Embed Size (px)
Citation preview

Nose and Sinus
Mr Christopher Brown ENT Surgeon
RVEEH
March 2020

Overview Anatomy Physiology Common conditions sinusitis fungal disorders epistaxis trauma nasal polyps rhinitis deviated septum hyposmia Future directions

Anatomy

Anatomy

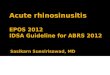
Anatomy 4 sinuses •Frontal •Maxillary •Ethmoid •Sphenoid
Frontal
Ethmoid OMC – osteomeatal complex
(middle meatus)
Maxillary
Sphenoid

Physiology Mucus is transported out of the sinuses through natural openings Blockage of these openings can lead to sinusitis

Physiology Mucociliary clearance – functioning cilia Innate immunity - lysozymes Cellular immunity
– pmns, lymphocytes

Sinusitis Definintion • Inflammatory response involving the mucous
membranes of the nasal cavity and paranasal sinuses Correct term actually rhinosinusitis

Sinusitis Acute rhinosinusitis < 4 weeks Chronic rhinosinusitis (CRS) > 12 weeks

Aetiology of CRS Predisposing factors • Viral URTI - 1-2 % develop sinusitis • Bacterial infections
Streptococcus pneumonia Hemophilus influenza Moraxella catarrhalis Staphylococcus aureus
• Bacterial biofilms and superantigens • Allergic rhinitis • Immunodeficiencies • Smoking • Mucociliary disorders – cystic fibrosis • Anatomical factors • Nasal polyps
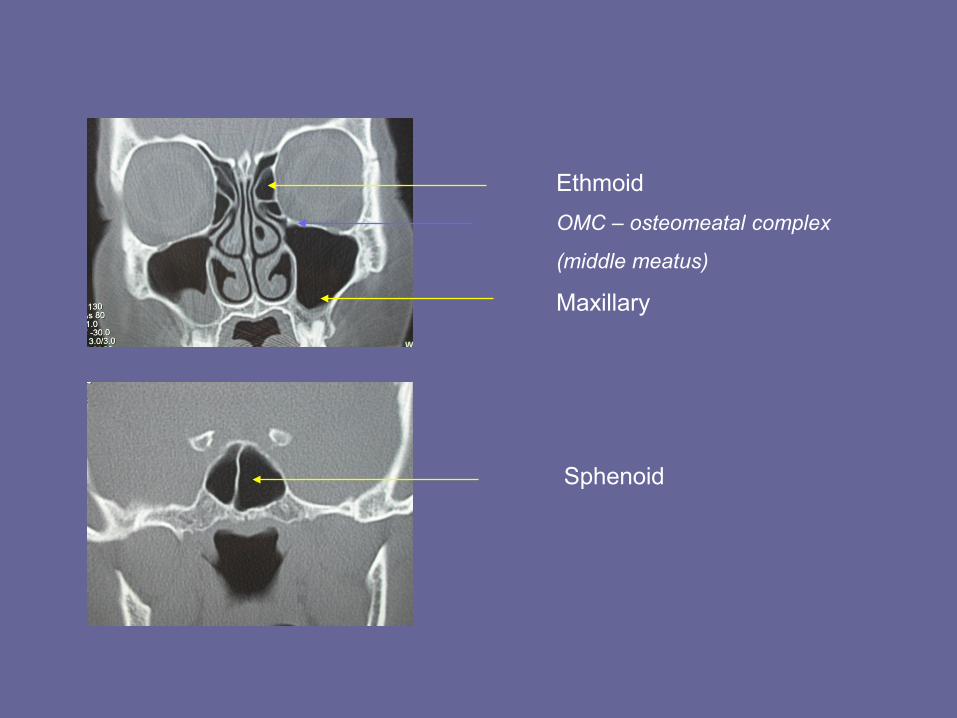
Aetiology of CRS Biofilms
Bacteria in polysaccharide matrix
• evade host defenses
Antibiotics ineffective
Forging a link between biofilms and disease Science 1999: 283; 1837-1839 Potera Bacterial biofilms in surgical specimens of patients with chronic rhinosinusits Sanclement et al Laryngoscope 2005: 115 April

Aetiology of CRS Superantigens S.aureus IgE to staphylococcal and streptococcal toxins in patients with chronic sinusitis / nasal polyps Laryngoscope; 2004
Pathogenesis
Ostial obstruction Inflammation
Bacterial infection


Symptoms The symptoms of CRS are varied, and include the following: • facial pressure/pain/congestion/fullness • nasal obstruction/blockage • nasal discharge/post nasal drip • other symptoms such as hyposmia/anosmia, headaches, halitosis,
fatigue, dental pain, cough and ear pressure.
Symptoms Traditionally obstructed sinuses are thought to have referred pain to
certain regions. This is a reasonable assumption but not foolproof. • Maxillary sinus – cheek/dental pain • Ethmoid sinus – pain between the eyes • Frontal sinus – forehead pain
• Sphenoid sinus– vertex pain

Examination Examination of the nose can be achieved in various ways • using an otoscope (cheapest) • using a headlight with magnification (more expensive) • using specialised endoscopes. This enables a more
detailed evaluation of the posterior aspect of the nose




Investigations for CRS CT scan sinuses Generally, a scan should be requested when • Unsure of the diagnosis • Patient not responding as expected to medical treatment • Surgery is planned (as per ENT specialist)
A plain sinus X-ray is no longer considered satisfactory as it is far
inferior to the information obtained from a CT scan.
MRI scans are rarely required in CRS.


Investigations for CRS Swab result • Not responding to medical therapy • Guides further appropriate selection of an antibiotic. • It is important that the swab is of mucopus visualised on nasal
examination. • A swab simply placed in the nose is of limited use due to bacteria already colonising the nose.
Investigations for CRS Allergy/immunology assessment Concomitant allergic disorders are more frequent than immunological
disorders in patients with CRS. Blood tests (radioallergosorbent testing; RAST) or skin prick tests may
be indicated Immunology assessment may also be indicated in patients that have
features suggesting an immunodeficiency.

1. Symptoms present for at least 12 consecutive weeks.
2. At least 2 of the following symptoms – Anterior and/or posterior mucopurulent drainage – Nasal obstruction – Facial pain-pressure-fullness.
3. The presence of inflammation on examination of a decongested nose (discoloured mucus or oedema in the middle meatus) and/or CT scanning showing evidence of rhinosinusitis.
Fokkens W, EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists
Diagnosis of CRS

Complications of CRS Orbital complications • Preseptal inflammation • Orbital cellulitis • Orbital cellulitis with SPA • Orbital cellulitis with orbital abscess • Cavernous sinus thrombosis
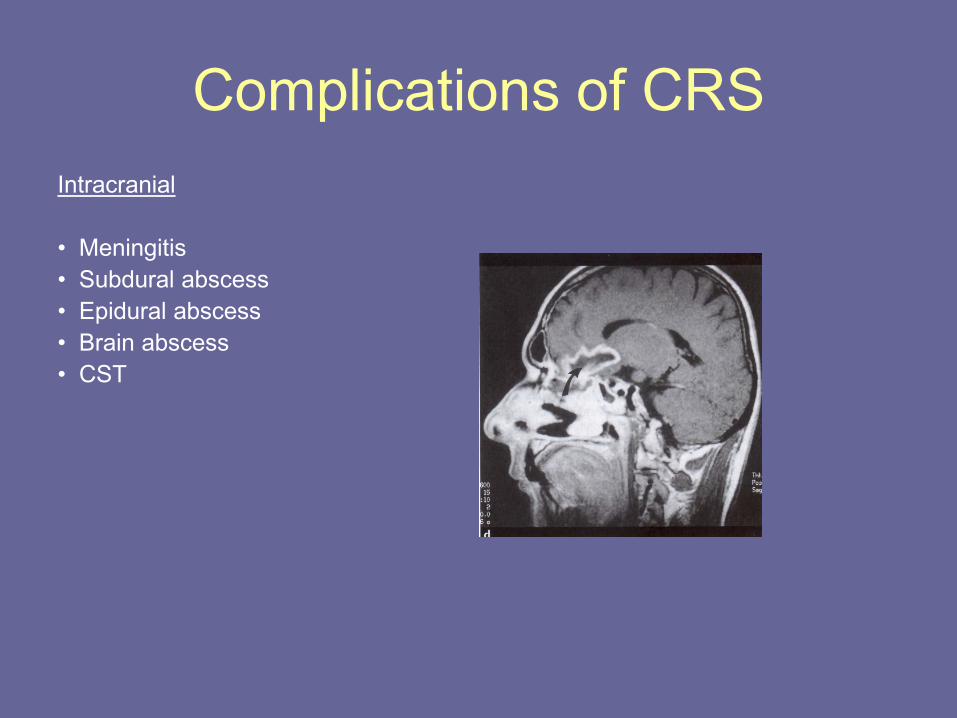
Complications of CRS Intracranial • Meningitis • Subdural abscess • Epidural abscess • Brain abscess • CST

Complications of CRS Other Complications of sinusitis •Mucocoeles

Differential Diagnosis 1 Neuralgic pain • migraine, cluster headaches and tension headaches. • minimal other symptoms to suggest CRS. • CT scan is within normal limits.

Differential Diagnosis 2 Fungal sinusitis Fungal ball/mycetoma • ‘double densities’ within the involved sinus, which is considered
pathognomonic for the disease. • surgery is indicated to remove the fungal ball. • antifungal agents are not required.

Differential Diagnosis 3 Tumours • atypical features • unilateral symptoms or signs • abnormal CT scans

Management • Nasal saline douching • Topical Steroids • Oral antibiotics • Concomitant treatment of predisposing factors – eg allergic rhinitis

Management Nasal irrigations 1. Simple 2. Safe 3. Effective 4. Minimal side effects
Mechanism of action • Simple removal of mucus • Removal of antigenic proteins • Effect on ciliary beat frequency Nasal irrigations: good or bad Opinions 2004: Jan Brown et al

Management Variables • Tonicity – hypotonic, isotonic, hypertonic • Buffering – alkaline - bicarbonate • Sterile vs non sterile • Solution – ringer lactate • Additives – antibacterial, xylitol, antifungal agents • Home produced vs commercial packages Nasal irrigations: good or bad Opinions 2004: Jan Brown et al

Management Topical intranasal corticosteroid sprays
• They are considered safe (lowest dose necessary should be used) • Some delay in onset of action • Using the opposite hand for the opposite nostril helps direct the
spray towards the middle meatus • The head tilted slightly forward is sufficient, and whether the patient
inhales or not is not paramount. • The most important factor is patient compliance. • A minimum trial for at least one month is reasonable

Management Oral antibiotics • Oral antibiotics are frequently used in patients with CRS • Randomised control trials showing the effectiveness in CRS are
limited. • Choice of antibiotic is best guided by anticipated micro-organisms in
the absence of meaningful culture/swab results. • Antibiotics should be given as a continuous course. • Macrolides are thought to have both an antibacterial effect as well
as an anti inflammatory effect so their use is appealing. • Duration of treatment is debatable and can be anywhere from 3- 6
weeks to 3 months

Management Allergic rhinitis • Environmental • Medication • Imunotherapy

Management Other • Numerous other modalities exist, all with varying benefits. • Decongestant sprays (prolonged use causes rhinitis medicamentosa
and so should be avoided) • Decongestant tablets • Mucolytics, antihistamines (sprays and tablets), and other sprays
(eg anticholinergic). • Avoidance of smoking is important. • Other modalities include adding various agents to topical saline
douches, such as xylitol and mupirocin

Management Nasal polyps Prednisolone is typically employed in patients with nasal polyps Samter’s triad / AERD (aspirin exacerbated respiratory disease)
consists of nasal polyposis, asthma and aspirin sensitivity

Management Surgery • Surgery in CRS is reserved for those patients who fail medical
treatment. • What constitutes ‘failed medical treatment’ is controversial. • Functional endoscopic sinus surgery (FESS) involves the
placement of minimally invasive endoscopes/instruments into the nose to open, drain and ventilate the sinuses whilst preserving normal sinus tissue.
• Evidence based surgery for CRS includes substantial level 4 evidence with supporting level 2 evidence that FESS is effective in improving symptoms and/or quality of life in patients with CRS.25

Management Surgery
• Day case surgery is now feasible due to the development of
dissolving nasal packing and other minimally invasive techniques • Major complications occur in less than 1% of cases • Revision surgery may be required, especially in patients with nasal
polyposis.

SUMMARY OF KEY POINTS • Rhinosinusitis is the preferred term rather than sinusitis • Chronic rhinosinusitis consists of at least 12 weeks of
symptoms • Medical therapy includes nasal saline douching,
intranasal corticosteroids and oral antibiotics • Consider CT scanning in those patients not responding
to medical treatment or when the diagnosis is unclear.

Fungal sinusitis Four types • Fungal ball • Allergic fungal sinusitis • Chronic fungal sinusitis • Acute invasive fungal sinusitis

Fungal sinusitis Fungal ball One sinus Surgery

Fungal sinusitis Allergic fungal sinusitis Nasal polyps Surgery Oral steroids

Fungal sinusitis Acute invasive fungal sinusitis Unstable diabetics or Immunocompromised 50-80 % mortality Treatment
– Surgery – Aggressive medical
management • amphotericin B • correct underlying problem

Hyposmia Normal smell – perception of odor by the nose taste – perception of salty, sweet, sour and bitter by the tongue flavor – combination of above

Hyposmia Physiology Danger fire, gas, spoiled foods Biological child / mother bonding Enjoyment perfume, food, flowers

Hyposmia

Hyposmia Pathological anosmia – complete inability to smell hyposmia – decreased ability to smell dysosmia – altered perception of smell
• phantosmia no stimulus - altered P • parosmia stimulus – altered P

Hyposmia

Hyposmia

Hyposmia Treatment
• Think could it be CNS • Steroids • Safety – fire, food, gas

Future Directions

Future Directions

Future Directions

Future Directions
Future Directions

Future Directions

Future Directions Xylitol Natural sugar Lowers salt concentration of the mucus lining the airway ( trachea, sinuses) Upregulates antimicrobial factors already present Injected xylitol with pseudomonas and compared it to pseudomonas and saline

Future Directions
Mean % of PAO1 retrieved from each solution after 20 minutes in maxillary sinus
0
2
4
6
8
10
12
saline xylitol
solution (containing PAO1) placed in maxillary sinus
% o
f ino
cula
tion
retri
eved
p = 0.034 n = 11 rabbits

Trauma Fractured Nose If patient thinks crooked – probably is broken. Exclude septal haematoma X-ray little use (?medicolegal reason) Driver’s licence 3 week window to fix

Trauma Septal haematoma In association with trauma/recent septoplasty Nasal obstruction Boggy swelling Palpation of septum Saddle nose Surgical drainage required

Epistaxis Classification Anterior vs posterior Anatomical basis Comfort level

Epistaxis Little’s area – confluence of blood vessels anterior septum

Epistaxis History Age Duration Quantity – tissues, towels, bucket! Which side ? Out the front or down the back Aspirin, warfarin Co-morbidities

Epistaxis Examination Overall – this looks bad General – PR, BP, pulse oximetry Left or right side Anterior or posterior bleed

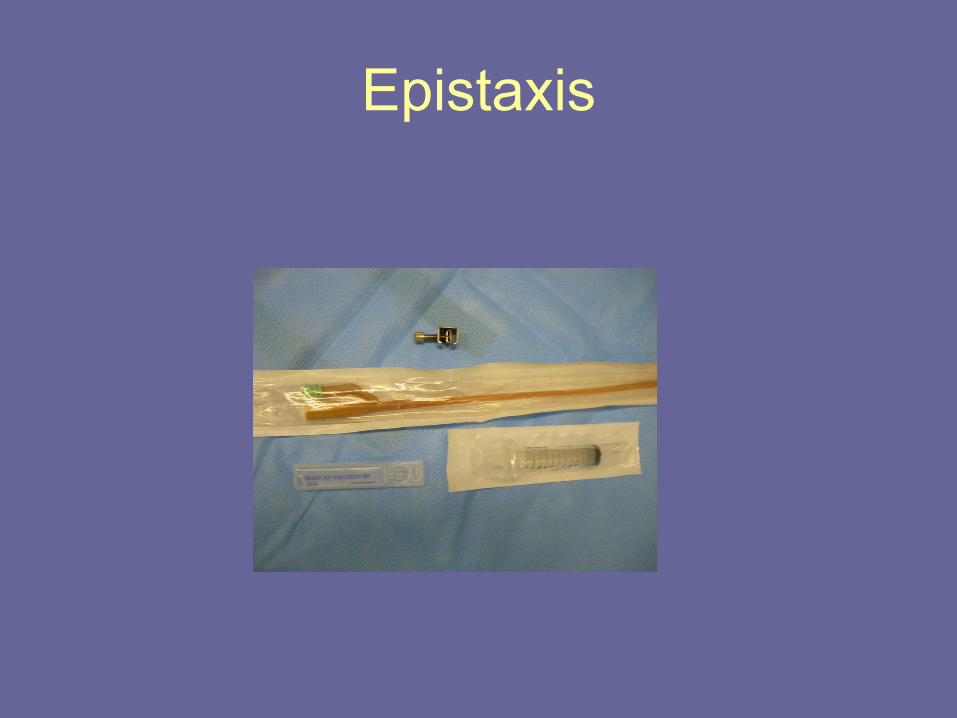
Epistaxis Set up Protection Light source Equipment Room

Epistaxis Treatment Overall IV access, resuscitation FBE Clotting G and H

Epistaxis Left or right sided
– Lean the patient forward
– ‘bleeding from both sides’ – ‘packed both sides’

Epistaxis Silver nitrate

Epistaxis
Epistaxis

Epistaxis Endoscopic sphenopalatine artery ligation for posterior bleeds Very effective Discharged same/next day Gets the pack out of the nose, and gets the patient out of the hospital

Thank you

![Are Chronic Rhinosinusitis and Paranasal Sinus ......2 = Maxillary nerve canal; VN = Vidian nerve canal. Sinusitis 2016, 1, 92 98 93 evaluating the extent of sinus pneumatization [9,10]](https://img.pdfslide.us/doc/110x75/607bc294e081f633c7431d7f/are-chronic-rhinosinusitis-and-paranasal-sinus-2-maxillary-nerve-canal.jpg)


![Research Article Can HLA-DRB4 Help to Identify Asthmatic ...downloads.hindawi.com/archive/2014/843804.pdfChronic rhinosinusitis and nasal polyposis are very common in CSS [ ] and paranasal](https://img.pdfslide.us/doc/110x75/60dc8f3b66068f174f65c7ec/research-article-can-hla-drb4-help-to-identify-asthmatic-chronic-rhinosinusitis.jpg)