few factsgraft infections-a few facts
• causes:Operative factors include:Operative factors include:- Reoperation during same hospital
d i iadmission- Preoperative shavingeope at e s a g- Open surgical drainage for more than 3
da sdays- Operations > 2 hoursp- Emergency surgery
IV li

graft infections a few factsgraft infections a few factsgraft infections-a few factsgraft infections-a few facts
• causes:Patient factors include:Patient factors include:- age, - obesity, - diabetes- diabetes, - steroid treatment and - wound hematoma
microbes involvedmicrobes involvedmicrobes involvedmicrobes involved
• Staphylococci are the commonest organisms isolated from graft wound g ginfections; S. aureus is most common in early graft infections while coagulaseearly graft infections while coagulase negative Staphylococci are prevalent in late infectionslate infections.
• Gram negative organisms and anaerobes are the next in line of organisms beingare the next in line of organisms being isolated.

graft infections a few factsgraft infections a few factsgraft infections-a few factsgraft infections-a few facts
• many suspected graft infections are t t d ith t k i id tittreated without knowing identity or antimicrobial susceptibilities of the causative organismscausative organisms
• this is due to suitable specimens not being p gobtained or because antibiotic treatment was instituted before collection of
i t l f ltappropriate samples for culture.
graft infections a few factsgraft infections a few factsgraft infections-a few factsgraft infections-a few facts
• once infected a prosthesis acts as a foreign bodyg y
d b t i i bl t Ab• renders bacteria inaccessable to Abx
• vein grafts are more resistant to bacterial erosion especiall if e posed in an openerosion especially if exposed in an open wound

diagnosis of graft infectiondiagnosis of graft infectiondiagnosis of graft infectiondiagnosis of graft infection
• clinical findings• radiologyradiology• microbiological tests
Clinical manifestations of graft infectionClinical manifestations of graft infection vary according to length of time that has elapsed since proced reelapsed since procedure.
clinical findings for diagnosisclinical findings for diagnosisclinical findings for diagnosisclinical findings for diagnosis
l tearly onset:
• occur within 4 months of surgery• systemically toxic with fever and• systemically toxic with fever and
leucocytosisf• bloodstream infection
• wound infection• graft dysfunction from thrombosis or
anastamotic bleeding may occuranastamotic bleeding may occur

clinical findings for diagnosisclinical findings for diagnosisclinical findings for diagnosisclinical findings for diagnosis
l t tlate onset:
• occur more than 4 months after surgery• tend to be more subtle non specific• tend to be more subtle – non-specific
signs and symptomsf f• fever usually absent often presenting with complications
• false aneurysm• osteomyelitis or nonhealing ulcers in distalosteomyelitis or nonhealing ulcers in distal
tissues
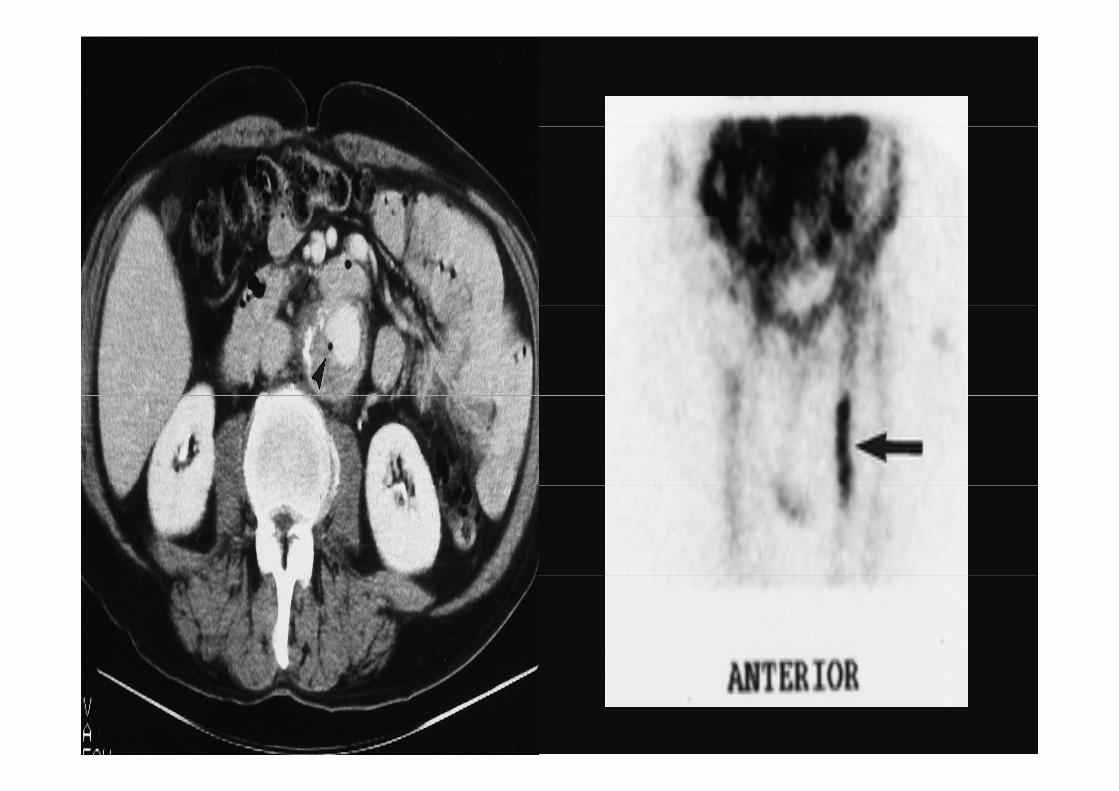
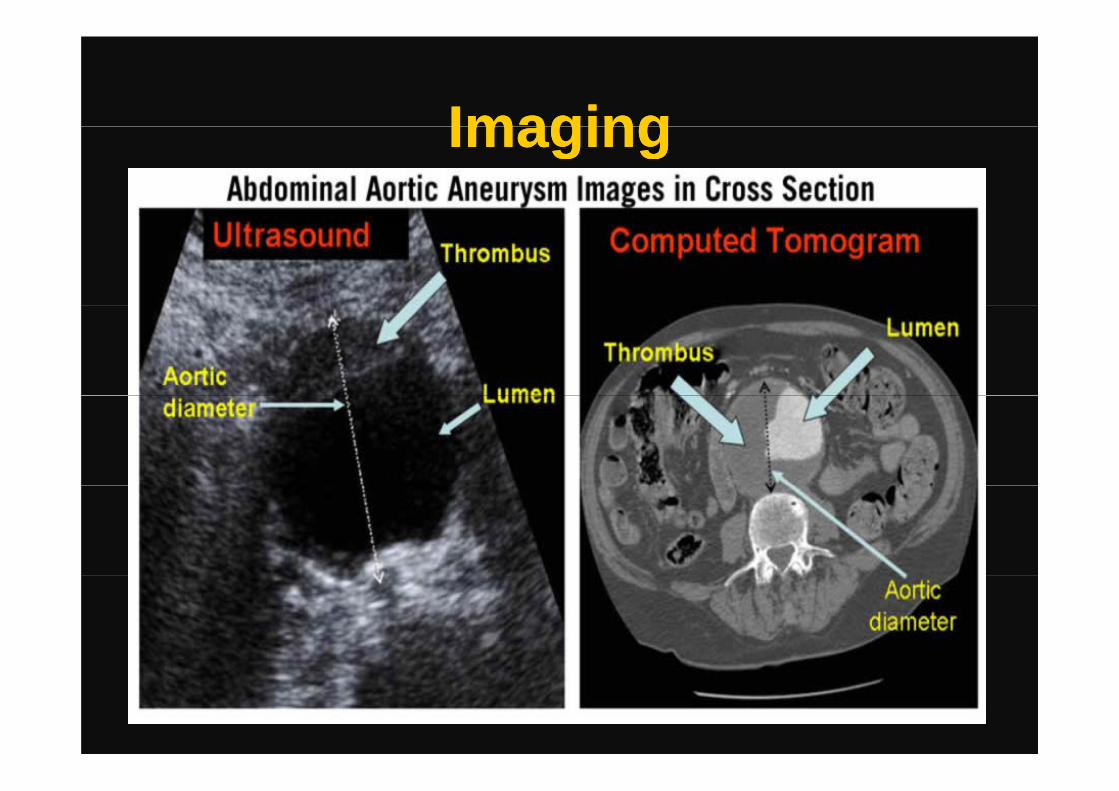
imaging modalities used for imaging modalities used for diagnosisdiagnosis
• CT scanning: preferred imaging modalityCT scanning: preferred imaging modality for diagnosis of graft infectionsMRI t t b l t d• MRI: yet to be evaluated
• Technetium -99m-hexametazime-labelled ec et u 99 e a eta e abe edleucocyte scanning (sensitivity up to 100%)100%)
• Sinography – determines whether a draining sinus extends to the graft -diagnostic of graft infection
microbiological aids to microbiological aids to diagnosisdiagnosis
l t d ft ti• explanted graft tissue • aspirated material from peri-graft collectionp p g• blood cultures often negative – especially
late onset infectionslate onset infections• contamination – organisms from overlying
wounds/ sinuses eg MRSAwounds/ sinuses – eg MRSA • postpone ABx in non-critically ill patient
until cultures taken

Treatment optionsTreatment optionsTreatment optionsTreatment optionstreatment options are usually divided intotreatment options are usually divided into
the following:
• Medical Therapy and IrrigationMedical Therapy and Irrigation
• Surgical Treatment
surgical treatment is considered the gold t d d f t f lstandard for management of vascular
graft infections
Treatment optionsTreatment optionsTreatment optionsTreatment optionsSurgical treatment options:Surgical treatment options:- 1 stage extra anatomic bypass(axillo-
bif b )bifem by-pass)- 2 stage extra anatomic bypass(axillo-2 stage extra anatomic bypass(axillo
bifem by-pass)A t ti l i it b- Autogenous native vessel in-situ bypass (aorto-iliac reconstruction)
- Homograft vessel in-situ bypass (aorto-iliac reconstruction)iliac reconstruction)
- Prosthetic drug impregnated in-situ b ( t ili t ti )
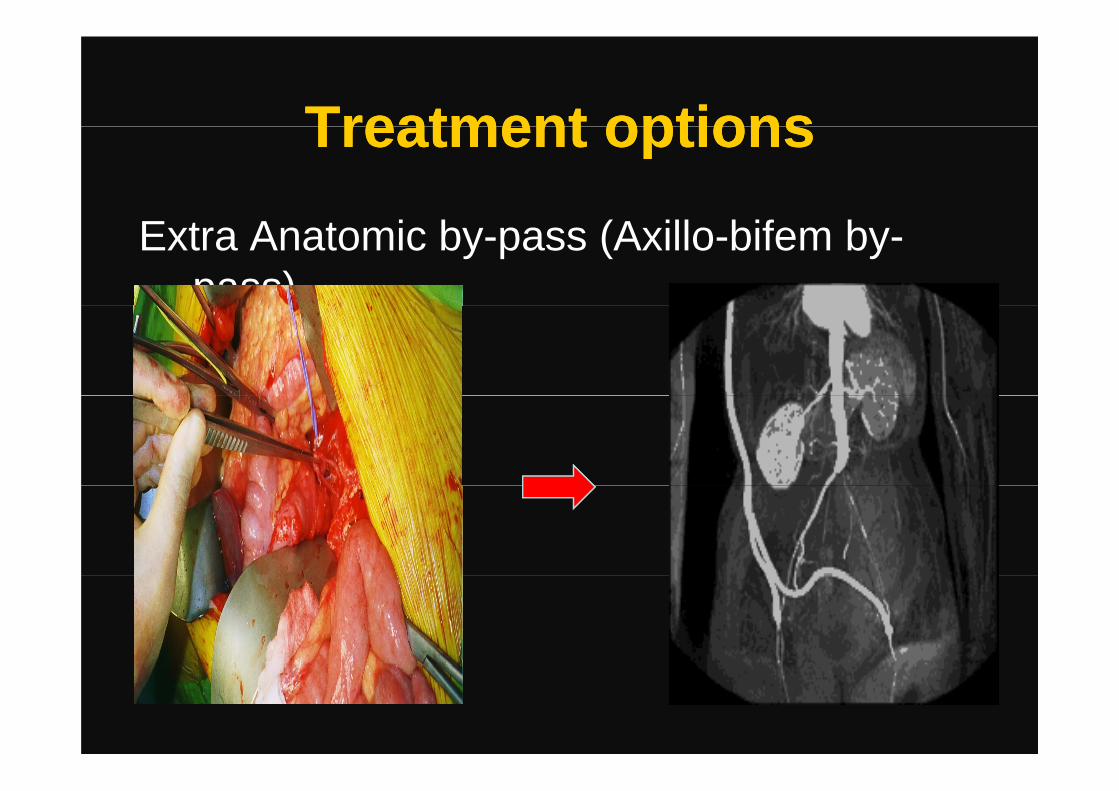
Treatment optionsTreatment optionsTreatment optionsTreatment options
Extra Anatomic by-pass (Axillo-bifem by-pass)p )
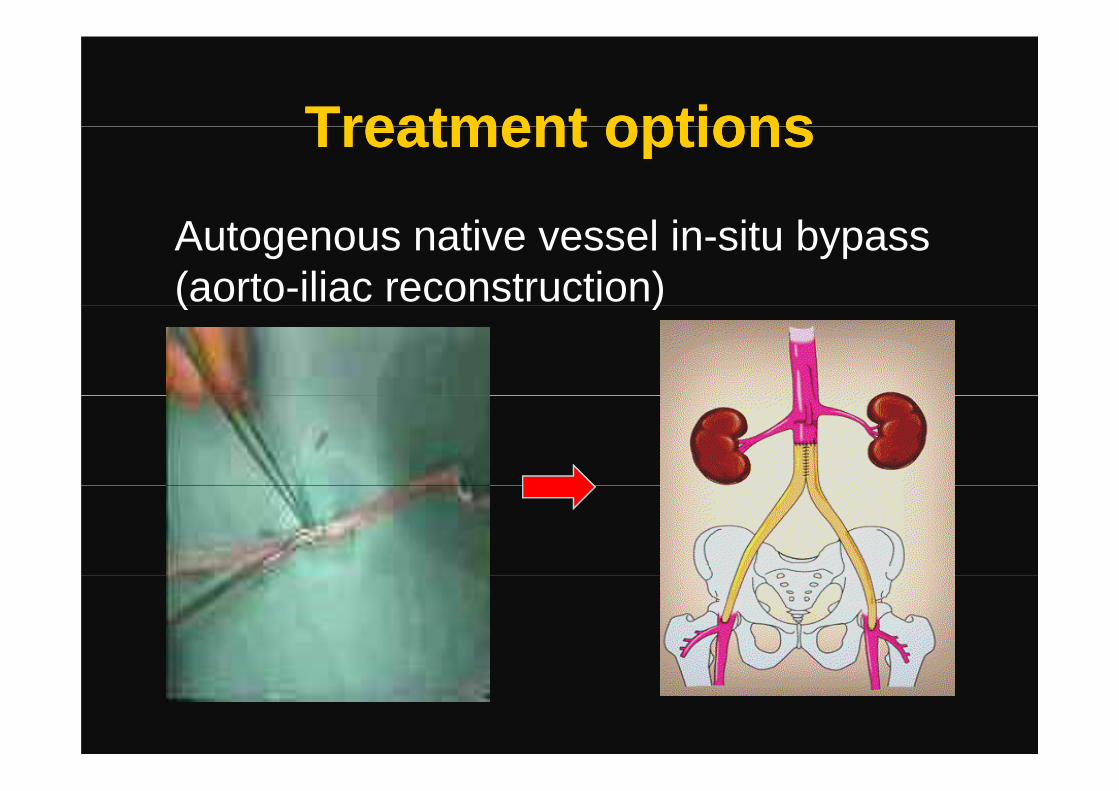
Treatment optionsTreatment optionsTreatment optionsTreatment options
Autogenous native vessel in-situ bypass (aorto-iliac reconstruction)( )

Treatment optionsTreatment optionsTreatment optionsTreatment options
Homogenous vessel in-situ b ( t ilibypass (aorto-iliac reconstruction)
In Jan ’05 the VSGBI inIn Jan. 05 the VSGBI in collaboration with the National Blood Service drew up a plan to develop p p pthe National Arterial Tissue bank(NATB)

Part TwoPart TwoPart TwoInfected Prosthetic Graft
Part TwoInfected Prosthetic Graft

Patient HistoryPatient HistoryPatient HistoryPatient History• 69yrs of age investigated for severe left69yrs of age investigated for severe left
hip painE k 40 k hi t• Ex-smoker – 40 pack year history
• Security guardy g• Past History: HT,IHD, CABG,
HypercholesterolemiaHypercholesterolemia• Investigation done: X-ray pelvis (AAA
found)USS abdomen-12cmUSS abdomen-12cm
aneurysm di d
ImagingImagingImagingImaging
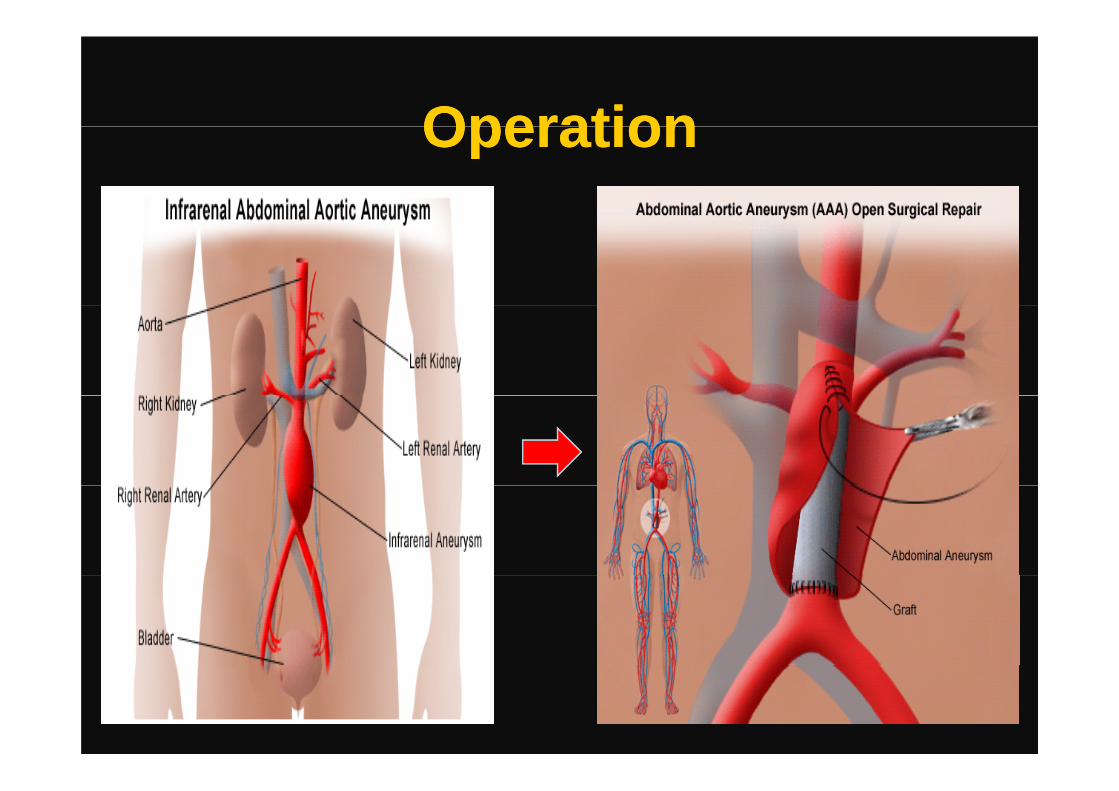
OperationOperationOperationOperation
Post operationPost operationPost operationPost operation
• Unremarkable recovery, discharged on day 5y
• 6/52 follow up normal.R t ti t GP ith• Re-presentation to GP with pyrexia(39.5C), rigors, night sweats. Rx: Amoxicillin (PO) followed by Ciprofloxacin (PO)(PO)
• Presented to A&E with peri-umblical pain, i (37 7)pyrexia(37.7),
WCC:15.5(Neutrophils:12.13), CRP:182
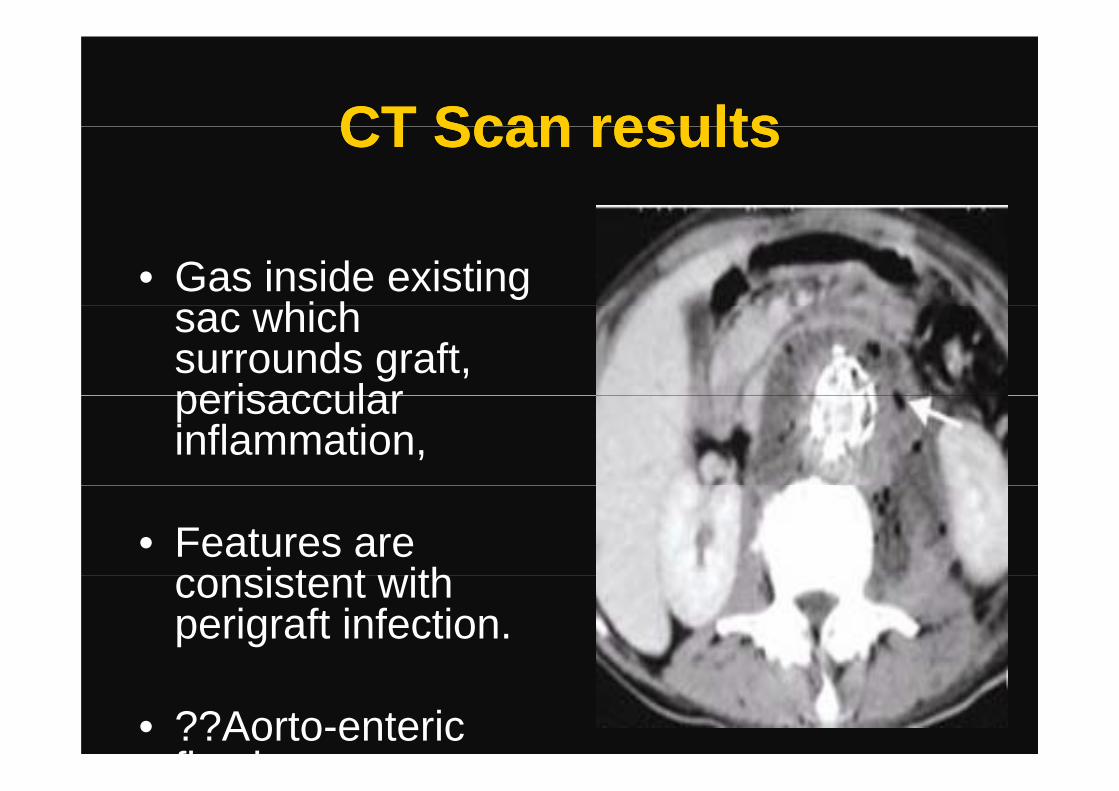
CT Scan resultsCT Scan resultsCT Scan resultsCT Scan results
• Gas inside existing hi hsac which
surrounds graft, perisaccularperisaccular inflammation,
• Features are consistent ithconsistent with perigraft infection.
• ??Aorto-enteric fi t l
CausesCausesCausesCauses
What are the commonest causes of graft infections?
A)Breakdown of sterility
B)Patient factors) at e t acto s
C)Operative factors

Microbes involvedMicrobes involvedMicrobes involvedMicrobes involved
Which is the commonest organism involved?
A)Gram negative organisms + Anaerobes
B)StaphylococciB)Staphylococci
A)Polymicrobial (including fungi)

Our patient’s microbial profileOur patient’s microbial profileOur patient s microbial profileOur patient s microbial profile
• Gram +ve rods and cocci from aortic tissue and pus.p
St t ill i iti t i illi• Streptococcus milleri sensitive to penicillin and vancomycin.
Treatment optionsTreatment optionsTreatment optionsTreatment optionsWhat is the best treatment option for thisWhat is the best treatment option for this
patient?
A) Medical Therapy and IrrigationA) Medical Therapy and Irrigation
A) SurgicalA) Surgical

Treatment optionsTreatment optionsTreatment optionsTreatment optionsSurgical treatment:Surgical treatment:A) 1 stage extra anatomic bypass(axillo-
bif b )bifem by-pass)B) 2 stage extra anatomic bypass(axillo-B) 2 stage extra anatomic bypass(axillo
bifem by-pass)C) A t ti l i it bC) Autogenous native vessel in-situ bypass
(aorto-iliac reconstruction)D) Homograft vessel in-situ bypass (aorto-
iliac reconstruction)iliac reconstruction)E) Prosthetic drug impregnated in-situ
b ( t ili t ti )
Treatment given to our patientTreatment given to our patientTreatment given to our patientTreatment given to our patient
• Autogenous native vessel in-situ bypass (aorto-iliac reconstruction)( )
A t i d f t ti• Autogenous vein used for reconstruction was the superficial femoral vein.
An graft enteric connection as also• An graft-enteric connection was also repaired.
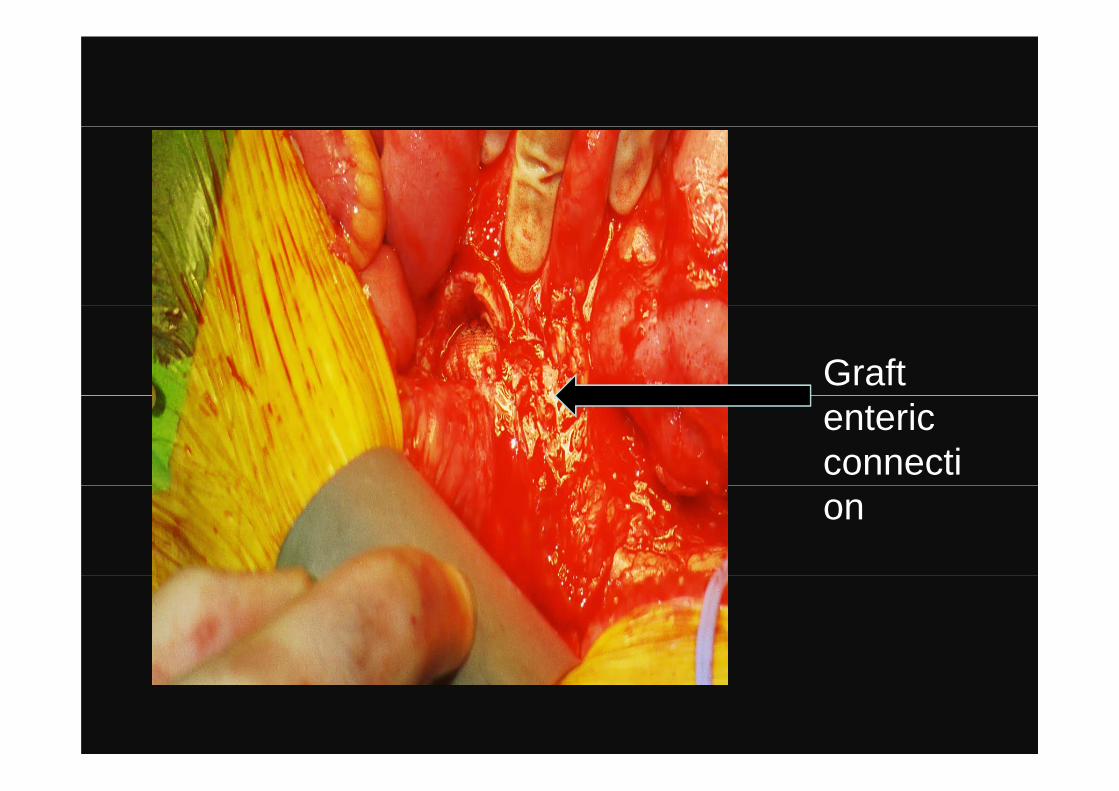
Graft enteric connection
Th k Y !Th k Y !Thank You!Thank You!Acknowledgements to the three women
who have influenced me in my life:yMy Mum
P f H V i i kProf. Homer-VanniasinkamProf. Val Edwards-Jones