Embed Size (px)
Citation preview
Motivational Interviewing to Improve Motivational Interviewing to Improve
Exercise Attitudes and Behavior: Exercise Attitudes and Behavior:
Implications for Antihypertensive TherapyImplications for Antihypertensive Therapy
Brian E. Sandoval, M.A.Brian E. Sandoval, M.A.
Stephanie C. Wood, Ph.D., MHAStephanie C. Wood, Ph.D., MHA
Christopher A. Neumann, Ph.D.Christopher A. Neumann, Ph.D.
Beverly Spray, Ph.D.Beverly Spray, Ph.D.
The School of Professional Psychology The School of Professional Psychology
at Forest Instituteat Forest Institute
Springfield, MissouriSpringfield, Missouri

Purpose of the Current Study:Purpose of the Current Study:�� To determine how Motivational Interviewing (MI) impacts To determine how Motivational Interviewing (MI) impacts
hypertension patientshypertension patients’’ adherence to exercise recommendations adherence to exercise recommendations
in primary carein primary care
�� Specifically, the current study examines how MI influences:Specifically, the current study examines how MI influences:
�� 1. Exercise behaviors1. Exercise behaviors
�� 2. Behavior change factors2. Behavior change factors
�� Stages of ChangeStages of Change
�� Intrinsic MotivationIntrinsic Motivation
�� SelfSelf--EfficacyEfficacy
Overview of HypertensionOverview of Hypertension
�� More than 73 million people in the U.S. have a diagnosis More than 73 million people in the U.S. have a diagnosis
of hypertension (140/90 mm Hg) and over 1 billion of hypertension (140/90 mm Hg) and over 1 billion
worldwide worldwide (AHA, 2009)(AHA, 2009)
�� Hypertension is a primary or contributing cause of Hypertension is a primary or contributing cause of
319,000 deaths annually and is a risk factor for stroke, 319,000 deaths annually and is a risk factor for stroke,
heart attack, and CHF which account for more than heart attack, and CHF which account for more than
50% of all deaths nationwide 50% of all deaths nationwide (Gatchel & Oordt, 2003)(Gatchel & Oordt, 2003)
�� Total expenditures are estimated at $73 billion annually Total expenditures are estimated at $73 billion annually
which is nearly twice the costs in 1999 which is nearly twice the costs in 1999 (AHA, 2009)(AHA, 2009)
Treatment Failure and NonTreatment Failure and Non--AdherenceAdherence
�� Only 25%Only 25% of hypertension patients have wellof hypertension patients have well--controlled blood controlled blood
pressure despite an abundance of lifestyle and pharmacologic pressure despite an abundance of lifestyle and pharmacologic
treatments available (treatments available (JNC, 2004)JNC, 2004)
�� NonNon--adherenceadherence is one of most common obstacles to treatment is one of most common obstacles to treatment
success, with 30% to 60% of patients NOT following success, with 30% to 60% of patients NOT following
recommendations recommendations (Baum et al., 1997)(Baum et al., 1997)
�� Among all antihypertensive therapies, physical Among all antihypertensive therapies, physical exerciseexercise programs programs
account for the account for the lowest levels of adherencelowest levels of adherence, with rates as low as , with rates as low as
14% to 17% 14% to 17% (Brodie & Inoue, 2005)(Brodie & Inoue, 2005)
�� However, exercise significantly reduces blood pressure in However, exercise significantly reduces blood pressure in
monotherapymonotherapy (Bacon et al., 2004) (Bacon et al., 2004) and and combinationcombination therapy therapy (Villareal et al., 2006) (Villareal et al., 2006)
while also leading to additional while also leading to additional CV risk reductionsCV risk reductions (Reaven et al., 1996)(Reaven et al., 1996)
Motivational Interviewing to Improve AdherenceMotivational Interviewing to Improve Adherence
�� Motivational Interviewing (MI) is Motivational Interviewing (MI) is ““a directive, clienta directive, client--centered centered counseling style for eliciting behavior change by helping patiencounseling style for eliciting behavior change by helping patients ts
explore and resolve ambivalenceexplore and resolve ambivalence”” (Rollnick & Miller, 1995, p. 325)(Rollnick & Miller, 1995, p. 325)
�� MI is wellMI is well--researched and has been shown to have positive researched and has been shown to have positive outcomes for alcohol, drugs, diet, and outcomes for alcohol, drugs, diet, and exerciseexercise(Burke et al., 2003; Dunn et al., 2001)(Burke et al., 2003; Dunn et al., 2001)
�� Only 3 studies total have examined MI and exercise in a Only 3 studies total have examined MI and exercise in a cardiovascular population, with only 1 study including patients cardiovascular population, with only 1 study including patients whose primary diagnosis was hypertension whose primary diagnosis was hypertension (Woollard et al., 1995).(Woollard et al., 1995).
�� Although understudied, these trials provide some support for MI Although understudied, these trials provide some support for MI to improve treatment adherence for a cardiovascular populationto improve treatment adherence for a cardiovascular population
(Brodie & Inoue, 2005; Brodie, Inoue, & Shaw, 2008; Woollard et (Brodie & Inoue, 2005; Brodie, Inoue, & Shaw, 2008; Woollard et al., 1995)al., 1995)
Purpose of Current StudyPurpose of Current Study
1) 1) To determine if MI can impact To determine if MI can impact exercise behavior changeexercise behavior change
for patients with hypertension for patients with hypertension
((Goal: Improve adherence by increasing exercise Goal: Improve adherence by increasing exercise behaviorsbehaviors ))
Hypothesis: Hypothesis:
Patients receiving MI would have better increases in Patients receiving MI would have better increases in exercise behavior exercise behavior
compared to those receiving a standard recommendation.compared to those receiving a standard recommendation.
Purpose of Current StudyPurpose of Current Study
2) To determine how MI influences 2) To determine how MI influences behavior change behavior change factorsfactors for hypertension patientsfor hypertension patients
(Goal: Improve exercise adherence by impacting (Goal: Improve exercise adherence by impacting change factorschange factors))
A) Stages of ChangeA) Stages of Change
B) Intrinsic MotivationB) Intrinsic Motivation
C) SelfC) Self--EfficacyEfficacy
Hypothesis:Hypothesis:
Patients receiving a MI session will experience better gains in Patients receiving a MI session will experience better gains in exercise change factorsexercise change factors when compared those receiving a standardwhen compared those receiving a standard
recommendationrecommendation
MethodsMethodsParticipantsParticipantsRecruited from outpatient primary health care clinic for low incRecruited from outpatient primary health care clinic for low income and uninsuredome and uninsured
Inclusion CriteriaInclusion Criteria
�� Age Age >> 18 years18 years
�� Hypertension diagnosis (SBP Hypertension diagnosis (SBP >> 140 mm Hg or DBP 140 mm Hg or DBP >> 90 mm Hg) 90 mm Hg)
�� Medically Suitable for ExerciseMedically Suitable for Exercise
�� Available for 30 day followAvailable for 30 day follow--up appointmentup appointment
Exclusion CriteriaExclusion Criteria
�� Age < 18 yearsAge < 18 years
�� No diagnosis of hypertensionNo diagnosis of hypertension
�� Contraindication or Inability to ExerciseContraindication or Inability to Exercise
�� Patients leaving clinic or Unavailable for 30 day followPatients leaving clinic or Unavailable for 30 day follow--upup
MethodsMethodsProceduresProcedures
�� Patients who met inclusion criteria were contacted by phonePatients who met inclusion criteria were contacted by phone
�� Those who agreed to participate were asked to arrive approximateThose who agreed to participate were asked to arrive approximately ly 1 hour prior to their scheduled appointment1 hour prior to their scheduled appointment
�� After informed consent, patients were randomly assigned to MI GrAfter informed consent, patients were randomly assigned to MI Group oup or ST Groupor ST Group
MI GroupMI Group
Completed measures, received 30 minute MI sessCompleted measures, received 30 minute MI sessionion
ST GroupST Group
Completed measures, received standard exercise recoCompleted measures, received standard exercise recommendation and mmendation and
psychoeducational handoutpsychoeducational handout
�� ALLALL patients were scheduled for 30 day followpatients were scheduled for 30 day follow--up to complete measuresup to complete measures
MethodsMethods
MeasuresMeasures
�� Godin LeisureGodin Leisure--Time Exercise QuestionnaireTime Exercise Questionnaire (LTEQ)(LTEQ)
(Godin & Shepard, 1985)(Godin & Shepard, 1985)
�� University of Rhode Island Change Assessment University of Rhode Island Change Assessment ––
Exercise 2Exercise 2 (URICA(URICA--E2)E2)
(Marcus et al., 1992; Reed, 1994)(Marcus et al., 1992; Reed, 1994)
�� Intrinsic Motivation InventoryIntrinsic Motivation Inventory (IMI)(IMI)
((Buckworth et al., 2007)Buckworth et al., 2007)
�� Barriers SelfBarriers Self--Efficacy ScaleEfficacy Scale (BARSE)(BARSE)
(McAuley, 1992)(McAuley, 1992)
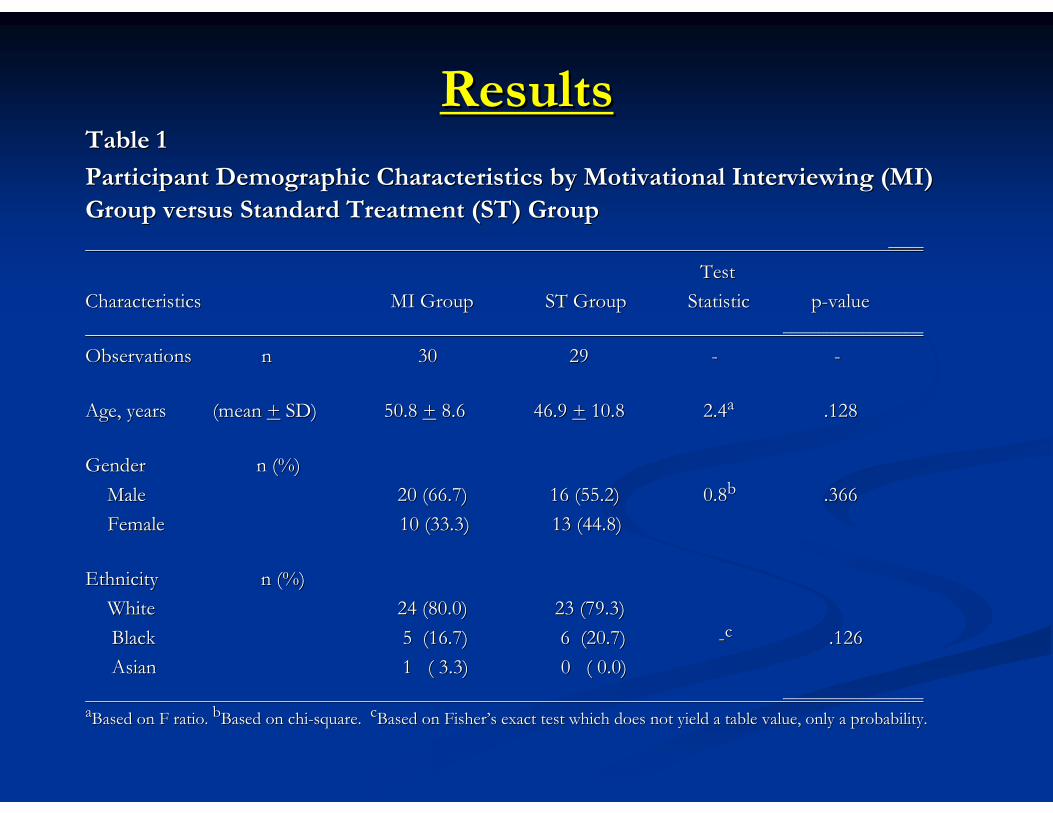
ResultsResultsTable 1Table 1
Participant Demographic Characteristics by Motivational IntervieParticipant Demographic Characteristics by Motivational Interviewing (MI) wing (MI)
Group versus Standard Treatment (ST) GroupGroup versus Standard Treatment (ST) Group
________
TestTest
Characteristics MI Group Characteristics MI Group ST Group Statistic pST Group Statistic p--value value
________________________________
ObservationsObservations nn 3030 29 29 -- --
Age, years (mean Age, years (mean ++ SD) 50.8 SD) 50.8 ++ 8.68.6 46.9 46.9 ++ 10.810.8 2.42.4aa .128.128
GenderGender n (%)n (%)
MaleMale 20 (66.7) 16 (55.2)20 (66.7) 16 (55.2) 0.80.8bb .366.366
FemaleFemale 10 (33.3) 13 (44.8)10 (33.3) 13 (44.8)
Ethnicity n (%)Ethnicity n (%)
WhiteWhite 24 (80.0) 23 (79.3)24 (80.0) 23 (79.3)
BlackBlack 5 (16.7) 6 (20.7)5 (16.7) 6 (20.7) --cc .126.126
AsianAsian 1 ( 3.3) 0 ( 0.0)1 ( 3.3) 0 ( 0.0)
________________________________aaBased on F ratio. Based on F ratio. bbBased on chiBased on chi--square. square. ccBased on FisherBased on Fisher’’s exact test which does not yield a table value, only a probabils exact test which does not yield a table value, only a probability.ity.
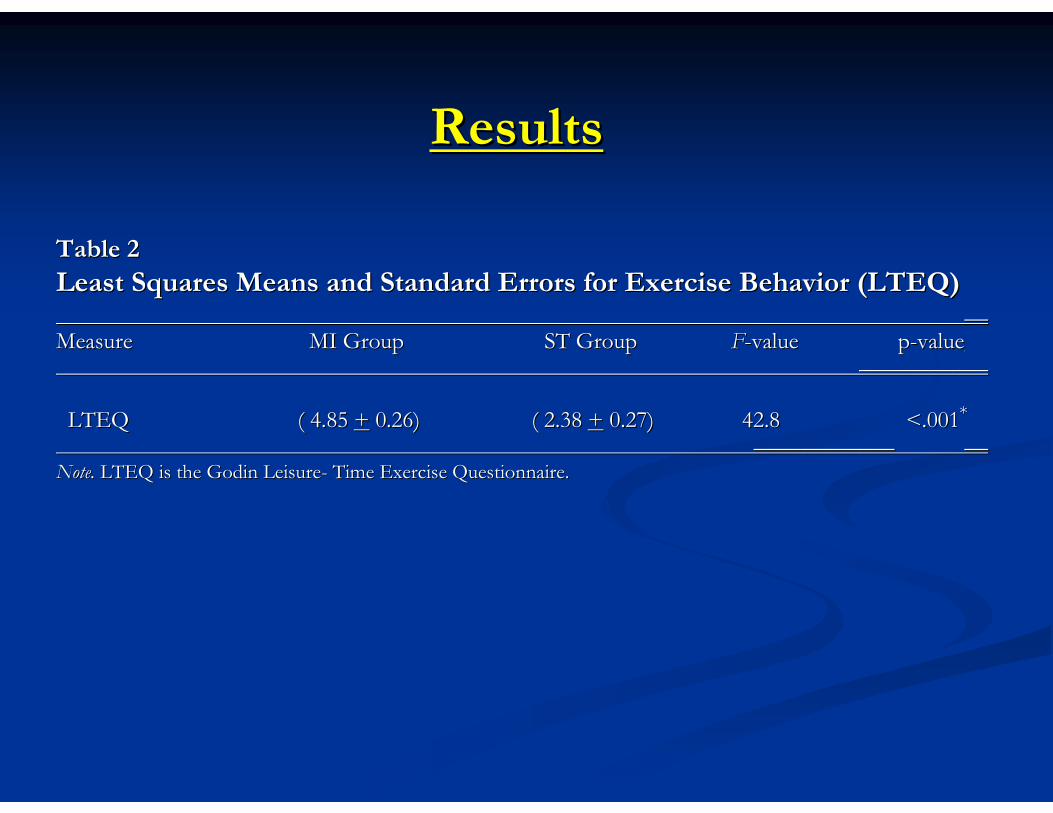
ResultsResults
Table 2Table 2
Least Squares Means and Standard Errors for Exercise Behavior (LLeast Squares Means and Standard Errors for Exercise Behavior (LTEQ)TEQ)____
Measure Measure MI Group ST Group MI Group ST Group FF--value pvalue p--valuevalue______________________
LTEQ LTEQ ( 4.85 ( 4.85 ++ 0.26) ( 2.38 0.26) ( 2.38 ++ 0.27) 42.8 0.27) 42.8 <.001<.001**
________________________ ____
Note.Note. LTEQ is the Godin LeisureLTEQ is the Godin Leisure-- Time Exercise Questionnaire.Time Exercise Questionnaire.
ResultsResults
ResultsResults
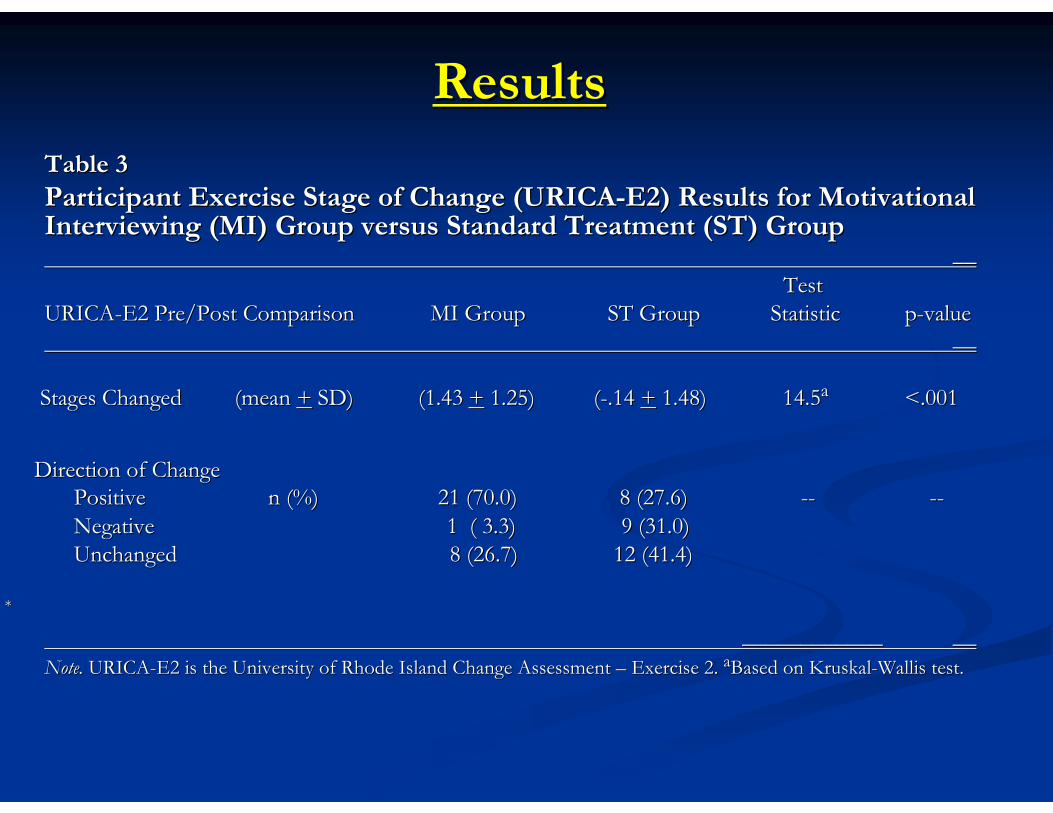
Table 3Table 3
Participant Exercise Stage of Change (URICAParticipant Exercise Stage of Change (URICA--E2) Results for Motivational E2) Results for Motivational Interviewing (MI) Group versus Standard Treatment (ST) GroupInterviewing (MI) Group versus Standard Treatment (ST) Group
____
TestTest
URICAURICA--E2 Pre/Post Comparison MI Group ST GrouE2 Pre/Post Comparison MI Group ST Group Statistic pp Statistic p--valuevalue
____
Stages Changed (mean Stages Changed (mean ++ SD) (1.43 SD) (1.43 ++ 1.25) (1.25) (--.14 .14 ++ 1.48) 14.51.48) 14.5aa <.001<.001
Direction of ChangeDirection of Change
PositivePositive n (%)n (%) 21 (70.0)21 (70.0) 8 (27.6)8 (27.6) ---- ----
Negative 1Negative 1 ( 3.3) 9 (31.0)( 3.3) 9 (31.0)
UnchangedUnchanged 8 (26.7)8 (26.7) 12 (41.4)12 (41.4)
**
________________________ ____
Note.Note. URICAURICA--E2 is the University of Rhode Island Change Assessment E2 is the University of Rhode Island Change Assessment –– Exercise 2. Exercise 2. aaBased on KruskalBased on Kruskal--Wallis test.Wallis test.
ResultsResults
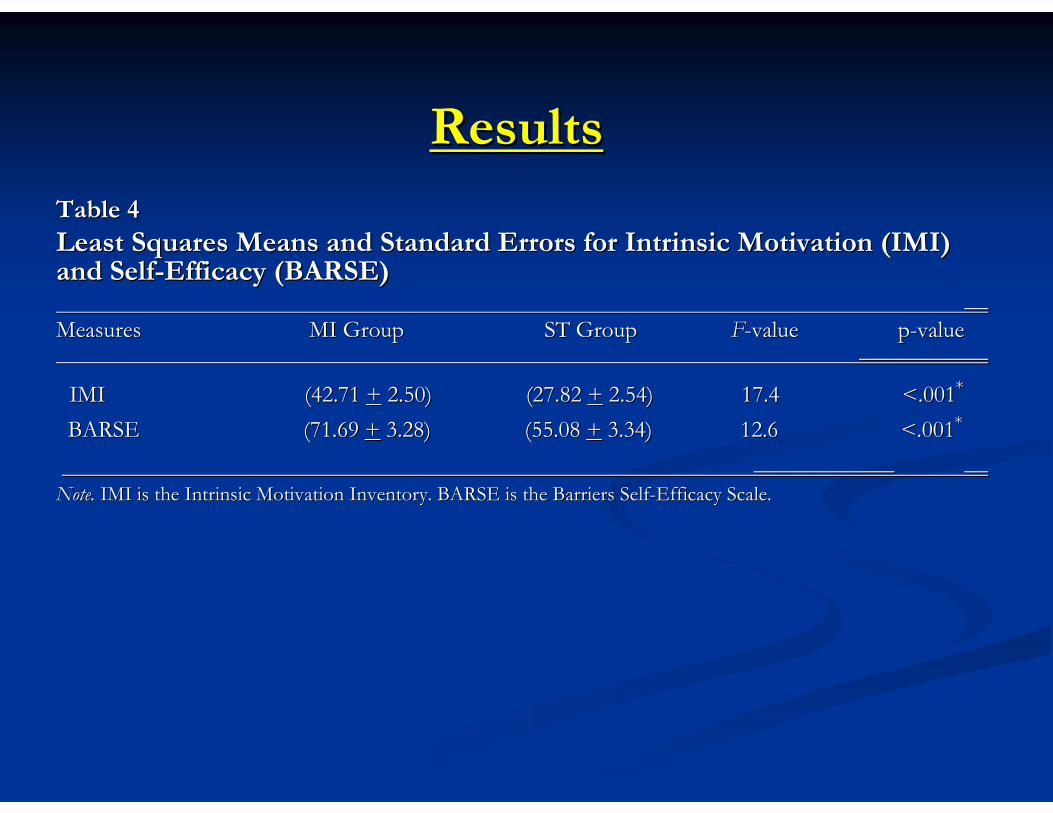
Table 4Table 4
Least Squares Means and Standard Errors for Intrinsic MotivationLeast Squares Means and Standard Errors for Intrinsic Motivation (IMI) (IMI) and Selfand Self--Efficacy (BARSE)Efficacy (BARSE)
____
Measures Measures MI Group ST Group MI Group ST Group FF--value pvalue p--valuevalue______________________
IMI (42.71 IMI (42.71 ++ 2.50) (27.82 2.50) (27.82 ++ 2.54) 17.4 <.0012.54) 17.4 <.001**
BARSE (71.69 BARSE (71.69 ++ 3.28) (55.08 3.28) (55.08 ++ 3.34) 12.6 <.0013.34) 12.6 <.001**
________________________ ____
Note.Note. IMI is the Intrinsic Motivation Inventory. BARSE is the BarrierIMI is the Intrinsic Motivation Inventory. BARSE is the Barriers Selfs Self--Efficacy Scale. Efficacy Scale.
DiscussionDiscussion
It was HypothesizedIt was Hypothesized::
Patients receiving MI would have better increases in Patients receiving MI would have better increases in exercise exercise behaviorbehavior compared to those receiving a standard recommendation.compared to those receiving a standard recommendation.
�� This hypothesis was This hypothesis was CONFIRMEDCONFIRMED
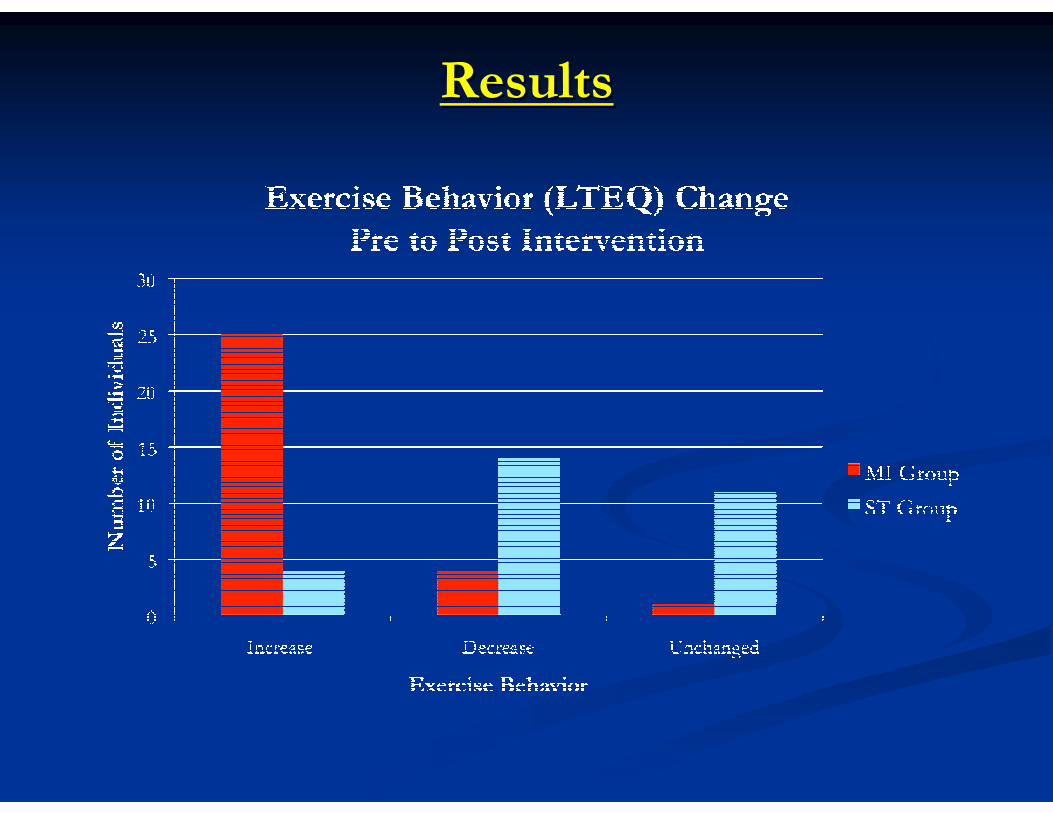
�� MI helped increase frequency and/or strenuousness of exercise MI helped increase frequency and/or strenuousness of exercise behaviors according to LTEQbehaviors according to LTEQ
�� Consistent with previous studies examining MIConsistent with previous studies examining MI’’s impact on exercise s impact on exercise behaviors for CHF (Brodie & Inoue, 2005) and other chronic diseabehaviors for CHF (Brodie & Inoue, 2005) and other chronic diseases ses (Ang et al., 2007; Bennett et al., 2007)(Ang et al., 2007; Bennett et al., 2007)
�� MI facilitated exercise behavior increases regardless of initialMI facilitated exercise behavior increases regardless of initialactivity levelactivity level
DiscussionDiscussion
It was HypothesizedIt was Hypothesized::
Patients receiving a MI session will experience better gains in Patients receiving a MI session will experience better gains in exercise change factorsexercise change factors when compared those receiving a standard when compared those receiving a standard
recommendationrecommendation
�� This hypothesis was also This hypothesis was also CONFIRMEDCONFIRMED
�� The MI Group had a The MI Group had a mean increasemean increase of nearly 1.5 Stages of Change, of nearly 1.5 Stages of Change, while ST Group showed while ST Group showed no mean changeno mean change with a slight decrease.with a slight decrease.
�� PostPost--intervention, the MI Group had significantly higher mean IMI intervention, the MI Group had significantly higher mean IMI and BARSE scores when compared to the ST Groupand BARSE scores when compared to the ST Group
�� Results provide insight into Results provide insight into howhow MI impacts the process of changeMI impacts the process of change
�� Addresses gap in literature Addresses gap in literature -- Few published trials have demonstrated Few published trials have demonstrated
how MI influences intrinsic motivation and selfhow MI influences intrinsic motivation and self--efficacyefficacy
DiscussionDiscussion
LimitationsLimitations�� Small Sample Size (n = 59)Small Sample Size (n = 59)
�� Racially homogenous sample (80% White)Racially homogenous sample (80% White)
�� Sample predominately middleSample predominately middle--agedaged
�� Short duration of followShort duration of follow--up to MI sessionup to MI session
�� Unequal time spent with MI vs. ST groupsUnequal time spent with MI vs. ST groups
StrengthsStrengths�� Brief MI session likely adaptable to other primary care/hospitalBrief MI session likely adaptable to other primary care/hospital settingssettings
�� LowLow--income sample (greater barriers to adherence)income sample (greater barriers to adherence)
�� Randomization produced homogenous groups for Randomization produced homogenous groups for comparisoncomparison
DiscussionDiscussion
Future DirectionsFuture Directions
�� Replicate current study design with larger, more diverse sampleReplicate current study design with larger, more diverse sample
�� Examine MIExamine MI’’s impact over longs impact over long--term followterm follow--up appointments up appointments
�� Assess if MI increases adherence for other antihypertensive Assess if MI increases adherence for other antihypertensive
therapiestherapies
DiscussionDiscussion
Implications for FindingsImplications for Findings
�� By demonstrating utility of one brief MI session may lead to incBy demonstrating utility of one brief MI session may lead to increased reased
utilization in primary careutilization in primary care
�� Understanding Understanding howhow MI affects MI affects behavior change factorsbehavior change factors may help may help
practitioners become more effective at delivering MI interventiopractitioners become more effective at delivering MI interventionsns
�� By improving exercise adherence, may rely less on pharmacologic By improving exercise adherence, may rely less on pharmacologic therapytherapy
�� Better adherence to hypertension treatment would lead to decreasBetter adherence to hypertension treatment would lead to decreased costs ed costs
to the patient and health care system as a wholeto the patient and health care system as a whole
ReferencesReferences
American Heart Association (2009). American Heart Association (2009). Heart disease and stroke statistics Heart disease and stroke statistics –– 2009 Update (AHA 2009).2009 Update (AHA 2009). Dallas, TX: Dallas, TX:
American Heart Association.American Heart Association.
Ang, D., Kesavalu, R., Lydon, J., Lane, K., & Bigatti, S. (2007)Ang, D., Kesavalu, R., Lydon, J., Lane, K., & Bigatti, S. (2007). Exercise. Exercise--based motivational interviewing for female based motivational interviewing for female
patients with fibromyalgia: A case series. patients with fibromyalgia: A case series. Clinical Rheumatology, 26, Clinical Rheumatology, 26, 18431843--1849.1849.
Bacon, S., Sherwood, A., Hinderliter, A., & Blumenthal, J. (2004Bacon, S., Sherwood, A., Hinderliter, A., & Blumenthal, J. (2004). Effects of exercise, diet, and weight loss on high ). Effects of exercise, diet, and weight loss on high
blood pressure. blood pressure. Sports Medicine, 34, Sports Medicine, 34, 307307--316.316.
Baum, A., Gatchel, R., & Krantz, D. (Eds.). (1997). Baum, A., Gatchel, R., & Krantz, D. (Eds.). (1997). An introduction to health psychologyAn introduction to health psychology (3rd ed.). New York: McGraw (3rd ed.). New York: McGraw
Hill.Hill.
Bennett, J., Lyons, K., WintersBennett, J., Lyons, K., Winters--Stone, K., Nail, L., & Scherer, J. (2007). Motivational intervieStone, K., Nail, L., & Scherer, J. (2007). Motivational interviewing to increase wing to increase
physical activity in longphysical activity in long--term cancer survivors. A randomized controlled trial. term cancer survivors. A randomized controlled trial. Nursing Research, 56, Nursing Research, 56, 1818--27.27.
Brodie, D., & Inoue, A. (2005). Motivational interviewing to proBrodie, D., & Inoue, A. (2005). Motivational interviewing to promote physical activity or people with chronic heart mote physical activity or people with chronic heart
failure. failure. Journal of Advanced Nursing, 50, Journal of Advanced Nursing, 50, 518518--527.527.
Brodie, D., Inoue, A., & Shaw, D.G. (2008). Motivational interviBrodie, D., Inoue, A., & Shaw, D.G. (2008). Motivational interviewing to change quality of life for people with ewing to change quality of life for people with
chronic heart failure: A randomized controlled trial. chronic heart failure: A randomized controlled trial. International Journal of Nursing Studies, 45, International Journal of Nursing Studies, 45, 489489--500.500.
Buckworth, J., Lee, R.E., Regan, G., Schneider, L.K., & DiClemenBuckworth, J., Lee, R.E., Regan, G., Schneider, L.K., & DiClemente, C.C. (2007). Decomposing intrinsic and te, C.C. (2007). Decomposing intrinsic and
extrinsic motivation for exercise: Application to stages of motiextrinsic motivation for exercise: Application to stages of motivational readiness. vational readiness. Psychology of Sport and Exercise, Psychology of Sport and Exercise,
8, 8, 441441--461.461.
ReferencesReferences
Burke, B., Arkowitz, H., & Menchola, M. (2003). The efficacy of Burke, B., Arkowitz, H., & Menchola, M. (2003). The efficacy of motivational interviewing: A metamotivational interviewing: A meta--analysis of analysis of controlled clinical trials. controlled clinical trials. Journal of Consulting and Clinical Psychology, 71, Journal of Consulting and Clinical Psychology, 71, 843843--861.861.
Dunn, C., Deroo, L., & Rivara, F. (2001). Dunn, C., Deroo, L., & Rivara, F. (2001). The use of brief interventions adapted from motivational interviThe use of brief interventions adapted from motivational interviewing ewing across behavioral domains: A systematic review. across behavioral domains: A systematic review. Addiction, 96, Addiction, 96, 17251725--1742.1742.
Gatchel, R., & Oordt, M. (2003). Gatchel, R., & Oordt, M. (2003). Clinical health psychology and primary care. Clinical health psychology and primary care. Washington, D.C.: American Psychological Washington, D.C.: American Psychological Association.Association.
Godin, G., & Shepherd, R. (1985). A simple method to assess exerGodin, G., & Shepherd, R. (1985). A simple method to assess exercise behavior in the community. cise behavior in the community. Canadian Journal Canadian Journal
of Applied Sport Science, 10, of Applied Sport Science, 10, 141141--146.146.
Joint National Committee on Detection, Evaluation, and TreatmentJoint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. (2004). of High Blood Pressure. (2004). The seventh The seventh
report of the Joint National Committee on Detection, Evaluation,report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC)and Treatment of High Blood Pressure (JNC). Bethesda, . Bethesda,
MD: National Heart, Lung, and Blood Institute. MD: National Heart, Lung, and Blood Institute.
Marcus, B.H., Selby, V.C., Niaura, R.S., & Rossi, J.S. (1992). SMarcus, B.H., Selby, V.C., Niaura, R.S., & Rossi, J.S. (1992). Selfelf--efficacy and the stages of exercise behavior change. efficacy and the stages of exercise behavior change.
Research Quarterly for Exercise and Sport, 63, Research Quarterly for Exercise and Sport, 63, 6060--66.66.
McAuley, E. (1992). The role of efficacy cognitions in the prediMcAuley, E. (1992). The role of efficacy cognitions in the prediction of exercise behavior in middlection of exercise behavior in middle--aged adults. aged adults.
Journal of Behavioral Medicine, 15, Journal of Behavioral Medicine, 15, 6565--88.88.
Reaven, G., Lithell, H., & Landsberg, L. (1996). Hypertension anReaven, G., Lithell, H., & Landsberg, L. (1996). Hypertension and associated metabolic abnormalities: The role of d associated metabolic abnormalities: The role of
insulin resistance and the sympathoadrenal system. insulin resistance and the sympathoadrenal system. New England Journal of Medicine, 334, New England Journal of Medicine, 334, 374374--381.381.
ReferencesReferences
Reed, G.R. (1994). Reed, G.R. (1994). Measuring stage of change for exercise behavior change, URICAMeasuring stage of change for exercise behavior change, URICA--E2E2. Unpublished doctoral dissertation, . Unpublished doctoral dissertation,
University of Rhode Island.University of Rhode Island.
Rollnick, S., & Miller, W. (1995). What is motivational intervieRollnick, S., & Miller, W. (1995). What is motivational interviewing? wing? Behavioral and Cognitive Psychotherapy, 23, Behavioral and Cognitive Psychotherapy, 23, 325325--334.334.
Villareal, D., Miller, B., Banks, M., Fontana, L., Sinacore, D.,Villareal, D., Miller, B., Banks, M., Fontana, L., Sinacore, D., & Klein, S. (2006). Effect of lifestyle intervention on & Klein, S. (2006). Effect of lifestyle intervention on
metabolic coronary heart disease risk factors in obese older adumetabolic coronary heart disease risk factors in obese older adults. lts. American Journal of Clinical Nutrition, 84, American Journal of Clinical Nutrition, 84, 13171317--
1323.1323.
Woollard, J., Beilin, L., Lord, T., Puddey, I., MacAdam, D., & RWoollard, J., Beilin, L., Lord, T., Puddey, I., MacAdam, D., & Rouse, I. (1995). A controlled trial of nurse ouse, I. (1995). A controlled trial of nurse
counseling on lifestyle change for hypertensives treated in genecounseling on lifestyle change for hypertensives treated in general practice: Preliminary results. ral practice: Preliminary results. Clinical and Clinical and
Experimental Pharmacology and Physiology, 23, Experimental Pharmacology and Physiology, 23, 466466--468.468.