Embed Size (px)
Citation preview

Moustafa K Eissa MD FRCOG, Hussam Shawkey MD,
Ahmad Samir MD, Yasser el-Mazney MBChB
Department of Obstetrics & Gynaecology, Minia University
and Minia Infertility Research & Treatment Center.

During ovulatory menstrual cycles, follicles develop and rupture releasing mature ova. Dysfunctional ovulation cysts arise when this physiologic release fails and follicular growth continues (Eissa etal 1986). This occurs either from excessive stimulation by follicle stimulating hormone (FSH) or from lack of the normal preovulatory luteinizing hormone (LH) surge (Altchek et al 2003 and Prat et al 2004). Others suggest abnormal follicle (Eissa etal 1987)

Follicular cysts grow larger than 28 mm and most are asymptomatic. Larger cysts may cause pelvic discomfort or heaviness. If the granulosa cells lining the follicular cyst produce excessive oestradiol, menstrual irregularities occur (DiSaia and Creasman 2002 and Altchek et al 2003).

Treatment of simple follicular cyst varies from expectant management (Nardo etal 2003), medical treatment (Turan et al., 1994). , transvaginal
aspiration under ultrasound guidance (Shawekey etal 2011), laparoscopic
aspiration or excision (Lin et al., 1995) and surgical ovarian cystectomy (Flynn and Niloff, 1999).

Durlinger (1999) suggested that in the absence of AMH, follicles may be more sensitive to FSH. In vitro and in-vivo studies confirmed this hypothesis (Durlinger et al., 2001).

The inhibitory effects of AMH on FSH-sensitivity of follicles may play an important role in the process of selection. During selection a group of follicles is selected from the group of AMH-producing growing follicles to continue growth up to the preovulatory stage. It is thought that, depending on its developmental stage. Each follicle requires a certain concentration of FSH to continue growth and this concentration has to be exceeded to ensure selection. Since AMH affects FSH-sensitivity of the follicles, it may play a role in the determination of follicles to undergo selection or be removed through atresia (Baarends 1995).

The primary aim of the study is to see if the AMH plays a role in cyst formation. The secondary aim is to test if AMH may be used as a predictor for response to medical treatment in patients with simple dysfunctional ovulation cyst.

This prospective randomized controlled study was conducted in the Department of Obstetrics and Gynecology, Faculty of Medicine, El-Minia University and El-Minia infertility research unit during the period from November 2009 to June 2010, after being approved by the Department’s Ethical Committee.

This study included 35 patients, divided into two groups. The control group included 10 infertile patients prepared for ICSI procedure. The study group included 25 patients, presented with simple dysfunctional ovulation cyst resistant to medical treatment for three months. They had transvaginal ultrasound criteria for cyst benignity being unilateral, less than 10 cm, thin walled with no internal trabiculae or septations and clear contents. They were subjected to transvaginal ultrasound aspiration as a method of treatment as previously described (Shawkey etal 2011).

Levels of AMH, testosterone and oestradiol were measured. These hormones were withdrawn from follicles aspirated during ovum pick up (group1) and from simple follicular cyst during therapeutic cyst aspiration (group 2). Levels of serum AMH and FSH were measured in all patients. Correlations between these hormones were done in a trial to explain pathophysiology of anovulation and cyst formation and to match between the pathophysiology and mode of treatment for each ovarian cyst.

Patients' characteristics
Group I(n= 25)
Group II(n= 10)
P value--
RangeMean ± SDrangeMean ± SD
Age (years)20-4028.04±6.122-4032.8±4.70.3 (NS)
Height (cm) 154-170162.7±7.6150-170163.9±5.80.6) NS(
Weight (kg) 60-8070.5±5.166-8072.6±4.60.2) NS(
BMI19.3-30.426.7±2.522.8-3227.1±2.60.6) NS(
Results1To our knowledge, this study is the first to measure
AMH in fluid aspirated from human simple ovarian cyst
Table (1): Patients' characteristics in both study groups

ComplaintsNoPercent
Primary infertility1352%
Secondary infertility624%
Amenorrhea28%
Metroragia28%
Menoragia 28%
Table (2)shows patient's clinical presentations of the group2 (study) more than half (52%) of the patients presented by primary infertility followed by (24%) secondary infertility While the rest of them presented by amenorrhea, metroragia and menoragia by (8%) for each.

Hormone
Group 1(n= 10)
Group 2(n= 25)P value
Mean ± SDMean ± SD
Serum FSH (ng\ml)4.65±1.55.41±1.90.2 (NS)
Serum AMH (ng\ml)5.9±2.0214.6±3.30.0001(S)
FF* AMH (ng\ml)29.5±25.7440.7±182.90.0001(S)
FF* Testosterones (ng\ml)5.8±4.25.2±3.70.6(NS)
FF* Estradiol (ng\ml)21.2±0.620.4±6.80.7(NS)
*FF: follicular fluid (means follicular fluid in group 1 and cyst fluid in group 2). Table (3) shows hormonal profiles in group1 (control) and group 2 (study):Serum and follicular fluid AMH in group 2 are higher than group 1 and this difference is statistically significant, while there is no statistical differences between the two groups as regard other hormones.

70.0060.0050.0040.0030.0020.0010.000.00
Intrafollicular AMH (ng/ml)
10.00
9.00
8.00
7.00
6.00
5.00
4.00
3.00
Ser
um
AM
H (ng/m
l)
r= 0.38 p= 0.2
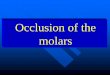
Fig(1) shows that there is a non significant fair positive association between follicular fluid and serum AMH (r=0.38, p =0.2).

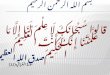
Fig (2 ) shows that there is non significant fair negative association between follicular fluid AMH and serum FSH with (r =-0.26, p =0.4)
70.0060.0050.0040.0030.0020.0010.000.00
Intrafollicular AMH (ng/ml)
6.00
5.50
5.00
4.50
4.00
3.50
Seru
m F
SH
(ng/m
l)r= - 0.26 p= 0.4

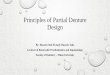
Fig (3 ) shows that there is non significant moderate negative association between AMH and estradiol levels in follicular fluid (r =-0.60, p =0.6).
70.0060.0050.0040.0030.0020.0010.000.00
Intrafollicular AMH (ng/ml)
22.00
21.50
21.00
20.50
20.00
Intrafollic
ula
r E
stradio
l (ng/m
l)
r= - 0.60 p= 0.06

Also in this group (Control group) there is no association between AMH and testosterone in follicular fluid (r =0.09, p =0.8), no association between serum AMH and serum FSH (r=0.17 ,p =0.6), non significant moderate negative association between serum AMH and follicular fluid esrtadiol (r =-0.52, p =0.1) and no association between serum AMH and follicular fluid Testosterone ( r=-0.11,p=0.7).

Fig(4)shows that there is no association between follicular fluid and serum AMH (r=0.07, p =0.7).
1500.001200.00900.00600.00300.000.00
Intrafollicular AMH (ng/ml)
20.00
18.00
16.00
14.00
12.00
10.00
8.00
Serum
AM
H (ng/m
l)
r= 0.07 p= 0.7

Fig (5 ) shows that there is a significant negative association between follicular fluid AMH and serum FSH (r =0.65, p =0.0001).
1500.001200.00900.00600.00300.000.00
Intrafollicular AMH (ng/ml)
8.00
6.00
4.00
2.00
Serum
FSH
(ng/m
l)
r= - 0.65 p= 0.0001

1500.001200.00900.00600.00300.000.00
Intrafollicular AMH (ng/ml)
40.00
30.00
20.00
10.00
0.00
Intr
afo
llic
ula
r E
str
adio
l (n
g/m
l)
r= - 0.47 p= 0.01
Fig (6) shows that there is a significant fair negative association between AMH and estradiol levels in follicular fluid with (r =-0.47, p =0.01).

Hormonal relation in this group revealed no association between AMH and testosterone in follicular fluid (r=0.24, p =0.3), no association between serum AMH and serum FSH (r=0.008, p=0.9), no association between serum AMH and follicular fluid esrtadiol (r=0.14, p =0.5) and no association between serum AMH and follicular fluid Testosterone (r=-0.16, p =0.4).

In the present study it was noted that there is a statistically significant higher levels of serum and follicular fluids’ AMH in study group than the controls. AMH alters FSH-sensitivity of the follicles leading to disturbance in the expression of the LH receptors of the growing follicle. So AMH prevents the FSH mediated selection of the follicle, prevents its removal and causes failure of its lutenization and rupture. This phenomenon may guide the growing follicle to lose its FSH-dependent maturation and lutenisation and to be transformed into cyst.

This explanation may shed some light about the resistance of these cysts to hormonal treatment.
High serum levels of AMH is a reflection of high FF AMH. High serum levels of AMH in cases with ovarian cyst may be used to distinguish cases that will respond to hormonal treatment from those which fail to achieve complete remission of their pathology.