Embed Size (px)
Citation preview
Motor Neuron Disease
Motor Neuron Disease
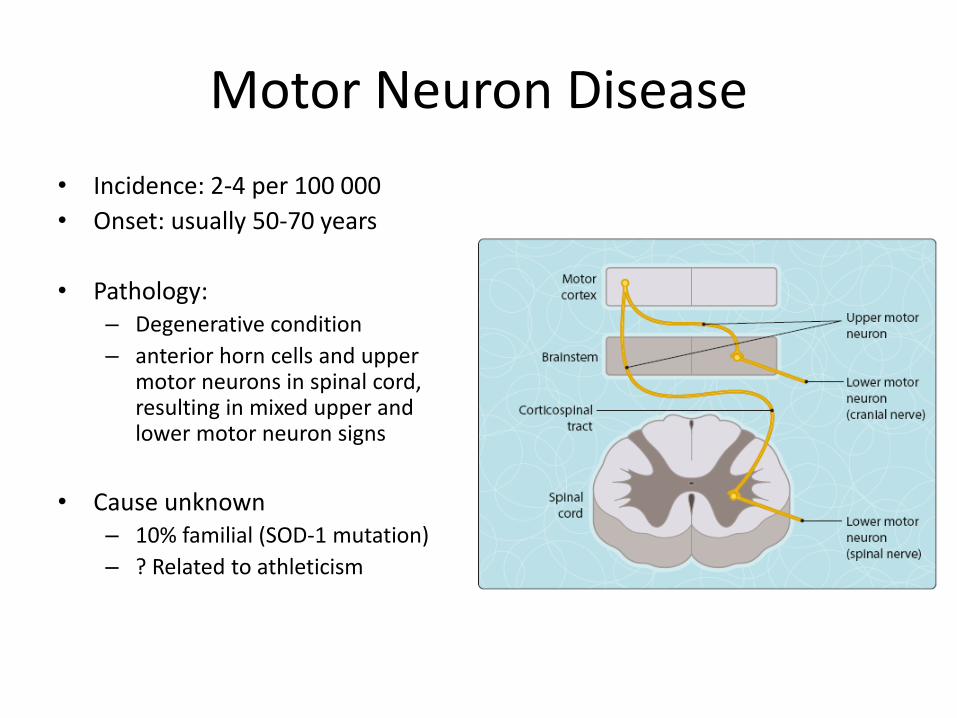
• Incidence: 2-4 per 100 000
• Onset: usually 50-70 years
• Pathology: – Degenerative condition
– anterior horn cells and upper motor neurons in spinal cord, resulting in mixed upper and lower motor neuron signs
• Cause unknown– 10% familial (SOD-1 mutation)
– ? Related to athleticism
Presentation
• Several variations in onset, but progress to the same endpoint
• Motor nerves only affected• May be just UMN or just LMN at onset, but other
features will appear over time
• Main patterns:– Amyotrophic lateral sclerosis– Bulbar presentaion– Primary lateral sclerosis (UMN onset)– Progressive muscular atrophy (LMN onset)
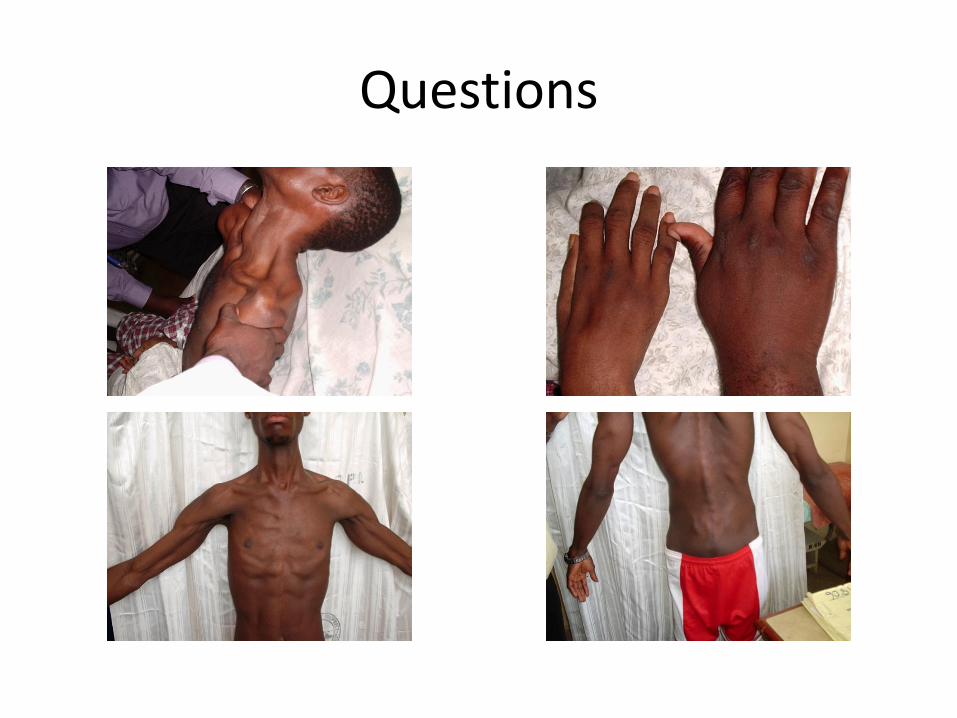
Questions
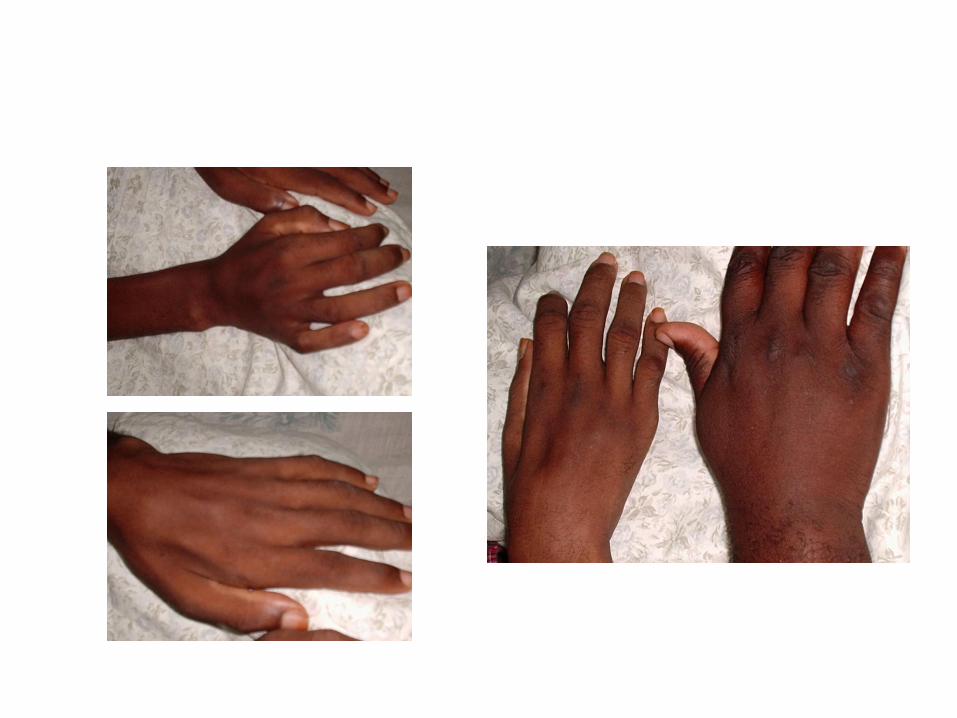
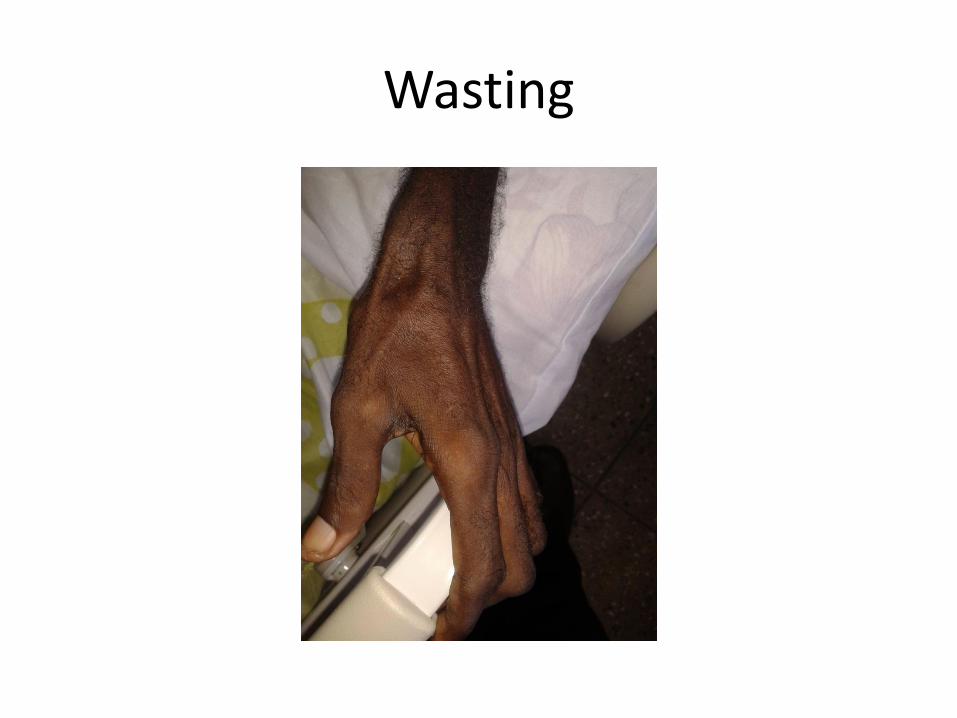
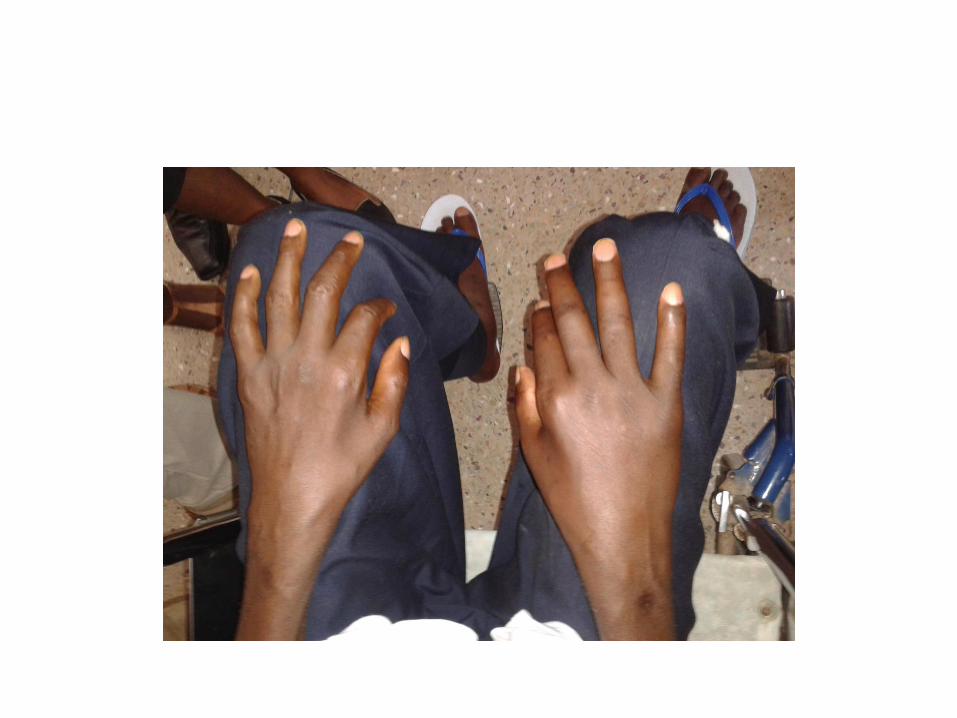
Wasting
Classification
• Amyotrophic Lateral Sclerosis
• Progressive Bulbar Palsy
• Progressive Muscular Atrophy
• Primary Lateral Sclerosis
• Multifocal Motor Neuropathy
• Spinal Muscular Atrophy
• Kennedy’s Disease
• Monomelic Amyotrophy
• Brachial Amyotrophic Diplegia
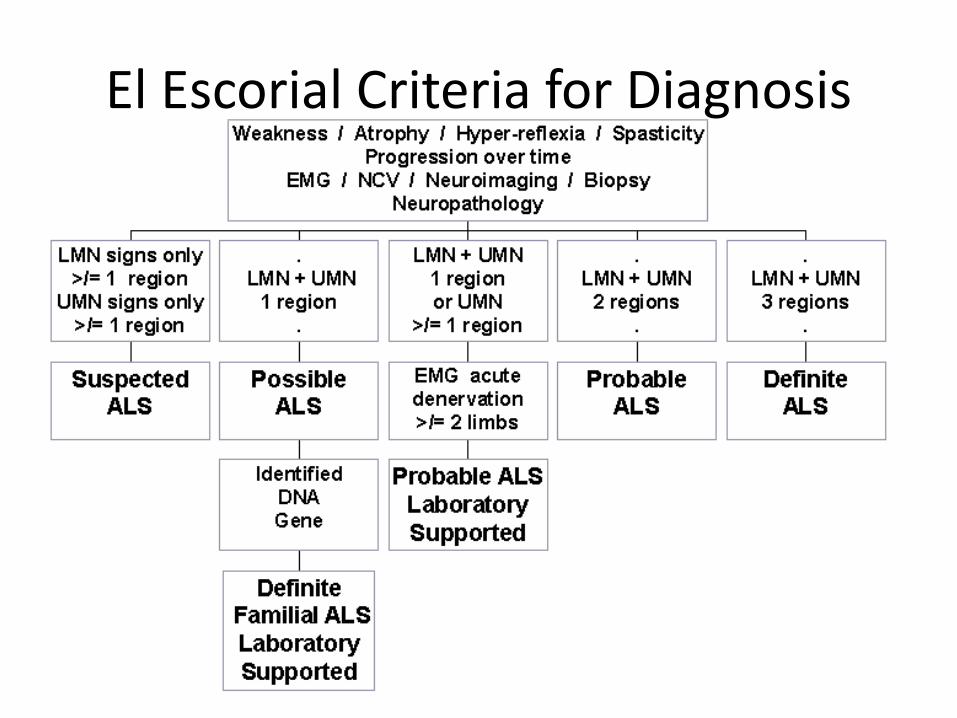
El Escorial Criteria for Diagnosis
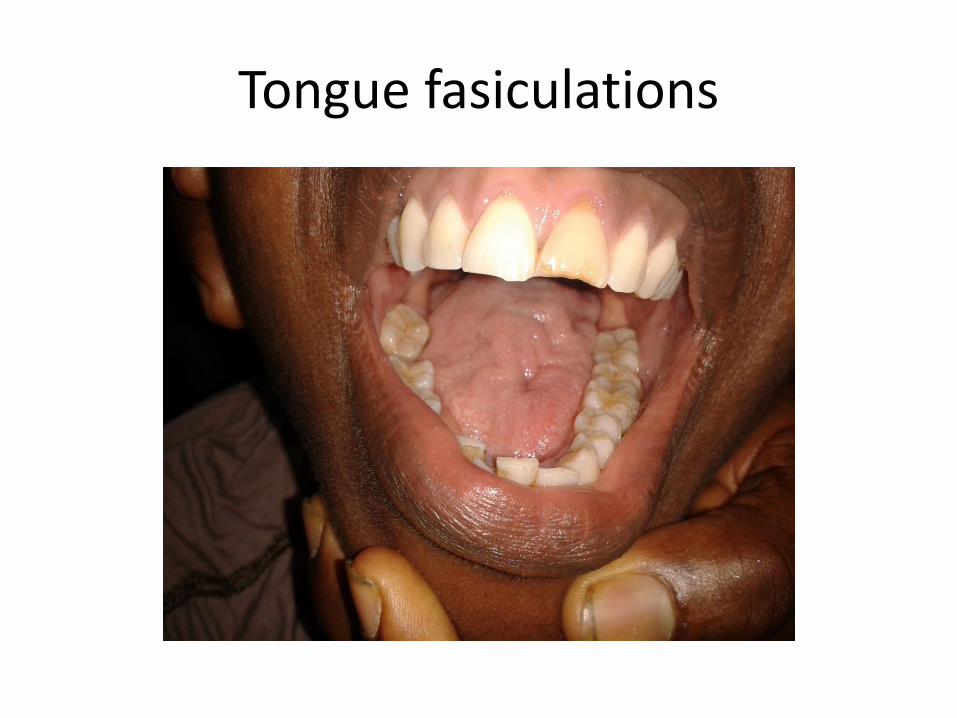
Tongue fasiculations
Amyotrophic lateral sclerosis
• ‘Typical’ presentation (60%+)• Usually one limb initially
– Foot drop– Clumsy weak hand– May complain of cramps
• Gradual progression over months
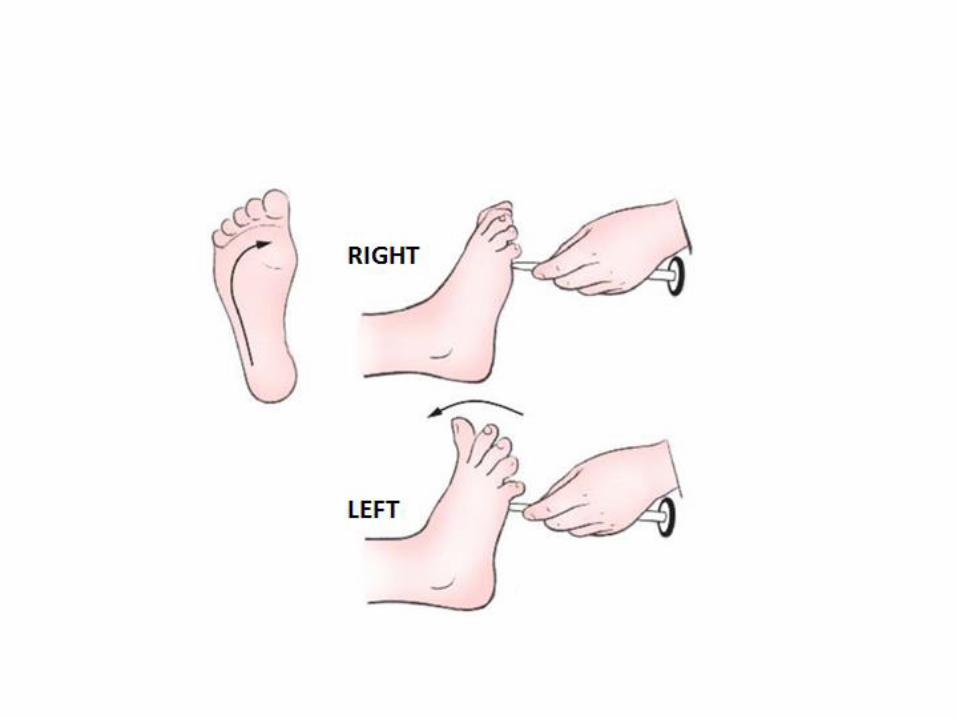
• May be some wasting at presentation• Usually fasiculations (often more widespread)• Brisk reflexes, extensor plantars• No sensory signs; MAY occasionally be mild symptoms
• Relentless progression, noticable over weeks/ months
Bulbar MND
• Approximately 30% of cases
• Onset with dysarthria, dysphagia
• Bulbar and pseudobulbar symptoms
• On examination– Dysarthria
– Tongue wasting, fasciculation
– Brisk jaw jerk
– May be other limb symptoms (but not always)
• Progression more rapid than ALS presentation
• Worse prognosis (approx 2 years)
Other presentations
• Primary lateral sclerosis (5%)
– Pure UMN onset
• Progressive muscular atrophy (5%)
– Pure LMN onset
– May be ‘flail limb’ appearance
• Probably slightly better prognosis

Progressive bulbar palsyDifficulty breathingMuscle weakness
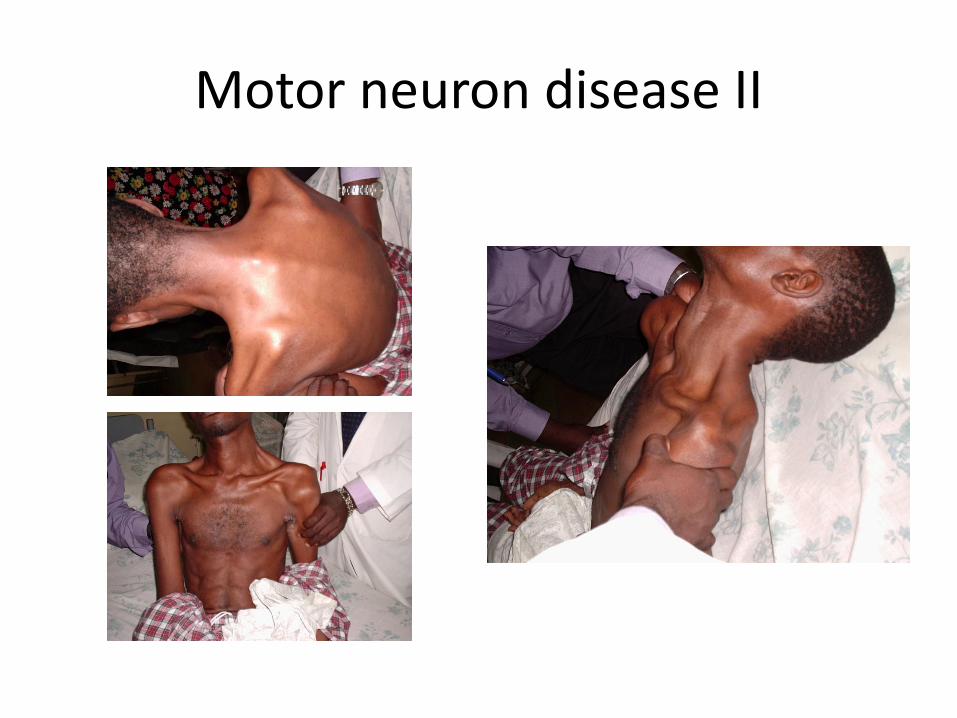
Motor neuron disease II
Differential diagnosis
• Diagnosis is clinical– EMG/ imaging may help
• MND is fatal – exclude other, less severe/treatable conditions
– Multilevel cervical/ lumbar degerative changes• May cause myelopathy + LMN features and fasciculation• Usually have sensory symptoms
– Benign fasciculation syndrome – Bulbar – cerebrovascular disease, MND
– Multifocal motor neuropathy– Hereditary spastic paraplegia– Kennedy’s disease (SMA)
Investigations
• Clinical diagnosis
• Check CK – modest elevation
• Investigations often aimed at excluding other causes– Often MRI cervical/lumbar spine– May image brain
• NCS/ EMG show “chronic active denervation” in areas supplied by multiple nerve roots (note this pattern may be seen in one territory by radiculopathy)
• Tongue/ Sternomastoid EMG sometimes performed
Treatment
• Riluzole– Glutamate antagonist – May extend left expectancy slightly (3-5 months on average)
– Low side effect profile• Occ nausea, fatigue• Can disturb LFTs (needs monitoring at onset)
– Expensive (?cost/ benefit)
• Palliative– Nutrition
• Soft diet• ‘Chin tuck’
– Hyoscine (excessive secretions/salivation)– Opiates/ benzodiazepines
MND dementia
• Proportion of patients develop frontotemporal dementia
– Flat affect
– Disinhibition
– Language disturbance/ dysphasia
– Impaired ‘executive function’
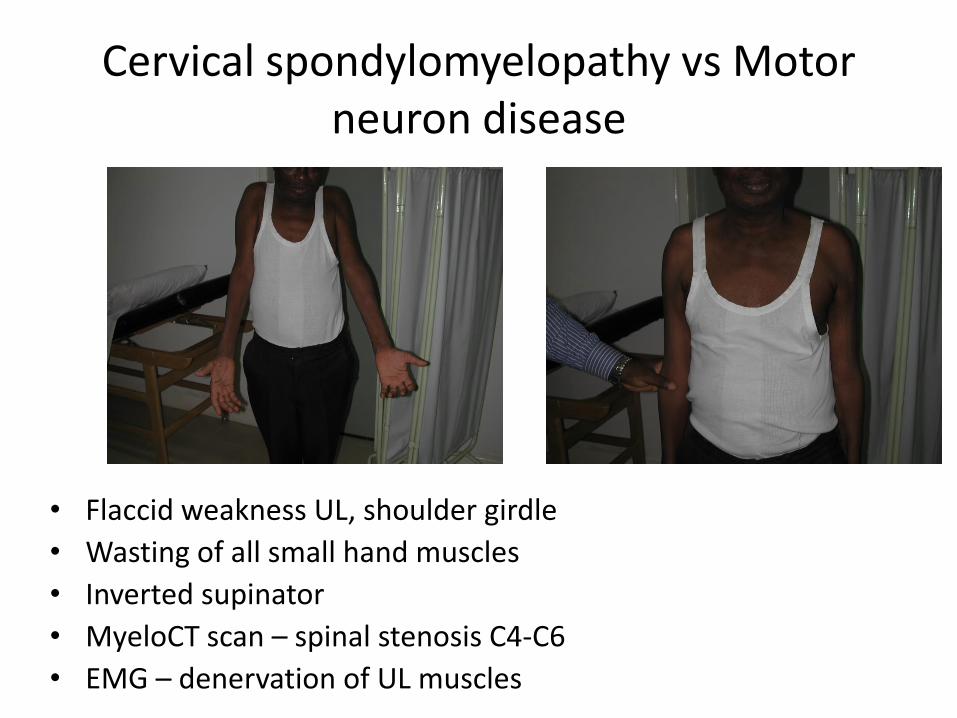
Cervical spondylomyelopathy vs Motor neuron disease
• Flaccid weakness UL, shoulder girdle
• Wasting of all small hand muscles
• Inverted supinator
• MyeloCT scan – spinal stenosis C4-C6
• EMG – denervation of UL muscles
Motor Neuron Disease
• Look for signs• Differential diagnosis• Counselling
• Good luck





























