Embed Size (px)
Citation preview
Move Over Pscyhotropics Here Come the
Antibiotics! Jennifer L. Hardesty, PharmD, FASCP Chief Clinical Officer,
Corporate Compliance Officer Remedi SeniorCare
William M. Vaughan BSN, RN
Vice President, Education and Clinical Affairs Remedi SeniorCare
Disclosure / Contact
• Jennifer Hardesty has no relevant disclosures
• William Vaughan is a contractor to CMS (QAPI) and a member of the Institute for Safe Medication Practices clinical advisory board (Long-Term Care Advise ERR)
• Contact : • [email protected]

“Welcome to the ISMP Long-Term Care Advise-ERR, a medication safety newsletter designed specifically to
meet the needs of administrators, nursing directors, and nurses who transcribe medication orders, administer medications, monitor the effects of medications on
residents, and/or supervise those who carry out these important tasks.”
http://www.ismp.org/Newsletters/longtermcare/default.aspx
Objectives
• Discuss current and proposed federal regulations which impact the use of antibiotics in nursing homes.
• Identify three clinical practices which maximize the benefits and minimize the risks associated with the use of antibiotics in long term care residents.
• Describe the concept of antibiotic stewardship and identify four core elements of an antibiotic stewardship program.
Regulatory “Priorities”
Antibiotics

“However, with the recent emergence of resistant organisms, pediatric organizations have strongly recommended initial antibiotics only for certain children” - Merck Manual
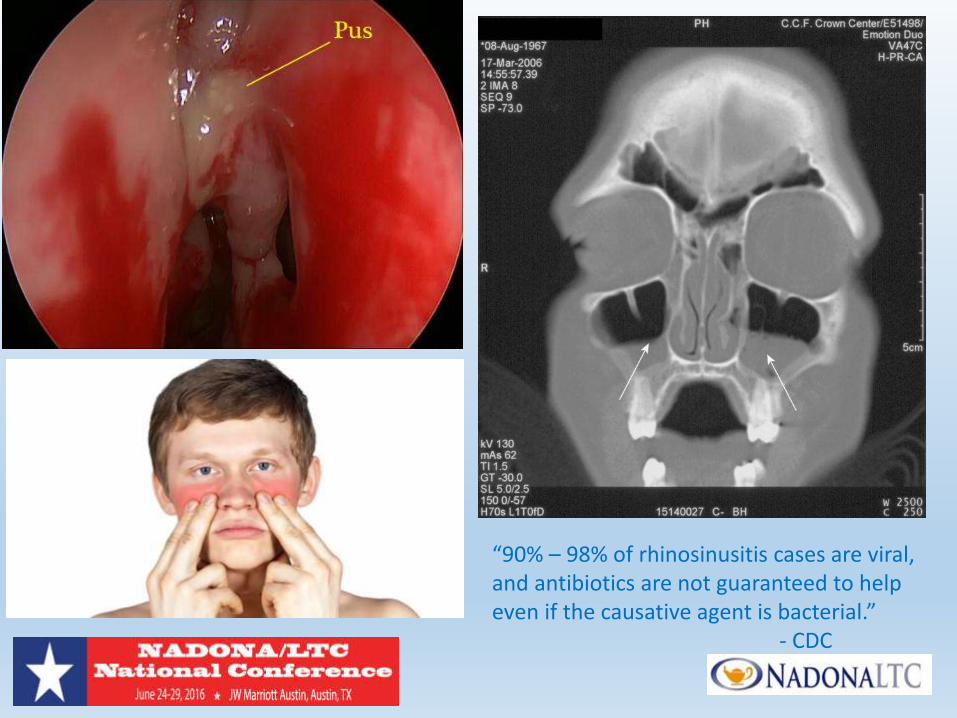
“90% – 98% of rhinosinusitis cases are viral, and antibiotics are not guaranteed to help even if the causative agent is bacterial.” - CDC
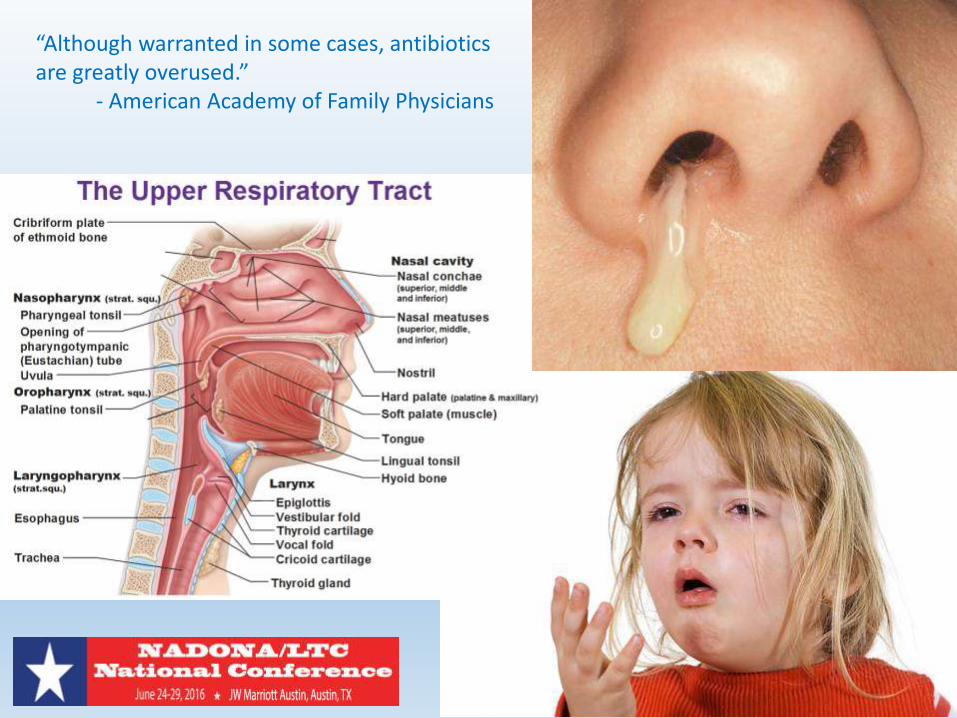
“Although warranted in some cases, antibiotics are greatly overused.” - American Academy of Family Physicians

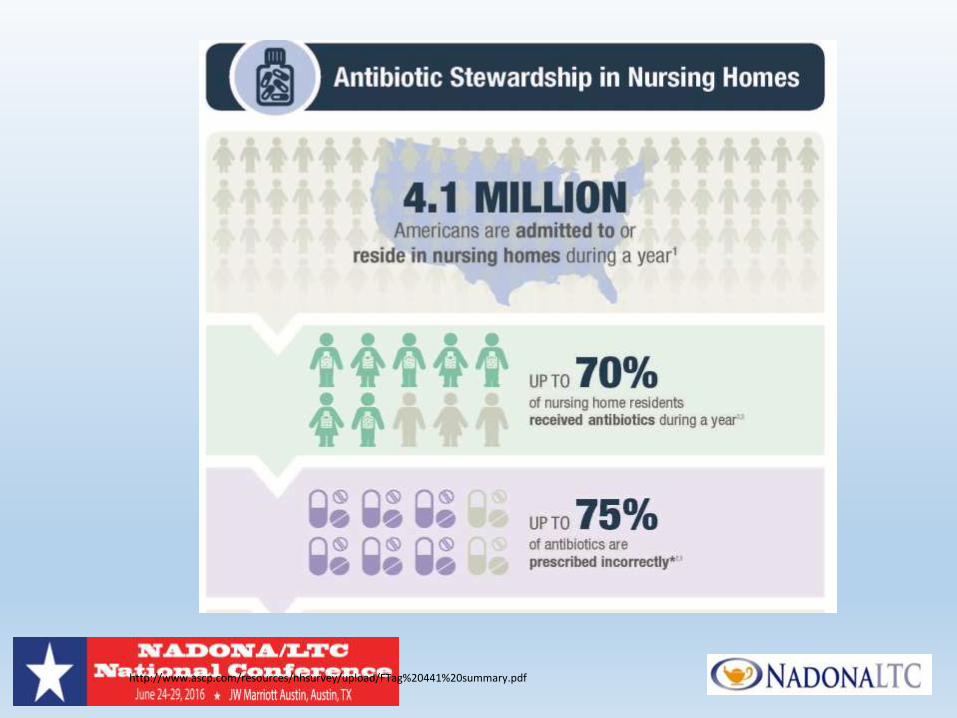
Nursing Homes
• ~ 4 million admissions / year
• ABT use common (up to 70% / year)
• Inappropriate prescribing (up to 75%) • Unnecessary
• Wrong drug, dose or duration
• Colonization common
Source: CDC (http://www.cdc.gov/media/releases/2015/p0915-nursing-home-antibiotics.html)
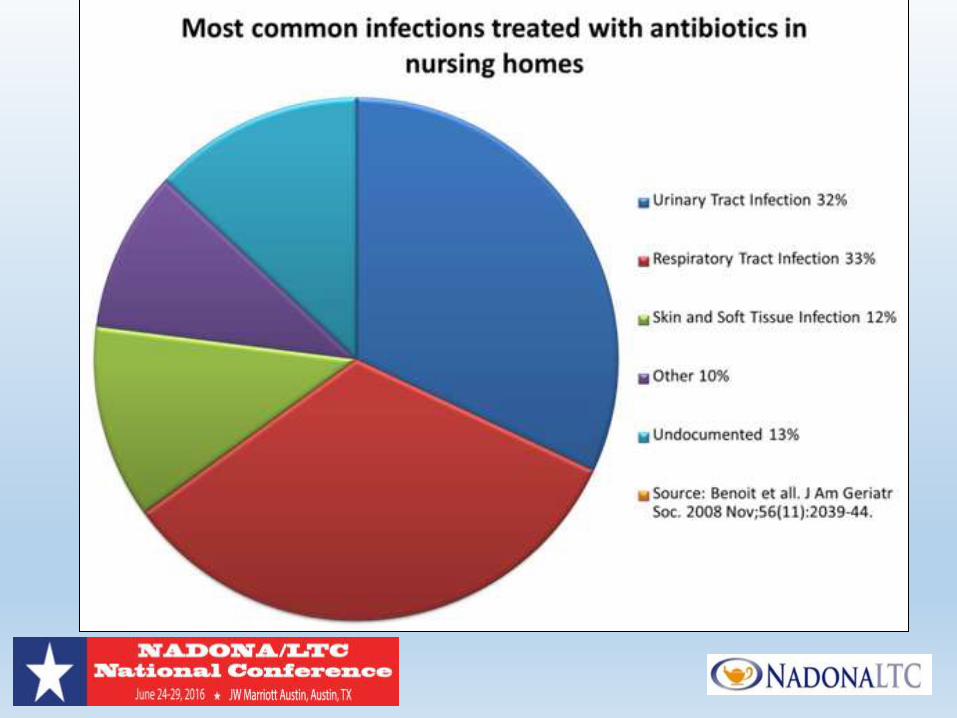
In the Crosshairs: Urinary Tract “Infections”
• Generalized change in condition (falls, mental status, etc.) • Adverse drug reaction ("Any symptom in an elderly
patient should be considered a drug side effect until proven otherwise.”– Gurwitz et al)
• Fluid / electrolyte imbalance
• Infection • + urine culture Antibiotics
colonization
In the Crosshairs: Urinary Tract “Infections”
• “Don’t obtain a urine culture unless there are clear signs and symptoms that localize to the urinary tract.” • AMDA
• “Don’t use antimicrobials to treat bacteriuria in older adults unless specific urinary tract symptoms are present.” • AGS
Guidance to Surveyors – F 315 (what's old is new again)
“In someone with nonspecific symptoms such as a change in function or mental status, bacteriuria alone does not necessarily warrant antibiotic treatment. Additional evidence that could confirm a UTI may include hematuria, fever (which could include a variation from the individual’s normal or usual temperature range), or evidence of pyuria (either by microscopic examination or by dipstick test). In the absence of fever, hematuria, pyuria, or local urinary tract symptoms, other potential causes of nonspecific general symptoms, such as fluid and electrolyte imbalance or adverse drug reactions, should be considered instead of, or in addition to, a UTI …”
In the Crosshairs: Urinary Tract “Infections”
• A patient with advanced dementia may be unable to report urinary symptoms … In this situation, it is reasonable to obtain a urine culture if there are signs of systemic infection such as fever … leukocytosis, or a left shift or chills in the absence of additional symptoms (e.g., new cough) to suggest an alternative source of infection. • AMDA

Other High Risk Areas
Current Regulations
• F 281 (Profession standards of quality) • “Standards published by professional organizations”
• F 329 (Unnecessary Drugs) • Indication
• Dose
• Duration
• Monitoring
• Adverse consequences (c. diff)
Inappropriate prescribing (up to 75%) Unnecessary Wrong drug, dose or duration - CDC on ABT (2105)
No Absolutes Rationale for Care Based on: • Evidence
• Thoughtful risk / benefit analysis
• Resident / surrogate involvement
Document especially in high risk situations
June 28, 2016
Cipro 500 mgs. PO q day x 7 days UTI
- VO Dr. Smith
76 year old Female : SDAT, HTN , DM, CHF
Actions to Consider
• Engage Medical Directors / Consultant Pharmacists
• Educate • Prescribers
• Nursing staff
• Residents / surrogates /families • “But what if your wrong?”
• Discuss / document goals of care
Actions to Consider
• Don’t succumb to perceived regulatory pressure to “do something” • Watchful waiting
• Antibiotic “time out”
• Quality assurance • Consistency of prescribing practices
• Type of antibiotic (broad spectrum)
• Duration of therapy
• Choosing Wisely (www.choosingwisely.org)
Proposed Regulations
• Infection and Prevention Control Officer
• Infection Prevention and Control Program • Antibiotic stewardship
• Quality Assurance Performance Improvement
QAPI: Think Like a Squirrel


http://www.ascp.com/resources/nhsurvey/upload/FTag%20441%20summary.pdf
Antibiotics- Some Facts
Each Year in the US:
• ~2 million people become infected with resistant bacteria
• At least 23,000 people die each year as a direct result of these infections
• 250,000 patients (hospitalization) get Clostridium difficile each year,
• C. difficile kills at least 14,000 people each year
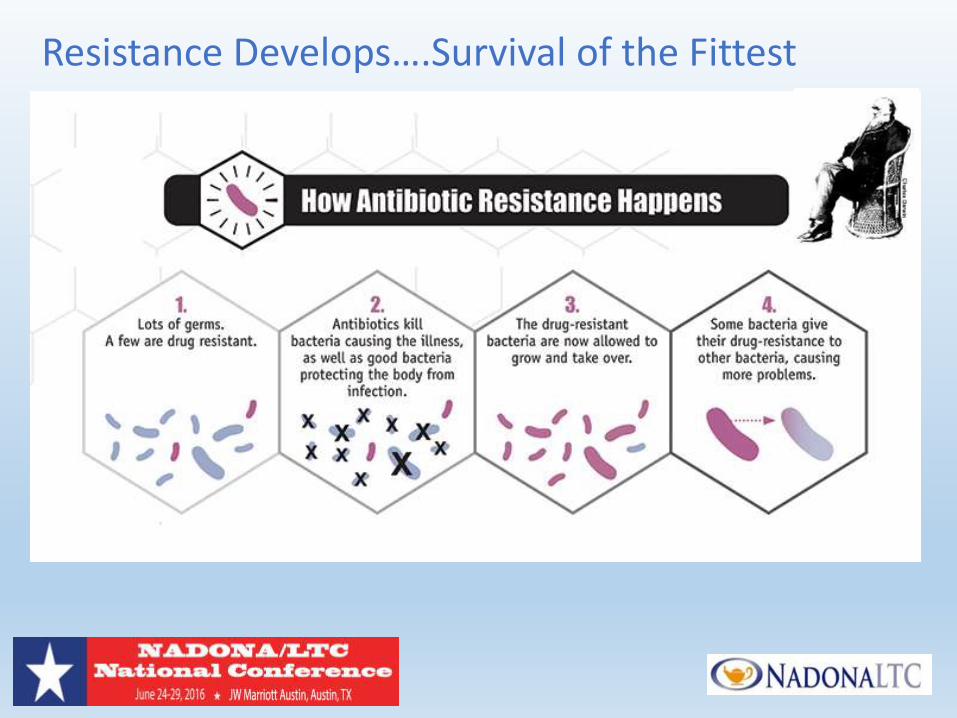
Resistance Develops….Survival of the Fittest
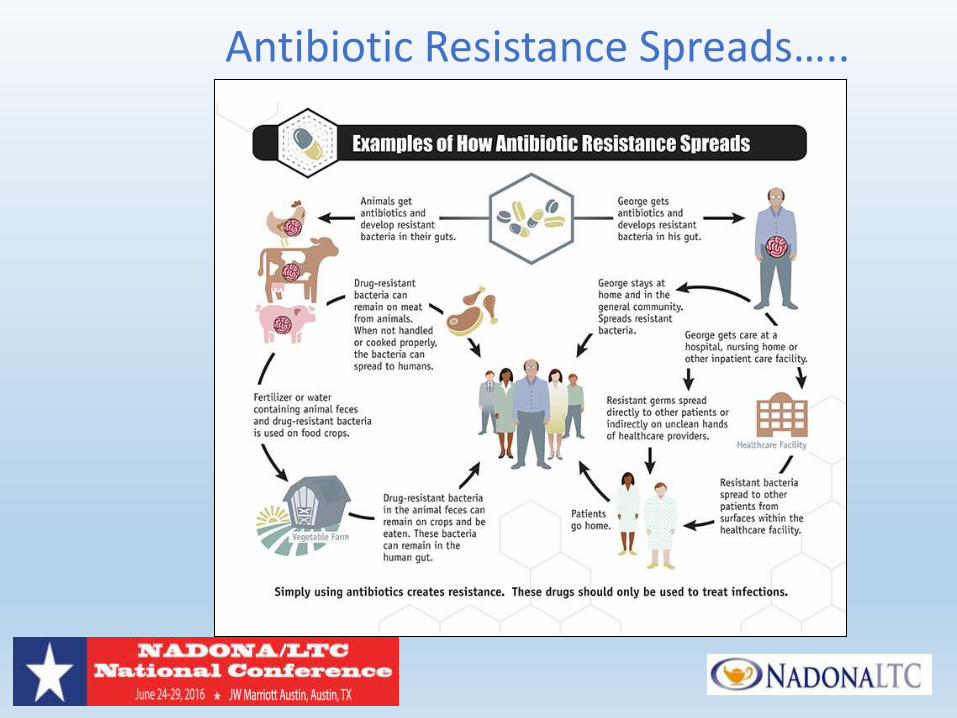
Antibiotic Resistance Spreads…..
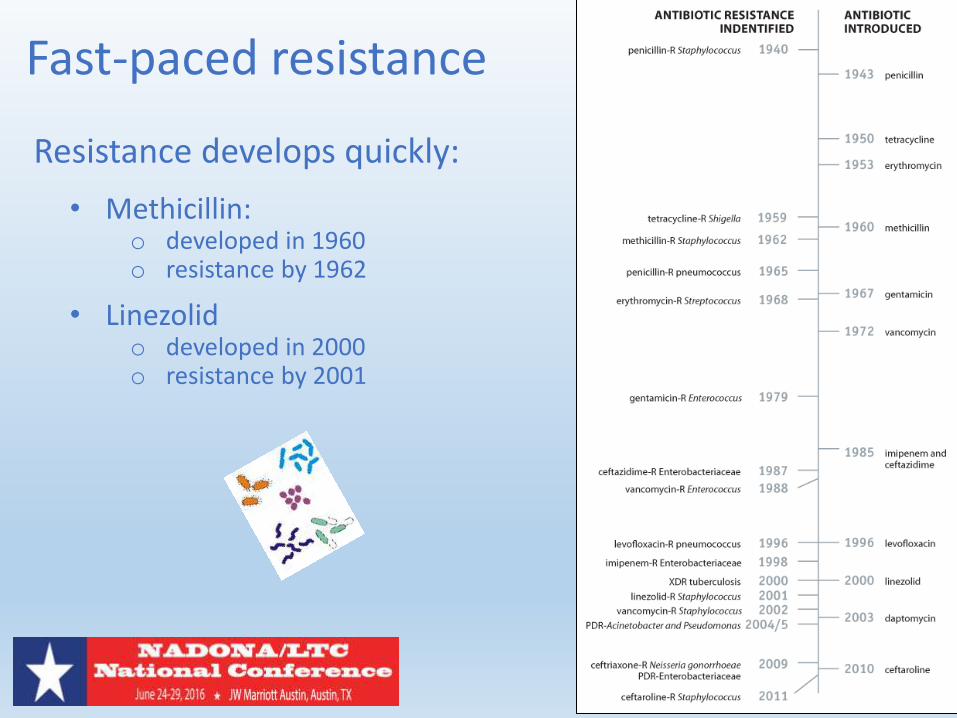
Fast-paced resistance
Resistance develops quickly:
• Methicillin: o developed in 1960 o resistance by 1962
• Linezolid o developed in 2000 o resistance by 2001
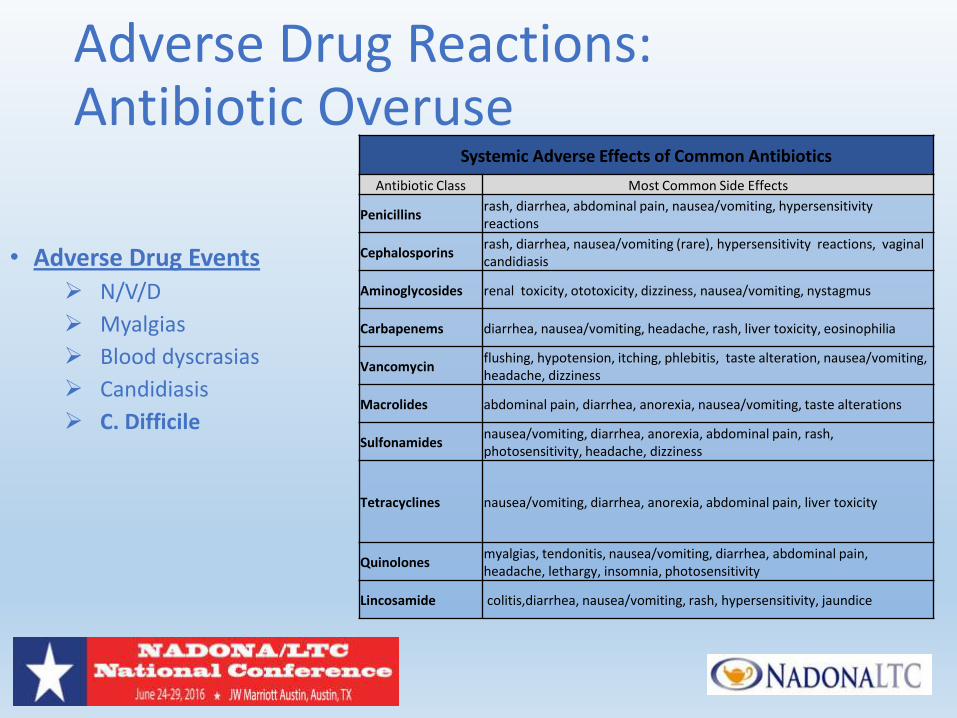
Adverse Drug Reactions: Antibiotic Overuse
• Adverse Drug Events N/V/D
Myalgias
Blood dyscrasias
Candidiasis
C. Difficile
Systemic Adverse Effects of Common Antibiotics
Antibiotic Class Most Common Side Effects
Penicillins rash, diarrhea, abdominal pain, nausea/vomiting, hypersensitivity reactions
Cephalosporins rash, diarrhea, nausea/vomiting (rare), hypersensitivity reactions, vaginal candidiasis
Aminoglycosides renal toxicity, ototoxicity, dizziness, nausea/vomiting, nystagmus
Carbapenems diarrhea, nausea/vomiting, headache, rash, liver toxicity, eosinophilia
Vancomycin flushing, hypotension, itching, phlebitis, taste alteration, nausea/vomiting, headache, dizziness
Macrolides abdominal pain, diarrhea, anorexia, nausea/vomiting, taste alterations
Sulfonamides nausea/vomiting, diarrhea, anorexia, abdominal pain, rash, photosensitivity, headache, dizziness
Tetracyclines nausea/vomiting, diarrhea, anorexia, abdominal pain, liver toxicity
Quinolones myalgias, tendonitis, nausea/vomiting, diarrhea, abdominal pain, headache, lethargy, insomnia, photosensitivity
Lincosamide colitis,diarrhea, nausea/vomiting, rash, hypersensitivity, jaundice
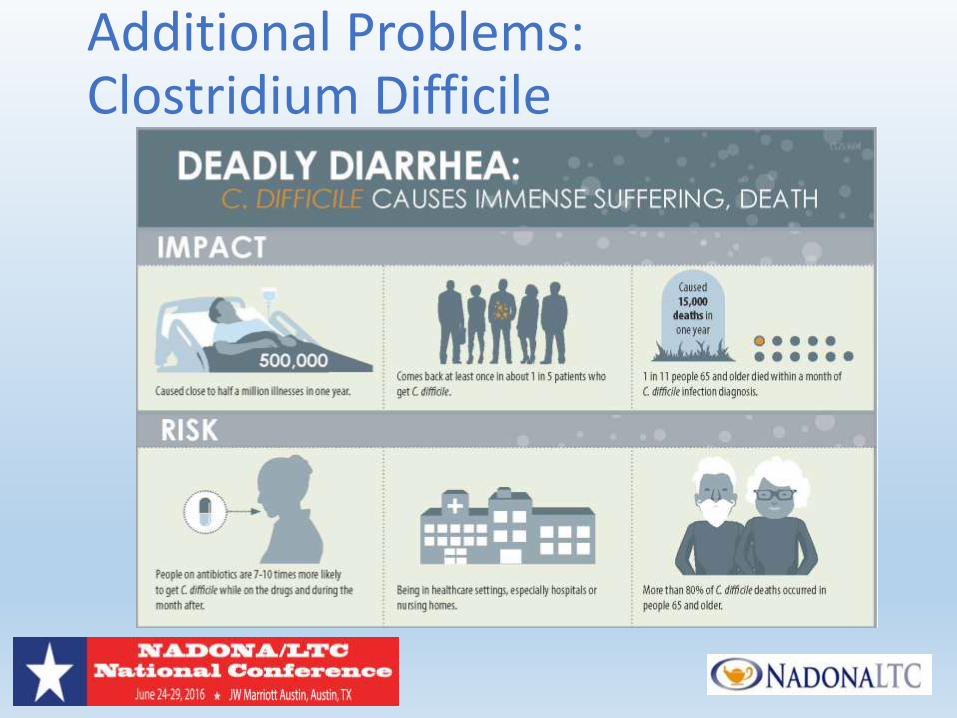
Additional Problems: Clostridium Difficile
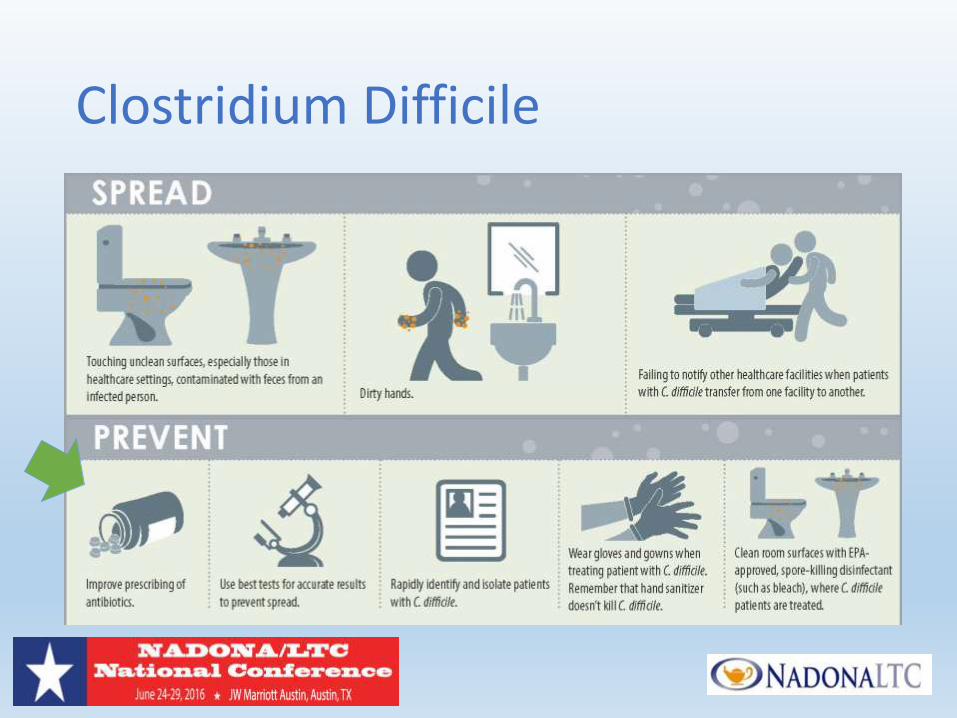
Clostridium Difficile
C.Difficile - Treatment Drug Treatment:
• Metronidazole $ • Vancomycin $$-$$$ • Fidaxomicin (Dificid) $$$$
Recurrence -can occur in up to 25% of patients (another episode of C. difficile within 8 weeks)
• Relapse of the initial infection • Re-infection with a new strain
Recurrence Treatment:
• First recurrence- the same medication • Second recurrence, a tapered or pulsed oral vancomycin • Third recurrence fecal transplant should be considered
Long-term care facility residents are particularly at risk for C. Difficile complications
CDC: What Can the Health Care Community Do?
CDC: What Can the Health Care Community Do?
Antimicrobial Stewardship
Patients receive the right antibiotic, at the right dose, at the right time, and for the right duration
Coordinated interventions designed to improve and measure the
appropriate use of antimicrobial agents by promoting the
selection of the optimal antimicrobial drug regimen
Antibiotic Stewardship Programs are a “win‐win” for all involved!
Antibiotic Stewardship will: • Decrease antibiotic resistance
• Decrease C. difficile infections
• Decrease costs
• Increase good patient outcomes
http://www.cdc.gov/getsmart/healthcare/factsheets/antibiotic-use.html
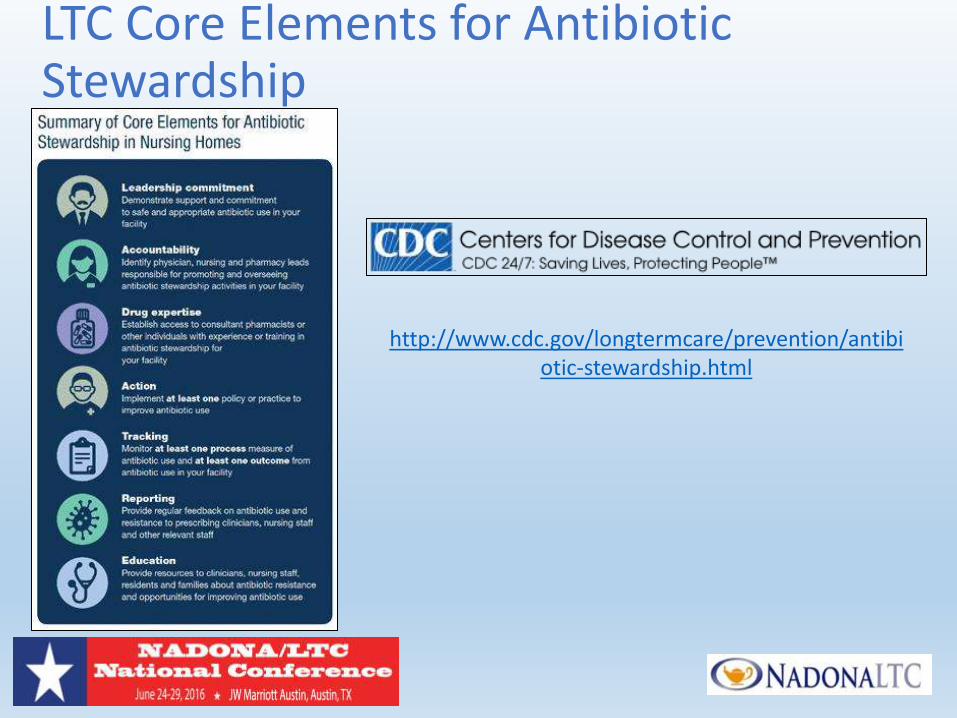
LTC Core Elements for Antibiotic Stewardship
http://www.cdc.gov/longtermcare/prevention/antibiotic-stewardship.html

Leadership Commitment
• Write statements in support of improving antibiotic use to be shared with staff, residents and families
• Include stewardship-related duties in position descriptions: o Medical Director o Clinical nurse leads, DON o Consultant pharmacist
• Communicate with nursing staff, prescribing clinicians o Expectations about use of antibiotics o Monitoring and enforcement of stewardship policies
• Create a culture which promotes antibiotic stewardship o Messaging o Education o Celebrating improvement
Accountability
• Medical Director: set standards for antibiotic prescribing practices for all clinical providers
• Director of Nursing: set the practice standards for assessing, monitoring and communicating changes in a resident’s condition by front-line nursing staff.
• Infection prevention program coordinator: o Track antibiotic starts o Monitor adherence to evidence-based published criteria o Review antibiotic resistance patterns in the facility
• Consultant pharmacist : support antibiotic stewardship oversight through quality assurance activities
• Laboratory Services: o Alerting facility if certain antibiotic-resistant organisms are identified, o Educate staff on the differences in diagnostic tests available o Antibiogram
Drug Expertise
• Partner with antibiotic stewardship program leads at the hospitals within your referral network
• Infectious Disease practitioners and consultants in your community
• Consultant Pharmacists
Action Through Policy/Practice Change
Policies that support optimal antibiotic use o Require dose, duration, indication for every order o Viewing culture data
Broad interventions to improve antibiotic use o Improving the evaluation and communication of clinical signs/symptoms
o “Communication Tool” o INTERACT Tools
o “Antibiotic time-out” o Developing antibiotic monitoring and infection management guidance
Infection and syndrome specific interventions to improve antibiotic use
o Asymptomatic bacteriuria (ASB) o Urinary tract infection prophylaxis o Lower Respiratory Tract Infections (Viral vs Bacterial)
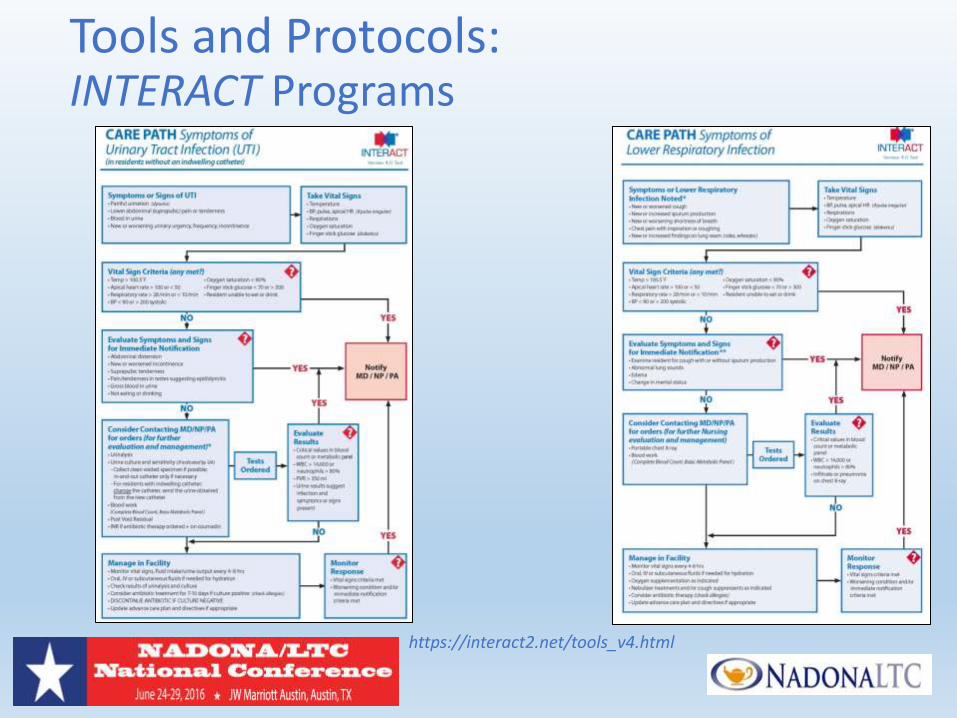
Tools and Protocols: INTERACT Programs
https://interact2.net/tools_v4.html
Tracking/Reporting: Use and Outcomes
• Process Measures: o Completeness of clinical assessment documentation at the time of the
antibiotic prescription o Completeness of antibiotic prescribing documentation o Antibiotic selection is consistent with recommended agents for specific
indications o Point prevalence of antibiotic use o Antibiotic days of therapy (DOT) o Post-prescription review of appropriateness
• Outcome Measures:
o Track C. difficile and resistant organisms o Track adverse drug events related to antibiotic use o Antibiotic resistance o Track costs related to antibiotic use
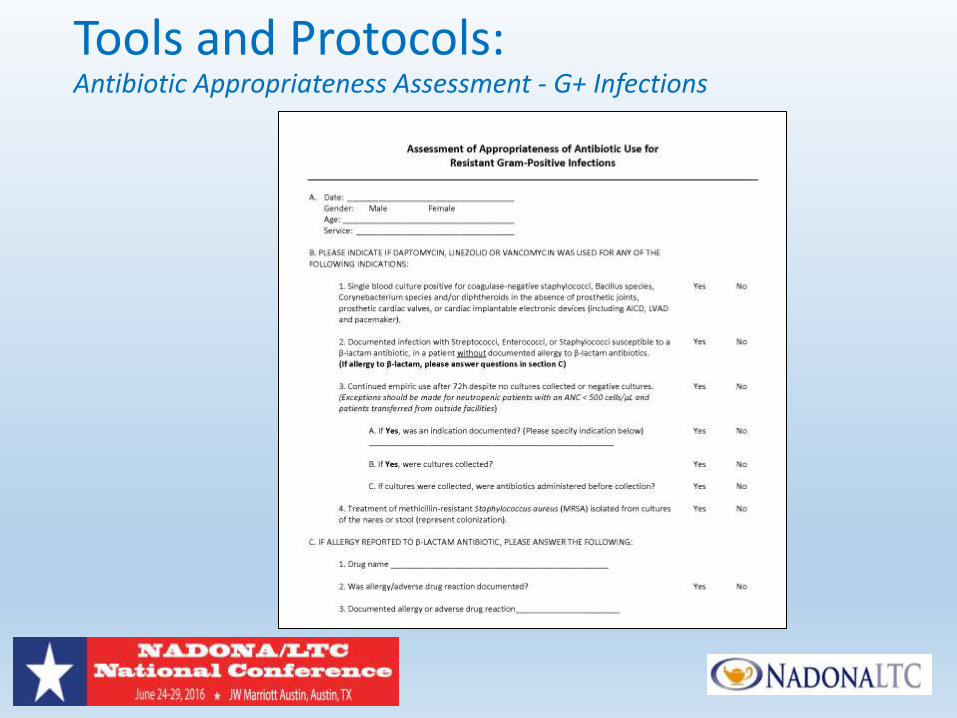
Tools and Protocols: Antibiotic Appropriateness Assessment - G+ Infections
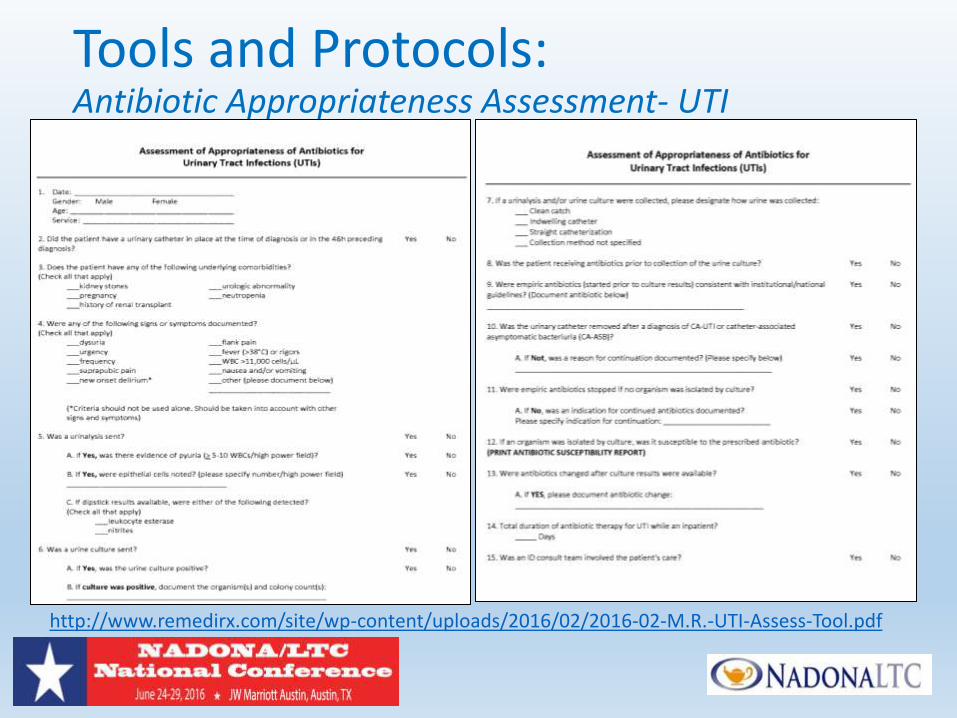
Tools and Protocols: Antibiotic Appropriateness Assessment- UTI
http://www.remedirx.com/site/wp-content/uploads/2016/02/2016-02-M.R.-UTI-Assess-Tool.pdf
Education
• Provide antibiotic stewardship education to clinicians, nursing staff, residents and families
• Linking education with feedback on physician prescribing practices
• Interactive academic detailing (e.g., face-to-face interactive workshops) has the strongest evidence for improving medication prescribing practices
• Providing feedback on individual physician prescribing practices and adherence to the guidelines over 12 months
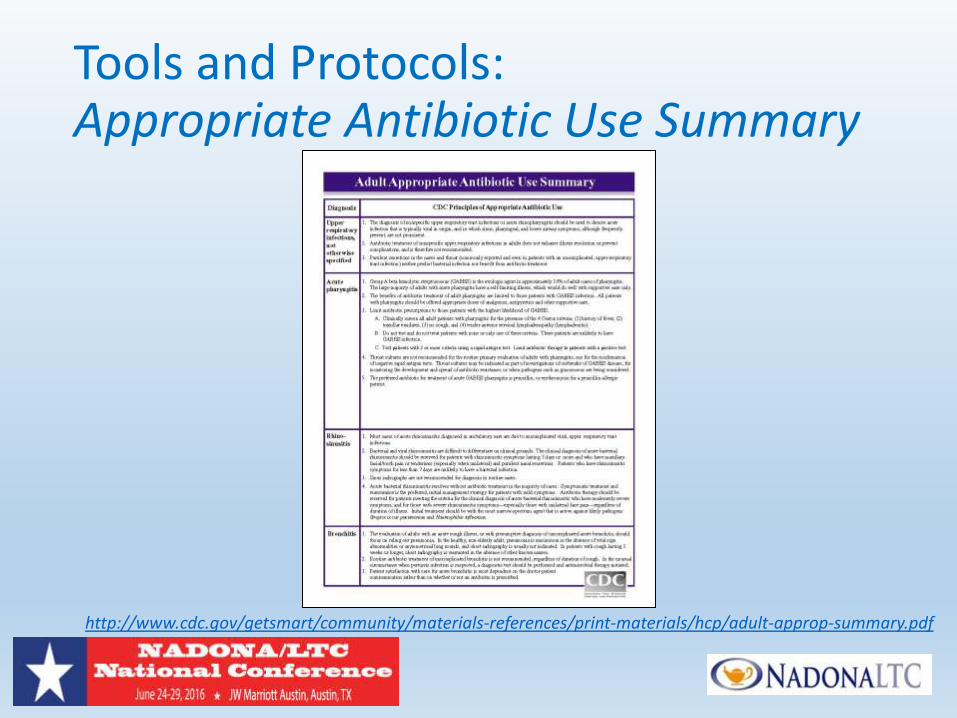
Tools and Protocols: Appropriate Antibiotic Use Summary
http://www.cdc.gov/getsmart/community/materials-references/print-materials/hcp/adult-approp-summary.pdf
The First Steps:
• Ensure all orders have dose, duration, and indications
• Get cultures before starting antibiotics
• Take an “antibiotic timeout,” reassessing antibiotics after 48–72 hours
• Implement policies that encourage best practices o Establishment of minimum criteria for prescribing antibiotics
o Review of antibiotic appropriateness/resistance patterns
o Nursing protocols for monitoring patients’ status for an evolving condition if there is no specific indication for antibiotics
Small, Sustainable Changes
• Facility should not attempt to implement all of the interventions at once.
• Interventions to implement should be tailored to the areas that most need improvement at your facility
• Essential to monitor and measure
o Measurement Framework- various measures of antibiotic use to assess effectiveness of improvements

http://www.remedirx.com/news-events/news/
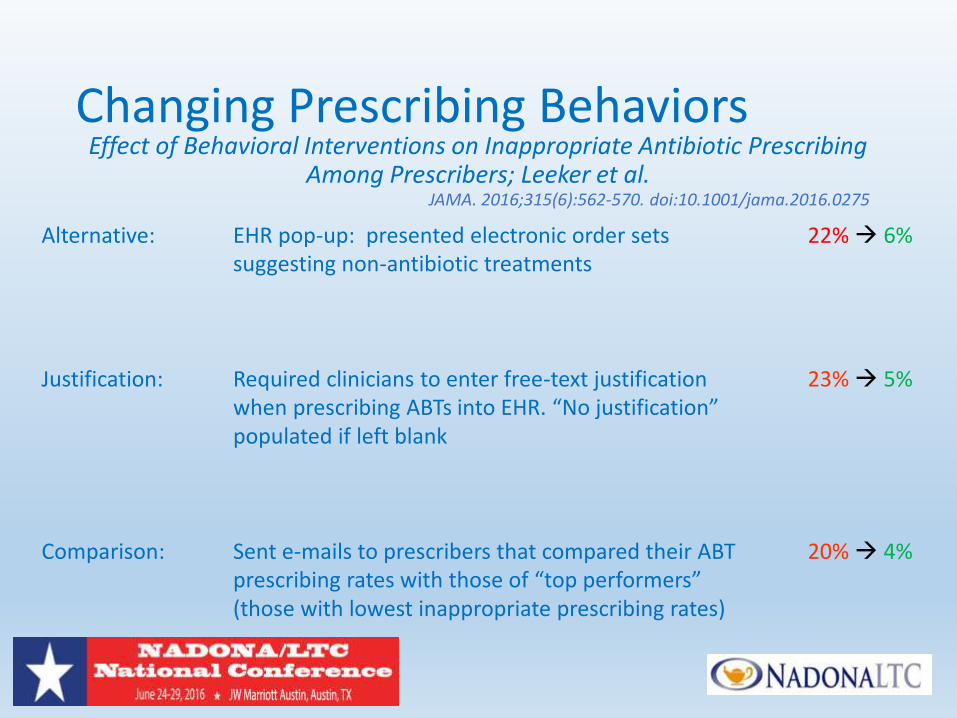
Changing Prescribing Behaviors Effect of Behavioral Interventions on Inappropriate Antibiotic Prescribing
Among Prescribers; Leeker et al. JAMA. 2016;315(6):562-570. doi:10.1001/jama.2016.0275
Alternative: EHR pop-up: presented electronic order sets 22% 6% suggesting non-antibiotic treatments Justification: Required clinicians to enter free-text justification 23% 5% when prescribing ABTs into EHR. “No justification” populated if left blank Comparison: Sent e-mails to prescribers that compared their ABT 20% 4% prescribing rates with those of “top performers” (those with lowest inappropriate prescribing rates)
Antibiotic Stewardship:
Are You Ready?
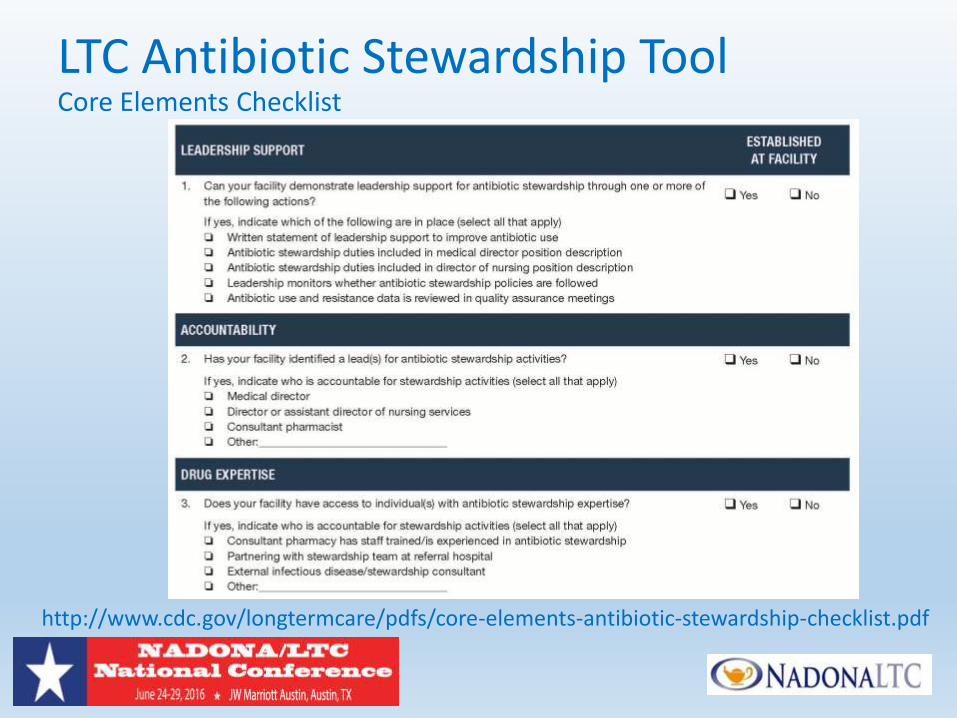
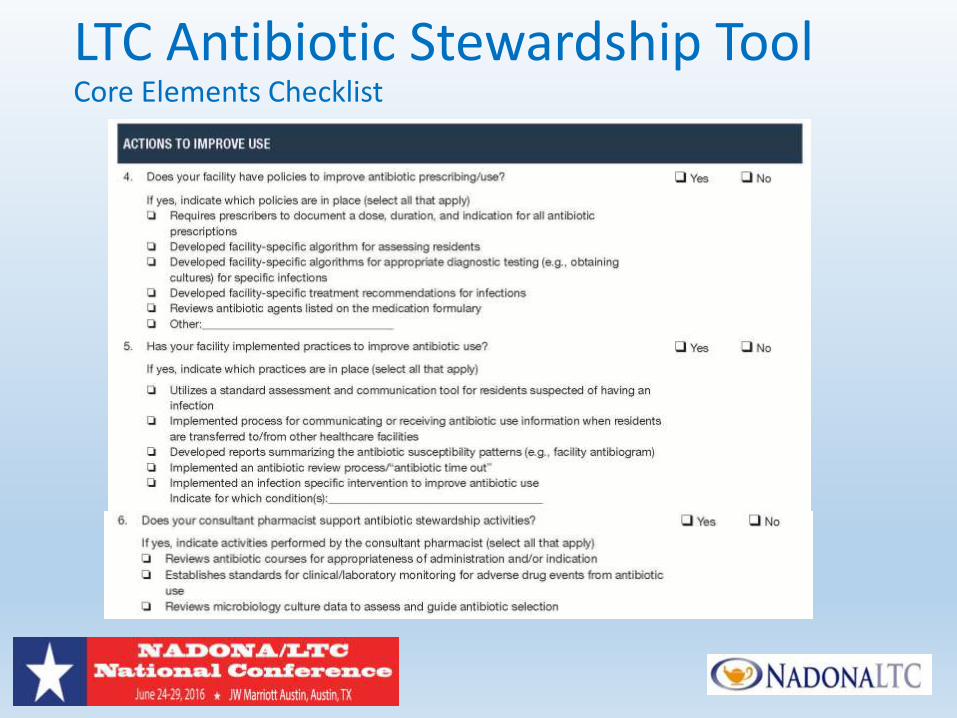
LTC Antibiotic Stewardship Tool Core Elements Checklist
http://www.cdc.gov/longtermcare/pdfs/core-elements-antibiotic-stewardship-checklist.pdf
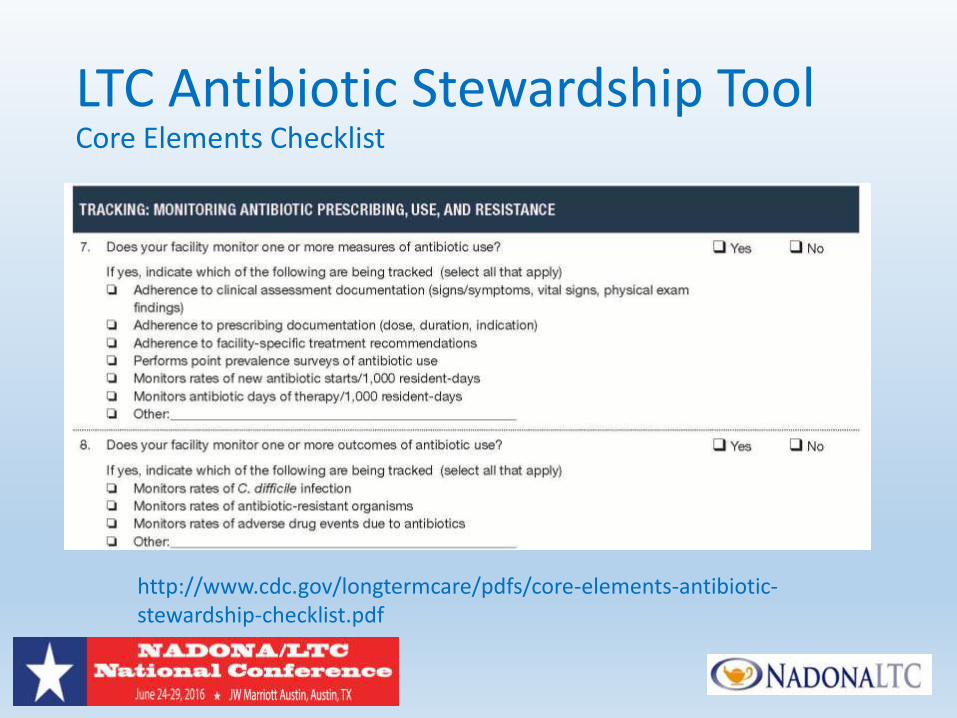
LTC Antibiotic Stewardship Tool Core Elements Checklist
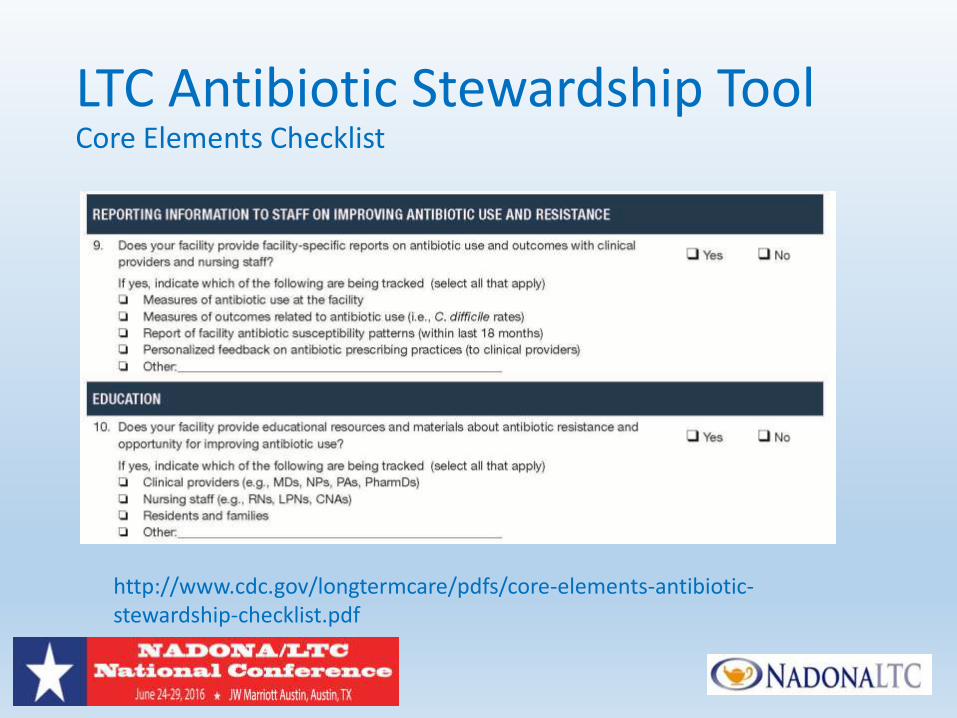
LTC Antibiotic Stewardship Tool Core Elements Checklist
http://www.cdc.gov/longtermcare/pdfs/core-elements-antibiotic-stewardship-checklist.pdf
LTC Antibiotic Stewardship Tool Core Elements Checklist
http://www.cdc.gov/longtermcare/pdfs/core-elements-antibiotic-stewardship-checklist.pdf
References • State Operations Manual: Appendix PP - Guidance to
Surveyors for Long Term Care Facilities • (https://www.cms.gov/Regulations-and-
Guidance/Guidance/Manuals/downloads/som107ap_pp_guidelines_ltcf.pdf)
• Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities • (https://www.federalregister.gov/articles/2015/07/16/2015-
17207/medicare-and-medicaid-programs-reform-of-requirements-for-long-term-care-facilities)
• Overview and Evidence to Support Stewardship • (http://www.cdc.gov/getsmart/healthcare/evidence.html)
Thank You
Questions?