Embed Size (px)
DESCRIPTION
Citation preview

Motivational Motivational Interviewing in Primary Interviewing in Primary Care: Quick Start GuideCare: Quick Start Guide
Carvajal de la Torre, Ana
Novo Rodríguez, Jesús
Campíñez Navarro, Manuel

Changing behaviours:The usual consultation – Where is the problem?

Changing behaviours:The usual consultation – Where is the problem?
-Up to 50% of non adherence for medical treatments in chronic conditions (HT, Cholesterol, DM2)
-DM patients refer suffering and revolt due to restrictions imposed by diet, physical activity and medication.
-Difficulties for counselling in Primary Care: expectancies (“people want treatments, doctors want success)”; lack of training…(DEmack1987)
-Doctors think that 3 most important CVRF (tobacco /HT / Chol) can be modified, but have low confidence in their ability to influence them – specially tobacco (Mann 1989)

Exercise:Pairing with your colleague, identify any type of
barriers /difficulties for change in this consultation (barriers from the patient, from the doctor, from the encounter...) 2min.
(We are not going to use them, the exercise is just to make a reflection on it!).

GP- Let´s talk about things we can try: diet and exercise. What about diet?P – Well, for me is difficult because when I feel anxious -I recognize- I eat a lot. It is difficult for me to control myself.GP – In that case you must try, at least, to eat low-fat meals.P – Yes, but it is difficult when you have to have meals outside!GP- And what about exercise? Can you try to do some more exercise?P – Oh, yes, I like walking, but I have almost no time for it…GP – You can try a little everyday…we consider it is enough 20 -30 min walking.P – Yes, but…when I finish lunch, I have to come back to work. And in the evenings, I feel so tired that I don’t want to go for a walk…what I really like is watching TV or having a beer with friendsGP – Yes. But it is necessary for you, if you want to prevent cardiovascular diseases, as you told me. We must do something about this. P – Yeees but…I understand, I am worried about it, but it seems difficult for me now. I try my best but…

Some theories to explain usual health behaviour
Protection Motivation Theory:
“A person tends to protect him or herself from a emergent risk if the threat is harmful and severe, if the behaviour advocated is seen as effective and achievable (few barriers) and if there is little benefit in a maladaptive behaviour”

Some theories to explain usual health behaviour
“Extended Parallel Process Model”:
When there is a threat, a person first assesses severity and susceptibility of the health threat. If these are perceived as low, one will cease to process the message. If perceived as high, then one assesses self-efficacy and response efficacy of the solution being offered

Some theories to explain usual health behaviour
“Theory of Planned Behaviour”:
Intentions to perform a behaviour can be predicted from:Attitudes toward the behaviourSubjective norms (“what others think”)Perceived behavioural control (self –efficacy)
Individuals weigh their own attitudes against their perceptions of others’ attitudes. If there is discordance, they decide how to behave based upon costs and benefits.

Some theories to explain usual health behaviour
“Cognitive Dissonance Theory”:
It focuses on the relationship among cognitive elements (beliefs, opinions, attitudes, knowledge) , which can be consonant or dissonant to each other.
Individuals tend to reduce psychological discomfort (produced if the Dissonance is of a strong magnitude) by changing / adding consonant cognitions, or changing its importance.
When reducing dissonance, one tends to use the easiest way
M I attempts to create dissonance within the patient, which is then used to encourage the patient to consider pros and cons of behaviour

Why do people change? How do people change?
Change occurs naturally Treatments facilitate the natural process of change; formal interventions imitate natural change
Brief Interventions Effects: A little counselling can lead to significant change
Dose Effects: Brief interventions as effective as longer ones.
Hope: people who believe that they are likely to change, do so. Counselor effects: characteristics of therapist associated with success in treatment (empathy). This style is manifested early in treatment.

What triggers Change?

Willingness/ importance Ability/ how to do it, solutionsReadiness / priorities
-All these three elements can be sources of the “yes but…” dilemma, which is a manifestation of ambivalence
-People usually get stuck by this inner contradictions, they feel two ways about it (ambivalence)
-To make change effective and possible, people need to explore their contradictions (between present behavior and future outcomes or desires), and to connect it with something valuable and important.

What could “diet” mean?
• Imagine that your family physician have just diagnosized you a diabetes and tells you to do a diet:
6 meals a day, low fat and no rapid absorption carbohydrates
• Brain storming sharing with your neighbour what ideas and feelings appear in your mind when you think about this diet and your life. Just one or two words for each idea without explanation.1 minute

What could “diet” mean?
Restrictions
Dominated by diabetesNot enjoying
meals
Eat without apetite
Apetite and not to eat
Health
No change
Better control
DifficultiesBeing fit

AmbivalenceNo change
Ideas and feelings about:positive aspects of present
behaviournegative aspects of new
behaviour
Change

AmbivalenceNo change
Ideas and feelings about:positive aspects of present
behaviournegative aspects of new
behaviourDifficulties of changing
ChangeIdeas and feelings about:negative aspects of
present behaviour

AmbivalenceNo change
Ideas and feelings about:positive aspects of present
behaviournegative aspects of new
behaviourDifficulties of changing
ChangeIdeas and feelings about:negative aspects of
present behaviourpositive aspects of new
behaviour

What happens with ambivalence when we give advice?
We place ourselves in the change side of ambivalenceWe tell the patient what to do
“Psychological reactance”.Yes, but …
The position of the patient is in part the result of a lot of advices they have listened to.

What is the problem if the patient tells aspects against changing?
• Self perception theory (Bem):We believe in what we say.
• It is difficult for me to control myself.• It is difficult when you have to have meals outside!• I have almost no time for it.• When I finish lunch, I have to come back to work. And
in the evenings, I feel so tired that I don’t want to go for a walk.

What do patients tell?

Change-Talk Effects
What people say about change is important:-Statements that reflect motivation /commitment to
change do predict subsequent behaviour-Arguments against change (resistance) make it less likely
to occur-Both types of talk can be influenced by the counsellor.

Changing talk
– NeedsI can´t breath.
– ReasonsIf I reduce my weight I will have less pain in my knees.
– DesiresI wish I could control my appetite.
– AbilitiesI did it before.

Changing talk
NeedsReasonsDesiresAbilities
Compromise talk-I´ll try to do it
Taking steeps- I am reducing my cigarettes
Behaviour change

Change/sustained talk during interview and change plan
Timothy R. Apodaca ICMI, Stockholm 2010

Motivational interviewingIs a collaborative guiding method,person centered,to elicit and strength motivation to change.
Guiding ≠ directing ≠ followingWorking with their ideas and targetsMotivation is built with their ambivalenceWe work in the way of improving their health

The basis of motivational interviewing
• Listen to your patient– Solutions are inside them.
• Understand your patient motivations– Only their arguments could move them.
• Resist the “righting reflex” – When we try to correct we generate resistance.
• Empower your patient– Is the one that is going to make the effort.

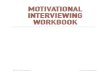
Pubmed citations by years

Results comparing MI
Lundahl B, Burke BL. The effectiveness and applicability of motivational interviewing: a practice-friendly review of four
meta-analyses. J Clin Psychol. 2009 Nov;65(11):1232-45. Targeted outcomes included:• Substance use (tobacco, alcohol, drugs, marijuana)• Health related behaviors (diet, exercise)• Engagement in treatment variables

Results comparing MI
• Lundahl B, Burke BL. The effectiveness and applicability of motivational interviewing: a practice-friendly review of four meta-analyses. J Clin Psychol. 2009 Nov;65(11):1232-45.
Group of comparison Effect size(1=standard deviation)
CI p
Weak (Waiting list, treatment as usual, written materials )
0.28 0.22-0.34 <0.001
Strong(12-step program or cognitive behavioral therapy)
0.09 -0.01-0.18 0.080

What for?
Sune Rubak, Annelli Sandbæk, Torsten Lauritzen and Bo Christensen. Motivational interviewing: a systematic review and meta-analysis. British Journal of General Practice, 55: 513, pp. 305-312

Is it suitable in a primary health care setting?

What can we do in ten minutes? . Ask open-ended questions. Listen with empathy. Understand the patients’ motivations. Elicit change talk
…and in a little more time, maybe some other day…
. Hear a commitment?
. Help in a change plan?
. Agree the follow-up plan?
. Prevent relapse/supervise change behaviour?

Four strategies(OARS)
. Ask Open-ended questions
. Affirm the patient
. Do Reflective listening
. Make Summaries

Open-ended questions
. What is your behaviour like?
. How do you feel about it?
. What happened/could happen when you/if you tried to?
. Which advantages/disadvantages do you see in…?
. How important is it to you?
. What should happen that would make you consider a change?
. Understand (with empathy) the patients’ motivations
. Elicit change talk

Affirmation . Listen carefully to what the patient says: they may have succeed, they may have strong abilities, they may be willing to change, they may have a good plan, they may know what it’s all about…
Tell them!!!
…it really empowers your patient…

Reflective listening . Try to evoke their reasons, their abilities, their desires, their needs, maybe their commitment…
Pick up the flowers and give them!!!
…that’s the energy that’s going to make them move…

Summaries
. Put all the information together, it will help you to clarify and understand your patient better, and give it back
…then ask what now?
…it may lead them to move forwards…

And then…?
. Agreeing a change plan and a follow-up must be done with the same collaborative, evocative and autonomy supportive spirit
…and if relapse occurs? …more of the same: “normalize”, listen with empathy, try to understand, ask for the next step and leave the door open!

What about feedback?
. Giving information is sometimes useful, it may give the patient reasons and needs to change…but first knock on the door!
…and all those scales and rulers, how do I use them?
. They are a good way to elicit change talk; you can ask how willing the patient is, how confident, which degree of commitment…

Getting back to reality… . Very often we have…
.. Other matters to talk about .. More than just one target behaviour .. Less time than we would like. What if I’m tired?
. First agree an agenda
. Let them choose which target behaviours are affordable
. We are in primary health care: we always have time to meet again or choose another day!